Embed Size (px)
DESCRIPTION
Psychiatric
Citation preview

MORNING REPORTSunday March 15th , 2015Supervisor:Dr. Sabar Siregar, Sp. KJ
I

Patient’s Identity
1. Name : Mr. H
2. Age : 29 years old
3. Sex : Male
4. Address : Kalibanger,Temanggung
5. Job : Employed
6. Marital status : Single
7. Ethnicity : Javanese
8. Educational status : Junior High School

Guardian IdentityAlloanamnesis was conducted to :
1. Name : Mr. Y
2. Age : 39 years old
3. Sex : Male
4. Address : Gemawang, Temanggung
5. Job : Farmer
6. Marital status : Married
7. Ethnicity : Javanese
8. Relation : Father

Reason brought to hospital
Patient was brought by his family because he did not want to work since one year ago.

Stressor
He work at a big company, and he expect that he will success with his job, but at reality he couldn’t met his expectation.

Progression of Illness(Alloanamnesis and autoanamnesis)

2014 (1 year ago)
Patient started not to work since one year ago, Patient felt that there was somebody look at him. He felt that the other people would do something harmed to him. He felt that his life uncomfortable. He think that the other people can read his mind. The patient hear some whisp which threatened him. He believe that some artist knew him. Sometimes the patient wait some artist arrived to met him.

15th March 2015 (day of admission)
Patient was brought by his family to RSJSM, because he didn’t want to work and disturbing the other people near him. He spit out the other people near him. Sometimes he broke some stuff too.
History of Past Illness
Psychiatric illness There is no history of psychiatric illness General medical illness There is no history of high fever, seizure,
head trauma, or any other serious illness which needs hospitalization
Substance abuse The patient smoke a pack of cigarette in a
day The patient also consume alcohol

Family History
There is no history of psychiatric illness in her family.
There is no history of high fever, seizure, head trauma, or any other serious illness which needs hospitalization

Progression of Illness
Symptoms
Role Function
2014
2015
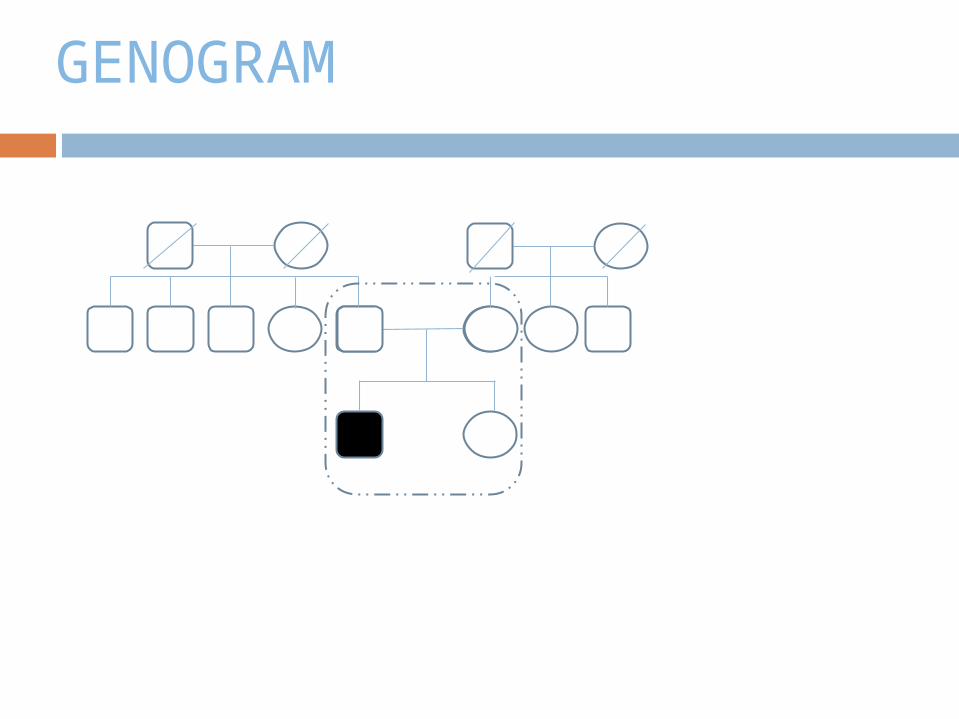
GENOGRAM

