Embed Size (px)
Citation preview
ECHOCARDIOGRAPY ECHOCARDIOGRAPY
IN ADULT IN ADULT
CONGENITAL HEART CONGENITAL HEART
DISEASEDISEASE
�� Adult congenital heart disease have a variety of Adult congenital heart disease have a variety of abnormalities.abnormalities.
�� Includes: Includes:
i. Left sided outflow abnormalitiesi. Left sided outflow abnormalities
ii. Right sided outflow abnormalitiesii. Right sided outflow abnormalities
iii. Left to Right shunting lesioniii. Left to Right shunting lesion
iv. Cyanotic congenital defectiv. Cyanotic congenital defect
v. Valve abnormalitiesv. Valve abnormalities
�� The most common diagnoses areThe most common diagnoses are
-- VSDVSD
-- ASDASD
-- ASAS
-- TOFTOF
-- CoartationCoartation
-- TGATGA
-- AVSDAVSD
( Ohio State University Medical Centre 1996 to 1999 )( Ohio State University Medical Centre 1996 to 1999 )
�� Untreated congenital heart disease during childhood Untreated congenital heart disease during childhood can become more complex in terms of patient can become more complex in terms of patient managementmanagement
�� Pulmonary hypertension is the primary cause a change Pulmonary hypertension is the primary cause a change in the patientin the patient’’s life.s life.
�� Medical therapy , cardiac intervention and also cardiac Medical therapy , cardiac intervention and also cardiac surgery is needed to treat these patient .surgery is needed to treat these patient .
�� In our institution a lot of complex congenital heart diseases arIn our institution a lot of complex congenital heart diseases are commonly e commonly seen.seen.
�� Almost all congenital heart diseases require particular attentiAlmost all congenital heart diseases require particular attention during the on during the echo assessment. These include: echo assessment. These include:
1. ASD1. ASD
2. VSD2. VSD
3. TOF3. TOF
4. PDA4. PDA
5. TGA5. TGA
6. CCTGA6. CCTGA
7. 7. EbsteinEbstein’’ss AnomalyAnomaly
8. 8. CoartationCoartation
9. Pulmonary Stenosis9. Pulmonary Stenosis
ASDASD
�� Deficiency of tissue from the Deficiency of tissue from the interatrialinteratrial septumseptum
�� About 7 to 10% of infants with congenital heart disease have ASDAbout 7 to 10% of infants with congenital heart disease have ASD
�� In 30 % of ASD other associated lesions are:In 30 % of ASD other associated lesions are:
1. Partial or total anomalous venous drainage1. Partial or total anomalous venous drainage
2. Congenital mitral stenosis2. Congenital mitral stenosis
3. Mitral Valve 3. Mitral Valve ProlapseProlapse
4. Ventricle Septal Defect4. Ventricle Septal Defect
5. PDA5. PDA
6. Pulmonary Stenosis6. Pulmonary Stenosis
7. Coarctation Of Aorta7. Coarctation Of Aorta
TYPES OF ASDTYPES OF ASD
ASDASD
OSTIUM OSTIUM
SECUNDUMSECUNDUM
OSTIUM OSTIUM
PRIMUMPRIMUM
SINUS SINUS
VENOSUSVENOSUS
CORONARY CORONARY
SINUS DEFECTSINUS DEFECT
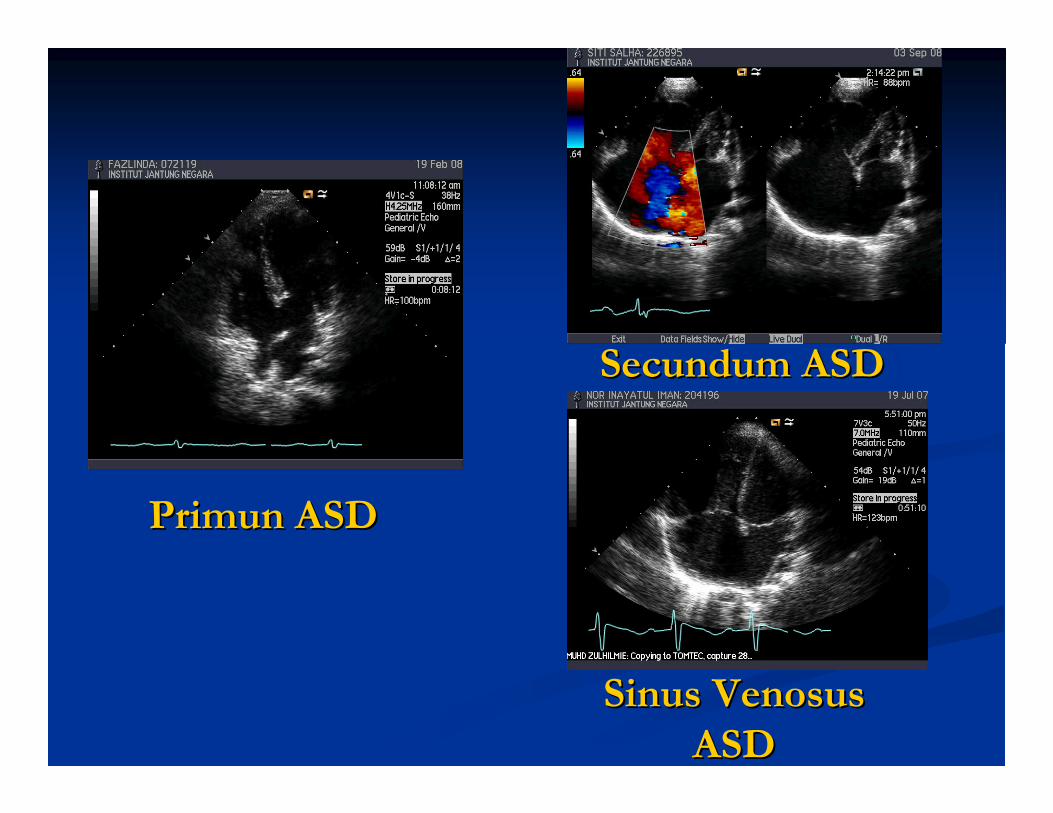
Primun ASDPrimun ASD
Secundum ASDSecundum ASD
Sinus Sinus VenosusVenosus
ASDASD
TYPES OF VSDTYPES OF VSD
VSDVSD
