Embed Size (px)
Citation preview
MIDTERM REPORT
AND
FOLLOW-UP PROPOSAL
FUNDING PERIOD 2002 - 2004

5
Abbreviations BM bone marrow
BMBF Ministry of Education and Research (Bundesministerium für Bildung und Forschung)
BMT bone marrow transplantation
B-NHL B-cell lymphoma
cDNA complementary desoxyribonucleic acid
CHMG Cochrane Hematological Malignancies Group
CHOEP chemotherapy regimen (cyclophosphamide, doxorubicin, vincristine, etoposide and prednisone
CHOP chemotherapy regimen (cyclophosphamide, doxorubicin, vincristine, prednisone)
CLL chronic lymphocytic leukemia
CMS content management system
CR complete remission
CRF case report form
CTA cancer-testis antigen
CT computer tomography
DFG Deutsche Forschungsgemeinschaft
DGHO German Society of Hematology and Oncology (Deutsche Gesellschaft für Hämatologie und Onkologie)
DGIM German Society of Internal Medicine (Deutsche Gesellschaft für Innere Medizin)
DLH German leukemia and lymphoma patients’ representation (Deutsche Leukämie- und Lymphom Hilfe)
DRST German Registry for Hematopoietic Stem Cell Transplantation (Deutsches Register für Stammzelltransplantationen)
DSHNHL German High-Grade Non-Hodgkin’s Lymphoma Study Group (Deutsche Studiengruppe Hochmaligne Non-Hodgkin Lymphome)
DSL digital subscriber line
EbM evidence-based medicine
EBMT European Group for Blood and Marrow Transplantation
e.V. registered association (eingetragener Verein)
EORTC European Organisation for Research and Treatment of Cancer
FFTF freedom from treatment failure
GCLLSG German CLL Study Group
GCP good clinical practice
GHSG German Hodgkin’s Lymphoma Study Group
GLSG German Low-Grade Non-Hodgkin’s Lymphoma Study Group
6
GSGL German Study Group Gastro-intestinal Lymphoma
GVHD graft versus host disease
HD Hodgkin’s disease
HDT high-dose therapy
HG high-grade
HLA human leukocyte antigen
IBMTR International Bone Marrow Transplant Registry
ICD International Classification of Diseases
ICH International Conference on Harmonisation
ID identity
IHECE Institute of Health Economics and Clinical Epidemiology, University of Cologne
ILI Italian Lymphoma Intergroup
IMISE Institute of Medical Informatics, Statistics and Epidemiology, University of Leipzig
ISDN integrated services digital network
ISST Institute for Software and System Technology (Fraunhofer Institut für Software and Systemtechnik)
IT information technology
KKS coordination centre for clinical studies (Koordinationszentrum für klinische Studien)
LDAP lightweight directory access protocol
LDH lactate dehydrogenase
LG low-grade
MCL mantle cell lymphoma
MERG Medical Economics Research Group, University of Cologne
MM multiple myeloma
NHL Non-Hodgkin’s lymphoma
NLL North German Leukemia and Lymphoma Study Group (Norddeutsche Leukämie- und Lymphomstudie)
ODBC open database connectivity
OS overall survival
OSHO Eastern German Study Group for Hematology and Oncology (Ostdeutsche Studiengruppe für Hämatologie und Onkologie)
ÖGHO Austrian Society of Hematology and Oncology (Österreichische Gesellschaft für Hämatologie und Onkologie)
Pats. patients
PBPCT peripheral blood progenitor cell transplantation
ProMISe Project Manager Internet Server
PT-LPD Post-Transplantation Lymphoproliferative Disorder Study Group
7
QM quality management
QSP quality assurance protocols (Qualitätssicherung Protokoll)
RCT randomised clinical trials
RDE remote data entry
R-FCM immunochemotherapy regimen (fludarabine, mitoxantron, cyclophosphamide plus rituximab)
RT-PCR reverse transcriptase polymerase chain reaction
SOP Standard operating procedures
SP sub-project
SR systematic review
TCO total cost of operation
TED data collection via telecommunication (Telefonische Datenerfassung)
TMF central telematic platform of the BMBF
T-NHL T-cell lymphoma
VPN virtual private networks
WG-QM working group on quality management (AG Qualitätsmanagement)
WHO World Health Organisation
WWW World Wide Web
9
Section 1
Speakers’ Midterm Report
Title Page
Network title: Competence Network Malignant Lymphoma Period covered by this report: 10/1999 – 09/2002 1st funding period 10/2002 – 09/2004 2nd funding period
Name of network speaker: Prof. Dr. Volker Diehl Institution: Klinik I für Innere Medizin, Universität zu Köln Address: Joseph-Stelzmann-Str. 9, D-50924 Köln Phone: +49 (0) 221 / 478 - 7400 or 7401 Fax: +49 (0) 221 / 478 - 7406 E-mail: [email protected] Network homepage: www.kompetenznetz-lymphome.de
Speakers’ Midterm Report: Section 1
10
Part A – Research Results A-1. Publications
§ See publication list after “Scientific Highlights” (A-3)
a) How many network-related English papers have been published in reviewed journals during the funding period or are momentarily in press?
38 b) How many of the publications listed in a) involved at least three network partners
from different universities or non-university research institutions?
10
c) How many of the publications listed in b) have an international partner?
8
A-2. Patents a) Are patents planned or applied for within your network?
No, not intended
Yes
A-3. Describe the scientific highlights of the network so far.
The most important achievement of the Competence Network Malignant Lymphoma is the formation of a highly cooperative network that connects everyone with an interest in the disease - across all forms of lymphoma and on every level from patient to general practitioner to specialist in hemato-oncology. Therefore the highlights of the competence network are often not scientific in a strict sense of the word, but strongly reflect the network’s mission of implementing a high-level quality management for the treatment of lymphoma. Still, true scientific highlights can be found within the more science-oriented sub-projects and the associated clinical study groups. Highlights of the competence network
Homepage: In December 2000, the network’s homepage was released to the public. It is a comprehensive information portal on malignant lymphoma and serves as the prime reference of the competence network. It contains the most recent clinical findings as well as information on the network itself. All major German clinical study groups on malignant lymphomas are represented with the latest data on their clinical trials. A part of the homepage has been specially designed for patients. In cooperation with different self-help groups and patients’ associations, an easier to comprehend guide on current information and data concerning malignant lymphoma has been installed. Around 4000 accesses per day were counted in December 2001.
IT-based communication infrastructure: Internet communication between the central pathology server (IMISE, Leipzig) and the local databases of all reference centres for lymph
Speakers’ Midterm Report: Section 1
11
node pathology has been established to support and enhance the pathological reference diagnosis of patients enrolled in lymphoma clinical trials. The electronic data transfer is currently running in a test phase in parallel to the conventional exchange of documents by standard mail. Radiation oncologists within the network initiated a similar quality assurance program to improve adequate radiotherapy nationwide. In a central prospective review of diagnostic imaging, over 1200 patients were analysed and received individual prescriptions for involved field radiotherapy. Currently, modern telemedical processes and electronic imaging transfer are implemented to improve communication between reference and study centres.
Evidence-based medicine: In October 2000, the Cochrane Hematological Malignancies Group (CHMG) of the competence network was granted Cochrane status by the Cochrane Collaboration. So far, the CHMG prepared or published two systematic Cochrane reviews and six Cochrane protocols (preliminary reviews) in the Cochrane Library. Furthermore, the private practices of the competence network designed a course on "Evidence-Based Medicine for Hematologists and Oncologists in Private Practices". A basic course on the subjects of "therapy, diagnosis and guidelines" has been held twice a year since May 2001.
Epidemiological and health economical aspects of lymphoma medical care: To survey the medical care of lymphoma patients, to compare care inside and outside of lymphoma clinical trials and to evaluate the economical impact of lymphoma care, a study with data collection relying mostly on patient notebooks has been initiated. In addition to the patient notebook, a structured interview to learn about complex personal aspects (early symptoms, concurrent disease, participation in a clinical trial) is carried out. To analyse the number of inpatient days and clinical departments involved, the patients fill out a special health economic questionnaire.
Vaccines for malignant lymphomas: In a truly scientific highlight, the analysis of cancer-testis antigen (CTA) expression in Non-Hodgkin’s lymphomas (NHL) led to the identification of SCP-1, a known CTA, as a promising candidate for lymphoma vaccine development. T-cell NHL expresses SCP-1 in >50% of the cases – a frequency that would allow for a vaccination of a significant proportion of patients with this sub-type of NHL. In a related project, the screening of the sera of 25 allogeneic patients with NHL led to the identification of 19 antigens encoded by known genes, and four novel transcripts. Nine of those 23 antigens reacted only with the sera from lymphoma patients suggesting their potential usefulness for diagnosis and follow-up of the disease. Highlights of the clinical study groups integrated in the competence network
The three major German lymphoma study groups GHSG1 , DSHNHL 2 and GLSG3 are founding members of the Competence Network Malignant Lymphoma. So far, five additional study groups (GCLLSG4, GSGL 5, OSHO 6, PT-LPD7 , Radioimmunotherapy in Malignant Lymphoma) have been associated with the network. The GSGL formed itself out of three smaller study groups on the initiative of the competence network. Based on guidelines for the association of a research or clinical study group developed by the board of directors, a category list, which defines the requirements for an association, became an appendix to the rules of the competence network. The scientific highlights of the study groups are summarised below. Though, due to the restricted space, only the founding members are taken into account.
1 German Hodgkin’s Lymphoma Study Group 2 German High-Grade Non-Hodgkin’s Lymphoma Study Group 3 German Low-Grade Non-Hodgkin’s Lymphoma Study Group 4 German CLL Study Group 5 German Study Group Gastro-intestinal Lymphoma 6 Eastern German Study Group for Hematology and Oncology 7 Post-Transplantation Lymphoproliferative Disorder Study Group
Speakers’ Midterm Report: Section 1
12
GHSG: The German Hodgkin’s Lymphoma Study Group (GHSG) has increased both, participating institutions and the number of recruited patients, steadily over the last twenty years. As of December 2001, a total of 8514 patients were recruited into first line studies. The major highlight of the GHSG is the development of a new chemotherapy regimen for patients in advanced stages (BEACOPP). BEACOPP in its basic and escalated version is superior to the old standard (COPP/ABVD), both, in terms of freedom from treatment failure (FFTF) and in overall survival (OS). Based on the results, BEACOPP escalated is the new standard for Hodgkin’s disease patients in advanced stages. Other scientific highlights of the GHSG include the final evaluation of the HD8-study for intermediate stages, clearly establishing four cycles of chemotherapy plus involved-field radiotherapy as standard treatment for this group.
DSHNHL: The German High-Grade Non-Hodgkin’s Lymphoma Study Group (DSHNHL) has made the first breakthrough in the treatment of aggressive Non-Hodgkin’s lymphomas (NHL) after 25 years of stagnancy in the field. With the NHL-B trial the DSHNHL established CHOEP (CHOP + etoposide) as the new standard regimen in younger (< 60 years of age) low-risk patients. At the same time, the NHL-B trial could show that by shortening the time intervals between chemotherapy cycles (CHOP-21 to CHOP-14) in older patients (> 60 years of age) complete remission rates, FFTF and OS are significantly improved. In the new 1999-1 trial the DSHNHL will investigate whether the addition of the monoclonal antibody rituximab – a strategy that has been shown to improve results of CHOP-21 by the French GELA group – will further improve the results of this new CHOP-14 standard for elderly patients with aggressive NHL.
GLSG: Since the initiation of the competence network, the German Low-Grade Non-Hodgkin’s Lymphoma Study Group (GLSG) has generated important scientific results that were substantially supported by the cooperation within the network. The GLSG could show that an intensive consolidation with myeloablative chemotherapy and total body irradiation with subsequent autologous peripheral stem cell transplantation (PBPCT) improves the progression-free survival of patients with indolent lymphoma significantly. Currently, this study is being extended to evaluate the effect on overall survival. In a European intergroup study, myeloablative chemotherapy and total body irradiation with subsequent PBPCT as part of the initial treatment reduced the risk of relapse in patients with mantle cell lymphoma (MCL) by more than 60%. In the meantime this procedure has been generally accepted as the standard treatment of MCL. In relapsed indolent lymphomas as well as mantle cell lymphomas, a combined immunochemotherapy (R-FCM) is superior to a fludarabine-containing chemotherapy concerning complete and overall response.
Based on the good interactions within the competence network the study groups decided to initiate interdisciplinary working groups. An epidemiological working group was formed and associated to complement the research within the network. The group investigates the incidence of malignant lymphoma in correlation with different demographical and medical factors. Moreover, to further accentuate their cooperation, members of the study groups and reference pathologists formed the steering committee “Scientific Projects in the Competence Network Malignant Lymphoma”. This committee is currently planning to submit a joint grant application to the “Deutsche Krebshilfe, e.V.”.
As a summary, the Competence Network Malignant Lymphoma has successfully started to implement a quality management for the treatment of lymphoma on many levels. Based on these successes, the efforts will be amplified in the future. By integrating all lymphoma study groups and through the continuous improvement of communication between all network partners, the network will further develop to be the high-level quality management tool envisioned by its founders.
Speakers’ Midterm Report: Section 1
13
List of Publications Publications that involved at least three network partners from different research institutions or have an international partner are marked as follows:
• At least 3 network partners: NET • International partner: INT
2002 Eich HT, Staar S, Gossmann A, Engert A, Franklin J, Sieber M, Krug B, Diehl V, Lackner KJ,
Mueller RP. The HD12 panel of the German Hodgkin’s Lymphoma Study Group (GHSG) - A quality assurance program based on a multidisciplinary panel reviewing all patients' imaging. Int J Radiat Oncol Biol Phys 2002 (submitted)
Staar S, Mueller RP, Eich HT, Engert A, Diehl V.
The value of prospective radiotherapy treatment planning in the multicentric German Hodgkin’s Study Group. Int J Radiat Oncol Biol Phys 2002 (submitted)
Xie X, Wacker H-H, Huang S, Preuss D, Parwaresch R, Tiemann M, Pfreundschuh M.
Expression of cancer testis genes in malignant lymphoma. (submitted)
Schmitz N, Sureda A, Robinson S.
Allogeneic transplantation of hematopoietic stem cells after non-myeloablative conditioning: indications and results. Seminars in Oncology (in press) INT
Robinson S, Goldstone AH, Mackinnon S, Carella A, Russell N, Taghipour G, Schmitz N.
Chemoresistant or aggressive lymphoma predicts for a poor outcome following non-myeloablative allogeneic stem cell transplantation: an analysis from the Lymphoma Working Party of the European Group for Blood and Bone Marrow Transplantation. Blood (in press) INT
Kaiser U, Uebelacker I, Abel U, Birkmann J, Trümper L, Schmalenberg H, Karakas T,
Metzner B, Hossfeld DK, Bischoff HG, Franke A, Reiser M, Müller P, Mantovani L, Grundeis M, Rothmann F, von Seydewitz CU, Mesters RM, Steinhauer EU, Krahl D, Schumacher K, Kneba M, Baudis M, Schmitz N, Pfab R, Köppler H, Parwaresch R, Pfreundschuh M, Havemann K. A randomised study to evaluate the use of high-dose therapy as part of primary treatment for aggressive lymphoma. Journal of Clinical Oncology (in press) NET
Schmitz N, Pfistner B, Sextro M, Sieber M, Carella AM, Haenel M, Boissevain F, Zschaber R,
Mueller P, Kirchner H, Lohri A, Decker S, Koch B, Hasenclever D, Goldstone AH, Diehl V. Aggressive conventional chemotherapy compared with high-dose chemotherapy requiring autologous hemopoietic stem cell transplantation for relapsed chemosensitive Hodgkin´s disease. Lancet (in press) INT
Speakers’ Midterm Report: Section 1
14
Porzsolt F, Stengel D, Flatau B, Thurmayr R, Ohletz A, Schmitz S, Tsamaloukas A, Aly A-F. Dissemination of methods for appraisal of health care services: Diagnostic tools. Gesundheitsökonomie & Qualitätsmanagement (in press) 2002
Uppenkamp M, Engert A, Diehl V, Bunjes D, Huhn D, Brittinger G. Monoclonal antibody therapy with CAMPATH-1H in patients with relapsed high- and low-grade Non-Hodgkin's lymphomas: a multicenter phase I/II study. Ann Hematol. 2002 Jan;81(1):26-32.
Sieber M, Tesch H, Pfistner B, Rueffer U, Lathan B, Brosteanu O, Paulus U, Koch T,
Pfreundschuh M, Loeffler M, Engert A, Josting A, Wolf J, Hasenclever D, Franklin J, Duehmke E, Georgii A, Schalk KP, Kirchner H, Doelken G, Munker R, Koch P, Herrmann R, Greil R, Anselmo AP, Diehl V. Rapidly alternating COPP/ABV/IMEP is not superior to conventional alternating COPP/ABVD in combination with extended-field radiotherapy in intermediate-stage Hodgkin's lymphoma: Final results of the German Hodgkin’s Lymphoma Study Group trial HD5. J Clin Oncol. 2002 Jan 15;20(2):476-84. NET
Re D, Benenson L, Wickenhauser C, Starostik P, Staratschek-Jox A, Muller-Hermelink HK,
Diehl V, Wolf J. Proficient mismatch repair protein expression in Hodgkin and Reed Sternberg cells. Int J Cancer. 2002 Jan 10;97(2):205-10.
Josting A, Franklin J, May M, Koch P, Beykirch MK, Heinz J, Rudolph C, Diehl V, Engert A.
New prognostic score based on treatment outcome of patients with relapsed Hodgkin's lymphoma registered in the database of the German Hodgkin's Lymphoma Study Group. J Clin Oncol. 2002 Jan 1;20(1):221-30.
2001 Trumper L, Jung W, Daus H, Mechtersheimer G, von Bonin F, Pfreundschuh M.
Assessment of clonality of rosetting T lymphocytes in Hodgkin's disease by single-cell polymerase chain reaction: detection of clonality in a polyclonal background in a case of lymphocyte predominance Hodgkin's disease. Ann Hematol. 2001 Nov;80(11):653-61.
Gandjour A, Lauterbach KW.
A method for assessing the cost-effectiveness and the break-even point of clinical practice guidelines. Int J Technol Assess Health Care. 2001 Fall;17(4):503-16.
Kunzmann V, Ruediger T, Hallek M, Mueller-Hermelink HK, Wilhelm M.
Tumor cell agglutination and not solely cytokine release as mechanism of adverse reactions during anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab) treatment. Blood. 2001 Sep 15;98(6):1991-2.
