Embed Size (px)
Citation preview

The Impact of Neonatal Seizures on the Ability to Encode, Store, and Retrieve Memories
Jamie L. Archambault
NSC 371 Evidence and Inquiry and Polymathic Scholars Program The University of Texas at Austin
December 2013
____________________________________________ Dr. Ann Repp
Department of Psychology Faculty Mentor

ABSTRACT
Throughout life, the prevalence of seizures is highest during the neonatal period, a
critical time for synaptic development. While neonatal seizures can be attributed to a
wide array of predisposed risk factors and underlying medical complications, the majority
of seizures result from hypoxic-ischemic encephalopathy, a condition that occurs when
the brain is deprived of adequate oxygen supply. Early life neonatal seizures often result
in cognitive deficits such as long-term impairments in learning and memory.
Additionally, the occurrence of seizure activity during the this developmental period
increases susceptibility to epilepsy far into adulthood. In this study, we propose two
distinct sets of hypotheses to explain the origin of cognitive dysfunction resulting from
neonatal seizures. From a psychological perspective, the extensive and far-reaching
effects of such seizures can be rationalized using components from existing memory
models. Furthermore, these deficits can be explained on a synaptic level through the
physiological association between long-term potentiation and the ability to encode, store,
and retrieve memories.

TABLE OF CONTENTS
INTRODUCTION 1 COGNITIVE EFFECTS OF NEONATAL SEIZURES 4 Long-Term Complications 4 Methods of Treatment 5 Etiology of Cognitive Dysfunction 6 MEMORY PROCESSES 7 Multi-Store Memory Model 7 Working Memory Model 10 Memory During Development 13 PSYCHOLOGICAL IMPACT ON MEMORY 15 Hypothesis 1.1 - Breakdown of Executive Functions 15 Hypothesis 1.2 - Developmental Amnesia 16 Hypothesis 1.3 - Verbal and Visual Deficits 16 BIOLOGICAL EFFECTS OF NEONATAL SEIZURES 18 Altered Electrical Activity 18 Calcification from Atrophy 19 Decreased Synaptic Plasticity 19 NEURAL SUBSTRATES OF MEMORY 20 Anatomical Structures 20 LTP and AMPA Receptor Cycling 24 PHYSIOLOGICAL IMPACT ON MEMORY 28 Hypothesis 2.1 - Induction and Saturation of LTP 28 Hypothesis 2.2 - Increased Phosphorylation of AMPA Receptors 29 Hypothesis 2.3 - Reduction of Silent Synapses 30 CONCLUSION 32 BIBLIOGRAPHY 34

1
INTRODUCTION
Neonatal seizures, which can be attributed to a variety of etiologies, occur in 1.8
to 3.5 per 1,000 live births (Cowan, 2002; Cowan et al., 2003; Silverstein & Jensen,
2007). Throughout life, the prevalence of seizures is highest during the neonatal period, a
critical time for both psychological and physiological development. Neurological
disruption during this period often has detrimental and far-reaching effects on the
cognitive function of affected infants. They are a problem in both term and pre-term
infants and are secondary to risk factors such as shortened gestational period, low birth
weight, and male sex (Kohelet, Shochat, Lusky, & Reichman, 2006a; Kohelet, Shochat,
Lusky, & Reichman 2006b; Kurabe, Sorimachi, Sasaki, Koike, & Fujii, 2009).
Additionally, these seizures can be associated with a host of underlying conditions, such
as transient metabolic disturbance, systemic or central nervous system infection,
cerebrovascular abnormalities, and hypoxic-ischemic encephalopathy (Hallberg &
Blennow, 2013). While an array of factors contributes to the onset of neonatal seizures,
neonatal encephalopathy due to hypoxia-ischemia is the most common cause of seizures
in neonates (Hallberg & Blennow, 2013; Silverstein & Jensen, 2007). During hypoxic-
ischemic encephalopathy (HIE), brain injury to both gray and white matter structures
often occurs as a result of asphyxia, most specifically, damage to the basal ganglia and
thalamus (Gano et al., 2013).
Unlike seizures that occur during adulthood, neonatal seizures are difficult to
detect and treat because they are most commonly associated with subtle behavior and a
lack of coordinated EEG pattern (Jensen, 2009). Given the range of variability in
neonatal seizures, it is important to distinguish the difference between these seizures and

2
general epilepsy. Epilepsy in children includes a body of disorders that is characterized
by recurrent, unprovoked seizure activity. Neonatal seizures, while not considered an
epileptic disorder, are a specific type of seizure that occur within the first 28 days of life
and often contribute to the future development of epilepsy. In addition, febrile seizures,
congenital malformations, metabolic disorders, head trauma, CNS infection, and family
history are specific risk factors that are indicative of epilepsy later in life (Cowan, 2002).
Interestingly, many of these risk factors for epilepsy independently contribute to the onset
of neonatal seizures. To fully understand how seizures affect memory, the pathology of
these seizures must first be understood.
The clinical expression of neonatal seizures often inhibits a clear diagnosis, as
both inward and outward symptoms tend to vary greatly depending on the etiology and
type of seizure. A review by Silverstein and Jensen (2007) detailing the clinical and
electrical differences in the types of seizures seen in neonates suggests that each of these
factors is associated with a specific outcome. Subtle seizures, which account for
approximately 50% of all neonatal seizures, are characterized by motions that imitate
normal behaviors in neonates and are not consistently associated with EEG seizure
activity. Tonic seizures, when focal, exhibit sustained muscle contractions and
coordinated EEG activity. Similarly, focal clonic seizures display evident EEG seizure
activity, but are outwardly associated with rhythmic jerks. Finally, myoclonic seizures are
characterized by rapid, single, arrhythmic jerks. Though the initial diagnosis is often
based on clinical observation, EEG seizure activity is the most definitive indicator of
short-term outcome. Since neonatal seizures commonly have a debilitating effect on

3
quality of life, early diagnosis using these indicators are critical in managing and
minimizing the risk to long-term cognitive function (Silverstein & Jensen, 2007).
Unfortunately, the spectrum of disorders that provoke the onset of neonatal
seizures is simply too broad for the scope of this study. For this reason, our analysis of
the effects of neonatal seizures on memory deficits will be limited to those resulting from
hypoxic-ischemic encephalopathy, the most prevalent cause of neonatal seizures. In an
effort to understand both the psychological and physiological impact of these seizures
and assess how cognition is affected, a thorough analysis of the neonatal stage of
development will be performed. The intent of this paper is to integrate a working
knowledge of memory formation with a physiological understanding of neonatal seizures
to fully explain how these seizures affect cognitive functioning. In doing this, we will
present two sets of original hypotheses: one set that relates the cognitive deficits from
neonatal seizures to existing memory models and another that explains the connection
between the neural substrates of memory and the neural substrates of seizures. We will
first discuss what is known regarding the cognitive deficits associated with neonatal
seizures, specifically those associated with learning and memory. To explain these
deficits from a psychological perspective, we will examine both early and revised models
that have been proposed to explain the process of memory formation. Following this, we
will explore the neural basis of memory formation and relate it to the molecular processes
that occur during seizures.