PERIMEMBRANOUSPERIMEMBRANOUS MUSCULARMUSCULAR DCSADCSA INLETINLET
�� Perimembranous VSDPerimembranous VSD-- Located at the junction of muscular, atrioventricular Located at the junction of muscular, atrioventricular & outlet portion of the septum& outlet portion of the septum
-- Immediately adjacent to the aortic and tricuspid Immediately adjacent to the aortic and tricuspid valvevalve
-- Muscular Muscular VSDsVSDs are surrounded by a complete muscular rim and are are surrounded by a complete muscular rim and are most often located in the apical two thirds of septal myocardiummost often located in the apical two thirds of septal myocardium..
-- Muscular defect can also presentMuscular defect can also present in the posterior inlet septumin the posterior inlet septum
�� Muscular VSDMuscular VSD
�� Doubly Committed Doubly Committed SubarterialSubarterial VSD VSD
( DCSA( DCSA ))
-- Located in the outlet septumLocated in the outlet septum
-- Defect adjacent to aortic & pulmonary valve annulusDefect adjacent to aortic & pulmonary valve annulus
-- RCC frequently prolapsed into VSD causing aortic valve RCC frequently prolapsed into VSD causing aortic valve
regurgitationregurgitation
�� Inlet VSD Inlet VSD
-- This VSD usually occur as part of a complete AV canal defect butThis VSD usually occur as part of a complete AV canal defect but it may it may
occasionally be seen in isolation.occasionally be seen in isolation.
-- This type VSD occur near the AV valves .This type VSD occur near the AV valves .
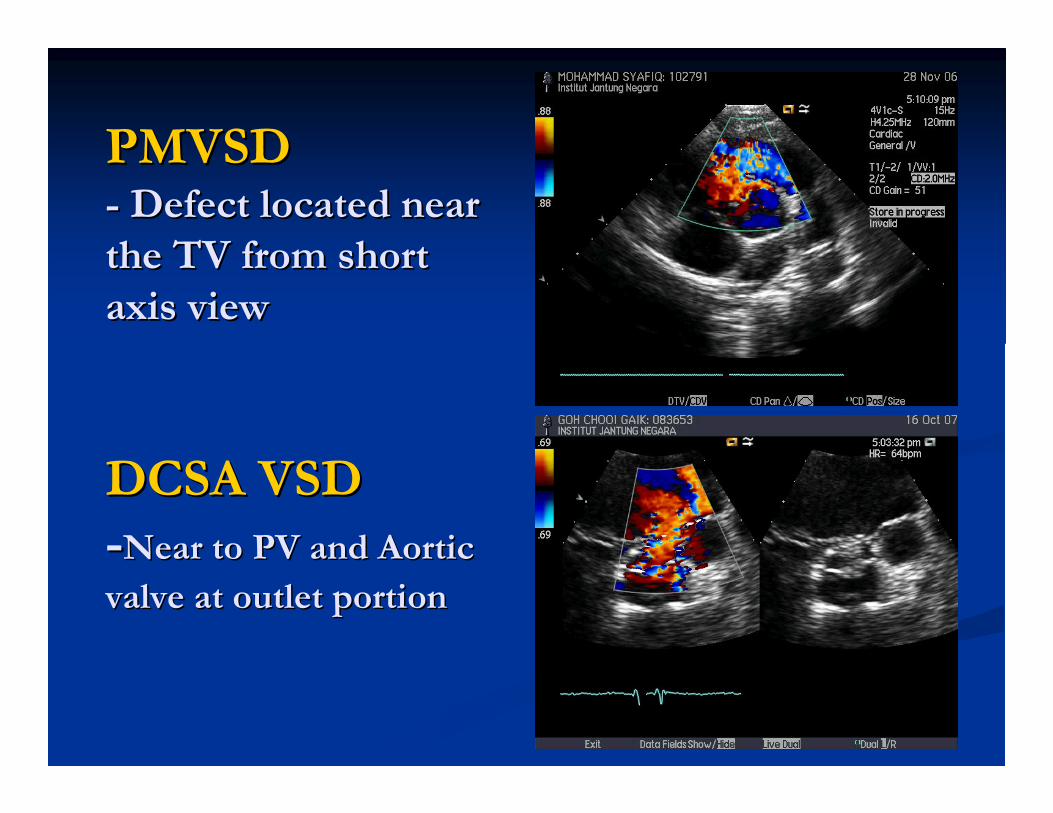
PMVSDPMVSD-- Defect located near Defect located near
the TV from short the TV from short
axis viewaxis view
DCSA VSDDCSA VSD
--Near to PV and Aortic Near to PV and Aortic
valve at outlet portionvalve at outlet portion
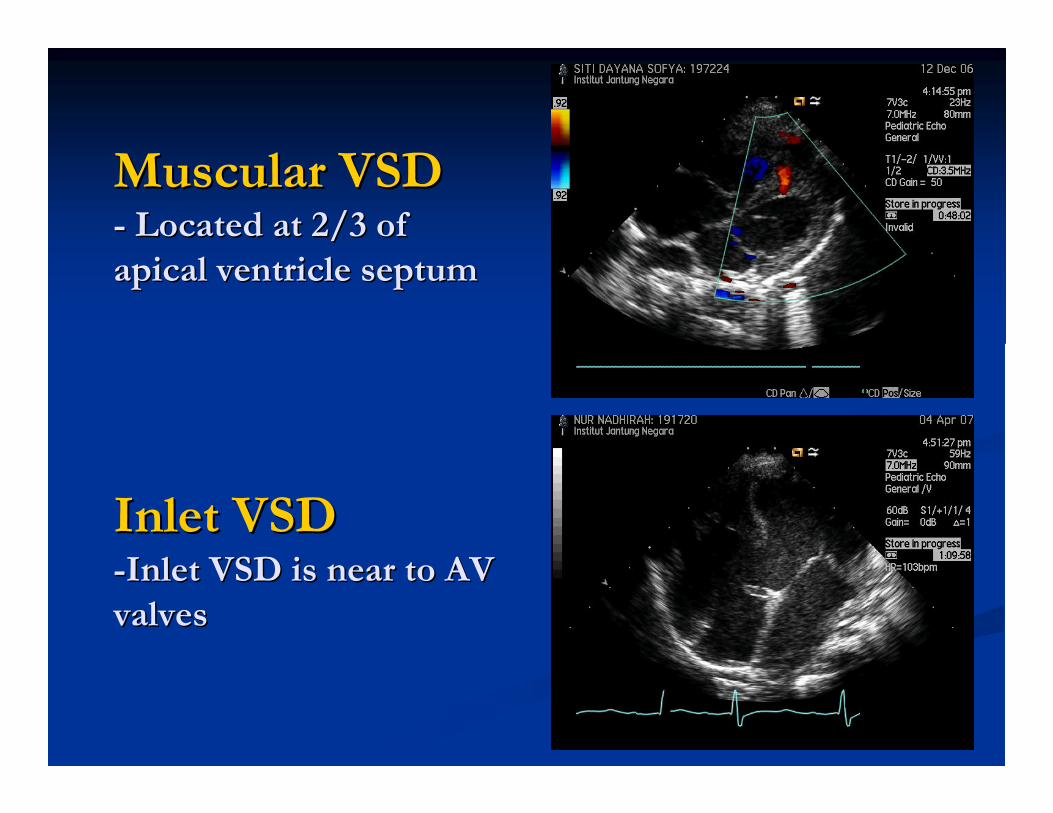
Muscular VSDMuscular VSD-- Located at 2/3 of Located at 2/3 of
apical ventricle septumapical ventricle septum
Inlet VSDInlet VSD--Inlet VSD is near to AV Inlet VSD is near to AV
valves valves
PDAPDA�� Ductus arteriosus close in the Ductus arteriosus close in the
first 48 hours after birthfirst 48 hours after birth
�� More common in female than More common in female than malemale
�� Size and origin of the duct variesSize and origin of the duct varies
�� PDA shunt is determined by the PDA shunt is determined by the resistance of the duct and the resistance of the duct and the level of PVRlevel of PVR
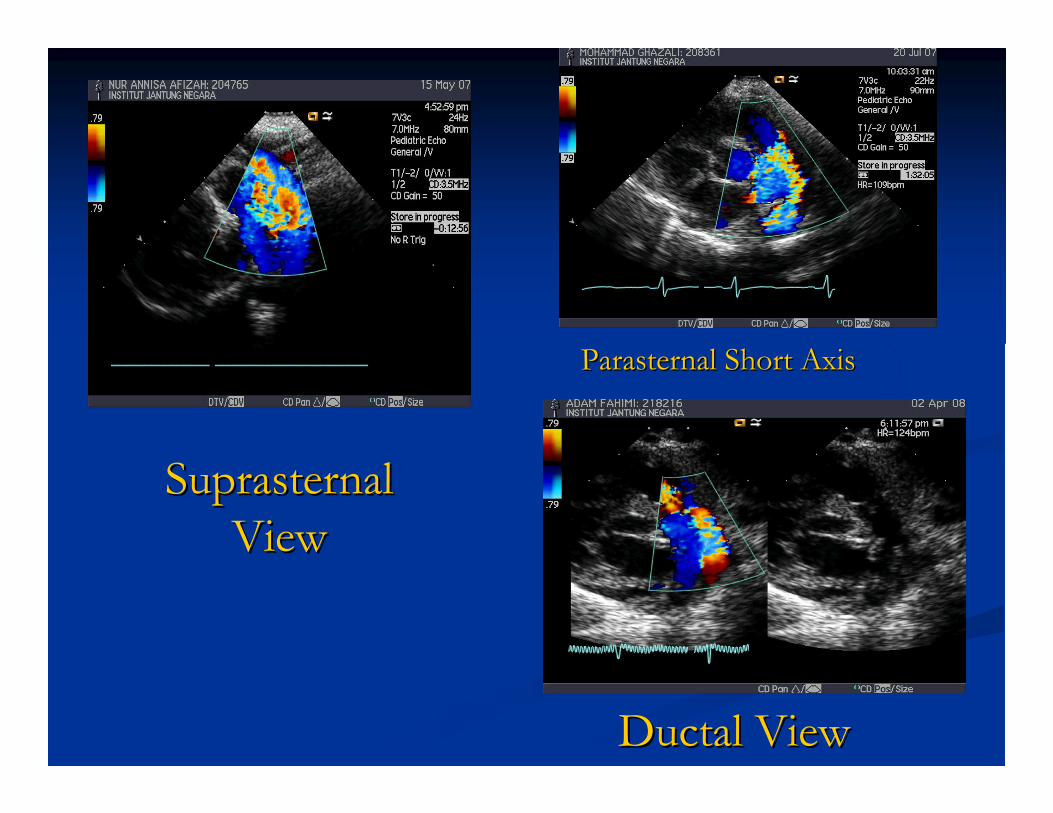
Ductal ViewDuctal View
Parasternal Short AxisParasternal Short Axis
Suprasternal Suprasternal
ViewView
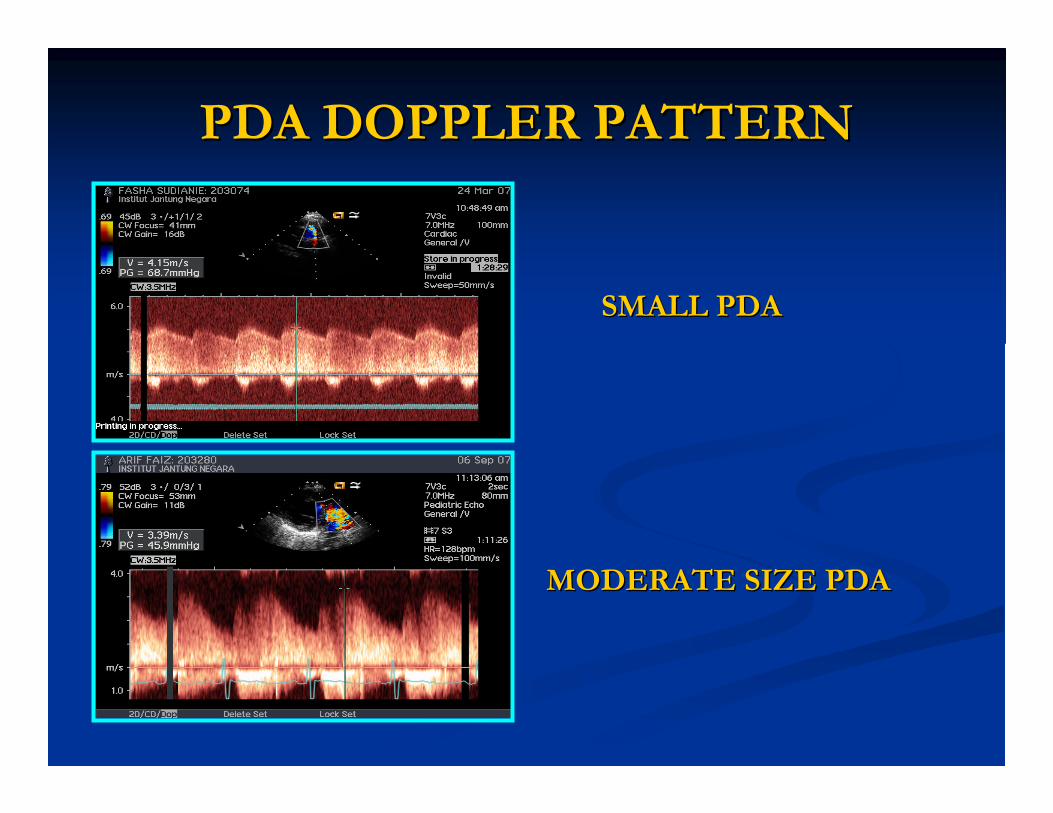
PDA DOPPLER PATTERNPDA DOPPLER PATTERN
SMALL PDASMALL PDA
MODERATE SIZE PDAMODERATE SIZE PDA
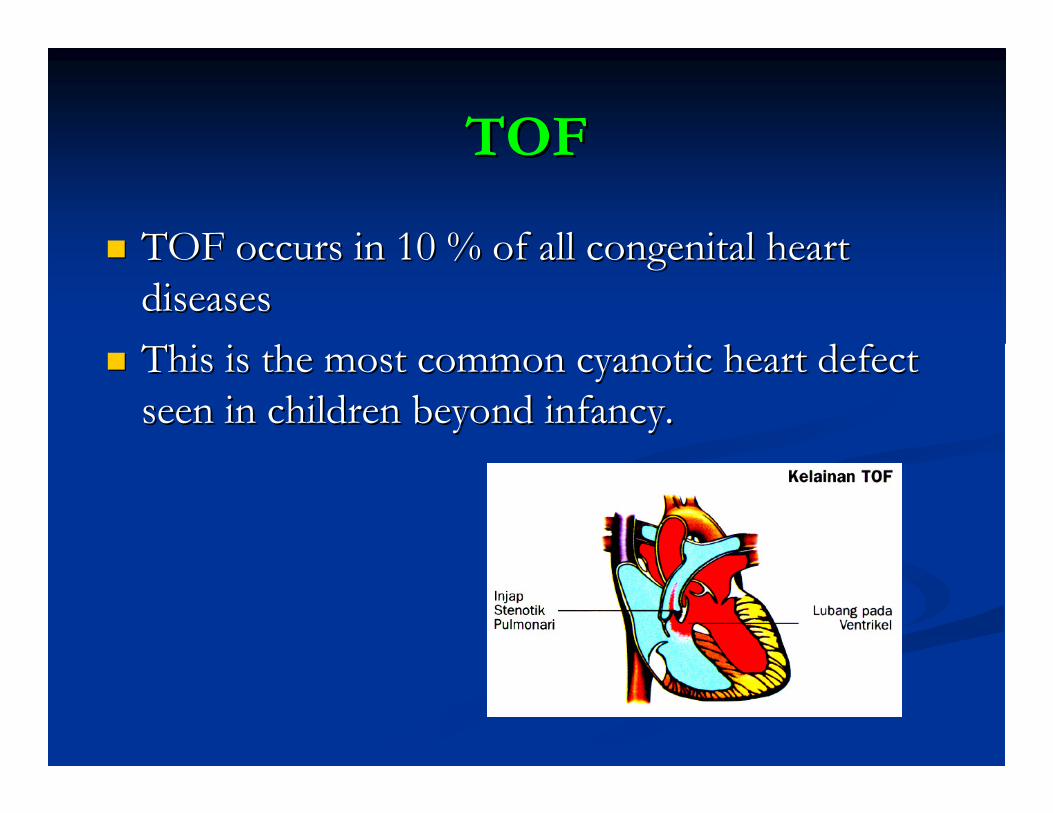
TOFTOF
�� TOF occurs in 10 % of all congenital heart TOF occurs in 10 % of all congenital heart
diseasesdiseases
�� This is the most common cyanotic heart defect This is the most common cyanotic heart defect
seen in children beyond infancy.seen in children beyond infancy.
