Embed Size (px)
Citation preview

Morphometric Evaluation andNonclassical Criteria for theDiagnosis of HPV Infection andCytological Atypia in CervicalSamplesDandara Emery Morais Sana, M.SC.,1
Priscila Mayrink de Miranda, M.SC.,2
Bruna Caroline Vieira Pitol, M.SC.,1 Mariana Soares Moran,1
Nayara Nascimento Toledo Silva,1
Ismael Dali Cotrim Guerreiro da Silva, PH.D.,3
Rita de C�assia Stocco, PH.D.,2 Willy Becak, PH.D.,2
Ang�elica Alves Lima, PH.D.,1 and Cl�audia Martins Carneiro, PH.D.4,5*
Herein, we evaluated cervical samples from normal tissue orHPV-infected tissue, to determine if the relative nuclear/cyto-plasmic ratio (NA/CA) and the presence of nonclassical cytolog-ical criteria are a novel cytological criterion for the diagnosisof HPV. Significantly, larger NA/CA ratios were found for theHPV2ATYPIA1 and HPV1ATYPIA1 groups compared withHPV2ATYPIA2 group, regardless of collection method. Forthe samples collected with a spatula, only three samples fromthe HPV2ATIPIA2 group showed four or more nonclassical
parameters (i.e., were positive), while a larger number of thesamples in the HPV2ATYPIA1, HPV1ATYPIA2, andHPV1ATYPIA1 groups were positive (13, 4, and 13 samples,respectively). Among those collected with a brush, no sampleshowed four or more nonclassical criteria in theHPV2ATYPIA2 group, while a number of samples were posi-tive in the HPV2ATYPIA1, HPV1ATYPIA2, andHPV1ATYPIA1 groups (4, 3, and 4 samples, respectively).HPV infection was associated with significant morphometricalchanges; no increase in the NA/CA ratio was found in theHPV1ATYPIA- samples, compared with the HPV2ATIPIA2samples collected with either a spatula or a brush. In conclusion,by including nonclassical cytological criteria into the patientdiagnosis, we were able to reduce the number of false negativeand false positive HPV diagnoses made using conventionalcytology alone. Diagn. Cytopathol. 2013;41:785–792. VC 2013
Wiley Periodicals, Inc.
Key Words: HPV; cervix-vaginal cytology; morphometry; non-classical criteria; molecular biology
A cytopathological diagnosis is based on the recognition
of morphological criteria within different cell types.
Despite the fact that most criteria are well established, an
embodiment of literature has demonstrated the influence
of marked interobserver and intraobserver variability.
Estimates have attributed up to 20% of false-negative
results to microscopic analysis error, with interobserver
discordance ratios varying from 10 to 100%.1,2 Koilocyto-
sis is described in the literature as a pathognomonic
1Departamento de An�alises Cl�ınicas, Escola de Farm�acia,Universidade Federal de Ouro Preto (UFOP), Ouro Preto, MG, Brasil
2Laborat�orio de Gen�etica, Instituto Butantan, S~ao Paulo, SP, Brasil3Departamento de Ginecologia, Universidade Federal de S~ao Paulo
(UNIFESP), S~ao Paulo, SP, Brasil4Laborat�orio de Imunopatologia, N�ucleo de Pesquisas em Ciencias
Biol�ogicas, ICEB II, Universidade Federal de Ouro Preto (UFOP), OuroPreto, MG, Brasil
5Laborat�orio de Pesquisas Cl�ınicas, CiPharma (Programa deP�os-Graduac~ao em Ciencias Farmaceuticas), Escola de Farm�acia,Universidade Federal de Ouro Preto (UFOP), Ouro Preto, MG, Brasil
Contract grant sponsor: Fundac~ao de Amparo �a Pesquisa do Estadode Minas Gerais (FAPEMIG); contract grant sponsor: Conselho Nacionalde Pesquisa (CNPq); contract grant sponsor: Universidade Federal deOuro Preto, Brazil.
