Embed Size (px)
Citation preview
MONITORING OF ANTICOAGULATION FOR PEDIATRIC CARDIOPULMONARY
BYPASS
David R. Jobes MDProfessor of Anesthesia and Critical CareThe Children’s Hospital of Philadelphia
University of Pennsylvania School of Medicine

MONITORING OF ANTICOAGULATION FOR PEDIATRIC CARDIOPULMONARY BYPASS
• Goal of Monitoring• History of Heparin in CPB• Mechanisms of Action and Monitoring• Pediatric Application• Problems – Use and Interpretation• The Big Picture and Future Improvements

GOALS OF MONITORING
• Inhibit Coagulation System Response to CPB– Prevent Thrombus Formation– Prevent Coagulopathy
• Establish and Maintain Optimal Heparin Effect
• Outcomes of Clinical Importance– Eliminate thrombus/bleeding/transfusion
related to heparin

HISTORY OF UFH USE IN CPB 1954 – 1970’s
• Trial And Error – Body Weight ; ½ Life
• Specific Patient Variability Unknown - Excess
• Prevention Of Visible Thrombus/Fibrin
• Fibrin Strands On Reservoir Wall

HISTORY OF UFH USE IN CPB 1970’s
• Test Based Dose, Maintenance and Reversal
• ACT = >300sInterchangeable with
Hep conc. >/= 3 u/ml• Accounts for Patient
Variability – Avoid Excess• Prevent Fibrin/Thrombus
Activated WB (ACT)
Protamine Titration

HISTORY OF UFH USE IN CPB 1980’s – 2011
• Change of Goal – – Fibrin precursor inhibition– Preservation of protein function for
hemostasis• Change of Pediatric Population –
– Younger smaller patients – TOF, Single Ventricle, ASO, etc.

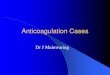
F1.2
+ ATIII
TAT

Copyright ©1994 The American Association for Thoracic Surgery
Despotis G. J. et al.; J Thorac Cardiovasc Surg 1994;108:1076-1082
ACT vs. ANTI Xa vs. HEPARIN CONCENTRATION
THE “PEDIATRIC” POPULATION
• Younger, Smaller Patients• Increased Complexity of Repair• Greater Dilution >50%
– Circuit Size– Polycthemia (Cyanosis) – Reduced Plasma
Volume• Greater Reactivity to CPB• Younger = Greater Risk Of Bleeding/Transfusion
1 Day 5 Day 1 Mo 3 Mo 6 Mo 1-5 Yr 6-10 Yr 11-16 Yr Adult0
0.2
0.4
0.6
0.8
1
1.2
1.4
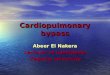
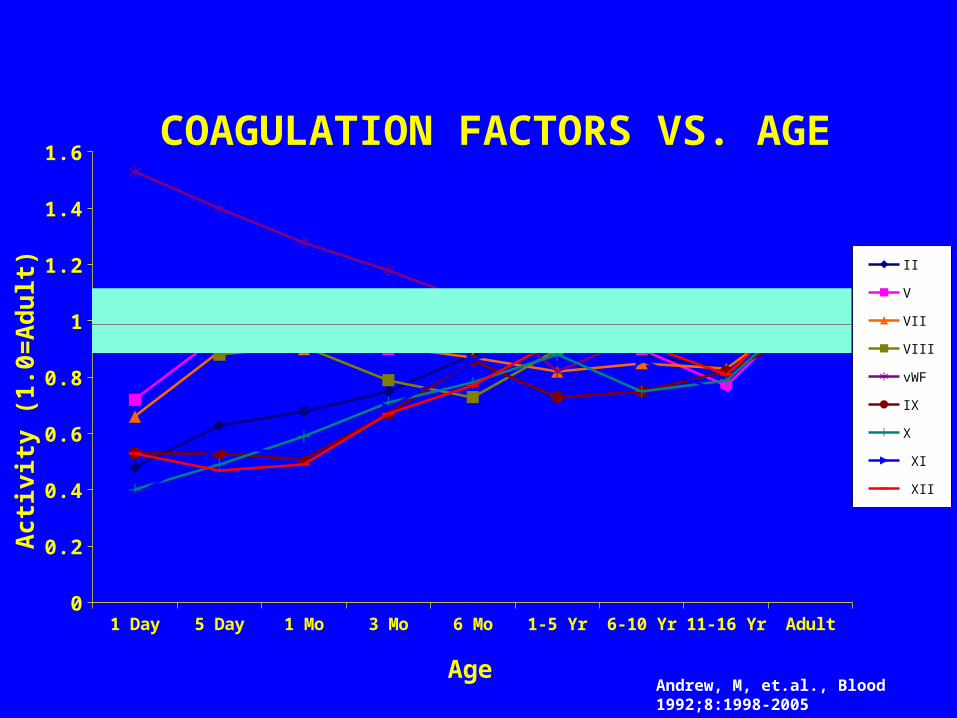
1.6COAGULATION FACTORS VS. AGE
II
V
VII
VIII
vWF
IX
X
XI
XII
Age
Ac
tivi
ty (
1.0
=A
du
lt)
Andrew, M, et.al., Blood 1992;8:1998-2005
1 Day 5 Day 1 Mo 3 Mo 6 Mo 1-5 Yr 6-10 Yr 11-16 Yr Adult0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
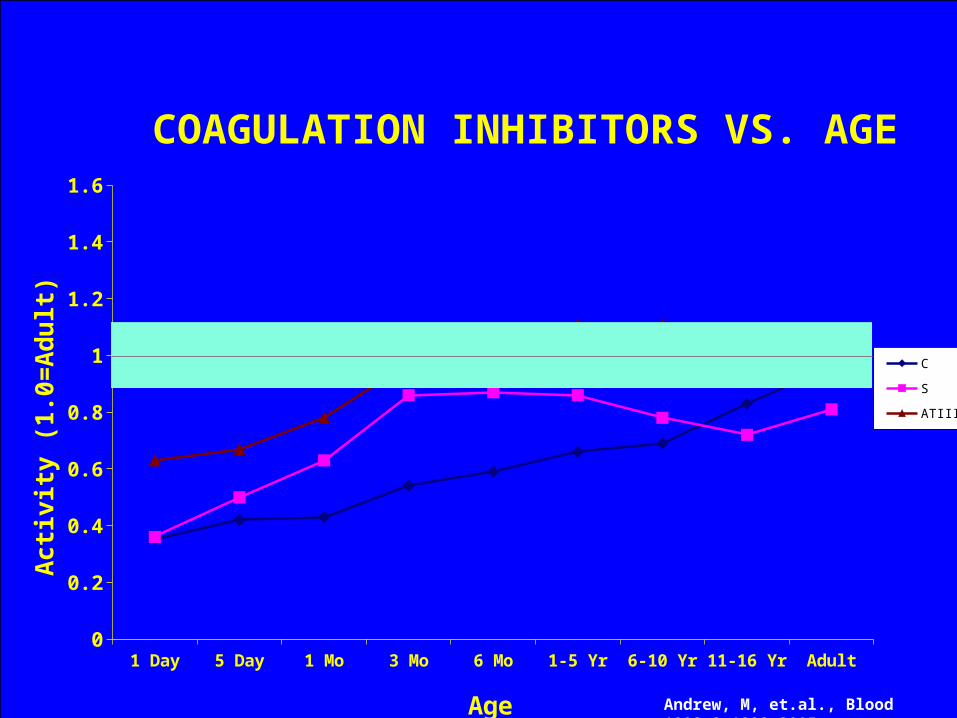
COAGULATION INHIBITORS VS. AGE
C
S
ATIII
Age
Act
ivit
y (1
.0=
Ad
ult
)
Andrew, M, et.al., Blood 1992;8:1998-2005

