Embed Size (px)
Citation preview
Module 4 1
Module 4Pharmacologic Management
of Hyperglycemia in the Hospital
Part 1: Understanding How to Use Insulin
Diabetes Special Interest GroupGeorgia Hospital Association
Module 4 2
Learning Modules
Module no. Topic
1 Hyperglycemia and hospital outcomes
2 Challenges and opportunities for care improvement
3 Initial recognition, triaging, and management
4 Pharmacologic management: Insulin 1
5 Pharmacologic management: Insulin 2
6 Review of policies and procedures
7 Getting patients ready for discharge
Module 4 3
Summary Thus Far
• Hospital hyperglycemia is associated with poorer patient outcomes
• Treating hospital hyperglycemia improves patient outcomes
• There is room to improve care at most hospitals
• Recognize and treat hyperglycemia early
Module 4 4
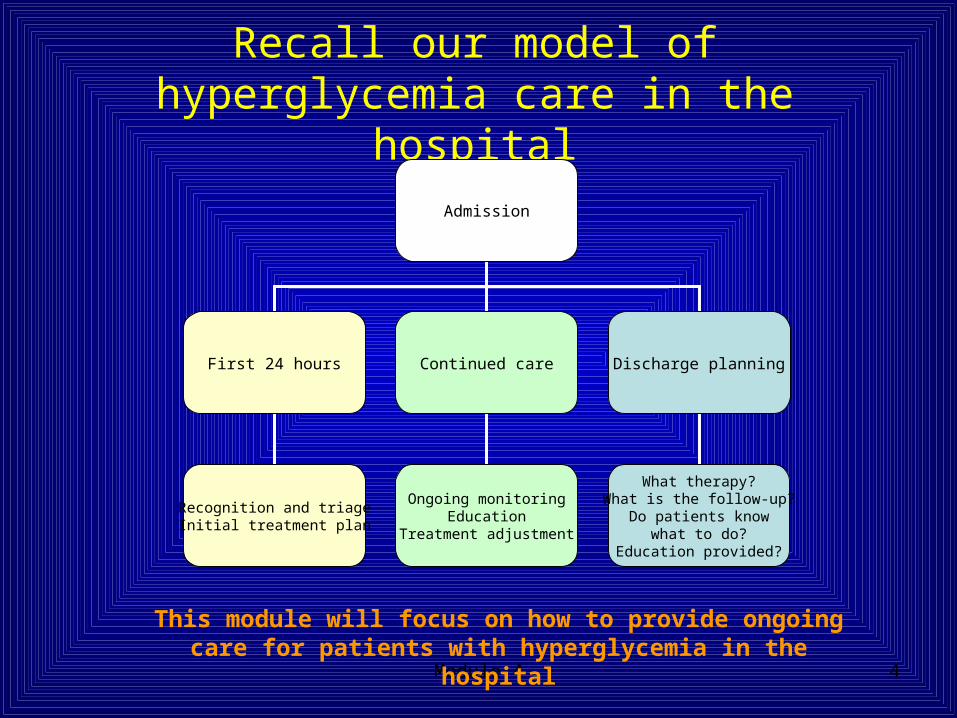
Recall our model of hyperglycemia care in the hospital
Admission
First 24 hours Continued care
Recognition and triageInitial treatment plan
Ongoing monitoringEducation
Treatment adjustment
Discharge planning
What therapy?What is the follow-up?
Do patients knowwhat to do?
Education provided?
This module will focus on how to provide ongoing care for patients with hyperglycemia in the hospital
Module 4 5
Objectives
• Review treatment of inpatient hyperglycemia
• Discuss principles of insulin therapy
• Review how to calculate insulin doses
• Describe how to adjust insulin therapy
Module 4 6
Continuing Care Actions• Evaluate bedside glucose values daily• Adjust therapy if needed• Assess patient knowledge and obtain
diabetes education consult if indicated• Document in progress notes:
– The problem of diabetes and hyperglycemia– Whether diabetes is controlled or uncontrolled
(that’s how our coders bill)—if you have to change therapy, it is probably uncontrolled
– Any changes in therapy
Module 4 7
Treating Inpatient HyperglycemiaWhat should we use?
• Concerns about oral hypoglycemic agents– Little data on outcomes in the hospital– Slow onset of action– Limited dose titration
• Concerns over specific agents– Sulfonylureas—worries over inpatient cardiovascular
outcomes and hypoglycemic events when meals are missed
– Metformin—concerns over lactic acidosis, creatinine should be less than 1.4, must be held when contrast studies performed
– TZDs—fluid retention, contraindicated if LFTs are elevated
Module 4 8
Treating Inpatient HyperglycemiaIs there any role for oral agents in
the hospital?
• Situations where we use oral agents– Patients already on oral agents admitted for
short stays (e.g. elective surgical procedures)– Rehab patients who have recovered from their
acute illness
Insulin is the favored drug for treatment of acutely ill inpatients with hyperglycemia.
