Embed Size (px)
Citation preview

Modulation of Erythrocyte Membrane Mechanical Stability by2,3-Diphosphoglycerate in the Neonatal Poikilocytosis/Elliptocytosis SyndromeWilliam C. Mentzer, Jr.,* Terri A. Iarocci,* Narla Mohandas,* Peter A. Lane,* Byron Smith,* Jack Lazerson,t and Taru Hays
*Departments of Pediatrics and Laboratory Medicine, University of California, San Francisco, California 94102;$The Department of Pediatrics, University of California, Davis, California 95616; §Denver Children's Hospitaland the Department of Pediatrics, University of Colorado School of Medicine, Denver, Colorado 80220
Abstract
To explain the transient anemia and poikilocytosis seen duringinfancy in hereditary elliptocytosis (HE), we resealed erythrocyte(RBC) ghosts from affected children or their elliptocytic parentswith 2,-diphosphoglycerate (DPG) (0-8 mM), a compound thatdissociates membrane skeletons, then measured ghost mechan-ical stability in the ektacytometer. Without added 2,3-DPG,ghost mechanical stability was subnormal in infantile poikilo-cytosis (IP) and HEbut was even more abnormal in hereditarypyropoikilocytosis (HPP). Addition of 2,3-DPG (2.55 mM) toIP or HEghosts, decreased their stability to that of HPPghosts(without 2,3-DPG). Nonphysiological 2,3-DPG levels (6-8 mM)were required to elicit a similar effect in normal ghosts. The datasuggest that free 2,3-DPG, present in neonatal RBCas a con-sequence of diminished binding to HbF, may render HEsuscep-tible to in vivo fragmentation. The developmental switch fromfetal to adult hemoglobin, by diminishing available free 2,3-DPG,may explain the abatement of poikilocytosis and hemolytic ane-mia that accompanies maturation.
Introduction
Transient hemolytic anemia and bizarre erythrocyte morphol-ogy, resembling that seen in hereditary pyropoikilocytosis, mayoccur in young infants from kindreds in which one parent haselliptocytosis (1-5). Affected infants, who have usually beenBlack, often require transfusion in early infancy for anemia orhyperbilirubinemia. At - 6 mo of age, hemolytic anemia dis-appears or diminishes in severity and, thereafter, erythrocytemorphology becomes more purely elliptocytic, like that of theaffected parent.
The cause of these transient hematologic abnormalities isunknown. One proposed explanation is that the skeletal abnor-mality responsible for elliptocytosis is itself different in fetal redcells than in adult cells. Although there are definite differencesthat distinguish the membrane of the fetal red cell from that ofadult erythrocytes (6), most available evidence indicates that themembrane skeleton and its component proteins are identical in
Address reprint requests to Dr. Mentzer, Room2108, Building 20, SanFrancisco General Hospital, 1001 Potrero Avenue, San Francisco, CA94110.
Presented in part to the American Society of Hematology, Miami,FL, December 1984.
Receivedfor publication 4 March 1986 and in revisedform 10 No-vember 1986.
fetal and adult red cells (7-9). Wetherefore considered it morelikely that developmental changes in nonskeletal red cell com-ponents capable of interacting with the underlying skeletal pro-tein abnormality were responsible for transient neonatal poi-kilocytosis and hemolysis. In this report, we provide evidencethat 2,3-diphosphoglycerate (DPG)' can dissociate the flawedmembrane skeleton of elliptocytic ghosts, causing such prepa-rations to reach the extreme levels of mechanical fragility char-acteristic of hereditary pyropoikilocyte ghosts.
Wepropose that the uniquely high levels of free 2,3-DPGin fetal red cells, a consequence of the extremely limited abilityof hemoglobin F to bind 2,3-DPG, render cells with an inheritedmembrane skeletal abnormality particularly susceptible to invivo fragmentation and premature destruction.
Methods
Glycerate-2,3-diphosphate (pentacyclohexylammonium salt) was pur-chased from Boehringer Mannheim, Indianapolis, IN; electrophoresisreagents from Bio-Rad Laboratories, Richmond, CA; Seakem MEagarosefrom FMCCorporation, Rockland, ME; DFP from Sigma Chemi-cal Co., St. Louis, MO; and Trypsin-N-tosyl-L-phenylalanine chloro-methyl ketone (TPCK) from Worthington/Cooper Biomedical, Inc.,Malvern, PA.
The study protocol was approved by the Committee on HumanRe-search of the University of California, San Francisco.
Routine hematology. Routine blood counts were measured by elec-tronic particle counter. The percentage of hemoglobin F was determinedby alkali denaturation or by densitometric scanning of cellulose acetatehemoglobin electrophoresis strips. The percentage of elliptocytes wasdetermined by counting 500 cells on well separated areas of a peripheralblood smear.
Red cell thermalfragility. Morphologic changes such as membranedistortions or budding were studied by Nomarski interference phase mi-croscopy after heating red cells suspended in BSKGbuffer (132 mMNaCl, 5 mMKCI, 10 mMNaHPO4, 11 mMglucose, 290 mosM, pH7.4) to various temperatures between 370 and 50°C for 10 min (10).Fragmentation of heated erythrocytes was estimated by measuring theaccumulation of small particles using a Coulter Counter (model ZBI,Coulter Electronics, Hialeah, FL) equipped with a channelizer 11 (10).
