Embed Size (px)
Citation preview

ORIGINAL RESEARCH
Micronized Purified Flavonoid Fractionin Hemorrhoid Disease: A Systematic Reviewand Meta-Analysis
Parvez Sheikh . Varut Lohsiriwat . Yury Shelygin
Received: March 3, 2020 / Published online: May 12, 2020� The Author(s) 2020
ABSTRACT
Introduction: Hemorrhoidal disease (HD) is acommon and recurrent problem for manyadults worldwide. Venoactive drugs, such asmicronized purified flavonoid fraction (MPFF;Daflon�), have been used to treat HD and theirclinical benefits have been demonstrated inprevious meta-analyses of clinical trials. Theaim of this study was to evaluate the efficacy ofMPFF across the broader spectrum of signs andsymptoms following treatment of patients withHD.Methods: We performed a systematic review ofthe literature to identify randomized clinicaltrials in which MPFF treatment was compared
to placebo or no treatment for acute HD or forrelief of symptoms after patients had undergonemedical management or a surgical procedure toremove hemorrhoids. The main endpointsinvestigated were bleeding, pain, pruritus, dis-charge or leakage, and overall improvement.There was no limit on treatment duration.Results: From 351 unique records retrieved, 11studies reported in 13 articles were included. Onthe basis of findings from qualitative analysis,MPFF was reported in most studies to be bene-ficial in treating bleeding, pain, pruritus, analdischarge/leakage, and tenesmus, and in overallimprovement. Quantitative meta-analysis offour studies indicated that MPFF treatmentprovided significant benefits for bleeding (oddsratio [OR] 0.082, 95% confidence interval [CI]0.027–0.250; P\ 0.001), discharge/leakage (OR0.12, 95% CI 0.04–0.42; P\0.001), and overallimprovement according to patients (OR 5.25,95% CI 2.58–10.68; P\ 0.001) and investigators(OR 5.51, 95% CI 2.76–11.0; P\0.001). MPFFalso tended to decrease pain (OR 0.11, 95% CI0.01–1.11; P = 0.06).Conclusion: Taken together, these results sug-gest that MPFF treatment can improve the mostimportant signs and symptoms of HD.
Keywords: Hemorrhoidal disease; Hemor-rhoidectomy; Hemorrhoids; Micronized puri-fied flavonoid fraction; MPFF; Venoactive drugs
Digital Features This article is published with digitalfeatures, including a video abstract, slide deck andsummary slide, to facilitate understanding of the article.To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12145386.
P. SheikhDepartment of Colorectal Surgery, Saifee Hospital,Mumbai, India
V. Lohsiriwat (&)Division of Colon and Rectal Surgery, Departmentof Surgery, Faculty of Medicine Siriraj Hospital,Mahidol University, Bangkok, Thailande-mail: [email protected]
Y. ShelyginState Scientific Center of Coloproctology, Ministryof Health of Russian Federation, Moscow, Russia
Adv Ther (2020) 37:2792–2812
https://doi.org/10.1007/s12325-020-01353-7

Key Summary Points
Why carry out this study?
This systematic review and meta-analysissought to evaluate the efficacy ofmicronized purified flavonoid fraction(MPFF) in comparison with placebo or notreatment in patients with hemorrhoidaldisease (HD).
A wide range of symptoms associatedwith acute HD or occurring after a medicalmanagement or surgical procedure for HDwere assessed across randomizedcontrolled studies using qualitative andquantitative analyses.
What was learned from this study?
Our results suggest that MPFF treatmentcan improve the most important signsand symptoms of HD including bleeding,pain, pruritus, tenesmus, and analdischarge/leakage.
INTRODUCTION
Hemorrhoidal disease (HD) is a common medi-cal problem among adults worldwide [1–3]. Inaddition to body mass index, other proposedrisk factors include conditions that elevateintra-abdominal pressure such as pregnancyand straining [4].