4
COGNITIVE EFFECTS OF NEONATAL SEIZURES Long-Term Complications The risk for seizures is highest in the neonatal period, a critical period for both
psychological and physiological development (Jensen, 2009). Seizures during this period
are predominantly caused by HIE, a pathology that contributes to motor and cognitive
deficits in up to 40% of surviving neonates (Silverstein & Jensen, 2007; Shankaran
2009). MRI findings indicate that the extent and severity of brain injury is commonly
associated with the duration of the seizure (Glass et al., 2009; van Rooij, van den Broek,
Rademaker, & de Vries, 2013).
The adverse outcomes associated with seizures resulting from HIE are most
severe in the absence of other disabilities, such as cerebral palsy. For instance, a
“normal” child is more likely to experience severe adverse outcomes from HIE-induced
neonatal seizures than a child who has already been diagnosed with a cognitive disorder.
These outcomes include intellectual impairments, memory and verbal problems,
difficulty in executive functions, and motor problems (Perez et al., 2013). Issues with
short-term memory and social interaction often extend far past childhood and into the
adult years (Lindstrom et al., 2008; Odd, Dunnell, Lewis, & Rasmussen 2011). A study
by van Handel, de Sonneville, de Vries, Jongmans, and Swaab (2012) found that seizures
from moderate HIE result in the compromised maintenance and retrieval of verbal,
visuospatial, and associative memories, while also decreasing the speed and efficiency of
working memory. In cases resulting from only mild HIE, patients showed normal short-
term and working memory with only a slightly weakened verbal learning capacity.
Additionally, neonatal HIE can contribute to later-life developmental amnesia.

5
Developmental amnesia is a selective disorder characterized by a patient’s frequent
failure to remember events from their everyday life. In these cases, deficits are observed
in episodic memory while the function of semantic memory and working memory remain
largely intact (Sans, 2011).
Methods of Treatment
In neonates that exhibit pharmacoreistant seizures, epileptic surgeries have been
effective in reducing the severity of cognitive deficits. Two and ten-year follow up
studies show improvement in social conduct, verbal learning capacity, figurative learning
capacity, and working memory (Viggedal, Kristjansdottir, Olsson, Rydenhag, &
Uvebrant, 2012). Interestingly, these patients exhibited signs of memory reorganization
both prior to and immediately following the procedure (Viggedal et al., 2012). Because
seizure disorders cause an inability to properly form memories, the brain attempts to
preemptively compensate for the lack of function by reorganizing the process for memory
consolidation. For instance, the posterior remnant of the hippocampus ipsilateral to the
damaged hemisphere appeared to take over the function of verbal memory after the
resection of an affected anterior temporal lobe (Bonelli et al., 2013). Despite the evident
success with surgical intervention for recurrent seizures, recent advances have employed
the use of therapeutic hypothermia to noninvasively treat and prevent future seizures
(Harbert et al., 2011). Clinical trials indicate that post-seizure hypothermia reduces the
extent of brain injury contributing to social dysfunction and impaired memory by
preventing the molecular cascade that leads to secondary energy failure and eventual cell
death (Dehaes et al., 2013).

6
Etiology of Cognitive Dysfunction
In understanding the foundation of developmental impairments from neonatal
seizures, as well as the success of treatment methods, we can begin to hypothesize
precisely how memory is affected. Memory is a complex concept that depends widely
upon the type of information to be stored and the current stage of processing in which it
resides. It is unknown whether seizure activity affects the capability to encode, store, or
retrieve information that is intended for memory.
Three separate models, as detailed in Figure 1, have been suggested as possible
explanations for reduced cognitive functioning in infants exhibiting seizure activity
(Martinos et al., 2012). The first explanation proposes that neonatal seizures themselves
directly cause the brain damage responsible for cognitive deficits. The second model
suggests that the relative risk factors that predispose neonates to seizures, such as
gestational length, birth weight and sex, act independently from seizures to hinder
cognition and contribute to memory deficits. The third possible explanation integrates the
first two models by suggesting that the overarching effect of a predisposition to brain
injury along with actual seizure activity causes the severe memory impairments
commonly seen in affected patients.
Figure 1. Models proposed by Martinos et al. (2012) to explain the relationship between neonatal seizures and memory deficits

7
MEMORY PROCESSES
Multi-Store Memory Model
As a topic of long-time psychological interest, various abstract models have been
proposed to provide representations of how memory is believed to work. One of the
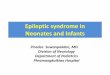
earliest models for memory, the multi-store model proposed by Atkinson and Shiffrin
(1968), divided memory into short-term and long-term components (Figure 2). Unlike
other theories of the time, the multi-store model supported the idea of a dichotomized
memory. Early studies demonstrated that patients with hippocampal lesions retained both
their previous long-term memories and the ability to create new short-term memories
(Milner, 1959; Milner, 1967). However, they lacked the ability to move these new short-
term memories into long-term storage (LTS), thus supporting the notion that there is a
distinct separation between short-term storage (STS) and LTS.
The multi-store model proposed that sensory stimuli are immediately registered
and used to create trace memories. Memory traces may vary in strength depending on the
Figure 2. Atkinson-Shiffrin model of multi-store memory

8
intensity of their associated meanings, a property that later affects the success of retrieval.
Unless these traces are committed to STS, and ultimately LTS, they will quickly decay.
Recent studies have noted that there is a maximum capacity, or buffer, for sensory
information during the initial encoding process. Often, the failure to filter input within
this buffer contributes to the loss of information from STS, rather than a failure of
memory consolidation itself (Buschman, Siegel, Roy, & Miller, 2011). Though other
forms of STS exist, Atkinson and Shiffrin relied heavily on auditory-verbal-linguistic
(AVL) short-term store to explain their model. AVL, most widely studied by Peterson
and Peterson (1959), demonstrated that stimuli that appeal to either the sense of sight or
sound could be registered by the other sense before being transferred to STS for coding.
They suggested that both task difficulty and the rate at which information is presented
directly decreases available rehearsal time, which causes a decay of STS and ultimately
affects the ability to accurately recall information. If coding is interrupted by additional
tasks or stimuli, the transfer is terminated and the memory trace, along with its associated
meaning, will decay before reaching STS.
The transfer of traces from STS to LTS is regulated by a variety of control
processes, which will be discussed shortly. However, it is important to note that this
transfer could be either probabilistic or continuous in manner depending upon the type of
stimuli and the order in which they are presented. Probabilistic transfer occurs in cases of
incidental learning where the subject does not make a conscious effort to store material,
yet retains it anyways. On the other hand, continuous transfer is most often employed
when material is repeatedly presented and gradually learned.

9
Once traces have been committed to LTS, they can be retrieved and brought
forward to STS by either recognition or recall. The difference between these is best
exemplified by the “tip of the tongue” phenomenon. Oftentimes, individuals find it
difficult to recall a memory from LTS without further prompting. The recall of
information is occasionally hindered by interferences from other stimuli, which can occur
during coding or retrieval. When given a cue, relevant information becomes available
through the process of recognition. The recognition of one trace brings forward others
through associative processes. The explanation for this phenomenon is rooted in the
belief that many partial traces are coded in LTS through their association with existing
complete traces. The idea that traces do not have to be stored “all or none” fashion is
supported by the observation that a second guess is often correct and not based
completely on chance when attempting to recall specific fragments of information
(Binford & Gettys, 1965).
The control processes utilized when coding, as previously mentioned, are
transient events managed by the subject and influenced by either the subject’s personal
history or the nature of the task at hand. These processes consist of schemes, coding
techniques, and mnemonics that increase the efficacy of encoding and retrieving
memories. At the level of the sensory register, individuals typically employ a scanning
process to determine which senses they will devote attention to. The rehearsal of
information regenerates STS traces and allows time for coding processes that assist in the
transfer to LTS to operate. However, there is a trade off between the buffer size of STS
and the ability to encode this information for LTS. While a large buffer size enables the
individual to retain more information in STS, it hinders the ability to accurately transfer