Deformability measurements. The deformability of intact red cellswas measured in the ektacytometer, a couette viscometer, which appliesa well-defined laminar shear stress to the cell, while simultaneously mon-itoring the extent of cell deformation by laser defractometry (11). Toobtain information about initial cell surface area, surface area to volumeratio, and cell water content, the deformability of red cells was contin-
1. Abbreviations used in this paper: DFP, diisopropyl fluorophosphate;DI, deformability index; DPG, diphosphoglycerate; HE, hereditary el-liptocytosis; HPP, hereditary pyropoikilocytosis; IP, infantile poikilo-cytosis; MCHC, mean corpuscular hemoglobin concentration; MCV,mean corpuscular volume; PAGE, polyacrylamide gel electrophoresis;PMSF, phenylmethylsulfonyl fluoride; TPCK, N-tosyl-L-phenylalaninechloromethyl ketone; T60, index of red cell or ghost mechanical stability.
Neonatal Poikilocytosis 943
J. Clin. Invest.© The American Society for Clinical Investigation, Inc.0021-9738/87/03/0943/07 $ 1.00Volume 79, March 1987, 943-949

uously recorded as the suspending medium osmolarity was linearly in-creased from 50 to 500 mosM/kg (1 1).
Membrane stability assay. Wemeasured membrane resistance toshear induced fragmentation by subjecting resealed ghosts to a constantshear stress of 575 dynes per square centimeter in the ektacytometer(12). Toward the end of 1984, the original analogue processing ektacy-tometer was replaced by a second generation digital processing machine.Ghost mechanical stability assays were run at a higher shear stress (650or 785 dyne/cm2) on this instrument. The major difference between thetwo instruments was the geometric location of the areas of the diffractionpattern selected for scattered light intensity measurements to generatethe deformability index (DI). In the earlier system, the DI values generatedwere higher than in the later system. Because of these design changes,the relative DI changes during membrane stability measurements weredifferent in the two systems. Ghosts were suspended in a dextran solutionof 97 centipoise (cp) viscosity and the ektacytometer chamber rotatedat a speed of 1 10-150 rpm to generate the desired shear stress. A decreasein the DI generated by the ektacytometer has been shown to reflect frag-mentation of the intact membranes into small, undeformable sphericalparticles. As an index of the rate of this fragmentation process we selectedthe time required for the DI to fall to 60% of its highest value (T60).The 60% level was chosen because the rate of fall in DI that accompaniedfragmentation exhibited greater variability at lower levels. To minimizesmall, day-to-day variation in the absolute value of the T60 due to fluc-tuations in such uncontrolled variables as room temperature, we alwaysmade comparison to simultaneously studied normal erythrocyte ghosts.The mechanical stability of intact red cells was also measured in theektacytometer, using a higher shear stress (1,300 dyne/cm2) (12).
Red cell membrane protein analyses. Red cell membrane ghosts wereprepared essentially as described by Dodge et al. (13). Phenylmethyl-sulfonyl fluoride (PMSF) 0.2 mM,was added to all preparative solutionsto minimize proteolysis. Red cell membrane proteins were analyzed byone-dimensional sodium dodecyl sulfate-polyacrylamide gel electropho-resis (SDS-PAGE) as described by Laemmli (14) using a 4.5% acrylamidestacking gel and a 4-15% nonlinear acrylamide gradient separating gel.A crude spectrin extract was obtained from fresh ghosts by dialysis for20-24 h at 0-40C in low ionic strength buffer containing 0.1 mMsodiumphosphate, 0.1 mMethylenediaminetetracetic acid, 0.1 mMfB-mercap-toethanol and 0.2 mMPMSFat pH 8 (10). The percentage of spectrindimers (expressed as dimers/dimers plus tetramers) present in this extractwas determined by nondenaturing polyacrylamide gel electrophoresis asdescribed by Liu and Palek (15). The crude spectrin extracts were alsosubjected to limited tryptic digestion at 04'C, essentially as describedby Lawler and his co-workers (8). For these studies, the crude spectrinextracts were dialyzed for 16 h at 00C against 200 vol of 20 mMTrisbuffer, pH 8, in order to remove PMSF. The protein concentration ofthe dialysed spectrin extract was determined using a Bio-Rad assay.Trypsin-TPCK was then added to the extract at ratios of 1:100 or 1:200.(wt/wt) and limited digestion allowed to proceed for 16-20 h at 0°C(16). The reaction was terminated by the addition of DFP to a finalconcentration of 1 mM(16). Analysis of the spectrin fragments producedby digestion was carried out using a two-dimensional isoelectric focusing/SDS-PAGEsystem (17).
Preparation of resealed ghosts containing 2,3-DPGFresh red cells were washed three times with Tris-saline buffer (5 mMTris, 140 mMNaCl, pH 7.4). 40 ml of cold lysing buffer (5 mMTris, 7mMNaCl, pH 7.4) was then added to 2 ml of packed red cells. Aftergentle shaking, the suspension was centrifuged at 20,000 g for 5 min andthe supernatant removed by aspiration. 2 ml of the ghosts thus obtainedwere added to 20 ml of cold resealing buffer (5 mMTris, pH 7.4, plus140 mMNaCl) to which had been added various concentrations (0-15mM)of 2,3-DPG (cyclohexylammonium salt). After incubation at 37°Cfor 1 h, the resealed ghosts were centrifuged at 20,000 g for 5 min. Packedghosts (100 $l) were added to 35% dextran in 180 mosMphosphate-buffered saline (pH 7.4, final osmolarity, 290 mosM) and the ghost me-chanical stability determined immediately in the ektacytometer as de-scribed earlier. Resealed ghosts could be held on ice for at least 2 h
without any change in mechanical stability. All measurements werecompleted in < 1 h from completion of ghost preparation. For deter-mination of 2,3-DGP levels, an aliquot of the packed ghosts were washedand suspended in saline at a hematocrit of 30-40%, then extracted withperchloric acid. To prepare the extracts, an aliquot (0.5 ml) of ghostswas added to 1 ml of ice-cold 1%perchloric acid. The clear supernatantwas neutralized with 5 Mpotassium carbonate and stored for subsequentassay. 2,3-DPG was assayed spectrophotometrically by the method ofKeitt (18).