HD occurs when hemorrhoids becomeinflamed and swollen with venous blood.External HD involves swelling of the externalperianal vasculature and the tissues lining theanal canal below the dentate line; external HDis thus associated with symptoms of pain andpruritus, and less frequently bleeding orthrombosis. Internal HD occurs when theinternal hemorrhoids swell and slide toward theanus, causing additional venous dilatation [4].Although they are often asymptomatic andpainless because the tissues are not innervated
with somatic nerves, they may be associatedwith bleeding during defecation.
Internal HD is classified according to degreeof prolapse (grade I, no prolapse; grade IV, per-manent prolapse below the dentate line). Pro-lapsed internal hemorrhoids may be removedthrough various outpatient procedures or sur-gical excision [4, 5]. Complications of surgicalprocedures can include pain and profusebleeding; rare but life-threatening complica-tions include abscess formation, sepsis, andfecal incontinence [6].
HD may also be treated conservatively. Thisapproach includes diet and lifestyle modifica-tion to increase fiber and fluid intake, increasephysical activity, avoid constipation, and avoidstraining during defecation. Topical treatmentswith creams containing anesthetics, corticos-teroids, and anti-inflammatory drugs may pro-vide some symptom relief for HD. Venoactivedrugs or phlebotonics, which are available inEurope and Asia for the treatment of chronicvenous disease (CVD; e.g., varicose veins), havealso been used to treat HD [7]. Of these, flavo-noids are the most common agent used.Micronized purified flavonoid fraction (MPFF;Daflon� [Servier, France]) is a well-known andwell-studied venoactive drug and is frequentlyprescribed for CVD symptom relief, especially inFrance [8]. In CVD patients, MPFF has beenshown to improve venous tone and to reducecapillary permeability, vascular endothelialactivation, and inflammation [9, 10].
With respect to MPFF treatment in HD, pre-vious non-systematic reviews have found evi-dence for the efficacy of MPFF not only inreducing pain, bleeding, anal discharge, andprolapse in acute HD but also in preventingrelapse and reducing the duration and severityof acute attacks in chronic HD [7, 11, 12]. A2006 meta-analysis of 14 studies investigatingflavonoid treatment (MPFF, diosmin, or ruto-sides) for hemorrhoids reported that flavonoidsreduced the risk of not improving globally by58%, with apparent reductions in the risks ofbleeding, pain, itching, and recurrences [8]. Amore recent Cochrane meta-analysis of hemor-rhoid treatment with phlebotonics, which cov-ered a wide variety of drugs including MPFF,found that phlebotonics provided statistically
Adv Ther (2020) 37:2792–2812 2793

significant benefits in bleeding and overallsymptom improvement in acute HD and inbleeding after hemorrhoidectomy [13].
To evaluate the efficacy of MPFF across thebroader spectrum of signs and symptoms fol-lowing treatment of patients with HD, we con-ducted a systematic review to identify studies tobe included in a meta-analysis of the magnitudeof MPFF treatment effects compared to eitherplacebo or no treatment for the symptoms andsigns associated with acute HD or after a medi-cal management or surgical procedure.
METHODS
Criteria for Considering Studies in thisReview
Study DesignWe included all published parallel-group ran-domized controlled trials (RCTs) investigatingthe effect of MPFF in relieving the signs andsymptoms in patients with acute HD (i.e.,within 7 days of the onset of symptoms—usu-ally either bleeding or pain) or after medical orsurgical procedure to remove hemorrhoids.
The design of the included studies should be:
• For acute HD: double-blind RCTs comparingtreatment with MPFF versus placebo
• After a medical or surgical procedure for HD:open-label, single-blind or double-blindRCTs comparing treatment with MPFF versusplacebo or versus no treatment wereaccepted
Quasi-randomized studies were excluded.There was no limit on treatment duration.
Study ParticipantsEligible participants were patients with HD ofall ages and both sexes, including pregnant orpostpartum women, and patients after a proce-dure for HD.