Hallek M, Schmitt B, Wilhelm M, Busch R, Krober A, Fostitsch HP, Sezer O, Herold M, Knauf W, Wendtner CM, Kuse R, Freund M, Franke A, Schriever F, Nerl C, Dohner H, Thiel E, Hiddemann W, Brittinger G, Emmerich B. Fludarabine plus cyclophosphamide is an efficient treatment for advanced chronic lymphocytic leukemia (CLL): results of a phase II study of the German CLL Study Group. Br J Hematol. 2001 Aug;114(2):342-8. NET
Speakers’ Midterm Report: Section 1
15
Sweetenham JW, Santini G, Qian W, Guelfi M, Schmitz N, Simnett S, Nagler A, Holte H, Kvaloy S, Bruzzi P, Goldstone AH. High-dose therapy and autologous stem cell transplantation versus conventional-dose consolidation/maintenance therapy as postremission therapy for adult patients with lymphoblastic lymphoma: results of a randomised trial of the European Group for Blood and Marrow Transplantation and the United Kingdom Lymphoma Group. J Clin Oncol. 2001 Jun 1;19(11):2927-36. INT
Duhmke E, Franklin J, Pfreundschuh M, Sehlen S, Willich N, Ruhl U, Muller RP, Lukas P, Atzinger A, Paulus U, Lathan B, Ruffer U, Sieber M, Wolf J, Engert A, Georgii A, Staar S, Herrmann R, Beykirch M, Kirchner H, Emminger A, Greil R, Fritsch E, Koch P, Drochtert A, Brosteanu O, Hasenclever D, Loeffler M, Diehl V. Low-dose radiation is sufficient for the noninvolved extended-field treatment in favorable early-stage Hodgkin's disease: long-term results of a randomised trial of radiotherapy alone. J Clin Oncol. 2001 Jun 1;19(11):2905-14. NET
Rueffer U, Josting A, Franklin J, May M, Sieber M, Breuer K, Engert A, Diehl V.
Non-Hodgkin's lymphoma after primary Hodgkin's disease in the German Hodgkin’s Lymphoma Study Group: incidence, treatment, and prognosis. J Clin Oncol. 2001 Apr 1;19(7):2026-32.
Bentz M, Barth TF, Bruderlein S, Bock D, Schwerer MJ, Baudis M, Joos S, Viardot A, Feller
AC, Muller-Hermelink HK, Lichter P, Dohner H, Moller P. Gain of chromosome arm 9p is characteristic of primary mediastinal B-cell lymphoma (MBL): comprehensive molecular cytogenetic analysis and presentation of a novel MBL cell line. Genes Chromosomes Cancer. 2001 Apr;30(4):393-401.
Pfreundschuh M, Hasenclever D, Loeffler M, Ehninger G, Schmitz N, Kirchner H, Koch P,
Lathan B, Rueffer U, Sextro M, Franklin J, Tesch H, Diehl V. Dose escalation of cytotoxic drugs using hematopoietic growth factors: a randomised trial to determine the magnitude of increase provided by GM-CSF. Ann Oncol. 2001 Apr;12(4):471-7. NET
Williams CD, Harrison CN, Lister TA, Norton AJ, Blystad AK, Coiffier B, Taghipour G,
Schmitz N, Goldstone AH. High-dose therapy and autologous stem cell support for chemosensitive transformed low-grade follicular Non-Hodgkin's lymphoma: a case-matched study from the European Bone Marrow Transplant Registry. J Clin Oncol. 2001 Feb 1;19(3):727-35. INT
Willich NA, Reinartz G, Reers B, Hiddemann W, Tiemann M, Parwaresch R, Grothaus-Pinke B, Kocik J, Koch P. Radiotherapy in early stage gastrointestinal lymphoma: results of the German GIT-NHL group. Ann Hematol. 2001;80 Suppl 3:B97-9. NET
Rube C, Nguyen TP, Kloss M, Loeffler M, Trumper L, Pfreundschuh M. Consolidation radiotherapy to bulky disease in aggressive NHL. First results of the NHL B-94 trial of the DSHNHL. Ann Hematol. 2001;80 Suppl 3:B84-5. NET
Speakers’ Midterm Report: Section 1
16
Hasenclever D, Loeffler M. Five theses concerning the clinical consequences of pathology and prognostic factors. Ann Hematol. 2001;80 Suppl 3:B58-60.
2000
Anagnostopoulos I, Hansmann ML, Franssila K, Harris M, Harris NL, Jaffe ES, Han J, van Krieken JM, Poppema S, Marafioti T, Franklin J, Sextro M, Diehl V, Stein H. European Task Force on Lymphoma project on lymphocyte predominance Hodgkin’s disease: histologic and immunohistologic analysis of submitted cases reveals 2 types of Hodgkin’s disease with a nodular growth pattern and abundant lymphocytes. Blood. 2000 Sep 1;96(5):1889-99. NET, INT
Engel C, Loeffler M, Schmitz S, Tesch H, Diehl V. Acute hematologic toxicity and practicability of dose-intensified BEACOPP chemotherapy for advanced stage Hodgkin's disease. German Hodgkin’s Lymphoma Study Group (GHSG). Ann Oncol. 2000 Sep;11(9):1105-14. NET
Feuring-Buske M, Kneba M, Unterhalt M, Engert A, Gramatzki M, Hiller E, Trumper L, Brugger W, Ostermann H, Atzpodien J, Hallek M, Aulitzky E, Hiddemann W. IDEC-C2B8 (rituximab) anti-CD20 antibody treatment in relapsed advanced-stage follicular lymphomas: results of a phase-II study of the German Low-Grade Lymphoma Study Group. Ann Hematol. 2000 Sep;79(9):493-500. NET
Josting A, Rueffer U, Franklin J, Sieber M, Diehl V, Engert A. Prognostic factors and treatment outcome in primary progressive Hodgkin’s lymphoma: a report from the German Hodgkin’s Lymphoma Study Group. Blood. 2000 Aug 15;96(4):1280-6.
Ott MM, Rosenwald A, Katzenberger T, Dreyling M, Krumdiek AK, Kalla J, Greiner A, Ott G, Muller-Hermelink HK. Marginal zone B-cell lymphomas (MZBL) arising at different sites represent different biological entities. Genes Chromosomes Cancer. 2000 Aug;28(4):380-6.
Assaf C, Hummel M, Dippel E, Goerdt S, Muller HH, Anagnostopoulos I, Orfanos CE, Stein H. High detection rate of T-cell receptor beta chain rearrangements in T-cell lymphoproliferations by family specific polymerase chain reaction in combination with the GeneScan technique and DNA sequencing. Blood. 2000 Jul 15;96(2):640-6. INT
Santoro A, Bredenfeld H, Devizzi L, Tesch H, Bonfante V, Viviani S, Fiedler F, Parra HS, Benoehr C, Pacini M, Bonadonna G, Diehl V. Gemcitabine in the treatment of refractory Hodgkin's disease: results of a multicenter phase II study. J Clin Oncol. 2000 Jul;18(13):2615-9. INT
Franklin J, Paulus U, Lieberz D, Breuer K, Tesch H, Diehl V. Is the international prognostic score for advanced stage Hodgkin's disease applicable to early stage patients? German Hodgkin’s Lymphoma Study Group. Ann Oncol. 2000 May;11(5):617-23.
Speakers’ Midterm Report: Section 1
17
Josting A, Reiser M, Wickramanayake PD, Rueffer U, Draube A, Sohngen D, Tesch H, Wolf J, Diehl V, Engert A. Dexa-BEAM: an effective regimen for cytoreduction prior to high-dose chemotherapy with autologous stem cell support for patients with relapsed/refractory mantle-cell lymphoma. Leuk Lymphoma. 2000 Mar;37(1-2):185-7.
Josting A, Reiser M, Wickramanayake PD, Rueffer U, Draube A, Sohngen D, Tesch H, Wolf J, Diehl V, Engert A. Dexamethasone, carmustine, etoposide, cytarabine, and melphalan (dexa-BEAM) followed by high-dose chemotherapy and stem cell rescue - a highly effective regimen for patients with refractory or relapsed indolent lymphoma. Leuk Lymphoma. 2000 Mar;37(1-2):115-23.
von Wasielewski R, Seth S, Franklin J, Fischer R, Hubner K, Hansmann ML, Diehl V, Georgii A. Tissue eosinophilia correlates strongly with poor prognosis in nodular sclerosing Hodgkin's disease, allowing for known prognostic factors. Blood. 2000 Feb 15;95(4):1207-13.
Lieberz D, Sextro M, Paulus U, Franklin J, Tesch H, Diehl V. How to restrict liver biopsy to high-risk patients in early-stage Hodgkin's disease. German Hodgkin’s Lymphoma Study Group. Ann Hematol. 2000 Feb;79(2):73-8.
Pfistner B, Paulus U, Glossmann JP, Walshe R, Tesch H, Diehl V. Can factors influencing in-patient treatment in Hodgkin's disease be identified? - Retrospective analysis of HD6 patients of the GHSG. Stud Health Technol Inform. 2000;77:399-403.
Speakers’ Midterm Report: Section 1
18
Part B – Network Organisation and Management
B-4. a) Which instruments were implemented to assure the quality and efficiency of the
collaboration within the network?
assessment of the progress of projects
joint measures for scientific/methodological quality assurance
joint measures for quality assurance of medical care
mechanisms for the management of conflicts between network members
mechanisms for the controlling of finances
questionings concerning satisfaction of network members and external clients with the network
mechanisms for the acceptance of new projects within the network
mechanisms for the dismissal of unsuccessful projects
other instruments b) List eventually newly accepted projects and/or dismissed projects.
Sub-project 8a: EbM – Meta Analysis not continued Sub-project 12: Epidemiology newly accepted Sub-project 13: Biologic Risk Factors newly accepted
c) Describe each of the instruments and mechanisms used in your network so far;
report the results achieved and problems with the handling of the instruments. Describe the proposed activities for the second funding period.
The rules of the competence network define the different categories of membership and the obligations of each member. In this way, the rules serve as an essential instrument for the network’s internal quality control. Further essential instruments are the annual reports of each sub-project as well as the project leader meetings.
In the annual reports, the project leaders inform about the results achieved and the use of funds. The annual reports have to be submitted to the speaker of the network. By this means, the speaker receives a detailed survey of the current state of the funded projects.
Speakers’ Midterm Report: Section 1
19
In addition, the project leaders meet twice per year. For one of these meetings, they have to prepare a summary and a report on the results achieved during the last year. On the one hand, all project leaders are thus informed about the ongoing projects. On the other hand, these meetings serve as an excellent discussion platform for medical/scientific and health care issues. In one of these meetings, the idea to establish an epidemiological working group was born. In the following, three groups engaged in epidemiology of lymphoma were invited to present their proposals. These proposals were taken to design a common working plan for the competence network. On behalf of this group, Dr. Hoffmann (Bremen) submitted a new proposal for the next funding period.
The meeting of the project leaders was also utilised to present the proposals for the next funding period. These proposals were evaluated by an internal committee elected for this purpose. Based on the recommendations of this committee, the board of directors decided on the acceptance of projects for the new common proposal of the competence network.
All members of the network, i.e. the project leaders and their co-investigators, participate in the network’s general meetings that take place once per year. If a new project has been proposed, it has to be accepted by the members of the network. In the case of acceptance, the project leader or the chairman of a working group will become an associate member of the network.
Both kinds of meetings not only serve as a discussion platform but also as an opportunity to discuss and manage potential conflicts within the network. If conflicts cannot be solved in these meetings, the discussion is forwarded to the board of directors.
To assure the quality of medical care, of related clinical trials and of methodological approaches, a working group “Quality Management” has been established. This working group is integrated in sub-project 2; the corresponding results and proposed future activities have been described in detail in section 3 of this sub-project. One of the most important approaches of this group is to prepare GCP-like guidelines for the ongoing and planned lymphoma studies. Moreover, network assistants regularly visit the hematological departments of non-university hospitals to support them in the documentation of the clinical trials run by the competence network. In general, the topics “quality management” and “evidence-based medicine” are addressed by several sub-projects of the network. For detailed information, please refer to the corresponding chapters of section 3.
For the next funding period, questionings concerning satisfaction of network members and external partners are being prepared. To facilitate the controlling of finances, a central administration of finances is planned. Beyond that, the arrangements to assure the quality and efficiency of networking will be continued as before.
B-5. a) Which organisational support and services for network partners are provided by
the network?
organisation of scientific and network meetings providing information about the state of the projects for the network
partners
brokerage of general information
providing information about the availability of devices and materials among the partner institutions
arrangement of joint purchases of devices, licenses etc.
Speakers’ Midterm Report: Section 1
20
set up, maintenance of, and user support for material banks
set up, maintenance of, and user support for data banks
set up, maintenance of, and user support for information and
knowledge services
providing advice on the requirements concerning:
ethics
biometry
human genome and gene technology
clinical pharmacology
patents
funding and legal requirements
others
set up and maintenance of reference centres coordination of clinical studies providing advice for media presentation other services and support, please list
§ Evidence-based Medicine
b) Describe each of the services which have been installed and which expert advice
and support is provided in your network so far, and describe the proposed activities for the second funding period.
One of the most important tasks of the network’s central office (sub-project 1) is to provide organisational support for the network partners. In a similar way, sub-project 2 (Telematics & Quality Management) provides IT support. These services are described in detail in the corresponding reports and proposals in section 3. For further information, please refer to the following chapter of this section, where the IT techniques used for networking will be described. Organisation of scientific and network meetings
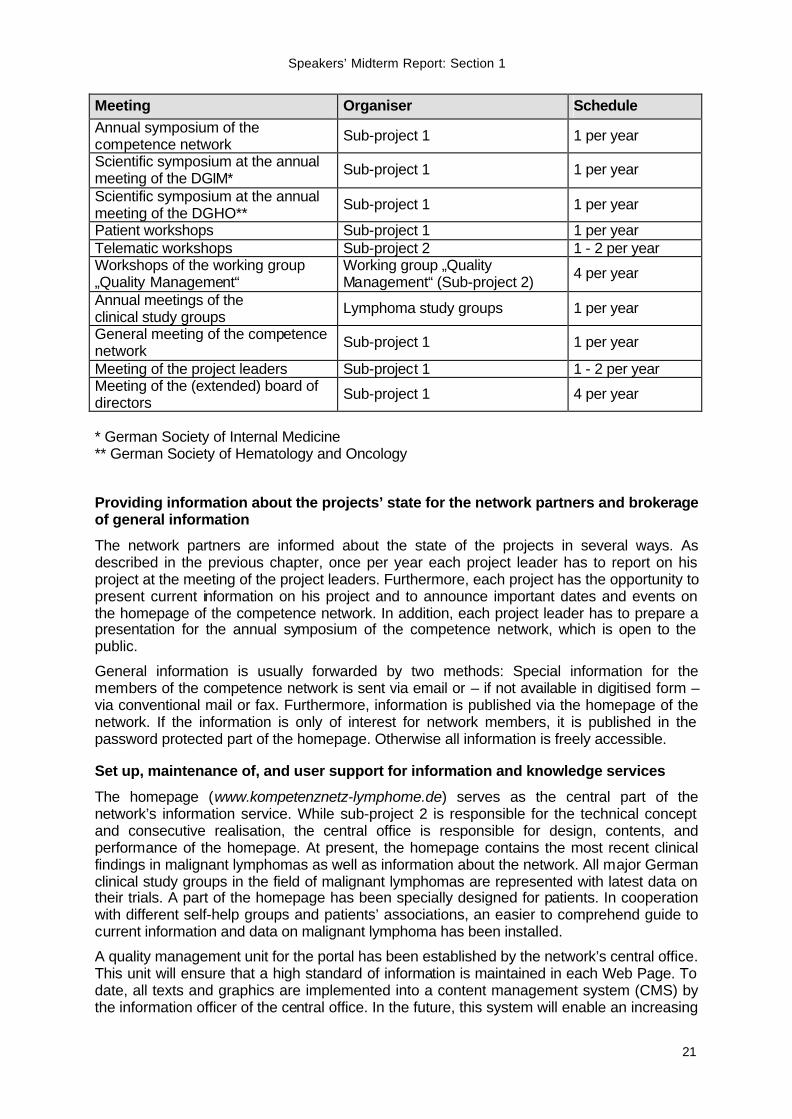
The following table gives an overview of the meetings and symposia, which are organised by the network on a regular basis. Members of the network organise further meetings on the occasion of various scientific meetings.
Speakers’ Midterm Report: Section 1
21
Meeting Organiser Schedule Annual symposium of the competence network Sub-project 1 1 per year
Scientific symposium at the annual meeting of the DGIM* Sub-project 1 1 per year
Scientific symposium at the annual meeting of the DGHO** Sub-project 1 1 per year
Patient workshops Sub-project 1 1 per year Telematic workshops Sub-project 2 1 - 2 per year Workshops of the working group „Quality Management“
Working group „Quality Management“ (Sub-project 2) 4 per year
Annual meetings of the clinical study groups Lymphoma study groups 1 per year
General meeting of the competence network Sub-project 1 1 per year
Meeting of the project leaders Sub-project 1 1 - 2 per year Meeting of the (extended) board of directors Sub-project 1 4 per year
* German Society of Internal Medicine ** German Society of Hematology and Oncology Providing information about the projects’ state for the network partners and brokerage of general information
The network partners are informed about the state of the projects in several ways. As described in the previous chapter, once per year each project leader has to report on his project at the meeting of the project leaders. Furthermore, each project has the opportunity to present current information on his project and to announce important dates and events on the homepage of the competence network. In addition, each project leader has to prepare a presentation for the annual symposium of the competence network, which is open to the public.
General information is usually forwarded by two methods: Special information for the members of the competence network is sent via email or – if not available in digitised form – via conventional mail or fax. Furthermore, information is published via the homepage of the network. If the information is only of interest for network members, it is published in the password protected part of the homepage. Otherwise all information is freely accessible. Set up, maintenance of, and user support for information and knowledge services
The homepage (www.kompetenznetz-lymphome.de) serves as the central part of the network’s information service. While sub-project 2 is responsible for the technical concept and consecutive realisation, the central office is responsible for design, contents, and performance of the homepage. At present, the homepage contains the most recent clinical findings in malignant lymphomas as well as information about the network. All major German clinical study groups in the field of malignant lymphomas are represented with latest data on their trials. A part of the homepage has been specially designed for patients. In cooperation with different self-help groups and patients’ associations, an easier to comprehend guide to current information and data on malignant lymphoma has been installed.
A quality management unit for the portal has been established by the network’s central office. This unit will ensure that a high standard of information is maintained in each Web Page. To date, all texts and graphics are implemented into a content management system (CMS) by the information officer of the central office. In the future, this system will enable an increasing
Speakers’ Midterm Report: Section 1
22
number of online editors to provide a highly dynamic stream of information on several topics. The CMS is available via sub-project 2 and it is part of the IT infrastructure in Leipzig. Arrangement of joint purchases of devices and licenses
One of the major tasks of sub-project 2 has been to design and realise an IT communication system for the network. In the first funding period, the server, network and telecommunication technology for the communication centre in Leipzig and the three study centres in Cologne, Leipzig and Munich was put into operation. For this purpose, the hard- and software and corresponding licenses were purchased by sub-project 2 and forwarded to the study groups. As outlined above, the content management system to install and to maintain the information portal of the network is also provided by sub-project 2. In a similar approach, sub-project 4 purchased the equipment for installing the telemedical devices connecting the reference centres of radiotherapy within the network. Coordination of clinical studies, providing advice on the requirements concerning biometry and ethics
The clinical study groups of the competence network are equipped with coordination centres having expertise in clinical data management and biometry. For the members participating in the corresponding studies, these coordination centres provide medical consulting service and advice in other issues, e.g. for the submission of study protocols to the ethics committee. In order to harmonise the procedures within the centres, the quality management group of the competence network has designed a suitable system of standard operating procedures for the study centres. Furthermore, the working group develops appropriate methods for the evaluation of quality assurance and its review process in the study groups. Maintenance of reference centres, maintenance and user support for material and data banks
All tissue materials of patients enrolled in the clinical trials of the study groups integrated in the Competence Network Malignant Lymphoma are collected in the associated reference centres for lymph node pathology. Within sub-project 3 a central database for the material will be established. While the frozen and paraffin-embedded tissue blocks are stored at the reference centres, the database will be centralised at the pathology server in Leipzig (IMISE). All available material information will be directly linked to corresponding patient data at the coordination centres of the clinical trials.