PathologyPathology
�� The description of TOF includes 4 The description of TOF includes 4
abnormalities :abnormalities :
-- Large VSDLarge VSD
-- Right Ventricle Outflow ObstructionRight Ventricle Outflow Obstruction
-- Right Ventricle HypertrophyRight Ventricle Hypertrophy
-- Overriding of AortaOverriding of Aorta
�� The most frequent form of RVOT obstruction The most frequent form of RVOT obstruction
is infundibular stenosis (45%) and is infundibular stenosis (45%) and PulmPulm. .
ValvularValvular stenosis (10%). A combination of 2 stenosis (10%). A combination of 2
may also occur (30%).may also occur (30%).
�� Usually Usually PulmPulm. Valve annulus and main PA are . Valve annulus and main PA are
hypoplastic in most patient.hypoplastic in most patient.
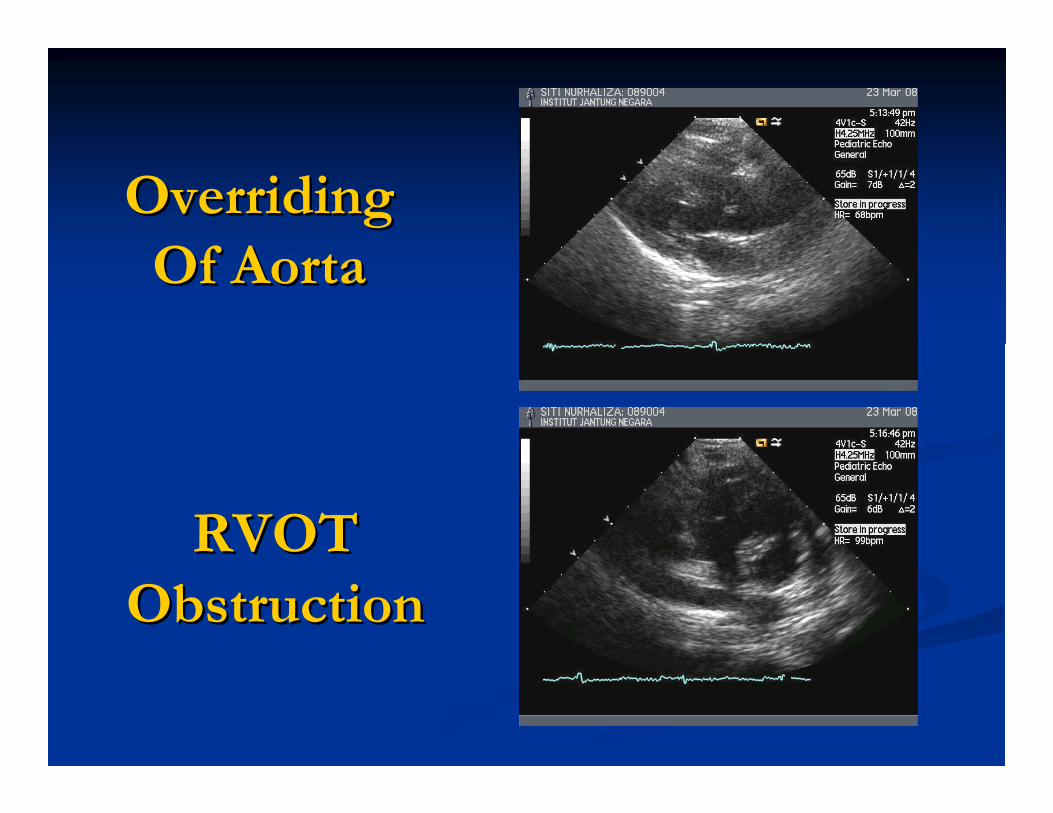
Overriding Overriding
Of AortaOf Aorta
RVOT RVOT
ObstructionObstruction
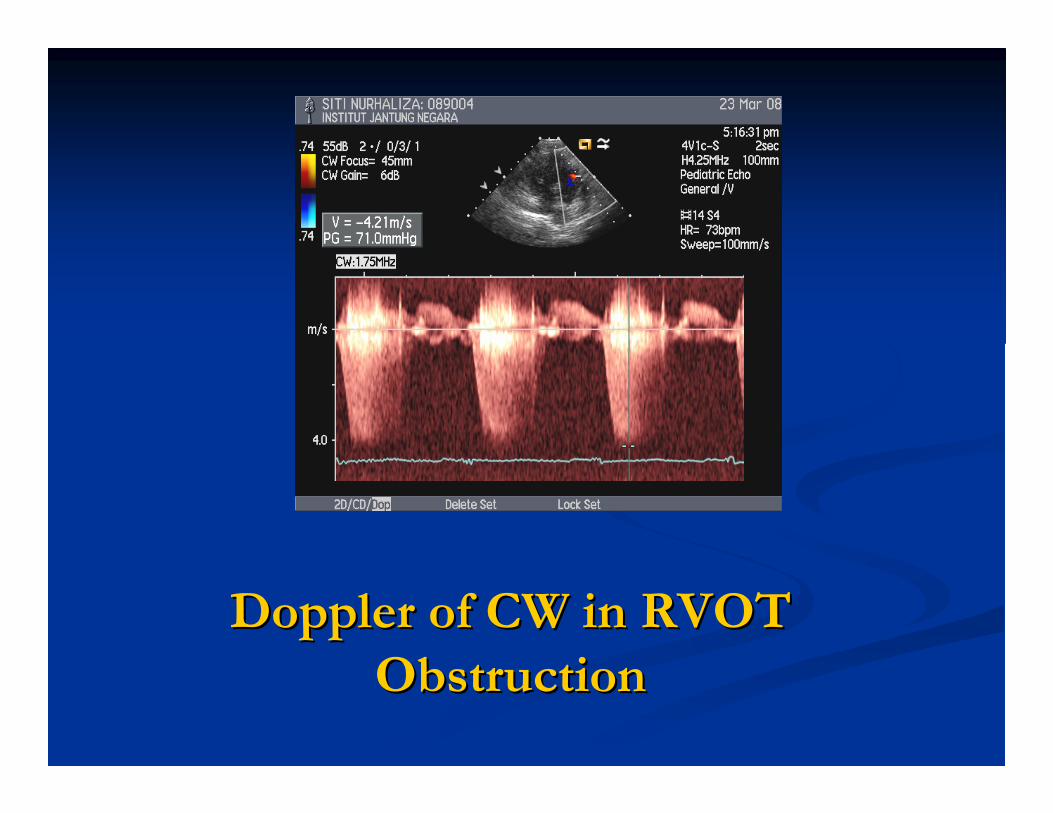
Doppler of CW in RVOT Doppler of CW in RVOT
ObstructionObstruction
What do u think?What do u think?
TGATGA
�� DD-- TGA occur in about 5 % of all congenital heart defect. It is TGA occur in about 5 % of all congenital heart defect. It is most common in males than in females ( 3 : 1)most common in males than in females ( 3 : 1)
�� In adult population DIn adult population D-- TGA (simple TGA) is a rare condition . TGA (simple TGA) is a rare condition . But TGA will present with other complex lesion in adult such as But TGA will present with other complex lesion in adult such as TGA with VSD and PS. TGA with VSD and PS.
�� TGA without ASD or VSD will not present in adult population TGA without ASD or VSD will not present in adult population because usually they either require early surgical intervention because usually they either require early surgical intervention or or die early.die early.
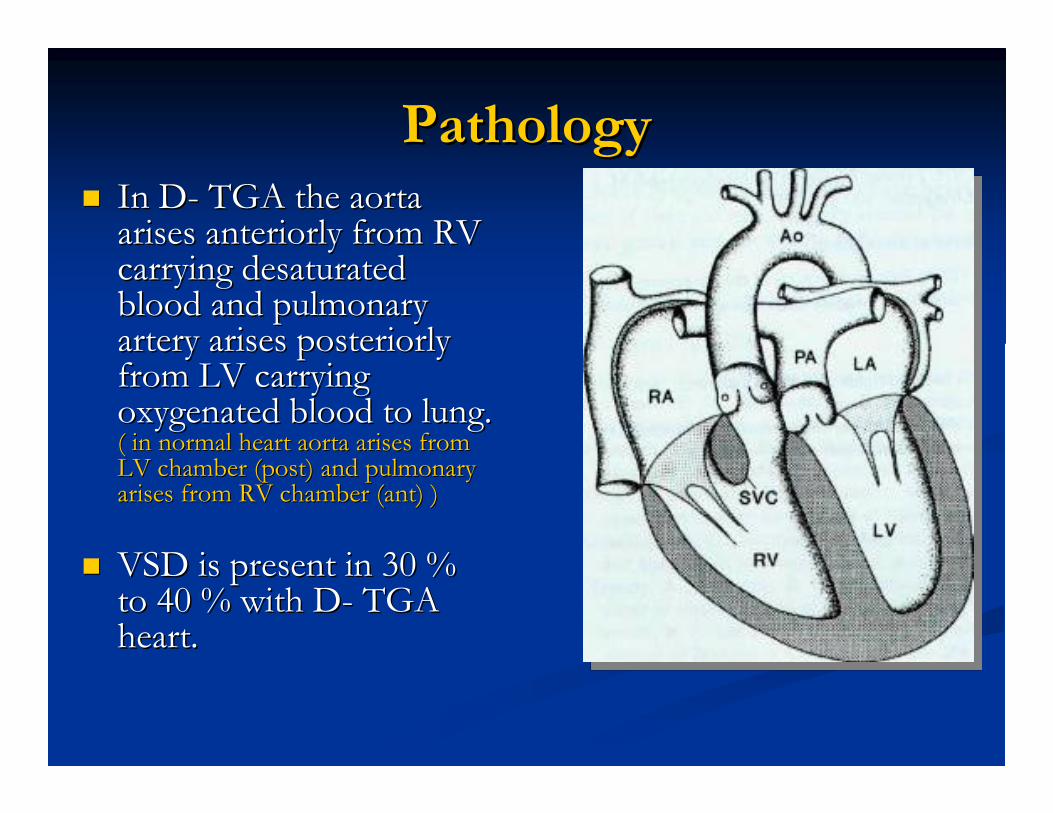
PathologyPathology�� In DIn D-- TGA the aorta TGA the aorta
arises arises anteriorlyanteriorly from RV from RV carrying carrying desaturateddesaturatedblood and pulmonary blood and pulmonary artery arises artery arises posteriorlyposteriorlyfrom LV carrying from LV carrying oxygenated blood to lung. oxygenated blood to lung. ( in normal heart aorta arises from ( in normal heart aorta arises from LV chamber (post) and pulmonary LV chamber (post) and pulmonary arises from RV chamber (ant) )arises from RV chamber (ant) )
�� VSD is present in 30 % VSD is present in 30 % to 40 % with Dto 40 % with D-- TGA TGA heart.heart.
