Embed Size (px)
Citation preview

Models of Cancer Survivorship Health Care: Moving ForwardKevin C. Oeffinger, MD, Keith E. Argenbright, MD, Gill A. Levitt, MBBS, FRCPCH, Mary S. McCabe, RN, MA,Paula R. Anderson, Emily Berry, Jane Maher, MBBS, MRCP, FRCR, Janette Merrill, and Dana S. Wollins, MPH
OVERVIEW
The population of cancer survivors in the United States and worldwide is rapidly increasing. Many survivors will develop healthconditions as a direct or indirect consequence of their cancer therapy. Thus, models to deliver high-quality care for cancer survivorsare evolving. We provide examples of three different models of survivorship care from a cancer center, a community setting, and acountry-wide health care system, followed by a description of the ASCO Cancer Survivorship Compendium, a tool to help providersunderstand the various models of survivorship care available and integrate survivorship care into their practices in a way that fits theirunique needs.
As noted by Parry et al, there is a “booming” population ofcancer survivors in the United States, largely as a result
of advances in early cancer detection and improved cancertherapy as well as the general aging of our society.1 By theyear 2020, it is estimated that there will be 18 million cancersurvivors in the United States.1 This phenomenon is occur-ring in many other countries as well.
As the number of long-term survivors has increased, therehas been a growing realization that many will develop healthconditions as a direct or indirect consequence of their cancertherapy.2-4 Some of these conditions occur during therapyand persist well after the therapy has been completed and canbecome permanent, such as oxaliplatin-induced peripheralneuropathy. However, many outcomes, such as the develop-ment of second cancers and therapy-induced heart failure,are not evident until a decade or two after the initial cancer.Collectively, these outcomes are generally referred to as lateeffects.
The hallmark 2005 Institute of Medicine (IOM) report,From Cancer Patient to Cancer Survivor: Lost in Transition,5highlighted the lack of quality care for cancer survivors in theUnited States, described the transition points where cancersurvivors fall through the cracks of our health care system,and provided a blueprint for the standard of care that shouldbe considered for all cancer survivors. The following wereessential components of lifelong proactive and anticipatorysurvivorship care: prevention of recurrent and new cancersand of other late effects; surveillance for cancer spread, recur-rence, and second cancers; assessment of medical and psy-chosocial late effects; interventions for consequences ofcancer and its treatment including medical and psychosocial
problems; and coordination between specialists and primarycare providers to ensure that all of the survivor’s health needsare met. It was recognized that the content, intensity, and fre-quency of such care would vary from survivor to survivor andbe based on a survivor’s risks related to the cancer, cancertherapy, genetic predispositions, lifestyle behaviors, and co-morbid health conditions. Indeed, the shared-care modelwas advocated as an approach to facilitate communicationand coordination or care between the cancer specialists andother health care providers, particularly primary care clini-cians.5,6 An integral component in this process, as advocatedby the authors of the IOM report, is the Survivorship CarePlan (SCP), which is a brief synopsis of the cancer, cancertherapy, and plan of care based on the survivor’s risks. Use ofthis document was intended to facilitate communication be-tween the cancer specialist, the patient, and other health careproviders. Survivorship care planning has since been en-dorsed by the Commission on Cancer7 and is integrated intothe American Society of Clinical Oncology (ASCO) QualityOncology Practice Initiative (QOPI Cores 17–19). To betterunderstand how best to deliver survivorship care, the IOMreport called for “demonstration programs to test models ofcoordinated, interdisciplinary survivorship care in diversecommunities and across systems of care.”
In 2011, ASCO established the Cancer Survivorship Com-mittee,3 which was tasked with, among other charges, ad-vancing our understanding of different models to deliversurvivorship care. In just a few short years, this committee,consisting of a multidisciplinary group of oncology providersand primary clinicians from academic and community set-tings, health psychologists, health services researchers, and
From the Memorial Sloan Kettering Cancer Center, New York, NY; University of Texas Southwestern Moncrief Cancer Institute, Fort Worth, TX; Great Ormond Street Hospital for Children NHSFoundation Trust, London, UK; Macmillan Cancer Support, London, UK; American Society of Clinical Oncology, Alexandria, VA.
