Embed Size (px)
Citation preview

MOTILITY MOTILITY DISORDERS OF DISORDERS OF
ESOPHAGUSESOPHAGUS
PROF DR OLCAY ALVERPROF DR OLCAY ALVERCerrahpaşa Medical Faculty, Cerrahpaşa Medical Faculty,
Department of General SurgeryDepartment of General Surgery

MOTILITY MOTILITY DISORDERS OF DISORDERS OF
ESOPHAGUSESOPHAGUS
PROF DR OLCAY ALVERPROF DR OLCAY ALVERCerrahpaşa Medical Faculty, Cerrahpaşa Medical Faculty,
Department of General SurgeryDepartment of General Surgery

MANOMETRIC FEATURES OF MANOMETRIC FEATURES OF ACHALASIAACHALASIA
1) APERISTALSIS or 1) APERISTALSIS or HYPOPERISTALTISMHYPOPERISTALTISM (incoordinated,feeble,simultaneous,and (incoordinated,feeble,simultaneous,and repetetive peristaltic pattern within the 2/3 of repetetive peristaltic pattern within the 2/3 of esophageal body)esophageal body)
2)BASAL HYPERTONICITY OF LES2)BASAL HYPERTONICITY OF LES ((pressure>45mmHgpressure>45mmHg))
3)INCOMPLETE RELAXATION OF 3)INCOMPLETE RELAXATION OF LES IN RESPONSE TO LES IN RESPONSE TO SWALLOWINGSWALLOWING (<70%)(<70%)


NEUROPATHOLOGYNEUROPATHOLOGY OF OF ACHALASIA ACHALASIA
Denervation of PRE-GANGLIONIC Denervation of PRE-GANGLIONIC CHOLINERGIC NERVE supply to CHOLINERGIC NERVE supply to esophagusesophagus
Denervation of INHIBITORY( relaxing NON-Denervation of INHIBITORY( relaxing NON-ADRENERGIC,NON-CHOLINERGIC) nerves ADRENERGIC,NON-CHOLINERGIC) nerves to LESto LES
Absence or degeneration of GANGLION Absence or degeneration of GANGLION CELLS OF AUERBACH’S MYENTERIC CELLS OF AUERBACH’S MYENTERIC PLEXUSPLEXUS
Ultrastructural alterations of VAGUS Ultrastructural alterations of VAGUS NERVE(WALLERIAN DEGENERATION)NERVE(WALLERIAN DEGENERATION)
Decreased and distorted motor cells of Decreased and distorted motor cells of VAGAL DORSAL NUCLEUS in brainstemVAGAL DORSAL NUCLEUS in brainstem


FUNCTIONAL NEUROPHARMACOLOGY OF FUNCTIONAL NEUROPHARMACOLOGY OF ACHALASIAACHALASIA
Supersensitivity (excessive motor response)of LES to Supersensitivity (excessive motor response)of LES to CHOLINERGIC drugsCHOLINERGIC drugs-CANNON’S LAW of DENERVATION -CANNON’S LAW of DENERVATION SUPERSENSITIVITYSUPERSENSITIVITY
Supersensitivity of LES to Supersensitivity of LES to GASTRINGASTRIN EDROPHONIUMEDROPHONIUM (anti-cholinesterase)↑ LES pressure(=post-gn. (anti-cholinesterase)↑ LES pressure(=post-gn.
Cholinergic nerves to LES are intact)Cholinergic nerves to LES are intact) CHOLECYSTOKININCHOLECYSTOKININ invokes a paradoxal excitatory response of invokes a paradoxal excitatory response of
LES (=dysfunction of post-gn. inhibitory /non-adr +non-Ch LES (=dysfunction of post-gn. inhibitory /non-adr +non-Ch nerves)nerves)
Marked ↓ in Marked ↓ in VIP nergic nerveVIP nergic nerve fibers and fibers and NEUROPEPTID-YNEUROPEPTID-Y (neurotransmitters of LES relaxation)(neurotransmitters of LES relaxation)
Marked ↓ in Marked ↓ in NITRINERGIC NEURONSNITRINERGIC NEURONS(=↓ NO (=↓ NO concentration=inhibitory neurotransmitter)concentration=inhibitory neurotransmitter)
ACHALASIA=NİTRİNERGİC NEURONITIS,AUTO-İMMUNE ACHALASIA=NİTRİNERGİC NEURONITIS,AUTO-İMMUNE DIS.?DIS.?