*Correspondence to: Cl�audia Martins Carneiro, PH.D., Escola deFarm�acia, Rua Costa Sena, 171, Centro, Ouro Preto, MG, Brasil, 35400-000. E-mail: [email protected]
Received 14 July 2011; Revised 27 September 2012; Accepted1 January 2013
DOI: 10.1002/dc.22955Published online 30 April 2013 in Wiley Online Library
(wileyonlinelibrary.com).
VC 2013 WILEY PERIODICALS, INC. Diagnostic Cytopathology, Vol. 41, No 9 785

criterion for HPV diagnosis, as it is a marker of viral ac-
tivity. Many authors stress, however, that this is not the
most frequent marker found in cervix-vaginal smears.3,4
New nonclassical or secondary morphological criteria
for HPV diagnosis have been proposed to increase the
sensitivity of the standard Papanicolaou test.5
Additionally, computerized image analyses, with their
high precision and reproducibility, have been employed in
the last decades to eliminate the diagnostic variability in
cytological and histopathological samples. Such methods
target the bidimensional measurement of parameters, such as
cellular and nuclear area (NA), perimeter, and mean diame-
ter, beyond the recognition of their shapes or staining inten-
sity.6,7 Thus, digital morphometry provides the observer
with precise, quantitative data that allow the construction of
a database of diverse parameters to characterize the cells as
normal, preneoplastic, or neoplastic. In addition, the system
is capable of detecting subtle variations in cell shape, size,
and/or texture that are mostly invisible to the human eye,
even by light, and electron microscopy.8
This study investigates novel criteria: the quantitative
assessment of NA, cytoplasmic area (CA), the nuclear/
cytoplasmic ratio (NA/CA), and a series of nonclassical
cytological criteria for HPV diagnosis. These criteria have
the potential of providing information not detected by
conventional cytology and, as a result, may be able to
explain the discordant results between the molecular and
morphological approaches.
Methods: Patient Cohort and Sample Collection
In total, 569 cervix samples were evaluated from 18- to
75-year-old women living in and around Ouro Preto, Bra-
zil. The samples for identification and typing of HPV
were collected between April 2008 and July 2010 by
physicians and nurses from the family health team
(Federal Government Health Care Program) of Ouro
Preto. Sample material was either collected with the aid
of a spatula to collect squamous cells, or with a brush to
collect cells of the squamous-columnar junction.
After collection, the brushes with endocervix material
were placed in tubes containing 1 mL of collection buffer
and disconnected from the handle. The samples were
refrigerated between 2 and 10�C, stored at 280�C, and
sent to the Laboratory of Genetics and Viral Oncogenesis
of the Butantan Institute, S~ao Paulo, for viral research.
The cervical smears were immediately fixed in 95% etha-
nol and sent to the Laboratory of Clinical Cytology of the
School of Pharmacy. They were analyzed using the Papani-
colaou method,9 dehydrated in xylene, and mounted in
Entellan. Microscopic evaluation was done using the 103
and 403 objectives, and the samples were classified accord-
ing to the Bethesda System for Cervix-Vaginal Cytology.10
Considering the results of virus research and inclusion/
exclusion criteria, the samples were divided into four
groups of 20 samples per group (Fig. 1).
For the HPV2ATYPIA2 and HPV1ATYPIA2
groups, cervix smears were selected based on the most
frequent microorganisms identified during the Papanico-
laou test (e.g., Lactobacillus sp., Gardnerella vaginalis,
Candida sp., and Trichomonas vaginalis). In the
HPV2ATYPIA1 and HPV1ATYPIA1 groups, the sam-
ples were selected randomly.
Morphometric Analysis
After cytological analysis, selected samples with satisfac-
tory technical conditions were used for image capture.
Fig. 1. Distribution of the groups analyzed in this study, based on viral research and results from the Papanicolaou test (n520 per group). TheHPV2ATYPIA2 group is represented in white boxes; the HPV2ATYPIA1 group is in light gray; the HPV1ATYPIA- group is in dark gray; theHPV1ATYPIA1 group is in black.
Diagnostic Cytopathology DOI 10.1002/dc
SANA ET AL.