The evaluation of biological parameters through lymphoma research projects requires a collection of fresh tissue materials. Therefore it is the key goal of a new sub-project termed “Improvement of the infrastructure for the analysis of biologic risk factors in malignant lymphomas” to provide an optimised infrastructure for the collection of fresh tumour tissue at the pathology reference centres. For further information on the central database, the new sub-project and the collection of sera and blood samples from patients with aggressive lymphomas by the DSHNHL, please refer to section 1, part C-12. Evidence-based medicine
Sub-project 8b founded the Cochrane group “Hematological Malignancies”. Within the first funding period, the group has already published eight Cochrane reviews. Furthermore, the group provides advice on how to prepare protocols and reviews according to the Cochrane guidelines. As outlined in various other chapters, sub-project 5 organises a special course on evidence-based medicine for private practitioners. A detailed description is given in the report of sub-project 5 in section 3.
Speakers’ Midterm Report: Section 1
23
Proposed activities
The services of the network will be extended in two fields:
Information on funding and legal requirements will be provided for the network partners, as the competence network has to develop and realise a strategy to maintain the network after the second funding period.
Furthermore, it is planned to provide advice for media presentations. Moreover, standardised templates for presentations and documents will be designed. Scientists, who often have to present their projects and the results of their research to public media should get the opportunity to attend media training specially designed for scientists. In this field, we intend to cooperate with other scientific institutions (e.g. Forschungszentrum Jülich).
B-6. a) Which IT techniques are used for networking?
network web-site
information server
network mailing-address
IT support for clinical studies (remote data entry or other)
electronic access to databanks
patient databanks
gene databanks
other databanks, please list
other IT techniques
§ Technical equipment b) Describe each of the strategies used for networking so far and problems with the
handling of the techniques. Describe the proposed activ ities for the second funding period.
Technical equipment
The server, network, and communication technology has been obtained, configured, and after a test phase put into service (see also sub-project 2). An IT security concept is being developed, the competence network’s server data is backed up regularly, a firewall saves the network of the IT communication central. The competence network’s partners communicate using encryption facilities via Internet as well as via ISDN router. In the second funding period the security concept will be implemented into the central network’s IT communication as well as into the local places of the partners.
Speakers’ Midterm Report: Section 1
24
Network web-site and information server
Due to the high requirements and resulting complexity in the management and maintenance of the information service, it is necessary to use suitable tools. After having carefully evaluated a number of different systems, the content management system (CMS) VIP by Gauss Interprise was chosen. An information and editorial server was installed in order to satisfy the CMS’s technical requirements, which is the basis for the network’s homepage. For storage of user, group and role data and for user authentication a central directory service was developed on the basis of the standard protocol lightweight directory access protocol (LDAP). In the second funding period the information service will be extended to an information and communication portal with further functionalities (e.g. groupware) and integrated applications for clinical trials. Distributed editor working places will be established on the basis of a multilevel concept for quality management processes.
Network mailing-address
Each member of the network has the possibility to use its own network email-address <[email protected]> as forwarding email-address. IT support for clinical studies
Following IT projects support clinical trials: SOP Management Tool, Data Dictionary (OntoBuilder), Therapy Guide, Therapy Management Guide, Central Pathology Database. Electronic access to patients’ databases
Based on the IT infrastructure, communication facilities between the competence network’s partners are being established to enable data and information exchange. Observing data privacy requirements, only pseudonymised patients data is exchanged. The pseudonyms are created using a minimal data set. This minimal data set was defined to identify patients in the competence network.
Speakers’ Midterm Report: Section 1
25
Part C – Added Value through Networking
C-7. Cooperation within the network
Design a matrix of the network projects indicating all research groups actively involved in each individual research project. Include associated projects which are funded through other funding organisations (DFG, EU, BMG, foundations, industry) and mark the respective funding organisation in footnotes.
§ See annex after “Cooperation with other Networks” (C-8)
C-8. Cooperation with other networks In which of the following network-overlapping joint activities is the network collaborating?
Telematic Platform
Brain-Net
Public Relations Team
other fields of cooperation
Telematic Platform
The BMBF installed a central telematic platform (TMF) in April 1999 with a management office at the “Fraunhofer Institut für Software und Systemtechnik” (ISST) in Berlin. Within the TMF, comprehensive solutions to general telematic problems are elaborated and shared by the different medical research networks (i.e. competence networks, coordination centres for clinical trials). General objectives of the TMF are focused on the effective application of financial and personal resources through the development of telematic infrastructure. The TMF established three working groups within the following main subjects:
1. Data security and confidentiality • General data protection requirements in research networks • Pseudonymisation of data and its implementation • Development of data security concepts for medical research collaborators
2. IT quality management • Web-based communication infrastructure • Guidelines for basic documentation of IT projects
3. System components for medical research and clinical trials • Installation and operation of an information and knowledge portal based on content
management systems (CMS) • Evaluation of clinical research software enabling electronic data collection (EDC)
and remote data entry (RDE). Software implementation with guidelines and suggestions for different medical research networks.
Added value and proposed activities With regards to the work on data security and confidentiality the Competence Network Malignant Lymphoma has written three research proposals as part of a research programme of the TMF. In addition, the network has appointed a coordinator for data security and
Speakers’ Midterm Report: Section 1
26
confidentiality. This coordinator will support the projects in finding solutions for current problems and gather information on emerging problems on data security and confidentiality in general.
Within the working group “System Components for Medical Research and Clinical Trials”, the network’s sub-project 2 gained special expertise in content management systems (CMS). They have been assigned to carry out a consulting project with the objective to evaluate the use of a CMS in medical research networks. The network’s CMS (see sub-project 2) has become an essential part of the information portal with an increasing amount of online editors.
The initial projects of the TMF will be continued in the second funding period. Results of the working groups are expected to contribute towards finding telematic solutions in different network sub-projects.
Public Relations Team
Contributions of our network The public relations officer of the network regularly takes part in the Public Relations Team of the ‘Competence Networks in Health Research’ since the very beginning of this group in March 2001. She has especially been involved in the preparation and support of the information booth presented for the first time on the “Science Street” in Cologne, October/November 2001. Moreover, she has supported the press officer of the Competence Network Rheumatism in preparing the first joint press conference of the networks (December 2001). She has published a press release to make known the joint web site of the Competence Networks in Health Research. Since March 2002 she is the coordinator of the group.
The projects of the Public Relations Team In cooperation with the DLR/PT, the team has published a joint press kit and an information brochure on the Competence Networks in Health Research, and each network has provided information for the joint web site (www.kompetenznetze-medizin.de). Moreover, an information booth, which may be used repeatedly, has been designed and utilised for the first time on the occasion of the “Science Street” in Cologne, October 30 – November 08, 2001. A press release on the joint web site has been published, and a press conference has been held on the occasion of the networks’ meeting in Darmstadt.
Added value The Competence Network Malignant Lymphoma experiences an added value from the activities of the Public Relations Team as synergistic effects will emerge and the term “Kompetenznetz” will become kind of a brand name. Additional attention from media and general public is to be expected. Moreover, our network benefits from the presentations of the Competence Networks in Health Care in print media as well as on joint web sites.
Proposed activities The projects, which have been initiated by the Public Relations Team so far, shall be continued in the second funding period. The competence networks will be presented on selected medical congresses and events for general public using the information booth. It is intended to hold one common press conference per year. Further print material and press releases will be published if necessary. Other fields of cooperation
The Competence Networks Malignant Lymphoma and Leukemia are organising joint symposia on the occasion of the annual meetings of the “Deutsche Gesellschaft für Innere Medizin” and the “Deutsche Gesellschaft für Hämatologie and Onkologie (DGHO)”. Both networks will be organisers of a patients’ seminar scheduled for the next annual meeting of DGHO in October 2002.
Speakers’ Midterm Report: Section 1
27
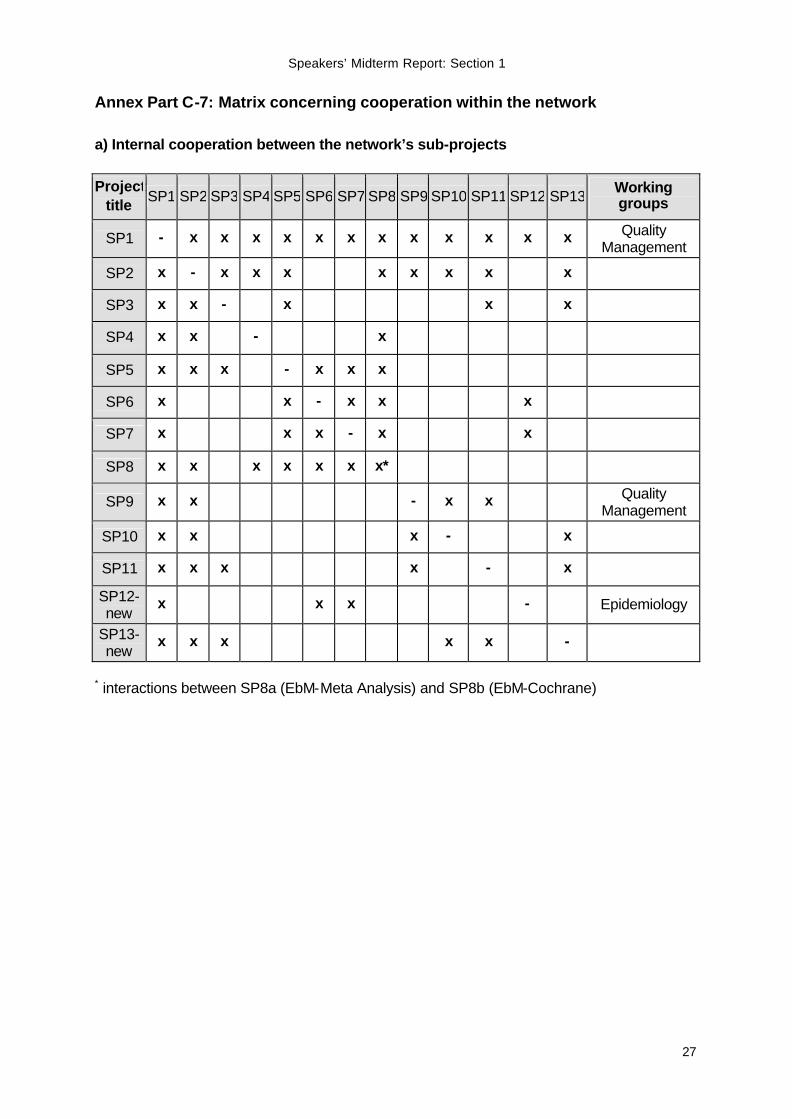
Annex Part C-7: Matrix concerning cooperation within the network
a) Internal cooperation between the network’s sub-projects Project
title SP1 SP2 SP3 SP4 SP5 SP6 SP7 SP8 SP9 SP10 SP11 SP12 SP13 Working groups
SP1 - x x x x x x x x x x x x Quality Management
SP2 x - x x x x x x x x
SP3 x x - x x x
SP4 x x - x
SP5 x x x - x x x
SP6 x x - x x x
SP7 x x x - x x
SP8 x x x x x x x*
SP9 x x - x x Quality Management
SP10 x x x - x
SP11 x x x x - x
SP12-new
x x x - Epidemiology
SP13-new
x x x x x -
* interactions between SP8a (EbM-Meta Analysis) and SP8b (EbM-Cochrane)
Speakers’ Midterm Report: Section 1
28
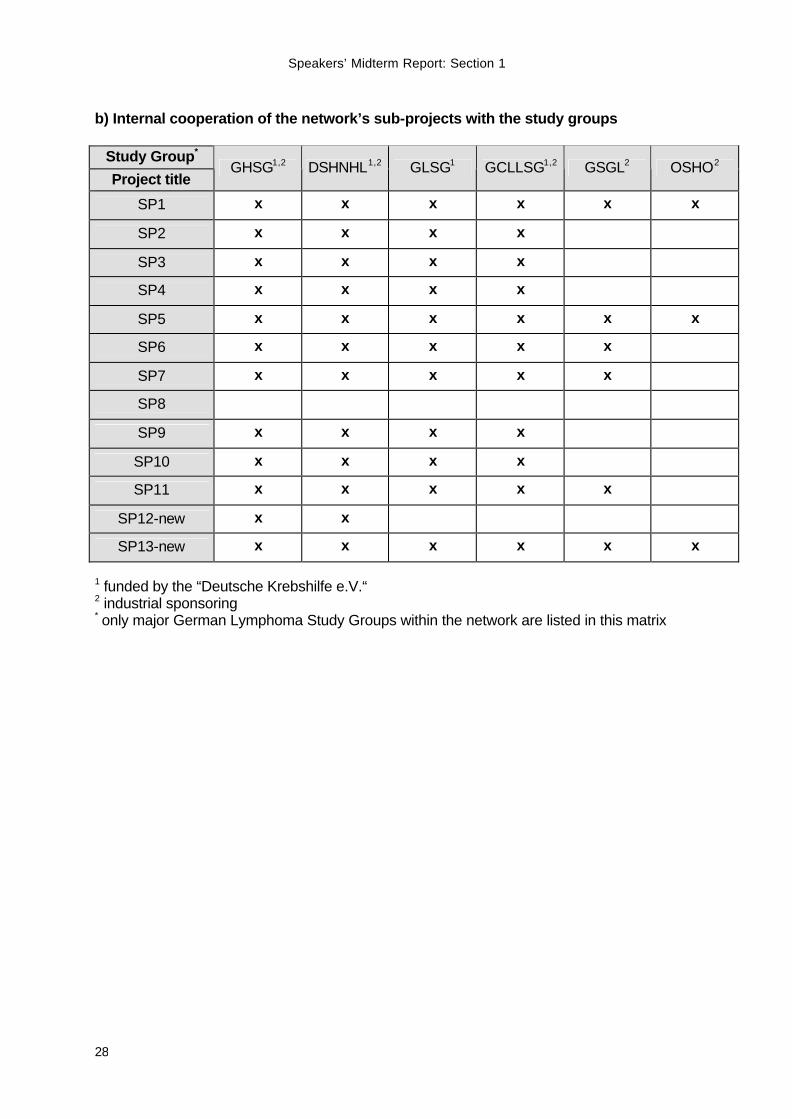
b) Internal cooperation of the network’s sub-projects with the study groups
Study Group*
Project title GHSG1,2 DSHNHL1,2 GLSG1 GCLLSG1,2 GSGL2 OSHO2
SP1 x x x x x x
SP2 x x x x
SP3 x x x x
SP4 x x x x
SP5 x x x x x x
SP6 x x x x x
SP7 x x x x x
SP8
SP9 x x x x
SP10 x x x x
SP11 x x x x x
SP12-new x x
SP13-new x x x x x x
1 funded by the “Deutsche Krebshilfe e.V.“ 2 industrial sponsoring * only major German Lymphoma Study Groups within the network are listed in this matrix
Speakers’ Midterm Report: Section 1
29
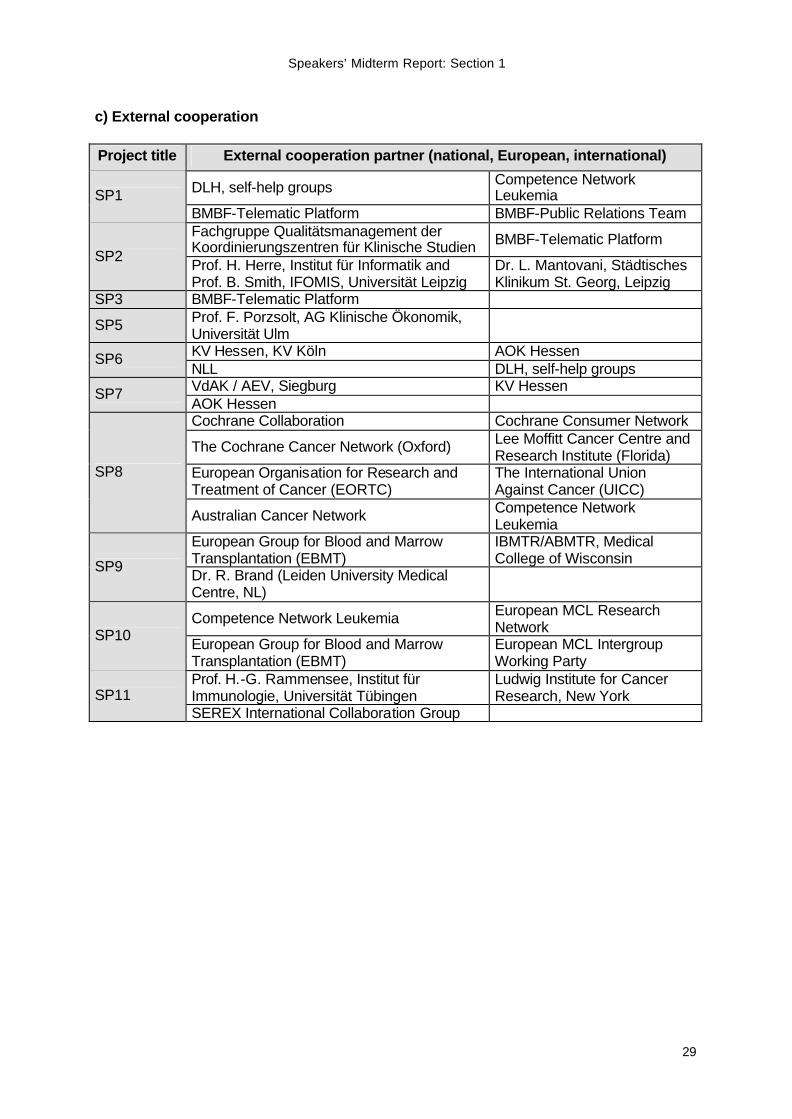
c) External cooperation
Project title External cooperation partner (national, European, international)
DLH, self-help groups Competence Network Leukemia SP1
BMBF-Telematic Platform BMBF-Public Relations Team Fachgruppe Qualitätsmanagement der Koordinierungszentren für Klinische Studien BMBF-Telematic Platform
SP2 Prof. H. Herre, Institut für Informatik and Prof. B. Smith, IFOMIS, Universität Leipzig
Dr. L. Mantovani, Städtisches Klinikum St. Georg, Leipzig
SP3 BMBF-Telematic Platform
SP5 Prof. F. Porzsolt, AG Klinische Ökonomik, Universität Ulm
KV Hessen, KV Köln AOK Hessen SP6 NLL DLH, self-help groups VdAK / AEV, Siegburg KV Hessen SP7 AOK Hessen Cochrane Collaboration Cochrane Consumer Network
The Cochrane Cancer Network (Oxford) Lee Moffitt Cancer Centre and Research Institute (Florida)
European Organisation for Research and Treatment of Cancer (EORTC)
The International Union Against Cancer (UICC)
SP8
Australian Cancer Network Competence Network Leukemia
European Group for Blood and Marrow Transplantation (EBMT)
IBMTR/ABMTR, Medical College of Wisconsin SP9 Dr. R. Brand (Leiden University Medical
Centre, NL)
Competence Network Leukemia European MCL Research Network SP10 European Group for Blood and Marrow
Transplantation (EBMT) European MCL Intergroup Working Party
Prof. H.-G. Rammensee, Institut für Immunologie, Universität Tübingen
Ludwig Institute for Cancer Research, New York SP11
SEREX International Collaboration Group
Speakers’ Midterm Report: Section 1
30
Part C – Added Value through Networking
C-9. a) Are clinical multi-centre studies performed in your network?
no yes
§ See annex after “Patient documentation” (C-11)
b) if yes, give the following numbers: total number of multi-centre studies
§ GHSG: 5 § DSHNHL: 6 concluded and 4 ongoing studies § GLSG: 5
total number of network members involved
§ All study groups of the competence network. number of multi-centre studies which have been newly initiated since the network exists
§ GHSG: 2 § DSHNHL: 5 § GLSG: 2
number of study groups which have started substantial cooperation through the network
§ Each of the study groups of the Competence Network Malignant Lymphoma started substantial cooperation with the others, e. g. for the improvement of study quality (see C-11 and sub-project 2)
number of new study groups which result from activities of the network
§ The German Study Group Gastro-intestinal Lymphoma (GSGL). c) Describe the activities and problems concerning clinical studies so far and
describe the proposed activities for the second funding period.