Module 4 9
Advantages of Insulin Therapy in the Hospital
• Adaptable to:– Rapidly changing clinical situations that affect
glucose levels– Various forms of nutritional support
• NPO• IV dextrose• Total parenteral nutrition• Enteral feeding• Eating
Module 4 10
Three components of insulin therapy
• Basal (long-acting) insulin: component needed to prevent gluconeogenesis and ketogenesis
• Meal (Prandial) Bolus insulin: component that covers meals and other carbohydrate sources
• Corrective insulin: component needed to cover unexpected glucose excursions (e.g. from stress) – Can be pre-calculated and written as algorithm– Not the same as “sliding scale”– Tries to account for individual insulin sensitivity
Module 4 11
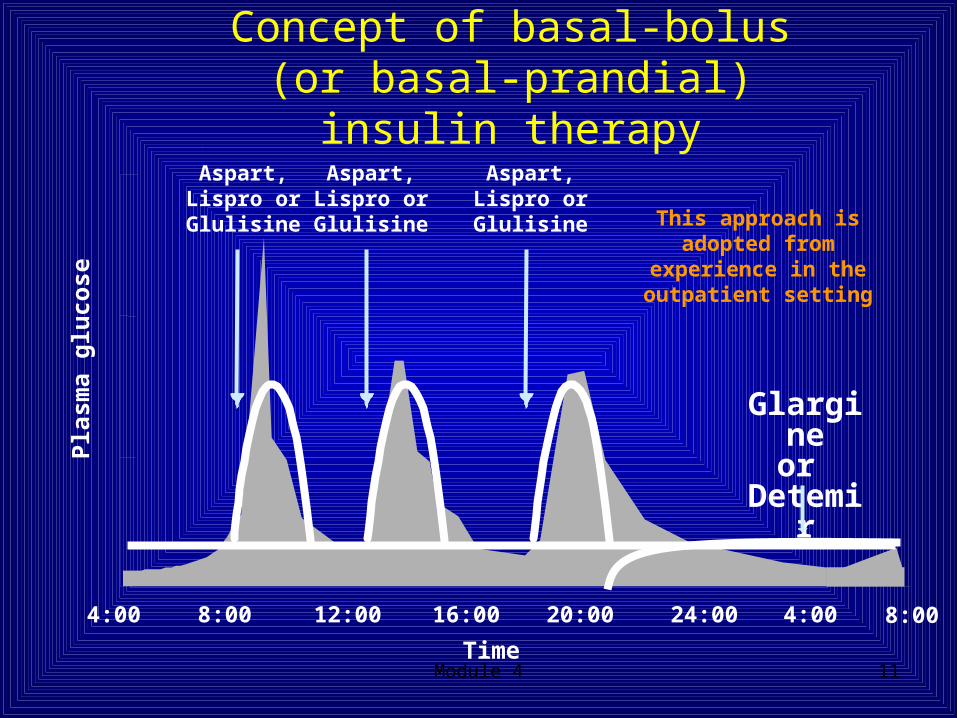
4:00 16:00 20:00 24:00 4:00 8:0012:008:00
Time
Glargineor
Detemir
Aspart, Lispro or Glulisine
Pla
sma
glu
cose
Aspart, Lispro or Glulisine
Aspart, Lispro or Glulisine This approach is adopted
from experience in the outpatient setting
Concept of basal-bolus (or basal-prandial) insulin therapy
Module 4 12
Corrective vs. Sliding ScaleWhat’s the difference?
• Similarities– Treat hyperglycemia before or between
meals or when intermittently eating– Dose finding strategy
• Contrasts– Corrective dose insulin is based on estimate
of patient’s insulin sensitivity– Sliding scale
• Typically written then not modified• Treats glucose “after the fact”—not preventive• Can result in rapid changes in glucose
Module 4 13
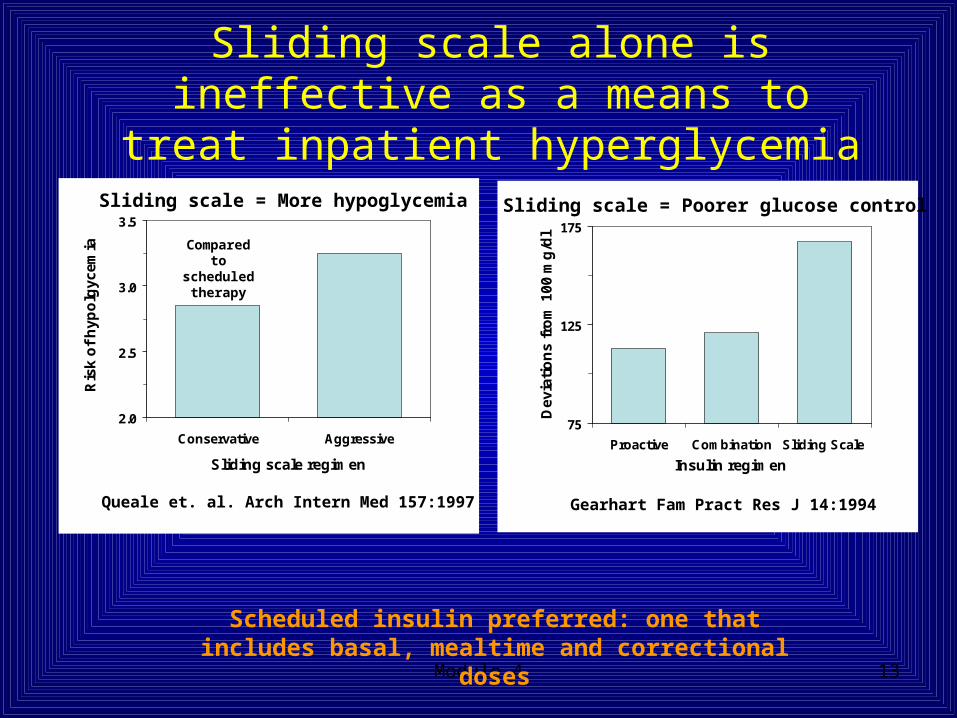
Sliding scale alone is ineffective as a means to treat inpatient hyperglycemia
