Embed Size (px)
Citation preview
BRAINA JOURNAL OF NEUROLOGY
Mild cognitive impairment associated withlimbic and neocortical lewy body disease:a clinicopathological studyJennifer Molano,1 Bradley Boeve,1 Tanis Ferman,2 Glenn Smith,2 Joseph Parisi,1,3
Dennis Dickson,4 David Knopman,1 Neill Graff-Radford,1 Yonas Geda,2 John Lucas,2
Kejal Kantarci,5 Maria Shiung,5 Clifford Jack,5 Michael Silber,1 V. Shane Pankratz6 andRonald Petersen1,6
1 Department of Neurology, Mayo Clinic College of Medicine, Rochester, MN 55905, and Jacksonville, FL 32224, USA
2 Psychology and Psychiatry, Mayo Clinic College of Medicine, Rochester, MN 55905, and Jacksonville, FL 32224, USA
3 Laboratory Medicine and Pathology, Mayo Clinic College of Medicine, Rochester, MN 55905, and Jacksonville, FL 32224, USA
4 Neuropathology Laboratory, Mayo Clinic College of Medicine, Rochester, MN 55905, and Jacksonville, FL 32224, USA
5 Diagnostic Radiology, Mayo Clinic College of Medicine, Rochester, MN 55905, and Jacksonville, FL 32224, USA
6 Health Science Research, Mayo Clinic College of Medicine, Rochester, MN 55905, and Jacksonville, FL 32224, USA
Correspondence to: Bradley F. Boeve, MD,
Mayo Clinic,
200 First Street SW,
Rochester, MN 55905,
USA
E-mail: [email protected]
There are little data on the relationship between Lewy body disease and mild cognitive impairment syndromes. The Mayo Clinic
aging and dementia databases in Rochester, Minnesota, and Jacksonville, Florida were queried for cases who were diagnosed
with mild cognitive impairment between 1 January 1996 and 30 April 2008, were prospectively followed and were subsequently
found to have autopsy-proven Lewy body disease. The presence of rapid eye movement sleep behaviour disorder was specif-
ically assessed. Mild cognitive impairment subtypes were determined by clinical impression and neuropsychological profiles,
based on prospective operational criteria. The diagnosis of clinically probable dementia with Lewy bodies was based on the
2005 McKeith criteria. Hippocampal volumes, rate of hippocampal atrophy, and proton magnetic resonance spectroscopy were
assessed on available magnetic resonance imaging and spectroscopy scans. Eight subjects were identified; six were male. Seven
developed dementia with Lewy bodies prior to death; one died characterized as mild cognitive impairment. The number of cases
and median age of onset (range) for specific features were: seven with rapid eye movement sleep behaviour disorder—60 years
(27–91 years), eight with cognitive symptoms—69 years (62–89 years), eight with mild cognitive impairment—70.5 years
(66–91 years), eight with parkinsonism symptoms—71 years (66–92 years), six with visual hallucinations—72 years (64–90
years), seven with dementia—75 years (67–92 years), six with fluctuations in cognition and/or arousal—76 years (68–92 years)
and eight dead—76 years (71–94 years). Rapid eye movement sleep behaviour disorder preceded cognitive symptom onset in six
cases by a median of 10 years (2–47 years) and mild cognitive impairment diagnosis by a median of 12 years (3–48 years). The
mild cognitive impairment subtypes represented include: two with single domain non-amnestic mild cognitive impairment, three
with multi-domain non-amnestic mild cognitive impairment, and three with multi-domain amnestic mild cognitive impairment.
The cognitive domains most frequently affected were attention and executive functioning, and visuospatial functioning.
Hippocampal volumes and the rate of hippocampal atrophy were, on average, within the normal range in the three cases
who underwent magnetic resonance imaging, and the choline/creatine ratio was elevated in the two cases who underwent
doi:10.1093/brain/awp280 Brain 2010: 133; 540–556 | 540
Received April 26, 2009. Revised August 26, 2009. Accepted September 13, 2009. Advance Access publication November 4, 2009
� The Author (2009). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved.
For Permissions, please email: [email protected]
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021

proton magnetic resonance spectroscopy when they were diagnosed as mild cognitive impairment. On autopsy, six had neo-
cortical-predominant Lewy body disease and two had limbic-predominant Lewy body disease; only one had coexisting high-
likelihood Alzheimer’s disease. These findings indicate that among Lewy body disease cases that pass through a mild cognitive
impairment stage, any cognitive pattern or mild cognitive subtype is possible, with the attention/executive and visuospatial
domains most frequently impaired. Hippocampal volume and proton magnetic resonance spectroscopy data were consistent with
recent data in dementia with Lewy bodies. All cases with rapid eye movement sleep behaviour disorder and mild cognitive
impairment were eventually shown to have autopsy-proven Lewy body disease, indicating that rapid eye movement sleep
behaviour disorder plus mild cognitive impairment probably reflects brainstem and cerebral Lewy body disease.
Keywords: mild cognitive impairment; dementia; dementia with Lewy bodies; Lewy body disease; neuropathology
Abbreviations: DRS = Mattis Dementia Rating Scale; REM = rapid eye movement
IntroductionMild cognitive impairment refers to the intermediate state between
normal ageing and dementia that was initially conceptualized
as a prodrome of Alzheimer’s disease. Subsequently, it has
been recognized that there are both amnestic and non-amnestic
forms of mild cognitive impairment. Patients with non-amnestic
mild cognitive impairment have deficits in the domains of language,
attention/executive functioning or visuospatial functioning. If mild
cognitive impairment is an intermediate state between normal
ageing and dementia, those with dementia due to other neuro-
degenerative aetiologies are also likely to pass through an mild
cognitive impairment state.
Dementia with Lewy bodies is a syndrome characterized by
dementia, plus at least two of the following features: (i) recurrent,
fully formed visual hallucinations; (ii) spontaneous parkinsonism;
and (iii) fluctuations in cognition and/or arousal (McKeith et al.,
2005). Neuropsychological data have shown that those with
dementia with Lewy bodies typically have impaired attention/
executive functioning and visuospatial skills (Salmon et al., 1996;
Ferman et al., 1999, 2002, 2006; Mori et al., 2000). Language
skills such as confrontation naming are often preserved (Ferman
et al., 2006), while performance on measures of learning and
memory is more variable. We hypothesized that patients with
a non-amnestic form of mild cognitive impairment, with impair-
ment in attention/executive functioning and/or visuospatial skills
would evolve to have other clinical features of dementia of Lewy
bodies and ultimately Lewy body disease on autopsy.
Rapid eye movement (REM) sleep behaviour disorder is a para-
somnia that is characterized by loss of normal skeletal muscle
atonia during REM sleep, with prominent motor activity and
dreaming (Schenck et al., 1986; Olson et al., 2000). REM sleep
behaviour disorder has been associated with synucleinopathies
such as dementia with Lewy bodies, Parkinson’s disease, multiple
system atrophy and pure autonomic failure, but is far less com-
monly associated with non-synucleinopathy disorders (Boeve
et al., 2001, 2003, 2007b; Iranzo et al., 2006; Postuma et al.,
2009). REM sleep behaviour disorder often precedes the onset of
cognitive impairment and/or parkinsonism by years or even dec-
ades (Schenck and Mahowald, 2002; Iranzo et al., 2006; Boeve
et al., 2007b; Postuma et al., 2009). We further hypothesized
that patients with mild cognitive impairment and REM sleep
behaviour disorder, regardless of the mild cognitive impairment
subtype, would represent prodromal Lewy body disease.
We characterized the clinical features, neuropsychological
profiles and structural neuroimaging patterns of those who were
diagnosed with mild cognitive impairment (any subtype), were
prospectively followed, and were subsequently found to have
autopsy-proven limbic or neocortical Lewy body disease.
Materials and methodsSubjects were identified through the combined databases of the
Alzheimer’s Disease Research Center at Mayo Clinic Rochester and
Mayo Clinic Jacksonville and the Alzheimer’s Disease Patient Registry
at Mayo Clinic Rochester. Both of these programmes are approved by
the Mayo Foundation Institutional Review Board. Written consent for
participation was provided by the subjects or their proxies. The data-
bases were queried to identify patients who were diagnosed with mild
cognitive impairment between 1 January 1996 and 30 April 2008,
were prospectively followed, and were subsequently found to have
autopsy-proven limbic- or neocortical-predominant Lewy body disease.
The clinical, neuropsychological, neuroimaging and neuropathological
features were analysed.
Clinical assessmentPatients were initially evaluated using a standardized clinical protocol
and followed prospectively. The same research protocol was com-
pleted at 12–15 month intervals, with additional evaluations in
between research assessments depending on active clinical issues. A
behavioural neurologist (B.B., D.K., R.P., N.G.R. or the late
Emre Kokmen) evaluated each patient by obtaining a medical history
from the patient and their corroborating sources and by performing a
complete neurological examination (Members of the Department of
Neurology, 1998). Features of parkinsonism (e.g. tremor, rigidity, bra-
dykinesia, postural instability, shuffling gait, masked facies, etc.) were
noted when present, and Parkinson’s disease was diagnosed if a
patient fulfilled United Kingdom Brain Bank criteria for the disorder
(Hughes et al., 1992). The Clinical Dementia Rating scale (Morris,
1993), Folstein Mini-Mental State Exam (Folstein et al., 1975),
and Kokmen Short Test of Mental Status (Kokmen et al., 1991;
Tang-Wai et al., 2003), were completed on all cases. The Mayo
Fluctuations Scale—a validated operationalized measure for determin-
ing the presence of fluctuations in cognition and/or arousal (Ferman
et al., 2004)—was completed by the informants. This scale has been
MCI-Lewy body disease Brain 2010: 133; 540–556 | 541
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021

used in the standard research protocol at our institution since it was
developed in 1999. Affirmative answers on at least three out of the
four questions were considered necessary for the presence of fluctua-
tions. All patients underwent a neuropsychological evaluation assessing
for memory, language, attention/executive functioning and visuospa-
tial functioning. Structural neuroimaging of the brain with magnetic
resonance imaging was performed in a subset of cases that were
having data acquired for volumetric magnetic resonance analyses
and magnetic resonance spectroscopic analyses.
Neuropsychological assessmentTesting included assessment of global cognitive functioning [Mattis
Dementia Rating Scale (DRS) (Mattis, 1988)]; learning and memory
[percent retention on immediate and delayed recall on the Logical
Memory subtest of the Weschler Memory Scale-Revised (Wechsler,
1987), learning over trials and percent retention on the Rey-
Auditory Verbal Learning Test (Rey, 1964)]; language functioning
[Boston Naming Test (Kaplan et al., 1978), Controlled Oral Word
Association Test (Benton and Hamsher, 1978), and category/semantic
fluency (animals, fruit, vegetables)]; attention/executive functioning
[Trail Making Test parts A and B (Reitan, 1958), and Digit Span of
the Wechsler Adult Intelligence Scale-Revised (Wechsler, 1981)]; and
visuospatial/perceptual functioning [Block Design and Picture
Completion subtests of the Wechsler Adult Intelligence Scale-
Revised, and copy of Rey-Osterreith Complex Figure (Rey, 1941;
Osterrieth, 1944)]. Additional tests were also administered and used
by the neuropsychologists in their assessments of individual patients.
Mayo Older American Normative Studies norms were used to deter-
mine scaled scores for these tests, in which 10 represents the mean
and the standard deviation is 3 (Ivnik et al., 1992, 1996, 1997; Lucas
et al., 1998a, b). Therefore, a Mayo Older American Normative
Studies scaled score of 7 is 1 SD below the mean and 4 is 2 SDs
below the mean.
Neuroimaging examinationsThree of the cases (Cases 3, 7 and 8) had MRI and two had1H-magnetic resonance spectroscopy (Cases 3 and 7) examinations
performed at the time they were diagnosed with mild cognitive
impairment. MRI was performed using a General Electric scanner at
1.5 Tesla, and images of the brain were obtained in the sagittal
(T1-weighted), axial (proton-density, T2-weighted and fluid attenua-
tion inversion recovery), and coronal (T1-weighted) planes.
Hippocampal volume measurements were derived from a
T1-weighted 3D volumetric spoiled gradient-recalled echo sequence
in the coronal plane by manually tracing their anatomic boundaries
for each image slice sequentially from posterior to anterior. Volumes
were adjusted for age, gender and head size; normal percentiles are
referred to as W scores, using age- and gender-specific normal per-
centiles based on a previous study (Jack et al., 2000). A value of zero
corresponds to the 50th percentile, +1.64 corresponds to the 95th
percentile, –1.64 corresponds to the 5th percentile among normal
subjects. The rate of change in hippocampal volumes was calculated
as the annualized percent change in hippocampal volume, which was
computed as the volume in cubic millimeters of scan 2 minus that of
scan 1 divided by volume on scan 1, divided by the duration (in years)
between the two scans (�100).