Study EndpointsThe studies were included if at least one of thefollowing endpoints was reported: bleeding,pain, pruritus, analgesic consumption,
discharge or leakage, overall improvementaccording to patient or investigator, hospital-ization duration after a procedure, anal dis-comfort, edema, tenesmus, and recurrence ofHD crisis.
Literature Search Strategy
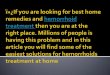
We systematically reviewed the literature toidentify articles investigating the effects of oralMPFF treatment for HD. We conducted thesearch in three different online databases(PubMed, Embase, and the Cochrane CentralRegister of Controlled Trials) on June 6, 2018.Search terms included hemorrhoid, flavonoid,hesperidin, diosmin, micronized purified flavo-noid fraction, MPFF, and Daflon, as well assynonyms and other brand names for MPFF.There was no restriction on language and pub-lication date. In addition, PRISMA guidelineswere used to report this review and meta-anal-ysis (Fig. 1) [14].
After using Citavi� (Swiss Academy Software,version 6.2) to remove duplicates, two reviewersindependently screened titles and abstracts ofthe retrieved records to identify relevant clinicaltrials and reviews for further analysis, and toexclude clearly noncompliant and ineligiblestudies. Following the selection of records, fulltexts were obtained for all selected articles andreviews. To identify additional potentially rele-vant trials, a manual search was then conductedon the reference list of the selected reviews. Amanual search was also performed in a Servierinternal database (Pharmanet). The tworeviewers independently assessed the full text ofthe selected articles to determine study eligi-bility using the predefined inclusion andexclusion criteria. In some cases, authors werecontacted for clarification. Conferenceabstracts, letters, notes, and editorials wereexcluded. Unpublished studies were not con-sidered. At all stages of the screening process,disagreements between reviewers were resolvedby discussion. A last manual search was thenconducted on the reference list of the includedarticles.
2794 Adv Ther (2020) 37:2792–2812

Data Extraction and Analysis
Data extraction was performed independentlyby the two reviewers using specifically designedExcel files. Collected data included studymethodology and patient baseline informationas well as MPFF efficacy and safety results. Sta-tistical analyses were carried out using SAS� forWindows (SAS Institute Inc., version 9.2).
Main efficacy outcomes were bleeding, pain,and pruritus. Other outcomes analyzed
included analgesic consumption, discharge orleakage, overall improvement (according topatient or investigator), anal discomfort,edema, tenesmus, recurrence of acute HD crises,and length of hospital stay after a procedure.For pain, pruritus, anal discomfort, and tenes-mus, the patient’s reported outcome was con-sidered first if available, whereas for bleeding,discharge/leakage, and edema, investigator’sreported outcome was considered first if avail-able. These endpoints were analyzed at day 4 (or
Fig. 1 PRISMA flow diagram. HD hemorrhoidal disease, MPFF micronized purified flavonoid fraction RCT randomizedcontrolled trial
Adv Ther (2020) 37:2792–2812 2795

at day 3 or 5 if not available) and at day 7 (orday 4–10 if not available).
When efficacy endpoints were reported by asingle study, only a descriptive analysis wasperformed (i.e., qualitative analysis). Mean dif-ferences or standard mean differences for con-tinuous endpoints and odds ratios (OR) forbinary endpoints were calculated with theirassociated 95% confidence intervals. Whenefficacy endpoints were reported by more thanone study, a meta-analysis on aggregated datawas performed (i.e., quantitative analysis).Fixed-effect (Mantel–Haenszel) and random-ef-fects (DerSimonian–Laird) methods were usedfor binary endpoints [15, 16], whereas inverse-variance fixed-effect and random-effects meth-ods were used for continuous endpoints.