Scheduled insulin preferred: one that includes basal, mealtime and correctional doses
75
125
175
Proactive Combination Sliding Scale
Insulin regimen
Dev
iati
on
s fr
om
100
mg
/dl
Gearhart Fam Pract Res J 14:1994
2.0
2.5
3.0
3.5
Conservative Aggressive
Sliding scale regimen
Ris
k o
f h
ypo
lgyc
emia
Queale et. al. Arch Intern Med 157:1997
Compared to scheduled
therapy
Sliding scale = More hypoglycemia Sliding scale = Poorer glucose control
Module 4 14
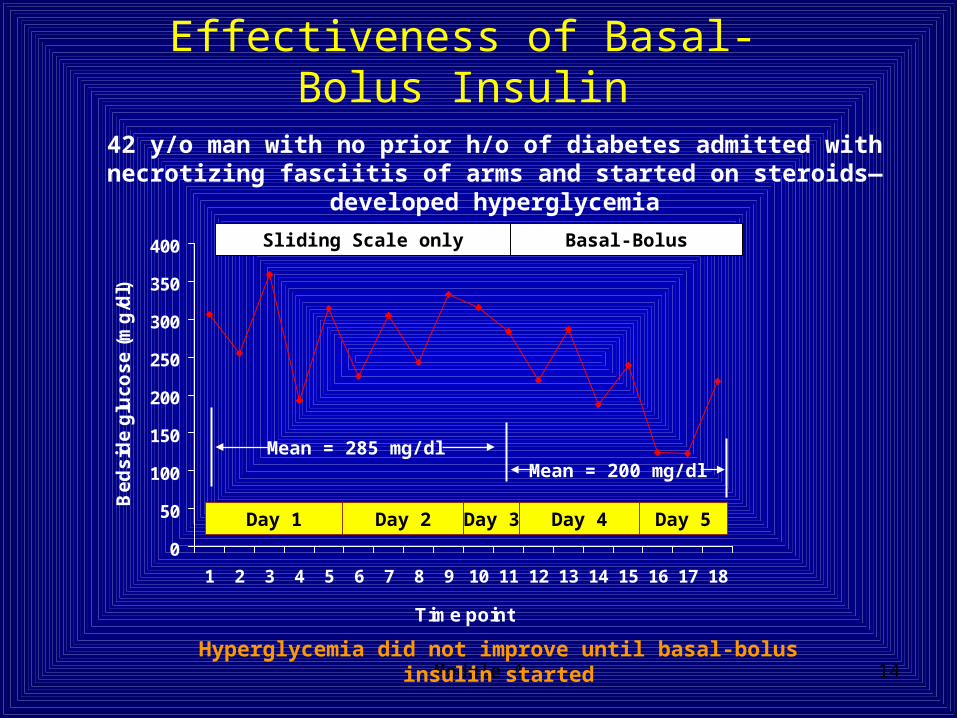
Effectiveness of Basal-Bolus Insulin
0
50
100
150
200
250
300
350
400
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Time point
Be
ds
ide
glu
co
se
(m
g/d
l)
Day 1 Day 2 Day 3
42 y/o man with no prior h/o of diabetes admitted with necrotizing fasciitis of arms and started on steroids—developed hyperglycemia
Day 4 Day 5
Mean = 285 mg/dlMean = 200 mg/dl
Sliding Scale only Basal-Bolus
Hyperglycemia did not improve until basal-bolus insulin started
Module 4 15
0
50
100
150
200
250
300
350
400
450
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Time point
Be
ds
ide
glu
co
se
(m
g/d
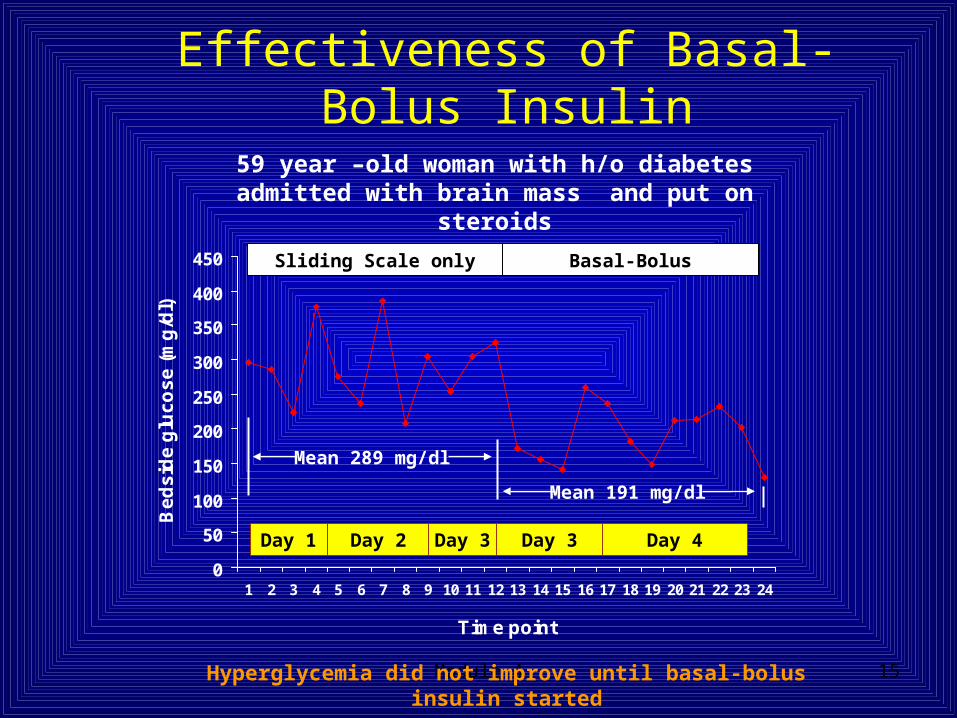
l)59 year –old woman with h/o diabetes admitted
with brain mass and put on steroids
Mean 289 mg/dl
Mean 191 mg/dl
Sliding Scale only Basal-Bolus
Effectiveness of Basal-Bolus Insulin
Hyperglycemia did not improve until basal-bolus insulin started
Day 1 Day 2 Day 3 Day 4Day 3
Module 4 16
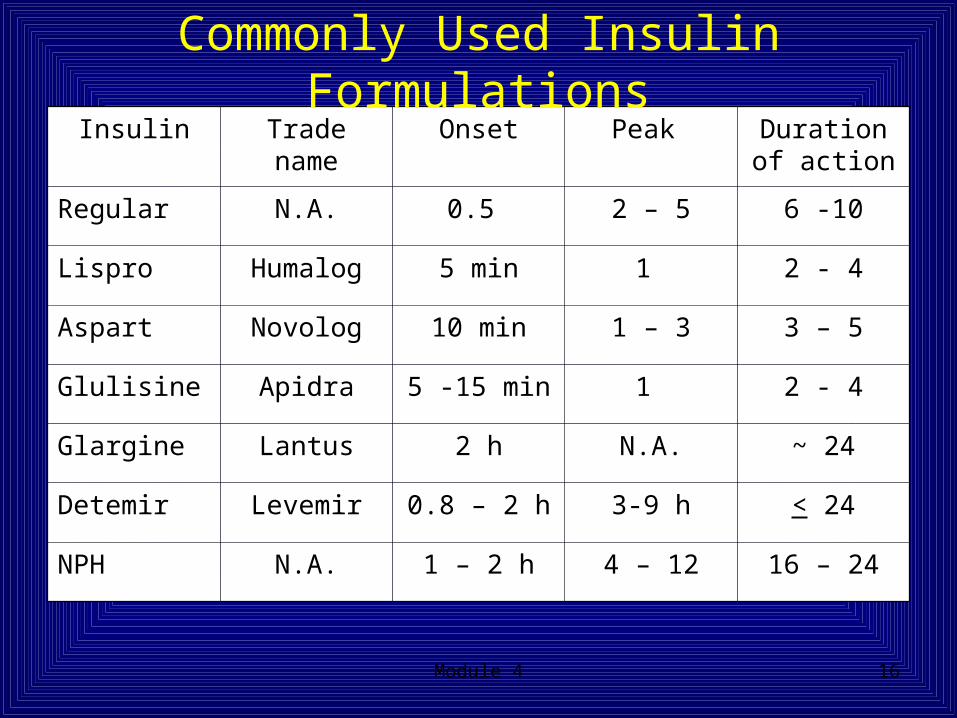
Insulin Trade name Onset Peak Duration of action
Regular N.A. 0.5 2 – 5 6 -10
Lispro Humalog 5 min 1 2 - 4