Case historiesFamily B. A.B., a Black infant born at term (birthweight, 3,525 g), re-quired a two volume exchange transfusion at 48 h of life for hyperbili-rubinemia. On the first day of life the hemoglobin was 13.4 g/dl, themean corpuscular volume (MCV) 79 fl, and the reticulocyte count 5%.Bizarre poikilocytes and elliptocytes were noted on the peripheral bloodsmear. At 19 wk of age the hemoglobin reached a nadir of 7.4 g/dl. Thereticulocyte count was 12.8% and the spleen tip was palpable. At 51 wkof age, the hemoglobin was normal (10.9 g/dl) but the reticulocyte countremained elevated (3.8%), and the red cell indices were abnormal (MCV65 fl, [mean corpuscular hemoglobin count] MCHC36.2%). At the ageof 2 yr, following 2 d of fever (1040) and diarrhea, he required transfusionsfor an episode of severe anemia (Hb = 5.9 g/dl). Red cell morphologycontinued to resemble that of hereditary pyropoikilocytosis and the spleenwas now palpable 2 cm below the left costal margin. Peripheral bloodcounts and reticulocyte counts were normal in both parents. Red cellmorphology was normal in the father but numerous elliptocytes wereevident on the mother's peripheral blood smear.
Family D. Patient B.D., born at term (birthweight, 3,059 g), requiredhospitalization at day 4 of life for neonatal hyperbilirubinemia (peakbilirubin 16.7 mg/dl). On admission, the hemoglobin was 11.7 g/dl, thereticulocyte count 2.8%, and the red cell morphology resembled that ofhereditary pyropoikilocytosis, with occasional pyknocytes also noted. By5 wk of age, the hemoglobin had fallen to 6.5 g/dl and the patient wastransfused. Thereafter, the hemoglobin remained above 9 g/dl and thereticulocyte count and red cell indices were normal. Elliptocytes becameincreasingly prevalent on the blood smear, but even at 22 mo of agepoikilocytic, microcytic fragments were still evident. Elliptocytes wereabundant in the peripheral blood of the father, who was Black, but hisperipheral blood counts were normal. Blood counts and red cell mor-phology were entirely normal in the mother, who was Caucasian. PatientP.D., the younger sibling of B.D., was treated with phototherapy forneonatal hyperbilirubinemia. A poikilocytic, hemolytic anemia (Hb= 13.3 g/dl on day 5 of life), exactly like that noted in B.D., was presentand gradually worsened, reaching a nadir (Hb = 8 g/dl) at 6 wk of age.Transfusions were not required and by 10 mo of age the hemoglobin(10.9 g/dl) and reticulocyte count (0.2%) were normal.
Family W. S.W., a full-term Caucasian male, required phototherapyfor neonatal hyperbilirubinemia. At birth, the hematocrit was 39% andthe erythrocyte morphology resembled that of hereditary pyropoikilo-cytosis. By 6 wk of age, the hemoglobin had fallen to 7.9 g/dl and thereticulocyte count was 13.7%. By 25 wk of age the hemoglobin had risento 12 g/dl but reticulocytosis persisted (5%). The red cell indices werenormal and the erythrocyte morphology was now that of elliptocytosisrather than pyropoikilocytosis. The patient's mother, who was reportedlyanemic during pregnancy but not at other times, had elliptocytosis buta normal reticulocyte count. The only sibling of S.W. required treatmentfor hyperbilirubinemia at birth and currently has elliptocytosis and re-ticulocytosis (1.8%) but not anemia (hemoglobin 11.8 g/dl). The fatherwas hematologically normal.
Family C. J.C., a full-term Caucasian female, (birthweight, 3,380 g),required phototherapy for neonatal hyperbilirubinemia. On the eighthday of life, the hemoglobin was 14.1 g/dl. Mild to moderate abnormalitiesof erythrocyte morphology were noted (anisocytosis, poikilocytosis, el-liptocytosis). By 9 wk of age the hemoglobin had dropped to 7.5 g/dl.The reticulocyte count was 4.1% and the erythrocyte morphology resem-bled that of hereditary pyropoikilocytosis, with 12%pyknocytes also notedon the peripheral blood smear. By 30 wk of age, anemia was no longer
944 Mentzer, Iarocci, Mohandas, Lane, Smith, Lazerson, and Hays

present (hemoglobin 10.8 g/dl). The reticulocyte count and red cell indiceswere normal and the blood cell morphology was now consistent withhereditary elliptocytosis. The mother was not anemic but had ellipto-cytosis. The father and one sibling were hematologically normal.
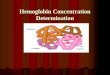
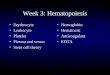
Hematologic studiesThe duration and extent of anemia in affected infants from the fourfamilies is shown in detail in Fig. 1. In general, the anemia reached anadir at from 1 to 3 moof age and was no longer present at 6 mo. Testsfor immune hemolysis were negative in each infant. The postnatal declinein the amount of hemoglobin F is also depicted in Fig. 1. In the fourinfants with poikilocytosis, the fall in hemoglobin F appeared to be slightlyaccelerated but still remained within the normal range. Serial red cellsize distribution plots obtained in two infants are shown in Fig. 2. Inpatient B.D., a persistent population of extremely microcytic red cellswas evident even at 22 mo of age. An equivalent population was notseen in the elliptocytic father. Red cell size distribution analyses werenot performed on B.D., during the first few months of life, but werecarried out on P.D., his younger brother, who had an identical poikilocyticanemia (Fig. 2). A sharp decline in the microcytic cell fraction was evidentby 8 wk of age in P.D. In another infant (A.B.), unrelated to the firsttwo, the fraction of cells that were extremely microcytic exceeded thefraction that were normal until 34 mo of age (data not shown). Eventhen, a large fraction of microcytic cells were present, the plot resemblingthat shown for P.D. at birth.