Disclosures of potential conflicts of interest are found at the end of this article.
Corresponding author: Kevin C. Oeffinger, MD, Memorial Sloan Kettering Cancer Center, 300 East 66th St., New York, NY 10065; email: [email protected].
© 2014 by American Society of Clinical Oncology.
MODELS OF CANCER SURVIVORSHIP CARE
asco.org/edbook | 2014 ASCO EDUCATIONAL BOOK 205

patient advocates, has witnessed a rapid evolution of survi-vorship care across North America and internationally.
In the following sections, we provide examples of threemodels of survivorship care from a cancer center, a commu-nity setting, and a country-wide health care system, followedby a description of the ASCO Cancer Survivorship Compen-dium, a tool to help providers understand the various modelsof survivorship care available and integrate survivorship careinto their practices in a way that fıts their unique needs.
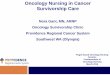
SURVIVORSHIP HEALTH CARE IN THE ACADEMICCANCER CENTERMany academic cancer centers in the United States have de-veloped, or are in the process of developing and evaluating,various models of survivorship care.3 Most programs operateaccording to either a consultative or longitudinal model. Inthe consultative model, survivors generally are referred bythe oncologist or are self-referred for a one-time survivorshipevaluation. Before the visit, the survivorship health care pro-vider(s) creates an SCP. At the visit, the survivor is evaluated,the SCP is shared with him or her, and any necessary referralsfor specialized services are made. Following the consultation,a copy of the SCP and the evaluation are sent to the referringoncologist and the primary care physician; the oncologistthen continues the long-term follow-up care of the survivor,at least for some time. In the longitudinal model, survivorsare transitioned from their oncologist(s) to a survivorshipclinic (either a generic or cancer-specifıc clinic) generally 1 to5 years after treatment and then followed for some period oftime before transitioning the survivor back to a communityprovider. Figure 1 describes a risk-stratifıed longitudinal ap-proach in which care is shared between the cancer center pro-viders and the primary care physician with a transition to thecommunity in most cases.6,8
The Memorial Sloan Kettering Cancer Center ModelAs an example of a longitudinal model, the following is a de-scription of the past, present, and future plans at a single in-stitution, Memorial Sloan Kettering Cancer Center(MSKCC). Similar to many academic centers where childrenare treated for cancer, a survivorship program for pediatriccancer survivors (the Pediatric Long-Term Follow-Up[LTFU] Program) was established in 1990. In this setting,children who are 1 to 2 years from completion of cancer ther-apy are transitioned to the Pediatric LTFU Program, staffedby two physicians and two pediatric oncology nurse practi-tioners (NPs). Patients continue to be evaluated by theirtreating oncologist for cancer recurrence, but the LTFU Pro-gram providers screen for and manage any sequelae of treat-ment. As with other similar programs, it was soon realizedthat although many survivors could be transitioned back tocommunity-based primary care physicians between age 18and 21 years, there were also high-risk survivors with multi-ple therapy-related comorbidities who could benefıt frommore specialized follow-up care at the cancer center.
Thus, in 2005 the Adult LTFU Program was established atMSKCC for high-risk adult survivors of a childhood, adoles-cent, or young adult cancer. This program is staffed by fıveprimary care physicians, three NPs, and a nurse. The Pediat-ric and Adult LTFU programs share a nurse who prepares anSCP for all new visits. Both programs also benefıt from theclinical support of a psychologist who is highly experiencedin working with cancer survivors with psychosocial prob-lems, including fears of recurrence, and with multiple serioushealth problems related to their cancer therapy.
Beginning in 2006, MSKCC began developing an innova-tive care model for survivors of adult-onset cancers in whichfollow-up care is solely provided by NPs (or physician assis-tants [PAs]). Initially, pilots were developed to evaluate thefeasibility of this model with a focus on common cancers. Itwas found that this model was successful in having a physi-cian refer and patients accept a transition from their oncolo-gist(s) to a survivorship NP without compromising theircare.