The lymphoma study groups of the Competence Network Malignant Lymphoma carry out a large number of multi-centre studies. In these studies numerous clinical institutions participate including institutions from neighbouring European countries. The clinical trials of the German Hodgkin's Lymphoma Study Group (GHSG) involve more than 400 clinical centres including university hospitals, community hospitals and private hemato-oncology practices. Altogether, more than 8.000 patients are registered in the database of the GHSG. The German High-Grade Non-Hodgkin’s Lymphoma Study Group (DSHNHL) recruited more than 2500 patients from more than 150 centres in clinical phase I/II and phase III trials. The
Speakers’ Midterm Report: Section 1
31
German Low-grade Lymphoma Study Group (GLSG) recruited over 1500 patients from more than 250 clinical institutions.
The competence network represents an essential platform for the interaction of the lymphoma study groups. Therefore its aim is to be open for all groups working in research and treatment of lymphoma. In consequence, the network invited interested groups to submit an application for an association. To date, five additional study groups (GCLLSG, GSGL, OSHO, PT-LPD, Radioimmunotherapy in Malignant Lymphoma) have been associated with the network. The GSGL formed itself out of three smaller groups on the initiative of the competence network.
The improvement of quality in all aspects of lymphoma treatment is an aim spanning all sub-projects of the competence network. One important aspect is to improve and simplify the interaction and communication between all professionals involved. Most clinical studies performed in the network are quality assurance protocols, i.e. trials for the optimisation of therapy, rather than new drug approvals. Therefore, it is the aim to interpret the guidelines for good clinical practice (GCP) as defined by the “International Conference on Harmonisation of Guidelines” and put them into defined terms for this kind of protocol. The working group on quality management (WG-QM) develops a suitable system of SOPs for study centres. Furthermore, the WG-QM develops appropriate methods for the evaluation of quality assurance and its review process in the study groups. In a third aspect, the competence network aims toward harmonisation of case report forms (CRFs) and clinical definitions. Here the network assistants of the competence network have an important influence on the quality management. They compare the methods of documentation and definitions of terms between the three study groups and are involved in the consensus process coordinated by the WG-QM (see sub-project 1).
The private practices for hematology and oncology are important partners of the clinical study groups, especially since a growing number of lymphoma patients is treated outside of hospitals (outpatients). The private practices within the competence network (sub-project 5) support the quality assurance protocols of the study groups by recruiting patients into their studies. To increase the number of outpatients in clinical studies, the project tries to optimise the inclusion process of patients from private practices. The organisational structures of private practices for hematology and oncology are usually highly complex. If patients are to be successfully included, the necessary steps must be incorporated into the everyday routine of the practices. Different workflow models were elaborated for this purpose. They are currently being implemented and optimised in two pilot practices. Recommendations and proposals for other practices are to be developed on the basis of the results obtained.
The clinical studies of the Competence Network Malignant Lymphoma and their associated projects have a profound impact on the health care system with regard to lymphoma therapy. A major problem for the future of clinical studies in Germany is the refusal of some health insurances to pay for the standard therapy of patients enrolled in clinical studies. Therefore further information on activities, problems and future goals of the network concerning clinical studies can be found in Section 1, Part E.
Speakers’ Midterm Report: Section 1
32
C-10. Are network projects performed together with international partners?
no yes, identify the international groups involved
§ Clinical trials of the lymphoma study groups with: EORTC, GELA, ILI, European MCL Working Party
§ Cochrane Hematological Malignancies Group (SP8b) with: Cochrane Collaboration
§ Comparison of allogeneic bone marrow and peripheral blood progenitor cell transplantation in the field of high-dose therapy for patients with lymphoma (SP9) with: EBMT, IBMTR
C-11. Patient documentation a) Is the network using standardised patient documentation?
no yes
b) Has the network developed standardised procedures for patient documentation?
no yes: new development yes: further development c) Is the data processing IT-based? no, not intended planned yes, already in use
d) Are the data collected supra-regionally and centrally analysed? no, not intended planned yes, already in use
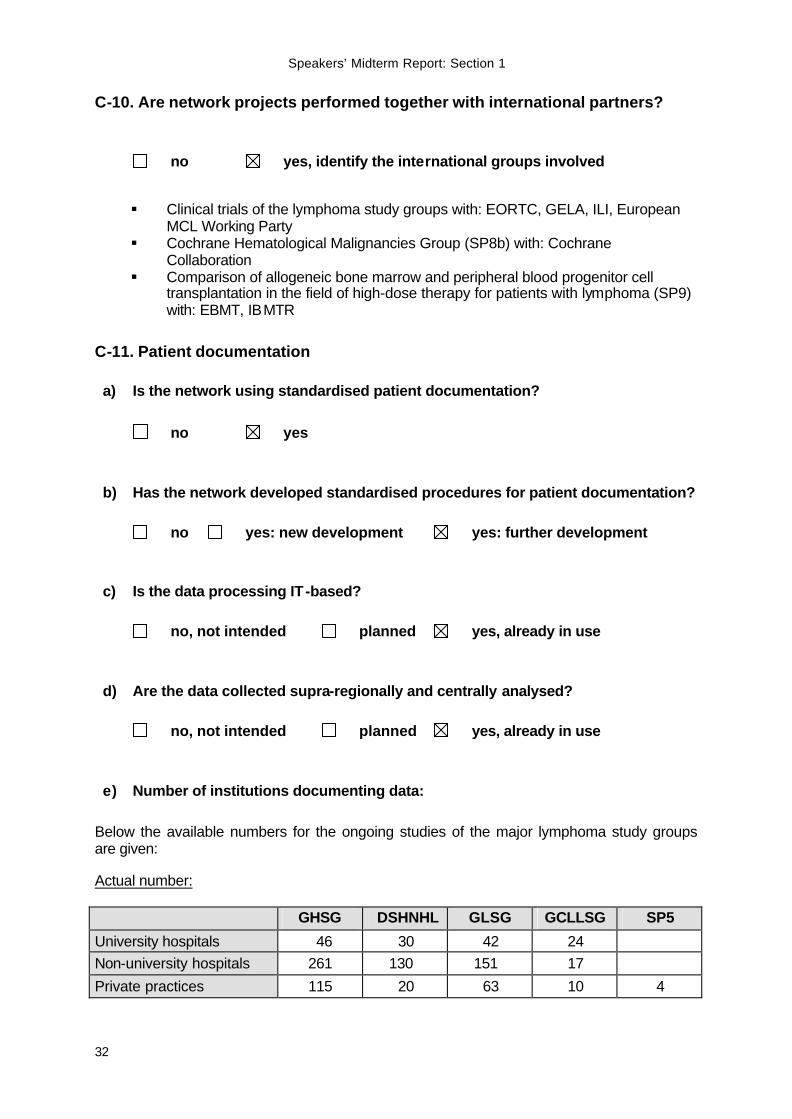
e) Number of institutions documenting data:
Below the available numbers for the ongoing studies of the major lymphoma study groups are given: Actual number: GHSG DSHNHL GLSG GCLLSG SP5
University hospitals 46 30 42 24 Non-university hospitals 261 130 151 17
Private practices 115 20 63 10 4
Speakers’ Midterm Report: Section 1
33
Planned number:
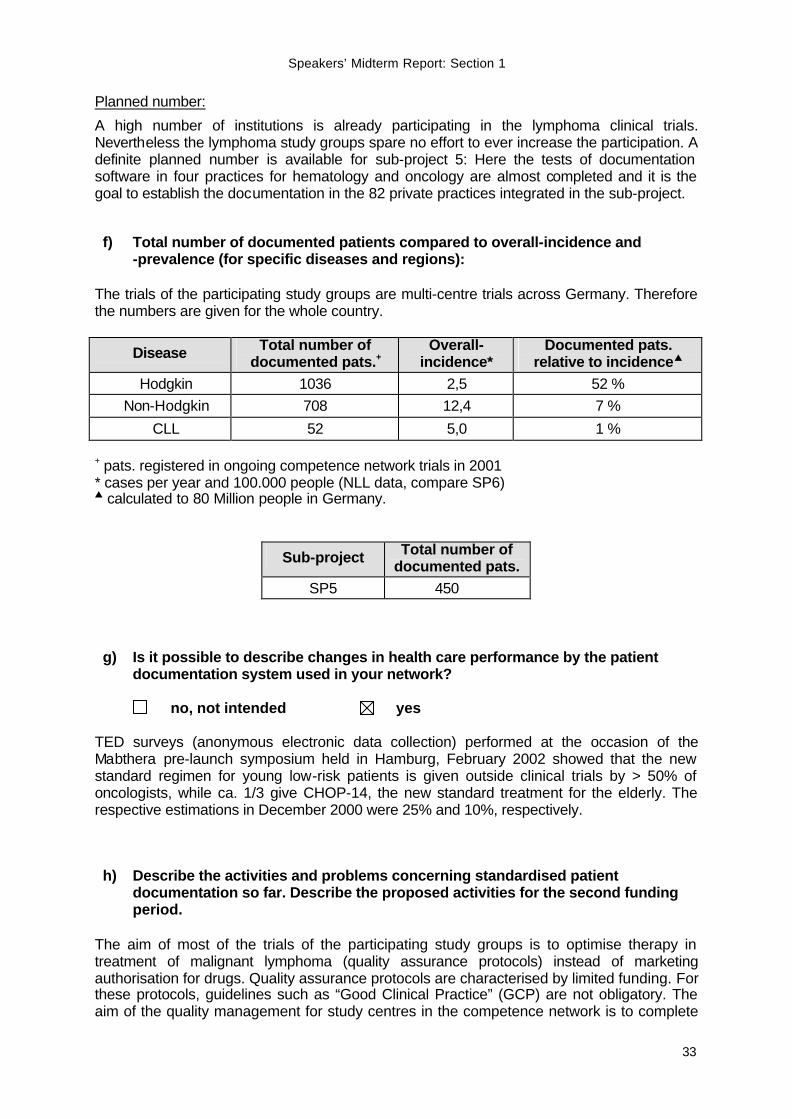
A high number of institutions is already participating in the lymphoma clinical trials. Nevertheless the lymphoma study groups spare no effort to ever increase the participation. A definite planned number is available for sub-project 5: Here the tests of documentation software in four practices for hematology and oncology are almost completed and it is the goal to establish the documentation in the 82 private practices integrated in the sub-project. f) Total number of documented patients compared to overall-incidence and
-prevalence (for specific diseases and regions): The trials of the participating study groups are multi-centre trials across Germany. Therefore the numbers are given for the whole country.
Disease Total number of documented pats.+
Overall-incidence*
Documented pats. relative to incidences
Hodgkin 1036 2,5 52 % Non-Hodgkin 708 12,4 7 %
CLL 52 5,0 1 % + pats. registered in ongoing competence network trials in 2001 * cases per year and 100.000 people (NLL data, compare SP6) s calculated to 80 Million people in Germany.
Sub-project Total number of documented pats.
SP5 450 g) Is it possible to describe changes in health care performance by the patient
documentation system used in your network? no, not intended yes TED surveys (anonymous electronic data collection) performed at the occasion of the Mabthera pre-launch symposium held in Hamburg, February 2002 showed that the new standard regimen for young low-risk patients is given outside clinical trials by > 50% of oncologists, while ca. 1/3 give CHOP-14, the new standard treatment for the elderly. The respective estimations in December 2000 were 25% and 10%, respectively. h) Describe the activities and problems concerning standardised patient
documentation so far. Describe the proposed activities for the second funding period.
The aim of most of the trials of the participating study groups is to optimise therapy in treatment of malignant lymphoma (quality assurance protocols) instead of marketing authorisation for drugs. Quality assurance protocols are characterised by limited funding. For these protocols, guidelines such as “Good Clinical Practice” (GCP) are not obligatory. The aim of the quality management for study centres in the competence network is to complete

Speakers’ Midterm Report: Section 1
34
and harmonise the quality standards of the participating lymphoma study groups according to GCP with regard to the special situation of quality assurance protocols.
The current projects of the working group “Quality Management” include the harmonisation of case report forms (CRFs), the collection and definition of trial terms and the development of a system of standard operating procedures (SOPs) for all procedures in a study centre. For a better handling of definitions and SOPs, electronic tools are developed. In the second funding period of the competence network these projects will be continued and the development and implementation of quality assurance processes, as well as re-evaluating and controlling will become more important (compare sub-projects 1 and 2).
Within sub-project 5 it is the goal to gather an accurate description of the current provision of medical care for lymphoma patients in private practices for hematology and oncology. Therefore, a computer program has been created and established that enables the use of information from the accounting data carrier of the practice information system for quality assurance purposes. As not all required data could be extracted in this way, the program transfers them into an electronic questionnaire and missing data can be added. In addition to the basic data, the form asks for important quality indicators for diagnosis, therapy and aftercare. All patients treated for lymphoma in the practices are included in the data survey in anonymous form. The tests of stability, accuracy and user-friendliness in four practices (Hamburg, Saarbrücken, Koblenz and Cologne) have now largely been completed. The goal of the second funding period is to gradually increase the number of practices taking part in the data survey from the current four pilot practices to all the practices participating in the project (currently 82). The user-friendliness of the program is a decisive criterion for the success of the project, as a complicated program would greatly reduce the level of compliance. For more information see sub-project 5.
Speakers’ Midterm Report: Section 1
35
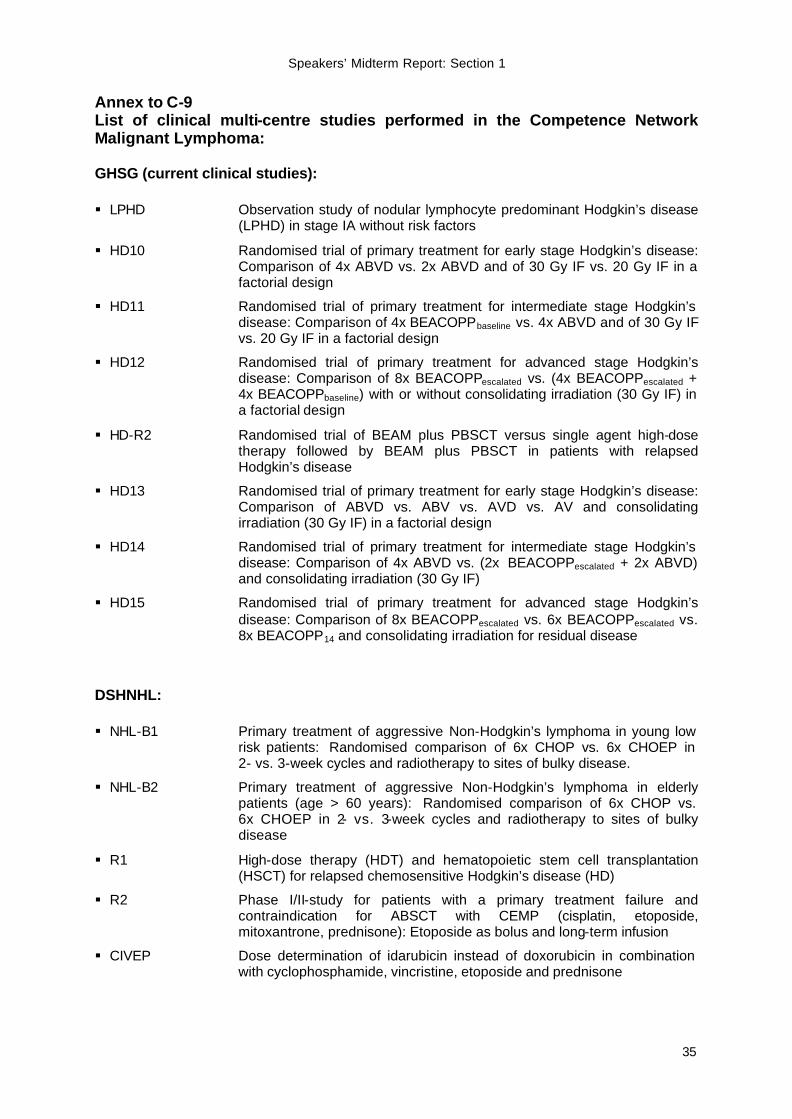
Annex to C-9 List of clinical multi-centre studies performed in the Competence Network Malignant Lymphoma: GHSG (current clinical studies): § LPHD Observation study of nodular lymphocyte predominant Hodgkin’s disease
(LPHD) in stage IA without risk factors
§ HD10 Randomised trial of primary treatment for early stage Hodgkin’s disease: Comparison of 4x ABVD vs. 2x ABVD and of 30 Gy IF vs. 20 Gy IF in a factorial design
§ HD11 Randomised trial of primary treatment for intermediate stage Hodgkin’s disease: Comparison of 4x BEACOPPbaseline vs. 4x ABVD and of 30 Gy IF vs. 20 Gy IF in a factorial design
§ HD12 Randomised trial of primary treatment for advanced stage Hodgkin’s disease: Comparison of 8x BEACOPPescalated vs. (4x BEACOPPescalated + 4x BEACOPPbaseline) with or without consolidating irradiation (30 Gy IF) in a factorial design
§ HD-R2 Randomised trial of BEAM plus PBSCT versus single agent high-dose therapy followed by BEAM plus PBSCT in patients with relapsed Hodgkin’s disease
§ HD13 Randomised trial of primary treatment for early stage Hodgkin’s disease: Comparison of ABVD vs. ABV vs. AVD vs. AV and consolidating irradiation (30 Gy IF) in a factorial design
§ HD14 Randomised trial of primary treatment for intermediate stage Hodgkin’s disease: Comparison of 4x ABVD vs. (2x BEACOPPescalated + 2x ABVD) and consolidating irradiation (30 Gy IF)
§ HD15 Randomised trial of primary treatment for advanced stage Hodgkin’s disease: Comparison of 8x BEACOPPescalated vs. 6x BEACOPPescalated vs. 8x BEACOPP14 and consolidating irradiation for residual disease
DSHNHL: § NHL-B1 Primary treatment of aggressive Non-Hodgkin’s lymphoma in young low
risk patients: Randomised comparison of 6x CHOP vs. 6x CHOEP in 2- vs. 3-week cycles and radiotherapy to sites of bulky disease.