T1-weighted images in the sagittal plane were used for localizing the1H-magnetic resonance spectroscopy voxel. Point resolved spectros-
copy pulse sequence with repetition time/echo time = 2000/30 ms
was used for the examinations. An 8 cm3 (2 cm�2 cm�2cm) voxel,
prescribed on a mid-sagittal T1-weighted image, included right and left
posterior cingulate gyri and inferior precunei (Kantarci et al., 2000).
We quantified metabolite intensities by referencing to an internal stan-
dard, the creatine peak, to correct for coil loading, relaxation times
and inter subject differences in atrophy (i.e. partial volume averaging
of the magnetic resonance spectroscopy voxel).
Consensus diagnosisWeekly consensus meetings were held to review each patient’s
diagnosis. All information, including neurological, neuropsychological,
laboratory and imaging sources, were used. Subjects were diagnosed
as having normal cognition, mild cognitive impairment using published
criteria (Petersen, 2004), or dementia according to the Diagnostic and
Statistical Manual of Mental Disorders, revised third edition (1987).
The specific dementia diagnosis for Alzheimer’s disease, dementia
with Lewy bodies, frontotemporal dementia and other dementia
syndromes were made based on established criteria (McKhann et al.,
1984; Neary et al., 1998; McKeith et al., 2005).
For the diagnosis of mild cognitive impairment, subjects are required
to meet the following criteria: (i) a cognitive complaint, preferably
corroborated by an informant; (ii) essentially normal activities of
daily living; (iii) normal general cognitive functioning; (iv) abnormal
performance in one or more cognitive domains; and (v) not demented.
Impairment in cognitive domains was determined by neuropsycholo-
gical test scores; scores one SD below the mean (i.e. a Mayo Older
Adult Normative Scale Standard Score 47) were considered borderline
to clearly abnormal, but clinical impression based on these and other
tests scores and all other available information were also considered, as
is routine in clinical practice. Some tests can be abnormal and reflect
abnormalities in one and/or another domain (e.g. impaired perfor-
mance on the Controlled Oral Word Association Test can be due to
language and/or attention/executive dysfunction), again underscoring
the need for the clinical impression to be based on all data. Based on
the domains which were impaired, subjects were further classified as
having amnestic mild cognitive impairment, multiple-domain amnestic
mild cognitive impairment, single-domain non-amnestic mild cognitive
impairment and multiple-domain non-amnestic mild cognitive
impairment.
Neuropathologic assessmentAll cases underwent a standardized neuropathologic assessment, with
evaluation of gross and microscopic findings and analysis of Alzheimer-
type pathology, Lewy body pathology, cerebrovascular pathology and
concomitant pathology according to established and published guide-
lines (Braak and Braak, 1997; Fujishiro et al., 2008). Sections were
taken from six regions of the cortex, hippocampus, amygdala, basal
ganglia, thalamus, midbrain, pons, medulla and cerebellum. Counts of
senile plaques and neurofibrillary tangles were made in six cortical
sections, four sectors of the hippocampus, two regions of the amyg-
dala, and the basal nucleus of Meynert with thioflavin-S fluorescent
and/or Bielschowsky microscopy. The presence of amyloid angiopathy
was assessed. Senile plaques and neurofibrillary tangles were counted
at �100 and �400, respectively, in cortex, hippocampus and amyg-
dale. A Braak neurofibrillary tangle stage (Braak and Braak, 1991) was
assigned to all cases based on the distribution of neurofibrillary tangles
with thioflavin-S fluorescent microscopy, as previously described (Togo
et al., 2002; Josephs et al., 2004). The severity of senile plaque
pathology was also assessed using the Consortium to Establish a
Registry for Alzheimer Disease guidelines (Mirra et al., 1991). All
cases underwent immunostaining with a monoclonal antibody to
542 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021

phospho-tau (CP13 [24]; Peter Davies, Albert Einstein College of
Medicine, Bronx, NY) and a polyclonal antibody to �-synuclein
(Gwinn-Hardy et al., 2000) using immunostaining with a Dako
Autostainer. The subtypes of Lewy body pathology (i.e. brainstem,
limbic/transitional, or neocortical/diffuse) were determined based on
Lewy body counts in five cortical sections and the amygdala.
Semiquantitative grading of Lewy body pathology and assignment of
Lewy body type were also determined according to recommendations
from the Third Consortium of Dementia with Lewy Bodies (McKeith
et al., 2005). The two methods gave similar results. The Lewy body
density was determined at �200 magnification from the following
regions: middle frontal (Brodmann area 46), superior temporal
(Brodmann area 38), inferior parietal (Brodmann area 39), anterior
cingulate (Brodmann area 24) and parahippocampal gyri (Brodmann
area 35). The recently published and validated Dementia with Lewy
Bodies Consensus criteria for the diagnosis of Lewy body disease was
used to characterize cases (Fujishiro et al., 2008).
Cerebrovascular pathology was assessed in all cases using
a semiquantitative scale similar to that previously reported (Jellinger
and Attems, 2003). Briefly, cases with no cerebrovascular lesions were
scored 0, those with minimal cerebrovascular pathology (including one
to two small lacunes, mild cerebral amyloid angiopathy or mild leu-
koencephalopathy) were scored 1, those with moderate lesions
(including more than 2 lacunes, severe cerebral amyloid angiopathy,
or diffuse leukoencephalopathy) were scored as 2, and those with
marked cerebrovascular pathology (including old cortical infarcts, mul-
tiple microinfarcts or hippocampal sclerosis) were scored 3.
Concomitant pathologies were noted when present. Argyrophilic
grains, neuronal threads, oligodendroglial coiled bodies, astrocytic pla-
ques and globose neurofibrillary tangles were assessed using monoclo-
nal antibody to phospho-tau (CP13). Glial intracytoplasmic inclusions
were assessed by �-synuclein immunohistochemistry.
The final neuropathologic diagnosis was made according to the
Dementia with Lewy Body Consensus criteria for the diagnosis
of Lewy body disease (Fujishiro et al., 2008; McKeith et al., 2005)
and the National Institute on Aging-Reagan criteria for Alzheimer’s
disease (Consensus recommendations for the post mortem diagnosis
of Alzheimer’s disease, 1997).
Results
Clinical and neuropsychological dataEight patients were identified. All had an education level of 10
years or greater, and six of the patients were male. The demo-
graphic and clinical features are indicated in Table 1, and the
neuropathologic findings are shown in Table 2. Narrative descrip-
tions of each patient’s clinical course are in Supplementary Text
E1, and the longitudinal clinical data and neuropsychological
profile of impairment at the time of mild cognitive impairment
diagnosis for each patient are shown in the Figures 1–8.
Neuroimaging dataQuantitative neuroimaging data were available in a subset of
cases. In the three cases who underwent serial magnetic reso-
nance imaging exams, baseline hippocampal volumes at the time
of mild cognitive impairment diagnosis and the rate of hippocam-
pal atrophy at follow-up were on average within the range of the
cognitively normal subjects, when compared to previously
published data (Jack et al., 2000). In two of the cases who under-
went baseline 1H-magnetic resonance spectroscopy exams, the
choline/creatine ratio and myoinositol/creatine ratio were elevated
in both cases, and the n-acetyl aspartate/creatine ratio was
decreased in one of the cases compared to previously published
data (Kantarci et al., 2000).
Summary of longitudinalante-mortem dataSeven patients’ condition declined and they experienced other
symptoms and received a diagnosis of clinically probable dementia
with Lewy bodies prior to death; one patient died while classified
as mild cognitive impairment. All patients had a Clinical Dementia
Rating score of 0.5 at the time of the mild cognitive impairment
diagnosis. The median age of cognitive symptoms onset was 69
years (range 61–89 years), mild cognitive impairment diagnosis
was 70.5 years (range 66–91 years), and dementia onset was
78 (range 67–90 years), with a median Clinical Dementia Rating
score of 2 (range 1–3). Mini-Mental State Examination data were
available for all patients when initially diagnosed with mild
cognitive impairment; the median Mini-Mental State Examination
score was 28 (range 23–29).The median number of years between
the onset of cognitive symptoms and dementia was 4 years (range
2–6 years) and between the onset of mild cognitive impairment and
dementia was 2.5 years (range 1–5 years). The median number of
years from a diagnosis of mild cognitive impairment onset to death
was 6.5 years (range 5–9 years). Among the seven patients who
developed dementia, the median number of years from dementia
onset to death was 3 years (range 0–4 years).
In this cohort, both amnestic mild cognitive impairment and
non-amnestic mild cognitive impairment subtypes were
represented, including three with multi-domain amnestic mild
cognitive impairment, three with multi-domain non-amnestic
mild cognitive impairment and two with single-domain non-
amnestic mild cognitive impairment. Attention/executive function-
ing (n = 6) and visuospatial functioning (n = 6) were the cognitive
domains most frequently affected.
Seven patients had REM sleep behaviour disorder with a median
onset age of 60 years (range 27–91 years). Polysomnogram was
performed in four cases, in whom REM sleep behaviour disorder
was confirmed in all. The onset of REM sleep behaviour disorder
features preceded onset of cognitive symptoms in six patients by
a median of 10 years (range 2–47 years) and mild cognitive
impairment diagnosis by of 12 years (range 3–48 years). One
patient developed REM sleep behaviour disorder 2 years after
the onset of cognitive symptoms and at the same time as the
diagnosis of mild cognitive impairment.
Six patients had visual hallucinations, with a median onset age
of 72 years (range 64–90 years). Among these patients, five
developed hallucinations at a median of 3 years after the onset
of cognitive symptoms (range 1–4 years); one patient developed
hallucinations 3 years prior to the onset of cognitive impairment.
Seven patients had parkinsonism, with a median onset age of 71
years (range 71–92 years). In five patients, parkinsonism occurred
MCI-Lewy body disease Brain 2010: 133; 540–556 | 543
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
at a median of 3 years after onset of cognitive symptoms (range
2–5 years). Two patients developed parkinsonism at the same time
as cognitive symptoms onset, and one patient developed
parkinsonism 1 year prior to onset of cognitive symptoms. None
of the patients fulfilled criteria for the diagnosis of Parkinson’s
disease prior to the onset of dementia.
Fluctuations were classified as present in six patients based on
Mayo Fluctuations Scale data, with a median onset age of 76 years
(range 68–92 years). Fluctuations evolved after onset of cognitive
symptoms in all six cases, at a median of 4.5 years (range
3–6 years). Mayo Fluctuations Scale data were not available in
one patient who died prior to the development of the scale;
however, the clinical notes did not suggest the presence of
fluctuations.
All three core features of dementia with Lewy bodies eventually
developed in five patients. Both patients with two core features
had spontaneous parkinsonism. The patient who died with a clas-
sification of mild cognitive impairment had parkinsonism and REM
sleep behaviour disorder, but no hallucinations or fluctuations.
Visual hallucinations and fluctuations tended to occur after the
onset of cognitive impairment at a median of 3 and 4.5 years,
respectively. Parkinsonism tended to manifest after the onset of
cognitive symptoms, though also did occur before and at the same
time as the cognitive symptoms onset in a few patients. Seven
patients had clinical evidence of REM sleep behaviour disorder,
with six patients having dream enactment behaviour preceding
the onset of mild cognitive impairment.
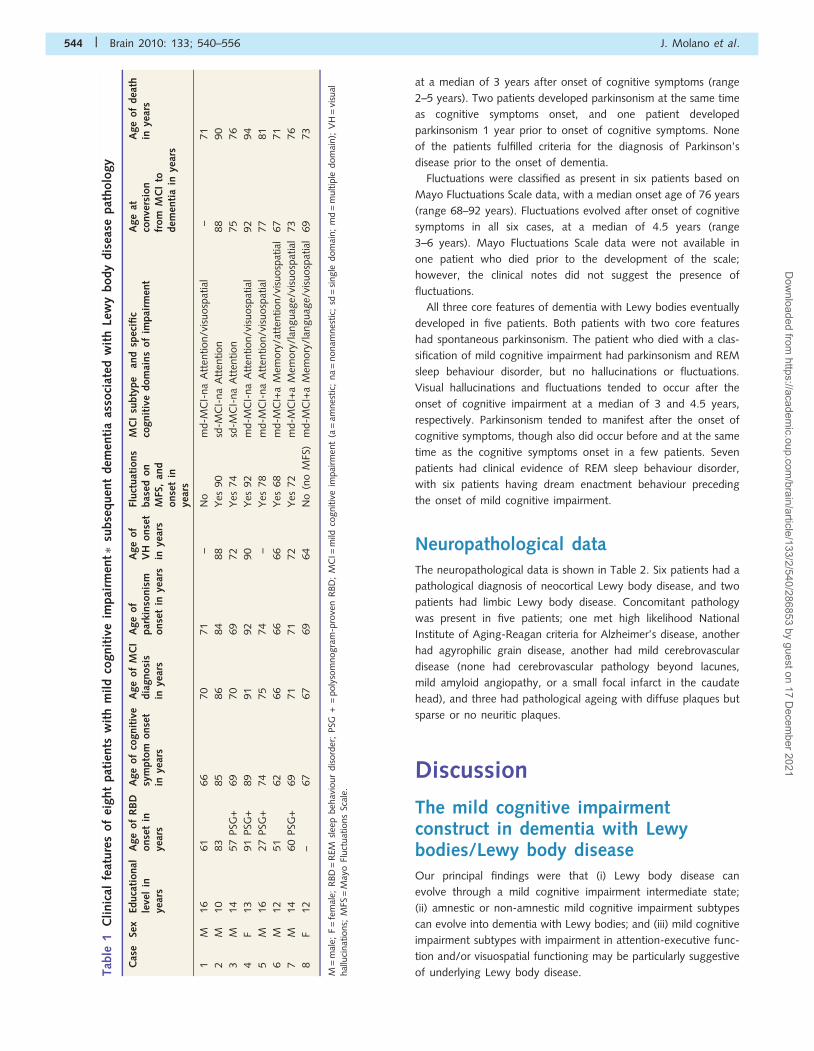
Neuropathological dataThe neuropathological data is shown in Table 2. Six patients had a
pathological diagnosis of neocortical Lewy body disease, and two
patients had limbic Lewy body disease. Concomitant pathology
was present in five patients; one met high likelihood National
Institute of Aging-Reagan criteria for Alzheimer’s disease, another
had agyrophilic grain disease, another had mild cerebrovascular
disease (none had cerebrovascular pathology beyond lacunes,
mild amyloid angiopathy, or a small focal infarct in the caudate
head), and three had pathological ageing with diffuse plaques but
sparse or no neuritic plaques.