Aspart Novolog 10 min 1 – 3 3 – 5
Glulisine Apidra 5 -15 min 1 2 - 4
Glargine Lantus 2 h N.A. ~ 24
Detemir Levemir 0.8 – 2 h 3-9 h < 24
NPH N.A. 1 – 2 h 4 – 12 16 – 24
Commonly Used Insulin Formulations
Module 4 17
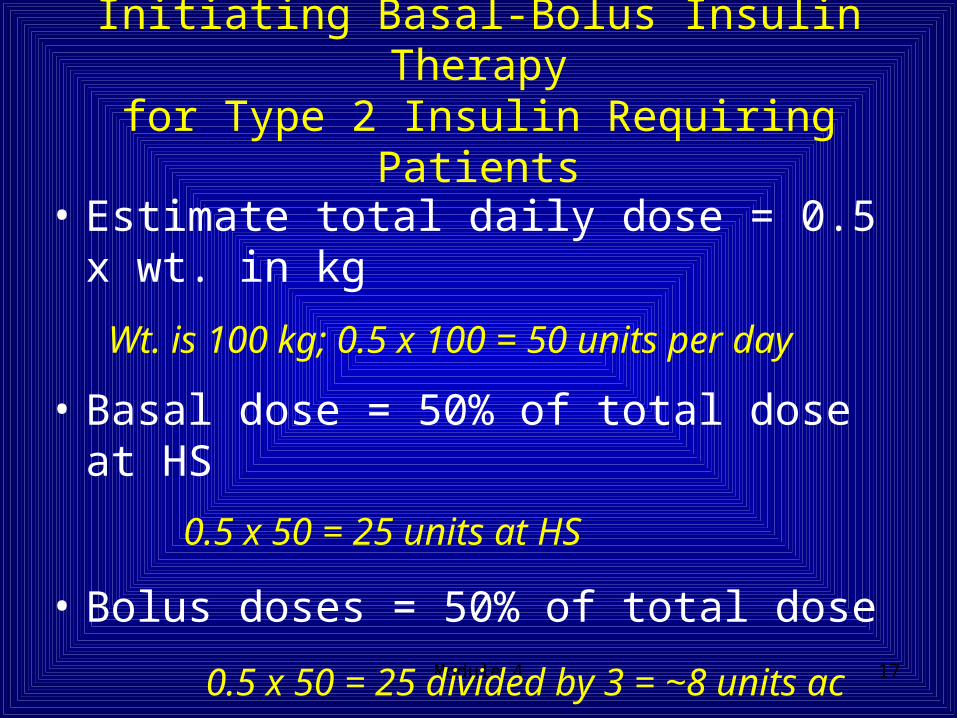
• Estimate total daily dose = 0.5 x wt. in kg
Wt. is 100 kg; 0.5 x 100 = 50 units per day
• Basal dose = 50% of total dose at HS
0.5 x 50 = 25 units at HS
• Bolus doses = 50% of total dose
0.5 x 50 = 25 divided by 3 = ~8 units ac
• Add a correctional insulin program
Initiating Basal-Bolus Insulin Therapyfor Type 2 Insulin Requiring Patients
Module 4 18
Initiating Basal-Bolus Insulin therapy
• The previous slide shows just one way to get started• Different people may calculate doses or distribute
prandial insulin differently• Conservative total daily dose estimate for Type 1
patients could be 0.3 x wt. in kg• Ultra conservative total daily dose estimate for Type 1
renal impaired or emaciated patients could be 0.2 x wt. in kg
Remember: You won’t go wrong as long as you reevaluate the effect of treatment every day and
make necessary changes

Module 4 19
Step One: Calculate the Correction Factor (CF)• The correction factor is the estimated drop in glucose
when 1 unit of rapid-acting insulin is given• Use 1700 Rule to estimate the CF
• CF = 1700/total daily dose (TDD or the total number of units of all insulin given in 24h)
Ex: Scheduled insulin: Glargine 26 units + Novolog 8 units prior to each
meal ≈ 50 units TDD
CF = 1700/50
CF = 30 meaning that 1 unit will lower the BG ~ 30 mg/dL
How do you calculate the correction bolus?