Heterogeneity between studies was measuredwith the Cochran Q statistic [17]. A non-signif-icant P value for the Q indicator indicated thatthe treatment effect among the studies washomogeneous. In addition, the degree ofheterogeneity between studies was measuredwith the I2 indicator [18]. If I2 was greater than50%, a model with random effects was usedinstead of a model with fixed effects. In onestudy (Jiang and Cao) [19], the results for binaryendpoints excluded the modality ‘‘mild’’, whichrequired an additional sensitivity analysis.
Assessment of Study Quality and Riskof Bias
The two reviewers independently assessed thequality of the selected studies using theCochrane risk of bias tool [20]. For each study,the reviewers evaluated and graded the risk ofbias as low, high, or unclear for each of thefollowing items: random sequence generation(selection bias), allocation concealment (selec-tion bias), blinding of participants and person-nel (performance bias) for symptoms and signsseparately, blinding of outcome assessment(detection bias), incomplete outcome data (at-trition bias), and selective reporting (reportingbias).
This article is based on previously conductedstudies and does not contain any studies with
human participants or animals performed byany of the authors.
RESULTS
Results of the Literature Search
A total of 493 records were identified throughPubMed, Embase, and Cochrane Central data-bases (Fig. 1). An additional four records wereidentified through manual search. Afterremoval of duplicates, 351 unique records werescreened using titles and abstracts. Of them, 49potentially relevant records were retrieved forfull text assessment. Finally, a total of 11 studiesreported in 13 articles [19, 21–32] were includedin the systematic review (qualitative analysis).As a result of substantial heterogeneity in theendpoints reported in the studies, only fourstudies could be included in the meta-analysis(quantitative analysis) [19, 21, 22, 30].
Risk of Bias in Studies Included
For 7 out of 11 studies, the risk of bias wasunclear or high in at least two aspects of thestudy designs (Table 1). The study by Lee et al.appeared to be at the highest risk of bias [29],with unclear risk in five study aspects, althoughthree studies were deemed to be at high risk intwo aspects [21, 28, 32]. In four studies, the riskof bias was low in all or most aspects of thestudy designs [19, 22–26].
Study Characteristics
All the studies included in the systematic reviewwere conducted in Europe or Asia and publishedbetween 1992 and 2010 (Table 2). Participantswere adult patients of both sexes, and the meanage of the study populations ranged between 33and 57 years. Patients with HD of all grades(I–IV) were included. Six studies investigatedthe effects of MPFF treatment vs placebo foracute HD and five investigated treatment fol-lowing a medical management or surgical pro-cedure. Treatment with MPFF was between 1000and 3000 mg/day for between 5 and 90 days.
