Embed Size (px)
Citation preview

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Modeling for decision making in clinical programs- Case Studies
Rolf Burghaus – Bayer Schering PharmaClinical Pharmacology / Modeling & Simulation

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Modeling & Simulation - Positioning
• Modeling & Simulation is a means to integrate knowle dge and data in order to:
– Check for consistency of different (types of) data sets and preexisting or derived knowledge – i.e. challenge hypotheses
– Generate in depth understanding of pharmacological processes– Provide predictions in accordance with all related information and data– Analyze and understand unexpected findings
• The overall goal of Modeling & Simulation is to provi de a basis for best informed decisions to comply with regulatory requi rements and create economic value

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Case 1
Female Cycle Simulationfor Clinical Development in Women’s Health

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)General Design
The Female Cycle Simulator comprises:• Physiology processes in following organs
– Hypothalamus– Pituitary– Ovaries– Blood
• Dynamic representation of– Hormones (e.g. progesterone (P4), estradiol (E2), F SH
and LH) – Enzymes– Receptors– Follicles/follicular states– GnRH pulse generating system
• Basic simulator is an academic tool integrating physiological/biological knowledge extracted from literature sources
• Simulator is adapted for industrial Clinical Pharmacology use by incorporating internal expertise and specific data
Basic FCS:Reinecke I, Deuflhard P, .J Theor Biol. 2007 Jul 21;247(2):303-30. Epub 2007 Mar 14

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Implementation
MoBI™/ PKSim®Implementation of FCS in standard software package:• allows for complex and efficient simulation work• enables quality management

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Model Establishment using Clinical Data
e.g. Gonadotropins (FSH), Progesterone (P4)
FCS adequately describes mean biological processes in great detail.

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Model Establishment using Clinical Data
e.g. Follicle Growth Pattern
• FCS adequately describes processes up to relevant clinical endpoints.
• How to qualify for prediction of drug actions?

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Qualification by Simulation of Clinical Study Data
Exo
geno
us h
orm
one
expo
sure
Exposure-
population
quantiles
FCS
Study population pharmacokinetics as described by compartmental non-linear mixed
effects model based on clinical study data
Hoogland score limits(clinical endpoint)
Follicle size-
population
quantiles
Study Population clinical endpointpredicted using
Female Cycle Simulator
• FCS adequately predicts:– Qualitative pharmacodynamic response pattern– Statistical distribution of response classes (Hoogland scores)
• FCS predicts effect of artificial exogenous hormones not used during simulator establishment!

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Application for Optimization of Dosing Schedules
Hoogland score limit 10 mmHoogland score limit 13 mm
Efficacy Classification System
quantiles quantiles
quantiles quantiles

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Application for Optimization of Dosing Schedules
(novel) hormones /
hormone combinations and dosages
FCS supports identification of promising treatment schemes
Effi
cacy
Cla
ssifi
catio
n C
lass
Non-trivial treatment schemes

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Application for Optimization of Dosing Schedules
varia
bilit
yof
popu
latio
n
variabilityof
population
Population
quantiles
Numeric treatment scheme property
extremecase
extremecase
covariates ?
Analysis of diverse set of virtual trials helps to gain understanding about the origin of differences in (expected) clinical performance.

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Female Cycle Simulator (FCS)Summary
• FCS is a detailed mechanistic simulator of academic origin
• FCS is continuously extended with expert knowledge v ia data from– Research studies– (clinical) development
studies
• FCS was integrated into company platform to support so phisticated simulation programs
• FCS serves as a tool to– Identify promising research and development options– Predict pharmacodynamic study results – Analyze and understand clinical development data

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Case 2
Modeling & Simulation to support Pediatric Developm ent

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Case Study 2: Pediatric Development
Pediatric Development
• Prerequisite for registration or patent life extension EU /US legislation for any submission of novel and marketed drugs
• Pediatric development is especially challenging as– PK or PD studies in healthy children are discouraged fo r ethical
reasons�First pediatric application are performed in diseased c hildren�Pediatric starting dose needs to be safe and efficac ious
• Pediatric dose selection requires consideration of all drug specific as well as relevant pediatric information.

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
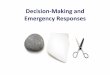
Pediatric DevelopmentKnowledge Management – Data Integration
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
A physiology based pharmacokinetic model•implements mechanistic hypotheses•integrates data from
•in vitro experiments•different preclinical species•clinical study data•data from different application routes
•Thus challenges pharmacokinetic understanding

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
VE
NO
US
BL
OO
D P
OO
L
AR
TE
RIA
L B
LO
OD
PO
OL
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTES
HEAR T
BRA INFAT
B ON E
SKIN
MU SC LE
VE
NO
US
BL
OO
D P
OO
L
AR
TE
RIA
L B
LO
OD
PO
OL
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTES
HEAR T
BRA INFAT
B ON E
SKIN
MU SC LE
Pediatric DevelopmentUtilization of Pediatric Knowledge
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAINFAT
BONESKIN
MUSCLE
Kea
rns
et a
l. 20
03
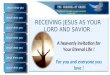
M&S enables prediction of drug exposure in pediatric populationsincorporating all relevant preexisting data and pediatric physiology
knowledge.