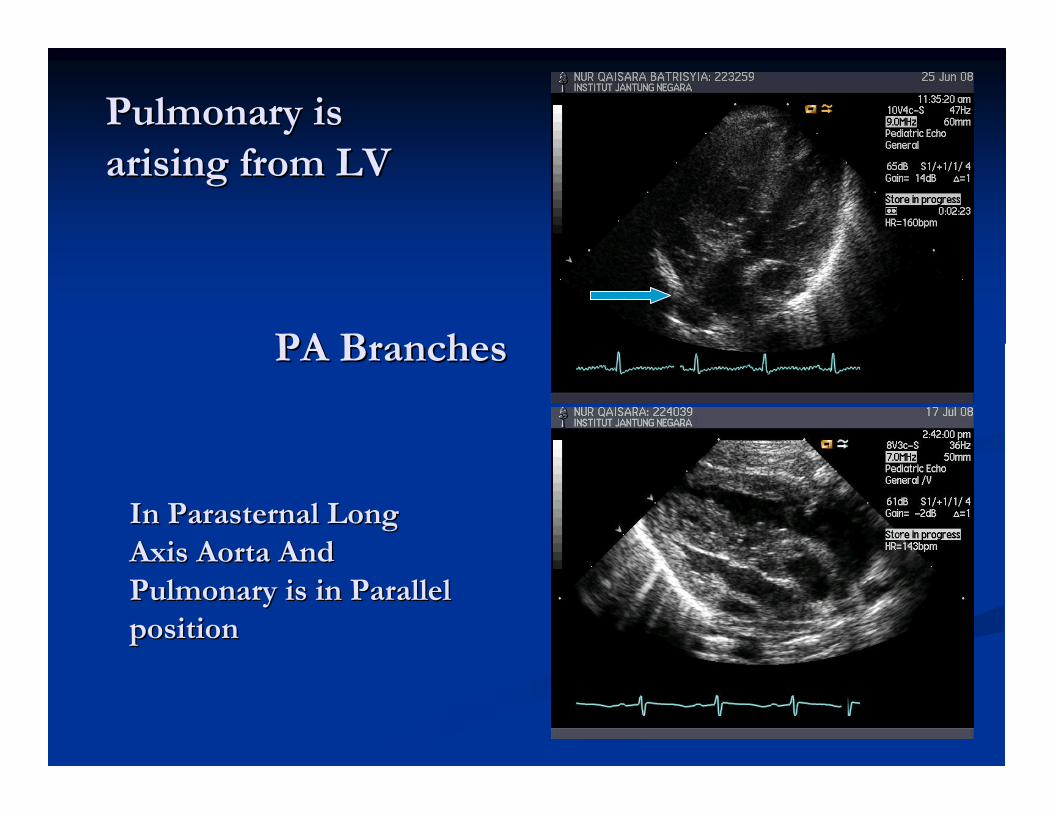
Pulmonary is Pulmonary is
arising from LVarising from LV
PA BranchesPA Branches
In Parasternal Long In Parasternal Long
Axis Aorta And Axis Aorta And
Pulmonary is in Parallel Pulmonary is in Parallel
positionposition
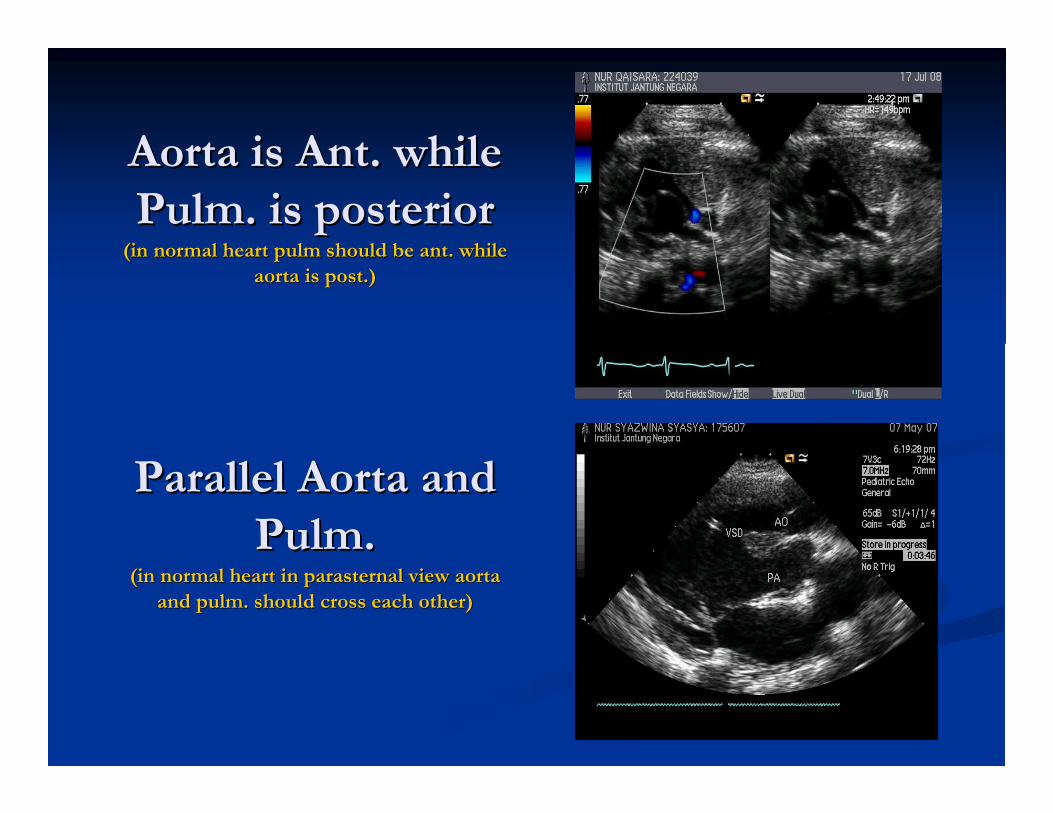
Aorta is Ant. while Aorta is Ant. while
PulmPulm. is posterior. is posterior(in normal heart (in normal heart pulmpulm should be ant. while should be ant. while
aorta is post.)aorta is post.)
Parallel Aorta and Parallel Aorta and
PulmPulm..(in normal heart in (in normal heart in parasternalparasternal view aorta view aorta
and and pulmpulm. should cross each other). should cross each other)
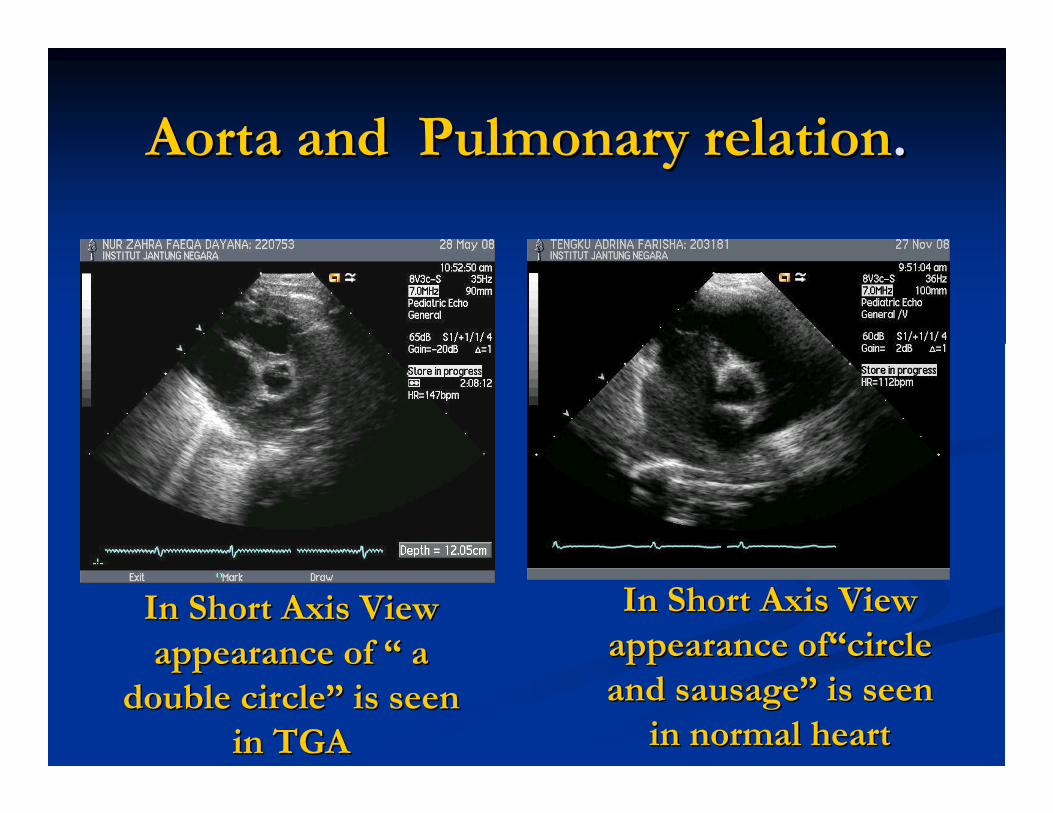
Aorta and Pulmonary relationAorta and Pulmonary relation..
In Short Axis View In Short Axis View
appearance of appearance of ““ a a
double circledouble circle”” is seen is seen
in TGAin TGA
In Short Axis View In Short Axis View
appearance appearance ofof““circlecircle
and sausageand sausage”” is seen is seen
in normal heartin normal heart
CCTGACCTGA
�� Congenitally Corrected Transposition Great Congenitally Corrected Transposition Great
Artery ( or ventricle inversion ) occurs in < 1 Artery ( or ventricle inversion ) occurs in < 1
% of all patient with congenital heart disease.% of all patient with congenital heart disease.
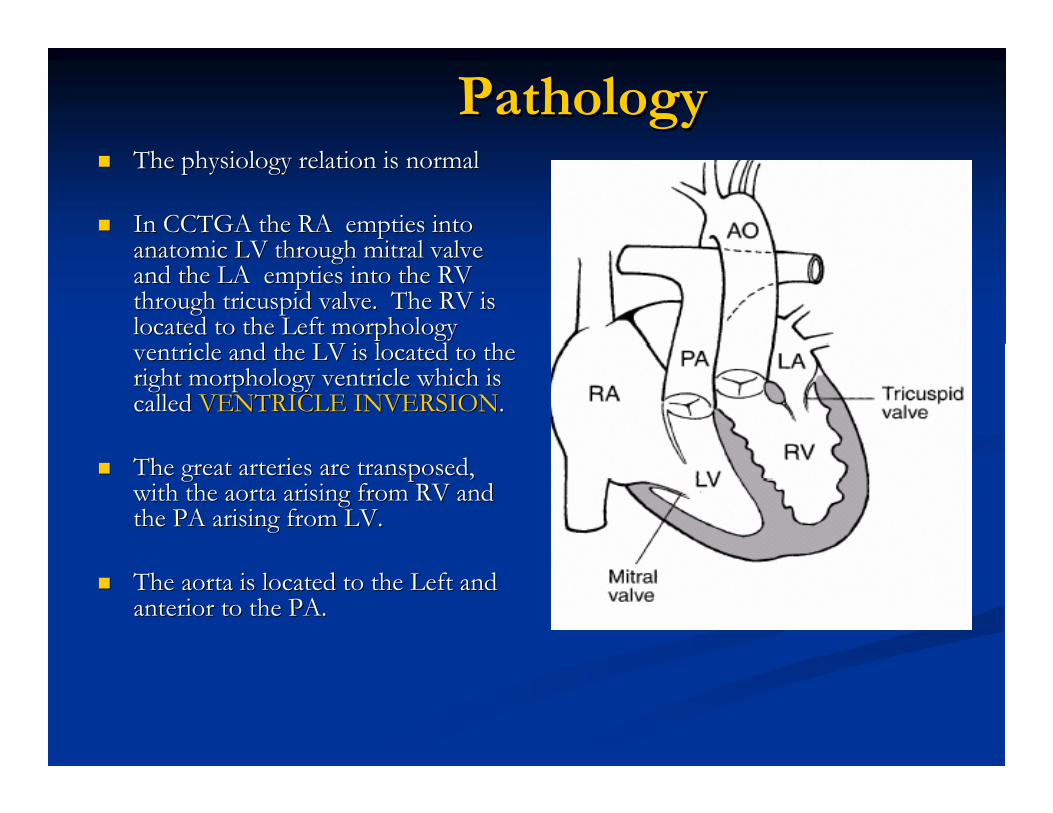
PathologyPathology�� The physiology relation is normalThe physiology relation is normal
�� In CCTGA the RA empties into In CCTGA the RA empties into anatomic LV through mitral valve anatomic LV through mitral valve and the LA empties into the RV and the LA empties into the RV through tricuspid valve. The RV is through tricuspid valve. The RV is located to the Left morphology located to the Left morphology ventricle and the LV is located to the ventricle and the LV is located to the right morphology ventricle which is right morphology ventricle which is called called VENTRICLE INVERSIONVENTRICLE INVERSION..