10
this information to LTS. Put simply, the mind is so focused on maintaining a large
quantity of information that there is a reduction in the quality of encoded information.
Conversely, a small buffer size limits the amount of information in STS but allows for a
more accurate encoding process.
When retrieving information from STS, it is more efficient for individuals to
employ a quick search along ordered dimensions, or to list facts in an organized manner
rather than at random. If partial decay has already occurred, it is often necessary to
retrieve associated traces from LTS to generate a complete idea. Information from the
sensory register can only enter STS indirectly, a process that is most effective if traces
have been accurately encoded in LTS. When a stimulus is presented, the brain must
perform a LTS search for previously encoded associations to this stimulus. The need to
create new associations can often be eliminated by relying on existing associations.
Encoding information through existing associations decreases the area of memory that
must be searched when attempting to retrieve information and protects against
interference from succeeding sensory inputs. The length of the search and the control
processes utilized when recalling information from LTS are indicative of the efficiency of
that search. As with searches in STS, those in LTS must be performed along ordered
dimensions and it is the nature of the task that typically determines the procedure that is
utilized. Individuals must know what information to search for, where to search for it,
and when to terminate unsuccessful searches.
Working Memory Model
Shortly after the proposal of the multi-store model of dichotomized memory,
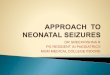
Baddeley and Hitch (1974) published the working memory model (Figure 3). In short,

11
working memory replaced simplistic STS by suggesting that there is an active
maintenance of short-term information, which further organizes a trace according to the
particular sense that it appeals to. The original model for working memory, which was
proposed in 1974, consisted of three major components: a central executive, a
phonological loop, and a visuo-spatial sketchpad. Baddeley and Hitch suggested that the
phonological loop and visuo-spatial sketchpad passively hold traces of sensory
information that can cycle back and forth to the central executive. Many years later,
Baddeley revised the model to include an episodic buffer, which provided a link to long-
term memory (Baddeley, 2000).
The phonological loop, which is controlled by the left hemisphere of the brain,
maintains speech and acoustic information. When auditory stimuli are presented, memory
traces can be held in the phonological store for up to two seconds. Individuals employ
Figure 2. Baddeley-Hitch working memory model

12
articulatory rehearsal processes to recite and prevent the decay of this information.
Covert verbalization, as opposed to speaking out loud, is typically used to carry out this
process internally. Unlike the information stored in the phonological loop, the right
hemisphere of the brain maintains the visual, spatial, and kinaesthetic information stored
in the sketchpad. Because visual information is typically more difficult to remember than
auditory information, it is often converted to speech using preexisting associations. For
example, an individual that views a word on a page will typically recite this word to
himself or herself in an attempt to memorize it, rather than simply relying on their
memory of the image of the word.
Information from these subcomponents of the working memory model is actively
directed to the central executive, which was initially proposed to support storage, provide
an interface with long-term memory, and allocate attention towards different resources.
Subsequently, Baddeley and Hitch adopted the model of a supervisory attention system
(SAS), to explain how the central executive directs changes in behavior when adjusted
planning is required. This revision to the working model removed storage from the
central executive’s list of functions and designated the function of an interface with long-
term memory to a component called the episodic buffer. Consequently, the central
executive was left with the primary task of focusing and dividing attention towards
executive processes. The episodic buffer acts as a multimodal temporary store that links
traces from the phonological loop and visuo-spatial sketchpad to long-term memory in an
effort to create meaningful ideas. The capacity of this buffer is limited to the amount of
information that can be maintained simultaneously without decay. Through the flexible

13
integration of these traces, the episodic buffer is ultimately responsible for a state of
conscious awareness.
Memory During Development
Long-term memory is subdivided into categories depending on if a memory is
implicit or explicit in nature. Implicit memory is the unconscious retention of procedural
information. Simply stated, these memories instruct us how to perform learned activities
such as brushing our teeth, eating a meal, or driving a car. On the other hand, explicit
memory is the intentional remembrance of declarative and factual information.
Declarative memories are further divided into semantic memories and episodic
memories. Semantic memories are made up of concept-based knowledge, ideas, and facts
that are not drawn from personal experiences. For example, the knowledge that fish live
in water or that the United States Capitol is located in Washington, D.C. is a semantic
memory that can be explicitly recalled. Episodic memories are autobiographical events
made up from one’s personal collection of experiences. Such memories could include the
birth of a sibling or the first day of school. Together, these two subcategories make up
long-term explicit memory.
Memory storage is a complex mechanism that is largely influenced by
developmental maturation. Implicit memory, specifically priming, matures at a fairly
young age and is often fully developed by the age of four (Russo, Nichelli, Gibertoni, &
Corina, 1995). Priming, which is a unique and unconscious aspect of implicit memory,
occurs when prior exposure to a stimulus influences later exposure to that stimulus.
Children who have undergone some degree of priming typically perform better on picture
fragmentation tasks, during which prior exposure to an object would help them to better

14
identify a partial picture of that object. Even so, the accuracy of implicit material
recognition is limited in early years and increases with age (Parkin & Streete, 1988)
Further, studies have shown that the processes utilized by children to encode and recall
these memories differ from those employed by fully matured adults (Carroll, Byrne, &
Kirsner, 1985).
Explicit memory develops significantly later than implicit memory. Despite this,
the immature recollection of explicit memories often contributes to implicit memory
performance (Cycowicz, Friedman, Snodgrass, & Rothstein, 2000). This is most
commonly exhibited in priming through early autobiographical memories, which are
established during childhood between the ages of three and eight (Nelson, 1989). For
instance, a young child who possesses an autobiographical memory of their most recent
birthday party could more accurately identify a fragmented picture of a birthday party.
However, it is not until adolescence that the ability to accurately recollect personal
experiences is fully functional. At this stage, individuals have cultivated personalized
rehearsal strategies, possess a larger knowledge base, and have developed a self-
awareness of their own capabilities and limitations with memory. These properties,
amongst others, allow for the fine tuning of encoding and retrieval processes that become
more efficient with age (Ceci & Howe, 1978).

15
PSYCHOLOGICAL IMPACT ON MEMORY
Neonatal seizures resulting from HIE often have long-term negative effects on
cognitive development. In particular, patients commonly present with deficits in memory,
verbal abilities, visual abilities, and executive functions. While animal models of these
disorders thoroughly explain the physiological effects of seizures, they often fail to
suggest exactly how these effects contribute to observable memory deficits later in life.
To address this, the focus of this paper will now turn to our first set of hypotheses, in
which we will address three main memory deficits and their relationship to existing
psychological models for memory formation.
Hypothesis 1.1 – Breakdown of Executive Functions
Neonatal seizures frequently result in poor social conduct resulting from the
breakdown of executive functions, a set of skills that regulates behavior. When executive
functions are impaired, patients experience an inability to integrate past experiences with
present actions. For example, a child who is scolded for inappropriate behavior lacks the
ability to learn from his or her mistake. Because these integration deficits also correlate
with the ability to self-monitor behavior, we can conclude that the shortcomings
experienced in executive functions result from a failure within the central executive
component of memory. As discussed, the central executive functions in the allocation of
attention resources towards working memory. An impairment of the central executive’s
ability to direct attention would presumably present as a lack of focus in the individual. In
this case, the inability to retrieve, reflect upon, and manipulate information would most
certainly result in the impairment of executive functions.