§ NHL-B2 Primary treatment of aggressive Non-Hodgkin’s lymphoma in elderly patients (age > 60 years): Randomised comparison of 6x CHOP vs. 6x CHOEP in 2- vs. 3-week cycles and radiotherapy to sites of bulky disease
§ R1 High-dose therapy (HDT) and hematopoietic stem cell transplantation (HSCT) for relapsed chemosensitive Hodgkin’s disease (HD)
§ R2 Phase I/II-study for patients with a primary treatment failure and contraindication for ABSCT with CEMP (cisplatin, etoposide, mitoxantrone, prednisone): Etoposide as bolus and long-term infusion
§ CIVEP Dose determination of idarubicin instead of doxorubicin in combination with cyclophosphamide, vincristine, etoposide and prednisone
Speakers’ Midterm Report: Section 1
36
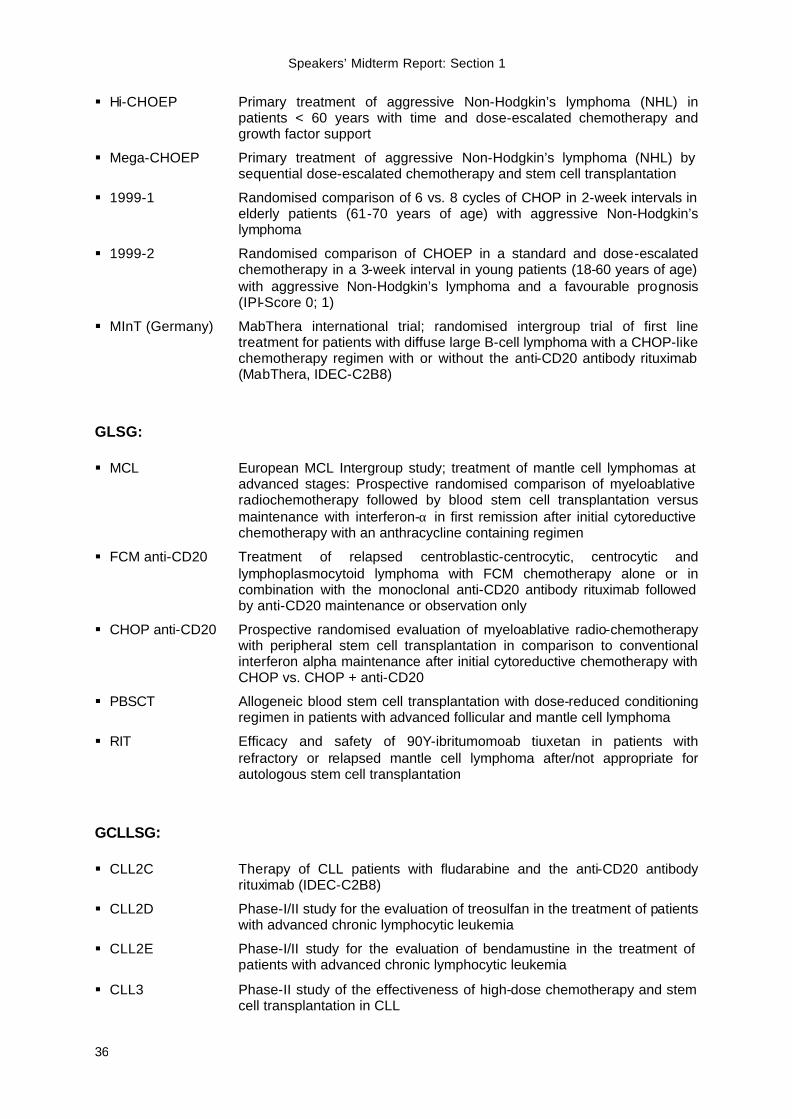
§ Hi-CHOEP Primary treatment of aggressive Non-Hodgkin’s lymphoma (NHL) in patients < 60 years with time and dose-escalated chemotherapy and growth factor support
§ Mega-CHOEP Primary treatment of aggressive Non-Hodgkin’s lymphoma (NHL) by sequential dose-escalated chemotherapy and stem cell transplantation
§ 1999-1 Randomised comparison of 6 vs. 8 cycles of CHOP in 2-week intervals in elderly patients (61-70 years of age) with aggressive Non-Hodgkin’s lymphoma
§ 1999-2 Randomised comparison of CHOEP in a standard and dose-escalated chemotherapy in a 3-week interval in young patients (18-60 years of age) with aggressive Non-Hodgkin’s lymphoma and a favourable prognosis (IPI-Score 0; 1)
§ MInT (Germany) MabThera international trial; randomised intergroup trial of first line treatment for patients with diffuse large B-cell lymphoma with a CHOP-like chemotherapy regimen with or without the anti-CD20 antibody rituximab (MabThera, IDEC-C2B8)
GLSG: § MCL European MCL Intergroup study; treatment of mantle cell lymphomas at
advanced stages: Prospective randomised comparison of myeloablative radiochemotherapy followed by blood stem cell transplantation versus maintenance with interferon-α in first remission after initial cytoreductive chemotherapy with an anthracycline containing regimen
§ FCM anti-CD20 Treatment of relapsed centroblastic-centrocytic, centrocytic and lymphoplasmocytoid lymphoma with FCM chemotherapy alone or in combination with the monoclonal anti-CD20 antibody rituximab followed by anti-CD20 maintenance or observation only
§ CHOP anti-CD20 Prospective randomised evaluation of myeloablative radio-chemotherapy with peripheral stem cell transplantation in comparison to conventional interferon alpha maintenance after initial cytoreductive chemotherapy with CHOP vs. CHOP + anti-CD20
§ PBSCT Allogeneic blood stem cell transplantation with dose-reduced conditioning regimen in patients with advanced follicular and mantle cell lymphoma
§ RIT Efficacy and safety of 90Y-ibritumomoab tiuxetan in patients with refractory or relapsed mantle cell lymphoma after/not appropriate for autologous stem cell transplantation
GCLLSG: § CLL2C Therapy of CLL patients with fludarabine and the anti-CD20 antibody
rituximab (IDEC-C2B8)
§ CLL2D Phase-I/II study for the evaluation of treosulfan in the treatment of patients with advanced chronic lymphocytic leukemia
§ CLL2E Phase-I/II study for the evaluation of bendamustine in the treatment of patients with advanced chronic lymphocytic leukemia
§ CLL3 Phase-II study of the effectiveness of high-dose chemotherapy and stem cell transplantation in CLL
Speakers’ Midterm Report: Section 1
37
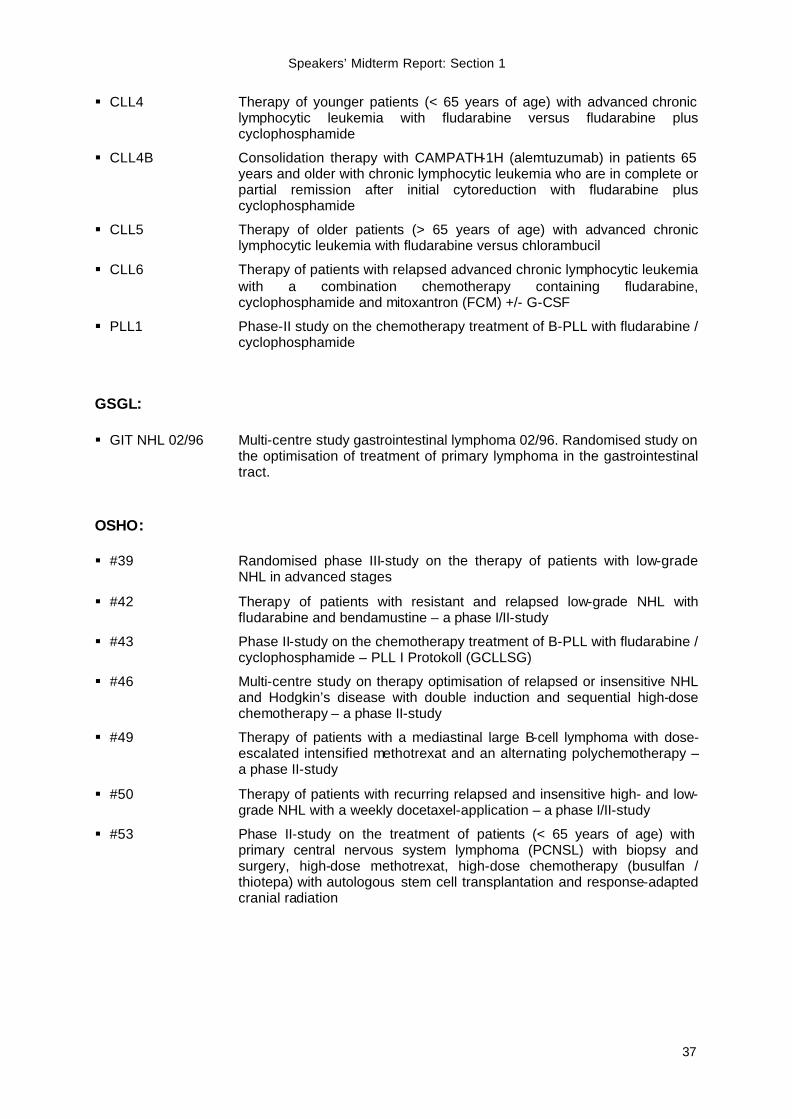
§ CLL4 Therapy of younger patients (< 65 years of age) with advanced chronic lymphocytic leukemia with fludarabine versus fludarabine plus cyclophosphamide
§ CLL4B Consolidation therapy with CAMPATH-1H (alemtuzumab) in patients 65 years and older with chronic lymphocytic leukemia who are in complete or partial remission after initial cytoreduction with fludarabine plus cyclophosphamide
§ CLL5 Therapy of older patients (> 65 years of age) with advanced chronic lymphocytic leukemia with fludarabine versus chlorambucil
§ CLL6 Therapy of patients with relapsed advanced chronic lymphocytic leukemia with a combination chemotherapy containing fludarabine, cyclophosphamide and mitoxantron (FCM) +/- G-CSF
§ PLL1 Phase-II study on the chemotherapy treatment of B-PLL with fludarabine / cyclophosphamide
GSGL: § GIT NHL 02/96 Multi-centre study gastrointestinal lymphoma 02/96. Randomised study on
the optimisation of treatment of primary lymphoma in the gastrointestinal tract.
OSHO: § #39 Randomised phase III-study on the therapy of patients with low-grade
NHL in advanced stages
§ #42 Therapy of patients with resistant and relapsed low-grade NHL with fludarabine and bendamustine – a phase I/II-study
§ #43 Phase II-study on the chemotherapy treatment of B-PLL with fludarabine / cyclophosphamide – PLL I Protokoll (GCLLSG)
§ #46 Multi-centre study on therapy optimisation of relapsed or insensitive NHL and Hodgkin’s disease with double induction and sequential high-dose chemotherapy – a phase II-study
§ #49 Therapy of patients with a mediastinal large B-cell lymphoma with dose-escalated intensified methotrexat and an alternating polychemotherapy – a phase II-study
§ #50 Therapy of patients with recurring relapsed and insensitive high- and low-grade NHL with a weekly docetaxel-application – a phase I/II-study
§ #53 Phase II-study on the treatment of patients (< 65 years of age) with primary central nervous system lymphoma (PCNSL) with biopsy and surgery, high-dose methotrexat, high-dose chemotherapy (busulfan / thiotepa) with autologous stem cell transplantation and response-adapted cranial radiation
Speakers’ Midterm Report: Section 1
38
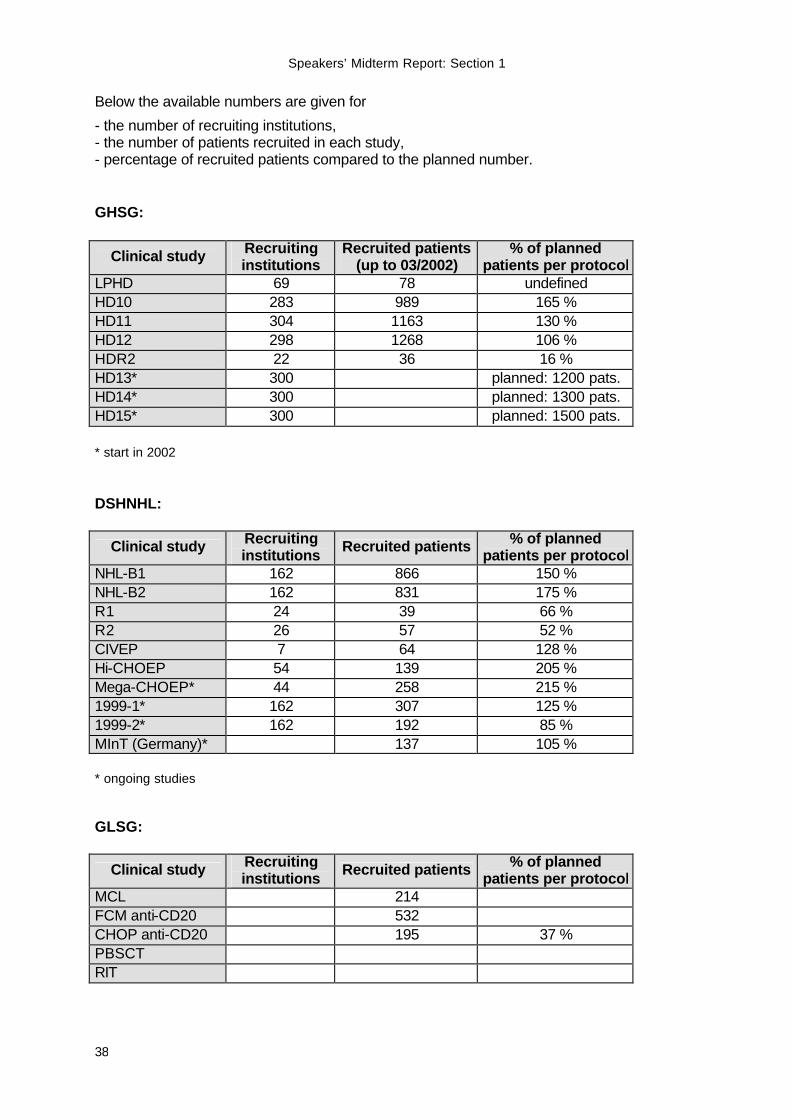
Below the available numbers are given for
- the number of recruiting institutions, - the number of patients recruited in each study, - percentage of recruited patients compared to the planned number. GHSG:
Clinical study Recruiting institutions
Recruited patients (up to 03/2002)
% of planned patients per protocol
LPHD 69 78 undefined HD10 283 989 165 % HD11 304 1163 130 % HD12 298 1268 106 % HDR2 22 36 16 % HD13* 300 planned: 1200 pats. HD14* 300 planned: 1300 pats. HD15* 300 planned: 1500 pats. * start in 2002 DSHNHL:
Clinical study Recruiting institutions Recruited patients % of planned
patients per protocol NHL-B1 162 866 150 % NHL-B2 162 831 175 % R1 24 39 66 % R2 26 57 52 % CIVEP 7 64 128 % Hi-CHOEP 54 139 205 % Mega-CHOEP* 44 258 215 % 1999-1* 162 307 125 % 1999-2* 162 192 85 % MInT (Germany)* 137 105 % * ongoing studies GLSG:
Clinical study Recruiting institutions Recruited patients % of planned
patients per protocol MCL 214 FCM anti-CD20 532 CHOP anti-CD20 195 37 % PBSCT RIT
Speakers’ Midterm Report: Section 1
39
Part C – Added Value through Networking C-12. Material banks a) Is your network setting up material banks?
no yes b) Which materials are collected within your network? § Tissue samples (frozen and paraffin-embedded)
§ Sera and blood samples of patients with aggressive lymphomas (DSHNHL)
c) Is the network using standardised documentation for materials?
§ Tissue samples: No (planned).
§ Sera and blood samples: Yes.
d) Are the material data correlated with the medical patient records?
§ Tissue samples: Yes, new development.
§ Sera and blood samples: Yes, further development.
e) Is the data processing IT-based?
§ Tissue samples: No (planned).
§ Sera and blood samples: Yes, already in use.
f) Are the data collected supra-regionally and centrally analysed? § Tissue samples: No, not intended.
§ Sera and blood samples: Yes, already in use.
g) Number of institutions sending materials and documenting data:
Tissue samples: The precise number of institutions sending tissue samples and documenting data has not been determined so far. However, all tissue materials of patients enrolled in the clinical trials are collected in the reference centres for lymph node pathology. The corresponding data will be stored in the central reference pathology database located at the IMISE in Leipzig.
Speakers’ Midterm Report: Section 1
40
Sera and blood samples Actual number: Sera and blood
samples University hospitals 12 Non-university hospitals 88 Private practices 4
Planned number: 200
h) Total number of documented materials:
Tissue samples: The number of documented materials is identical to the number of cases. Each tissue sample is re-diagnosed in a reference centre for lymph node pathology. In the future the final diagnosis will be automatically transmitted to the coordination centres of the corresponding clinical trial and stored in the central pathology database. The diagnostic and clinical data will be linked to the storage information (see also C-12 paragraph i). Therefore, an extensive documentation of all study cases stored in the reference centres is guaranteed. Sera and blood samples: 3108 from 1298 patients with aggressive lymphomas.
i) Total number of documented materials correlated with patient data: 100%
j) Are the materials and the material data used as diagnostic reference samples?
no, not intended yes
k) Other use of the materials and/or the material data: It is intended that the collected material should be utilised for basic research projects.
l) Describe the activities and problems concerning material collection and documentation so far and describe the proposed activities for the second funding period.
The prognostic impact of biological parameters in malignant lymphomas is still poorly understood despite the fact that significant progress has been made with respect to the understanding of molecular events leading to the development of the diseases. Many of the network’s projects and clinical study groups require tissue material from corresponding lymphoma entities for their investigations. At the moment, the retrieval of tissue material in sufficient quantity and quality is a major challenge since there is no common database covering all relevant patient data, including final reference diagnosis and type and number of tissue blocks available. Within sub-project 3 a central database for tissue material will be established to overcome these limitations. In each collaborating reference centre for lymph node pathology the tissues are collected for the purpose of a reference-pathological diagnosis. Whereas the database will be centralised, the tissue blocks are stored at the reference centres. The storage location and the number of tissue blocks per case will be recorded in the central database. The database itself is integrated into the central pathology server in Leipzig (IMISE). All available material information will be directly linked to corresponding patient data at the coordination centres of the clinical trials. This allows a very precise cataloguing and categorisation off all available tissue materials.