�� The great arteries are transposed, The great arteries are transposed, with the aorta arising from RV and with the aorta arising from RV and the PA arising from LV.the PA arising from LV.
�� The aorta is located to the Left and The aorta is located to the Left and anterior to the PA.anterior to the PA.
�� About 50 % of CCTGA have About 50 % of CCTGA have dextrocardiadextrocardia..
�� In CCTGA theoretically no functional In CCTGA theoretically no functional anomalies but most cases are complicated by anomalies but most cases are complicated by associated associated intracardiacintracardiac defect and arrhythmiasdefect and arrhythmias
�� The main issue is that the RV is now the The main issue is that the RV is now the systemic ventricle and the natural history is that systemic ventricle and the natural history is that it will start to fail in the 3it will start to fail in the 3rdrd--44thth decade of life.decade of life.
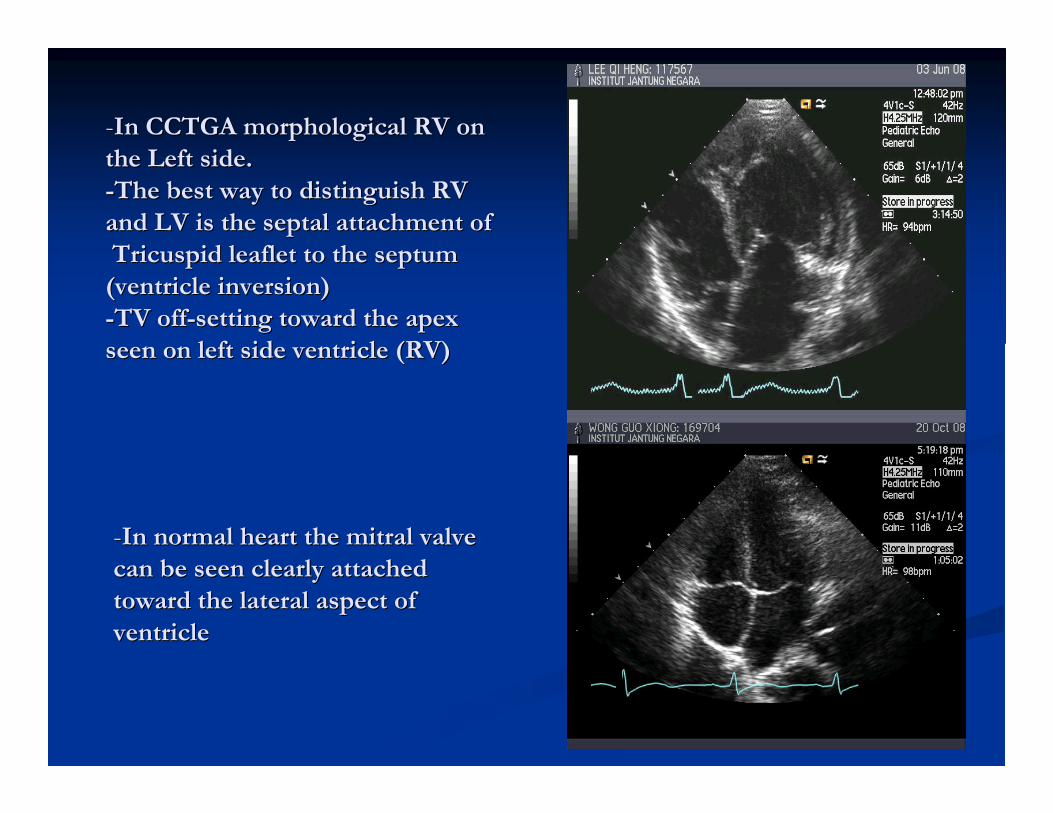
--In CCTGA morphological RV on In CCTGA morphological RV on
the Left side.the Left side.
--The best way to distinguish RV The best way to distinguish RV
and LV is the septal attachment of and LV is the septal attachment of
Tricuspid leaflet to the septum Tricuspid leaflet to the septum
(ventricle inversion)(ventricle inversion)
--TV offTV off--setting toward the apex setting toward the apex
seen on left side ventricle (RV)seen on left side ventricle (RV)
--In normal heart the mitral valve In normal heart the mitral valve
can be seen clearly attached can be seen clearly attached
toward the lateral aspect of toward the lateral aspect of
ventricleventricle
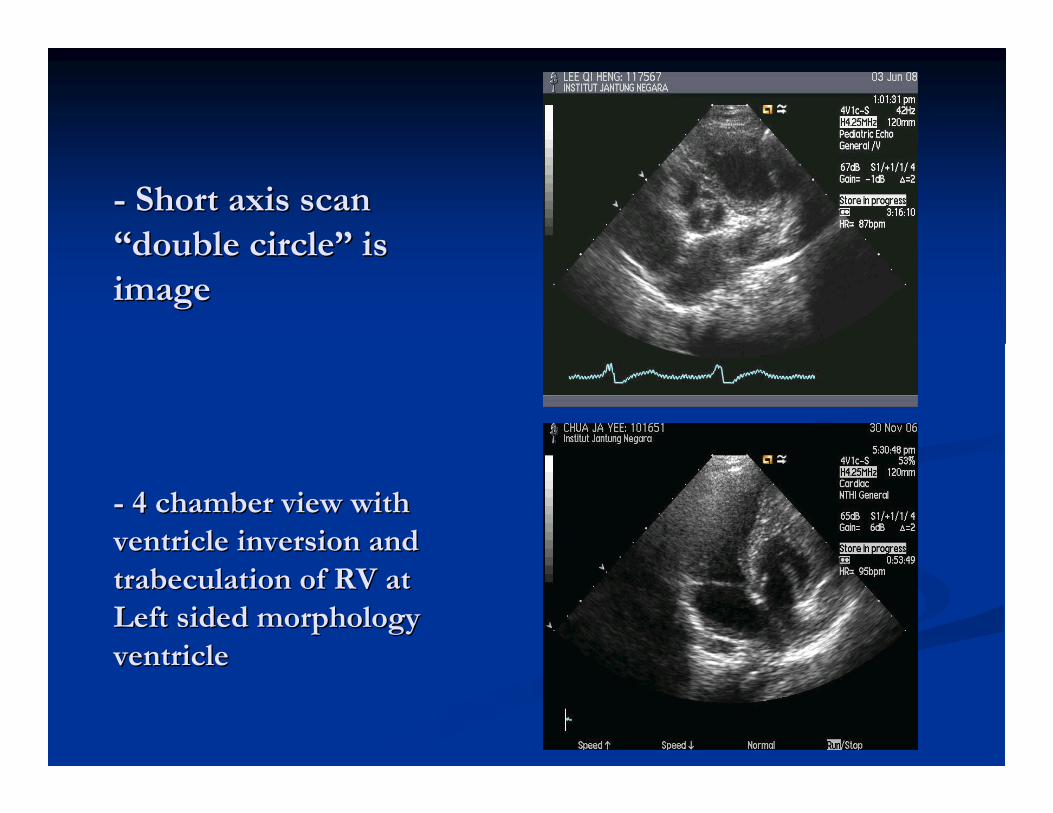
-- Short axis scan Short axis scan
““double circledouble circle”” is is
imageimage
-- 4 chamber view with 4 chamber view with
ventricle inversion and ventricle inversion and
trabeculationtrabeculation of RV at of RV at
Left sided morphology Left sided morphology
ventricleventricle
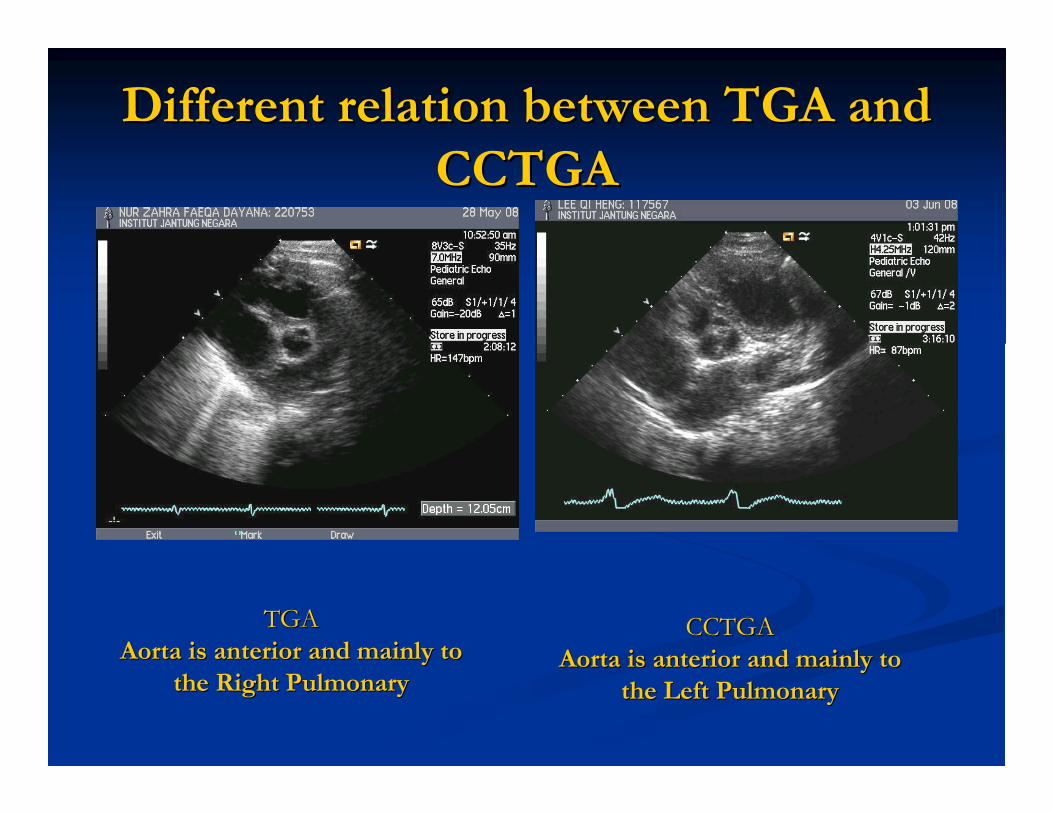
Different relation between TGA and Different relation between TGA and
CCTGACCTGA
TGATGA
Aorta is anterior and mainly to Aorta is anterior and mainly to
the Right Pulmonarythe Right Pulmonary
CCTGACCTGA
Aorta is anterior and mainly to Aorta is anterior and mainly to
the Left Pulmonarythe Left Pulmonary
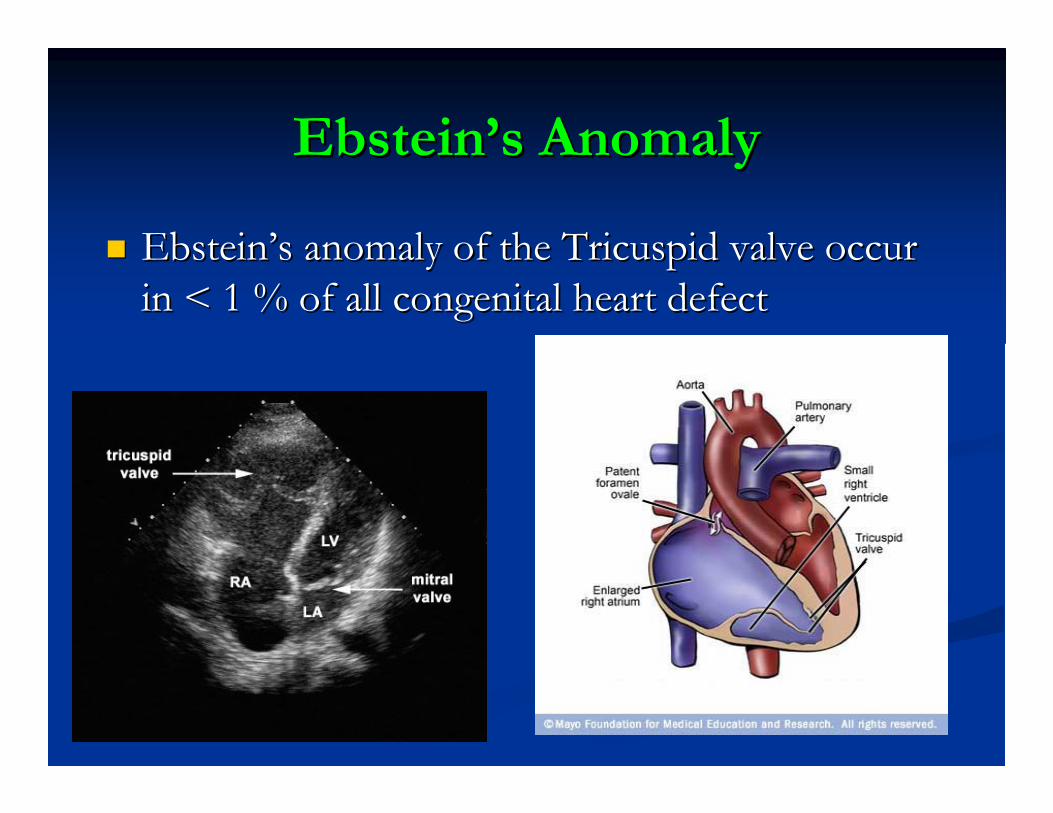
EbsteinEbstein’’ss AnomalyAnomaly
�� EbsteinEbstein’’ss anomaly of the Tricuspid valve occur anomaly of the Tricuspid valve occur