SYMPTOMS OF SYMPTOMS OF ACHALASIAACHALASIA
1)DYSPHAGIA:80-100% 1)DYSPHAGIA:80-100% paradoxal paradoxal dysphagia; adoption of certain manoevres to dysphagia; adoption of certain manoevres to facilitate swallowing; odynophagiafacilitate swallowing; odynophagia
2)REGURGITATION : 70% 2)REGURGITATION : 70% undigested undigested food,foamy mucoid saliva ; nocturnal food,foamy mucoid saliva ; nocturnal regurgitation,and aspiration into the respiratory regurgitation,and aspiration into the respiratory tract; halitosis, foul eructationtract; halitosis, foul eructation
3)WEIGHT LOSS : 40% 3)WEIGHT LOSS : 40% sitophobia; sitophobia; odynophagia; anemia ; avitaminosis ;cachexiaodynophagia; anemia ; avitaminosis ;cachexia
4)CHEST PAIN : 30% 4)CHEST PAIN : 30% early stage;vigorous early stage;vigorous achalasia :odynophagiaachalasia :odynophagia


DIAGNOSIS OF DIAGNOSIS OF ACHALASIAACHALASIA
RADIOLOGICAL FEATURESRADIOLOGICAL FEATURES Proximal esophageal dilatationProximal esophageal dilatation Smoothly tapered distal endSmoothly tapered distal end Fluid level in post mediastinumFluid level in post mediastinum Absence of gastric air bubbleAbsence of gastric air bubble ENDOSCOPIC FEATURESENDOSCOPIC FEATURES Esophageal dilatation+retained foodEsophageal dilatation+retained food Retention esophagitisRetention esophagitis Passage of scope through resistant LES produces Passage of scope through resistant LES produces
characteristic “pop” sensationcharacteristic “pop” sensation Endoscopic biopsy excludes esophageal caEndoscopic biopsy excludes esophageal ca MANOMETRIC FEATURESMANOMETRIC FEATURES



ACHALASIA

DIFFERENTIAL DIAGNOSIS OF ACHALASIADIFFERENTIAL DIAGNOSIS OF ACHALASIA
SYMPTOSYMPTOM+ SIGNM+ SIGN
achalasıaachalasıa Diffuse Diffuse spasmspasm
Vigorous Vigorous achalasiaachalasia
PainPain
obstructioobstructionn
RegurgitaRegurgitat.t.
RetentionRetention
UncommoUncommonn
AlwaysAlways
CommonCommon
FrequentFrequent
Almost Almost alwaysalways
SometimeSometimess
RareRare
NeverNever
FrequentFrequent
Nearly Nearly alwaysalways
FrequentFrequent
FrequentFrequent
DilatationDilatation
SpasmSpasmCommonCommon
UncommoUncommonn
NeverNever
FrequentFrequentOccasionaOccasionall
CommonCommon