2796 Adv Ther (2020) 37:2792–2812

Table 1 Risk of bias summary for the studies included in the systematic review
Ran
dom
sequ
ence
gen
erat
ion
(sel
ectio
n bi
as)
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
Blin
ding
of p
artic
ipan
ts a
nd p
erso
nnel
(per
form
ance
bia
s) (p
ain,
pru
ritus
,
disc
omfo
rt, te
nesm
us a
nd o
vera
ll im
prov
emen
t acc
ordi
ng to
pat
ient
)B
lindi
ng o
f par
ticip
ants
and
per
sonn
el (p
erfo
rman
ce b
ias)
(ble
edin
g,
disc
harg
e, e
dem
a an
d ov
eral
lim
prov
emen
t acc
ordi
ng to
inve
stig
ator
)
Blin
ding
of o
utco
me
asse
ssm
ent (
dete
ctio
n bi
as)
Inco
mpl
ete
outc
ome
data
(attr
ition
bia
s)
Sele
ctiv
e re
porti
ng (r
epor
ting
bias
)
Godeberge 1992 (25, 26)
Cospite 1994 (22, 23)
Vajrabukka 1994 (32)
Ho 1995 (27) NA
Lee 1998 (29)
Misra 2000 (30) NA
Colak 2003 (21) NA
La Torre 2004 (28)
Dimitroulopoulos 2005 (24) NA
Jiang 2006 (19)
Panpimanmas 2010 (31)
NA, not applicable
Adv Ther (2020) 37:2792–2812 2797

Table2
Characteristics
ofthestudiesincluded
inthesystem
aticreview
Stud
y,year,coun
try/
intervention
s
Stud
ydesign/
Nparticipants
Participants:
inclusionandexclusioncriteria
Outcomes
analyzed
(MPFF
vscontrol)
Param
eter
Day
MPFF
Con
trol
Significant
(Y/N
)
Investigations
ofdirect
effectsof
MPF
Fon
acuteHD
Cospite
(1994)
[22,
23]
Italy
MPF
For
placebo
3000
mg/dayfor3days,
2000
mg/dayfor4days
Double-blind
RCT
N=100
MPF
F:n=50
Placebo:
n=50
Meanage*
43–4
5years
53%
wom
en
Inclusioncriteria:adultoutpatientsor
inpatientsof
anysexandage,withknow
nHD,diagnosed
byproctoscopy,sufferingfrom
anun
complicated
acutehemorrhoidalcrisiswithout
any
previous
treatm
entforamaxim
umof
3days.T
hepatientshadto
suffer
from
symptom
ssuch
asbleeding,analdiscom
fort,p
ainandpruritus,and
objectiveproctoscopicsigns
Exclusion
criteria:patientsrequiringasurgicalprocedure,sufferingfrom
analfistulaor
rectal
prolapse
System
icanalgesic
consum
ption
70.2±
0.1
1.6±
0.2
Y
Pain
a7
42/50
(84%
)
8/50 (1
6%)
Y
Analdiscom
fort
719/49
(39%
)
3/49
(6%)
Y
Bleeding
719/20
(95%
)
9/18 (5
0%)
Y
Discharge/leakage
721/26
(81%
)
7/23 (3
0%)
Y
Overallim
provem
ent
748/49
(74.1%
)
34/45
(75.6%
)
Y
Overallsatisfaction
(patient
‘‘satisfied’’o
r
‘‘verysatisfied’’)b
742/50
(84%
)
21/50
(42%
)
Y
Overallim
provem
ent
(investigator‘‘very
good’’,‘‘good’’,‘‘useful’’)
c
745/50
(90%
)
29/50
(58%
)
Y
Godeberge
(1994)
[25,
26]
France
MPF
For
placebo
1000
mg/dayfor60
days
Double-blind
RCT
N=120
MPF
F:n=60
Placebo:
n=60
Meanage*
46–4
8years
80%
wom
en
Inclusioncriteria:am
bulatory
patients,agedover
18years,withsymptom
aticHD
(1st–3
rd
degree);withan
acuteepisodein
preceding2months
Exclusion
criteria:com
plicated
HD
asaresultof
previous
surgery,associated
analfissure,orthose
requiringim
mediate
surgery;bleeding
disorder;treatm
entwithavenotropicagentin
the
previous
2months;anocutaneous
parasiticinfestation,
orarectosigmoidaldisorder
Pain
d60
98%
47%
Y
Pruritus
6086%
58%
Y
Tenesmus
6098%
50%
Y