Speakers’ Midterm Report: Section 1
41
Another major obstacle, especially for the evaluation of biological parameters, is the collection of fresh and/or frozen tissue materials urgently needed for many up-to-date lymphoma research projects The collection of fresh tumour tissue samples obtained from patients treated within the trials of the clinical study groups of the competence network will allow an analysis of histopathologically and clinically well characterised and homogeneously treated patient cohorts. Therefore it is the key goal of a new sub-project termed “Improvement of the infrastructure for the analysis of biologic risk factors in malignant lymphomas” to provide an optimised infrastructure for the collection of fresh tumour tissue at the pathology reference centres. To achieve this goal, established structures of the network will be further optimised. The “network assistants” (see sub-project 1) will support the logistics required for the collection of fresh/cryopreserved tumour tissue materials and the documentation of the relevant parameters. In addition, the network’s IT infrastructure will be utilised to survey the acquisition, storage and further use of the samples.
C-13. a) Which programs for the promotion of young scientists are realised by the
network?
Promotion of scientific exchange
Organisation of continuing medical education (“Fort- und
Weiterbildung")
Career development paths for young clinical scientists
Others
b) Describe the programs and activities realised in your network so far and describe the proposed activities for the second funding period.
Continuing medical education A course on "Evidence-Based Medicine for Hematologists and Oncologists in Private Practice" was designed by sub-project 5. In the two-day seminars, questions arising from everyday clinical practice of the participants are discussed on the basis of methods of EbM. A basic course on "Therapy, Diagnosis and Guidelines" has been held two times since May 2001. The course is held in cooperation with the Clinical Economics Working Group of Ulm University. Prof. Porzsolt (Ulm), the main speaker, is a renowned expert in the field of EbM. Career development paths for young scientists The ”Deutsche Ärztekammer“ has accredited the annual meetings of the competence network as part of the medical education programme. Proposed activities
• It is intended to extend the programme of medical education seminars.
• As outlined in Part F of this section „Sustainability“, the competence network aims to participate in the 6th EU Framework Programme for Research, Technology and Development. Of special interest for the competence networks is the sub-programme „Networks of Excellence“. The promotion of scientific exchange, especially for young scientists, will be part of this proposal.
Speakers’ Midterm Report: Section 1
42
Part D – Visibility of the Network
D-14. Has the network been presented comprehensively at scientific congresses?
no yes
§ See annex after D-18.
D-15. a) Which public relations activities have been performed by the network for which
addressees/multipliers?
§ See annex after D-18.
b) Do you evaluate the echo of such presentations for instance via the collection of press reports (Pressespiegel)?
no yes
In the first funding period, systematic evaluation of media echo could not be performed. Nevertheless, the public relations officer compiled all articles she could find in a kind of a “Pressespiegel”. In the second funding period, financial resources for professional media monitoring should be provided. D-16. Is your network cooperating with self help groups / other lay groups?
no yes
D-17. Is the network offering medical information for external groups?
no yes, information for patients yes, information and family members for doctors
D-18. Describe the activities and problems concerning the visibility of your network so far and describe the proposed activities for the second funding period.
Activities The visibility of the network for scientists and physicians, patients, media, and the general public should be reached utilising different instruments:
• homepage (provides information on the network’s activities as well as scientific data and current clinical studies; separate area for patients; information for journalists)
• newsletter (information on the network activities, reports of the project leaders, presentation of new study protocols; serves as an instrument for vertical communication between research and clinical practice)
Speakers’ Midterm Report: Section 1
43
• brochures (“Kompetenznetz Maligne Lymphome – Medizin 2000”, presentation of the network and its projects)
• scientific symposia (presentation of the latest results with respect to the state-of-the-art in diagnosis and therapy of malignant lymphoma)
• presentations for patients (lectures, patients seminars, information booths)
• presentations for general public (information booths)
• press conferences & press releases (information for public as well as for specialised medical/scientific media)
Problems Financial resources and manpower for public relations activities have been limited in the first funding period. A part of the information material (e.g. newsletter, flyer for the patients’ seminar) could only be realised by industrial sponsoring, professional media monitoring for evaluation of the network’s media work could not be performed. With a half part position, the public relations officer has been quite restricted in realising various projects at the same time. Proposed activities All activities that have been listed above shall be continued in the second funding period. There will be enlargements and/or new emphasis in some fields:
• the sub-projects and the study groups will to a greater extent be supported in their public relations activities by the central office
• the visibility for and the dialogue with the physicians who are involved in the networks projects will be intensified
• symposia for patients will be performed more often at several places all over Germany
• information booths will be set up in the exhibition area of medical meetings
• the network’s information brochure will be updated
• background information for journalists (on malignant lymphoma, therapy, study groups etc.) will be delivered via the network’s homepage
• attention of public media and general public for the network shall be increased
Speakers’ Midterm Report: Section 1
44
Annex Part D-14 – Visibility – presentation of the network at scientific congresses
- DGIM Congress
date: May 3, 2000 site: Wiesbaden organiser: German Society of Internal Medicine topic: symposium of the network
- DGHO/ÖGHO Congress date: October 25, 2000 site: Graz (Austria) organiser: German and Austrian Society of Hematology and Oncology topic: joint symposium with the Competence Network Leukemia
- DGIM Congress date: April 24, 2001 site: Wiesbaden organiser: German Society of Internal Medicine topic: joint symposium with the Competence Network Leukemia
- Patients’ Symposium date: September 22, 2001 site: Cologne organiser: German Hodgkin’s Lymphoma Study Group (Fifth International Symposium on Hodgkin’s lymphoma, September 22-25, 2001) topic: Patients’ seminar on malignant lymphoma external participants: 300
- DGHO/ÖGHO Congress date: October 01, 2001 site: Mannheim organiser: German and Austrian Society of Hematology and Oncology topic: “state-of-the-art”; joint symposium with the Competence Network Leukemia
- DGIM Congress date: April 10, 2002 site: Wiesbaden organiser: German Society of Internal Medicine topic: treatment of elderly patients; joint symposium with the Competence Network Leukemia
Remark: We were not able to count the participants but at least 200 persons took part in each of the scientific symposia.
Speakers’ Midterm Report: Section 1
45
Public Relations Activities Press Conferences Date Occasion Addressee
2000-01-12 Start-up-symposium National public media and medical press 2000-06-19 Start of sub-project 6 Local public media and medical press 2001-03-16 1st annual symposium Medical press and local public media
2001-09-20 5th International Symposium on Hodgkin’s lymphoma Local and national public media
2001-09-24 5th International Symposium on Hodgkin’s lymphoma Medical press
Press Releases Date Topic / Title 2000-01-06 Invitation press conference 2000-01-12
2001-02-14 “Lymphom-Netzwerk unter dem Dach von ‘Haus Lebenswert’. Lebensqualität-Projekt stellt Raum für Forschung zur Verfügung“
2001-03-08 Invitation panel discussion and press conference 16.03.2001
2001-03-16 “Kompetenznetze machen klinische Forschung international konkurrenzfähig. Patienten profitieren von intensivierter Zusammenarbeit“
2001-06-21 Advance notice on 5th International Symposium on Hodgkin’s lymphoma with patients’ seminar and press conferences
2001-09-12 Invitation press conference 5th International Symposium on Hodgkin’s lymphoma for public media, 2001-09-20
2001-09-12 Invitation press conference 5th international symposium on Hodgkin’s lymphoma for medical press, 2001-09-24
2001-09-20 “Heilungschancen bei Hodgkin’scher Erkrankung steigen weiter an. Hodgkin-Weltkongress beginnt am Samstag in Köln“
2001-09-24 “Erfolgsraten stabilisieren, Spätfolgen vermeiden. Hodgkin-Experten diskutieren neue Therapiekonzepte“
2001-11-15 Invitation press conference Competence Networks of Health Research, 2001-12-14
2001-12-12 “Internetportal der Kompetenznetze in der Medizin. Gebündelte Informationen für Ärzte und Patienten“
2002-01-30 “Radioimmuntherapie bei malignen Lymphomen.“ International symposium in Göttingen: invitation for medical press
Press Reports (Not collected systematically, voucher copies scarcely received) Newspaper/journal/ online news service Date Title of the article
Express 2000-01-13 “Krebs-Info im Internet“ Kölnische Rundschau 2000-01-13 “Ärzte gründen Netzwerk gegen Lymphknotenkrebs“
Kölner Stadt-Anzeiger
2000-01-13
“Lymphdrüsenkrebs: Moderne Technik als ‚sinnvoller Assistent’“
Speakers’ Midterm Report: Section 1
46
Ärzte Zeitung 2000-01-25 “Infodienst in Köln. Netzwerk widmet sich den malignen Lymphomen“
Süddeutsche Zeitung 2000-02-01 “Zusammenarbeit als Experiment. Eine neue Brücke zwischen Medizin-Forschung und Anwendung“
Rheinisches Ärzteblatt 02/2000 “Um Mithilfe wird gebeten“ unknown 2000-03-03 “MedNet Maligne Lymphome gestartet” KV Aktuell 03/2000 article on SP6 UHK-Report 05/2000 article on SP6 (Saarländisches Lymphomprojekt)
Kölnische Rundschau 2000-06-20 “Neues Projekt bei Lymphdrüsenkrebs. ‚Das Wissen der Uni-Kliniken an die Basis geben’”
unknown unknown “Netzwerk ‚Malignes Lymphom’. Kölner Einrichtung will neue wissenschaftliche Erkenntnisse schneller zum Patienten bringen”
Saarländisches Ärzteblatt 08/00 “Das Saarländische Lymphomprojekt. Ein neuartiges
Projekt zur Versorgungsepidemiologie im Saarland” Kölnische Rundschau 2001-02-28 “Mit der Kunst die Sorge ausdrücken”
OncoCon 2001-02-15 “Neue Zentrale für das ‚Kompetenznetz Maligne Lymphome’ in Köln: Forschung koordinieren, Patienten und Ärzte informieren”
Ärzte Zeitung 2001-02-21 “Netzwerk über Lymphome”
Ärzte Zeitung 2001-03-07 “Infos von allen für alle. Kompetenznetzwerke zu Lymphomen und Leukämien”
OncoCon 2001-03-21 “Kompetenznetze machen klinische Forschung international konkurrenzfähig. Patienten profitieren von intensivierter Zusammenarbeit”
Kölnische Rundschau 2001-04-19 “Medizin-Netzwerk ‚Maligne Lymphome’ jetzt in ‚Haus Lebenswert’. Infos für Ärzte und Patienten“
Symposium Medical – Onkologie
2001, Ausg. 1
“Kompetenznetz Maligne Lymphome”
Kölner Stadt-Anzeiger 2001-05-02 supplement concerning the dies academicus of the University of Cologne, notice on the networkk’s information booth
Neue Apotheken Illustrierte 2001-08-15 “Patienten-Seminar zu malignen Lymphomen”
Gesundheit (Apotheken Magazin) 08/2001 “Medizinische Kompetenznetze. Verbesserungen für
die Patienten erreichen”
DLH-Info 15 2001-08-20 “Aktuelles aus dem Kompetenznetz Maligne Lymphome”
Rheinisches Ärzteblatt 09/2001 article on SP6 Kölnische Rundschau 2001-09-11 “Drüsenkrebs. Seminar für Patienten”
Express 2001-09-21 “Lymphknotenkrebs: Patienten können sich in Köln informieren”
Kölner Stadt-Anzeiger 2002-09-21 “Der große Schritt, der den Durchbruch brachte. Internationaler Kongress zu Lymphdrüsenkrebs”
Kölnische Rundschau
2001-09-22
“Beste Chancen auf Heilung. Weltkongress in Köln zur Hodgkin-Krankheit”
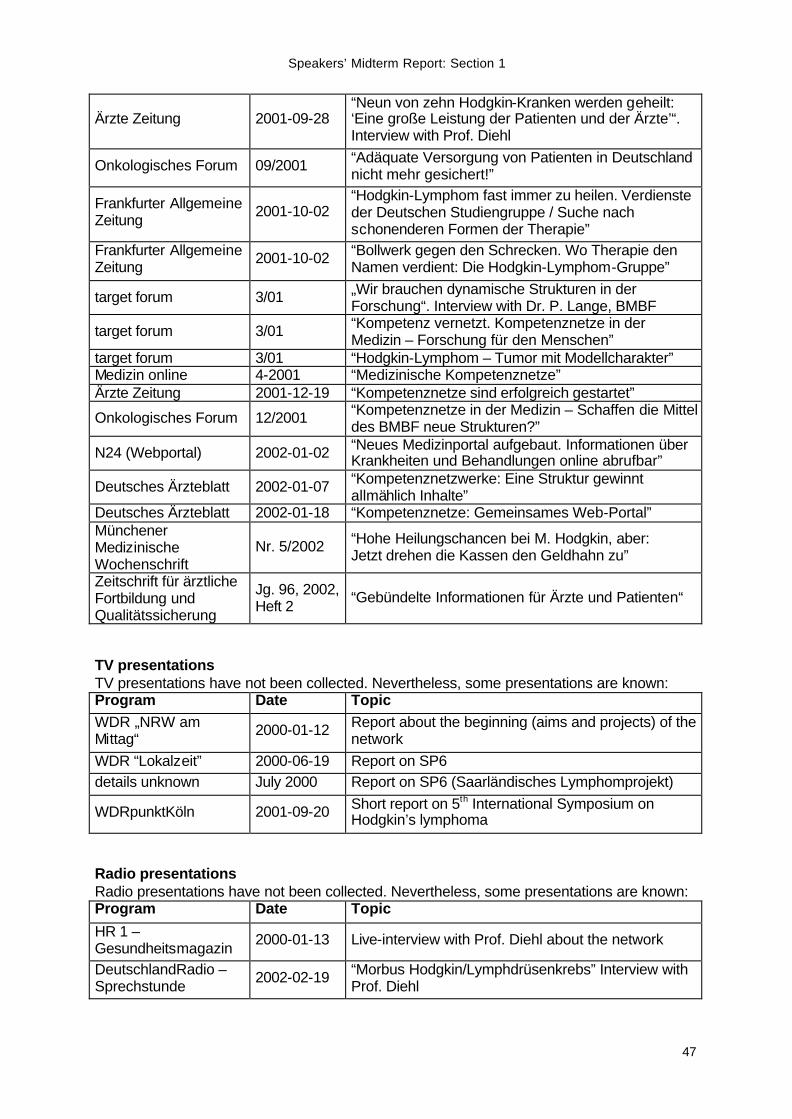
Speakers’ Midterm Report: Section 1
47
Ärzte Zeitung 2001-09-28 “Neun von zehn Hodgkin-Kranken werden geheilt: ‘Eine große Leistung der Patienten und der Ärzte’“. Interview with Prof. Diehl
Onkologisches Forum 09/2001 “Adäquate Versorgung von Patienten in Deutschland nicht mehr gesichert!”
Frankfurter Allgemeine Zeitung 2001-10-02
“Hodgkin-Lymphom fast immer zu heilen. Verdienste der Deutschen Studiengruppe / Suche nach schonenderen Formen der Therapie”
Frankfurter Allgemeine Zeitung 2001-10-02 “Bollwerk gegen den Schrecken. Wo Therapie den
Namen verdient: Die Hodgkin-Lymphom-Gruppe”
target forum 3/01 „Wir brauchen dynamische Strukturen in der Forschung“. Interview with Dr. P. Lange, BMBF
target forum 3/01 “Kompetenz vernetzt. Kompetenznetze in der Medizin – Forschung für den Menschen”
target forum 3/01 “Hodgkin-Lymphom – Tumor mit Modellcharakter” Medizin online 4-2001 “Medizinische Kompetenznetze” Ärzte Zeitung 2001-12-19 “Kompetenznetze sind erfolgreich gestartet”
Onkologisches Forum 12/2001 “Kompetenznetze in der Medizin – Schaffen die Mittel des BMBF neue Strukturen?”