Module 4 20
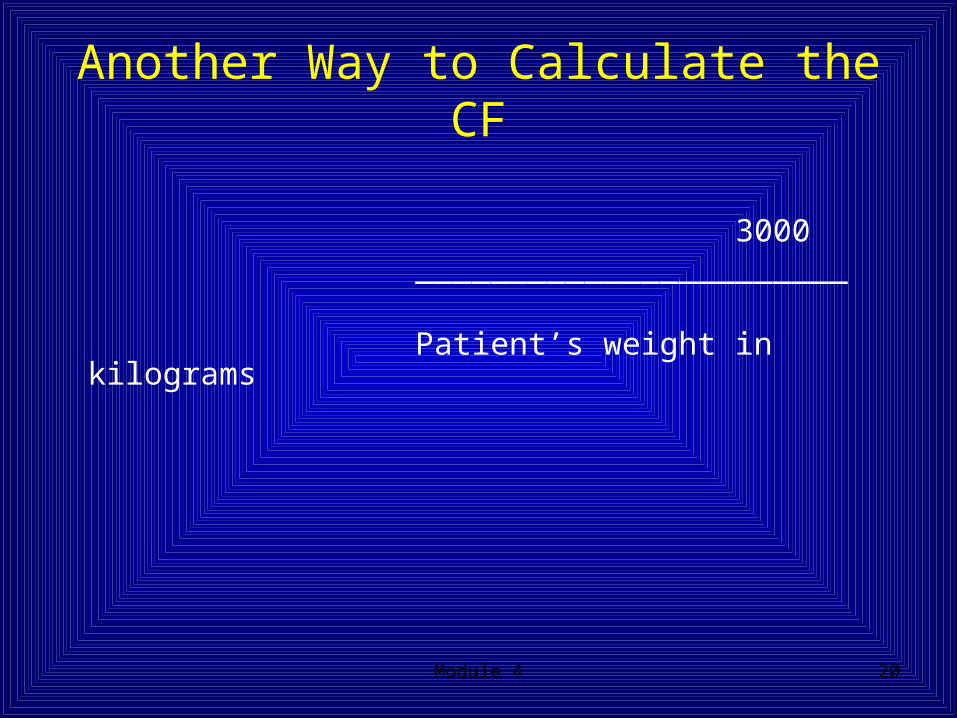
Another Way to Calculate the CF
3000 _______________________ Patient’s weight in kilograms
Module 4 21
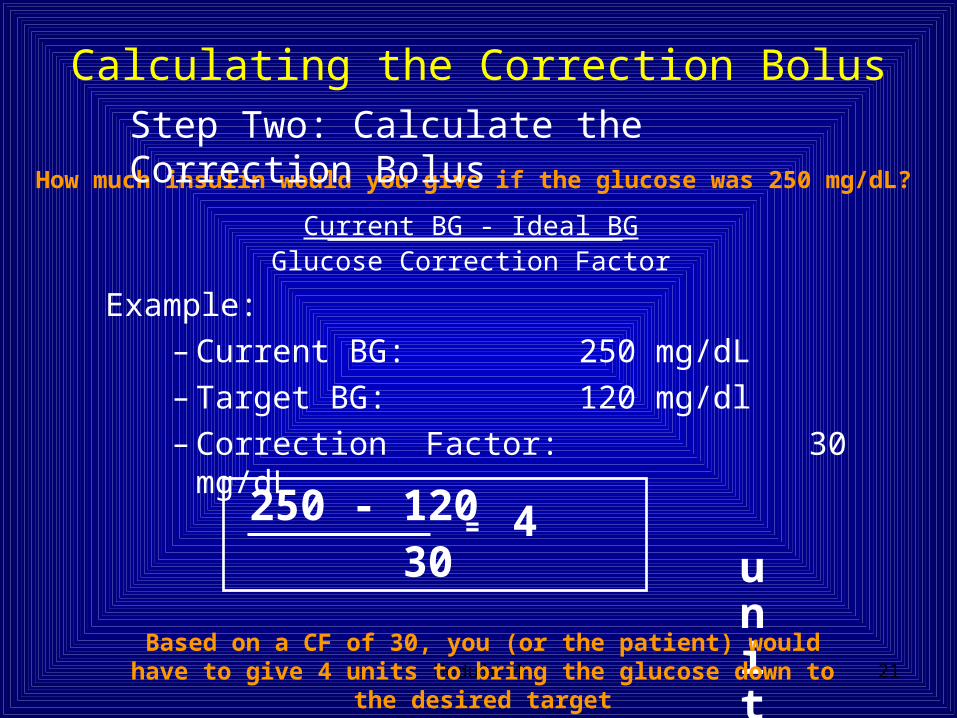
Example:– Current BG: 250 mg/dL– Target BG: 120 mg/dl– Correction Factor: 30 mg/dL
Current BG - Ideal BGGlucose Correction Factor
250 - 120 30
= 4 units
How much insulin would you give if the glucose was 250 mg/dL?
Step Two: Calculate the Correction Bolus
Based on a CF of 30, you (or the patient) would have to give 4 units to bring the glucose down to the desired target
Calculating the Correction Bolus

Module 4 22
Using the Correction Bolus
For example:
You have a 23 year old woman with Type 1 diabetes. She takes 30 units of Lantus at bedtime and 5 units of Apidra with each meal. Her CF is 30 and her target glucose is 120.
Her pre-lunch glucose is 250 mg/dL. In order to correct to 120, she will need to take 5 units to cover the meal plus an additional 4 units to correct for the pre-meal hyperglycemia.
Module 4 23
How does the CF concept work in the hospital?
• The concept of the CF works well if a patients are knowledgeable and can do their own care—typical outpatient scenario
• In the hospital—patients are sick and often cannot participate in their own diabetes management
• In the hospital, we use correctional insulin to try to achieve a target range, rather than a target value.