Using this approach, clinics have been developed withinmany of the MSKCC disease management teams and ser-vices, including bone marrow transplant, breast, colorectal,endocrinology, gynecology, head and neck, melanoma, tho-racic, and urology/prostate. In each of these settings, a sharedcare approach is employed for all patients. At each visit in theNP/PA or high-risk survivorship clinics, a copy of the prog-ress note and an updated SCP are autofaxed to the commu-nity clinician with an accompanying letter highlighting anynecessary coordination of responsibilities. In 2013, therewere more than 12,000 patient visits in the MSKCC survivor-ship clinics, of which more than 10,000 were in an NP/PAsurvivorship clinic.
Looking to the future needs of the institution and evolvingcare paradigms, MSKCC is establishing a Center for CancerSurvivorship. Five-year clinical care goals include establish-ment of a multidisciplinary Survivorship ManagementTeam; implementation of an institution-wide risk-stratifıed
KEY POINTS
� Many cancer survivors will develop health conditions as adirect or indirect consequence of their cancer therapy.
� The 2005 Institute of Medicine (IOM) report, From CancerPatient to Cancer Survivor: Lost in Transition, provided ablueprint for the standard of care that should beconsidered for all cancer survivors.
� The Survivorship Care Plan, a brief synopsis of the cancer,cancer therapy, and plan of care based on the survivor’srisks, is an integral component of survivorship health care.
� Models of survivorship health care will vary based onavailable resources and the needs of the local survivorshippopulation. Nurse practitioners and physicians assistantsare essential in cancer center and community-basedsurvivorship programs.
� The ASCO Survivorship Care Compendium will serve as arepository of tools and resources to enable oncologyproviders to implement or improve survivorship care withintheir practices.
OEFFINGER ET AL
206 2014 ASCO EDUCATIONAL BOOK | asco.org/edbook

plan for the care of all new patients with cancer diagnosedand treated at MSKCC; development of institution-wideguidelines and guidance for screening, assessment, and man-agement of long-term and late effects including second pri-mary cancers; development of an integrated plan forspecialized cancer survivorship services; and periodic evalu-ation of survivorship clinical care delivered at the institution.
SURVIVORSHIP HEALTH CARE IN THE COMMUNITYSETTINGIn the community setting, many oncology practices havesimilarly implemented survivorship clinics or expanded thesurvivorship services they provide. The National Cancer In-stitute (NCI) provides funding to 30 community cancer cen-ters in 22 states through the NCI Community Cancer CenterProgram (NCCCP). A key aim of this program is to enhance
cancer survivorship care services available at communityhospitals. Resources developed through the NCCCP networkare made available to other community cancer programsthrough publications, presentations at national meetings,and the NCCCP website.9
Integrating a Community Solution for CancerSurvivorship CareProviding multidisciplinary services for all oncology patientsthrough an integrated community survivorship model is theaim of the Fort Worth Program for Community Survivorship(ProComS). Before its establishment, survivorship servicesin the community were fragmented, offered only in a fewhospitals and clinics for specifıc diagnoses and providers, andinadequate in meeting the needs of uninsured and underin-sured cancer survivors. To address this issue, the Universityof Texas Southwestern Medical Center Moncrief Cancer In-
FIG 1. Risk-stratified shared care model of cancer survivors.From McCabe MS, Partridge AH, Grunfeld E, et al. Risk-based health care, the cancer survivor, the oncologist, and the primary care physician. Reprinted from Semin Oncol. 2013;40:804-812, withpermission from Elsevier.
MODELS OF CANCER SURVIVORSHIP CARE
asco.org/edbook | 2014 ASCO EDUCATIONAL BOOK 207

stitute (UTSW-MCI) obtained funding from the Cancer Pre-vention Research Institute of Texas to lead a community-wide partnership for local oncology providers, consolidatingsurvivorship care and placing emphasis on the underserved.