Discussion
The mild cognitive impairmentconstruct in dementia with Lewybodies/Lewy body diseaseOur principal findings were that (i) Lewy body disease can
evolve through a mild cognitive impairment intermediate state;
(ii) amnestic or non-amnestic mild cognitive impairment subtypes
can evolve into dementia with Lewy bodies; and (iii) mild cognitive
impairment subtypes with impairment in attention-executive func-
tion and/or visuospatial functioning may be particularly suggestive
of underlying Lewy body disease.Tab
le1
Cli
nic
alfe
ature
sof
eight
pat
ients
wit
hm
ild
cognit
ive
impai
rmen
t�su
bse
quen
tdem
enti
aas
soci
ated
wit
hLe
wy
body
dis
ease
pat
holo
gy
Cas
eSe
xEd
uca
tional
leve
lin
year
s
Age
of
RB
Donse
tin
year
s
Age
of
cognit
ive
sym
pto
monse
tin
year
s
Age
of
MC
Idia
gnosi
sin
year
s
Age
of
par
kinso
nis
monse
tin
year
s
Age
of
VH
onse
tin
year
s
Fluct
uat
ions
bas
edon
MFS
,an
donse
tin
year
s
MC
Isu
bty
pe
and
spec
ific
cognit
ive
dom
ains
of
impai
rmen
tA
ge
atco
nve
rsio
nfr
om
MC
Ito
dem
enti
ain
year
s
Age
of
dea
thin
year
s
1M
16
61
66
70
71
–N
om
d-M
CI-
na
Att
ention/v
isuosp
atia
l–
71
2M
10
83
85
86
84
88
Yes
90
sd-M
CI-
na
Att
ention
88
90
3M
14
57
PSG
+69
70
69
72
Yes
74
sd-M
CI-
na
Att
ention
75
76
4F
13
91
PSG
+89
91
92
90
Yes
92
md-M
CI-
na
Att
ention/v
isuosp
atia
l92
94
5M
16
27
PSG
+74
75
74
–Y
es78
md-M
CI-
na
Att
ention/v
isuosp
atia
l77
81
6M
12
51
62
66
66
66
Yes
68
md-M
CI+
aM
emory
/att
ention/v
isuosp
atia
l67
71
7M
14
60
PSG
+69
71
71
72
Yes
72
md-M
CI+
aM
emory
/lan
guag
e/vi
suosp
atia
l73
76
8F
12
–67
67
69
64
No
(no
MFS
)m
d-M
CI+
aM
emory
/lan
guag
e/vi
suosp
atia
l69
73
M=
mal
e;F
=fe
mal
e;R
BD
=R
EMsl
eep
beh
avio
ur
dis
ord
er;
PSG
+=
poly
som
nogra
m-p
rove
nR
BD
;M
CI=
mild
cognitiv
eim
pai
rmen
t(a
=am
nes
tic;
na
=nonam
nes
tic;
sd=
single
dom
ain;
md
=m
ultip
ledom
ain);
VH
=vi
sual
hal
luci
nat
ions;
MFS
=M
ayo
Fluct
uat
ions
Scal
e.
544 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
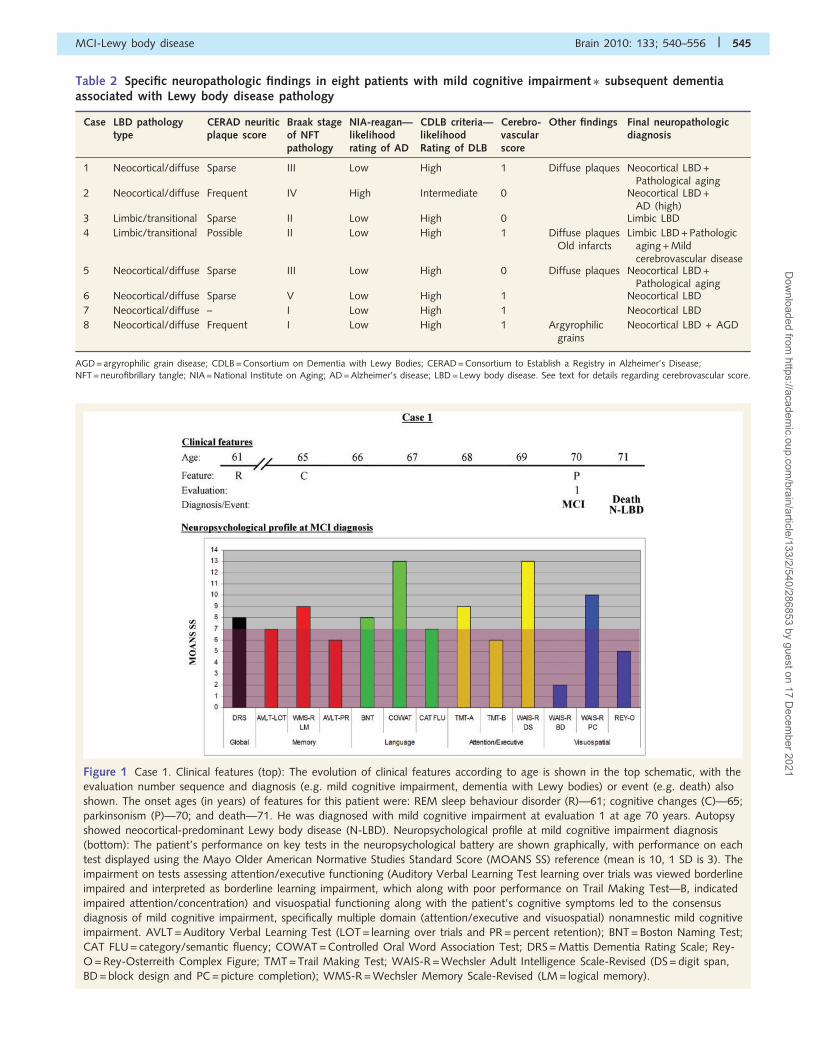
Figure 1 Case 1. Clinical features (top): The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: REM sleep behaviour disorder (R)—61; cognitive changes (C)—65;
parkinsonism (P)—70; and death—71. He was diagnosed with mild cognitive impairment at evaluation 1 at age 70 years. Autopsy
showed neocortical-predominant Lewy body disease (N-LBD). Neuropsychological profile at mild cognitive impairment diagnosis
(bottom): The patient’s performance on key tests in the neuropsychological battery are shown graphically, with performance on each
test displayed using the Mayo Older American Normative Studies Standard Score (MOANS SS) reference (mean is 10, 1 SD is 3). The
impairment on tests assessing attention/executive functioning (Auditory Verbal Learning Test learning over trials was viewed borderline
impaired and interpreted as borderline learning impairment, which along with poor performance on Trail Making Test—B, indicated
impaired attention/concentration) and visuospatial functioning along with the patient’s cognitive symptoms led to the consensus
diagnosis of mild cognitive impairment, specifically multiple domain (attention/executive and visuospatial) nonamnestic mild cognitive
impairment. AVLT = Auditory Verbal Learning Test (LOT = learning over trials and PR = percent retention); BNT = Boston Naming Test;
CAT FLU = category/semantic fluency; COWAT = Controlled Oral Word Association Test; DRS = Mattis Dementia Rating Scale; Rey-
O = Rey-Osterreith Complex Figure; TMT = Trail Making Test; WAIS-R = Wechsler Adult Intelligence Scale-Revised (DS = digit span,
BD = block design and PC = picture completion); WMS-R = Wechsler Memory Scale-Revised (LM = logical memory).
Table 2 Specific neuropathologic findings in eight patients with mild cognitive impairment� subsequent dementiaassociated with Lewy body disease pathology
Case LBD pathologytype
CERAD neuriticplaque score
Braak stageof NFTpathology
NIA-reagan—likelihoodrating of AD
CDLB criteria—likelihoodRating of DLB
Cerebro-vascularscore
Other findings Final neuropathologicdiagnosis
1 Neocortical/diffuse Sparse III Low High 1 Diffuse plaques Neocortical LBD +Pathological aging
2 Neocortical/diffuse Frequent IV High Intermediate 0 Neocortical LBD +AD (high)
3 Limbic/transitional Sparse II Low High 0 Limbic LBD
4 Limbic/transitional Possible II Low High 1 Diffuse plaquesOld infarcts
Limbic LBD + Pathologicaging + Mildcerebrovascular disease
5 Neocortical/diffuse Sparse III Low High 0 Diffuse plaques Neocortical LBD +Pathological aging
6 Neocortical/diffuse Sparse V Low High 1 Neocortical LBD
7 Neocortical/diffuse – I Low High 1 Neocortical LBD
8 Neocortical/diffuse Frequent I Low High 1 Argyrophilicgrains
Neocortical LBD + AGD
AGD = argyrophilic grain disease; CDLB = Consortium on Dementia with Lewy Bodies; CERAD = Consortium to Establish a Registry in Alzheimer’s Disease;NFT = neurofibrillary tangle; NIA = National Institute on Aging; AD = Alzheimer’s disease; LBD = Lewy body disease. See text for details regarding cerebrovascular score.
MCI-Lewy body disease Brain 2010: 133; 540–556 | 545
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
Results from previous research have shown that those who
died with an amnestic mild cognitive impairment subtype
(n = 15) may have some degree of medial temporal lobe changes
in essentially every case (e.g. neurofibrillary tangles, argyrophilic
grain disease, hippocampal sclerosis, etc), with only a few
meeting criteria for fully expressed Alzheimer’s disease (Petersen
et al., 2006). While data in those who evolved from amnestic
mild cognitive impairment to dementia did show that most met
criteria for Alzheimer’s disease (Jicha et al., 2006), a minority of
patients had other pathological diagnoses (note the single case
with Lewy body disease pathology in that series was not included
in the current series of eight cases as she developed dementia
prior to 1996). Three of the patients in our series had an amnes-
tic mild cognitive impairment subtype and Lewy body disease on
autopsy. Though it has been suggested that all cases of amnestic
mild cognitive impairment reflect evolving Alzheimer’s disease
(Morris et al., 2001; Dubois and Albert, 2004; Sarazin
et al., 2007), our findings suggest that the neuropathological
substrate for amnestic mild cognitive impairment is more
heterogeneous.
The cognitive domains most frequently affected in the mild
cognitive impairment of dementia with Lewy bodies were atten-
tion/executive functioning and visuospatial functioning. Moreover,
seven patients had a history of dream enactment behaviour during
sleep, even if it was no longer an active problem. Our experience
suggests that patients with a history of dream enactment
behaviour during sleep who present with attention/executive
and/or visuospatial difficulty despite preserved complex activities
of daily living may represent underlying Lewy body disease.
Indeed, seven of the eight patients were followed longitudinally
and eventually developed a dementia and corresponding core
clinical features of dementia with Lewy bodies.
Several of the subjects in this series were relatively easy to char-
acterize, with clear cognitive complaints that were corroborated by
their informants and neuropsychological features that permitted a
straight-forward determination of which domains were impaired.
However, the neuropsychological features of mild cognitive
impairment associated with Lewy body disease are variable.