786 Diagnostic Cytopathology, Vol. 41, No 9

Included samples had to be homogeneous, well estab-
lished, and with good representation of the squamous-co-
lumnar junction. Samples with inadequate color,
overlapping, and/or crowded cells were excluded. Sixty
microscopic fields per sample were captured (30 by each
sampling procedure) using conventional bright field mi-
croscopy, a 103 ocular, and a 403 objective, by a Leica
DFC340FX digital microcamera attached to a Leica
DM5000B microscope.
The morphometric analysis of cells was performed
using Image J software for Windows Vista 1:43. One cell
presenting clear nuclear and cytoplasmic boundaries per
field was evaluated for each sample. The outlines were
traced using a mouse, yielding the NA and the CA. The
resulting NA/CA ratio was then calculated for each cell,
amounting to 60 cell measurements for each of the 20
samples, or 1,200 cell measurements per group.
The same images acquired for morphometric analysis
were evaluated for the presence of HPV on the screen of
a computer with Pentium Dual Core Intel 2.0 GHz, 3.0
GB RAM with a 15.4 inch monitor. Nonclassical cytolog-
ical criteria were used to identify the presence of HPV
and included binucleation or multinucleation, mild dys-
keratosis, keratinization, hyperchromatic nucleus, smudge
nucleo, spindle nucleo, mild koilocytosis, perinuclear
halo, karyorrhexis, keratohyalin-like granules, condensa-
tion of filaments, anucleate squames, ghost cells, spindle
cells, macrocytes, and koilocytotic parabasal cells.
Statistical Methods
The normality of the data was tested according to the
Kolmogorov-Smirnov, D’Agostino and Pearson, and
Shapiro-Wilk methods, followed by a Student’s t-test for
parametric samples and the Mann Whitney test for non-
parametric samples. These were analyzed by GraphPad
Prism 5 software with a confidence interval of 95%.
Results
Morphometric Evaluation
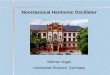
Figure 2 shows the results obtained for the NA/CA ratio
for the different categories of microrganisms (Lactobacil-lus sp., G. vaginalis, Candida sp., and T. vaginalis). This
set of data did not show a normal distribution and the
applied tests gave a significant difference of P<0.05
between the samples collected with a spatula or a brush
between T. vaginalis and Lactobacillus sp., or T. vagina-lis and G. vaginalis.
The mean and standard deviations of the NA measure-
ment, the CA measurement, and the NA/CA ratio
obtained for the squamous cells (collected with either the
spatula or the brush) are shown in Tables I and II.
For the cells found in the region collected with a spat-
ula, the statistical tests pointed to a normal distribution
and a homogeneous variance between groups. The
HPV2ATYPIA1 and HPV1ATYPIA1 groups had a
higher NA compared with the HPV2ATYPIA2 and
Fig. 2. Morphometrical analysis of the nuclear/cytoplasm area ratio insquamous cells sampled with the aid of a spatula or with a brush in theHPV2ATYPIA2 group, considering the different microorganisms foundin the cervix flora. Letters “a,” “b,” “c,” and “d” represent significantdifferences between the groups of Lactobacillus sp., G. vaginalis, Can-dida sp., and T. vaginalis.
Table I. Nuclear Area, Cytoplasm Area, and Nuclear/Cytoplasm Area Ratio Observed in Squamous Cells After Sampling with a Spatula in the Differ-ent Groups.
HPV2ATYPIA2 HPV2ATYPIA1 HPV1ATYPIA2 HPV1ATYPIA1
Nuclear Area (NA) 81.73 6 10.59 97.64a,c 6 19.95 78.20 6 1921 88.39a,c 6 14.26Cytoplasm Area (CA) 235.86c 6 44.30 217.58 6 41.47 202.64 6 37.49 230.73c 6 49.36NA/CA 0.04 6 0.01 0.05a 6 0.02 0.04 6 0.02 0.05a 6 0.01
The letters “a”, “b”, “c” and “d” represent significant differences between HPV2ATIPIA2, HPV2ATIPIA1, HPV1ATIPIA2 HPV1ATIPIA1groups, respectively.