Combining principles from the shared care survivorshipmodel6,10 and the Folsom Report,11,12 UTSW-MCI addressedthe challenges associated with a competitive oncology envi-ronment and organizational concerns. The Folsom Reportplaced emphasis on resolving population health care frag-mentation through the committed involvement of the entiremedical and public health community, forming a “commu-nity of solution.” These collaborations enable the delivery ofcomprehensive health care to be a sustainable, community-wide endeavor, successfully addressing survivorship as apopulation health issue. Integrating these concepts, UTSW-MCI leadership brought together representatives from thelocal safety-net hospital, three area full-service hospitals, twolarge oncology provider groups, and three local cancer agen-cies to address this challenge as a community problem andproposed to provide consistent survivorship services for alloncology patients. Recognizing that UTSW-MCI does notprovide direct oncology treatment, its leadership role was feltto be “competitively neutral” in working to build trust amongcommunity partners in a competitive patient environment.As such, the ProComS clinic core services are offered onsiteat UTSW-MCI, while some patient-specifıc services (speech/language and lymphedema therapy) are referred to a com-munity partner. UTSW-MCI has further incorporated theFolsom Report recommendations through the initiation ofthe Community Advisory Board (CAB) and quarterly meet-ings, providing oversight and recommendations regardingpatient referrals, treatment expertise, and feedback mecha-nisms to the primary oncology provider.
ProComS is open to all adult cancer survivors, enrollingparticipants regardless of health care provider, gender, diag-nosis, stage, functional status, insurance level, or ability topay. Providing ongoing supportive, psychosocial, and behav-ioral care for survivors, the clinic offers oncology-certifıedregistered nurse evaluations, social worker assessments, ex-ercise training, registered dietitian consultations, and psy-chologic and certifıed genetic counseling. In addition to thesecore components, ProComS offers diagnosis-driven supportgroups and a variety of group learning opportunities. All ser-vices are provided at no cost to the patient and are supportedthrough various funding sources. The Folsom Report en-courages accountability through measurable outcomes usingreliable and valid tools for program evaluation. As such, theeffect on multiple psychosocial and behavioral domains isevaluated using four questionnaires that are well validatedamong patients with cancer and survivors; these self-reportsurveys are completed at enrollment and at three additionaltime points. These four instruments include: the FunctionalAssessment of Cancer Treatment General version (FACT-G)13 to evaluate quality of life, including physical, social,emotional, and functional well-being; the Brief Symptom In-ventory (BSI-18)14 to measure psychologic distress; the Inter-national Physical Activity Questionnaire (IPAQ-short
version)15 to assess participation in physical activity; and theMulti-Factor Screener from the 2000 National Health Inter-view Survey (NHIS) Cancer Control Supplement16 to evalu-ate dietary intake, including processed meat, fruits andvegetables, saturated fats, and grains and beans.
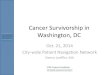
In 2 years, the program has received more than 1,400 pa-tient referrals from community partners, internal staff, andprogram participants. During this time, the bi-lingual multi-disciplinary survivorship team has enrolled more than 400cancer survivors, with more than 6,000 patient encounters(Fig. 2). ProComS survivors averaged 14 encounters acrossthe various disciplines. Preliminary analysis indicates im-proved function for these participants with improvements inquality of life, physical activity, and dietary intake and a de-crease in psychosocial distress. These intermediate measuresare reviewed with the CAB along with other short-term out-comes such as patient satisfaction. Although approximately30% of survivors referred actually participated in the pro-gram, an estimated 20% of nonparticipants reside in rural ar-eas surrounding Dallas-Fort Worth. Distance to the programis a formidable barrier to care, despite invitation and ex-pressed interest in the clinic and the services provided.
Leveraging its relationships with stakeholders in eight sur-rounding rural counties established through other programs,UTSW-MCI will expand its multidisciplinary survivorshipservices using a mobile delivery model (Fig. 3). Recognizingthat mobile care programs have been used to successfullyprovide a variety of clinical services including primary care,17
perinatal care,18 preventive services, and health education inrural populations,19 UTSW-MCI intends to implement itsevidence-based program using this health delivery model.Recognizing that the survivorship phase of care represents adistinct opportunity to improve health and quality of life forrural cancer survivors, the program will address lingeringmedical and psychosocial effects of treatment, detect recur-rent or new cancers, and promote healthy lifestyle changes.