TREATMENT OF SPASTIC MOTOR TREATMENT OF SPASTIC MOTOR DISORDERS OF ESOPHAGUSDISORDERS OF ESOPHAGUS
PHARMACOTHERAPYPHARMACOTHERAPY SMOOTH MUSCLE RELAXANTSSMOOTH MUSCLE RELAXANTS NITRATESNITRATES ( ( ISOSORBIDE DINITRATE)ISOSORBIDE DINITRATE) CALCIUM-CHANNEL BLOCKERSCALCIUM-CHANNEL BLOCKERS
(NIFEDIPINE,VERAPAMIL)(NIFEDIPINE,VERAPAMIL) ANTICHOLINERGICS , SILDENAFİLANTICHOLINERGICS , SILDENAFİL HYDRALAZINEHYDRALAZINE(ARTERİAL MUSCLE RELAXANT)(ARTERİAL MUSCLE RELAXANT) PSYCHOTROPIC AGENTSPSYCHOTROPIC AGENTS BOTULİNUM TOXİNBOTULİNUM TOXİN NON-PHARMACOLOGIC MEASURESNON-PHARMACOLOGIC MEASURES REASSURANCE, BEHAVIOR MODIFICATION/BIOFEEDBACKREASSURANCE, BEHAVIOR MODIFICATION/BIOFEEDBACK ESOPHAGEAL DILATATIONESOPHAGEAL DILATATION OPEN OR LAPAROSCOPIC MYOTOMY OPEN OR LAPAROSCOPIC MYOTOMY ±± PARTIAL FUNDOPLICATION PARTIAL FUNDOPLICATION
( H E L L E R + D O R procedure)( H E L L E R + D O R procedure)






DIFFUSE ESOPHAGEAL DIFFUSE ESOPHAGEAL SPASMSPASM
Hypertrophy and spasms of smooth musle layers Hypertrophy and spasms of smooth musle layers of the esophageal body,Wallerian degeneration of the esophageal body,Wallerian degeneration of the vagal fibers,denervation supursensitivity of the vagal fibers,denervation supursensitivity to cholinergic compoundsto cholinergic compounds
MAJOR CLINICAL SYMPTOMSMAJOR CLINICAL SYMPTOMS INTERMITTENT SUBSTERNAL PAIN-INTERMITTENT SUBSTERNAL PAIN-variesvaries fromfrom
slight discomfort to severe spasmodic pain slight discomfort to severe spasmodic pain mimicking ANGINA PECTORIS with radiation to mimicking ANGINA PECTORIS with radiation to back,jaws,arms aggravated by emotional back,jaws,arms aggravated by emotional upsets,very hot,cold,carbonated drinksupsets,very hot,cold,carbonated drinks
DYSPHAGIA / HEARTBURN /ODYNDPHAGIA / no DYSPHAGIA / HEARTBURN /ODYNDPHAGIA / no weight lossweight loss



MANOMETRIC FEATURES OF MANOMETRIC FEATURES OF DIFFUSE ESOPHAGEAL SPASMDIFFUSE ESOPHAGEAL SPASM
Synchronous,non-spesific , Synchronous,non-spesific , repetetive(at least three peaks) repetetive(at least three peaks) peristaltic contractions with peristaltic contractions with prolonged duration (>6 sec),high-prolonged duration (>6 sec),high-amplitude (>120mm)amplitude (>120mm)
Failure of hypertensive LES to relax Failure of hypertensive LES to relax completely in 30% of the casescompletely in 30% of the cases
Denervation supersensitivity to Denervation supersensitivity to cholinergic,anticholinesterase,ergonocholinergic,anticholinesterase,ergonovine compoundsvine compounds

DIAGNOSIS OF DIFFUSE ESOPHAGEAL DIAGNOSIS OF DIFFUSE ESOPHAGEAL SPASM SPASM
RADIOLOGICAL FEATURESRADIOLOGICAL FEATURES Delayed esophageal transit due to segmental Delayed esophageal transit due to segmental
spasms, areas of narrowing , irregular spasms, areas of narrowing , irregular uncoordinated peristalsis described as uncoordinated peristalsis described as
“ “ C U R L I N GC U R L I N G “ , “ “ , “ C O R K S C R E WC O R K S C R E W “ or “ or “ “ R O S A R Y B E A D ESOPHAGUSR O S A R Y B E A D ESOPHAGUS “ and “ and “ “ P S E U D O D İ V E R T I C U L O S I SP S E U D O D İ V E R T I C U L O S I S “ “
involving the two-thirds of the esophageal bodyinvolving the two-thirds of the esophageal body with coexisting small sliding hiatal hernia, with coexisting small sliding hiatal hernia,
epiphrenic diverticulaepiphrenic diverticula ENDOSCOPY-ENDOSCOPY- Normal unless reflux esophagitis or Normal unless reflux esophagitis or
other lesion is associatedother lesion is associated MANOMETRYMANOMETRY



