Embed Size (px)
Citation preview

Monitoring of neonatal
seizures by aEEG
Lena Hellström-Westas, MD PhDProfessor of Perinatal Medicine
Dept. of Women’s and Children’s HealthUppsala University, Sweden
3rd Kuwait Neonatology Conference
18-21 December 2019, Kuwait

EEG definition of neonatal seizures
– Seizure
• “Sudden repetitive, evolving and stereotyped ictal pattern with a clear beginning middle and ending and a minimum duration of (5-) 10 sec.”
– Status epilepticus
• Seizure duration >30 min. or >50% of tracing
– BIRD (?): Brief (potentially) Ictal Rhythmic Discharges
– PLED (?): Periodic Lateralized Epileptiform Discharges

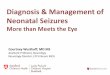
Postoperative monitoring in newborn
infant with congenital heart disease
• Continuous normal voltage background (3.5 hours) but
slightly depressed lower border due to sedation
• No sleep wake cycling
• Two subclinical seizures* with duration around 10 minutes
* *

Postoperative seizures in infant with
congenital heart disease
1
2
3
4
5
1-2-3-4-5

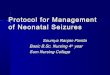
Postoperative subclinical seizures in
infant with congenital heart disease
(Hellström-Westas, de Vries, Rosén. Atlas of aEEGs in the Newborn, 2008)

A
A
B
B
C
C
D
D
E
E
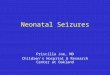
Subclinical status epilepticus in a severely
asphyxiated infant
Medication
(Hellström-Westas, de Vries, Rosén. Atlas of aEEGs in the Newborn, 2008)

Subclinical status epilepticus in severely
asphyxiated term infant
(Hellström-Westas, de Vries, Rosén. Atlas of aEEGs in the Newborn, 2008)

Four subclinical seizures in a term infant with
Zellweger disease
(Hellström-Westas, de Vries, Rosén. Atlas of aEEGs in the Newborn, 2008)
Sleeping

Status epilepticus in a hypothermia-
treated asphyxiated term infant

4-week old infant (GA 32 w) with viral meningitis;
Irritable and apneas but no clinical seizures;
aEEG/EEG revealed 6 h status epilepticus

4-week old infant (GA 32 w) with viral meningitis;
Irritable and apneas but no clinical seizures;
aEEG/EEG revealed 6 h status epilepticus


Status epilepticus in asphyxiated full-term
infant treated with hypothermia

Some seizures in extremely preterm infants contain very low-
frequencies = are filtered in the aEEG
= not possible to detect in aEEG trend
Sharp-wave frequency 0.5 Hz

Study Characteristics Main findingsHellström-Westas, Acta
Paediatr 1992
a) 1-ch aEEG vs 1-ch EEG (N=10 infants)
b) 5-ch aEEG vs 5-ch EEG (N=5 infants)
1-ch aEEG: 15/48 (31%) sz detected
5-ch aEEG: all sz detected.
Toet et al, Pediatrics 2002 1-ch aEEG vs 30 min 19-ch EEG (N=33
monitored infants, 10 had sz on EEG)
1-ch aEEG: detected sz in 8/10 infants and suspected sz in 1 .
Shellhaas et al, Pediatrics
2007
1-ch aEEG (C3-C4) vs cEEG (6 assessors, 125
EEGs from 121 infants with 851 sz)
1-ch aEEG: detected median 26% of sz and median 40% of rec containing
sz. Experienced assessors detected more sz.
Shellhaas et al, Clin
Neurophysiol 2007
1-ch EEG (C3-C4) vs cEEG
(125 EEGs from 121 infants with 851 sz)
1-ch EEG: detected 78% of sz and 94% of recordings containing sz,
underestimated duration of sz.
Shah et al, Pediatrics
2008
2-ch aEEG/EEG vs cEEG (N= 41 sz in 7 of 21
monitored infants)
2-ch aEEG/EEG: detected 31/41 sz, i.e. sensi 76%; spec 78%; posi pred
value 78%; neg pred value 78%.
Wusthoff et al, J Perinatol
2009
1-ch EEG (Fp3-Fp4) vs cEEG (125 EEGs with
330 sz)
1-ch EEG (Fp3-Fp4): detected 46% of sz and 66% rec with sz.
Bourez-Swart et al, Clin
Neurophysiol 2009
1-ch aEEG or 9-ch aEEG vs 9-ch EEG (N=12
infants with 121 ss)
1-ch aEEG: detected 30% sz (95% CI: 0.22-0.38) in 11 infants. C3-C4 best.
9-ch aEEG: detected 39% sz (95% CI: 0.31-0.48) and all 12 infants with sz.
van Rooij et al, Arch Dis
Child Fetal Neonatal Ed
2010
2-ch aEEG/EEG vs 1-ch aEEG/EEG
(N=34 infants with sz; 18 unilateral injury, 14
bilateral injury, and 2 no injury
2-ch aEEG/EEG: detected 18% more sz + more sz on ipsilateral side in 79%
of infants with unilateral injury; and 39% more sz in infants with diffuse brain
damage.
Evans et al, ADC Fetal
Neonatal Ed 2010
2-ch aEEG vs 12-ch EEG (44 infants, sz
detected in EEG of 20 infants (45.5%)).
2-ch aEEG: suspected sz in 28 (63.6% = overdiagnosed, most frequently
due to movement artefacts): sens 80%, spec 50%.
Frenkel et al, Clin
Neurophysiol 2011
1-ch aEEG/EEG vs 8-ch EEG (10 infants with 41
sz). Experienced/less experienced.
1-ch aEEG/EEG detection of individual sz: sensi 71-84%, speci 36-96%.
Specialist higher detection rate than student/fellow.
Zhang et al, Neurosci Bull
2011
1-ch aEEG or aEEG/EEG vs cEEG (62 infants
with 876 sz)
1-ch aEEG: detected 44% sz; 1-ch aEEG/EEG: detected 86% sz
Higher detection rate: >5 sz/hour, sz duration > 60 seconds, central origin.
How good is aEEG for seizure identification?