Red cellfragmentation and deformabilityThe temperature at which heated erythrocytes first exhibited morphologicchanges (budding or fragmentation) is reported in Table I. Erythrocytesfrom the three Black infants (A.B., P.D., and B.D.) underwent thermalchanges at temperatures up to 5 degrees below those characteristic ofcontrol erythrocytes. Between 1 and 2 yr of age the temperature requiredto induce morphologic changes rose toward normal in B.D. but showedno improvement in A.B. Erythrocytes from the elliptocytic parent ofB.D. but not A.B. were susceptible to heat induced morphologic changesand fragmentation at temperatures 1-2 degrees lower than normal. Thetwo Caucasian infants (S.W. and J.C.) and their family members were
a
-o
\
b
U-
-oI
80 rT
60 L
20L
hr
i1. 0 a ; t ..f .n1~~~~~~~~~~~~1
I~
5 10 15 20 25 30
AGE (Weeks)
Figure 1. Hemoglobin (a) and hemoglobin F (b) levels during infancyin four infants with neonatal poikilocytosis and transient hemolyticanemia. v S.W., A J.C., o A.B., o B.D., t transfusion. The normalrange (shown by the shaded area), mean, and standard deviation arealso indicated (26, 31).
RELATIVENUMBER
5 DAYSF = 74%
8 WEEKSF = 22%
7 MONTHSF = 4.9%
10 MONTHS
A
Nt(Fa
RELATIVE SIZE
13 MONTHSF = 4.2%
17 MONTHS Figure 2. Red cell sizeF = 3% distribution in neonatal
poikilocytosis and tran-22 MONTHS sient hemolytic anemia
F = 2.4% (family D). (Top 2 pan-
ADULT els) P.D. (Panels 3-7)ther-elliptocytosis) B.D. (Bottom panel) fa-
ther with elliptocytosis(K.D.).
normal (J.C.) or exhibited a one degree decline (S.W.) in the temperatureat which thermal changes occurred.
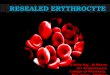
To evaluate whole cell deformability and investigate cell surface tovolume relationships, erythrocytes were studied by the technique of os-motic gradient ektacytometry (Fig. 3). In this procedure the deformabilityof erythrocytes in a continuously changing osmotic environment is mea-sured in the ektacytometer. Erythrocytes from three infants with transientpoikilocytosis exhibited varying reductions in maximal deformability.In these three infants (J.C., S.W., and B.D.), the results were nearlyidentical to those obtained using erythrocytes from their elliptocytic par-ents (data not shown). In a fourth infant (A.B.), whose poikilocytosispersisted beyond age 2 yr, the reduction in deformability was more severethan that noted in his elliptocytic mother but not so severe as that typicalof classic hereditary pyropoikilocytosis. In this family, but not in theothers, the nonelliptocytic parent also exhibited a modest reduction inred cell deformability.
The mechanical stability of erythrocyte ghosts was measured by ek-tacytometry. In the infants with transient poikilocytosis and in theirelliptocytic parents, ghost mechanical stability was reduced to roughlyhalf normal (Table I). No consistent changes in ghost mechanical stabilitywere associated with maturation in those infants in whom sequentialstudies were performed. In three families, the nonelliptocytic parent hadno abnormalities of ghost mechanical stability but in the fourth (familyB) a moderate reduction (to 74% of normal) was noted.
In family D, the mechanical stability of intact red cells was alsoevaluated by ektacytometry. Red cells from P.D. (age 5 d), B.D. (age 22mo) and normal adult or neonatal controls were separated from sub-populations of equivalent buoyant density by Stractan density gradientcentrifugation and a representative layer from the center of each gradient(red cell density = 1.093-1.098) was subjected to ektacytometry. Redcell mechanical stability (T60 expressed as a percentage of the normalcontrol), was subnormal (30% of normal) in B.D. and even more strikinglyabnormal in P.D. (T60 = 20% of normal). Subsequently, when P.D. was10 moold and no longer had poikilocytic hemolytic anemia, these studieswere repeated. Red cell mechanical fragility, which had improved inboth P.D. (51%) and B.D. (42%), now was identical to the value obtainedfor their elliptocytic father (45%).
Red cell membrane proteinsOne-dimensional SDS-PAGEof membrane proteins obtained from in-fants with transient poikilocytosis and their relatives was normal in threefamilies. In the fourth (S.W.), an abnormal alpha spectrin mutant (ap-parent 235,000 mol wt) which migrated between the positions of normal
Neonatal Poikilocytosis 945

Table L Properties of Erythrocytes from Children with Infantile Poikilocytosis and Their Families
RBCmorphology RBCthermal changes Ghost mechanical stabilitySpectrin
Age Appearance* Elliptocytes Morphology5 Fragmentation Analogue' Digital" dimers
wk %
Family BInfant (A.B.)
MotherFather
16325182
2 yr2 "/,2 yr
Family DInfant (P.D.) 1
940
Infant (B.D.) 5173245577397
2'/12 yrFatherMother
Family WInfant (S.W.)
MotherSiblingFather
Family CInfant (J.C.)