Community needs assessments have identifıed a shortageof organized evidence-based cancer survivorship serviceswithin the specifıed service area in addition to a lack of publicor charitable transportation services. These barriers, whencombined with health professional and facility shortages, pa-tient inexperience in accessing care within a complex medicalnetwork, and an overarching hesitation among residents toseek help outside of a zone of familiarity, negatively affect acancer survivor’s ability to receive appropriate post-treatment survivorship care. As such, the implementation ofthis mobile survivorship clinic is anticipated to have pro-found effect on addressing these barriers.
SURVIVORSHIP HEALTH CARE IN THEINTERNATIONAL SETTINGParalleling the activity in the United States, many centersaround the world are developing survivorship programs andinitiatives. Here we provide an example of a program outsideof the United States that is being implemented nationwide.
OEFFINGER ET AL
208 2014 ASCO EDUCATIONAL BOOK | asco.org/edbook

Implementation of Survivorship Programs in theSetting of a Nationalized Health Care SystemThe National Health System (NHS) in the United Kingdom,established in 1948, provides health care to all free at thepoint of delivery including primary, secondary, and tertiarycare. During the fırst decade of the 21st century, there was aswell of opinion that cancer survivors were not adequatelyserved, highlighted in the Cancer Reform Strategy publishedin 2007.20 Key information included the publication ofthe prevalence of those alive in the United Kingdom after adiagnosis of cancer21 and the description of the prevalence ofunmet needs in the year following treatment.22 A multidisci-
plinary Think Tank event was held involving a range of stake-holders including survivors, parents, and caregivers (i.e.,people who support cancer survivors) together with charitiesinvolved in cancer care. Patient focus groups were held todefıne the scope of the program. As a result, the NationalCancer Survivorship Initiative (NCSI) launched in 2008 as apartnership between the Department of Health (England),Macmillan Cancer Support (cancer charity), NHS Improve-ment (national organization supporting quality improve-ment), and other third-sector organizations (not-for-profıtorganizations such as CLIC Sargent and the Teenage CancerTrust). The primary aim of the NCSI is to reduce the effect ofcancer and its treatment on the health and well-being of sur-vivors of cancer in adults, young people, and children. Thedefınition of cancer survivor used included anyone living fol-lowing a diagnosis of cancer. The initiative focused much ofits work on adults after completion of fırst treatment.
The partnership funded workstreams focusing on the fol-lowing topics: assessment and care planning; consequencesof treatment of adult cancers; supported self-management;work and fınance; physical activity; active and advanced dis-ease; research; and children and young people’s needs.23
Their preliminary work contributed to a Vision document24
and a summary of research fındings and questions.25
FIG 2. Community model of survivorship care.
FIG 3. University of Texas Southwestern Moncrief CancerInstitute (UTSW-MCI) mobile survivorship expansion map.
MODELS OF CANCER SURVIVORSHIP CARE
asco.org/edbook | 2014 ASCO EDUCATIONAL BOOK 209

A strategy of “investigate, innovate, and implement“ wastaken forward over the following 7 years. Five major phasesin the cancer pathway were identifıed, and cancer prevalencewas estimated for each phase to understand resource impli-cations for each cancer. These phases included diagnosis andtreatment (taken to be the fırst year after diagnosis), recovery(taken to be the second year after diagnosis), early monitor-ing (2 to 5 years following diagnosis when the risk of recur-rence and fırst onset of persistent treatment-relatedconsequences is highest), late monitoring (greater than 5years postdiagnosis, when late consequences usually
emerge), progressive disease (including complex treatment-related consequences, taken from the point of recurrence oridentifıcation of complex treatment consequences), and end-of-life care (defıned as care during the last year of life) (Fig.4).26
Four cancer types (breast, colorectal, prostate, and lung)were selected to test and pilot models of care, with the goal ofredesigning pathways of care after primary treatment forcancer and shifting activity from routine follow-up appoint-ments, which do not always add value, to rehabilitation andsupport for self-management after treatment when indi-
FIG 4. United Kingdom National Health Service breast and lung cancer pathways.