Module 4 24
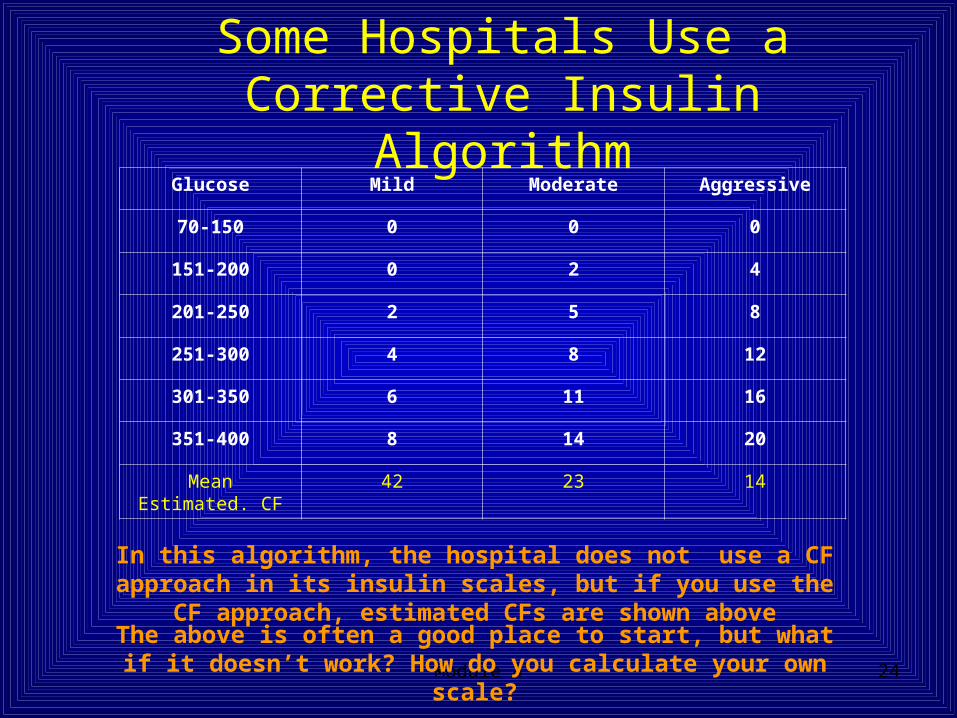
Some Hospitals Use a Corrective Insulin Algorithm
Glucose Mild Moderate Aggressive
70-150 0 0 0
151-200 0 2 4
201-250 2 5 8
251-300 4 8 12
301-350 6 11 16
351-400 8 14 20
Mean Estimated. CF
42 23 14
In this algorithm, the hospital does not use a CF approach in its insulin scales, but if you use the CF approach, estimated
CFs are shown aboveThe above is often a good place to start, but what if it doesn’t
work? How do you calculate your own scale?
Module 4 25
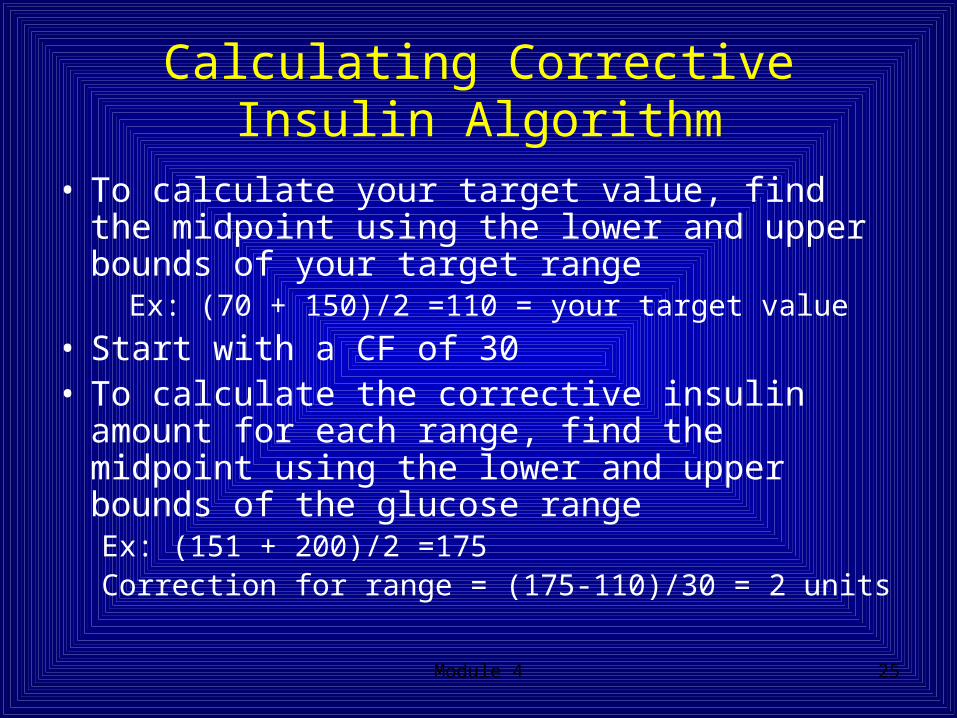
Calculating Corrective Insulin Algorithm
• To calculate your target value, find the midpoint using the lower and upper bounds of your target range
Ex: (70 + 150)/2 =110 = your target value
• Start with a CF of 30• To calculate the corrective insulin amount for
each range, find the midpoint using the lower and upper bounds of the glucose rangeEx: (151 + 200)/2 =175 Correction for range = (175-110)/30 = 2 units
Module 4 26
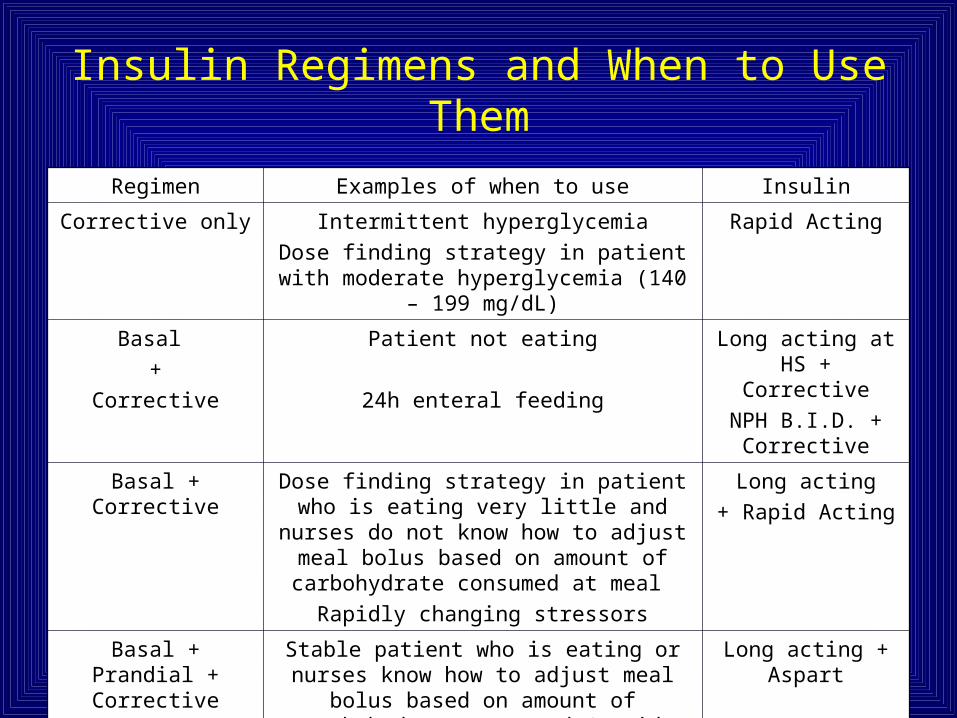
Insulin Regimens and When to Use Them
Regimen Examples of when to use Insulin
Corrective only Intermittent hyperglycemia
Dose finding strategy in patient with moderate hyperglycemia (140 – 199 mg/dL)
Rapid Acting
Basal
+
Corrective
Patient not eating
24h enteral feeding
Long acting at HS + Corrective
NPH B.I.D. + Corrective
Basal + Corrective Dose finding strategy in patient who is eating very little and nurses do not know
how to adjust meal bolus based on amount of carbohydrate consumed at meal
Rapidly changing stressors
Long acting
+ Rapid Acting
Basal + Prandial + Corrective
Stable patient who is eating or nurses know how to adjust meal bolus based on amount
