Embed Size (px)
Citation preview

Mood Disorders &
Eating Disorders
March 24, 2014
PSYC 2340: Abnormal Psychology
Brett Deacon, Ph.D.

• FDA approval process
• Publication bias in clinical trials of antidepressant medications
• Long-term outcomes: the STAR*D study
• Adverse effects of antidepressants
• The antidepressant-suicide controversy: TADS study
• Trends in national suicide rates
From Last Class

Bipolar Disorder
• Refresher on diagnostic criteria:
• DSM-IV diagnostic criteria:• Presence of manic episode or hypomanic
episode• Person may or may not have a history of
major depressive episodes• Episode not part of a psychotic disorder

Bipolar Disorder
• Interesting questions:
• What symptoms signify mania?
• Why are rates childhood bipolar disorder skyrocketing?

DSM-IV Manic Episode
• A) A distinct period of abnormally and persistently elevated, expansive or irritable mood, lasting at least 1 week (or any duration if hospitalization is necessary)B) During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree:1) inflated self-esteem or grandiosity2) decreased need for sleep (e.g., feels rested after only 3 hours of sleep)3) more talkative than usual or pressure to keep talking4) flight of ideas or subjective experience that thoughts are racing5) distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli)6) increase in goal-directed activity (at work, at school, or sexually) or psychomotor agitation7) excessive involvement in pleasurable activities that have a high potential for painful consequences (e.g., engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments)

DSM-IV Hypomanic Episode
• A) A distinct period of persistently elevated,
expansive or irritable mood, lasting throughout at
least 4 days, that is clearly different from the
usual nondepressed mood.

DSM-V Bipolar Disorder Not Elsewhere Classified
• 1. Major Depressive Episodes and Short (2-3 day)
Hypomanic Episodes. A lifetime history of one or more
Major Depressive Episodes in persons who have never
met full criteria for a Manic or Hypomanic Episode, but
have experienced one or more episodes of ‘short-duration
hypomania’ that meet the full symptomatic criteria for a
Hypomanic Episode, but only last for two to three days.

DSM-V Bipolar Disorder Not Elsewhere Classified
• 2. Major Depressive Episodes and Hypomanic Episodes
characterized by insufficient symptoms. A lifetime history
of one or more Major Depressive Episodes in persons
who have never met full criteria of a Manic or Hypomanic
Episode, but have experienced one or more episodes of
‘subthreshold hypomania’—at least four consecutive days
of elevated mood and one or two of the other symptoms
of a Hypomanic Episode OR irritable mood and two or
three of the other symptoms of a Hypomanic Episode.

Bipolar Disorder
• Is “irritability,” in the absence of elevated mood, consistent with mania?
• How much subjectivity exists in determining whether or not a person has mania?
• Why might rates of childhood bipolar disorder be skyrocketing?

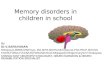
Bipolar Disorder in Children: Creation of an Epidemic (www.1boringoldman.com)
From 1994–1995 to 2002–2003, the number of
outpatient physician visits for bipolar disorder
among people aged < 21 increased by a factor
of more than 40 (Moreno et al., 2007)

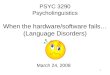
Bipolar Disorder in Children: Creation
of an Epidemic
Joseph Biederman Harvard psychiatrist and former director of the Johnson & Johnson Center for Pediatric
Psychopathology
Pediatric bipolar disorder articles (1995 to 2008)
70
Biederman’s articles (1978 to 2010)
60

Medications for Child Bipolar Disorder
• 90% of children with bipolar disorder were prescribed a mood stabilizer, antipsychotic, or antidepressant medication (Moreno et al., 2007)
• Risperdal (2007) and Abilify (2008) approved by FDA for child bipolar disorder

Medications for Child Bipolar Disorder
• In 2007, Bristol-Myers Squibb paid $515 million fine for illegally promoting Abilify for off-label use (principally for children and nursing home residents)• 2006 Abilify sales: $2.6 billion
• In 2012, Johnson & Johnson agreed to $2.2 billion fine for fraudulent marketing of Risperdal and other drugs• Risperdal sales from 2003-2010: $24.2
billion

Financial Conflicts of Interest
• Biederman’s Johnson & Johnson Center for Pediatric Psychopathology at Harvard had goal to “move forward the commercial goals of J &J”
• From 2000 to 2007, Biederman earned $1.6 million on consulting fees from drug companies• Failed to report this income to Harvard
University• Violated NIMH disclosure rules• Biederman was being paid by drugmakers
whose products he was studying in taxpayer-funded clinical trials