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Pediatric StudiesClinical Trial SimulationBSP Standard Workflow
establish kinetic population model(PBPK/population module)
simulate virtual study population
define / refine study designi.e. sampling schema and power
apply study design to virtualpopulation and establish
NLME model
derive study endpoints forvirtual study population
Study design established
iden
tific
atio
nno
t suf
ficie
nt
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAI N
FATBONE
SKI N
MUSCLE
VE
NO
US
BLO
OD
PO
OL
AR
TE
RIA
L B
LOO
D P
OO
L
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GALL BLADDER
STOMACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TESTESHEART
BRAI N
FATBONE
SKI N
MUSCLE
VE
NO
US
BLO
OD
PO
OL
ART
ER
IAL
BLO
OD
PO
OL
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GA LL BLADDER
STO MACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TES TESH EA RT
BR AI NFA T
B O NESK IN
MU SC LE
VE
NO
US
BLO
OD
PO
OL
ART
ER
IAL
BLO
OD
PO
OL
PANCREAS
SPLEEN
PORTAL VEIN
LIVER
KIDNEY
LUNG
DOSEi.v.
p.o.
GA LL BLADDER
STO MACH
WALL
SMALL INTESTINE
WALL
LARGE INTESTINE
WALL
TES TESH EA RT
BR AI NFA T
B O NESK IN
MU SC LE
Figure 23-31: Age-dependence of AUC(6-7)days[mg*h/l] for female. Graph (A) presents data in a linear graph, and (B) in a semi-log graph.
1 2 3 6 9 1 1.5 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
100
200
300
400
500
AU
C(6
-7)d
ays
[mg
*h/l]
months years
A
1 2 3 6 9 1 1.5 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
101
102
AU
C(6
-7)d
ays
[mg*
h/l]
B
Depot1
K30
F1F2 F3
K12
K31
K32
K23
K27 K72K20 K24
K63 = 0
Dose
Central2
Lung3
Peripher7
Urine4
Sputum (interval)5
Sputum (reduction) 6
=Depot1
K30
F1F2 F3
K12
K31
K32
K23
K27 K72K20 K24
K63 = 0
Dose
Central2
Lung3
Peripher7
Urine4
Sputum (interval)5
Sputum (reduction) 6
=
����

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Pediatric DevelopmentSummary
• Recent EU/US legislations require pediatric developmen t for every drug to be registered.
• Due to the special conditions of pediatric developme nt an extrapolation of available scientific knowledge (drug and pediatric conditions) for dose selection is mandatory.
• Bayer Schering Pharma has implemented a workflow combin ing mechanistic and statistical modeling.

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Challenges

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Comparison of PB and NLME modelingFeatures
V2/F
K20
K23V3/F
KA
K32
DADT(2) = KA*A(2)-K23*A(2)+K32*A3-K20*A(2)DADT(3) = K23*A(2)-K32*A(3)
Time
Con
cent
rati
on
NLME Modeling:• Approach to
�characterize (pre-) clinical study data
�identify structural properties�generate individual (post-hoc)
estimates from sparse data�simulate defined sub-
populations• Statistically sound procedure• High level of standardization• Good authority acceptance
PB Modeling:• Approach to
�integrate scientific knowledge�analyze/understand
pharmacological processes, mechanistically
�extrapolate to populations/ conditions/ properties not covered by data
�challenge consistency of hypotheses and data
• Means of knowledge management
How to combine?

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
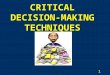
Combined statistical and physiologically-based mode ling Theophylline
PK-Sim® and MoBi®
Structure PBPK-Model for theophylline
intestinal permeability (Pint)
clearance (cl)
intestinal transit time (ITT)
per patient
Lipophilicity (Lip)per drug Error (σ)

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Combined statistical and physiologically-based mode lingBayesian approach
0 500 1500
05
1015
20
Patient 1
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 2
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 3
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 4
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 5
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 6
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 7
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 8
Time [min]V
enou
s P
lasm
a C
once
ntra
tion
0 500 1500
05
1015
20
Patient 9
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 10
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20
Patient 11
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
0 500 1500
05
1015
20Patient 12
Time [min]
Ven
ous
Pla
sma
Con
cent
ratio
n
PK-Sim® and MoBi®
� ?

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Conclusions
• Modeling and simulation serves as prospective tool f or decision making
– integrating in vitro and in vivo data to translatio nal pharmacology– to anticipate new clinical study data
• Mechanistic and classical compartmental population modeling are complementary in terms of
– Capacity for extrapolation (prediction)– Statistical performance (retrospective analysis)
• Both technologies are technically feasible and matu re– need for innovation in bridging the gap is recogniz ed
• Mechanistic modeling is shifting the paradigm from ret rospective data evaluation to predictive pharmacology

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”
Acknowledgements
Female Cycle Simulation• Hartmut Blode• Peter Deuflhard - Zuse Institute Berlin (ZIB)• Christoph Gerlinger• Stefanie Reif• Isabel Reinecke
Pediatric Simulations• Corina Becker• Martin Blunck• Matthias Frede• Wolfgang Mück• Stefan Willmann – Bayer Technology Services GmbH
Mechanistic population modeling• Michael Block – Bayer Technology Services GmbH• Linus Görlitz – Bayer Technology Services GmbH• Jörg Lippert – Bayer Technology Services GmbH

Join
t Mee
ting
MH
RA
/EF
SP
I 201
0-03
-30,
R. B
urgh
aus
“Mod
elin
g fo
r de
cisi
on m
akin
g in
clin
ical
pro
gram
s -
Cas
e S
tudi
es”