MotherFather
HPPHPPHPPHPPHPPHPPHEN
IPIPIP/HEIPIP/HEIP/HEIP/HEIP/HEIP/HEHEHEHEN
7 IP/HE25 HE70 HE
HE5 yr HE
N
818
4'0/12 yr
Normalcontrols
IP/HEHEHEHEN
N
24263639394645<1
292942314751485456634362<1
5671648370
2
9262235
3
<410
<4644454545
4949
4647
474646474748
4849
494848494949
4949
4930
4849495049
5050
4949
494949495050
4950
505049505050
5050
5050
5030
39 354229 28.5
12 27.7
16 -60 36 20.574 39 16.1
6+21+ -23
45 18.957 13.54131 15
192918+24
41 30+, 1692 100
3646
1267 3246 1295 100
5978
5577 61
100 88
10018
10018
14.7
15.54.4
22.815.315.115.7
3.4
9.07.45.25.1
5.72±2.0545
* HPP, hereditary pyropoikilocytosis; HE, hereditary elliptocytosis; IP, infantile poikilocytosis; IP/HE, transitional morphology; N, normal.t Lowest temperature (0C) at which membrane budding observed in > 109% of RBC. I Determined at 575 dyne/cm2 in 1st generation analogueprocessing ektacytometer. II Determined at 653 (+) or 784 dyne/cm2 in Technicon 2nd generation digital processing ektacytometer. Note thatsimultaneous assay of mechanical stability on the same sample yielded different results in the two ektacytometer systems (as an example see resultsfor family B parents).
alpha and beta spectrin, was identified. Details of this unique mutantare presented elsewhere (19). The percentage of spectrin dimers presentin low ionic strength extracts of membrane ghosts, prepared at 0°C, wasconsiderably greater than normal in three infants and in their elliptocyticparents (Table I). No consistent change in the amount of spectrin dimerswas detected during the evolution from poikilocytosis to elliptocytosisin these infants. In the fourth family, the percentage of spectrin dimerswas normal to slightly increased in the affected infant (J.C.) and wasnormal in both parents.
Spectrin extracts were also subjected to limited tryptic digestion andthe tryptic fragments obtained were analyzed by two-dimensional (iso-electric focusing/SDS-PAGE) electrophoresis. In one Black family, theinfant (A.B.) exhibited a striking reduction in the normal 80-kD spectrinalpha chain fragment accompanied by the appearance of 65-, 50-, and21-kD fragments. Digested spectrin from this infant's father, who wasnot elliptocytic, exhibited a less striking reduction in the 80-kD fragment.Two of the abnormal fragments (50 kD, 21 kD) noted in infant A.B.were also found in the father's digest. Digested spectrin from the ellip-
946 Mentzer, larocci, Mohandas, Lane, Smith, Lazerson, and Hays

LU
Z06Z06 ~~~~~~D
0 200 300 400
OSMOLALITY ( mosmol/kg )
tocytic mother of infant A.B. contained less than the normal amount ofthe 80-kD fragment along with a reciprocal increase in a 65-kD fragment.In the second Black family (family D), the spectrin tryptic digestionpattern in the elliptocytic father and in both elliptocytic children (B.D.and P.D.) showed an increase in the amount of a 65-kD fragment anda concomitant reduction in the amount of the normal 80-kD fragment.The mother's pattern was normal. In the two Caucasian infants (S.W.and J.C.) and their parents, the pattern of tryptic fragments was normal.
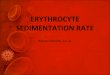
Effect of 2,3-DPG on membrane mechanical stabilityTo evaluate the effect of 2,3-DPG on membrane mechanical stability,ghosts were resealed in the presence of varying amounts of 2,3-DPG.The mechanical stability of 2,3-DPG loaded ghosts was then measuredusing the ektacytometer. As shown in Fig. 4, a reduction in ghost me-chanical stability was first noted in normal ghosts (from either adults ornewborns) at 2,3-DPG concentrations > 3 mmol/liter of ghosts. A half-maximal effect was evident at 5 mmol/liter of ghosts. Sufficient bloodwas obtained to pefform similar experiments in two of the four infantswith poikilocytosis. At the time they were studied, the 2,3-DPG concen-tration in fresh red cells (normal = 4.5±0.6 mmol/liter red blood cells,RBC) was 6.7 mmol/liter RBCin infant A.B. (age 7 mo) and 5.4 mmol/liter RBC in infant B.D. (age 8 mo). Ghost mechanical stability wasconsiderably less than normal, even in the absence of 2,3-DPG. In thepresence of 2,3-DPG, ghost mechanical stability decreased further,reaching the extremely fragile levels charceristic of hereditary pyro-poikilocytosis at 4 mmol/liter of ghosts. Ghosts from the elliptocyticparent of each of the four poikilocytic infants also exhibited diminishedmechanical stability in the absence of 2,3-DPG. The addition of 2,3-DPGfurther diminished their mechanical stability and, as was the casewith the poikilocytic infants, they became as fraile as hereditary pyro-poikilocyte ghosts at 2,3-DPG levels of 3.5-5 mmol/liter of ghosts.
In one family (D), a direct comparison between two individuals withan identical molecular defect in spectrin was possible. In this family, thepoikilocytic infant's ghosts (B.D.) reached the level of mechanical fragilitycharacteristic of hereditary pyropoikilocytosis at a 2,3-DPG level of 2.5mmol/liter ghosts (Fig 4), while ghosts from his elliptocytic father (LD.),studied on two separate occasions, reached the same level at 2,3-DPGlevels of 4.5 mmol/liter ghosts (Fig. 4) or 2.6 mmol/liter ghosts (data notshown).