Bleeding
6091%
59%
Y
Discharge/leakage
6097%
54%
Y
Edema
6098%
47%
Y
Erythem
a60
95%
48%
Y
Recurrenceof
acute
episodeon
treatm
ent
6040%
76%
Y
Patientsatisfaction
6090%
40%
Y
2798 Adv Ther (2020) 37:2792–2812

Table2
continued
Stud
y,year,coun
try/
intervention
s
Stud
ydesign/
Nparticipants
Participants:
inclusionandexclusioncriteria
Outcomes
analyzed
(MPFF
vscontrol)
Param
eter
Day
MPFF
Con
trol
Significant
(Y/N
)
Jiang(2006)
[19]
China
MPF
For
placebo
3000
mg/dayfor4days,
then
1500
mg/dayfor3days
Double-blind
RCT
N=90
MPF
F:n=49
Placebo:
n=41
Meanage
43.2
years
46%
wom
en
Inclusioncriteria:maleor
femalepatients,aged[
18years,followed
upas
out-or
inpatients,
presenting
forthefirsttimewithan
acutehemorrhoidalepisode(diagnosisconfi
rmed
by
clinicalandendoscopicexam
ination)
oflessthan
48h,
withsymptom
ssuch
aspain,itching
andedem
a,and/or
signs(bleeding,mucus
leakage,andprolapse),having
notreceived
other
priortherapies(any
phlebotropicmedication,
anticoagulantandantiplatelet
agents,analgesic
oranti-in
flammatorydrugs)
Exclusion
criteria:presence
ofsevere
hemorrhoidalmanifestations
requiringsurgery,analfissure,
perm
anentprolapsedhemorrhoids,and
parasiticinfection
Bleedinge(%
grades2or
3)
[meanscore]
42/49
(4%)
[1.3]
2/41 (4
.9%)
[1.5]
Y
71/49
(2%)
[1.2]
3/41 (7
.3%)
[1.4]
Y
Pain
(%grades
2or
3)
[meanscore]
49/49 (1
8.3%
)
[2.0]
8/41 (1
9.5%
)
[2.1]
N
73/49 (6
.1%)
[1.4]
6/41 (1
4.6%
)
[1.8]
Y
Itching(%
grades
2or
3)
[meanscore]
41/49
(2%)
[1.2]
2/41 (4
.9%)
[1.3]
N
70/49
(0%)
[1.1]
2/41 (4
.9%)
[1.3]
Y
Leakage
(%grades
2or
3)
[meanscore]
41/49
(2%)
[1.2]
1/41 (2
.4%)
[1.2]
N
70/49
(0%)
[1.1]
1/41 (2
.4%)
[1.2]
N
Edema(%
grades
2or
3)
[meanscore]
412/49
(24.5%
)
[2.1]
10/41
(24.4%
)
[2.0]
N
Adv Ther (2020) 37:2792–2812 2799

Table2
Characteristics
ofthestudiesincluded
inthesystem
aticreview
Stud
y,year,coun
try/intervention
sStud
ydesign/
Nparticipants
Participants:
inclusionandexclusioncriteria
Outcomes
analyzed
(MPFF
vscontrol)
Param
eter
Day
MPFF
Con
trol
Significant
(Y/N
)
74/49
(8.1%)
[1.6]
8/41
(19.5%
)
[1.7]
N
Prolapse
(%grades
2or
3)
[meanscore]
70/49
(0%)
[1.1]
2/41
(4.9%)
[1.3]
Y
Overalltherapeutic
evaluation
(patient)(%
reporting‘‘good’’o
r
‘‘excellent’’)
775.6%
39.0%
Y
Overalltherapeutic
evaluation
(investigator)
(%reporting‘‘good’’o
r
‘‘excellent’’)
775.5%
39.0%
Y
Misra
(2000)
[30]
India
MPF
For
placebo3000
mg/dayfor
4days,then2000
mg/dayfor
3days,then1000
mg/dayfor
83days
Double-blind
RCT
N=100
MPF
F:n=50
Placebo:
n=50
Meanage*
33–3
5years
21%
wom
en
Inclusioncriteria:O
utpatientsof
either
sex,[
18yearsold,withpasthistoryof
HD
of\
18monthsandpresenting
withacuterectalbleeding
of\
3days
inassociationwithvisiblydistendedor
displacedanalcushions
conformingto
grade1or
2internalhemorrhoids
identifiedon
proctoscopicexam
ination
Exclusion
criteria:patientswithanalfissure,infl
ammatoryboweldisease,
colorectalcancer
orpregnancy;previous
lasertreatm
entor
useof
aflavonoid
drug
1month
before
inclusion.