Diagnostic Cytopathology DOI 10.1002/dc
HPV DIAGNOSES USING CONVENTIONAL CYTOLOGY
Diagnostic Cytopathology, Vol. 41, No 9 787

HPV1ATYPIA2 groups. With respect to CA, the
HPV2ATYPIA2 and HPV1ATYPIA1 groups had
higher CA measurements than the HPV1ATYPIA2
group. Overall, the NA/CA ratio was significantly higher
in the HPV2ATYPIA1 and HPV1ATYPIA1 groups
compared with the HPV2ATYPIA2 group.
The cells from the samples collected with a brush also
showed a normal distribution and homogeneous variance
between the groups. The NA measurements were higher
for the HPV2ATYPIA1 group compared with the
HPV2ATYPIA2 and HPV1ATYPIA2 groups, and for
the HPV1ATYPIA1 group compared with the
HPV2ATYPIA2 and HPV1ATYPIA2 groups. With
respect to CA, no significant differences were found
between groups. Accordingly, the NA/CA ratio was
higher in the HPV2ATYPIA1 and HPV1ATYPIA1
groups, compared with the HPV2ATYPIA2 group.
Evaluation of Nonclassical Criteria for theCytologic Diagnostic of HPV Infection
Table III depicts the nonclassical criteria that were used
for the cytologic diagnosis of HPV infection, including
the number of samples in which the respective criterion
was observed, regardless of intensity. Mild diskeratosis,
smudge nucleus, condensation of filaments, spindle cells,
and koillocytotic parabasal cells were not found in either
group. Conversely, binucleation or multinucleation, peri-
nuclear halo, keratohyalin-like granules, anucleate
squames, and ghost cells were observed in most of the
samples in each group, so they are not isolated markers
of HPV infection.
A number of the criteria were associated with specific
groups. Keratinization was only found in the
HPV1ATYPIA1 group, whereas the detection of a spin-
dle nucleus was found in the groups with positive cyto-
logical diagnostics, regardless of presence of virus. The
detection of a hyperchromatic nucleus, mild koilocytosis,
and karyorrhexis were not found in the HPV2ATYPIA2
group. Macrocytes were only observed in samples from
the HPV1ATYPIA1 group.
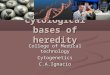
Figure 2 presents the median (dashed line) obtained
from the sum of the number of nonclassical criteria
observed in the samples collected with either the spatula
or brush for all groups evaluated, independent of the in-
tensity for each criterion.
In the region collected by spatula, only three samples
in the HPV2ATYPIA2 group showed four or more non-
classical criterion (i.e., a positive reading), while the other
samples showed three (n58), two (n56), or only one
(n53) nonclassical criteria and were considered negative.
In the HPV2ATYPIA1, HPV1ATYPIA2, and
HPV1ATYPIA1 groups, 13, 4, and 13 samples showed
4 or more nonclassical criteria, respectively.
In the regions collected with a brush, all samples in the
HPV2ATYPIA2 group were negative for nonclassical
criteria. Conversely, in the HPV2ATYPIA1,
HPV1ATYPIA2, and HPV1ATYPIA1 groups, four,
three, and four samples, respectively, showed four or
more nonclassical criteria.
Discussion
The diagnosis of uterine dysplasias and neoplasias is
based on morphological changes, particularly in the cell
nucleus. These changes can include size variation, shape,
and chromatin distribution. In addition to these criteria, it
is also necessary to evaluate the amount of cytoplasm in
relation to the nuclear size, as a nucleus/cytoplasm ratio,
Table II. Nuclear Area, cytoplasm Area, and Nuclear/Cytoplasm Area Ratio Observed in Squamous Cells After Sampling with a Brush in the Differ-ent Groups
HPV2ATYPIA2 HPV2ATYPIA1 HPV1ATYPIA2 HPV1ATYPIA1
Nuclear Area (NA) 82.83 6 14.94 106.96a,c 6 29.55 83.42 6 19.10 109.37a,c 6 41.84Cytoplasm Area (CA) 204.23 6 41.20 207.64 6 51.98 200.91 6 36.09 216.07 6 60.84NA/CA 0.04 6 0.02 0.06a 6 0.03 0.05 6 0.02 0.06a 6 0.03
The letters “a”, “b”, “c” and “d” represent significant differences between HPV2ATIPIA2, HPV2ATIPIA1, HPV1ATIPIA2 HPV1ATIPIA1
groups, respectively.