Determining which domains are impaired and classifying them
into a specific mild cognitive impairment subtype can be
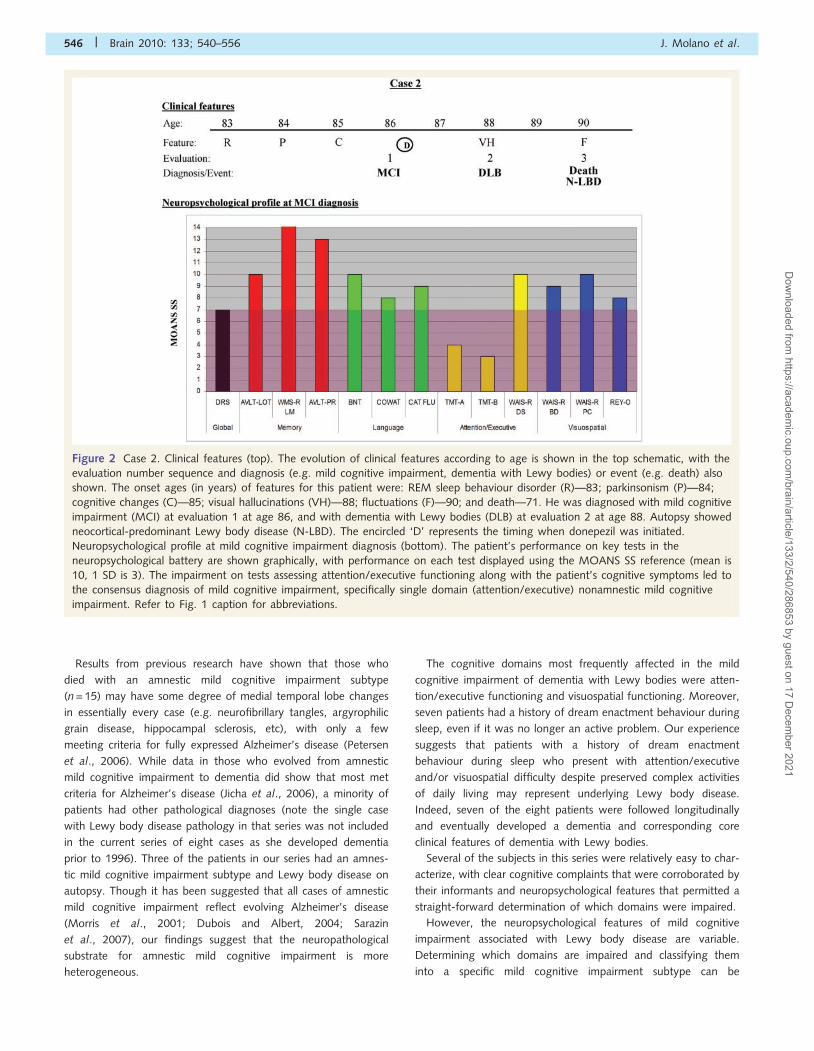
Figure 2 Case 2. Clinical features (top). The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: REM sleep behaviour disorder (R)—83; parkinsonism (P)—84;
cognitive changes (C)—85; visual hallucinations (VH)—88; fluctuations (F)—90; and death—71. He was diagnosed with mild cognitive
impairment (MCI) at evaluation 1 at age 86, and with dementia with Lewy bodies (DLB) at evaluation 2 at age 88. Autopsy showed
neocortical-predominant Lewy body disease (N-LBD). The encircled ‘D’ represents the timing when donepezil was initiated.
Neuropsychological profile at mild cognitive impairment diagnosis (bottom). The patient’s performance on key tests in the
neuropsychological battery are shown graphically, with performance on each test displayed using the MOANS SS reference (mean is
10, 1 SD is 3). The impairment on tests assessing attention/executive functioning along with the patient’s cognitive symptoms led to
the consensus diagnosis of mild cognitive impairment, specifically single domain (attention/executive) nonamnestic mild cognitive
impairment. Refer to Fig. 1 caption for abbreviations.
546 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
challenging in some patients. Case 3 exemplifies this challenge, as
he repeatedly voiced concerns over his cognitive symptoms and
used notes obsessively, yet his performance on neuropsychological
testing over the initial 4 years of his symptoms was normal or only
mild impaired. Even on testing just prior to the diagnosis of
dementia with Lewy bodies, performance was in the average
range across most tests. To what degree this represents cognitive
fluctuations, or the ability of some patients to ‘rise to the occasion’
and perform better than expected on formal testing despite florid
symptoms and modest functional changes, is unclear. This case
also underscores that not all patients who voice strong cognitive
concerns yet perform normally on neuropsychological testing are
‘worried well’; indeed, this patient had autopsy-proven Lewy body
disease.
We again emphasize the need to incorporate all clinical and
neuropsychological data when making determinations on mild
cognitive impairment diagnoses; following a strict algorithmic
approach to interpreting neuropsychological data does not capture
the complexity of some cases. On the other hand, it may be
argued that the more impaired multi-domain mild cognitive
impairment cases may have been much closer to a diagnosis of
dementia than those with more restricted patterns of cognitive
difficulty. Nonetheless, adamant assurances from family members
that their activities of daily living continued to be unchanged at
the time of the evaluation warranted that a diagnosis of mild
cognitive impairment be made, rather than dementia. In either
case, the family’s observations are critically important when
making a determination of functional status. As noted in the
‘Methods’ section, many of the tests included in the study
cannot be completely compartmentalized to a single cognitive
domain, so poor performance on some tests can be interpreted
as reflecting impairment in more than one domain. Also, we
purposefully gave more weight to delayed recall than immediate
recall of paragraph material, given data that shows delayed recall
is a useful discriminator of Alzheimer’s disease from dementia with
Lewy bodies (Ferman et al., 2006), realizing that results on
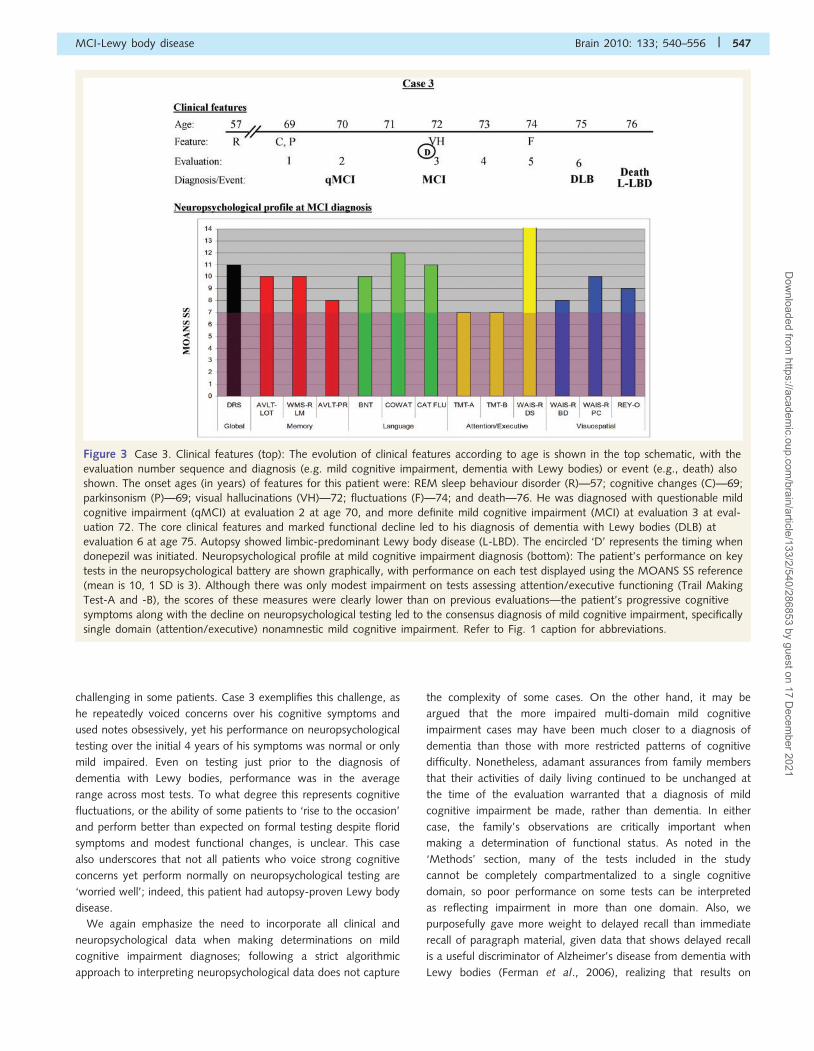
Figure 3 Case 3. Clinical features (top): The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g., death) also
shown. The onset ages (in years) of features for this patient were: REM sleep behaviour disorder (R)—57; cognitive changes (C)—69;
parkinsonism (P)—69; visual hallucinations (VH)—72; fluctuations (F)—74; and death—76. He was diagnosed with questionable mild
cognitive impairment (qMCI) at evaluation 2 at age 70, and more definite mild cognitive impairment (MCI) at evaluation 3 at eval-
uation 72. The core clinical features and marked functional decline led to his diagnosis of dementia with Lewy bodies (DLB) at
evaluation 6 at age 75. Autopsy showed limbic-predominant Lewy body disease (L-LBD). The encircled ‘D’ represents the timing when
donepezil was initiated. Neuropsychological profile at mild cognitive impairment diagnosis (bottom): The patient’s performance on key
tests in the neuropsychological battery are shown graphically, with performance on each test displayed using the MOANS SS reference
(mean is 10, 1 SD is 3). Although there was only modest impairment on tests assessing attention/executive functioning (Trail Making
Test-A and -B), the scores of these measures were clearly lower than on previous evaluations—the patient’s progressive cognitive
symptoms along with the decline on neuropsychological testing led to the consensus diagnosis of mild cognitive impairment, specifically
single domain (attention/executive) nonamnestic mild cognitive impairment. Refer to Fig. 1 caption for abbreviations.
MCI-Lewy body disease Brain 2010: 133; 540–556 | 547
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
immediate recall are also similarly different between mild cognitive
impairment associated with Alzheimer’s disease pathology com-
pared with that associated with Lewy body disease pathology
(Jicha et al., 2008).
The neuroimaging features of mildcognitive impairment associated withLewy body diseaseOur observations should be considered preliminary since we had
structural MRI on only three subjects and 1H-magnetic resonance
spectroscopy on only two. Hippocampal volumes and atrophy
rates were within the normal range of values in all three of the
mild cognitive impairment cases. This result is consistent with
results from studies of patients who have dementia with Lewy
bodies, in whom hippocampal volumes are notably larger than
patients with Alzheimer’s disease (Whitwell et al., 2007).1H-magnetic resonance spectroscopy analysis showed significantly
elevated choline/creatine ratios in the two mild cognitive
impairment cases we studied. Dementia with Lewy body patients
are characterized by significantly elevated choline/creatine ratios,
which tend to be higher than the choline/creatine elevation in
patients with Alzheimer’s disease (Kantarci et al., 2004).
Although the number of subjects with 1H-magnetic resonance
imaging was very small, our results in mild cognitive impairment
are consistent with those of dementia with Lewy bodies.