16
Hypothesis 1.2 - Developmental Amnesia
When patients present with later-life developmental amnesia, explicit and
episodic memories of personal facts are affected. Despite this, semantic memories and
working memory remain intact. Because these amnesic effects appear later on in life, we
can conclude that this deficit does not result from difficulty encoding memories for
storage, but perhaps from ineffective maintenance and retrieval. In this case, we could
postulate that dysfunction occurs within the central executive, episodic buffer, or both.
The central executive accesses the episodic buffer through the medium of conscious
awareness. Thus, attention is managed. If attention is not efficiently regulated due to
failure of the central executive, retrieval and reflection on information cannot be directed
appropriately. Similarly, if developmental amnesia is due to a failure within the episodic
buffer, episodic memories cannot be retrieved from long-term memory. Therefore, it is
reasonable to construe that developmental amnesia resulting from HIE affects the
maintenance and retrieval of memories through defects in the functions of both the
central executive and the episodic buffer.
Hypothesis 1.3 - Verbal and Visual Deficits
Verbal and visual deficits are an additional concern for HIE-induced neonatal
seizures. In these cases, it is semantic memory, not episodic memory, which is affected.
As in the case of developmental amnesia, individuals experience no challenge in learning
new material but struggle to successfully carry out the transfer phase. When familiar
information is presented with new features or in novel combinations, patients fail to
associate these modified tasks to the previous ones. The deficit in recall stems from the
inability to utilize information residing in the phonological loop and visuospatial

17
sketchpad when conducting LTS searches for previously encoded associations. Impaired
control processes prevent patients from performing efficient searches and relating new
information to existing memories. In short, these individuals must create entirely new
memories without utilizing valuable associations with previously encoded memories.

18
BIOLOGICAL EFFECTS OF NEONATAL SEIZURES
With any abstract psychological phenomena, there are underlying neural
substrates that provide explanation for clinical observations. To fully understand the
origin of the cognitive deficits that result from neonatal seizures, we must explore how
seizure activity affects brain function at a molecular level. We will now present a second
set of theories that explain how synaptic plasticity at the neuronal level influences the
behavioral plasticity that is necessary for memory formation. However, before we can
delve into the neural substrates of memory we must first review the physiological effects
of seizures.
Altered Electrical Activity
During seizures, neurons abandon normal function and begin to fire in sporadic
bursts of activity, inhibiting normal brain function. Depending on the area of the brain
involved, patients may exhibit varied states of consciousness (Cavanna & Monaco,
2009). If only an isolated portion of the brain is affected, then some degree of
consciousness may be preserved, indicating a more positive long-term outcome. In the
case of HIE-induced seizures, a chronic period of ischemia and consequent hypoxia
continually deprives neurons of the substrates needed for cellular metabolism. When this
occurs during the neonatal stage, the immature brain responds by inducing a complete
and rapid necrosis of the affected tissue (Shin, Hong, Taem, & Kim, 2002). If these
effects are progressive over time, cerebral blood flow in the affected region of the brain
may be significantly altered, including changes in venous pressure, arterial pressure, etc
(Shin et al., 2002).

19
Calcification from Atrophy
After recurrent exposure to hypoxic conditions, the affected region of the brain
may begin to atrophy, resulting in an overall reduction of tissue volume (Jensen, 2009).
Atrophy from neonatal seizures is characterized by a decrease in neuronal size as well as
a loss of synaptic connections between neurons, contributing to a decrease in functional
capabilities. Additionally, atrophy from HIE often results in the calcification of ischemic
lesions. As detailed in a review by Ansar, Chincanchan, and Armstrong (1990), HIE
causes a rapid decay of the extracellular Ca2+ gradient, which plays a significant role in
the propagation of normal action potentials. Hypoxic conditions cause large quantities of
extracellular Ca2+ to rapidly flow into the cell, where it is taken up by mitochondira. This
drastic increase in mitochondrial Ca2+ inhibits normal function, ultimately resulting in
necrosis and irreversible cell death.
Decreased Synaptic Plasticity
Overall the increased propensity to seizures during the neonatal period results
from heightened neuroexcitability and augmented potential for synaptic plasticity. When
hypoxic conditions contribute to a general reduction in both the size and function of
affected regions, the developing brain exhibits a decreased potential for synaptic
plasticity. Long term potentiation (LTP), a process that is widely accepted to play a role
in learning and memory, is associated with a change in synaptic strength in response to
varied levels of transmission. Seizure-induced alterations in LTP during critical
developmental stages commonly result in the aforementioned cognitive, behavioral, and
motor deficits that plague patients far beyond childhood.

20
NEURAL SUBSTRATES OF MEMORY
The potential for plasticity, both at a synaptic and behavioral level, is highest
during early developmental periods, particularly the perinatal period that lasts from the
22nd week of gestation until seven weeks after birth (Nagy, 2011). Synaptogenesis begins
during the sixth gestational week and undergoes a prominent increase during the two
months before and after birth (Silverstein & Jensen, 2007). Initial encounters with
sensory stimuli induce fine-tuning of the neural circuit, and these connections are
strengthened by subsequent encounters (Hebb, 1949). The variation of responses to both
novel and previously encountered stimuli are influenced by trace memories from prior
experiences. These associations between stimuli are built into memory and are the basis
for the capacity to learn. The following sections will examine the various structures
associated with memory formation, as well as the molecular processes that occur within
these structures.
Anatomical Structures
The process of encoding information as a memory is complex and involves a
large number of anatomical structures. Because the first step in memory storage,
regardless of the model employed, involves the registration of sensory input, virtually
every lobe of the cortex is involved. The parietal lobe assists in the internal mediation of
attention when filtering input (Berryhill, Chein, & Olson, 2011). Further, it can facilitate
recall but cannot incorporate external cues into recognition (Dobbins, Jaeger, Studer, &
Simons, 2012). The frontal lobe functions in coordination of behaviors, working memory,
and non-task based long-term memories. Studies have found that epileptics with frontal

21
lobe damage must recruit wider areas of the brain when encoding memories for storage
(Centeno et al., 2012). In the temporal lobe, domain specificity, which suggests there are
specialized learning devices for different aspects of cognition, plays a significant role in
the recognition of information from cues. This function is critically important to the
ability to draw on associations between memories (Staresina, Cooper, & Henson, 2013).
While the perirhinal cortex is devoted specifically to object-processing, the
parahippocampal cortices are specific to scene-processing. One of the most striking
associations between an anatomical structure and memory formation occurs within the
cerebellum, which functions in the acquisition and storage of procedural memory. When
cerebellar degeneration occurs, the degree of cellular atrophy directly correlates with the
reduced capacity for motor learning (Thieme et al., 2013)
The limbic system is perhaps the greatest contributor to both the formation of
memories and the emotions associated with them (Prada-Alcala, Medina, Lopez, &
Quirarte, 2012). It encompasses a collection of structures that lie beneath the cerebrum
and on both sides of the thalamus. Two major components of the limbic system are the
amygdala and the hippocampus. The amygdala contributes primarily to emotion and fear
learning (Prada-Alcala et al., 2012; Ross & Slotnick, 2008). Conditioned fear learning
leaves a trace in the basolateral amygdala. In storing these traces, individuals either
associate the stimuli with fear or acclimate themselves to suppress fear in future
encounters. Interestingly, reactivation of this trace followed by suppressed fear can
abolish this memory altogether, in essence, attenuating the connectivity of the fear circuit
(Agren et al., 2012). Through the discovery of its participation in fear learning, the
amygdala has been recognized as a structure essential for the aversion to emotionally

22
unpleasant experiences. The hippocampus, like the amygdala, is capable of associating an
emotional response to a memory. A recent study by Bellace, Williams, Mohamed, and
Faro (2013) found that the type of stimuli associated with emotional responses dictates
the geographical location of where the memory is stored. While the right hippocampus
generates emotional responses to visual stimuli, the left hippocampus constructs
associations with auditory stimuli (Wimmer & Shohamy, 2012). In addition, the
hippocampus functions in the consolidation of memories from STS to LTS, specifically
those associated with spatial learning. When attempting to retrieve memories, fMRI
studies have shown hippocampal activation is most significant during recall rather than
during recognition (Rugg et al., 2012)
Despite the amygdala’s significant contribution to memory, the synaptic basis of
memory provided in this paper will focus specifically on studies performed in the
hippocampus. The hippocampus is unique in that it has the capacity to store large
quantities of unrelated information as well as self-generate temporally evolving
memories, those that continue to be modified over time (Buzsáki & Moser, 2013). Early
hippocampal activation indicates that there is a rapid recruitment of memory processes
within this structure that enables memory retrieval (Horner et al., 2012). During
hippocampal activity, theta waves and slow oscillations drive the preferential firing of
hippocampal cell assemblies (Battaglia, Benchenane, Sirota, Pennartz, & Wiener, 2011).
Through the propagation of these waves to other structures, the hippocampus regulates
the exchange of information with nearby structures.
Memory consolidation, the process of preparing traces for LTS, has been most
extensively studied in the CA1 region of the hippocampus, one of four subdivisions in the