010
020
030
040
0H
epar
in S
ensi
tivity
(se
c/(u
nit/m
l))
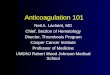
0 1.5 3 4.5 6Pediatric
010
020
030
040
0
40 55 70Adult
Age (years)
Heparin Sensitivity vs. Age
** 3 Patients (all three days of age) had heparin sensitivities which exceeded test capabilities
Jobes, DR, et.al., Cardiology in the Young 1993
INVITRO HEPARIN SENSITIVITY VS. AGE

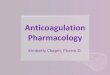
UFHINVIVO VARIABILITY & AGE
• 1,183 Patients – CHOP –1995-2004• No Precedent Anticoagulants • UFH 200units/kg• ACT (Hemochron CA510)• 600 sec Maximum ACT Recorded

010
0P
erce
nt
300 400 500 600ACT (sec) 200 u/kg Heparin
N = 826
1-5 Years
29%

010
0P
erce
nt
300 400 500 600ACT (sec) 200 u/kg Heparin
N = 57
6 Months
47%
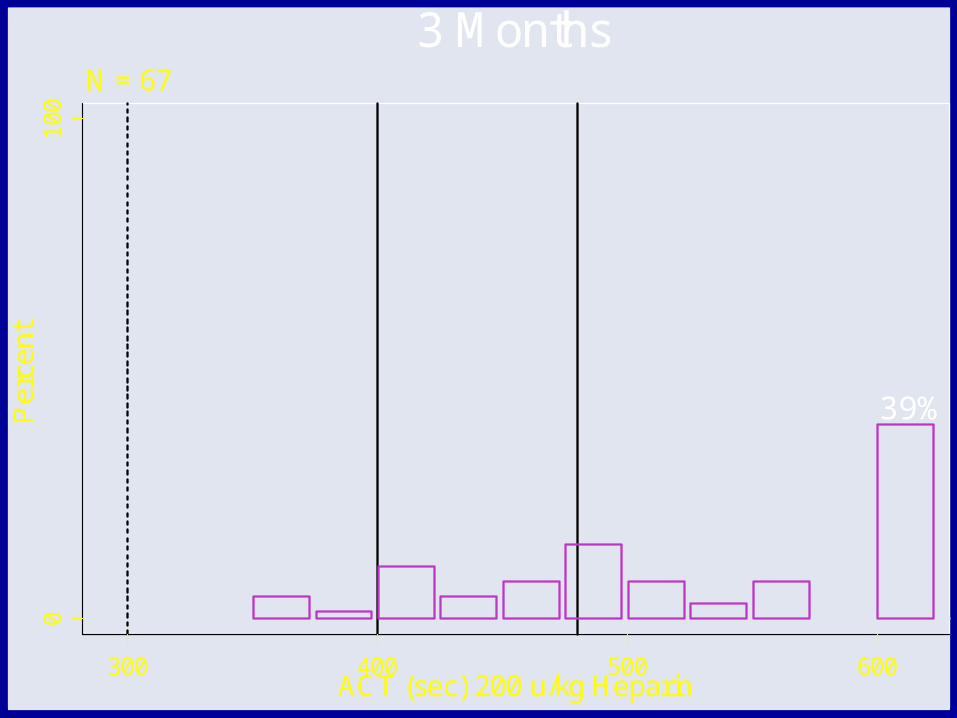
010
0P
erce
nt
300 400 500 600ACT (sec) 200 u/kg Heparin
N = 67
3 Months
39%