OEFFINGER ET AL
210 2014 ASCO EDUCATIONAL BOOK | asco.org/edbook

cated, with identifıcation and management of those withcomplex problems. The principles behind risk stratifıcationfor each pathway are similar for adults and for children andyoung people (CYP). Personalized care linked to individualcircumstances, needs, and preferences is key, rather than asole dependence on the cancer type, treatment, or time fromtreatment. To help empower survivors, they receive a struc-tured holistic needs assessment and care plan, treatmentsummary, support and education events, and a review by aprimary care physician. The treatment summary providesclear written instructions on how to obtain rapid access toany necessary care via a care coordinator. These key princi-ples support survivors to self-manage as much as possible.Implementation is ongoing with early pathway evaluationapproved by the National Institute for Health and Care Ex-cellence (NICE) with a how-to guide published to assist localteams.27 In 2013, the NCSI published Living With and Be-yond Cancer: Taking Actions to Improve Outcomes,28 whichset out the knowledge gained to date to support commission-ers, providers, and others to take the actions necessary to im-prove outcomes for cancer survivors.
The CYP workstream had the same objectives as above;however, the process differed as it covered the whole survi-vorship pathway for all cancers diagnosed. This was becausethe organization of childhood cancer services differs. Only 22centers in the United Kingdom treat all children with cancer,amounting to about 1,500 new patients per year with 30,0005-year survivors,29 a fraction of the adult population. In ad-dition, the community has been delivering follow-up servicesfor childhood cancer survivors for at least 2 decades. There-fore, there was relevant background information, albeit withconsiderable variation across the country.30
The CYP workstream, with the help of Children’s Cancerand Leukemia Group (CCLG) centers reviewed care deliv-ered, refıned models of care, and formulated patient path-ways.31 The participants involved in this workstreamincluded pediatric cancer providers; NIH commissioners;young people, patients, and families; and members of thethird sector (e.g., charities, volunteers, and communitygroups). Three key questions were asked before embarkingon the change program: what are we trying to achieve? whatchange will result in improvement? and how will we knowchange has made a difference? Changes were identifıed, andthen there was a process of testing followed by implementa-tion. This work is supported by NHS Improvement and in-volves close monitoring of progress with regular workshopsand publications of progress.32
Three patient pathways were developed for children andyoung adults. The pathways require that each survivor re-ceive a personalized SCP. Each patient is stratifıed to a differ-ent model of care depending on his risk of late effects. Thepathway is flexible and includes elements of informationtransfer and education. At different time points, each survi-vor will be discussed in a multidisciplinary team meeting.Underpinning this pathway was the testing performed by the
different centers (Fig. 5).32 “National champions” supportedby the NCSI assisted in the program alongside the effectiveprofessional national network of the CCLG and the Teenag-ers and Young Adults with Cancer. Implementation is, inpart, dependent on the health providers receiving enoughrecognition from commissioners to commission this service.A cost-benefıt analysis was performed that suggested an ef-fective service may not be cost-effective in the short term;however, providing effective monitoring and health preven-tion services should benefıt survivors by reducing those lostto follow-up, thereby reducing hospital appointments andemergency admissions.
THE ASCO CANCER SURVIVORSHIP COMPENDIUMOne of the major initiatives of the ASCO Cancer Survivor-ship Committee since its inception in 2010 has been to de-velop a toolbox for providers. Emanating from this aim is theASCO Survivorship Compendium, recently launched on theASCO website. As an accompaniment to the educational op-portunities and clinical guidance ASCO offers on survivor-ship care, the Survivorship Care Compendium will serve as arepository of tools and resources to enable oncology provid-ers to implement or improve survivorship care within theirpractices. Although ASCO endorses the National Coalitionfor Cancer Survivorship defınition of a cancer survivor asstarting at the point of diagnosis, the focus of the informationand resources offered throughout this compendium will beon those individuals who have completed curative treatmentor who have transitioned to maintenance or prophylactictherapy.