23
cornu ammonis. The hippocampus receives the majority of its input from the entorhinal
cortex and is believed to be largely responsible for memory formation and consolidation,
processes that are frequently studied by examining spatial memory in rats. Information
from the entorhinal cortex travels via the perforant pathway to the dentate gyrus, CA3,
CA1, or the subiculum. Hippocampal studies often focus most closely on a pathway
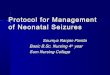
known as the trisynaptic circuit (Figure 3). In this circuit, information passes from
granule cells of the dentate gyrus to CA3 pyramidal neurons via mossy fibers. Neural
transmission runs through CA3 axons to CA1 pyramidal neurons via Schaffer collaterals.
Axons from CA1 synapse in the deep layers of the subiculum, where information can
loop back around to the entorhinal cortex or pass to the fornix. Because the trisynaptic
circuit has been widely recognized for its role in memory formation, it is important to
understand the physiologic changes that take place in these neurons.
Figure 3. Schematic of the neural circuitry within the trisynaptic circuit of the hippocampus

24
LTP and AMPA Receptor Cycling
As mentioned, LTP is an imperative process in the maintenance of synaptic
plasticity, during which synapses undergo a change in strength in response to varied
levels of transmission. These changes often directly correlate with the size of the
postsynaptic density (PSD), number of receptors, and amount of neurotransmitter
released. Since both learning and memory formation are believed to result from synaptic
plasticity, it is widely accepted that LTP plays a major role in these processes.
Neurotransmission begins when a depolarizing action potential propagates to the
terminal of a presynaptic axon. As depicted in Figure 4, presynaptic vesicles are
exocytosed from the axon terminal and their contents diffuse across the synaptic cleft.
The concentration of neurotransmitter in the synaptic cleft remains high for only a short
time, resulting in brief synaptic currents (Luscher & Malenka, 2012). Whereas receptors
on the presynaptic side participate in a feedback mechanism that modulates
neurotransmitter release, those on the postsynaptic dendrites bind neurotransmitters to
elicit a variety of cellular responses.
Figure 4. Depiction of synaptic neurotransmission that occurs during LTP (Sadava, 2008)

25
During LTP, glutamate, an important neurotransmitter, is released from the
presynaptic axon and binds to two types of ionotropic receptors: N-methyl-D-aspartate
(NMDA) receptors and α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA)
receptors. These receptors directly form ion channel pores, unlike metabotropic receptors
that indirectly link with ion channels on the plasma membrane through signal
transduction mechanisms. Both NMDARs and AMPARs are permeable to a strong
inward current of Na+ and a weak outward current of K+, in addition to a Ca2+ current.
AMPARs carry a net inward current at negative potentials and a net outward current at
positive potentials.
AMPARs are either a homomeric or heteromeric mixture of four possible
subunits: GluA1, GluA2, GluA3, and GluA4. While homomeric AMPARs contain only
one type of subunit, heteromeric AMPARs consist of two sets of symmetric subunits. The
hippocampus, which is the primary site of LTP, is characterized by heteromeric
AMPARs containing GluA2, along with either GluA1, GluA3, or GluA4 (Kauer &
Malenka, 2006). The GluA2 subunit is unique in that it undergoes RNA editing after
transcription, during which the codon for a glutamine residue in the ion channel pore is
replaced by a codon for arginine (Luscher & Malenka, 2012). This exchange of codons
enables the subunit to move out of the endoplasmic reticulum where it can be
incorporated into the AMPAR. The size of the arginine residue in modified GluA2
subunits prevents the passage of divalent ions such as Ca2+. As a result, AMPARs lacking
GluA2 are permeable to Ca2+ and have an inward-rectifying current.
Synapses that contain NMDARs with few to no AMPARs are considered “silent,”
as their ability to transmit depolarizing action potentials is significantly impaired. The

26
silent synapse hypothesis, which states that AMPARs are recruited to inactive synapses
by the induction of LTP, is based on the belief that NMDARs are capable of detecting
twice the quanta of glutamate that can be detected by AMPARs (Kullmann, Asztely, &
Walker, 2000). In theory, LTP can be modulated by NMDARs alone if the amount of
glutamate released from the presynaptic axon terminal is insufficient to open the
AMPARs located on the membrane. However, NMDARs are occluded by an Mg2+ block
that requires depolarization to be expelled. As a result, the flow of Na+, K+, and Ca2+
through the cell is a voltage-dependent process. Thus, accentuating the need for
AMPARs, which drive synaptic signaling.
It has been mentioned that the absence of AMPARs renders the synapse silent.
Therefore, it is reasonable to conclude that AMPARs are recruited to the membrane
during LTP. During cycling, AMPARs come from a reserve pool of receptors that are
stored within early endosomes (Park, Penick, Edwards, Kauer, & Ehlers, 2004). AMPAR
degradation within neurons is regulated in an activity-dependent manner that is specific
to both the type of subunit receptor and the nature of its internalization, the process of
endocytosing AMPARs from the synaptic membrane. AMPA-induced internalization
causes GluA2 subunits to enter the recycling pathway. However, NMDA-induced
internalization causes GluA2 subunits to be sent to late endosomes and lysosomes for
degradation. On the other hand, this same type of internalization causes GluA1 to remain
active in the recycling pathway (Lee, Simonetta, & Sheng, 2004). Further, the source of
AMPARs during cycling induced by LTP has been confirmed by studies using mutants
that prevent endocytotic translocation to the plasma membrane. In these cases, the overall
expression of AMPARs was significantly decreased (Park et al., 2004). AMPAR cycling

27
is regulated by the Ca2+-induced activation of Ca2+/calmodulin-dependent protein kinase
II (CaMKII) and protein kinase A (PKA), which phosphorylate serine residues on the
AMPAR subunits. The phosphorylation of serine 831 (S831) and serine 845 (S845) sites
on the GluA1 subunit during the induction of LTP causes these subunits to be inserted to
the plasma membrane (Santos, Carvalho, Caldeira, & Duarte, 2009). Interestingly, this
process depends largely on the history of the synapse itself. Immature or previously
depressed synapses can experience an intense upregulation of serine residue
phorphorylation upon the administration of high frequency stimulation (Lee et al., 2004).
However, these subunits are not delivered directly to the PSD and require NMDA
activation for their localization (Santos et al., 2009). Lipid membrane and proteins
accompany the delivery of GluA1 subunits, which explains why AMPAR cycling plays a
vital role in the increase of both synaptic strength and size.