010
0P
erce
nt
300 400 500 600ACT (sec) 200 u/kg Heparin
N = 55
1 Month
44%

80%
010
0P
erce
nt
300 400 500 600ACT (sec) 200 u/kg Heparin
N = 91
5 Days
77%

010
0P
erce
nt
300 400 500 600ACT (sec) 200 u/kg Heparin
N = 87
1 Day
94%

HEPARIN CONCENTRATION & ANTI Xa – PEDIATRIC CPB
• Gruenwald 2000 – < 1 yr. No (not significantly correlated)
• Codespoti 2001 – 4- 5 yr. Yes (“interchangeable”)
• Guzzetta 2010 – < 6 mos. Yes (“satisfactory agreement”) - (less hemodilution?)

OPTIMIZING UFH IN PEDIATRIC CPB
• Focus on Precursor Suppression – No thrombus/fibrin– Suppress thrombin formation- inhibit FXa – Eliminate F1.2, TAT
• UFH Dose Based on Individual Sensitivity (not empiric)
• Combine ACT and Heparin Concentration• Protamine Dose Based on Actual Circulating
Heparin (not empiric)

Control Codespoti 2001 Guzzetta 2008 Gruenwald 2010N 26 25 90Age 4-5yo average < 6 mos. < 1yr.Circuit ?
oxygenator Silicone membrane Hollow fiber ?coated ? Yes ?volume ~ 50% dilution 300 ml. ?PRBC No Yes Yes
plasma No No Yesplatelets No No Yesalbumin ? ? ?
MUF Yes No YesUFH initial Body weight ACT+Conc. ACT+Conc. ACT+Conc.
Prot DoseRatio or Body
Weight ACT+Conc. ACT+Conc. ACT+Conc.ACT 480s 480s 480s 480s ?Hep. Conc. No qs - ACT qs - ACT qs - ACTF1.2
eliminated No No Noreduced Yes Yes Yes
Blood loss Reduced Not different Increased/Not differentTotal Donor exp. ? Increased Not different/Not different
ACT+CONCENTRATION

ISSUES
• UFH Is Poor Inhibitor Of Coagulation – Limits• Heparin and Protamine Negatively Affect Platelets• Studies Not Generalizable – Lack Standardization
– Population – age– Circuit –surface type and area, prime volume
and quality– Duration of exposure – pump time– Surgical issues – operator, materials, tissue
integrity

ISSUESCHANGING ELEMENTS OVER TIME
• Activated Clotting Time– Activators – celite, kaolin, tissue factor,
glass beads, etc. – End point detection- mechanical
(rotating magnet, iron filing+magnet), optical, pressure, etc.
• Heparin– Source – bovine lung, porcine mucosa,
other?– Variability - “unfractionated”
composition– Potency – FDA – 10% reduction
LESSONS LEARNED
• Test Based Monitoring Prevents Thrombus/Fibrin Formation
• Test Based Dosing + Monitoring (ACT or ACT+Conc.) Reduced Bleeding/Transfusion In Older Patient Populations
• Concepts Or Formulas Derived In Older Patients May Not Benefit And May Cause Problems
• Neonates And Infants Most Difficult – Maturation of Factors And Dilution
• Many Confounding Variables – Can Reduce F1.2 But Not Change Bleeding/Transfusion Outcome

WHAT TO DO• Patient Specific Dosing Is Right Direction - Both
Heparin And Protamine - Maintain Effect & Avoid Excess
• Recognize Limits Of An Imperfect Drug (UFH), Test Methodology (POC), Study Results
• Platelet Protection
• Lysis Contribution – Measure/Treat – Patient Specific

BIG PICTURE
• Dilution – Reduce circuit size– “Bloodless” CPB surgery neonates
• Stimulus– Biocompatible surfaces- pump, oxygenator,
tubing– Biocompatible materials – patches, conduits– Bypass time – fast and accurate surgery
• Meticulous surgical hemostasis

THE CHILDREN’S HOSPITAL OF PHILADELPHIA
“HOPE LIVES HERE”
THANK YOU FOR LISTENING!