Table III. Analysis of Nonclassical Criteria Per Sample in theHPV2ATYPIA2, HPV2ATYPIA1, HPV1ATYPIA2, andHPV1ATYPIA1 Groups, Irrespective of Intensity
Nonclassical criteriaHPV2
ATYPIA2
HPV2
ATYPIA1
HPV1
ATYPIA2
HPV1
ATYPIA1
Binucleation orMultinucleation
17 18 18 19
Mild diskeratosis 0 0 0 0Keratinization 0 0 0 2Hyperchromatic
nucleus0 2 3 9
Smudge nucleus 0 0 0 0Spindle nucleus 0 1 0 1Mild koilocytosis 0 6 1 8Perinuclear halo 19 20 20 17Karyorrhexis 0 1 1 4Keratohyalin-like
granules12 19 15 15
Condensation offilaments
0 0 0 0
Anucleate squames 5 7 8 4Ghost cells 3 10 3 6Spindle cells 0 0 0 0Macrocytes 0 0 0 1Koilocytotic
parabasal cells0 0 0 0
Total 56 84 69 86
Diagnostic Cytopathology DOI 10.1002/dc
SANA ET AL.
788 Diagnostic Cytopathology, Vol. 41, No 9

as this criterion is markedly higher in dysplastic and neo-
plastic cells compared with their normal counterparts.11
The literature has shown that the quantitative analysis
of parameters, such as area, perimeter, roundness, elonga-
tion, major axis length, major axis angle, secondary axis
length, and secondary axis angle, provides reliable prog-
nostic factors and contributes to improving the diagnostic
parameters.12,13 Accordingly, the objective of the present
study was to define the NA, the CA and the NA/CA in
squamous cells of the uterine cervix collected with the
aid of either a spatula or with a brush, or in smears from
HPV-infected and noninfected patients and with or with-
out cellular atypia. Our goal was to identify significant
morphometric changes, which went unnoticed by conven-
tional cytological analysis. Because of its central role in
the etiology of virtually all cases of cervical cancer, HPV
is correctly called a “virtually necessary but generally not
sufficient” cause of cervical cancer. With the exception of
rare HPV-negative cases, cervical cancer arises via the
following distinct and sequential steps: (1) acute infection
with carcinogenic HPV type(s), (2) detectable viral per-
sistence, (3) the development of cervical precancer, and
(4) invasion.12
We compared the morphometric analyses of the differ-
ent categories of microrganisms selected as control
groups (HPV2ATYPIA2). With respect to the cytopa-
thogenesis of T. vaginalis, the literature agrees that as
this microrganism promotes a pronounced inflammatory
process that is difficult to distinguish from a pre-neoplas-
tic lesion. As expected, the samples infected with T. vagi-nalis showed high NA/CA ratios, compared with other
samples.
The smears showed nuclear changes, such as aniso-
karyosis, karyomegaly, nuclear membrane thickening
due to cell degeneration, clumps of chromatin material,
hyperchromacy, and frequent binucleation and
multinucleation.14,15
Regarding the mean values obtained for the NA, CA,
and NA/CA ratios for all of the groups collected with ei-
ther the spatula or the brush, the results showed the exis-
tence of significant morphometric changes in NA of
samples with positive cytology, compared with the sam-
ples with negative cytology, irrespective of the presence
of HPV. In addition, the groups with positive cytological
diagnoses also showed significantly higher NA/CA ratio
in the HPV2ATYPIA2 group.
These results are similar to those of Athanassiadou
et al.,16 who measured the NA/CA in 110 cervix smears
in women aged 18–55 years. These patients had cytologic
diagnoses of NIC I, NIC II, or NIC III associated or not
with the cytopathic effect resulting from HPV infection.