Discussion
The five infants described in this report each had significantnonimmune hemolytic anemia during the first few months oflife. In three, (J.C., B.D., P.D.), anemia and reticulocytosis dis-
Figure 3. Red cell osmotic gradient ektacytometry inwj~i four infants (J.C., age 9 mo; S.W., age 7 wk; B.D., age
5 wk; A.B., age 16 wk) with neonatal poikilocytosisand transient hemolytic anemia. Results are identified
500 by last name initial. Normal values (shaded area) andrepresentative results in a patient (age 4 yr) with clas-sic HPPare also indicated.
appeared by 6 mo of age, poikilocytes disappeared or becameless prevalent, and elliptocytes became the predominant circu-lating red cell. The residual erythrocyte abnormality now presentin these children is best classified as the mild form of commonhereditary elliptocytosis (20). The fourth infant (S.W.), also nowhas mild common hereditary elliptocytosis but, unlike the firsttwo infants, shows evidence of persistent compensated hemolysisat age 2 yr. The last infant (A.B.), who at age 2 yr and 10 moalso continues to exhibit compensated hemolysis, appears torepresent an example of mild or variant hereditary pyropoikilo-cytosis, since his red cells remain bizarrely poikilocytic and ex-hibit striking thermal fragility that has not improved as he hasmatured. The abnormalities in red cell rheology and in spectrinbiochemistry discovered in both parents suggest that this infantis a compound heterozygote for two different membrane ab-normalities, an inheritance pattern reported previously in he-reditary pyropoikilocytosis (10). In contrast, in the other threefamilies, one parent had elliptocytosis accompanied by a reduc-tion in ghost mechanical fragility while the other parent wasnormal, suggesting that the cytoskeletal abnormalities presentin the infant were inherited solely from the elliptocytic parent.
Our attempts to define the erythrocyte membrane proteinabnormalities present in these infants highlighted the differencesbetween them. A spectrin alpha subunit defect (Spa"65) wasdetected in family D, and in family Wa previously undescribedelectrophoretic variant of the spectrin alpha subunit was found.In family B, two different spectrin mutations (Spa"/65, Spa1/50)were found in the parents. Both mutations appeared to havebeen inherited by the infant (A.B.), who had hereditary pyro-poikilocytosis. In family C, no evidence of a spectrin mutationwas discovered. Thus the clinical, rheological, and biochemicalevidence all indicated that a different membrane skeletal defectwas present in each of the four families.
In searching for a commoncause for the transient hemolyticanemia, we considered three possibilities. The first was thatunique fetal membrane skeletal proteins were present at birthbut were replaced during early infancy by adult counterpart pro-teins. This possibility seemed unlikely since others have foundno evidence that the normal erythrocyte membrane skeleton isstructurally different in neonatal red cells than in adult cells (7-9). Consistent with these observations, we found that ghosts pre-pared from either normal neonatal or adult erythrocytes had
Neonatal Poikilocytosis 947

-oc0
-
o-
F-
V-C-,)
z
UILU
5-C-)
0
0
200 -
100I
0
0 2
GHOST2, 3-C
Figure 4. Effect of 2,3-DPG on ghost rwere loaded with varying amounts of 2chanical stability then determined in tlrange for normal adult (- *) andghosts. Results for elliptocytic parentsv v = mother ofS.W., o o= father of B.D.) and for infants with :transient hemolytic anemia (0-. -a-a- -
are also presented. The cross-hatched a
ghost mechanical stability (without ad(tients (4-29 yr of age) who had hereditnormal 2,3-DPG concentration in neomillimolars per liter. RBCis shown byjust above the abscissa.
equivalent mechanical stability ai2,3-DPG induced mechanical fraythere was no discernable relationsistability and age. No consistent chadimers was noted in the serial studi
Wealso considered the possibreticuloendothelial system of the nodamaged red cells efficiently andpopulation of poikilocytes. Howeva shortening of red cell survival woicircumstances so that the hemol'poikilocytosis is unlikely to be exrdothelial function.
The final possibility we considchanges in the concentration of ftransient neonatal hemolytic anei
established that 2,3-DPG dissociates membrane skeletons orghosts in vitro (22, 23), probably by interfering with spectrin-actin binding (24). Our studies with 2,3-DPG loaded ghosts pre-pared from normal red cells demonstrate a similar effect onghost mechanical stability with a half maximum effect noted ata 2,3-DPG concentration of 5 mmol/liter of ghosts. At 2,3-DPGlevels greater than 6 mmol/liter of ghosts, normal adultor neonatal ghosts become as fragile as those of hereditary pyro-poikilocytes (studied in the absence of 2,3-DPG).