28
PHYSIOLOGICAL IMPACT ON MEMORY
Because LTP is viewed as a long-lasting enhancement of synaptic transmission, it
is no surprise that seizure activity, which is characterized by sporadic and uncoordinated
synaptic excitation, has an effect on this process. The risk for seizures is highest during
the neonatal period, a critical time for synaptic development, during which dendritic
processes are constantly expanding and retracting, sampling their environment for
potential synaptic partners (Cline & Haas, 2008). During this time, the expression of
ionotropic glutamate receptors is at its peak and contributes to the neonate’s increased
susceptibility to seizures. In the hippocampus beginning in the first postnatal week, the
synapses gradually become functional as purely NMDAR-based synapses, silent
synapses, are converted to functional AMPAR/NMDAR synapses. This transformation is
input specific and dependent upon the occurrence of LTP (Durand, Kovalchuk, &
Konnerth, 1996). The increase in the number of activated receptors modulates the
increase in amplitude of excitatory post-synaptic currents (EPSCs) (Stubblefield &
Benke, 2010).
Hypothesis 2.1 - Induction and Saturation of LTP
The excitability observed during seizure activity induces LTP by stimulating
AMPAR cycling. Phosphorylation of the GluA1 and GluA2 subunits is evident shortly
after seizures, resulting in hyperexcitability that increases sensitivity to future seizures.
This excitability may reduce the number of silent synapses present in the neonatal brain
by recruiting AMPARs to the plasma membrane.

29
Early studies investigating the connection between seizures and synaptic plasticity
examined the effects of electroconvulsive therapy (ECT) on cognitive function. ECT, an
early form of treatment for severe affective disorder, was administered via electrical
seizure induction. Patients undergoing ECT reported difficulty in learning new material
for up to six months after treatment, especially when multiple seizures were induced
(Reid et al., 1997). Additional studies performed using adult male hooded Lister rats
aimed to emulate these effects through the induction of electroconvulsive seizures (ECS)
(Reid et al.). The study showed that the amplitude and frequency of excitatory
postsynaptic potentials (EPSPs) associated with LTP increased with each application of
ECS, stabilizing around 4-5 seizures. However, when the researchers attempted to induce
LTP following the seizures, the rats showed impaired performance in their ability to form
memories regarding spatial bias in a water maze. Overall, the over expression of EPSPs
resulted in decreased LTP. From this, it can be concluded that ECS itself induces LTP
and saturates its mechanism of action in a widespread and indiscriminate manner,
reducing overall synaptic potential.
Hypothesis 2.2 - Increased Phosphorylation of AMPA Receptors
More recent studies have focused on the effects of seizures on synaptic plasticity
in neonates, who are undergoing a period of critical synaptic development and have the
potential to experience long-term effects. In subjecting postnatal day 10 (P10) rat pups to
hypoxia-induced seizures (HS), Rakhade et al. (2008) demonstrated an increase in the
amplitude of AMPAR-mediated excitatory postsynaptic currents (EPSCs) from CA1
pyramidal neurons. The observed changes in EPSCs correlated with increased
phosphorylation of the S831 and S845 sites on GluA1. Therefore, it is reasonable to

30
conclude that increased AMPAR-mediated currents were a result of increased GluA1
phosphorylation.
In addition to the alterations experienced by GluA1, HS appeared to cause a
significant increase in the phosphorylation of GluA2. P10 rat pups naturally have Ca2+
permeable AMPARs due to decreased GluA2 expression. HS further decreased the
expression of GluA2 on the synaptic membrane 48 hours after stimulation via
phosphorylation of the serine 880 (S880) site, resulting in GluA2-lacking AMPARs that
produced an inward rectifying current. PKA and CaMKII are responsible for the
phosphorylation of S845, while protein kinase C (PKC) phosphorylates both S831 and
S880 (Santos et al., 2009). Since increased stimulation of LTP correlates with an increase
in the phosphorylation of S831, S845, and S880, it is reasonable to suspect that increased
activity of PKA, CaMKII, and PKC is also observed. Further, it was found that the
GluA2-lacking AMPAR antagonist philanthotoxin was capable of blocking LTP if
applied before and during stimulation (Plant et al., 2006). Combined, these results
provide further evidence that the Ca2+ flow permitted by GluA2-lacking AMPARs is
necessary for the induction of LTP during development.
Hypothesis 2.3 - Reduction of Silent Synapses
Because studies have established that the HS-stimulated increase in
phosphorylation of AMPAR subunits caused a profound effect on LTP, it can be
hypothesized that the phosphorylation induced by HS may alter the fraction of silent
synapses present on the postsynaptic membrane. Silent synapses, which lack AMPARs
altogether, are characterized by a large failure rate when attempting to evoke EPSCs at
negative membrane potentials of -55mV to -65mV (Rakhade et al., 2008). A study by

31
Zhou, Lippman, Sun, and Jensen (2011) noted that as predicted, the ratio of silent to
functional synapses in P10 rat pups was reduced during HS. The possibility of Mg2+
insensitivity was ruled out as a factor, indicating that NMDARs did not contribute to the
failure rate of EPSCs used to calculate these ratios (Zhou et al., 2011). Additionally, the
effects of hypoxia alone were found to be negligible due to the lack of difference between
hypoxic pups that did not experience seizures and the control group. Together, these
results suggest that HS diminished silent synapses by simply introducing AMPARs to the
membrane.
Further, HS appeared to increase the colocalization of AMPARs and NMDARs
across the membrane. Synaptophysin, GLUR1, and NR1, functional subunits from each
receptor, were triple immunolabeled to detect the presence of NR1 puncta that were in
contact with both synaptophysin puncta and GLUR1 puncta (Zhou et al., 2011). HS
decreased the percentage of synapses containing only contacts between NR1 puncta and
synaptophysin puncta, indicating that HS decreased the number of silent synapses (Zhou
et al., 2011). The reduction in silent synapses by increased colocalization can be inferred
to be a result of AMPAR subunit phosphorylation, which ultimately moves AMPARs to
the membrane. It is important to note that these processes occur during normal
stimulation of LTP. However, the occurrence of a seizure magnifies these effects and
unnecessarily induces LTP in an unregulated manner. In effect, seizures saturate the
mechanism and inhibit the ability to induce LTP during actual learning and memory
formation.

32
CONCLUSION
Neonatal seizures, particularly those due to HIE, are a significant problem in both
term and pre-term infants and are influenced by a variety of inherent risk factors.
Neonates exhibit the highest proclivity to seizure activity due to their heightened
potential for neuroexcitation, a property that has a profound impact on the potential for
synaptic plasticity. Early life neonatal seizures are commonly associated with long-term
cognitive impairments, such as those seen in learning and memory. While not classified
as an epileptic disorder, the occurrence of seizures during the neonatal period increases
susceptibility to epilepsy far into adulthood.
Through a comprehensive understanding of existing memory paradigms, such as
Atkinson and Schiffrin’s multi-store model and Baddeley and Hitch’s working memory
model, we can begin to explain how neonatal seizures result in impaired executive
function, verbal and visual function, and memory storage processes. During this critical
time for development, seizure activity alters the function of memory components that are
critical to both STS and LTS. Additionally, seizures disrupt the control processes used
when attempting to process sensory stimuli, to prevent the decay of traces from STS, and
to retrieve memories from LTS. From this, we can deduce that the apparent memory
damage resulting from neonatal seizures is attributed to the third model proposed by
Martinos et al. (2012) in an effort to explain the source of cognitive dysfunction. In this
model, it is suggested that both an inherent predisposition to neonatal seizures, as well as
the seizure itself, contribute to the cognitive deficits seen in these individuals.
On a physiologic level, the impairments seen in these individuals can be
explained through the relationship between memory formation and LTP. LTP, a process

33
that is widely accepted to play a role in learning and memory, is associated with a change
in synaptic strength in response to varied levels of transmission. Alterations in LTP
during critical developmental stages commonly result in cognitive, behavioral, and motor
deficits that plague patients far beyond childhood. Rat studies have found that HIE-
induced seizures induce the activation of various kinases that phosphorylate serine
residues on AMPAR subunits. This process triggers the mobilization of AMPARs to the
synaptic membrane, thus decreasing the ratio of silent to active synapses and allowing for
heightened synaptic potential. Overall, these studies have found that seizure activity
overstimulates LTP, thus saturating its mechanism and reducing the potential for
effective memory storage. Thus, resulting in many forms of memory impairment and
cognitive setbacks.
In this paper, we have presented two related, yet distinctly separate sets of
hypotheses that explain the cognitive deficits from seizures by means of both
psychological and physiological perspectives. Using the various STS and LTS
components from existing memory models, we have explained the theoretical basis of
seizure-induced cognitive deficits. Additionally, we have used findings from studies at a
synaptic level to propose an association between the neural substrates of memory and the
neural substrates of seizures. However, the direct relationship between these neural
substrates and the memory components that they ultimately affect is beyond the scope of
this paper and future studies are needed to more clearly elucidate this relationship.