Statistical analyses showed that the increased severity of
the lesion was associated with an increased NA/CA ratio,
irrespective of the presence of HPV, that is, there was no
morphometric differences between the samples in groups
NIC I and NIC I with HPV, NIC II, and NIC II with
HPV, NIC III and NIC III with HPV, and NIC III and
NIC III with HPV and carcinoma.
It is worth stressing that this study addressed only sam-
ples with positive cytological diagnoses (e.g., NIC I, NIC
II, and NIC III), which excludes the possibility of observ-
ing significant morphometric changes between samples
diagnosed as either positive or negative by cytological
analysis. Furthermore, the presence of HPV was deter-
mined using a morphological approach (i.e., cytology),
which has inherent limitations.
The results from this study also confirm previous data
of Cavaliere et al.,17 who studied the NA/CA ratio in 44
smears with koilocytotic changes, classified according to
the World Health Organization (WHO, 1984) and then
evaluated for the presence of HPV antigen using the
peroxidase-antiperoxidase reaction. Statistical analysis in
this study showed that the NA/CA in the control group
was significantly smaller than in the inflamed and NIC
groups, irrespective of the presence of HPV. The inflamed
group also had a significantly smaller ratio than the HPV
antigen-positive and antigen-negative NIC groups.
The second objective of this study was to evaluate the
samples using nonclassical criteria for the detection of HPV
in squamous cells from the uterine cervix. Koillocytosis
and diskeratosis are classical cytological features associated
with HPV effects in genital infections; these are considered
pathognomonic criteria for the diagnosis of HPV infec-
tion.18–20 However, many authors suggest that classical cri-
teria are not those most frequently observed in cytological
preparations and, in spite of being specific, are only moder-
ately sensitive for the HPV diagnosis. For instance, approx-
imately one third of HPV cases would go unnoticed if the
only criteria were koilocytosis and diskeratosis.21
Nonclassical cytological criteria have been suggested to
improve the sensitivity of the cytological detection of
HPV infection (Fig. 3). They are grouped as: (1) slight
nuclear changes (mild hyperchromacy, mild anisocytosis
and binucleation or multinucleation); (2) keratinization
disorders (mild diskeratosis and parakeratosis); (3) kerato-
hyaline-like granules and perinuclear halo, and (4) degen-
erative changes (macrocytes and condensation of
filaments).22 These nonclassical criteria are significantly,
but not independently, associated with HPV infection,
that is, the presence of four or more nonclassical criteria
in the same sample are required to consider it HPV-posi-
tive by cytological examination.23
From 40 samples collected with the aid of a spatula and
previously determined to be HPV-negative by conven-
tional cytological analysis, seven were further found to be
HPV-positive using nonclassical criteria. In turn, three
samples collected with a brush and previously determined
to be HPV-negative were found to be HPV-positive after
Diagnostic Cytopathology DOI 10.1002/dc
HPV DIAGNOSES USING CONVENTIONAL CYTOLOGY
Diagnostic Cytopathology, Vol. 41, No 9 789

Fig. 3. The number of nonclassical criteria observed in individual samples collected either with a spatula or a brush, per group, irrespective of the indi-vidual criterion. Each circle represents one sample in each group. The dashed line corresponds to the median obtained from the sum of the number ofcriteria for all groups evaluated.
Diagnostic Cytopathology DOI 10.1002/dc
SANA ET AL.
790 Diagnostic Cytopathology, Vol. 41, No 9

consideration of nonclassical criteria. These cases repre-
sent an increased HPV diagnosis of 17.5 and 7.5%, after
either spatula or brush collection, respectively.
However, and irrespective of viral research, 40 samples
collected either using a spatula or a brush was previously
determined to be positive, according to conventional cyto-
logical analysis. Of these, 14 samples were found to be
HPV-negative after sampling with a spatula while 32
samples were found to be HPV-negative after sampling
with a brush, representing a decreased accuracy of 35 and
80% for spatula and brush collection, respectively.