Study Characteristics Main findingsHellström-Westas, Acta
Paediatr 1992
a) 1-ch aEEG vs 1-ch EEG (N=10 infants)
b) 5-ch aEEG vs 5-ch EEG (N=5 infants)
1-ch aEEG: 15/48 (31%) sz detected
5-ch aEEG: all sz detected.
Toet et al, Pediatrics 2002 1-ch aEEG vs 30 min 19-ch EEG (N=33
monitored infants, 10 had sz on EEG)
1-ch aEEG: detected sz in 8/10 infants and suspected sz in 1 .
Shellhaas et al, Pediatrics
2007
1-ch aEEG (C3-C4) vs cEEG (6 assessors, 125
EEGs from 121 infants with 851 sz)
1-ch aEEG: detected median 26% of sz and median 40% of rec containing
sz. Experienced assessors detected more sz.
Shellhaas et al, Clin
Neurophysiol 2007
1-ch EEG (C3-C4) vs cEEG
(125 EEGs from 121 infants with 851 sz)
1-ch EEG: detected 78% of sz and 94% of recordings containing sz,
underestimated duration of sz.
Shah et al, Pediatrics
2008
2-ch aEEG/EEG vs cEEG (N= 41 sz in 7 of 21
monitored infants)
2-ch aEEG/EEG: detected 31/41 sz, i.e. sensi 76%; spec 78%; posi pred
value 78%; neg pred value 78%.
Wusthoff et al, J Perinatol
2009
1-ch EEG (Fp3-Fp4) vs cEEG (125 EEGs with
330 sz)
1-ch EEG (Fp3-Fp4): detected 46% of sz and 66% rec with sz.
Bourez-Swart et al, Clin
Neurophysiol 2009
1-ch aEEG or 9-ch aEEG vs 9-ch EEG (N=12
infants with 121 ss)
1-ch aEEG: detected 30% sz (95% CI: 0.22-0.38) in 11 infants. C3-C4 best.
9-ch aEEG: detected 39% sz (95% CI: 0.31-0.48) and all 12 infants with sz.
van Rooij et al, Arch Dis
Child Fetal Neonatal Ed
2010
2-ch aEEG/EEG vs 1-ch aEEG/EEG
(N=34 infants with sz; 18 unilateral injury, 14
bilateral injury, and 2 no injury
2-ch aEEG/EEG: detected 18% more sz + more sz on ipsilateral side in 79%
of infants with unilateral injury; and 39% more sz in infants with diffuse brain
damage.
Evans et al, ADC Fetal
Neonatal Ed 2010
2-ch aEEG vs 12-ch EEG (44 infants, sz
detected in EEG of 20 infants (45.5%)).
2-ch aEEG: suspected sz in 28 (63.6% = overdiagnosed, most frequently
due to movement artefacts): sens 80%, spec 50%.
Frenkel et al, Clin
Neurophysiol 2011
1-ch aEEG/EEG vs 8-ch EEG (10 infants with 41
sz). Experienced/less experienced.
1-ch aEEG/EEG detection of individual sz: sensi 71-84%, speci 36-96%.
Specialist higher detection rate than student/fellow.
Zhang et al, Neurosci Bull
2011
1-ch aEEG or aEEG/EEG vs cEEG (62 infants
with 876 sz)
1-ch aEEG: detected 44% sz; 1-ch aEEG/EEG: detected 86% sz
Higher detection rate: >5 sz/hour, sz duration > 60 seconds, central origin.
How good is aEEG for seizure identification?