in < 1 % of all congenital heart defectin < 1 % of all congenital heart defect
PathologyPathology
�� Downward displacement of septal and posterior leaflet of tricuspDownward displacement of septal and posterior leaflet of tricuspid valve into id valve into RV cavity ( RV cavity ( atrializedatrialized RV ) and the functional RV cavity is small RV ) and the functional RV cavity is small
�� Usually the septal leaflet is plastered toward septum and the anUsually the septal leaflet is plastered toward septum and the anterior leaflet terior leaflet elongated (redundant ,resembling like sail).elongated (redundant ,resembling like sail).
�� May be associated with tricuspid regurgitation.May be associated with tricuspid regurgitation.
�� ASD/PFO usually present and occasionally other defect such as PSASD/PFO usually present and occasionally other defect such as PS, VSD , VSD might occur.might occur.
�� Severe form of Severe form of EbsteinEbstein usually will present at early age and requires early usually will present at early age and requires early interventionintervention
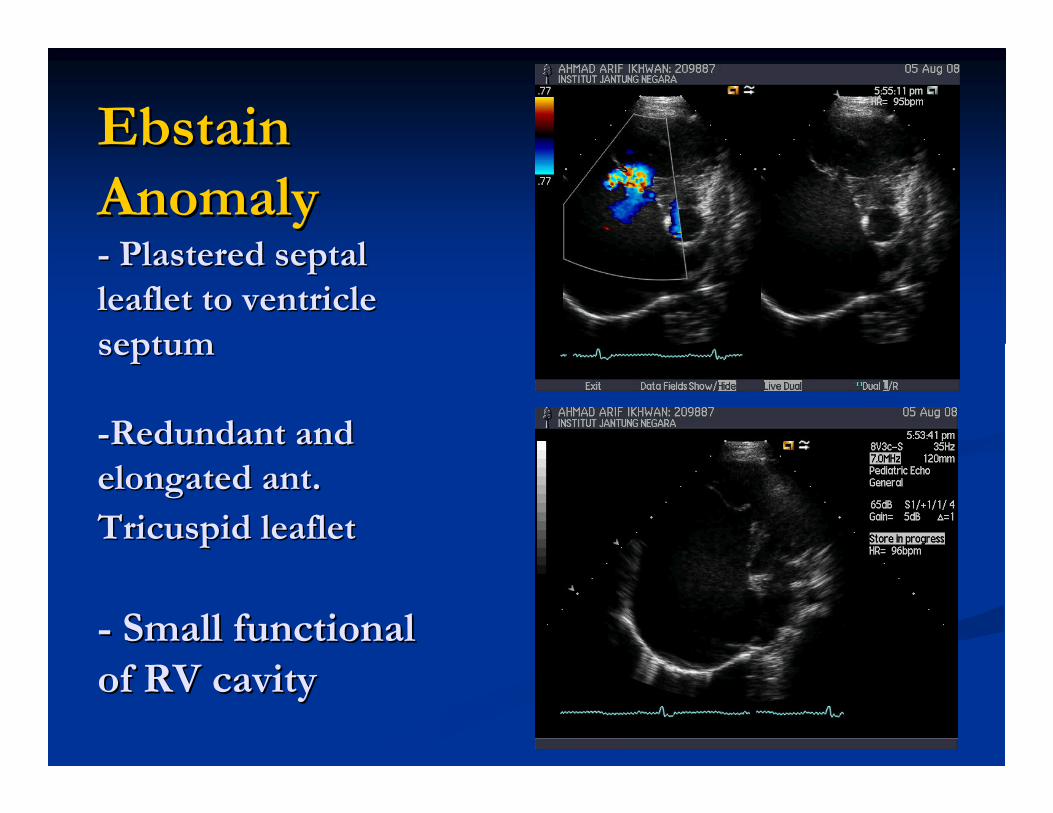
Ebstain Ebstain
AnomalyAnomaly-- Plastered septal Plastered septal
leaflet to ventricle leaflet to ventricle
septumseptum
--Redundant and Redundant and
elongated ant. elongated ant.
Tricuspid leafletTricuspid leaflet
-- Small functional Small functional
of RV cavityof RV cavity
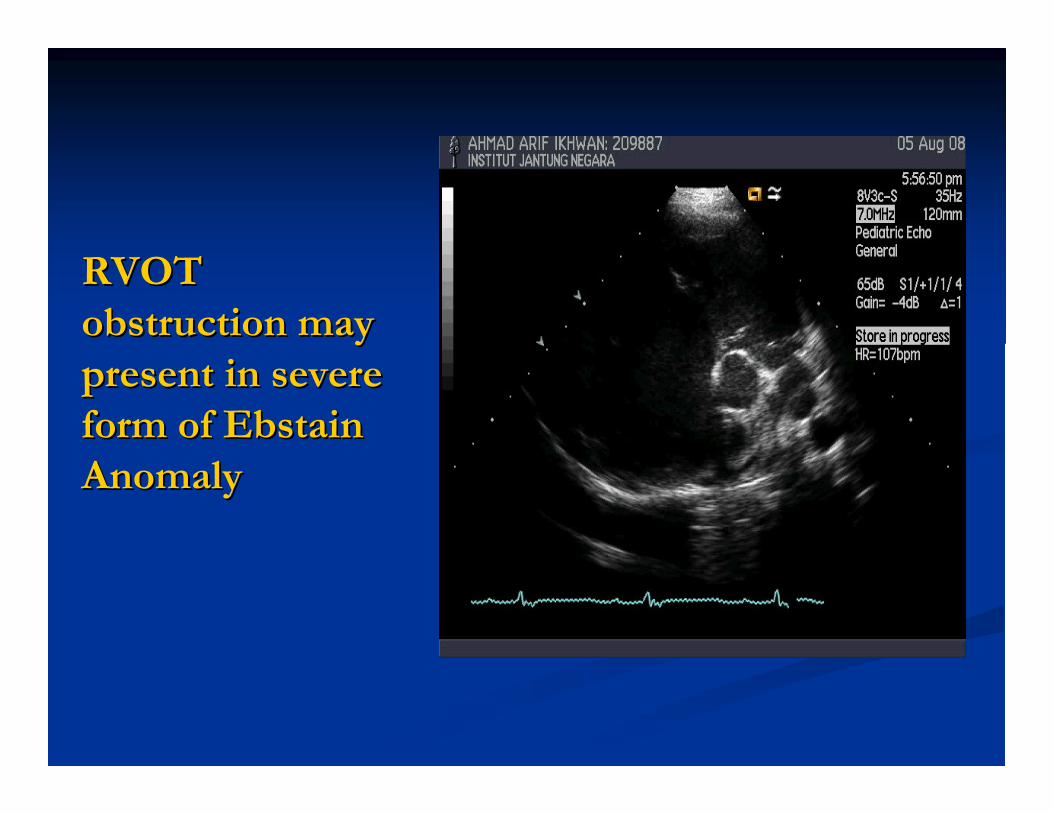
RVOT RVOT
obstruction may obstruction may
present in severe present in severe
form of Ebstain form of Ebstain
AnomalyAnomaly
Coarctation AortaCoarctation Aorta
�� Coarctation of Aorta occur in 8 % to 10 % of all Coarctation of Aorta occur in 8 % to 10 % of all
cases of congenital heart defect. It is more cases of congenital heart defect. It is more
common in males than female ratio 2 : 1 .common in males than female ratio 2 : 1 .
PATHOLOGYPATHOLOGY
�� Coarctation is a restrictive flow through the aortic arch . Coarctation is a restrictive flow through the aortic arch .
�� Type of coarctation varies like long tubular hypoplastic Type of coarctation varies like long tubular hypoplastic
arch, discrete aortic arch etc.arch, discrete aortic arch etc.
�� Coarctation is almost always in a Coarctation is almost always in a juxtaductaljuxtaductal position.position.
�� As many as 85 % of patient with COA have a bicuspid As many as 85 % of patient with COA have a bicuspid
aortic valve.aortic valve.