Validity of Bipolar Disorder in Children: Clinical Presentation
• Geller et al. (2012) drug trial for childhood bipolar disorder in 279 children ages 6 to 15:• 92.8% had a comorbid diagnosis of ADHD• Average duration of manic episode: 4.9
years• 99.3% had “daily rapid cycling:” periods of
intense irritability and agitation interspersed with other symptoms of bipolar disorder such as elation and grandiosity

DSM-5: Child Bipolar Disorder
• Pressure to take action
• Solution: creation of a new diagnosis• “Disruptive Mood Dysregulation
Disorder”

DSM-5: Disruptive Mood Dysregulation Disorder
• A. Severe recurrent temper outbursts manifested verbally (e.g., verbal rages) and/or behaviorally (e.g., physical aggression toward people or property) that are grossly out of proportion or intensity to the situation or provocation
• B. The temper outbursts are inconsistent with developmental level
• C. The temper outbursts occur, on average, three or more times per week
• D. The mood between temper outbursts is persistently irritable or angry most of the day, nearly every day, and is observable by others (e.g., parents, teachers, peers)
• E. Criteria A-D have been present for 12 or more months. Throughout that time, the individual has not had a period lasting 3 or more consecutive months without all of the symptoms in criteria A-D
• F. Criteria A and D are present in at least 2 of 3 settings (i.e., at home, at school, with peers) and are severe in at least one of these
• G. The diagnosis should not be made for the first time before age 6 years or after age 18 years.

Allen Frances: DMDD is the #1 Worst Change in DSM-5
“DSM 5 will turn temper tantrums into a mental disorder- a
puzzling decision based on the work of only one research
group. We have no idea whatever how this untested new
diagnosis will play out in real life practice settings, but my
fear is that it will exacerbate, not relieve, the already
excessive and inappropriate use of medication in young
children…DSM 5 should not be adding a new disorder
likely to result in a new fad and even more inappropriate
medication use in vulnerable children.”

Treatments for Bipolar Disorder
• Lithium for bipolar disorder• Helps prevent and treat manic episodes• Side effects may be severe (e.g., weight gain,
drowsiness, fatigue)
• In the NIMH-funded Systematic Treatment Enhancement Program for Bipolar Disorder study (STEP-BD; Schneck et al., 2008), only 23% of patients with bipolar disorder who received treatment in accordance with best-practice psychiatric guidelines (APA, 2002) remained well and continuously enrolled in the study during the one-year follow-up period. The remainder either dropped out (32%) or suffered a recurrence of a mood episode (45%).

Treatments for Mood Disorders
• Electroconvulsive therapy (ECT)• Applies brief electrical current to the brain
causing temporary seizures • Effective for severe depression in the short-
term• Significant cognitive side effects• Relapse afterwards is common (about 60%)

Treatments for Mood Disorders
• Transcranial magnetic stimulation• NIMH: TMS "uses a magnet instead of an electrical current to
activate the brain. An electromagnetic coil is held against the forehead and short electromagnetic pulses are administered through the coil. The magnetic pulse easily passes through the skull, and causes small electrical currents that stimulate nerve cells in the targeted brain region. And because this type of pulse generally does not reach further than two inches into the brain, scientists can select which parts of the brain will be affected and which will not be. The magnetic field is about the same strength as that of a magnetic resonance imaging (MRI) scan."
• http://www.youtube.com/watch?v=FiUL7pm4w3A

Treatments for Mood Disorders
• Transcranial magnetic stimulation: how well does it work?
• How should researchers study TMS?
• Efficacy of TMS based on a “gold standard” Cochrane Review of 16 controlled trials (http://www.ncbi.nlm.nih.gov/pubmed/12076483)
• “No difference was seen between rTMS and sham TMS using the Beck Depression Inventory or the Hamilton Depression Rating Scale, except for one time period (after two weeks of treatment) for left dorsolateral prefrontal cortex and high frequency; and also for right dorsolateral prefrontal cortex and low frequency, both in favour of rTMS and both using the Hamilton scale.”
• “The information in this review suggests that there is no strong evidence for benefit from using transcranial magnetic stimulation to treat depression, although the small sample sizes do not exclude the possibility of benefit.”