aEEG versus conventional EEG (Shellhaas et al, Pediatrics 2007)
• N=125 EEGs with 851 seizures (121 infants)
• aEEG (C3-C4) reviewed by 6 neonatologists
• 26% (12-38) of seizures detected
• 40% (22-58) of EEGs with seizures detected

1-ch EEG versus conventional EEG (Shellhaas et al, Clin Neurophysiol 2007 and Pediatrics 2007 )
• N=125 EEGs with 851 seizures (121 infants)
• 1-ch EEG (C3-C4)
• 78% of seizures identified
• 94% of EEGs with seizures
• Underestimates number of seizures
• Underestimates duration of seizures

Fewer seizures detected with
electrodes on the forehead(Wusthoff et al, J Perinatol 2009)
• 125 EEGs with 330 seizures:
– 46% appeared in frontal electrodes (Fp3-Fp4)
– 73% appeared in central electrodes (C3-C4)
– Seizures briefer in Fp3-Fp4 than in C3-C4

62 infants with 876 seizures on conventional EEG (cEEG)
Seizure detection aEEG aEEG+rawEEG
• >5 sz per hour 52.5.% 96.8%
• Duration >60 sec 50.6% 84.1%
• Central origin 57.9% 90.9%

Topographic localization of seizures
Patrizi et al,
Brain Dev 2003
(n=71 seizures)
Shellhaas et al,
Pediatrics 2007
(n=851 seizures)
Frontal 11.3% 5%
Central 26.8% 56%
Temporal 45% 25%
Parietal 9.9%
Occipital 7% 14%

How good is aEEG/EEG for seizure
identification?• Shellhaas et al (Pediatrics 2007, Clin Neurophysiol 2007) recorded
125 EEGs with 851 seizures
• Detection rate in 1-ch aEEG (C3-C4)
– 26% (12-38) seizures, median (range)
– 40% (22-58) of aEEGs containing seizures
• Detection rate in 1-ch EEG (C3-C4)
– 78% of seizures identified
– 94% of EEGs containing seizures were identified
• Zhang et al (Neurosci Bull 2011) recorded 876 EEG seizures
in 62 infants
Seizure detection aEEG aEEG+rawEEG
>5 sz per hour 52.5.% 96.8%
Duration >60 sec 50.6% 84.1%
Central origin 57.9% 90.9%

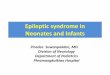
1-ch versus 2-ch aEEG/EEG (van Rooij et al, Arch Dis Child Fetal Neonatal Ed 2010)
2-ch, Number of seizures 1-ch, Number of seizures
Unilateral lesion
(14 infants)
Ipsilat:166
Contralat: (36) + 6
(126/166) + 15 new (!)
Bilateral lesion
(18 infants)
199, incl 4 SE (167/199, incl 4 SE) + 24 new
(!)
2-ch
1-ch

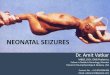
Term baby with stroke Clinical + aEEG/EEG sz during the night, cUS=0,
EEG the following day = seizures left side →
MRI: Left MCAI infarction

Term baby with left-sided stroke
Lt
Rt
Rt
Lt

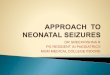
Impact of aEEG on clinical care for
neonates with suspected seizures (Shellhaas & Barks, Pediatr Neurol 2012)
• More infants with clinical seizures had electrographic confirmation
• Earlier seizure-diagnosis in infants with HIE
p<0.05 vs control

2 hours8 h aEEG
2 h aEEG

10 mm/sec
15 mm/sec
30 mm/sec

30µV/cm
100µV/cm


Conclusion
• aEEG/EEG may detect 80-90% of seizures in the cEEG
EEG, when also the 1-ch raw-EEG is inspected, but
underestimates the duration of seizures
• aEEG without raw-EEG detects much fewer suspected
seizures, and cannot verify their epileptic nature
• aEEG/EEG identifies seizures that would otherwise go
clinically undetected, and is associated with earlier
diagnosis of seizures in asphyxiated infants
• Higher seizure frequency, longer seizure duration, central
origin and experienced assessor are factors associated with
better aEEG/EEG seizure detection
• 2-ch aEEG/EEG is recommended – better artefact detection

Distinct ictal aEEG
pattern in neonatal
epilepsy associated with
KCNQ2 mutations (Vilan et al, Neonatology 2017)