TREATMENT OF DIFFUSE TREATMENT OF DIFFUSE ESOPHAGEAL SPASMESOPHAGEAL SPASM
MEDICAL-MEDICAL- Long-acting nitrates,isosorbide,ca-Long-acting nitrates,isosorbide,ca-
channel channel blockers(nifedipine,verapamil)blockers(nifedipine,verapamil)
Bougienage,pneumatic dilatationBougienage,pneumatic dilatation SURGICAL- long esophageal SURGICAL- long esophageal
myotomy(Long HELLER operation)myotomy(Long HELLER operation) Extending from LES to aortic arch + Extending from LES to aortic arch +
anterior hemifundoplication(DOR anterior hemifundoplication(DOR procedure )procedure )


HYPERCONTRACTING HYPERCONTRACTING ESOPHAGUSESOPHAGUS
““NUTCRACKER” / HYPERTENSIVE NUTCRACKER” / HYPERTENSIVE ESOPHAGUSESOPHAGUS
Hıgh-amplitude contractions(>Hıgh-amplitude contractions(>180 180 mmHg)mmHg) Prolonged duration contraction (>Prolonged duration contraction (>66 sec) sec) Normal peristalsisNormal peristalsis HYPERTENSIVE LESHYPERTENSIVE LES Hıgh resting LES pressure (>Hıgh resting LES pressure (>4545mmHg)mmHg) Normal or incomplete LES relaxationNormal or incomplete LES relaxation Normal peristalsisNormal peristalsis



HYPOCONTRACTING HYPOCONTRACTING ESOPHAGUSESOPHAGUS
INEFFECTIVE ESOPHAGEAL MOTILITYINEFFECTIVE ESOPHAGEAL MOTILITY NONSPECIFIC ESOPHAGEAL MOTOR DYSFUNCTIONNONSPECIFIC ESOPHAGEAL MOTOR DYSFUNCTION FREQUENT NON-PROPULSIVE OR FREQUENT NON-PROPULSIVE OR
RETROGRADE CONTRACTIONS (RETROGRADE CONTRACTIONS (30%30% or more) or more)
LOW-AMPLITUDE CONTRACTIONS (< LOW-AMPLITUDE CONTRACTIONS (< 3030mmHg)mmHg)
PROLONGED DURATION CONTRACTION(>PROLONGED DURATION CONTRACTION(>66 Sec) Sec) BODY PERISTALSIS WITH NORMAL LESBODY PERISTALSIS WITH NORMAL LES
LOW RESTING LES PRESSURE (< LOW RESTING LES PRESSURE (< 1010mmHg )mmHg )

PATHOPHYSIOLOGY OF PATHOPHYSIOLOGY OF SCLERODERMASCLERODERMA
NEURAL DYSFUNCTION OF ESOPHAGUSNEURAL DYSFUNCTION OF ESOPHAGUS Normal sphincteric response to cholinergic drugs but not to Normal sphincteric response to cholinergic drugs but not to
gastrin or a cholinesterase inhibitor/ loss of intrinsic Ach gastrin or a cholinesterase inhibitor/ loss of intrinsic Ach mechanism(?)mechanism(?)
RAYNAUD’s phenomenon usually presentRAYNAUD’s phenomenon usually present Functional abnormalities precede morphologic changes by Functional abnormalities precede morphologic changes by
light microscopylight microscopy OTHER POSSIBLE PATHOGENIC MECHANISMS- OTHER POSSIBLE PATHOGENIC MECHANISMS- abnormal abnormal
fibrotic process ; marked smooth musle atrophy with fibrotic process ; marked smooth musle atrophy with fibrous replacement / primary muscle disease:smooth fibrous replacement / primary muscle disease:smooth muscle atrophy with aperistalsis / evidence lacking muscle atrophy with aperistalsis / evidence lacking vascular abnormality / Raynaud’s phenomenon /prolonged vascular abnormality / Raynaud’s phenomenon /prolonged warming time after swallow of cold boluswarming time after swallow of cold bolus