The compendium has two primary sections: Putting Survi-vorship Care into Practice and Online Resources. The formersection includes key components of survivorship care, build-ing a survivorship care program, implementing survivorshipcare in practice, and measuring the quality of survivorshipcare. Online resources linked to the website include clinicaltools and resources, coverage and reimbursement informa-tion, educational opportunities, resources for patients andfamilies, and research resources. ASCO’s updated SCP tem-plate is included in the Compendium as well. In developingthis resource, the intent of the Committee is to provide a fastand effıcient method to download or print information thatwould be helpful in different settings by different types ofproviders.
CONCLUSIONSince the 2005 IOM report on cancer survivors, much hasoccurred in the United States and worldwide to improve thecare of cancer survivors. Although there remains much to doin terms of testing different models and components of thosemodels to see what works in different settings, the paradigmof survivorship health care has rapidly evolved and is increas-ingly being adopted.
MODELS OF CANCER SURVIVORSHIP CARE
asco.org/edbook | 2014 ASCO EDUCATIONAL BOOK 211

Disclosures of Potential Conflicts of Interest
Relationships are considered self-held and compensated unless otherwise noted. Relationships marked “L” indicate leadership positions. Relationships marked “I” are those held by an immediatefamily member; those marked “B” are held by the author and an immediate family member. Relationships marked “U” are uncompensated.
Employment or Leadership Position: None. Consultant or Advisory Role: None. Stock Ownership: None. Honoraria: None. Research Funding: KeithE. Argenbright, Cancer Prevention and Research Institute of Texas. Expert Testimony: None. Other Remuneration: None.
References
1. Parry C, Kent EE, Mariotto AB, et al. Cancer survivors: a booming pop-ulation. Cancer Epidemiol Biomarkers Prev. 2011;20:1996-2005.
2. Ganz PA. Why and how to study the fate of cancer survivors: observa-tions from the clinic and the research laboratory. Eur J Cancer. 2003;39:2136-2141.
3. McCabe MS, Bhatia S, Oeffınger KC et al. American Society of ClinicalOncology statement: achieving high-quality cancer survivorship care.J Clin Oncol. 2013;31:631-640.
4. Oeffınger KC, Robison LL. Childhood cancer survivors, late effects, and anew model for understanding survivorship. JAMA. 2007;297:2762-2764.
5. Hewitt M, Greenfıeld S, Stovall E (eds). From Cancer Patient to CancerSurvivor: Lost in Transition. Washington, DC: The National AcademiesPress; 2005.
6. Oeffınger KC, McCabe MS. Models for delivering survivorship care.J Clin Oncol. 2006;24:5117-5124.
7. American College of Surgeons Commission on Cancer. Cancer Pro-gram Standards 2012: Ensuring Patient Centered Care, V1.2. http://www.facs.org/cancer/coc/programstandards2012.html. AccessedJanuary 22, 2014.
8. McCabe MS, Partridge AH, Grunfeld E, et al. Risk-based health care, thecancer survivor, the oncologist, and the primary care physician. SeminOncol. 2013;40:804-812.
9. National Cancer Institute. NCI Community Cancer Centers Program.http://ncccp.cancer.gov/. Accessed January 14, 2014.
10. McCabe MS, Jacobs L. Survivorship care: models and programs. SeminOncol Nurs. 2008;24:202-207.
FIG 5. United Kingdom National Health Service pediatric aftercare pathway.
OEFFINGER ET AL
212 2014 ASCO EDUCATIONAL BOOK | asco.org/edbook

11. Folsom Group. Communities of solution: the Folsom Report revisited.Ann Fam Med. 2012;10:250-260.
12. Griswold KS, Lesko SE, Westfall JM, et al. Communities of solution:partnerships for population health. J Am Board Fam Med. 2013;26:232-238.