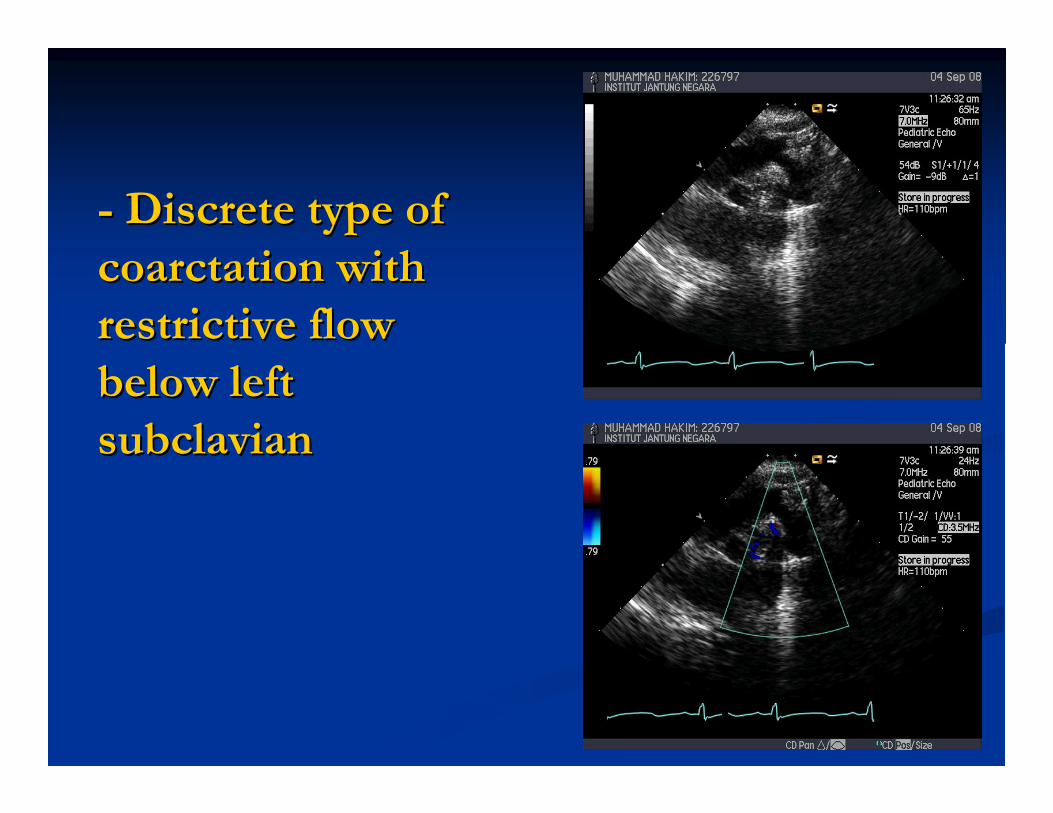
-- Discrete type of Discrete type of
coarctation with coarctation with
restrictive flow restrictive flow
below left below left
subclaviansubclavian
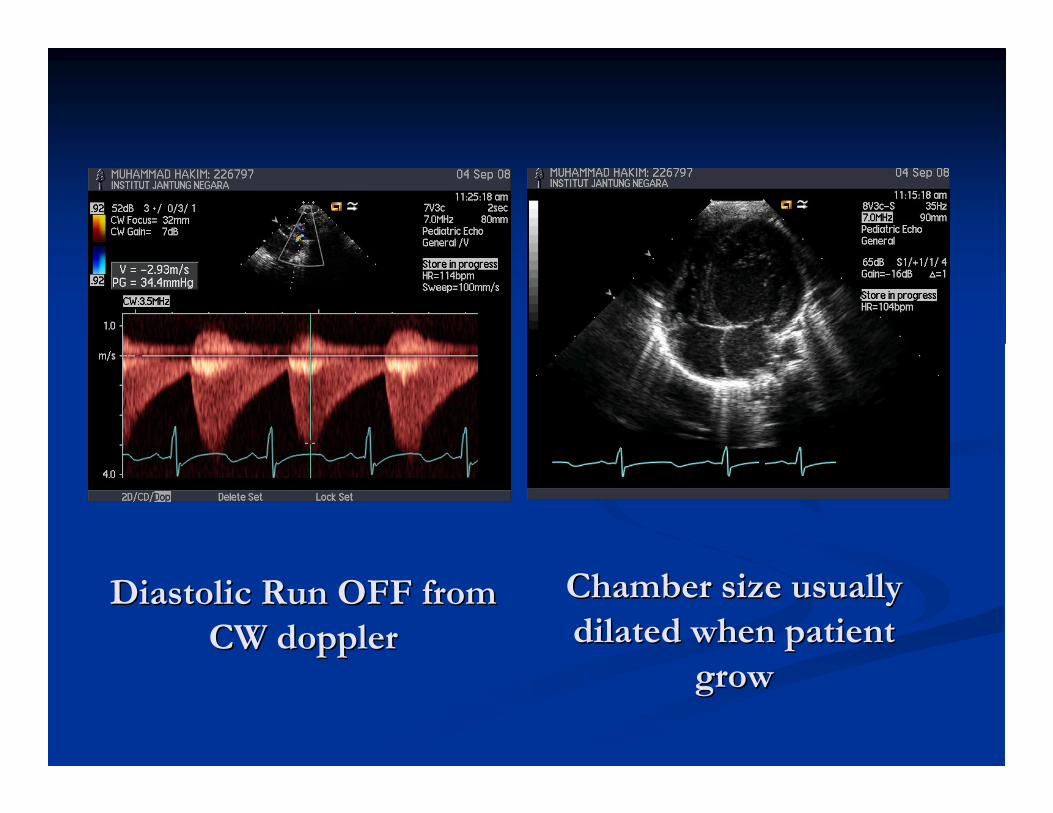
Diastolic Run OFF from Diastolic Run OFF from
CW CW dopplerdoppler
Chamber size usually Chamber size usually
dilated when patient dilated when patient
grow grow
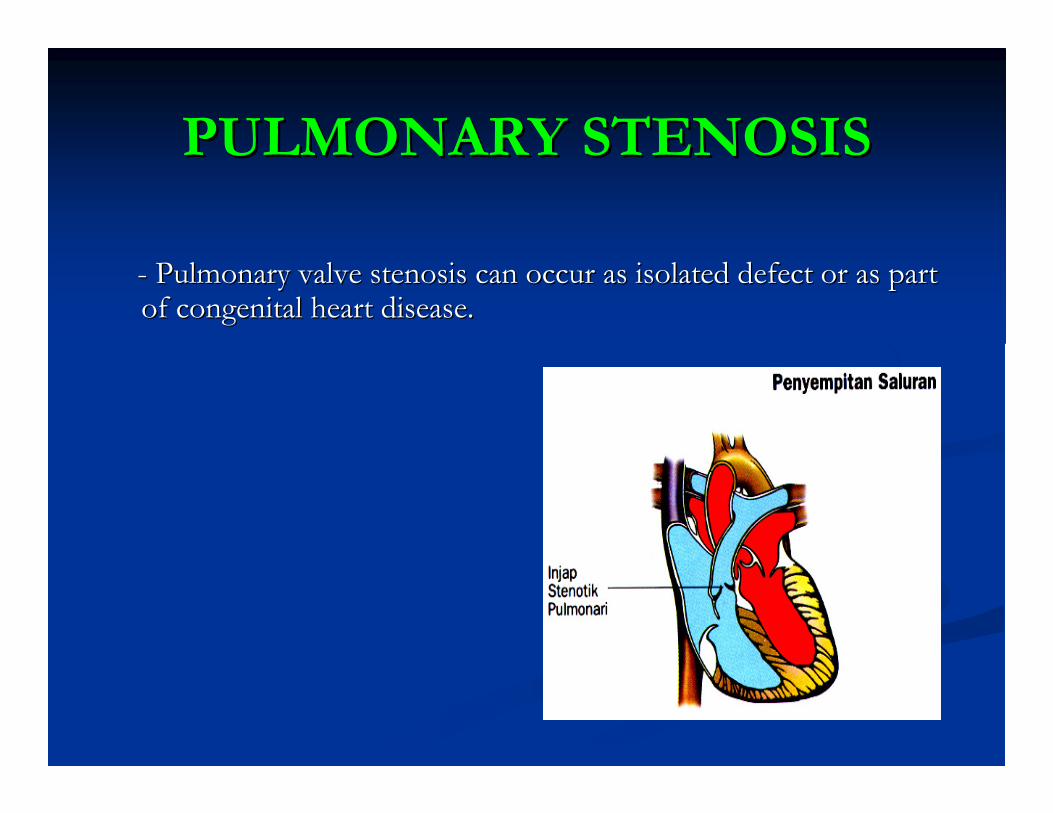
PULMONARY STENOSISPULMONARY STENOSIS
-- Pulmonary valve stenosis can occur as isolated defect or as parPulmonary valve stenosis can occur as isolated defect or as part t of congenital heart disease.of congenital heart disease.
�� Several type of Pulmonary Stenosis includeSeveral type of Pulmonary Stenosis include
1. Infundibular stenosis.1. Infundibular stenosis.
2. Valvular pulmonary stenosis2. Valvular pulmonary stenosis
3. Subvalvular pulmonary stenosis3. Subvalvular pulmonary stenosis
4. Supravalvular pulmonary stenosis4. Supravalvular pulmonary stenosis..
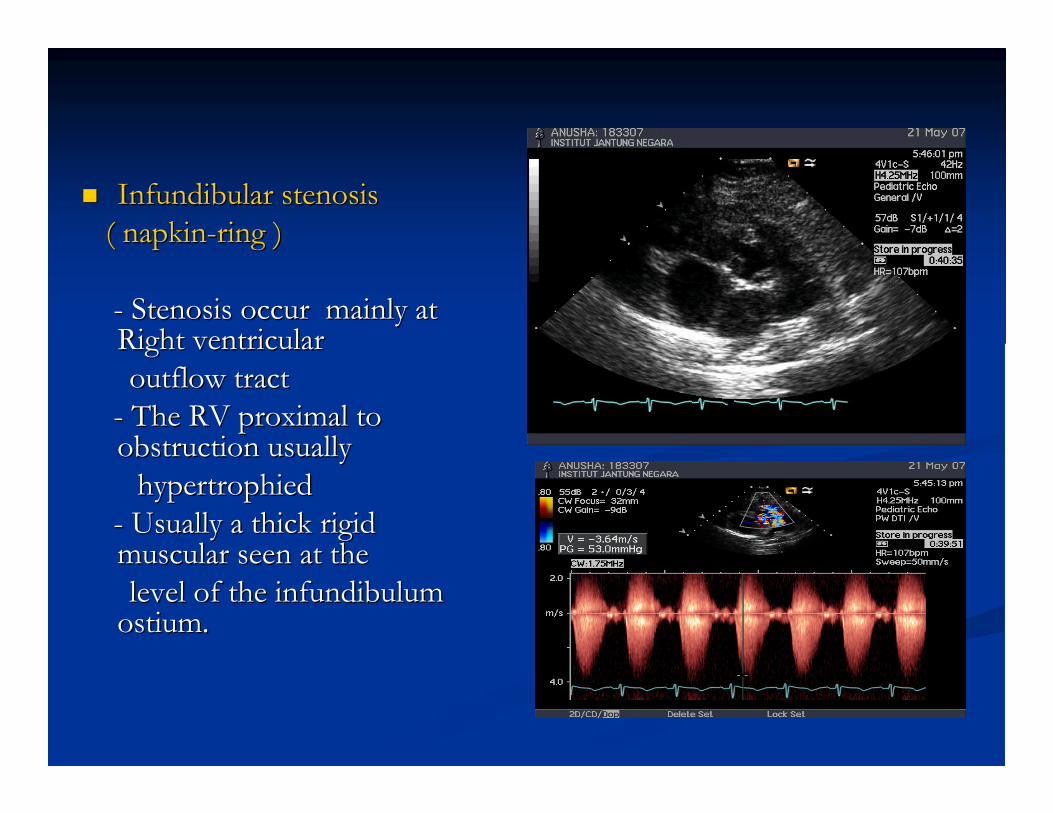
�� Infundibular stenosis Infundibular stenosis
( napkin( napkin--ring )ring )
-- Stenosis occur mainly at Stenosis occur mainly at Right ventricular Right ventricular
outflow tract outflow tract
-- The RV proximal to The RV proximal to obstruction usually obstruction usually
hypertrophiedhypertrophied
-- Usually a thick rigid Usually a thick rigid muscular seen at the muscular seen at the
level of the level of the infundibuluminfundibulumostiumostium..