The early characterization andevolution of clinical featuresThis series is small, but a relatively consistent evolution of clinical
features occurred. All but one had REM sleep behaviour disorder
preceding the onset of mild cognitive impairment, and most devel-
oped parkinsonism concurrently or after the onset of their cogni-
tive symptoms. None of these patients fulfilled criteria for
Parkinson’s disease prior to the onset of cognitive symptoms,
nor during their phase of mild cognitive impairment; and hence
none could be considered as representing Parkinson’s disease with
dementia. Visual hallucinations tended to evolve after both
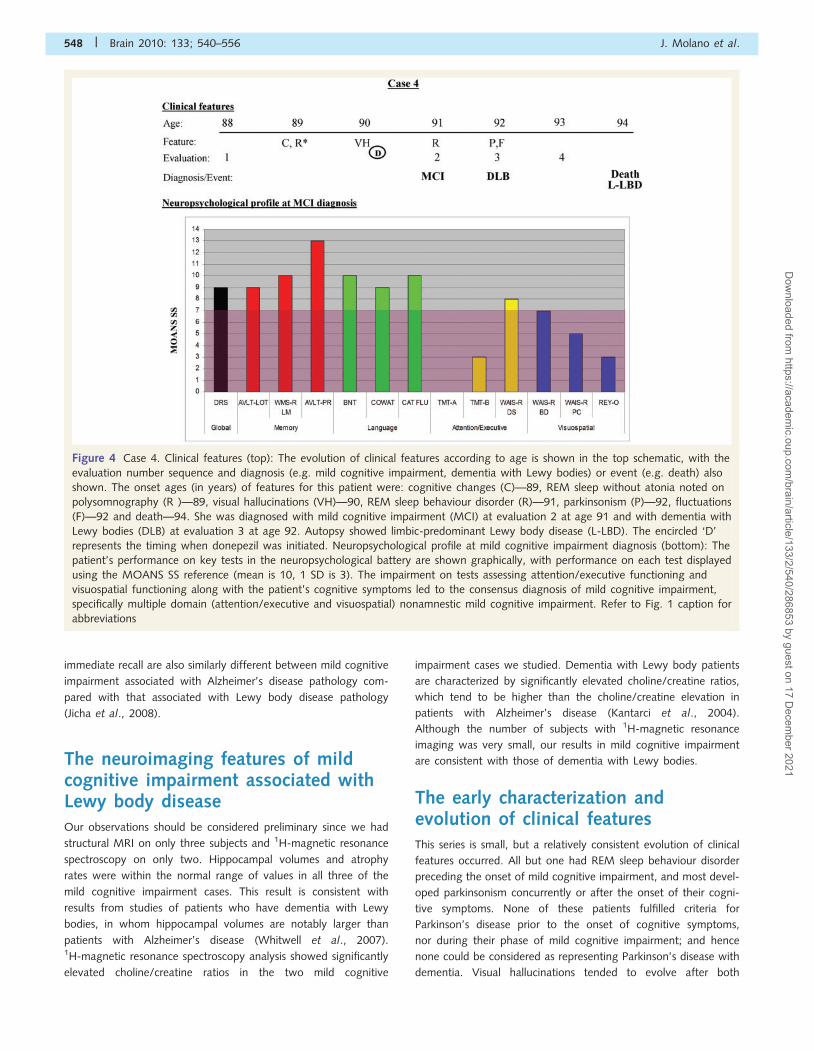
Figure 4 Case 4. Clinical features (top): The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: cognitive changes (C)—89, REM sleep without atonia noted on
polysomnography (R�)—89, visual hallucinations (VH)—90, REM sleep behaviour disorder (R)—91, parkinsonism (P)—92, fluctuations
(F)—92 and death—94. She was diagnosed with mild cognitive impairment (MCI) at evaluation 2 at age 91 and with dementia with
Lewy bodies (DLB) at evaluation 3 at age 92. Autopsy showed limbic-predominant Lewy body disease (L-LBD). The encircled ‘D’
represents the timing when donepezil was initiated. Neuropsychological profile at mild cognitive impairment diagnosis (bottom): The
patient’s performance on key tests in the neuropsychological battery are shown graphically, with performance on each test displayed
using the MOANS SS reference (mean is 10, 1 SD is 3). The impairment on tests assessing attention/executive functioning and
visuospatial functioning along with the patient’s cognitive symptoms led to the consensus diagnosis of mild cognitive impairment,
specifically multiple domain (attention/executive and visuospatial) nonamnestic mild cognitive impairment. Refer to Fig. 1 caption for
abbreviations
548 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
cognitive impairment and parkinsonism, and fluctuations, at least
as measured by the Mayo Fluctuations Scale (Ferman et al.,
2004), tended to be the final core feature to evolve. Dementia
onset along with two or more of the other core features led to
the diagnosis of clinically probable dementia with Lewy bodies
2–6 years after a diagnosis of mild cognitive impairment was
made. These data are consistent with prior work that has
shown that dementia plus REM sleep behaviour disorder in the
absence of other core features of dementia with Lewy bodies
probably reflects underlying Lewy body disease (Ferman et al.,
2002).
There were exceptions to the evolution of features noted above.
One patient initially experienced recurrent fully formed visual
hallucinations and was thought to have Charles–Bonnet syndrome
due to the absence of any other neurological signs or symptoms.
The hallucinations spontaneously remitted but were followed
3 years later by cognitive decline, with the hallucinations returning
years later. Another patient complained vehemently about his
memory problems, urinary incontinence and erectile dysfunction,
though neuropsychological performance early in his course was
minimally abnormal. And one patient underwent a polysomno-
gram to evaluate obstructive sleep apnoea as a possible con-
tributor to her cognitive symptoms. While REM sleep without
atonia—the electrophysiologic substrate for REM sleep behaviour
disorder—was evident on her polysomnogram, she did not begin
exhibiting recurrent dream enactment behaviour until 2 years
later.
In addition, it may be challenging to elicit a history of fluctua-
tions in a clinical setting. For this study, the Mayo Fluctuations
Scale was used to operationalize a more consistent determination
of fluctuations. Asking whether the patient fluctuates does not
distinguish dementia with Lewy bodies from Alzheimer’s disease
(Ferman et al., 2004). In order to make more definitive general-
izations about the early characteristics and evolution of dementia
with Lewy bodies/Lewy body disease, more subjects need to be
assessed in a comprehensive manner and followed longitudinally
using scales that adequately capture the concept of fluctuations in
cognition and/or arousal.
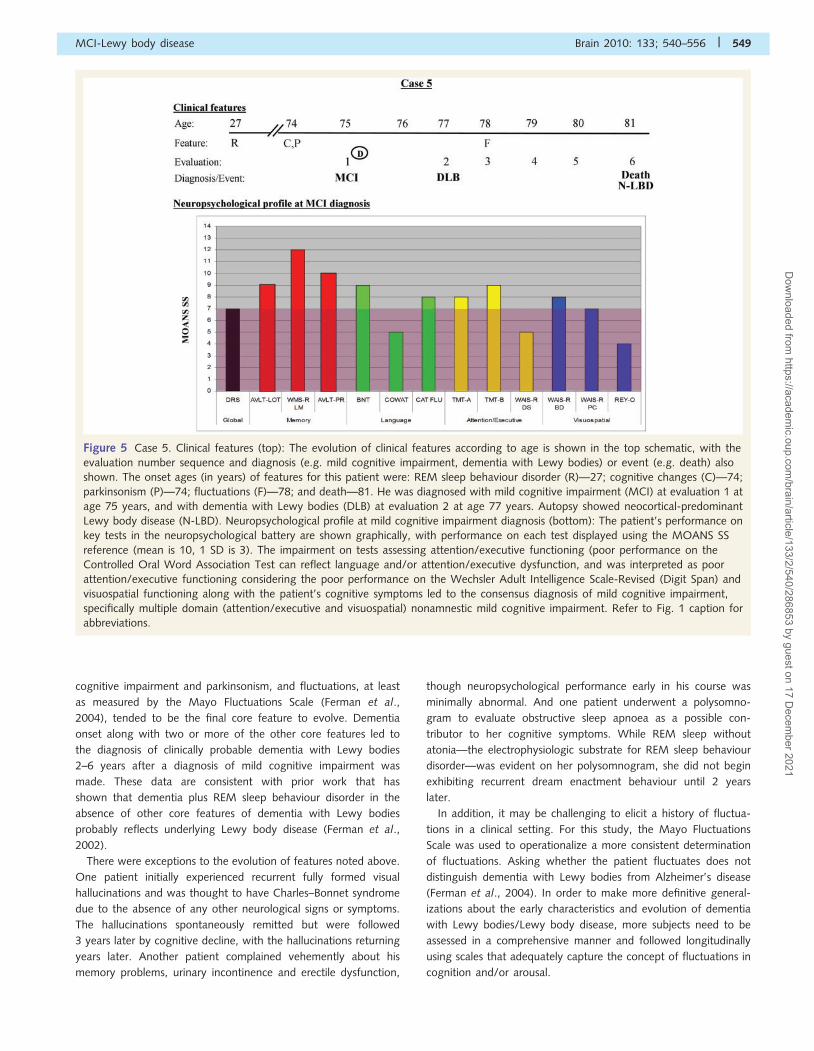
Figure 5 Case 5. Clinical features (top): The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: REM sleep behaviour disorder (R)—27; cognitive changes (C)—74;
parkinsonism (P)—74; fluctuations (F)—78; and death—81. He was diagnosed with mild cognitive impairment (MCI) at evaluation 1 at
age 75 years, and with dementia with Lewy bodies (DLB) at evaluation 2 at age 77 years. Autopsy showed neocortical-predominant
Lewy body disease (N-LBD). Neuropsychological profile at mild cognitive impairment diagnosis (bottom): The patient’s performance on
key tests in the neuropsychological battery are shown graphically, with performance on each test displayed using the MOANS SS
reference (mean is 10, 1 SD is 3). The impairment on tests assessing attention/executive functioning (poor performance on the
Controlled Oral Word Association Test can reflect language and/or attention/executive dysfunction, and was interpreted as poor
attention/executive functioning considering the poor performance on the Wechsler Adult Intelligence Scale-Revised (Digit Span) and
visuospatial functioning along with the patient’s cognitive symptoms led to the consensus diagnosis of mild cognitive impairment,
specifically multiple domain (attention/executive and visuospatial) nonamnestic mild cognitive impairment. Refer to Fig. 1 caption for
abbreviations.
MCI-Lewy body disease Brain 2010: 133; 540–556 | 549
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
Implications of the presence andevolution of clinical features onthe topography of degenerationin Lewy body diseaseA clinical feature or sign in neurodegenerative disease reflects
sufficient neuronal/glial/neurotransmitter dysfunction in a critical
neuronal network. While some of these features or signs have
known or suspected networks of dysfunction, the underlying
substrate for other features or signs is less clear. Parkinsonism is
most likely to be associated with dopaminergic depletion due
to sufficient degeneration in the nigrostriatal system, and cognitive
impairment is likely to be associated, at least in part, with choli-
nergic depletion due to basal forebrain/limbic system/neocortex
degeneration. It is highly likely that REM sleep behaviour dis-
order reflects sufficient degeneration in brainstem networks,
although the precise structures have yet to be identified in
humans (for review, see Boeve et al., 2007b). The underlying
pathology of visual hallucinations and fluctuations is not well
understood.
The evolution of clinical features must reflect the topography of
degeneration over time. Many of our patients tended to experi-
ence REM sleep behaviour disorder prior to cognitive impairment,
with subsequent development of parkinsonism. This evolution sug-
gests that dysfunction in the pontomedullary circuitry precedes
dysfunction in the basal forebrain, limbic system and neocortical
circuitry. Dysfunction in the nigrostratial circuitry appears to occur
subsequently. One could argue that this evolution of features and
presumed pathophysiologic basis does not support the Braak
staging scheme (Braak et al., 2003, 2004) of Parkinson’s disease
(Burke et al., 2008), yet it may provide some clues into Lewy
body disease pathology of the dementia with Lewy bodies
phenotype.
A ‘bottom-to-top’ or ascending progression of Lewy neurites,
Lewy bodies and neuronal degeneration as proposed in Stages 1–6
of the Braak scheme explains the evolution of features in typical
Parkinson’s disease quite well (Braak et al., 2003, 2004) but is
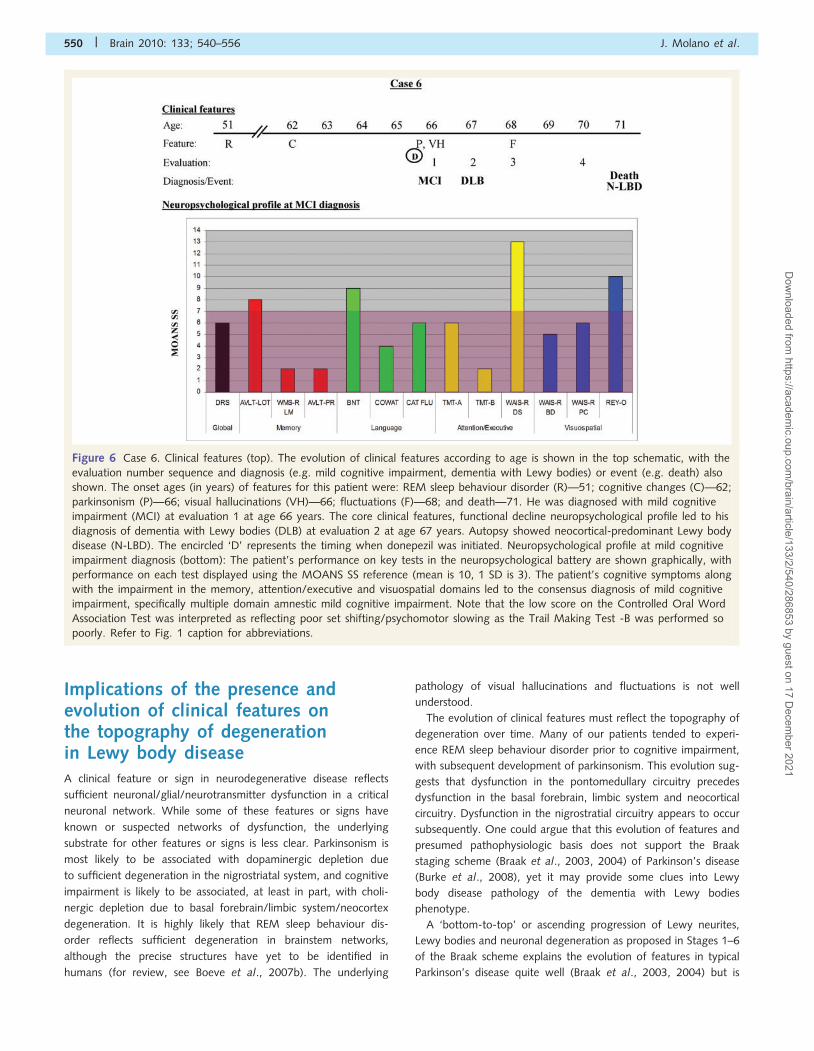
Figure 6 Case 6. Clinical features (top). The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: REM sleep behaviour disorder (R)—51; cognitive changes (C)—62;
parkinsonism (P)—66; visual hallucinations (VH)—66; fluctuations (F)—68; and death—71. He was diagnosed with mild cognitive
impairment (MCI) at evaluation 1 at age 66 years. The core clinical features, functional decline neuropsychological profile led to his
diagnosis of dementia with Lewy bodies (DLB) at evaluation 2 at age 67 years. Autopsy showed neocortical-predominant Lewy body
disease (N-LBD). The encircled ‘D’ represents the timing when donepezil was initiated. Neuropsychological profile at mild cognitive
impairment diagnosis (bottom): The patient’s performance on key tests in the neuropsychological battery are shown graphically, with
performance on each test displayed using the MOANS SS reference (mean is 10, 1 SD is 3). The patient’s cognitive symptoms along
with the impairment in the memory, attention/executive and visuospatial domains led to the consensus diagnosis of mild cognitive
impairment, specifically multiple domain amnestic mild cognitive impairment. Note that the low score on the Controlled Oral Word
Association Test was interpreted as reflecting poor set shifting/psychomotor slowing as the Trail Making Test -B was performed so
poorly. Refer to Fig. 1 caption for abbreviations.