CLINICAL FEATURES OF CLINICAL FEATURES OF SCLERODERMASCLERODERMA
SYMPTOMS: SYMPTOMS: DYSPHAGIA / HEARTBURN / DYSPHAGIA / HEARTBURN / REGURGITATION / SKIN + SYSTEMIC REGURGITATION / SKIN + SYSTEMIC CHANGES OF SCLERODERMA / CHANGES OF SCLERODERMA / RAYNAUD’S PHENOMENONRAYNAUD’S PHENOMENON
SIGNS: SIGNS: SKIN CHANGES / RAYNAUD’S SKIN CHANGES / RAYNAUD’S PHENOMENON , PHENOMENON , C R E S T SYNDROMEC R E S T SYNDROME
CCalcinosis cutis alcinosis cutis R Raynaud aynaud EEsophageal sophageal involvement involvement S Sclerodactyly clerodactyly TTelangiectasiaelangiectasia


DIAGNOSIS OF DIAGNOSIS OF SCLERODERMASCLERODERMA
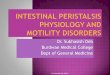
RADIOGRAPHYRADIOGRAPHY: aperistalsis of distal 2/3 : aperistalsis of distal 2/3 esophagus/mild dilatation / gastroesophageal esophagus/mild dilatation / gastroesophageal reflux / possible peptic stricture + shortening reflux / possible peptic stricture + shortening of distal esophagus/impaired esophageal of distal esophagus/impaired esophageal clearenceclearence
MANOMETRYMANOMETRY:Upper sphincter+ 1/3 :Upper sphincter+ 1/3 esophagus-NORMAL / feeble or no peristalsis esophagus-NORMAL / feeble or no peristalsis (<30mmHg)in distal 2/3 esophagus / feeble or (<30mmHg)in distal 2/3 esophagus / feeble or sphincter(LES absent lower esophageal p-<10 sphincter(LES absent lower esophageal p-<10 mmHg )mmHg )
ENDOSCOPYENDOSCOPY:mildly dilated,tubular :mildly dilated,tubular esophagus /distal esophagus and LES remains esophagus /distal esophagus and LES remains open/ free reflux /peptic esophagitis with open/ free reflux /peptic esophagitis with possible stricture formation(60%)possible stricture formation(60%)


ESOPHAGEAL SCLERODERMAESOPHAGEAL SCLERODERMA(LONG TUBULER STRICTURE) (LONG TUBULER STRICTURE)

TREATMENT OF TREATMENT OF SCLERODERMASCLERODERMA
MEDICAL TREATMENTMEDICAL TREATMENT Proton pump inhibitors/ prokinetic drugs Proton pump inhibitors/ prokinetic drugs
(metoclopramide,domperidon)(metoclopramide,domperidon) SURGICAL TREATMENTSURGICAL TREATMENT Combined gastroplasty+antireflux Combined gastroplasty+antireflux
procedureprocedure(COLLIS-NISSEN (COLLIS-NISSEN ±± BELSEY MARK IV ) BELSEY MARK IV ) / DISTAL / DISTAL ESOPHAGECTOMY replacement with a ESOPHAGECTOMY replacement with a colonic or an isoperistaltic jejunal segmentcolonic or an isoperistaltic jejunal segment

ESOPHAGECTOMY + COLONIC ESOPHAGECTOMY + COLONIC INTERPOSITIONINTERPOSITION