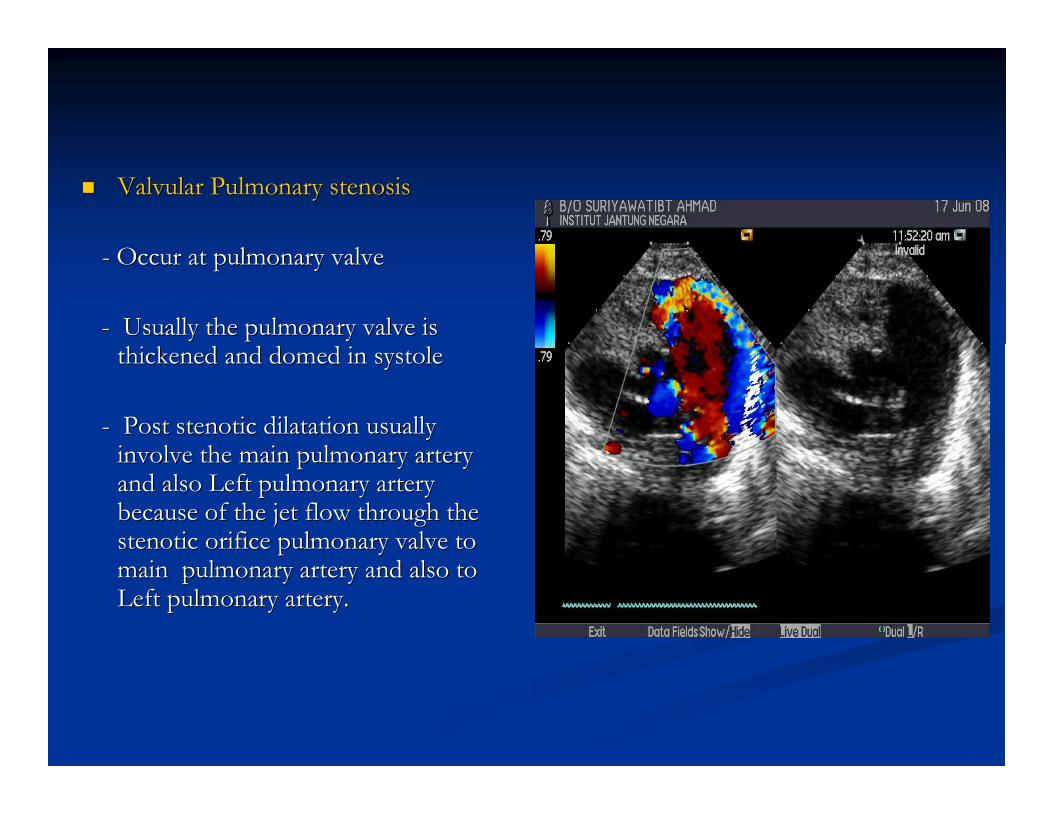
�� Valvular Pulmonary stenosisValvular Pulmonary stenosis
-- Occur at pulmonary valveOccur at pulmonary valve
-- Usually the pulmonary valve is Usually the pulmonary valve is thickened and domed in systolethickened and domed in systole
-- Post stenotic dilatation usually Post stenotic dilatation usually involve the main pulmonary artery involve the main pulmonary artery and also Left pulmonary artery and also Left pulmonary artery because of the jet flow through the because of the jet flow through the stenotic orifice pulmonary valve to stenotic orifice pulmonary valve to main pulmonary artery and also to main pulmonary artery and also to Left pulmonary artery.Left pulmonary artery.
�� Subvalvular Pulmonary stenosisSubvalvular Pulmonary stenosis
-- Subvalvular pulmonary stenosis occur between Subvalvular pulmonary stenosis occur between
the RV and pulmonary the RV and pulmonary conusconus
-- Usually the stenosis at the level just below the Usually the stenosis at the level just below the
pulmonary valve (proximal) and between the pulmonary valve (proximal) and between the
infundibuluminfundibulum.( discrete stenosis of the .( discrete stenosis of the
infundibuluminfundibulum ostiumostium).).
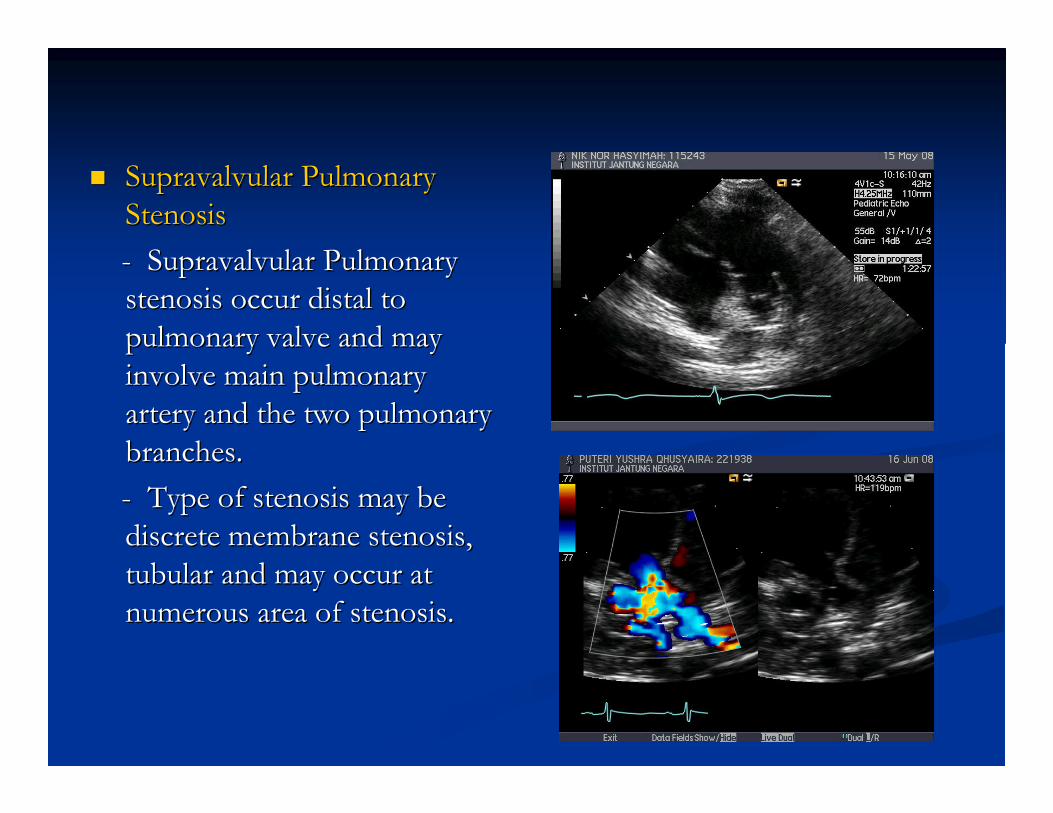
�� Supravalvular Pulmonary Supravalvular Pulmonary
StenosisStenosis
-- Supravalvular Pulmonary Supravalvular Pulmonary
stenosis occur distal to stenosis occur distal to
pulmonary valve and may pulmonary valve and may
involve main pulmonary involve main pulmonary
artery and the two pulmonary artery and the two pulmonary
branches.branches.
-- Type of stenosis may be Type of stenosis may be
discrete membrane stenosis, discrete membrane stenosis,
tubular and may occur at tubular and may occur at
numerous area of stenosis.numerous area of stenosis.
�� Suggestion grading of Pulmonary Stenosis Suggestion grading of Pulmonary Stenosis
according to the peak gradient.according to the peak gradient.
-- Peak gradient of Pulmonary stenosisPeak gradient of Pulmonary stenosis
less then I/3 Systemic blood pressure is less then I/3 Systemic blood pressure is
Mild PS.Mild PS.
-- Peak gradient 2/3 of systemic blood Peak gradient 2/3 of systemic blood
pressure is moderate PS.pressure is moderate PS.
-- Peak gradient of more than 2/3 systemic Peak gradient of more than 2/3 systemic
pressure is equal to severe PS.pressure is equal to severe PS.
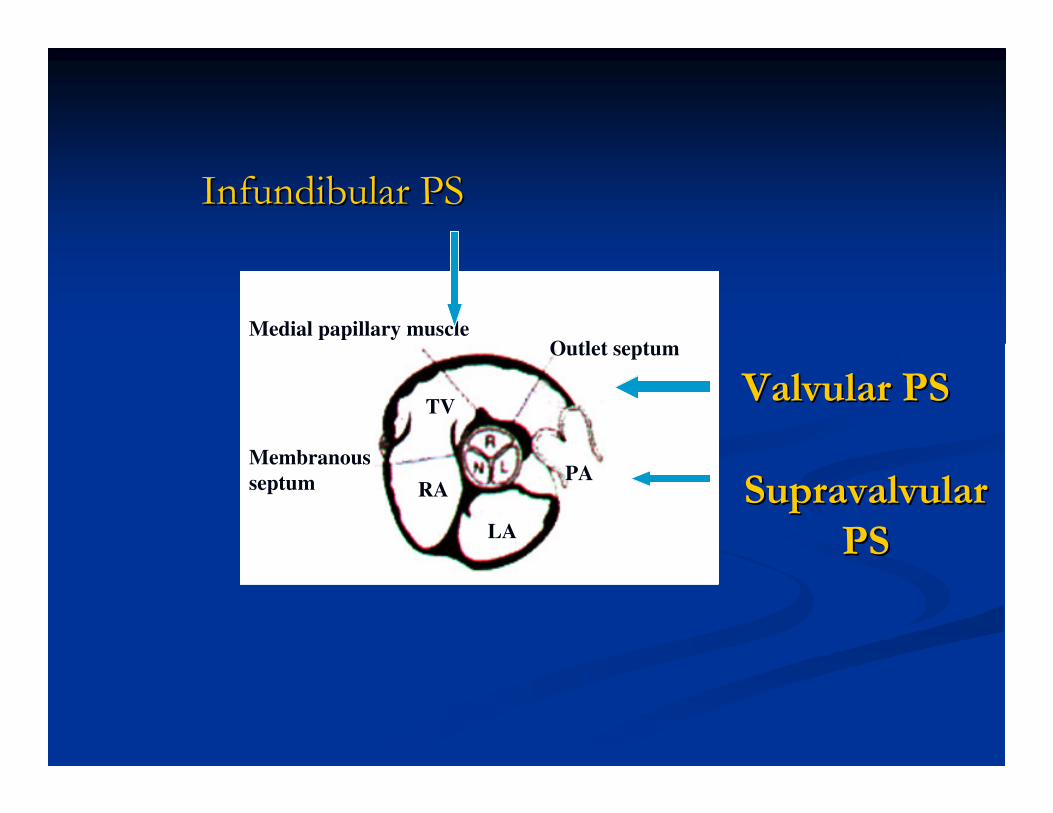
Valvular PSValvular PS
Infundibular PSInfundibular PS
RAPA
TV
LA
Membranous
septum
Medial papillary muscleOutlet septum
Supravalvular Supravalvular
PSPS
Have a nice dayHave a nice day

THANK YOUTHANK YOU
HANIF OSMAN , HANIF OSMAN , RDCSRDCS