550 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
less satisfactory for dementia with Lewy bodies. Findings on many
ancillary tests support the contention that those with idiopathic
REM sleep behaviour disorder (i.e. REM sleep behaviour disorder
not associated with any other neurological symptoms
or disorders) reflects underlying Lewy body disease (Albin et al.,
2000; Eisensehr et al., 2000, 2003; Ferini-Strambi et al., 2004;
Stiasny-Kolster et al., 2005; Caselli et al., 2006; Mazza et al.,
2006; Terzaghi et al., 2008; Postuma et al., 2009) and brain-
stem-predominant Lewy body disease has been documented
in two cases of idiopathic REM sleep behaviour disorder
(Uchiyama et al., 1995, Boeve et al., 2007a), which also supports
this staging system.
A similar evolution of degenerative changes may occur in both
Parkinson’s disease and dementia with Lewy bodies, and the
timing of clinical features may reflect when the critical thresholds
of neuronal network degeneration are reached. Consider a hypo-
thetical example (this example is for illustrative purposes and does
not imply these percent depletions are entirely accurate), in which
an 80% depletion of dopaminergic neurons may be needed to
manifest parkinsonism, and a 50% depletion of cholinergic neu-
rons may be needed to manifest cognitive impairment; it would
be reasonable to suggest a ‘bottom-to-top’ progression of Lewy
body disease pathology could still explain the onset of cognitive
symptoms prior to parkinsonism if both systems are affected grad-
ually over years but the thresholds for the expression of clinical
deficits are different such that cognitive impairment becomes
evident prior to parkinsonism. In other words, the evolution of
features in the dementia with Lewy bodies phenotype does not
necessarily refute the Braak staging system for Lewy body disease
progression.
Another explanation is that, at least in some cases, a ‘top-to-
bottom’ or descending progression of degenerative changes from
the neocortex/limbic system to the nigrostriatal system may better
explain the onset of cognitive impairment prior to parkinsonism in
many dementia with Lewy bodies cases. Or a more patchy and
discontinuous progression could evolve (Frigerio et al., 2009),
with the cholinergic neurotransmitter system reaching a critical
threshold of degenerative changes prior to the nigrostriatal
neuronal networks. This is similar to variations of neurodegenera-
tive disease progression in Alzheimer’s disease. Most cases of
evolving Alzheimer’s disease tend to follow the Braak stages of
neurofibrillary tangle deposition and develop amnestic mild
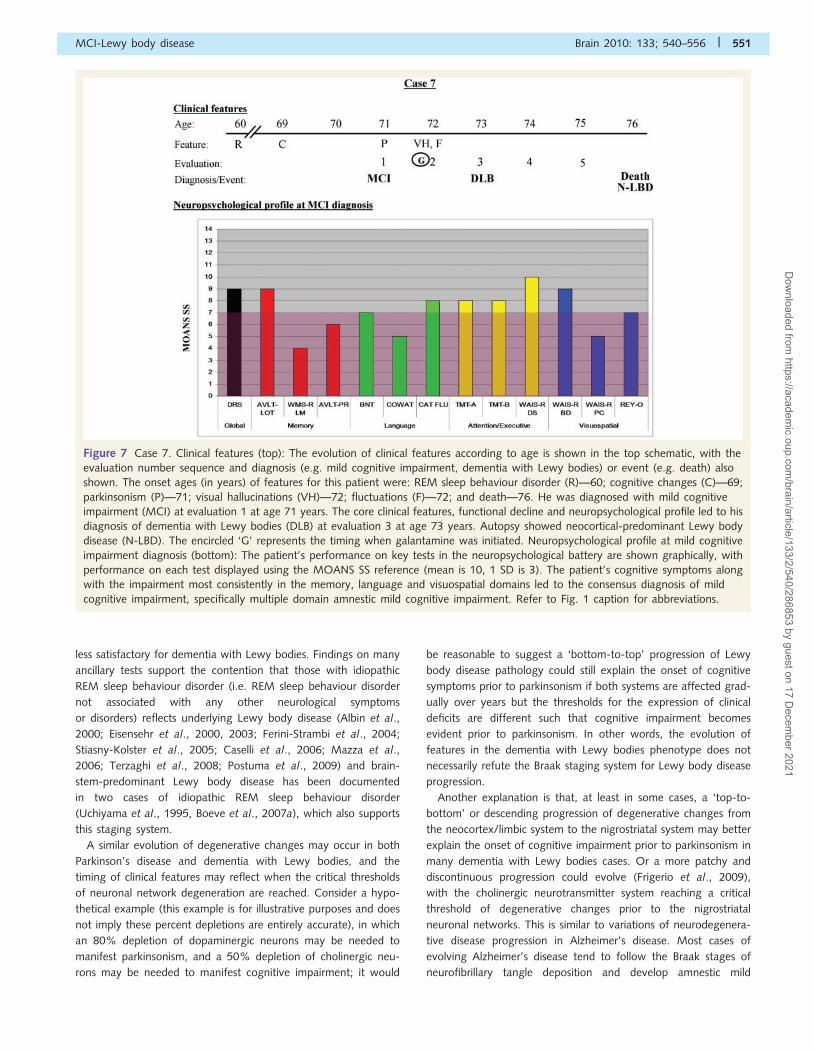
Figure 7 Case 7. Clinical features (top): The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: REM sleep behaviour disorder (R)—60; cognitive changes (C)—69;
parkinsonism (P)—71; visual hallucinations (VH)—72; fluctuations (F)—72; and death—76. He was diagnosed with mild cognitive
impairment (MCI) at evaluation 1 at age 71 years. The core clinical features, functional decline and neuropsychological profile led to his
diagnosis of dementia with Lewy bodies (DLB) at evaluation 3 at age 73 years. Autopsy showed neocortical-predominant Lewy body
disease (N-LBD). The encircled ‘G’ represents the timing when galantamine was initiated. Neuropsychological profile at mild cognitive
impairment diagnosis (bottom): The patient’s performance on key tests in the neuropsychological battery are shown graphically, with
performance on each test displayed using the MOANS SS reference (mean is 10, 1 SD is 3). The patient’s cognitive symptoms along
with the impairment most consistently in the memory, language and visuospatial domains led to the consensus diagnosis of mild
cognitive impairment, specifically multiple domain amnestic mild cognitive impairment. Refer to Fig. 1 caption for abbreviations.
MCI-Lewy body disease Brain 2010: 133; 540–556 | 551
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
cognitive impairment prior to language, attention/executive and
visuospatial dysfunction; however, there are certainly cases of
pathologically confirmed atypical Alzheimer’s disease that have
presented as focal cortical syndromes such as primary progressive
aphasia (Josephs et al., 2008), corticobasal syndrome (Boeve
et al., 1999), and posterior cortical atrophy (Tang-Wai et al.,
2004). As a result, exceptions to any model of neurodegenerative
disease progression will always exist, and surely Lewy body disease
will evolve in more than one manner.
Further support of the REM sleepbehaviour disorder-synucleinopathyassociationThese cases add to growing evidence that REM sleep behaviour
disorder in the setting of neurodegenerative disease strongly
suggests an underlying synucleinopathy—particularly Lewy body
disease or multiple system atrophy (Boeve et al., 2001, 2003,
2007b; Gagnon et al., 2006; Iranzo et al., 2006; Postuma et al.,
2009). Furthermore, REM sleep behaviour disorder tends to pre-
cede the onset of cognitive and motor features by years or
decades in the synucleinopathies, whereas REM sleep behaviour
disorder typically evolves concurrently or after the onset of motor
and cognitive features in the non-synucleinopathy disorders.
Hence, REM sleep behaviour disorder preceding the motor and
cognitive features of a neurodegenerative disorder may be partic-
ularly specific for synucleinopathies (Boeve et al., 2003, 2007b;
Gagnon et al., 2006; Iranzo et al., 2006; Postuma et al., 2009).
The almost complete absence of REM sleep behaviour disorder
in autopsy-proven cases of amyloidopathies and tauopathies con-
vincingly suggests that selective vulnerability of key brainstem net-
works underlying REM sleep behaviour disorder occurs in the
synucleinopathies. There are virtually no features in clinical neu-
rology which are 100% specific for an aetiological category of
disease, and such degeneration therefore is not specific to a partic-
ular proteinopathy, but rather the same neuronal network(s) is
(are) involved in patients with REM sleep behaviour disorder
associated with any neurodegenerative disorder. Yet the REM
sleep behaviour disorder-synucleinopathy association is strong.
Knowledge about the associated neuronal networks of REM
sleep behaviour disorder in humans may provide insights into
why these and other key structures such as the dorsal motor
nucleus of the vagus, olfactory bulb and substantia nigra pars
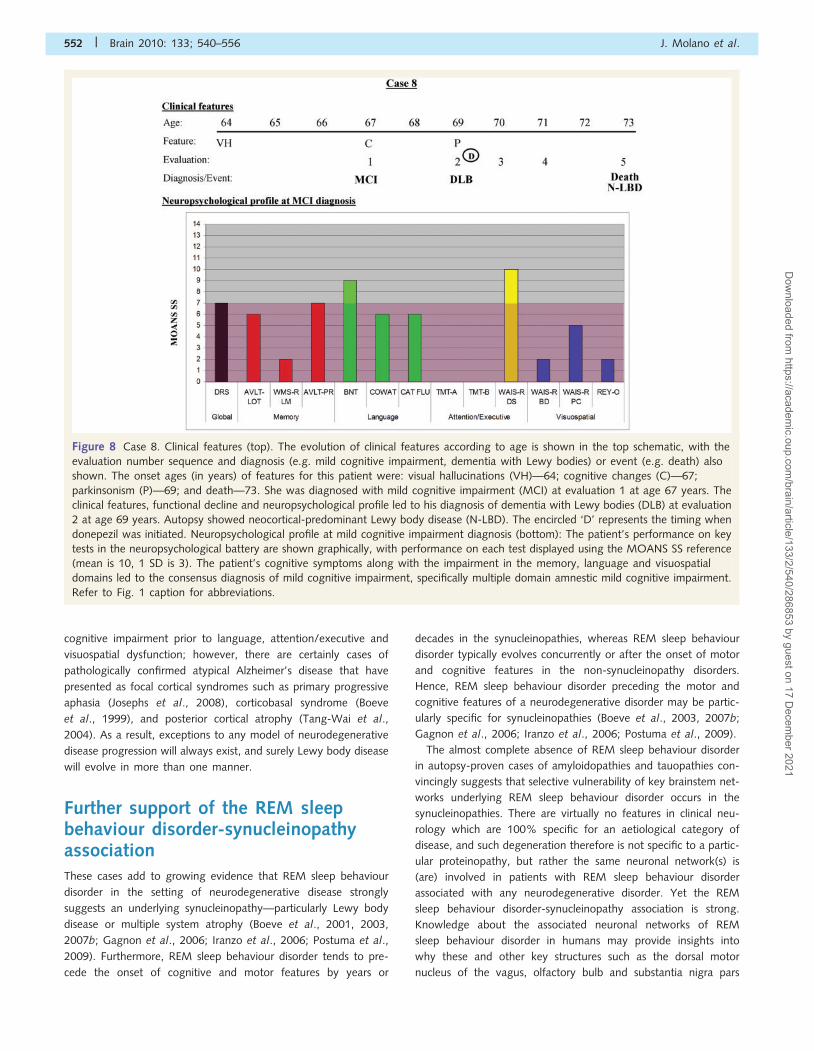
Figure 8 Case 8. Clinical features (top). The evolution of clinical features according to age is shown in the top schematic, with the
evaluation number sequence and diagnosis (e.g. mild cognitive impairment, dementia with Lewy bodies) or event (e.g. death) also
shown. The onset ages (in years) of features for this patient were: visual hallucinations (VH)—64; cognitive changes (C)—67;
parkinsonism (P)—69; and death—73. She was diagnosed with mild cognitive impairment (MCI) at evaluation 1 at age 67 years. The
clinical features, functional decline and neuropsychological profile led to his diagnosis of dementia with Lewy bodies (DLB) at evaluation
2 at age 69 years. Autopsy showed neocortical-predominant Lewy body disease (N-LBD). The encircled ‘D’ represents the timing when
donepezil was initiated. Neuropsychological profile at mild cognitive impairment diagnosis (bottom): The patient’s performance on key
tests in the neuropsychological battery are shown graphically, with performance on each test displayed using the MOANS SS reference
(mean is 10, 1 SD is 3). The patient’s cognitive symptoms along with the impairment in the memory, language and visuospatial
domains led to the consensus diagnosis of mild cognitive impairment, specifically multiple domain amnestic mild cognitive impairment.