N24 (Webportal) 2002-01-02 “Neues Medizinportal aufgebaut. Informationen über Krankheiten und Behandlungen online abrufbar”
Deutsches Ärzteblatt 2002-01-07 “Kompetenznetzwerke: Eine Struktur gewinnt allmählich Inhalte”
Deutsches Ärzteblatt 2002-01-18 “Kompetenznetze: Gemeinsames Web-Portal” Münchener Medizinische Wochenschrift
Nr. 5/2002 “Hohe Heilungschancen bei M. Hodgkin, aber: Jetzt drehen die Kassen den Geldhahn zu”
Zeitschrift für ärztliche Fortbildung und Qualitätssicherung
Jg. 96, 2002, Heft 2 “Gebündelte Informationen für Ärzte und Patienten“
TV presentations TV presentations have not been collected. Nevertheless, some presentations are known: Program Date Topic WDR „NRW am Mittag“ 2000-01-12 Report about the beginning (aims and projects) of the
network WDR “Lokalzeit” 2000-06-19 Report on SP6 details unknown July 2000 Report on SP6 (Saarländisches Lymphomprojekt)
WDRpunktKöln 2001-09-20 Short report on 5th International Symposium on Hodgkin’s lymphoma
Radio presentations Radio presentations have not been collected. Nevertheless, some presentations are known: Program Date Topic
HR 1 – Gesundheitsmagazin 2000-01-13 Live-interview with Prof. Diehl about the network
DeutschlandRadio – Sprechstunde 2002-02-19 “Morbus Hodgkin/Lymphdrüsenkrebs” Interview with
Prof. Diehl
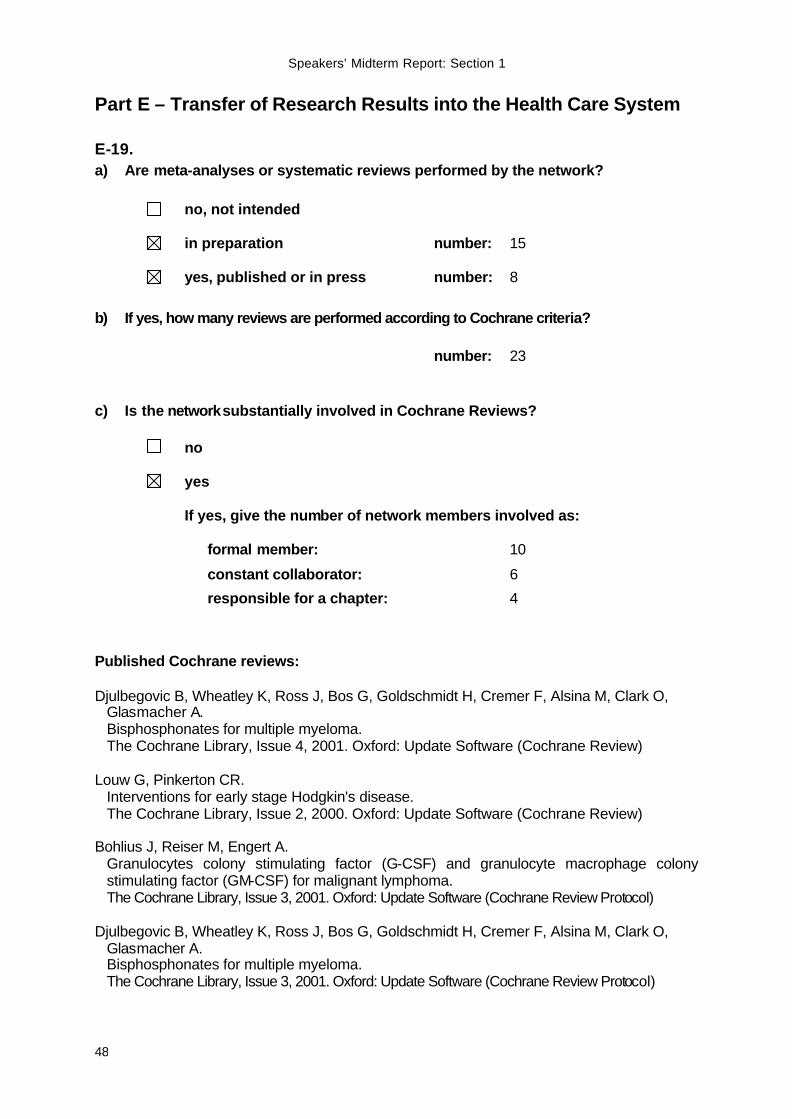
Speakers’ Midterm Report: Section 1
48
Part E – Transfer of Research Results into the Health Care System
E-19. a) Are meta-analyses or systematic reviews performed by the network?
no, not intended
in preparation number: 15
yes, published or in press number: 8
b) If yes, how many reviews are performed according to Cochrane criteria? number: 23
c) Is the network substantially involved in Cochrane Reviews?
no
yes If yes, give the number of network members involved as:
formal member: 10
constant collaborator: 6
responsible for a chapter: 4
Published Cochrane reviews:
Djulbegovic B, Wheatley K, Ross J, Bos G, Goldschmidt H, Cremer F, Alsina M, Clark O, Glasmacher A. Bisphosphonates for multiple myeloma. The Cochrane Library, Issue 4, 2001. Oxford: Update Software (Cochrane Review)
Louw G, Pinkerton CR. Interventions for early stage Hodgkin's disease. The Cochrane Library, Issue 2, 2000. Oxford: Update Software (Cochrane Review)
Bohlius J, Reiser M, Engert A. Granulocytes colony stimulating factor (G-CSF) and granulocyte macrophage colony stimulating factor (GM-CSF) for malignant lymphoma. The Cochrane Library, Issue 3, 2001. Oxford: Update Software (Cochrane Review Protocol)
Djulbegovic B, Wheatley K, Ross J, Bos G, Goldschmidt H, Cremer F, Alsina M, Clark O, Glasmacher A. Bisphosphonates for multiple myeloma. The Cochrane Library, Issue 3, 2001. Oxford: Update Software (Cochrane Review Protocol)
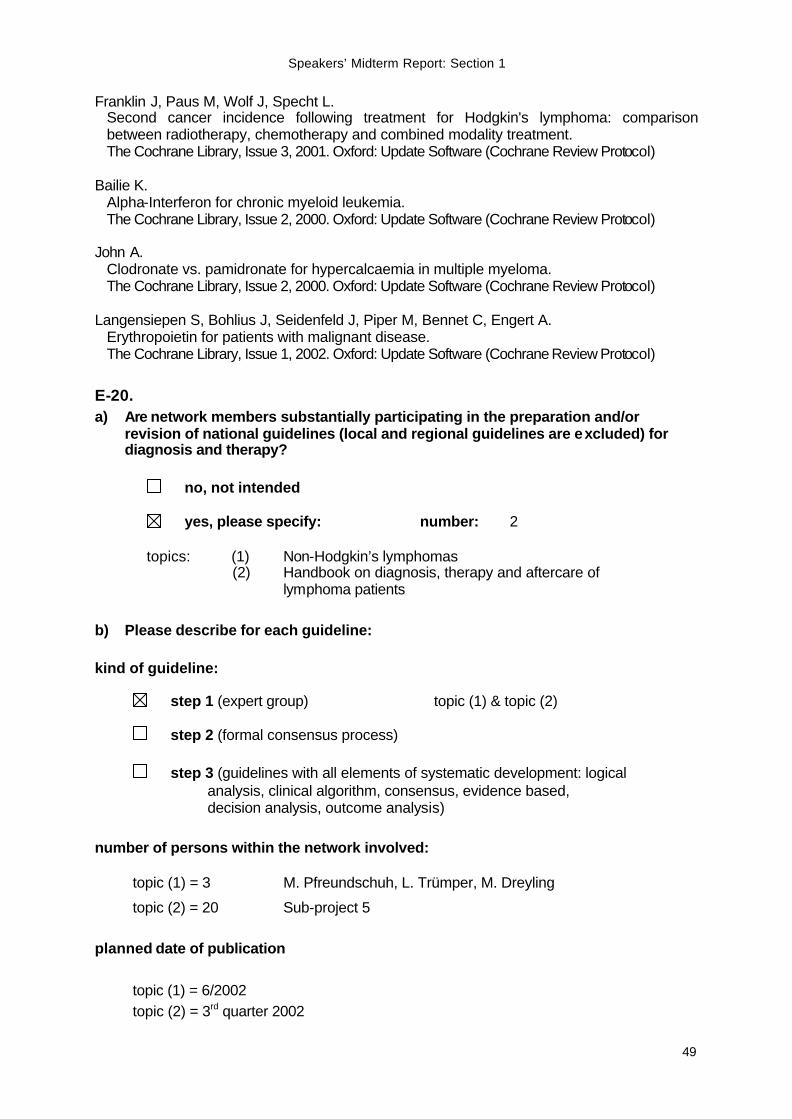
Speakers’ Midterm Report: Section 1
49
Franklin J, Paus M, Wolf J, Specht L. Second cancer incidence following treatment for Hodgkin's lymphoma: comparison between radiotherapy, chemotherapy and combined modality treatment. The Cochrane Library, Issue 3, 2001. Oxford: Update Software (Cochrane Review Protocol)
Bailie K. Alpha-Interferon for chronic myeloid leukemia. The Cochrane Library, Issue 2, 2000. Oxford: Update Software (Cochrane Review Protocol)
John A. Clodronate vs. pamidronate for hypercalcaemia in multiple myeloma. The Cochrane Library, Issue 2, 2000. Oxford: Update Software (Cochrane Review Protocol)
Langensiepen S, Bohlius J, Seidenfeld J, Piper M, Bennet C, Engert A. Erythropoietin for patients with malignant disease. The Cochrane Library, Issue 1, 2002. Oxford: Update Software (Cochrane Review Protocol)
E-20. a) Are network members substantially participating in the preparation and/or
revision of national guidelines (local and regional guidelines are excluded) for diagnosis and therapy?
no, not intended
yes, please specify: number: 2
topics: (1) Non-Hodgkin’s lymphomas
(2) Handbook on diagnosis, therapy and aftercare of lymphoma patients
b) Please describe for each guideline: kind of guideline:
step 1 (expert group) topic (1) & topic (2) step 2 (formal consensus process) step 3 (guidelines with all elements of systematic development: logical analysis, clinical algorithm, consensus, evidence based, decision analysis, outcome analysis) number of persons within the network involved:
topic (1) = 3 M. Pfreundschuh, L. Trümper, M. Dreyling
topic (2) = 20 Sub-project 5 planned date of publication topic (1) = 6/2002 topic (2) = 3rd quarter 2002
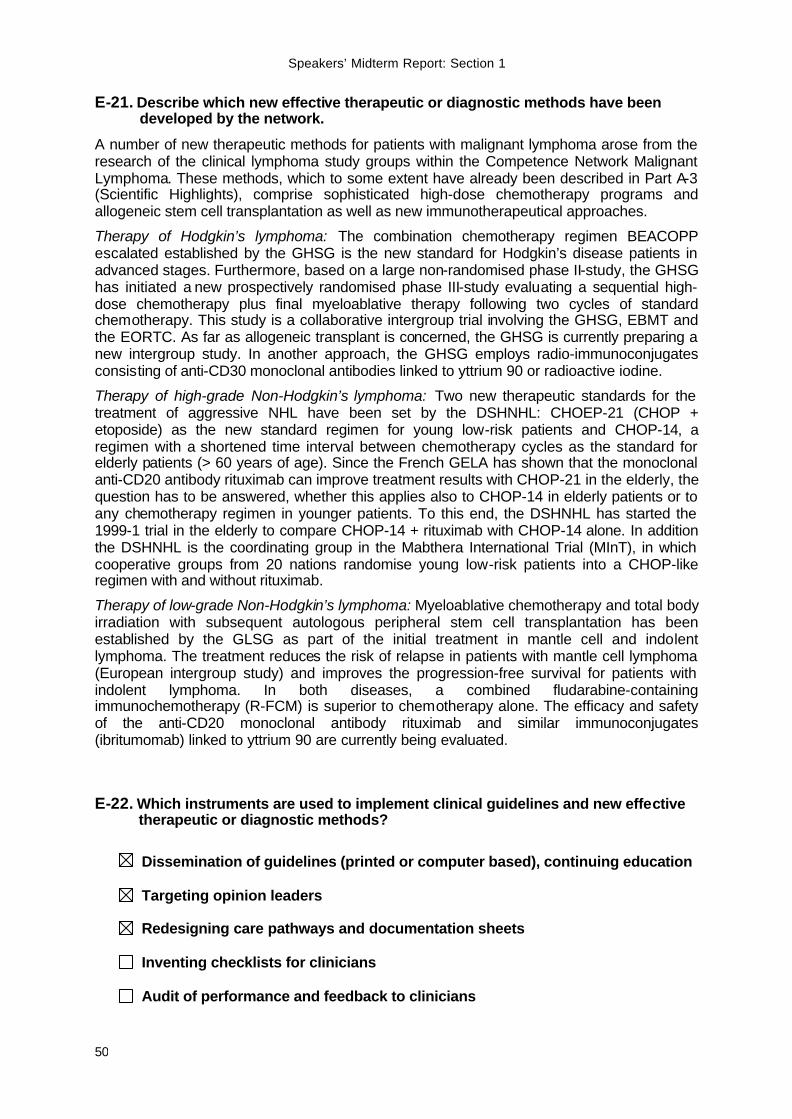
Speakers’ Midterm Report: Section 1
50
E-21. Describe which new effective therapeutic or diagnostic methods have been developed by the network.
A number of new therapeutic methods for patients with malignant lymphoma arose from the research of the clinical lymphoma study groups within the Competence Network Malignant Lymphoma. These methods, which to some extent have already been described in Part A-3 (Scientific Highlights), comprise sophisticated high-dose chemotherapy programs and allogeneic stem cell transplantation as well as new immunotherapeutical approaches.
Therapy of Hodgkin’s lymphoma: The combination chemotherapy regimen BEACOPP escalated established by the GHSG is the new standard for Hodgkin’s disease patients in advanced stages. Furthermore, based on a large non-randomised phase II-study, the GHSG has initiated a new prospectively randomised phase III-study evaluating a sequential high-dose chemotherapy plus final myeloablative therapy following two cycles of standard chemotherapy. This study is a collaborative intergroup trial involving the GHSG, EBMT and the EORTC. As far as allogeneic transplant is concerned, the GHSG is currently preparing a new intergroup study. In another approach, the GHSG employs radio-immunoconjugates consisting of anti-CD30 monoclonal antibodies linked to yttrium 90 or radioactive iodine.
Therapy of high-grade Non-Hodgkin’s lymphoma: Two new therapeutic standards for the treatment of aggressive NHL have been set by the DSHNHL: CHOEP-21 (CHOP + etoposide) as the new standard regimen for young low-risk patients and CHOP-14, a regimen with a shortened time interval between chemotherapy cycles as the standard for elderly patients (> 60 years of age). Since the French GELA has shown that the monoclonal anti-CD20 antibody rituximab can improve treatment results with CHOP-21 in the elderly, the question has to be answered, whether this applies also to CHOP-14 in elderly patients or to any chemotherapy regimen in younger patients. To this end, the DSHNHL has started the 1999-1 trial in the elderly to compare CHOP-14 + rituximab with CHOP-14 alone. In addition the DSHNHL is the coordinating group in the Mabthera International Trial (MInT), in which cooperative groups from 20 nations randomise young low-risk patients into a CHOP-like regimen with and without rituximab.
Therapy of low-grade Non-Hodgkin’s lymphoma: Myeloablative chemotherapy and total body irradiation with subsequent autologous peripheral stem cell transplantation has been established by the GLSG as part of the initial treatment in mantle cell and indolent lymphoma. The treatment reduces the risk of relapse in patients with mantle cell lymphoma (European intergroup study) and improves the progression-free survival for patients with indolent lymphoma. In both diseases, a combined fludarabine-containing immunochemotherapy (R-FCM) is superior to chemotherapy alone. The efficacy and safety of the anti-CD20 monoclonal antibody rituximab and similar immunoconjugates (ibritumomab) linked to yttrium 90 are currently being evaluated.
E-22. Which instruments are used to implement clinical guidelines and new effective therapeutic or diagnostic methods?
Dissemination of guidelines (printed or computer based), continuing education
Targeting opinion leaders
Redesigning care pathways and documentation sheets
Inventing checklists for clinicians
Audit of performance and feedback to clinicians
Speakers’ Midterm Report: Section 1
51
Others
• Workflow sheets for including patients in clinical studies • Course "Evidence-Based Medicine for Hematologists and Oncologists in
Private Practice" • Handbook on diagnosis, therapy and aftercare of lymphoma patients
Number of network members involved
Sub-project 5 GHSG DSHNHL
GLSG
E-23. Describe each of the efforts in your network and – if possible – their impact and the problems to transfer innovative research results into the health care system so far. Describe your collaboration with scientific societies in this respect. Describe the proposed activities for the second funding period.
Targeting opinion leaders: The recent results of the German lymphoma study groups already have a profound impact on the routine clinical care of lymphoma patients and the general health care system. An immediate progress has been established by the participation of a large number of hemato-oncologists in multi-centre trials. Furthermore, the presentation of the superiority of new treatment regimens at regional, national and international hemato-oncology meetings led to a broad acceptance of these new standard regimens by the oncology community. TED surveys of oncologists in private practices at different national meetings confirmed that e.g. the new chemotherapy regimens of the DSHNHL have replaced the old standard regimens for the treatment of aggressive NHL in younger patients. The worldwide acceptance of new regimens will be further improved by the publication of study results in top-ranking international journals. Moreover, this should also result in an increasing number of patients participating in clinical lymphoma trials.
Redesigning documentation sheets and pathways: The quality management projects of sub-project 2 and the employment of network assistants (sub-project 1) have a direct impact on the quality of documentation sheets and their pathways from clinicians to study centres. On-site visits of the network assistants in hospitals uncover documentation problems. The network assistants work out proposals for the reorganisation of the documentation pathways regarding the basic conditions in hospitals and the necessity of quality of documentation for the study centres. The project “Harmonisation of Documentation Items“ simplifies the documentation for all lymphoma trials involved in the Competence Network Malignant Lymphoma. The network assistants carried out comparative analyses on selected topics (e.g. documentation of laboratory findings). The working group “Quality Management” is coordinating the elaboration of consensus features between clinicians and biometrists (see also sub-project 2).
Workflow sheets: The organisational structures of private practices for hematology and oncology are usually highly complex. If patients treated in these practices (outpatients) are to be included in clinical studies successfully, the necessary steps must be incorporated into the practices’ everyday routine. For this purpose, different workflow models, which are currently being implemented and optimised in two pilot practices, were elaborated. Recommendations and proposals for other practices are to be developed on the basis of the obtained results. First assessments have shown that for a successful inclusion of outpatients in clinical studies an infrastructure for several steps is obligate:
• Selection of suitable studies • Administration of studies • List of active studies
Speakers’ Midterm Report: Section 1
52
• Screening for patients in time • Awareness of the doctor
EbM-course: A special impact on the health care system, especially on the hematologists and oncologists in private practices, is exerted through sub-project 5: A course on "Evidence-Based Medicine" (EbM) was designed in cooperation with the Clinical Economics Working Group of Ulm University. As the main speaker acts Prof. Porzsolt, a medical professional in hemato-oncology and a known expert in the field of EbM. In elaborating the curriculum of the course, special attention was paid to the needs of the hematologists and oncologists in private practices. The two-day course is based on questions arising from the everyday clinical practice of the participants, discussing and analysing them with the use of EbM-derived methods (e.g. the likelihood ratio for medical tests). The basic course on the subjects of "therapy, diagnosis and guidelines" has been held two times since May 2001.
Therapy handbook: In a second approach, sub-project 5 also compiled a handbook on the diagnosis, therapy, and aftercare of lymphoma patients. Within the handbook, entities and sub-groups of B-NHL and Hodgkin's disease, which are important for hemato-oncologists in private practices, were specified and subdivided according to relevant risk groups. In addition, the current clinical studies performed by the study groups of the competence network were referenced to the different lymphoma sub-groups. On this basis, the heads of the study groups were provided with a questionnaire containing questions, which are relevant to physicians in private practices in relation to standard therapy. The answers given by the study groups will be integrated into the therapy handbook and made available to the private practices via secure Internet access in close cooperation with sub-project 2.
Collaborations & problems: The Competence Network Malignant Lymphoma represents an important instrument in the cooperation of all major German lymphoma study groups. It bundles and coordinates political activities – often in collaboration with the German Society of Hematology and Oncology (DGHO) and other scientific societies – to enable the future development of a successful clinical research in Germany. Despite the increasing acceptance of new therapies introduced by the members of the competence network, administrational drawbacks still hamper the transfer of these innovative treatment options into the general health care system. As has been referred to in Part A-3, important scientific results were achieved by all the clinical lymphoma study groups involved in the network. While the BMBF has supported the clinical study groups for a long time and also initiated the competence network, these measures are actively counteracted by health insurances. The most important problems are the off-label use of drugs and the treatment of patients in clinical trials. Resulting costs – often the costs of standard therapy – are not refunded in these cases. Here, a clear regulation is required to ensure a successful clinical research in Germany.
Speakers’ Midterm Report: Section 1
53
Part F – Sustainability
F-24. a) Which measures have been installed or are planned to secure the network and its
central facilities and services on the long run?
formal alliance
• company constituted under German law (“Gesellschaft bürgerlichen Rechts“), statutes installed (“Satzung“)?
planned installed
• foundation of a registered association (“eingetragener Verein“)
planned installed
• foundation of a limited liability company (Ltd., "GmbH")
planned installed
engagement of long term financiers (for instance for the instalment of the coordinating unit and the central
services)
acquisition of scientific grants, which were provided due to the existence of the network
acquisition of donations to the benefit of the network ("Spenden")
further measures, please list
b) Describe the strategy to continue the network after the BMBF grant ended. Give the financiers, the amount, kind and period of all additional financial support obtained by the network so far.