To explore the effect of 2,3-DPG on the membrane skeletaldefects present in the four families we studied, we obtained bloodfrom two affected infants and from each elliptocytic parent. Be-cause elliptocytic ghosts were more mechanically fragile thannormal ghosts, less 2,3-DPG was required to reduce their fragilityto the levels encountered in pyropoikilocytosis. These effects of
.... 2,3-DPG on membrane stability are unlikely to be of any phys-iologic relevance in adult red cells because most of the 2,3-DPG
.......... ... ..... in such cells is bound to deoxyhemoglobin A. However in new-...........Ji born red blood cells, the predominant hemoglobin is fetal he-
............... moglobin which binds 2,3-DPG only to a very limited extent........,,.. #a (25). Therefore, the majority of intracellular 2,3-DPG should
\ ...... ...... be continually available to interact with cytoskeletal membrane;\ A. proteins. The concentration of 2,3-DPG in neonatal red cells is
5.4±1.0 mmol/liter of red cells, a level that is maintainedthroughout the first year of life (26). Expressed per liter of redcell water, which should more accurately reflect the concentrationof 2,3-DPG in the vicinity of the membrane, the value wouldbe - 30% higher, or - 7 mmol/liter cell H20. Bunn and his
4 6 8 colleagues have calculated for adult red cells, assuming the total)PG 2,3-DPG concentration to be 7.2 mmol/liter cell H20, that free
2,3-DPG levels in oxygenated red cells would be 5.9 mmol/litermechanical stability. Ghosts cell H20 and in deoxygenated red cells 0.53 mmol/liter cell H202,3-DPG in vitro and their me- (27). In both oxygenated and deoxygenated neonatal red cells,he ektacytometer. Shaded area, the free 2,3-DPG concentration should be equivalent to that ofneonatal (- --- *) red cell oxygenated adult cells, since deoxyhemoglobin F does not bind(A t~A = mother of J.C., 2,3-DPG. Clearly, such levels are sufficient to weaken the mem-= mother of A.B., o o brane skeleton. The effect would be particularly striking in theneonatal poikilocytosis andn a=B.D., o -*l-ci- = A.B.) presence of an inherited defect of the membrane skeleton. Asarea labeled HPP indicates the hemoglobin F is replaced by hemoglobin A during the first severalded 2,3-DPG) found in five pa- months after birth an increasing proportion of 2,3-DPG is boundtary pyropoikilocytosis. The to hemoglobin A and thus unavailable to interact with the mem-inatal red cells (25), expressed in brane skeleton. Once hemoglobin A levels have risen beyond athe horizontal bar (mean±SD) certain critical point, the membrane dissociating effect of 2,3-
DPGshould largely vanish and only the underlying inheritedprotein abnormality responsible for elliptocytosis would remain.
Several questions raised by our observations cannot be fullynd the same susceptibility to addressed at this time. First, if the cells that contain HbF aregility. In the anemic infants, preferentially destroyed, one might expect HbFlevels to fall morelip between ghost mechanical precipitously than normal after birth in affected infants. Theange in the percent of spectrin limited data available (Fig. 1) is inconclusive in this regard andies carried out in three infants. cannot be interpreted since the possibility of compensatoryAility that the hypofunctional stimulation of HbF synthesis remains unexplored. Second, ineonate (21) might not remove one of our patients (B.D.) and in several described by others (5),allow the accumulation of a the transition from poikilocytic to elliptocytic morphology ander, a prolongation rather than the rise toward normal in the temperature at which heat induceduld be anticipated under these morphological abnormalities are seen did not occur until afterysis associated with infantile 12 mo of age, long after hemoglobin F levels had declined toPlained by altered reticuloen- < 5%. The underlying basis for these events is not clear but,
unlike the extent of hemolysis, they are unlikely to be relatedlered was that developmental to changes in hemoglobin F or free 2,3-DPG levels. Third, notree 2,3-DPG might result in all individuals with HE exhibit poikilocytosis and hemolysismia. The work of others has during infancy, despite the fact that all newborns have high levels
948 Mentzer, Iarocci, Mohandas, Lane, Smith, Lazerson, and Hays

of HbF. The molecular basis of HE is heterogeneous and, in themajority of instances, not well defined (20). Presumably, thelocation or severity of the membrane skeletal defect does not
always favor the appearance of poikilocytosis and hemolysis in
the presence of increased levels of free 2,3-DPG. Lastly, our
studies were largely carried out in ghosts. Whether the effects of2,3-DPG on ghosts will also be seen in intact red cells has recentlybeen questioned by Waugh (28). Our data in infant P.D. showsthat red cell mechanical stability improves during the transitionfrom neonatal poikilocytosis to elliptocytosis, consistent withthe hypothesized effect of free 2,3-DPG. However, a direct eval-uation of the effect of 2,3-DPG on the mechanical stability of
red cells remains to be performed.Our studies confirm that physiologic levels of 2,3-DPG can
produce striking mechanical fragility in red cell ghosts obtainedeither from adults with elliptocytosis or from their infants withtransient poikilocytosis. The abatement of hemolysis in theseinfants coincides with the developmental decline in hemoglobinF levels. It is reasonable to expect that 2,3-DPG would exert a
similar dissociating effect upon a variety of other skeletal proteindefects, explaining the heterogeneous nature of the elliptocyticdefects susceptible to transient neonatal hemolysis. In fact, thestriking degree of hemolysis in early infancy with modest im-provement after 6 mo of age observed in severe spherocytosisassociated with spectrin deficiency (29) suggests that other, non-elliptocytic, membrane skeletal disorders may also be influencedby 2,3-DPG. Finally, it is conceivable that the membrane dis-sociating effects of free 2,3-DPG may also contribute to the longrecognized but poorly understood shortened lifespan of normalfetal and neonatal red cells (30). Such speculations are the stim-ulus for further investigations now under way in our laboratories.
Acknowledgments
Weare grateful for the expert secretarial assistance of Cathy Falletta and
Jane Lee.This work was supported by grants from the National Institutes of
Health (AM-26263, HD-06633, and AM-32094).
References
1. Austin, R. F., and J. F. Desforges. 1969. Hereditary elliptocytosis:An unusual presentation of hemolysis in the newborn associated with
transient morphologic abnormalities. Pediatrics. 44:196-200.2. Carpentieri, U., L. P. Gustavson, and M. E. Haggard. 1977. Pyk-
nocytosis in a neonate: An unusual presentation of hereditary ellipto-cytosis. Clin. Pediat. 16:76-78.