Refer to Fig. 1 caption for abbreviations.
552 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
reticularis are consistently affected in the synucleinopathy spec-
trum disorders.
Clinical relevance of REM sleepbehaviour disorder in the evaluationof patients with cognitive impairmentREM sleep behaviour disorder was incorporated into the dementia
with Lewy bodies diagnostic criteria and functions as a feature
that increases the diagnostic confidence from one of clinically pos-
sible, to clinically probable dementia with Lewy bodies (McKeith
et al., 2005). This feature has been added as a variable of interest
by the National Alzheimer’s Coordinating Center. Currently, the
presence of recurrent dream enactment behaviour suggests a clin-
ical diagnosis of dementia with Lewy bodies in the setting of
dementia, particularly when REM sleep behaviour disorder can
be verified by polysomnogram. Given that all seven patients
with REM sleep behaviour disorder and mild cognitive impairment
developed Lewy body disease on autopsy, the presence of
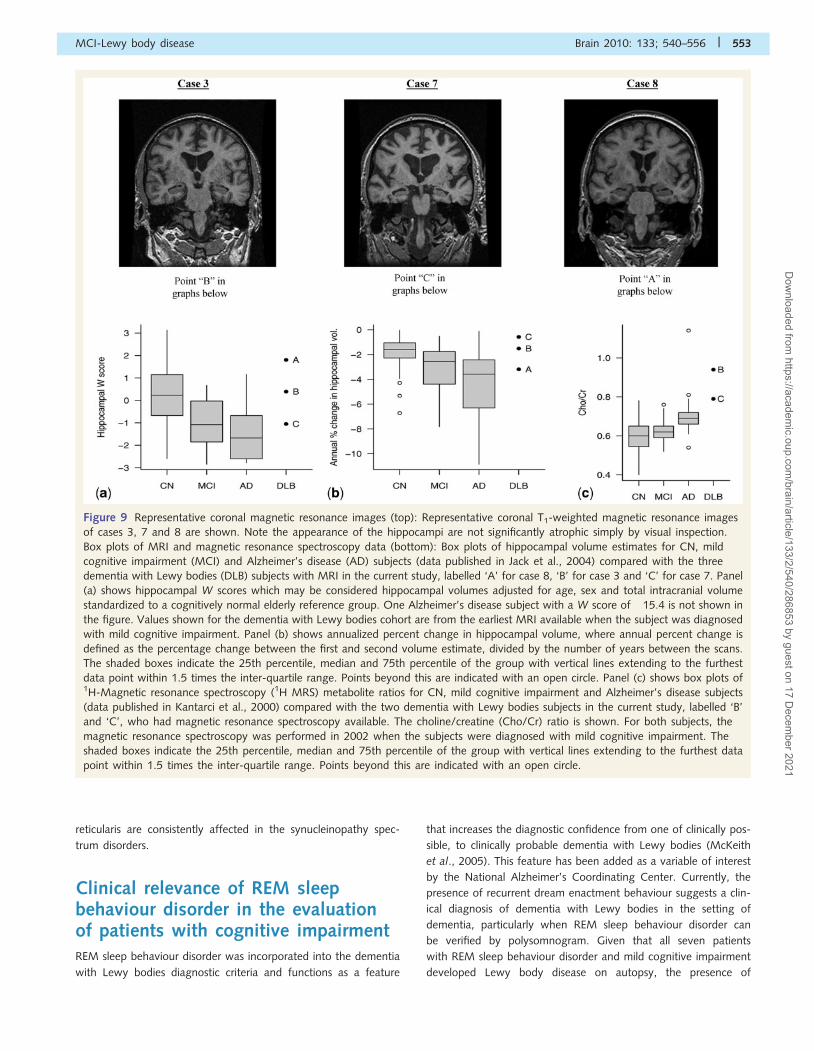
Figure 9 Representative coronal magnetic resonance images (top): Representative coronal T1-weighted magnetic resonance images
of cases 3, 7 and 8 are shown. Note the appearance of the hippocampi are not significantly atrophic simply by visual inspection.
Box plots of MRI and magnetic resonance spectroscopy data (bottom): Box plots of hippocampal volume estimates for CN, mild
cognitive impairment (MCI) and Alzheimer’s disease (AD) subjects (data published in Jack et al., 2004) compared with the three
dementia with Lewy bodies (DLB) subjects with MRI in the current study, labelled ‘A’ for case 8, ‘B’ for case 3 and ‘C’ for case 7. Panel
(a) shows hippocampal W scores which may be considered hippocampal volumes adjusted for age, sex and total intracranial volume
standardized to a cognitively normal elderly reference group. One Alzheimer’s disease subject with a W score of �15.4 is not shown in
the figure. Values shown for the dementia with Lewy bodies cohort are from the earliest MRI available when the subject was diagnosed
with mild cognitive impairment. Panel (b) shows annualized percent change in hippocampal volume, where annual percent change is
defined as the percentage change between the first and second volume estimate, divided by the number of years between the scans.
The shaded boxes indicate the 25th percentile, median and 75th percentile of the group with vertical lines extending to the furthest
data point within 1.5 times the inter-quartile range. Points beyond this are indicated with an open circle. Panel (c) shows box plots of1H-Magnetic resonance spectroscopy (1H MRS) metabolite ratios for CN, mild cognitive impairment and Alzheimer’s disease subjects
(data published in Kantarci et al., 2000) compared with the two dementia with Lewy bodies subjects in the current study, labelled ‘B’
and ‘C’, who had magnetic resonance spectroscopy available. The choline/creatine (Cho/Cr) ratio is shown. For both subjects, the
magnetic resonance spectroscopy was performed in 2002 when the subjects were diagnosed with mild cognitive impairment. The
shaded boxes indicate the 25th percentile, median and 75th percentile of the group with vertical lines extending to the furthest data
point within 1.5 times the inter-quartile range. Points beyond this are indicated with an open circle.
MCI-Lewy body disease Brain 2010: 133; 540–556 | 553
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021

REM sleep behaviour disorder—regardless of the mild cognitive
impairment subtype—is likely to reflect evolving Lewy body
disease.
The strengths of the study include well-characterized and pro-
spectively followed patients who developed mild cognitive impair-
ment and had autopsy-proven Lewy body disease. Importantly,
mild cognitive impairment diagnoses were made in real-time.
Subjects were not assigned mild cognitive impairment diagnoses
retrospectively after a diagnosis of dementia with Lewy bodies had
been made. A weakness of this clinicopathologic series is that it
involves only eight cases. As a result, generalizations about the
progression of symptoms in mild cognitive impairment to dementia
with Lewy bodies will require further longitudinal studies. Another
limitation is that due to slight changes in the neuropsychological
battery over time, an identical set of neuropsychological data was
not obtained on all patients. Also, at least one patient was not
testable, and another was unable to complete testing due to
fatigue.
Our findings indicate that Lewy body disease can pass through
a mild cognitive impairment intermediate state, with any mild
cognitive impairment subtype potentially evolving into dementia
with Lewy bodies. All cases with REM sleep behaviour disorder
and mild cognitive impairment eventually were shown to have
autopsy-proven Lewy body disease, indicating that REM sleep
behaviour disorder plus mild cognitive impairment probably
reflects brainstem and cerebral Lewy body disease. These findings
also underscore the importance of expanding the characterization
beyond cognition in the dementing neurodegenerative disorders;
attempts should be made to perform longitudinal assessments of
the cognitive/neuropsychological, neuropsychiatric/behavioural,
motor, sleep, autonomic and other features to improve the under-
standing of early clinical manifestations of Lewy body disease and
other neurodegenerative disorders.
AcknowledgementsThe authors thank their staff at the Mayo Alzheimer’s Disease
Research Center and Mayo Center for Sleep Medicine for their
evaluation and education/counselling for many of the patients
and families included in this report. They particularly extend
their gratitude to the patients and their families for participating
in research on ageing, cognition and sleep.
FundingNational Institutes of Health [AG15866 to B.F.B., T.J.F. (PI),
G.E.S., V.S.P., D.W.D.; AG16574 to B.F.B., T.J.F., G.E.S., J.E.P.,
D.W.D., D.S.K., N.G.R., J.A.L., K.K., C.J., V.S.P., R.C.P. (PI);
NS40256 to B.F.B., T.J.F., D.W.D. (PI); AG06786 to B.F.B.,
G.E.S., J.E.P., D.S.K., Y.E.G., V.S.P., R.C.P. (PI); and AG23195
to K.K., M.S., C.R.J. (PI)], and the Robert H. and Clarice Smith
and Abigail Van Buren Alzheimer’s Disease Research Program of
the Mayo Foundation.
Supplementary materialSupplementary material is available at Brain online.
ReferencesAmerican Psychiatric Association.Diagnostic and Statistical Manual of
Mental Disorders. 3rd edn., Rev Washington, DC: AmericanPsychiatric Association; 1987.
Consensus recommendations for the postmortem diagnosis of
Alzheimer’s disease.The National Institute on Aging, and Reagan
Institute Working Group on Diagnostic Criteria for the Neuropatholo-
gical Assessment of Alzheimer’s Disease. Neurobiol Aging 1997; 18:S1–S2.
Albin R, Koeppe R, Chervin R, Consens F, Wernette K, Frey K, et al.
Decreased striatal dopaminergic innervation in REM sleep behavior
disorder. Neurology 2000; 55: 1410–12.
Benton A, Hamsher Kd. Multilingual Aphasia Examination (Manual).Iowa City, IA: University of Iowa; 1978.
Boeve B, Dickson D, Olson E, Shepard J, Silber M, Ferman T, et al.
Insights into REM sleep behavior disorder pathophysiology in
brainstem-predominant Lewy body disease. Sleep Med 2007a; 8:
60–4.Boeve B, Silber M, Ferman T, Lucas J, Parisi J. Association of REM sleep
behavior disorder and neurodegenerative disease may reflect an
underlying synucleinopathy. Mov Disord 2001; 16: 622–30.
Boeve B, Silber M, Parisi J, Dickson D, Ferman T, Benarroch E, et al.
Synucleinopathy pathology and REM sleep behavior disorder plusdementia or parkinsonism. Neurology 2003; 61: 40–5.
Boeve B, Silber M, Saper C, Ferman T, Dickson D, Parisi J, et al.
Pathophysiology of REM sleep behaviour disorder and relevance to
neurodegenerative disease. Brain 2007b; 130: 2770–88.Boeve BF, Maraganore DM, Parisi JE, Ahlskog JE, Graff-Radford N,
Caselli RJ, et al. Pathologic heterogeneity in clinically diagnosed corti-
cobasal degeneration. Neurology 1999; 53: 795–800.
Braak H, Braak E. Neuropathological stageing of Alzheimer-related
changes. Acta Neuropathol (Berl) 1991; 82: 239–59.Braak H, Braak E. Diagnostic criteria for neuropathologic assessment of
Alzheimer’s disease. Neurobiol Aging 1997; 18: S85–8.
Braak H, Del Tredici K, Rub U, de Vos R, Jansen Steur E, Braak E. Staging
of brain pathology related to sporadic Parkinson’s disease. Neurobiol
Aging 2003; 24: 197–211.Braak H, Ghebremedhin E, Rub U, Bratzke H, Del Tredici K. Stages in the
development of Parkinson’s disease-related pathology. Cell Tissue Res
2004; 318: 121–34.
Burke R, Dauer W, Vonsattel J. A critical evaluation of the
Braak staging scheme for Parkinson’s disease. Ann Neurol 2008; 64:485–91.
Caselli R, Chen K, Bandy D, Smilovici O, Boeve B, Osborne D, et al.
A preliminary fluorodeoxyglucose positron emission tomography study
in healthy adults reporting dream-enactment behavior. Sleep 2006; 29:
927–33.Dubois B, Albert M. Amnestic MCI or prodromal Alzheimer’s disease.
Lancet Neurol 2004; 3: 246–8.
Eisensehr I, Linke R, Noachtar S, Schwarz J, Gildehaus F, Tatsch K.
Reduced striatal dopamine transporters in idiopathic rapid eye move-
ment sleep behaviour disorder: Comparison with Parkinson’s diseaseand controls. Brain 2000; 123: 1155–60.
Eisensehr I, Linke R, Tatsch K, Kharraz B, Gildehaus JF, Wetter CT, et al.
Increased muscle activity during rapid eye movement sleep correlates
with decrease of striatal presynaptic dopamine transporters. IPT and
IBZM SPECT imaging in subclinical and clinically manifest idiopathicREM sleep behavior disorder, Parkinson’s disease, and controls. Sleep
2003; 26: 507–12.