These numbers differ slightly from those reported by
Schneider et al.,21 who studied 200 smears from asymp-
tomatic patients with no previous abnormal cytological
diagnostics. One hundred of these patients showed posi-
tive HPV infection, as determined by in situ hybridiza-
tion. The results showed that after inclusion of the
nonclassical diagnostic criteria and cytological examina-
tion, 84 samples were considered to be positive for HPV
infection. This means that from the 200 patients initially
characterized as negative by cytological examination, 92
of them were diagnosed as HPV-positive, yielding a 46%
increase in the frequency of HPV infection by the incor-
poration of nonclassical diagnoses.
In a retrospective study, Cavaliere et al.24 used the same
nonclassical morphological parameters described by
Schneider et al.21 to examine 40 cervix-vaginal smears
with a previous positive diagnosis (NIC, in situ carcinoma,
or invasive carcinoma) that had no evidence of HPV
cytophagy. In this study, it was possible to detect the pres-
ence of HPV in 17 cases by cytological examination, that
is, a 42.5% increase in HPV diagnostic frequency.
It is worth stressing that both the Schneider et al.21 and
Cavaliere et al.24 studies considered a partially limited list
of cytological criteria, and only samples with negative
diagnoses in the former and only positive diagnoses in
the latter. In both cases, the evaluation was unilateral,
and did not allow the confirmation of additional changes
in diagnostic frequency by either increased or decreased
frequencies within the counter-groups. Furthermore, no
attempt was made to distinguish the impact of the sam-
pling procedure, which potentiates the finding of four or
more nonclassical criteria.
This study showed that T. vaginalis promoted signifi-
cant morphometrical changes in squamous cells collected
by spatula or by brush in the control group. In addition,
HPV was partially capable of inducing significant mor-
phometrical changes, as no increase in the NA/CA ratio
was found in the HPV1ATYPIA2 group compared with
the HPV2ATYPIA2 group, irrespective of the sampling
procedure.
A higher frequency of nonclassical criteria was observed
in the samples collected with a spatula, compared with
similar samples collected with a brush. Finally, the inclu-
sion of nonclassical criteria for the diagnosis of HPV
resulted in an increased frequency of HPV infection in
groups initially categorized as negative by conventional cy-
tology. These cases were outnumbered by the decrease in
the diagnostic frequency of HPV in groups initially catego-
rized as positive by conventional cytology.
References
1. Gupta DK, Komaromy-Hiller G, Raab SS, Nath ME. Interobserverand intraobserver variability in the cytologic of normal and abnor-mal metaplastic squamous cells in pap smears. Acta Cytol2001;35:697–703.
2. Geisinger KR, Vrbin C, Grzybicki DM, Wagner P, Garvin AJ,Raab SS. Interobserver variability in human papillomavirus testresults in cervico-vaginal cytologic specimens interpreted as atypi-cal squamous cells. Am J Clin Pathol 2007;128:1010–1014.
3. Azocar J, Abad SM, Acosta H, et al. Prevalence of cervical dyspla-sia and HPV infection according to sexual behavior. Int J Cancer1990;45:622–625.
4. Yoshinouchi M, Hongo A, Nakamura K, et al. Analysis by multi-plex PCR of the physical status of human papillomavirus type 16DNA in cervical cancers. J Clin Microbiol 1999;37:3514–3517.
5. Collaco LM, Pinto AP. Aspectos citol�ogicos na colorac~ao de Papa-nicolaou da associac~ao de HPV com displasia e carcinoma de colouterino. J Bras Ginec 1994;104:419–421.
6. Eldar S, Sabo E, Cohen A, et al. The value of histomorphometricnuclear parameters in the diagnosis of well differentiated follicularcarcinomas and follicular adenomas of the tyroid gland. Histopa-thology 1999;34:453–461.
7. Strefezzi RF, Xavier JG, Cat~ao-Dias JL. Morphometry of caninecutaneous mast cell tumours. Vet Pathol 2003;40:268–275.