34
BIBLIOGRAPHY
Agren, T., Engman, J., Frick, A., Björkstrand, J., Larsson, E. M., Furmark, T., &
Fredrikson, M. (2012) Disruption of reconsolidation erases a fear memory trace in
the human amygdala. Science, 337(6101), 1550-1552.
Ansari, M. Q., Chincanchan, C. A., & Armstrong, D. L. (1990) Brain calcifications in
hypoxic-ischemic lesions: an autopsy review. Pediatric Neurology, 6(2), 94-101.
Baddeley, A. D. (2000) The episodic buffer: a new component of working memory?
Trends in Cognitive Science, 4(11), 417-423.
Baddeley, A. D., & Hitch, G. J. (1974) Working memory. New York: Academic Press.
Battaglia, F. P., Benchenane, K., Sirota, A., Pennartz, C. M. A., & Wiener, S. I. (2011)
The hippocampus: hub of brain network communication for memory. Trends in
Cognitive Sciences, 15(7), 310-318.
Bellace, M., Williams, J. M., Mohamed, F. B., & Faro, S. H. (2013) An fMRI study of
the activation of the hippocampus by emotional memory. International Journal of
Neuroscience, 123(2), 121-127.
Berryhill, M. E., Chein, J., & Olson, I. R. (2011) At the intersection of attention and
memory: the mechanistic role of the posterior parietal lobe in working memory.
Neuropsychologia, 49(5), 1306-1315.
Binford, J. R., & Gettys C. (1965) Nonstationarity in paired-associate learning as
indicated by a second guess procedure. Journal of Mathematical Psychology, 2,
190-195.
Bonelli, S. B., Thompson, P. J., Yogarajah, M., Powell, R. H. W., Samson, R. S.,
McEvoy, A. W., . . . Duncan, J. S. (2013) Memory reorganization following

35
anterior temporal lobe resection: a longitudinal functional MRI study. Brain: A
Journal of Neurology, 136(6), 1889-1900.
Buschman, T. J., Siegel, M., Roy, J. E., & Miller, E. K. (2011) Neural substrates of
cognitive capacity limitations. Proceedings of the National Academy of Sciences
of the United States of America, 108(27), 11252-11255.
Buzsáki, G., & Moser, E. I. (2013) Memory, navigation and theta rhythm in the
hippocampal-entorhinal system. Nature Neuroscience, 16(2), 130-138.
Carroll, M. V., Byrne, B., & Kirsner, K. (1985) Autobiographical memory and perceptual
learning: a developmental study using picture recognition, naming latency, and
perceptual identification. Memory and Cognition, 13(3), 273-279.
Cavanna, A. E., & Monaco, F. (2009) Brain mechanisms of altered conscious states
during epileptic seizures. Nature Reviews Neurology, 5, 267-276.
Ceci, S. J., & Howe, M. J. A. (1978) Semantic knowledge as determinant of
developmental differences in recall. Journal of Experimental Child Psychology,
26, 230-245.
Centeno, M., Vollmar, C., O'Muircheartaigh, J., Stretton, J., Bonelli, S. B., Symms, M.
R., . . . Koepp, M. J. (2012) Memory in frontal lobe epilepsy: an fMRI study.
Epilepsia, 53(10), 1756-1764.
Cline, H., & Haas, K. (2008) The regulation of dendritic arbor development and plasticity
by glutamatergic synaptic input: a review of the synaptotrophic hypothesis.
Journal of Physiology, 586(6), 1509-1517.
Cowan, L. D. (2002) The epidemiology of the epilepsies in children. Mental Retardation
and Developmental Disabilities Research Reviews, 8(3), 171-181.

36
Cowan, L. D., Rutherford, M., Groenendaal, F., Eken, P., Mercuri, E., Bydder, G. M., . . .
de Vries, L. S. (2003) Origin and timing of brain lesions in term infants with
neonatal encephalopathy. Lancet, 361(9359), 736-742.
Cycowicz, Y. M., Friedman, D., Snodgrass, J. G., & Rothstein, M. (2000) A
developmental trajectory in implicit memory is revealed by picture fragment
completion. Memory, 8(1), 19-35.
Dehaes, M., Aggarwal, A., Lin, P.-Y., Rosa Fortuno, C., Fenoglio, A., Roche-Labarbe,
N., . . . Grant, P. E. (2013) Cerebral oxygen metabolism in neonatal hypoxic
ischemic encephalopathy during and after therapeutic hypothermia. Journal of
Cerebral Blood Flow and Metabolism, August, 1-8.
Dobbins, I. G., Jaeger, A., Studer, B., & Simons, J. S. (2012) Use of explicit memory
cues following parietal lobe lesions. Neuropsychologia, 50(13), 2992-3003.
Durand, G. M., Kocalchuk, Y., & Konnerth, A. (1996) Long-term potentiation and
functional synapse induction in developing hippocampus. Nature, 381, 71-75.
Gano, D., Sargent, M. A., Miller, S. P., Connolly, M. B., Wong, P., Glass, H. C., . . .
Chau, V. (2013) MRI findings in infants with infantile spasms after neonatal
hypoxic-ischemic encephalopathy. Pediatric Neurology, 49(6), 401-405.
Glass, H. C., Glidden, D., Jeremy, R. J., Barkovich, A. J., Ferriero, D. M., & Miller, S. P.
(2009) Clinical neonatal seizures are independently associated with outcome in
infants at risk for hypoxic-ischemic brain injury. The Journal of Pediatrics,
155(3), 318-323.
Hallberg, B., & Blennow, M. (2013) Investigations for neonatal seizures. Seminars in
Fetal & Neonatal Medicine, 18(4), 196-201.

37
Harbert, M. J., Tam, E. W. Y., Glass, H. C., Bonifacio, S. L., Haeusslein, L. A.,
Barkovich, a. J., . . . Ferriero, D. M. (2011) Hypothermia is correlated with
seizure absence in perinatal stroke. Journal of Child Neurology, 26(9), 1126-
1130.
Hebb, D. O. (1949) The Organization of Behavior: A Neuropsychological Theory. New
York: Wiley and Sons.
Horner, A. J., Gadian, D. G., Fuentemilla, L., Jentschke, S., Vargha-Khadem, F., &
Duzel, E. (2012) A rapid, hippocampus-dependent, item-memory signal that
initiates context memory in humans. Current Biology, 22(24), 2369-2374.
Jensen, F. E. (2009) Developmental factors in the pathogenesis of neonatal seizures.
Journal of Pediatric Neurology, 7(1), 5-12.
Kauer, J. A., & Malenka, R. C. (2006) News and views: LTP and AMPA receptors
trading places. Nature Neuroscience, 9(5), 593-594.
Kohelet, D., Shochat, R., Lusky, A., & Reichman, B. (2006a) Risk factors for neonatal
seizures in very low birthweight infants: population-based survey. Journal of
Child Neurology, 19(2), 123-128.
Kohelet, D., Shochat, R., Lusky, A., & Reichman, B. (2006b) Risk factors for seizures in
very low birthweight infants with periventricular leukomalacia. Journal of Child
Neurology, 21(11), 965-970.
Kullmann, D. M., Asztely, F., & Walker, M. C. (2000) The role of mammalian ionotropic
receptors in synaptic plasticity: LTP, LTD and epilepsy. Cellular and Molecular
Life Sciences, 57(11), 1551-1561.