History of Personal Life
Prenatal and perinatal Patient’s mother was 22 years old
during pregnancy and labor, and had no illness
Patient was delivered by normal labor, and by traditional birth attendants
Patient consumed pure breast milk for 6 months
History of Personal Life
Early childhood phase (0-3 years old) Psychomotor
There was no valid data in patient’s psychomotor aspect (such as tilting the body, supine to prone, sitting, standing, walking, smiling, holding her own hand, scoop up object, holding pencil and pilling up two objects)
Psychosocial There was no valid data in patient’s psychosocial aspect (such as replying to
smile, smiling when seeing interesting object, playing cilukba, knowing her family members and pointing what she wanted without crying)
Communication There was no valid data in patient’s communication aspect (such as bubbling,
cooing, making sounds without meaning, telling 2-3 syllables without meaning and calling mama/papa)
Emotion There no valid data in patient’s emotion aspect (such as when patient playing,
frightened by strangers, starting to show jealousy or competitiveness towards other, and toilet training)
Patient didn’t pee or defecate in her pants when she was two years old Cognitive
There was no valid data in patient’s cognitive aspect (such as copying sounds that she heard for the first time and understanding simple orders)

History of Personal Life Intermediate childhood phase (3-11 years old)
PsychomotorThere is no valid data on when patient’s first time playing hide and seek or if patient ever involved in any kind of sports.
PsychosocialThere was no valid data in patient’s psychosocial data (such as developing initiative capacity, seeking for socialization, starting social interaction with others, developing self worth in own’s abilities and competitive capacity).
CommunicationThere is no valid data on patient’s communication data (ability to communicate with same age friends/peers, and express needs and wants).
EmotionThere is no valid data on patient’s emotion data (such as ability to experience physiologic response due to emotion)
CognitiveThere is no valid data in patient’s cognitive data (such as knowlegde, understanding , application of knowledge, anylisis, and evaluation abilities)
History of Personal Life Late childhood and teenage phase (11-18 years old)
PsychomotorThere is no valid data on patient’s psychomotor data (such as favorite activities or games, if patient involved in any kind of sports).
PsychosocialThere is no valid data in patient’s psychosocial data
(such as seeking for self identity)Communication
There is no valid data in patient’s communication data (ability to interact with peers – others, ability to discuss subjects and question, tolerate opposite opinions)
EmotionThere is no valid data in patient’s emotion data
(ability to control physiologic response due to emotion; such as palpitation, increased sweating when angry)
Cognitive

History of Personal Life Adulthood phase (18 years old-now)
Educational The patient didn’t continue to senior high school, he finish his study
on junior high school Occupational
Employee Marital status
Patient is single Criminal
He has no criminal history Current situation
Patient lives with his family.

Erikson’s stages of psychosocial development

Examination

Morning Report
Physical Examination

General physical examination
General appearance : well groomed, well nourished
Vital sign : BP : 130/90 mmHgHR : 84x/minto : afebrisRR : 20x/min

General physical examination
Head : normocephali, mouth deviation (-) anemic conjungtiva (-), icteric sclera (-), pupil isocore
Neck : normal, no rigidity, no palpable lymph nodes Thorax :
Cor : S1 S2 regular, murmur -, gallop – Lung : vesicular sound +/+, wheezing -/-, ronchi-/-
Abdomen : flat, abdominal wall//chest wall, normal peristaltic, tympany
sound, tenderness -, mass -, liver, spleen and kidney not papable Extremity : Warm acral, capp refill <2”, edema (-)

Neurological examination
Level of Consciousness : compos mentis, E4V5M6 (15)
General Appearance : Body posture : normal Abnormal movement : no abnormal
movement Walking style : normal

Neurological examination
Cranial nerves examination: CN I : in normal finding CN II : in normal finding CN III,IV,VI : in normal finding CN V : in normal finding CN VII : in normal finding CN VIII : in normal finding CN IX : in normal finding CN X : in normal finding CN XI : in normal finding CN XII : in normal finding

Neurological examination
Motoric Upper extremities: tonus (+), trophy : eutrophic, power
of movement : shoulder joint : 5, elbow joint : 5, wrist joint : 5, radial nerve function : 5, ulnar nerve function : 5, median nerve function : 5
Lower extremities: tonus (+), trophy : eutrophic, power of movement : hip joint : 5, knee joint : 5, ankle joint : 5
Sensorium DCML system : proprioception, fine touch : no
abnormalities AL system : vibration, temperature, crude touch, pain :
no abnormalities