of carbohydrate consumed (rapid acting insulin can be administered immediately
after the meal instead of before)
Long acting + Aspart
Module 4 27
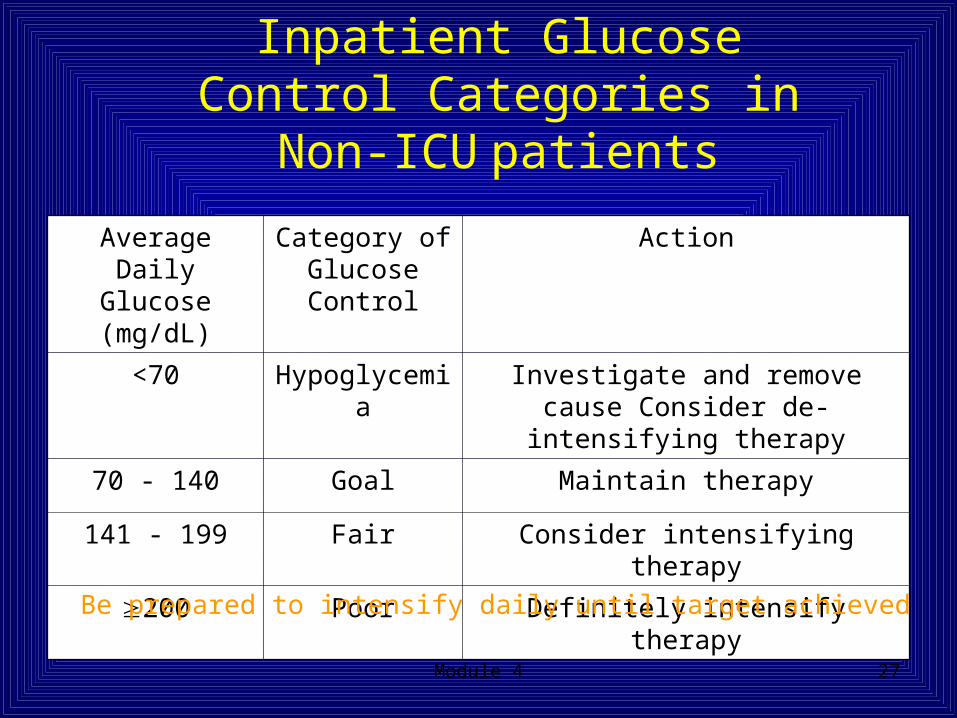
Inpatient Glucose Control Categories in Non-ICU patients
Average Daily Glucose (mg/dL)
Category of Glucose Control
Action
<70 Hypoglycemia Investigate and remove cause Consider de-intensifying therapy
70 - 140 Goal Maintain therapy
141 - 199 Fair Consider intensifying therapy
200 Poor Definitely intensify therapy
Be prepared to intensify daily until target achieved
Module 4 28
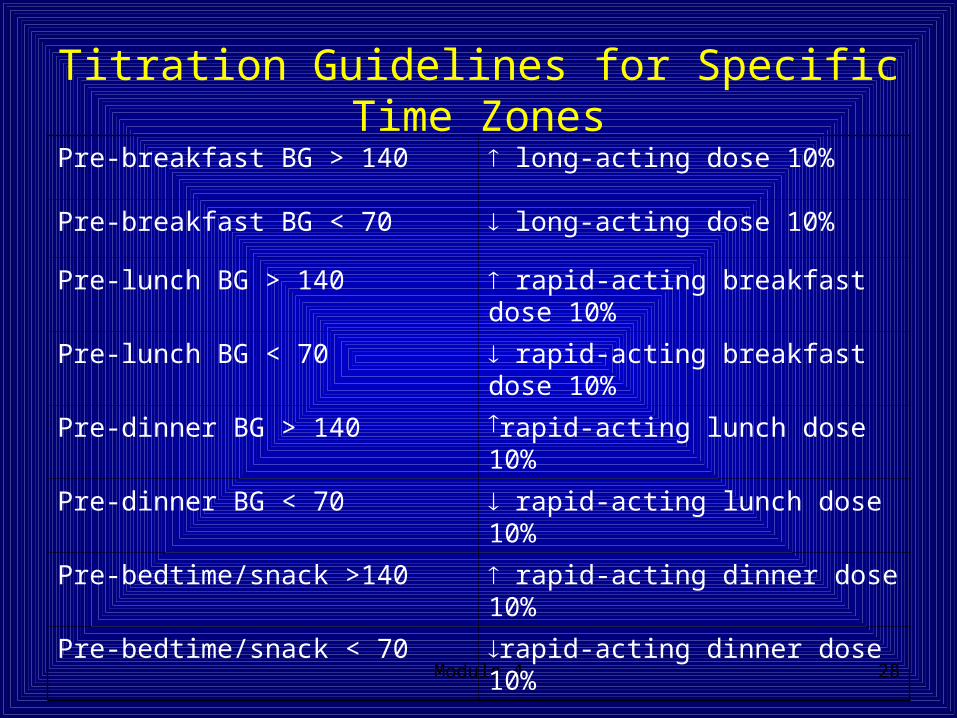
Titration Guidelines for Specific Time Zones
Pre-breakfast BG > 140 long-acting dose 10%
Pre-breakfast BG < 70 long-acting dose 10%
Pre-lunch BG > 140 rapid-acting breakfast dose 10%
Pre-lunch BG < 70 rapid-acting breakfast dose 10%
Pre-dinner BG > 140 rapid-acting lunch dose 10%
Pre-dinner BG < 70 rapid-acting lunch dose 10%
Pre-bedtime/snack >140 rapid-acting dinner dose 10%
Pre-bedtime/snack < 70 rapid-acting dinner dose 10%
Module 4 29
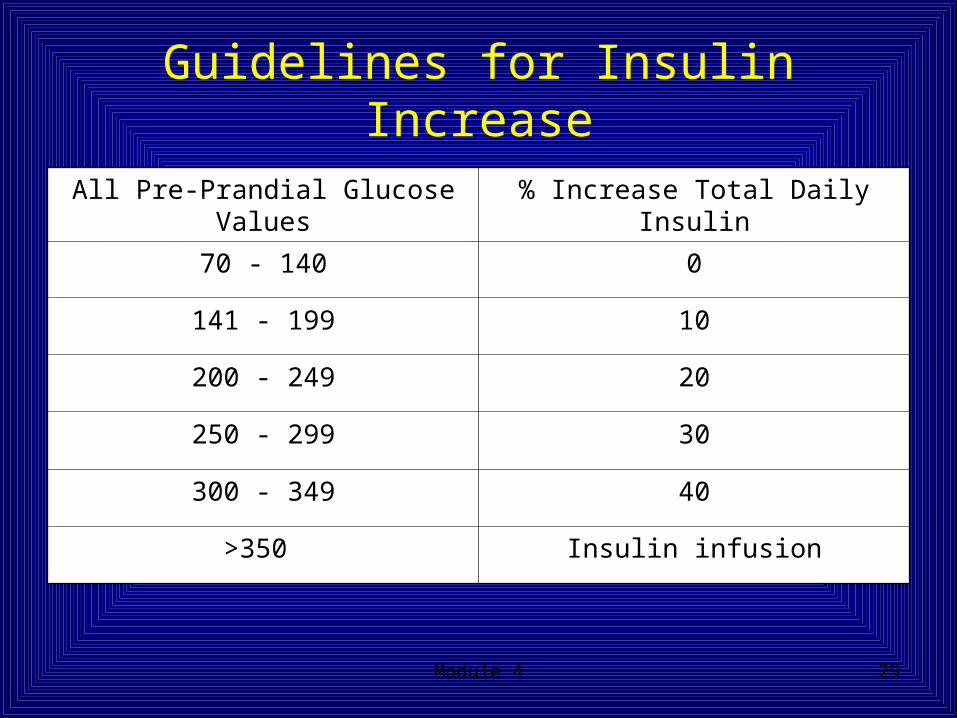
Guidelines for Insulin Increase
All Pre-Prandial Glucose Values % Increase Total Daily Insulin
70 - 140 0
141 - 199 10
200 - 249 20
250 - 299 30
300 - 349 40
>350 Insulin infusion
Module 4 30
IV Insulin Infusion Data
• IV insulin infusion data can be used for dose finding. This will be discussed in another module.
Module 4 31
Titration Precautions and ConsiderationsFractions of Units
• In general, it is not recommended to round up when fractions of units are being considered.