8. Dardick I, Payne CM. Rationale and potencial for image analysis inhistopathology: An overview. Ultrastruct Pathol 1992;16:97–98.
9. Liu W. A simplified cytologic staining technic. Am J Clin Pathol1970;54:767–768.
10. Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda Sys-tem: terminology for reporting results of cervical cytology. JAMA2002;287:2114–2119.
11. Wied GL, Bartels PH, Bibbo M, Dytch HE. Image analysis inquantitative cytopathology and histopathology. Hum Pathol1989;20:549–571.
12. Collan Y, Torkkeli T, Pesonen E, Jantunen E, Kosma VM. Applica-tion of morphometry in tumor pathology. Anal Quant Cytol Histol1987;9:79–88.
13. Millot C, Dufer J. Clinical applications of image cytometry tohuman tumor analysis. Histol Histopathol 2000;15:1185–1200.
14. Gram IT, Macaluso M, Churchill J, Stalsberg H. Trichomonas vagi-nalis (TV) and human papillomavirus (HPV) infection and the inci-dence of cervical intraepithelial neoplasia (CIN) grade III. CancerCauses Control 1992;3:231–236.
15. Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and microbiologi-cal aspects of Trichomonas vaginalis. Clin Microbiol Rev1998;11:300–317.
16. Athanassiadou P, Kavantzas N, Gonidi M, et al. Correlationsbetween nuclear/cytoplasmic area ratio and classification of cervicalsmears. J Exp Clin Cancer Res 2001;20:481–486.
17. Cavaliere MJ, Pereira GMC, De Lima MAN, Pereira SMM, MaedaMYS, Santos RTM. Alterac~oes coilocit�oticas em esfregacosc�ervico-vaginais: inter-relac~oes entre os aspectos citol�ogico, imuno-citoqu�ımico para papilomav�ırus e morfom�etrico. J Brasileiro deGinecologia 1990;100:275–279.
Diagnostic Cytopathology DOI 10.1002/dc
HPV DIAGNOSES USING CONVENTIONAL CYTOLOGY
Diagnostic Cytopathology, Vol. 41, No 9 791

18. zur Hausen H. Human papillomaviruses and their possible role insquamous cell carcinomas. Curr Top Microbiol 1977;78:1–30.
19. Meisels A, Morin C, Casas-Cordero M. Human papillomavirusinfection of the uterine cervix. Int J Gynecol Pathol 1982;1:75–94.
20. Schneider A, Kraus H, Schuhmann R, Gissman L. Papillomavirusinfection of the lower genital tract: Detection of viral DNA ingynecological swabs. Int J Cancer 1985;35:443–448.
21. Schneider A, Meinhardt G, De Villiers EM, Gissmann L. Sensitivityof the cytologic diagnosis of cervical condyloma in comparison withHPV-DNA hybridization studies. Diagn Cytopathol 1987;3:250–255.
22. Bollmann M, Bankfalvi A, Trosic A, Speich N, Schmitt C, Boll-mann R. Can we detect cervical human papillomavirus (HPV)
infection by cytomorphology alone? Diagnostic value of non-classiccytological signs of HPV effect in minimally abnormal Pap tests.Cytopathology 2005;16:13–21.
23. Kaneshima EN, Suzuki LE, Irie MMT, Yoshida CS, Silva SFM,Consolaro MEL. Importancia da aplicac~ao de crit�erios morfol�ogicosn~ao-cl�assicos para o diagn�ostico citopatol�ogico de Papillomavirushumano (HPV) previamente detectado por PCR. Acta Bioqu�ım Cl�ınLatinoam 2005;39:61–68.
24. Cavaliere MJ, Filho AL, Pereira GMC, Maeda MYS, Di Loreto C.Papilomavirus em sa�ude p�ublica: Importancia da aplicac~ao denovos crit�erios morfol�ogicos para sua detecc~ao em trato genitalfeminino. Bol Inform Union 1990;15:24–39.
Diagnostic Cytopathology DOI 10.1002/dc
SANA ET AL.
792 Diagnostic Cytopathology, Vol. 41, No 9