In January 2000, the Competence Network Malignant Lymphoma formed itself according to the structure of a registered association. The current statutes define
• the categories of membership
• the election and constitution of the board
• the obligations of each individual member
• the utilisation of research results and patents
• the prerequisites for study groups to join the network
Speakers’ Midterm Report: Section 1
54
In summary, the current competence network „Malignant Lymphoma“ is organised like a scientific society focusing on research and treatment of lymphoma patients. Members of the network are the representatives of the lymphoma study groups, the network’s project leaders and their collaborators. Due to the overall goal of the network to develop a high quality management for the treatment of lymphoma patients, other groups of the health care system have been included in the network’s activities. These „joint“ activities are performed at different levels:
• Members from patient initiatives, the “German Association of Statutory Health Insurance Physicians“ (“Kassenärztliche Bundesvereinigung”) and the pharmaceutical industry participate in the extended board of directors. They are important partners both for the discussion of health-political issues and general questions concerning the current and long-lasting development of the network.
• Close cooperation has been established with the patients’ self-help groups and
the pharmaceutical industry. Together with the “Deutsche Leukämie- und Lymphomhilfe (DLH)” special symposia for patients have been organised. In addition, the patient information on the network’s homepage has been implemented and is currently maintained in collaboration with the DLH. Together with partners from the pharmaceutical industry, a project to support non-university hospitals in clinical documentation has been started in early 2002.
The overall strategy to maintain the network beyond the BMBF grant period is to transform it into a registered association, which offers a membership with equal rights to all groups involved in lymphoma research and therapy, to partners from patient initiatives and from the health insurance system, and to the pharmaceutical industry. Major long-term financial support is especially expected from the pharmaceutical industry and the Statutory Health Insurance. The pharmaceutical industry is a potential financier for project-related sponsoring. A first joint project has already been started, as outlined above. To date, most of the lymphoma study groups are supported by the “Deutsche Krebshilfe e.V.”. Since this support will be available only for a limited period of time, the Statutory Health Insurance is expected to be a potential future financier to support the study groups and health economic projects. One of the most important approaches of the network is to implement GCP-like guidelines for the ongoing and planned lymphoma studies. Here, the network will serve as a guarantor for high quality lymphoma treatment. Furthermore, two approaches have been initiated to ensure the maintenance of the medical/scientific projects of the network: The lymphoma study groups and the reference centres for lymph node pathology are preparing a joint grant application entitled “Molecular Mechanisms in Malignant Lymphoma” which will be submitted to the “Deutsche Krebshilfe”. It is intended to focus the proposal on gene expression in malignant lymphoma. In addition, it is planned to participate in the 6th Framework Programme of the European Community for research, technological development and demonstration activities, which has just been announced. Together with other European lymphoma study and research groups, the competence network will submit a so-called “Expression Of Interest” for the new EU programme „Networks of Excellence“ in June 2002. The speaker of the network is currently establishing contacts to initiate a foundation. By this means, the central structures of the network, i.e. the central office, the IT communication centre and the related IT and telemedical infrastructure, may be further sustained. In order to develop a coherent overall strategy, we have recently contacted an agency for social marketing. On the basis of an informal meeting with this agency, we are considering the
Speakers’ Midterm Report: Section 1
55
following strategy and time schedule for fundraising activities to ensure the long-term sustainability of the network:
• A vision of the future structure and the mission of the network should be formulated until June 2002.
• An analysis of the market and a survey of the resources to be utilised for fundraising activities should be performed until the beginning of the second funding period.
• Potential partners that are already known should be contacted and informed in autumn 2002. A strategy for the acquisition of partners and for accompanying public relations activities has to be worked out until the end of the year 2002.
The beginning of the actual fundraising activities has been scheduled for January 2003. With respect to financial stability, it needs to be taken into account that in an early stage of up to three years the fundraising costs most likely will exceed the fundraising revenues.
Speakers’ Midterm Report: Section 1
56
Part G – Summary of the Status quo and Proposed Activities for the Second Funding Period
G-25. Status Quo. The overall objective of the Competence Network Malignant Lymphoma is to transfer the high standard of lymphoma treatment developed by the lymphoma study groups into the primary health care system. In the first funding period, the network has successfully begun to establish an infrastructure for horizontal and vertical communication among all groups working in lymphoma research and treatment:
1. To date, seven lymphoma study groups are integrated in the network. While the German Hodgkin’s group and the study groups for low- and high-grade lymphoma are founding members, five further study groups were associated within the last two years. In addition, four groups working on the epidemiology of lymphoma joined the network and founded the working group ”Epidemiology of Lymphoma“.
2. The statutes of the network were designed according to those of a registered association. Instruments for communication within the network, for quality assurance and for controlling of finances have been implemented.
3. Close collaborations have been established with different partners from the health care system, patient associations and the pharmaceutical industry. Recently, a joint project between a group of pharmaceutical companies and the network has been initiated to support non-university hospitals in medical documentation.
4. Dissemination of information and knowledge is achieved via Internet, print media, scientific symposia and workshops for patients. Joint symposia have been held with the Competence Network Leukemia. Moreover, press releases and smaller articles are published regularly.
5. The IT technology connecting the network’s IT communication centre at Leipzig University and the three study centres of the major lymphoma study groups is operating. A computer network for the exchange of histo-pathological data between the pathology reference and clinical study centres has been established. Telemedical devices have been set up to exchange diagnostic data between the reference centres for radiotherapy.
6. The topics ”quality management“, “evidence-based medicine” and “health economical aspects” have been addressed by several sub-projects:
o A working group “Quality Management“ has been founded. In the first funding period, the group has elaborated a system of standard operating procedures (SOP system) for the study centres.
o The Cochrane Group “Hematological Malignancies” was founded in October 2000. Two reviews according to the Cochrane guidelines have already been published; six further reviews are in preparation.
o A course on "Evidence-Based Medicine for Hematologists and Oncologists in Private Practices" was designed and is currently held twice per year.
o Network assistants regularly visit the hematological departments of non-university hospitals to support them in their documentation of patients in clinical trials run by the competence network.
o The treatment and medical care of lymphoma patients inside and outside of clinical trials have been compared. In a related approach, the cost effectiveness of both pathways is analysed.
Speakers’ Midterm Report: Section 1
57
7. In three sub-projects, the validity of currently used therapy concepts has been investigated and new therapy concepts are being developed:
o To define the role of high-dose therapy in the treatment of lymphoma patients, the data quality and availability and the communication (IT-based and conventional) between study groups and transplant centres are evaluated.
o A prospective determination of the frequency of secondary hematological neoplasias after myeloablative chemotherapy has been initiated. The detection of early molecular alterations is in the focus of the investigation.
o The analysis of cancer-testis antigen (CTA) expression in Non-Hodgkin’s lymphomas led to the identification of SCP-1, a known CTA, as a promising candidate for lymphoma vaccine development.
Proposed objectives for the second funding period
The objectives from the first funding period are still relevant and will be further pursued in the second part. In the majority of projects, the first results - as listed above - were achieved during the first funding period. In some projects, i.e. epidemiological projects, the relevant data were collected; the corresponding analysis will be performed in the next funding period.
The overall objective of the Competence Network Malignant Lymphoma is to make the best information and treatment available to each lymphoma patient in Germany. To achieve this goal, the following general and specific objectives have been drafted for next funding period:
1. Integration of all German lymphoma study groups
2. Dissemination of information:
o Transfer of the present Internet presentation into an information portal for lymphoma research and treatment
o Expansion of the information provided on the patients’ part of the network’s homepage
o Extension of public relations activities
3. Vertical transfer of information and support:
o Intensification of the contact between private practitioners and community hospitals on the one hand and university clinics on the other hand
o Further integration of practitioners into clinical trials
o Increased support in medical documentation for non-university hospitals and practitioners
4. Quality management:
o Extension of the catalogue of “Standard Operation Procedures” for the lymphoma study groups
o Implementation of GCP-like guidelines in lymphoma studies
o Harmonisation of the patient documentation forms in lymphoma studies
5. Medical education:
o Development of an educational program for physicians
o Designing special training courses for lymphoma documentation
Speakers’ Midterm Report: Section 1
58
7. Health political issues:
o Implementation and support of patients’ advocacy
o Negotiation with insurance companies and politicians to ascertain funding for clinical trials in Germany
8. Sustainability:
o Transfer of the present network into a registered association
o Integration of all relevant groups from the health care system into the future association
o Starting professional fundraising activities
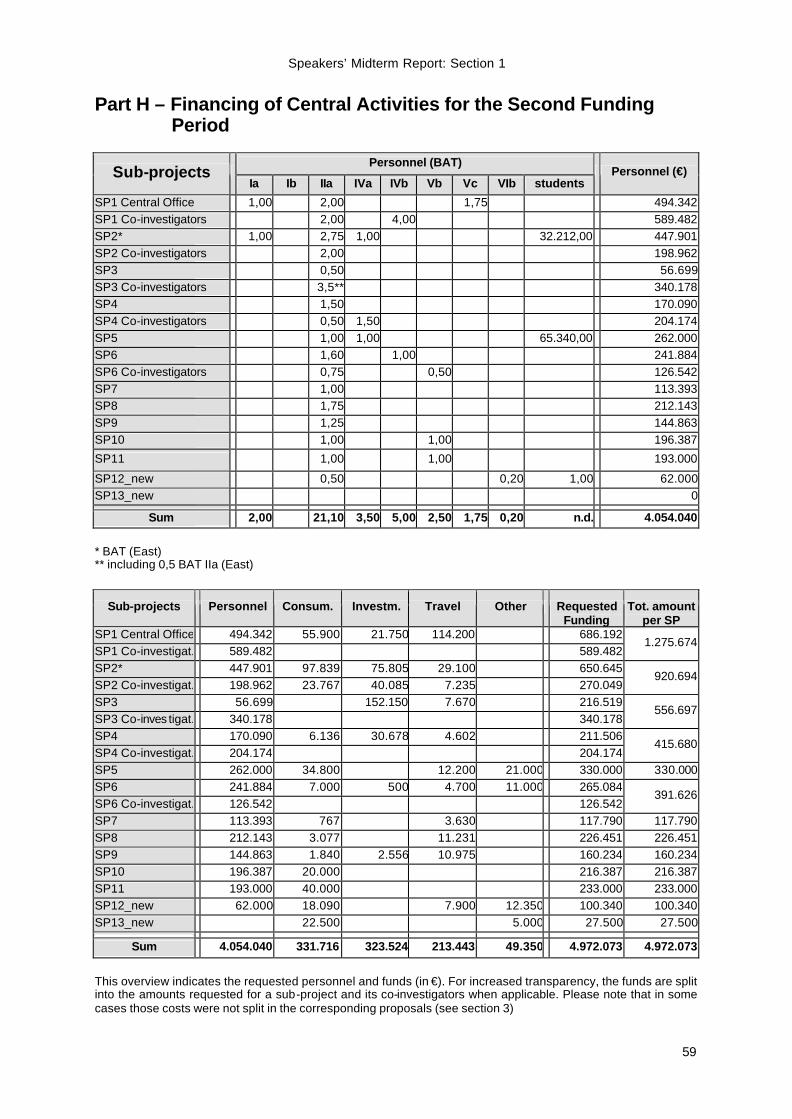
Speakers’ Midterm Report: Section 1
59
Part H – Financing of Central Activities for the Second Funding Period
Personnel (BAT)
Sub-projects Ia Ib IIa IVa IVb Vb Vc VIb students
Personnel (€)
SP1 Central Office 1,00 2,00 1,75 494.342SP1 Co-investigators 2,00 4,00 589.482SP2* 1,00 2,75 1,00 32.212,00 447.901SP2 Co-investigators 2,00 198.962SP3 0,50 56.699SP3 Co-investigators 3,5** 340.178SP4 1,50 170.090SP4 Co-investigators 0,50 1,50 204.174SP5 1,00 1,00 65.340,00 262.000SP6 1,60 1,00 241.884SP6 Co-investigators 0,75 0,50 126.542SP7 1,00 113.393SP8 1,75 212.143SP9 1,25 144.863SP10 1,00 1,00 196.387
SP11 1,00 1,00 193.000
SP12_new 0,50 0,20 1,00 62.000SP13_new 0 Sum 2,00 21,10 3,50 5,00 2,50 1,75 0,20 n.d. 4.054.040
* BAT (East) ** including 0,5 BAT IIa (East)
Sub-projects Personnel Consum. Investm. Travel Other Requested Funding
Tot. amount per SP
SP1 Central Office 494.342 55.900 21.750 114.200 686.192SP1 Co-investigat. 589.482 589.482
1.275.674
SP2* 447.901 97.839 75.805 29.100 650.645SP2 Co-investigat. 198.962 23.767 40.085 7.235 270.049
920.694
SP3 56.699 152.150 7.670 216.519SP3 Co-inves tigat. 340.178 340.178
556.697
SP4 170.090 6.136 30.678 4.602 211.506SP4 Co-investigat. 204.174 204.174
415.680
SP5 262.000 34.800 12.200 21.000 330.000 330.000SP6 241.884 7.000 500 4.700 11.000 265.084SP6 Co-investigat. 126.542 126.542
391.626
SP7 113.393 767 3.630 117.790 117.790SP8 212.143 3.077 11.231 226.451 226.451SP9 144.863 1.840 2.556 10.975 160.234 160.234SP10 196.387 20.000 216.387 216.387SP11 193.000 40.000 233.000 233.000SP12_new 62.000 18.090 7.900 12.350 100.340 100.340SP13_new 22.500 5.000 27.500 27.500 Sum 4.054.040 331.716 323.524 213.443 49.350 4.972.073 4.972.073
This overview indicates the requested personnel and funds (in €). For increased transparency, the funds are split into the amounts requested for a sub-project and its co-investigators when applicable. Please note that in some cases those costs were not split in the corresponding proposals (see section 3)
61
Section 2
Cover Page to list the Research Projects
Title Page
Network title: Malignant Lymphoma Period covered by this report: 10/1999 – 09/2002 1st funding period 10/2002 – 09/2004 2nd funding period
List of projects covered by this report: Grant No.: 01GI9991
Project Title: Sub-project 1 - Central Office
Scientist-in-charge: Prof. Dr. Volker Diehl PD Dr. Annegret Herrmann-Frank
Institution: Kompetenznetz Maligne Lymphome Klinik I für Innere Medizin Universität zu Köln Page: 65 Grant No.: 01GI9995
Project Title: Sub-project 2 - Telematics and computer-based quality management in a communication network
Scientist-in-charge: Dr. Barbara Heller Prof. Dr. Markus Löffler
Institution: Institut für Medizinische Informatik, Statistik und Epidemiologie (IMISE) Universität Leipzig Page: 83 Grant No.: 01GI9996
Project Title: Sub-project 3 - Integrated network of the reference panel for lymph node pathology
Scientist-in-charge: PD Dr. Michael Hummel
Institution: Institut für Pathologie Universitätsklinikum Benjamin Franklin Freie Universität Berlin Page: 107
Speakers’ Midterm Report: Section 2
62
Grant No.: 01GI9991
Project Title: Sub-project 4 - Quality assurance of radiotherapy due to initiation of a medical network for patients in German lymphoma studies
Scientist-in-charge: Prof. Dr. Rolf-Peter Müller PD Dr. Susanne Staar
Institution: Klinik und Poliklinik für Strahlentherapie Universität zu Köln Page: 121 Grant No.: 01GI9995
Project Title: Sub-project 5 - Quality management in the care of lymphoma patients in private outpatient clinics for hematology and oncology
Scientist-in-charge: PD Dr. Stephan Schmitz
Institution: Schwerpunktpraxis für Hämatologie und Onkologie
Köln Page: 135 Grant No.: 01GI9991
Project Title: Sub-project 6 - Diagnosis, treatment and treatment results of lymphoma patients: comparison between clinical trials and general care
Scientist-in-charge: Dr. Ursula Paulus
Institution: Klinik I für Innere Medizin Universität zu Köln Page: 151 Grant No.: 01GI9991
Project Title: Sub-project 7 - Prospective health economic evaluation of medical care for patients with malignant lymphomas
Scientist-in-charge: Dr. Ronald Walshe Prof. Dr. Dr. Karl Lauterbach
Institution: Klinik I für Innere Medizin Universität zu Köln Page: 173 Grant No.: 01GI9995
Project Title: Sub-project 8a - Model-based meta-regression to estimate dose/efficacy relationships of poly-chemotherapies
Scientist-in-charge: Dr. Dirk Hasenclever Prof. Dr. Markus Löffler
Institution: Institut für Medizinische Informatik, Statistik und Epidemiologie (IMISE) Universität Leipzig Page: 193
Speakers’ Midterm Report: Section 2
63
Grant No.: 01GI9991
Project Title: Sub-project 8b - Establishment of a Cochrane Hematological Malignancies Group (CHMG)
Scientist-in-charge: Prof. Dr. Andreas Engert
Institution: Klinik I für Innere Medizin Universität zu Köln Page: 199 Grant No.: 01GI9992
Project Title: Sub-project 9 - High-dose therapy and transplantation of hematopoietic stem cells in malignant lymphoma
Scientist-in-charge: Prof. Dr. Norbert Schmitz Dr. Astrid Schloen Stefan Wolf PD Dr. Bertram Glaß
Institution: Hämatologische Abteilung Allgemeines Krankenhaus St. Georg, Hamburg Page: 215 Grant No.: 01GI9994
Project Title: Sub-project 10 - Long term effects of myeloablative radiochemotherapy with consecutive autologous peripheral blood stem cell transplantation in patients with malignant lymphomas - frequency and early diagnosis of secondary hematological neoplasias
Scientist-in-charge: Prof. Dr. Wolfgang Hiddemann PD Dr. Martin Dreyling
Institution: Medizinische Klinik III Universitätsklinikum Großhadern LMU München Page: 235 Grant No.: 01GI9993
Project Title: Sub-project 11 - Development of strategies for immunological and genetherapeutic vaccines for malignant lymphomas
Scientist-in-charge: Prof. Dr. Michael Pfreundschuh
Institution: Medizinische Klinik I Universität des Saarlandes Page: 253 Grant No.: new
Project Title: Sub-project 12_new - Clinical therapy optimisation protocols in cytostatic and radiotherapy of patients with Hodgkin's disease and high-grade lymphoma (TOPiCS-ML)
Scientist-in-charge: PD Dr. Wolfgang Hoffmann
Institution: Bremer Institut für Präventionsforschung, Sozialmedizin und Epidemiologie (BIPSE) Universität Bremen Page: 265
Speakers’ Midterm Report: Section 2
64
Grant No.: new
Project Title: Sub-project 13_new - Improvement of the infrastructure for the analysis of biologic risk factors in malignant lymphomas
Scientist-in-charge: PD Dr. Martin Bentz PD Dr. Martin Dreyling
Institution: Abt. Innere Medizin III Universität Ulm Medizinische Klinik III Universitätsklinikum Großhadern LMU München Page: 283





