Ferini-Strambi L, Di Gioia M, Castronovo V, Oldani A, Zucconi M,
Cappa S. Neuropsychological assessment in idiopathic REM sleep
554 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021
behavior disorder (RBD): Does the idiopathic form of RBD really exist?
Neurology 2004; 62: 41–5.
Ferman T, Boeve B, Smith G, Silber M, Lucas J, Graff-Radford N, et al.
Dementia with Lewy bodies may present as dementia with REM sleep
behavior disorder without parkinsonism or hallucinations. J Internat
Neuropsychol Soc 2002; 8: 907–14.
Ferman T, Smith G, Boeve B, Graff-Radford N, Lucas J, Knopman D,
et al. Neuropsychological differentiation of dementia with Lewy
bodies from normal aging and Alzheimer’s disease. Clin
Neuropsychol 2006; 20.Ferman T, Smith G, Boeve B, Ivnik R, Petersen R, Knopman D, et al. DLB
fluctuations: Specific features that reliably differentiate DLB from AD
and normal aging. Neurology 2004; 62: 181–7.Ferman TJ, Boeve BF, Smith GE, Silber MH, Kokmen E, Petersen RC,
et al. REM sleep behavior disorder and dementia: cognitive differences
when compared with AD. Neurology 1999; 52: 951–7.Folstein M, Folstein S, McHugh P. ‘‘Mini-mental state’’. A practical
method for grading the cognitive state of patients for the clinician.
J Psychiatr Res 1975; 12: 189–98.
Frigerio R, Fujishiro H, Ahn T, Josephs K, Maraganore D, Delledonne A,
et al. Incidental Lewy body disease: Do some cases represent a pre-
clinical stage of dementia with Lewy bodies? Neurobiol Aging 2009;
Jun 25. [Epub ahead of print].
Fujishiro H, Ferman T, Boeve B, Smith G, Graff-Radford N, Uitti R, et al.
Validation of the neuropathologic criteria of the third consortium for
dementia with Lewy bodies for prospectively diagnosed cases.
J Neuropathol Exp Neurol 2008; 67: 649–56.
Gagnon J-F, Postuma R, Mazza S, Doyon J, Montplaisir J. Rapid-eye-
movement sleep behaviour disorder and neurodegenerative diseases.
Lancet Neurol 2006; 5: 424–32.Gwinn-Hardy K, Mehta ND, Farrer M, Maraganore D, Muenter M,
Yen SH, et al. Distinctive neuropathology revealed by alpha-synuclein
antibodies in hereditary parkinsonism and dementia linked to chromo-
some 4p. Acta Neuropathologica 2000; 99: 663–72.
Hughes A, Ben-Shlomo Y, Daniel S, Lees A. What features improve the
accuracy of clinical diagnosis in Parkinson’s disease? A clinicopatholo-
gic study. Neurology 1992; 42: 1142–6.
Iranzo A, Molinuevo J, Santamarıa J, Serradell M, Martı M,
Valldeoriola F, et al. Rapid-eye-movement sleep behaviour disorder
as an early marker for a neurodegenerative disorder: a descriptive
study. Lancet Neurol 2006; 5: 572–77.
Ivnik R, Malec J, Smith G, Tangalos E, Petersen R. Neuropsychological
tests’ norms above age 55: COWAT, BNT, MAE Token, WRAT-R
reading, AMNART, STROOP, TMT and JLO. Clin Neuropsychol
1996; 10: 262–78.Ivnik R, Malec J, Smith G, Tangalos E, Petersen R, Kokmen E, et al.
Mayo’s Older American Normative Studies: WAIS-R, WMS-R, and
AVLT norms for ages 56-97. Clin Neuropsychol 1992; 6 (Suppl):
1–104.
Ivnik RJ, Smith GE, Lucas JA, Tangalos EG, Kokmen E, Petersen RC. Free
and cued selective reminding test: MOANS norms. J Clin Exp
Neuropsychol 1997; 19: 676–91.
Jack CR Jr, Petersen RC, Xu Y, O’Brien PC, Smith GE, Ivnik RJ, et al.
Rates of hippocampal atrophy correlate with change in clinical status in
aging and AD. Neurology 2000; 55: 484–9.
Jack CR Jr, Shiung MM, Gunter JL, O’Brien PC, Weigand SD,
Knopman DS, et al. Comparison of different MRI brain atrophy rate
measures with clinical disease progression in AD. Neurology 2004; 62:
591–600.
Jellinger K, Attems J. Incidence of cerebrovascular lesions in Alzheimer’s
disease: a postmortem study. Acta Neuropathol 2003; 105: 14–17.
Jicha G, Parisi J, Dickson D, Johnson K, Cha R, Ivnik R, et al.
Neuropathologic outcome of mild cognitive impairment following
progression to clinical dementia. Arch Neurol 2006; 63: 674–81.
Jicha G, Schmitt F, Abner E, Nelson P, Cooper G, Smith C, et al.
Prodromal clinical manifestations of neuropathologically confirmed
Lewy body disease. Neurobiol Aging 2008; Nov 19. [Epub ahead of
print].
Josephs K, Tsuboi Y, Cookson N, Watt H, Dickson D. Apolipoprotein E
epsilon 4 is a determinant for Alzheimer-type pathologic features in
tauopathies, synucleinopathies, and frontotemporal degeneration. Arch
Neurol 2004; 61: 1579–84.Josephs K, Whitwell J, Duffy J, Vanvoorst W, Strand E, Hu W, et al.
Progressive aphasia secondary to Alzheimer disease vs FTLD pathol-
ogy. Neurology 2008; 70: 25–34.
Kantarci K, Jack CR Jr, Xu YC, Campeau NG, O’Brien PC, Smith GE,
et al. Regional metabolic patterns in mild cognitive impairment and
Alzheimer’s disease: A 1H MRS study. Neurology 2000; 55: 210–17.
Kantarci K, Petersen RC, Boeve BF, Knopman DS, Tang-Wai DF,
O’Brien PC, et al. 1H MR spectroscopy in common dementias.
Neurology 2004; 63: 1393–8.Kaplan E, Goodglass H, Weintraub S. The Boston naming test. Boston: E.
Kaplan & H. Goodglass; 1978.Kokmen E, Smith G, Petersen R, Tangalos E, Ivnik R. The short test of
mental status: correlations with standardized psychometric testing.
Arch Neurol 1991; 48: 725–8.
Lucas JA, Ivnik RJ, Smith GE, Bohac DL, Tangalos EG, Graff-Radford NR,
et al. Mayo’s older Americans normative studies: category fluency
norms. J Clin Exp Neuropsychol 1998a; 20: 194–200.
Lucas JA, Ivnik RJ, Smith GE, Bohac DL, Tangalos EG, Kokmen E, et al.
Normative data for the Mattis Dementia Rating Scale. J Clin Exp
Neuropsychol 1998b; 20: 536–47.
Mattis S. Dementia rating scale: professional manual. Odessa: Psycholo-
gical Assessment Resources; 1988.Mazza S, Soucy J, Gravel P, Michaud M, Postuma R, Massicotte J, et al.
Assessing whole brain perfusion changes in REM sleep behavior dis-
order. Neurology 2006; 67: 1618–22.
McKeith I, Dickson D, Lowe J, Emre M, O’Brien J, Feldman H, et al.
Dementia with Lewy bodies: diagnosis and management: Third report
of the DLB Consortium. Neurology 2005; 65: 1863–72.
McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan E.
Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-
ADRDA work group under the auspices of the Department of
Health and Human Services Task Force on Alzheimer’s disease.
Neurology 1984; 34: 939–44.
Members of the Department of Neurology MC.Clinical Examinations in
Neurology. St. Louis: Mosby – Year Book, Inc.; 1998.
Mirra S, Heyman A, McKeel D, Sumi S, Crain B, Brownlee L, et al. The
Consortium to Establish a Registry for Alzheimer’s Disease (CERAD).
Part II. Standardization of the neuropathologic assessment of
Alzheimer’s disease. Neurology 1991; 41: 479–86.Mori E, Shimomura T, Fujimori M, Hirono N, Imamura T, Hashimoto M,
et al. Visuoperceptual impairment in dementia with Lewy bodies. Arch
Neurol 2000; 57: 489–93.
Morris J, Storandt M, Miller J, McKeel D, Price J, Rubin E, et al. Mild
cognitive impairment represents early-stage Alzheimer disease. Arch
Neurol 2001; 58: 397–405.
Morris JC. The Clinical Dementia Rating (CDR): current version and
scoring rules. Neurology 1993; 43: 2412–14.
Neary D, Snowden J, Gustafson L, Passant U, Stuss D, Black S, et al.
Frontotemporal lobar degeneration: a consensus on clinical diagnostic
criteria. Neurology 1998; 51: 1546–54.Olson E, Boeve B, Silber M. Rapid eye movement sleep behavior disor-
der: demographic, clinical, and laboratory findings in 93 cases. Brain
2000; 123: 331–9.
Osterrieth P. Le test de copie d’une figure complexe. Arch Psychol 1944;
30: 206–356.
Petersen R. Mild cognitive impairment as a diagnostic entity. J Intern
Med 2004; 256: 183–94.
Petersen R, Parisi J, Dickson D, Johnson K, Knopman D, Boeve B, et al.
Neuropathologic features of amnestic mild cognitive impairment. Arch
Neurol 2006; 63: 665–72.
Postuma R, Gagnon J, Vendette M, Fantini M, Massicotte-Marquez J,
Montplaisir J. Quantifying the risk of neurodegenerative disease in
idiopathic REM sleep behavior disorder. Neurology 2009; 72:
1296–300.
MCI-Lewy body disease Brain 2010: 133; 540–556 | 555
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021

Reitan R. Validity of the trail-making test as an indication of organicbrain damage. Percept Mot Skills 1958; 8: 271–6.
Rey A. L’examen psychologique dan les cas d’encephalopathie trauma-
tique. Arch Psychol 1941; 28: 286–340.
Rey A. L’Examen Clinique en Psychologie. Paris, France: PressesUniversitaires de France; 1964.
Salmon D, Galasko D, Masliah E, Butters N, Thal L, Hansen L, et al.
Neuropsychological deficits associated with diffuse Lewy body disease.
Brain Cogn 1996; 31: 148–64.Sarazin M, Berr C, De Rotrou J, Fabrigoule C, Pasquier F, Legrain S, et al.
Amnestic syndrome of the medial temporal type identifies prodromal
AD: a longitudinal study. Neurology 2007; 69: 1859–67.Schenck C, Mahowald M. REM sleep behavior disorder: Clinical, devel-
opmental, and neuroscience perspectives 16 years after its formal
identification in SLEEP. Sleep 2002; 25: 120–38.
Schenck CH, Bundlie SR, Ettinger MG, Mahowald MW. Chronic beha-vioral disorders of human REM sleep: a new category of parasomnia.
Sleep 1986; 9: 293–308.
Stiasny-Kolster K, Doerr Y, Moller J, Hoffken H, Behr T, Oertel W, et al.
Combination of ‘idiopathic’ REM sleep behaviour disorder and olfactorydysfunction as possible indicator for – synucleinopathy demonstrated
by dopamine transporter FP-CIT-SPECT. Brain 2005; 128: 126–37.
Tang-Wai D, Graff-Radford N, Boeve B, Dickson D, Parisi J, Crook R,
et al. Clinical, genetic, and neuropathologic characteristics of posteriorcortical atrophy. Neurology 2004; 63: 1168–74.
Tang-Wai DF, Knopman DS, Geda YE, Edland SD, Smith GE, Ivnik RJ,
et al. Comparison of the short test of mental status and the mini-
mental state examination in mild cognitive impairment. Arch Neurol
2003; 60: 1777–81.
Terzaghi M, Sinforiani E, Zucchella C, Zambrelli E, Pasotti C,
Rustioni V, et al. Cognitive performance in REM sleep behaviour
disorder: a possible early marker of neurodegenerative disease?
Sleep Med 2008; 9: 343–51.
Togo T, Cookson N, Dickson D. Argyrophilic grain disease:
Neuropathology, frequency in a dementia brain bank and
lack of relationship with apolipoprotein E. Brain Pathol 2002; 12:
45–52.
Uchiyama M, Isse K, Tanaka K, Yokota N, Hamamoto H, Aida S, et al.
Incidental Lewy body disease in a patient with REM sleep behavior
disorder. Neurology 1995; 45: 709–12.
Wechsler D. Wechsler Adult Intelligence Scale-Revised (Manual). San
Antonio: The Psychological Corporation; 1981.
Wechsler D. Wechsler Memory Scale-Revised (Manual). New York:
Psychological Corporation; 1987.
Whitwell J, Weigand S, Shiung M, Boeve B, Ferman T, Smith G, et al.
Focal atrophy in dementia with Lewy bodies on MRI: a distinct pattern
from Alzheimer’s disease. Brain 2007; 130: 708–19.
556 | Brain 2010: 133; 540–556 J. Molano et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article/133/2/540/286853 by guest on 17 D
ecember 2021