• For example rounding 0.5 to 1.0 may drop an insulin resistant patient’s BG 10 mg/dL while a patient that is very sensitive to insulin might experience a 40 mg/dL drop in BG from the same 0.5 unit dose.
Module 4 32
Additional Considerationsin an Imperfect World
Patient and Staff ComplianceAdditional considerations before titrating include assessing
the patient and staff for compliance with diet, testing and medication administration.
The dose you prescribed may have been correct but:• The patient may have consumed more carbs than you
prescribed (Is the diet order correct? Are family members bringing food to the patient? Is the patient consuming snacks between meals?) An informed patient is part of the healthcare team.
• The BG may have been checked after the meal instead of before
• The insulin may have been given late, early, or not at all.
Module 4 33
Communicate, Communicate, Communicate!
Team work is required to control hyperglycemia in the hospital. Communicating with patients and staff may identify and overcome the barriers to control.
Not only does the physician need to order the correct insulin but also
• dietary needs to provide the proper carb count per meal,• the patient needs to avoid carb intake between meals, • the BG needs to be checked pre-prandial, • the nurse needs to administer the correct dose at the
right time. The nurse needs to notify the physician when a dose has
been missed in order to avoid unsafe titration increases.
Module 4 34
• Don’t ignore hyperglycemia
• The higher the glucose levels, the more frequent the monitoring
• Initiate or change treatment when glucose is high
• All hyperglycemia responds to insulin unless the patient is coding
Summary General Rules for Hospital
Management of Hyperglycemia