38
Kurabe, S., Sorimachi, T., Sasaki, O., Koike, T., & Fujii, Y. (2009) Low birth weight as a
risk factor for seizure following acute subdural hematoma. Child's Nervous
System, 25(9), 1101-1104.
Lee, S. H., Simonetta, A., & Sheng, M. (2004) Subunit rules governing the sorting of
internalized AMPA receptors in hippocampal neurons. Neuron, 43, 221-236.
Lindstrom, K., Hallberg, B., Blennow, M., Wolff, K., Fernell, E., & Westgren, M. (2008)
Moderate neonatal encephalopathy: pre- and perinatal risk factors and long-term
otcome. Acta Obstetricia et Gynecologica Scandinavica, 87, 503-509.
Luscher, C., & Malenka, R. C. (2012) NMDA receptor-dependent long-term potentiation
and long-term depression (LTP/LTD). Cold Spring Harbour Perspectives in
Biology, 4, 1-15.
Martinos, M. M., Yoong, M., Patil, S., Chin, R. F., Neville, B. G., Scott, R. C., & de
Haan, M. (2012) Recognition memory is impaired in children after prolonged
febrile seizures. Brain, 135(10), 3153-3164.
Milner, B. (1959) The memory defect in bilateral hippocampal lesions. Psychiatric
Research Reports, 11, 43-58.
Milner, B. (1967) Amnesia following operation on the temporal lobes. In O. L. Zangwill
and C. W. M. Whitty (Eds.), Amnesia (109-133). London and Washington, D.C.:
Butterworth.
Nagy, E. (2011) The newborn infant: a missing stage in developmental psychology.
Infant and Child Development, 20, 3-19.
Nelson, K. (1989) Remembering: A Functional Developmental Perspective. New York:
Springer.

39
Odd, D. E., Gunnell, D., Lewis, G., & Rasmussen, F. (2011) Long-term impact of poor
birth condition on social and exonomic outcomes in early adulthood. Pediatrics,
127, 1498-1504.
Park, M., Penick, E. C., Edwards, J. G., Kauer, J. A., & Ehlers, M. D. (2004) Recycling
endosomes supply AMPA receptors for LTP. Science, 305(5692), 1972-1975.
Parkin, A. J., & Streete, S. (1988) Implicit and explicit memory in young children and
adults. British Journal of Psychology, 79(3), 361-369.
Perez, A., Ritter, S., Brotschi, B., Werner, H., Caflisch, J., Martin, E., & Latal, B. (2013)
Long-term neurodevelopmental outcome with hypoxic-ischemic encephalopathy.
The Journal of Pediatrics, 163(2), 454-459.
Peterson, L. R., & Peterson, M. (1959) Short-term retenion of individual verbal items.
Journal of Experimental Psychology, 58, 193-198.
Plant, K., Pelkey, K. A., Bortolotto, Z. A., Morita, D., Terashima, A., McBain, C. J., . . .
Isaac, J. T. R. (2006) Transient incorporation of native GluR2-lacking AMPA
receptors during hippocampal long-term potentiation. Nature Neuroscience, 9(5),
602-604.
Prada-Alcala, R. A., Medina, A. C., Lopez, N. S., & Quirarte, G. L. (2012) Intense
emotional experiences and enhanced training prevent memory loss induced by
post-training amnesic treatments administered to the striatum, amygdala,
hippocampus or substantia nigra. Annual Review of Neuroscience, 23(5-6), 501-
508.

40
Rakhade, S. N., Zhou, C., Aujla, P. K., Fishman, R., Sucher, N. J., & Jensen, F. E. (2008)
Early alterations of AMPA receptors mediate synaptic potentiation induced by
neonatal seizures. The Journal of Neuroscience, 28(32), 7979-7990.
Reid, I. A. N. C., Stewart, A., & Stewart, C. A. (1997) Seizures, memory and synaptic
plasticity. Seizure: European Journal of Epilepsy, 6(5), 351-359.
Ross, R. S., & Slotnick, S. D. (2008) The hippocampus is preferentially associated with
memory for spatial context. Journal of Cognitive Neuroscience, 20(3), 432-446.
Rugg, M. D., Vilberg, K. L., Mattson, J. T., Yu, S. S., Johnson, J. D., & Suzuki, M.
(2012) Item memory, context memory and the hippocampus: fMRI evidence.
Neuropsychologia, 50(13), 3070-3079.
Russo, R., Nichelli, P., Gibertoni, M., & Corina, C. (1995) Developmental trends in
implicit and explicit memory: a picture completion study. Journal of
Experimental Child Psychology, 59, 566-578.
Sadava, D. E. (2008) Life: The Sciences of Biology. Maryland: Sinauer Associates.
Sans, A. (2011) Developmental amnesia as a focal cognitive sequela of a neonatal
pathology. Revista de Neurologiá, 52(1), S29-38.
Santos, S. D., Carvalho, A. L., Caldeira, M. V., & Duarte, C. B. (2009) Regulation of
AMPA receptors and synaptic plasticity. Neuroscience, 158(1), 105-125.
Shankaran, S. (2009) Neonatal encephalopathy: treatment with hypothermia. Journal of
Neurotrama, 26(3), 437-443.
Shin, W. C., Hong, S. B., Tae, W. S., & Kim, S. E. (2002) Ictal hyperfusion patterns
according to the progression of temporal lobe seizures. Neurology, 58, 373-380.

41
Silverstein, F. S., & Jensen, F. E. (2007) Neonatal seizures. Annals of Neurology, 62(2),
112-120.
Staresina, B. P., Cooper, E., & Henson, R. N. (2013) Reversible information flow across
the medial temporal lobe: the hippocampus links cortical modules during memory
retrieval. The Journal of Neuroscience, 33(35), 14184-14192.
Stubblefield, E. A., & Benke, T. A. (2010) Distinct AMPA-type glutamatergic synapses
in developing rat CA1 hippocampus. Journal of Neurophysiology, 104, 1899-
1912.
Thieme, A., Thürling, M., Galuba, J., Burciu, R. G., Göricke, S., Beck, A., . . . Timmann,
D. (2013) Storage of a naturally acquired conditioned response is impaired in
patients with cerebellar degeneration. Brain: A Journal of Neurology, 136(7),
2063-2076.
van Handel, M., de Sonneville, L., de Vries, L. S., Jongmans, M. J., & Swaab, H. (2012)
Specific memory impairment following neonatal encephalopathy in term-born
children. Developmental Neuripsychology, 37, 30-50.
van Rooij, L. G. M., van den Broek, M. P. H., Rademaker, C. M. A., & de Vries, L. S.
(2013) Clinical management of seizures in newborns: diagnosis and treatment.
Paediatric Drugs, 15(1), 9-18.
Viggedal, G., Kristjansdottir, R., Olsson, I., Rydenhag, B., & Uvebrant, P. (2012)
Cognitive development from two to ten years after pediatric epilepsy surgery.
Epilepsy & Behavior, 25(1), 2-8.
Wimmer, G. E., & Shohamy, D. (2012) Preference by association: how memory
mechanisms in the hippocampus bias decisions. Science, 338(6104), 270-273.

42
Zhou, C., Lippman, J. J. B., Sun, H., & Jensen, F. E. (2011) Hypoxia-induced neonatal
seizures diminish silent synapses and long-term potentiation in hippocampal CA1
neurons. The Journal of Neuroscience, 31(50), 18211-18222.