3. Zarkowsky, H. S. 1979. Heat-induced erythrocyte fragmentationin neonatal elliptocytosis. Br. J. Haematol. 41:515-518.
4. Macdougall, L. G., G. Moddley, and M. Quirk. 1982. The pyro-
poikilocytosis-elliptocytosis syndrome in a black South African infant.Clinical and hematological features. Am. J. Ped. Hematol./Oncol. 4:344-
349.5. Prchal, J. T., R. P. Castleberry, R. T. Parmley, W. M. Crist, and
A. Malluh. 1982. Hereditary pyropoikilocytosis and elliptocytosis: Clin-
ical, laboratory, and ultrastructural features in infants and children. Pe-
diatr. Res. 16:484-489.6. Matovcik, L. M., and W. C. Mentzer. 1985. The membrane of
the human neonatal red cell. Clin. Haematol. 14:203-221.7. Hajjar, K. A. 1985. Structural and functional analysis of spectrin
from neonatal erythrocytes. Biochim. Biophys. Acta. 827:460-465.8. Lawler, J., S.-. Liu, J. Palek, and J. Prchal. 1984. A molecular
defect of spectrin in a subset of patients with hereditary elliptocytosis.
Alterations in the alpha-subunit domain involved in spectrin self-asso-ciation. J. Clin. Invest. 73:1688-1695.
9. Palek, J., and S. E. Lux. 1983. Red cell membrane skeletal defectsin hereditary and acquired hemolytic anemias. Semin. Hematol. 20:189-224.
10. Mentzer, W. C., T. Turetsky, N. Mohandas, S. Schrier, C.-S. C.
Wu, and H. Koenig. 1984. Identification of the hereditary pyropoikilo-cytosis carrier state. Blood. 63:1439-1446.
11. Clark, M. R., N. Mohandas, and S. B. Shohet. 1983. Osmoticgradient ektacytometry. Comprehensive characterization of red cell vol-
ume and surface maintenance. Blood. 61:889-910.12. Mohandas, N., M. R. Clark, B. P. Health, M. Rossi, L. C. Wolfe,
S. E. Lux, and S. B. Shohet. 1982. A technique to detect reduced me-
chanical stability of red cell membranes. Relevance to elliptocytic dis-orders. Blood. 59:768-774.
13. Dodge, J. T., C. Mitchell, and D. J. Hanahan. 1963. The prep-
aration and chemical characteristics of hemoglobin-free ghosts of human
erythrocytes. Arch. Biochem. Biophys. 100: 119-130.14. Laemmli, U. K. 1970. Cleavage of structural proteins during the
assembly of the head of bacteriophage T4. Nature (Lond.). 227:680-685.
15. Liu, S. C., and J. Palek. 1980. Spectrin tetramer-dimer equilibriumand the stability of erythrocyte membrane skeletons. Nature (Lond.).285:586-588.
16. Knowles, W., and M. L. Bologna. 1983. Isolation of chemicaldomains of human erythrocyte specrin. Methods Enzymol 96:305-313.
17. Speicher, D. W., J. S. Morrow, W. J. Knowles, and V. T. Marchesi.1982. A structural model of human erythrocyte spectrin. J. Biol. Chem.257:9093-9101.
18. Keitt, A. S. 1971. Reduced nicotinamide adenine dinucleotide-linked analysis of 2,3-diphosphoglyceric acid. Spectrophotometric and
fluorometric procedures. J. Lab. Clin. Med. 77:470-475.19. Lane, P. A., R. L. Shew, T. A. Iarocci, N. Mohandas, T. Hays,
and W. C. Mentzer. 1987. A unique alpha-spectrin mutant in a kindredwith commonhereditary elliptocytosis. J. Clin. Invest. 79:989-996.
20. Palek, J. 1985. Hereditary elliptocytosis and related disorders.Clin. Haematol. 14:45-88.
21. Holroyde, C. P., F. A. Oski, and F. H. Gardner. 1969. The
"pocked" erythrocyte. Red-cell surface alterations in reticuloendothelialimmaturity of the neonate. N. Engl. J. Med. 281:516-520.
22. Sheetz, M. P., and J. Casaly. 1980. 2,3-Diphosphoglycerate and
ATP dissociate erythrocyte membrane skeletons. J. Biol. Chem. 200:
9955-9960.23. Chasis, J. A., and N. Mohandas. 1986. Erythrocyte membrane
deformability and stability. Two distinct membrane properties that are
independently regulated by skeletal protein associations. J. Cell Biol.103:343-350.
24. Wolfe, L. C., S. E. Lux, and V. Ohanian. 1981. Spectrin-actingbinding in vitro: Effect of protein 4.1 and polyphosphates. J. Supramol.Struct. 5(Suppl.):123.
25. Bunn, H. F., and R. W. Briehl. 1970. The interaction of 2,3-diphosphoglycerate with various human hemoglobins. J. Clin. Invest.
49:1088-1095.26. Oski, F. A., and M. Delivoria-Papadopoulos. 1970. The red cell,
2,3-diphosphoglycerate, and tissue oxygen release. J. Pediatr. 77:941-
956.27. Bunn, H. F., B. J. Ransil, and A. Chao. 1971. The interaction
between erythrocyte organic phosphates, magnesium ion, and hemoglo-bin. J. Biol. Chem. 246:5273-5279.
28. Waugh, R. E. 1986. Effects of 2,3-Diphosphoglycerate on the
mechanical properties of erythrocyte membrane. Blood. 68:231-238.29. Agre, P., E. P. Orringer, and V. Bennett. 1982. Deficient red-cell
spectrin in severe, recessively inherited spherocytosis. N. Engl. J. Med.306:1155-1161.
30. Pearson, H. A. 1967. Life-span of the fetal red blood cell. J.
Pediatr. 70:166-17 1.31. Lubin, B. H. 1981. Reference values in infancy and childhood.
In Hematology of Infancy and Childhood. D. G. Nathan and F. A. Oski,editors. Second ed. W. B. Saunders Co., Philadelphia. 1552-1574.
Neonatal Poikilocytosis 949