Neurological examination Physiological reflex
Upper extremities: biceps reflex (+), triceps reflex (+), brachioradial (+)
Lower extremities: patella reflex (+), achilles tendon reflex (+)
Pathological reflex Upper extremities: Hoffman (-), Tromner (-) Lower extremities: babinski (-), chaddok (-),gordon
(-),oppenheim (-), rossolimo (-), clonus -/- Meningeal sign
Neck stiffness (-), brudzinski neck sign (-), brudzinski contralateral leg sign (-), kernig sign (-)
Cerebellum function Adhyadokokinesia (-), romberg test (-), finger to nose test
(no abnormalities), tip to toe walk (no abnormalities)

Morning Report
Mental State Examination

General Appearance
A man, age 29 years old, appropriate to his age, looked tense, wearing clothes, well groomed and well nourished

Orientation
Time : good People : good Place : good Situation : good
ConsciousnessConsciousness• Clear

Behavior

Attitude

Emotion

Disturbance in Perception

Progression of Thought

Content of Thought
• Idea of Reference
• Preoccupation
• Obsession
• Phobia
• Fantasy
• Delusion of Persecution
• Delusion of Reference
• Delusion of Envious
• Delusion of Hypochondriac
• Delusion of Magic-mystic
• Idea of suicidal
• Idea of Reference
• Preoccupation
• Obsession
• Phobia
• Fantasy
• Delusion of Persecution
• Delusion of Reference
• Delusion of Envious
• Delusion of Hypochondriac
• Delusion of Magic-mystic
• Idea of suicidal
• Delusion of Grandiose
• Delusion of Control
• Delusion of Religion
• Delusion of Influence
• Delusion of Passivity
• Delusion of Suspicious
• Idea of Suspicion
• Thought of Echo
• Thought of Insertion
• Thought of withdrawal
• Thought of
Broadcasting

Form of Thought
Non - realistic

Cognitive Function
Level of education : finished Junior High School
General knowledge : good Working/short/long memory : good Writing and reading skills : good Visuospatial : good Abstract thinking : good Ability to self care : good

Impulse Control When Examined
Self control: poor Patient response to examiners question: good
InsightInsight• Impaired insight

Morning Report
Resume

Symptom: Mental Status: Impairment:
• Didn’t work• Delusion of Suspicious (The
patient felt that the other people would do harm to him)
• Delusion of grandious (The patient felt that he knew some artists)
• Tought of broadcasting (The patient tought that the other people could read his mind)
• Behavior:Normoactive, Bizzare
• Mood : Euthymic,
• Affect : Inappropriate, Flat, Stabil
• Progression of Thought:Remming, Coherent, Relevant
• Content of thought : Delusion of Suspicious, Delusion of Grandiose, tought of broadcasting
• Form of thought : non-realistic
• Insight: Impaired insight
• Patient lose interest in his job
A man, 29 years old, single, employed, didn’t work, change in behavior, grandious, suspicious to other people
Morning Report
Diagnosis

Syndrome
SchizophreniasyndromeParanoid Syndrome
Auditorik Halutination
Thought of broadcasting
Delusion of suspicious
Delusion of GrandiousManiac syndrome

Differential Diagnosis
F20.3 Schizophrenia Paranoid F25.0 Schizoaffective maniac type

Multiaxial Diagnosis
Axis I : F20.3 Schizofrenia Paranoid Axis II : F60.0 Paranoid personality type Axis III : No diagnosis Axis IV : Stressor: Problem with his job Axis V : GAF admission 40-31

Patient’s problems
Biological problem Positive symptoms because of an
imbalance in dopamine activity, receptors and sensibility in the post synaptic neuron.
Psychological problems Conflict with his job
Social problem He can’t socialize well with others

Morning Report
Management

PLANNING MANAGEMENT

Management Planning
HospitalizationPatient was hospitalized.Patient Spit to other people
Emergency Department• Inj. Haloperidol 5 mg 1 Amp IM• Inj. Diazepam 5 mg 1 Amp IV

Response Phase
Target Therapy• 50% decrease of symptoms
Maintenance Therapy Haloperidol 2 x 2 mg

Remission phase
Target therapy : 100% remission of symptom
Inpatient management Haloperidol tab 5mg 2x1 Improving the patient quality of life :
Teach patient about his social & environment (interact with his family, socialize with his neighbor or friends, find a hobby to do on his spare time)
Outpatient management Continuation of pharmacotherapy Psychosocial therapy

Recovery Phase
Continue the medication, control to psychiatrist Rehabilitation :
- Consult to psychologist to help patient finding a hobby
- Help patient to interact normally with his family and neighboor
Family Education
Mental disorders can be controlled by medicines, so it is important to take the medicines routinely
Treat patient like you treat any other people
Help patient if he should be helped Don’t push patient to understand the
family, but his family that has to understand him
Don’t be too emotional to patient

THANK YOU!