13. Cella DF, Tulsky DS, Gray G, et al. The Functional Assessment of Can-cer Therapy scale: development and validation of the general measure.J Clin Oncol. 1993;11:570-579.
14. Derogatis LR. BSI-18 Administration, scoring and procedures manual.Minneapolis, MN: National Computer Systems; 2000.
15. Hallal PC, Victora CG. Reliability and validity of the International Phys-ical Activity Questionnaire (IPAQ). Med Sci Sports Exerc. 2004;36:556.
16. National Cancer Institute Applied Research. Multifactor screener in the2000 NHIS Cancer Control Supplement. http://appliedresearch.cancer-.gov/surveys/nhis/multifactor/. Accessed January 12, 2014.
17. Heller BR, Goldwater MR. The Governor’s Wellmobile: Maryland’smobile primary care clinic. J Nurs Educ. 2004;43:92-94.
18. Edgerley LP, El-Sayed YY, Druzin ML, et al. Use of a community mobilehealth van to increase early access to prenatal care. Matern Child HealthJ. 2007;11:235-239.
19. Garrett DK. Mobile access: opening health care doors. Nurs Manage.1995;26:31-33.
20. National Health Service. Cancer Reform Strategy. http://www.nhs.uk/NHSEngland/NSF/Documents/Cancer Reform. Accessed January 15,2014.
21. Maddams J, Utley M, Moller H. Projections of cancer prevalence in theUnited Kingdom, 2010-2040. Br J Cancer. 2012;107:1195-1202.
22. Armes J, Crowe M, Colbourne L, et al. Patients’ supportive care needsbeyond the end of cancer treatment: a prospective, longitudinal survey.J Clin Oncol. 2009;27:6172-6179.
23. Jefford M, Rowland J, Grunfeld E, et al. Implementing improved post-
treatment care for cancer survivors in England, with reflections fromAustralia, Canada and the USA. Br J Cancer. 2013;108:14-20.
24. National Cancer Survivorship Initiative. NCSI Vision Document. http://www.ncsi.org.uk/wp-content/uploads/NCSI-Vision-Document.pdf.Accessed January 17, 2014.
25. Richards M, Corner J, Maher J. The National Cancer Survivorship Ini-tiative: new and emerging evidence on the ongoing needs of cancer sur-vivors. Br J Cancer. 2011;1:S1-4 (105 suppl).
26. Maher J, McConnell H. New pathways of care for cancer survivors: add-ing the numbers. Br J Cancer. 2011;1:S5-10 (105 suppl).
27. National Cancer Survivorship Initiative. Innovation to implementation:stratifıed pathways of care for people living with or beyond cancer- “ahow to guide.” www.ncsi.org.uk/resources/nhs-reports/adults/innova-tion-to-implementation-stratifıed-pathways-of-care-for-people-living-with-or-beyond-cancer-a-how-to-guide/. Accessed January 17, 2014.
28. National Cancer Survivorship Initiative. Living with and beyond can-cer: taking action to improve outcomes. http://www.ncsi.org.uk/wp-content/uploads/Living-with-and-beyond-2013.pdf. Accessed January22, 2014.
29. Jenney M, Levitt G. Survivors of childhood cancer. BMJ. 2009;339:b4691.
30. Taylor A, Hawkins M, Griffıths A et al. Long-term follow-up of survi-vors of childhood cancer in the UK. Pediatr Blood Cancer. 2004;42:161-168.
31. National Cancer Survivorship Initiative. Building the evidence: devel-oping the winning principles for children and young people. http://www.ncsi.org.uk/wp-content/uploads/CYP-Building-The-Evidence.pdf. Accessed January 17, 2014.
32. Glaser A, Levitt G, Morris P, et al. Enhanced quality and productivity oflong-term aftercare of cancer in young people. Arch Dis Child. 2013;98:818-824.
MODELS OF CANCER SURVIVORSHIP CARE
asco.org/edbook | 2014 ASCO EDUCATIONAL BOOK 213