Previous
treatm
entwithanalgesics,topical
antihemorrhoidalointments,n
onsteroidalanti-in
flammatorydrugs,steroids,
anticoagulantsor
antiplatelet
agents
Bleedingcessation
340/50(80%
)19/50(38%
)Y
446/50(92%
)20/50(40%
)Y
546/50(92%
)26/50(52%
)Y
647/50(94%
)29/50(58%
)Y
747/50(94%
)30/50(60%
)Y
Bleedingcessationto
recurrence
(interval
days)
53.1
±22.7
34.2
±22.6
N
2800 Adv Ther (2020) 37:2792–2812

Table2
continued
Stud
y,year,coun
try/intervention
sStud
ydesign/
Nparticipants
Participants:
inclusionandexclusioncriteria
Outcomes
analyzed
(MPFF
vscontrol)
Param
eter
Day
MPFF
Con
trol
Significant
(Y/N
)
Panp
imanmas
(2010)
[31]
Thailand
CQ,M
PFF,
orplacebo
3000
mg/dayfor4days,then
2000
mg/dayfor3days
Double-blind
RCT
N=570
CQ:n=191
MPF
F:
n=189
Placebo:
n=190
Meanagenot
reported
49–5
5%
wom
en
Inclusioncriteria:acuterectalbleeding
within5days
Exclusion
criteria:p
revioushemorrhoidectom
y,treatm
entwithanticoagulantor
acetylsalicylicacid,treatmentwithotherantihemorrhoiddrugsat
that
time,
perm
anentprolapsedinternalhemorrhoidrequiringsurgery,moderateto
severe
hypertension;cardiovasculardiseases;renalfailure,cirrhosis,pregnancy,
andlactation
Bleeding(patient)f
7118/ 17
4(67.8%
)
132/ 17
8(74.2%
)
N
Pain
(patient)
757/174
(32.8%
)
58/ 17
8(32.6%
)
N
Discharge
(patient)
79/174(5.2%)
11/178
(6.2%)
N
Pruritus
(patient)
712/174
(6.9%)
17/178
(9.6%)
N
Prolapse
(patient)
76/174(3.4%)
11/178
(6.2%)
N
Bleeding(investigator)
728/174
(16.1%
)
25/178
(14.0%
)
N
Edema(investigator)
754/174
(31.0%
)
68/178
(38.2%
)
N
Vajrabukka(1994)
[32]
Thailand
MPF
For
placebo3000
mg/dayfor
4days,then2000
mg/dayfor
3days
Double-blind
RCT
N=226
MPF
F:
n=121
Placebo:
n=105
Meanage*
35–3
7years
50%
wom
en
Inclusioncriteria:non-pregnant
outpatient
[18
yearsof
agewithacute
symptom
sof
hemorrhoids
nolonger
than
3days
withpain,d
iscomfort,
bleeding
anddischargesymptom
s
Exclusion
criteria:perm
anently
prolapsedhemorrhoids
(grade
4)or
associated
anorectaldiseases
such
asanalfissure,fi
stula-in-ano,and
abscesses
Pain
g7
69/84(82.1%
)66/78(84.6%
)N
Analdiscom
fort
757/85(67.1%
)39/69(56.8%
)N
Bleeding
779/92(85.9%
)73/90(81.1%
)N
Discharge/leakage
740/51(78.9%
)27/42(64.7%
)N
Adv Ther (2020) 37:2792–2812 2801

Table2
continued
Stud
y,year,coun
try/intervention
sStud
ydesign/
Nparticipants
Participants:
inclusionandexclusioncriteria
Outcomes
analyzed
(MPFF
vscontrol)
Param
eter
Day
MPFF
Con
trol
Significant
(Y/N
)
Investigations
ofeffectsof
MPF
Ftreatm
entfollowingamedical/surgicalprocedure
Colak
(2003)
[21]
Turkey
MPF
F(dosenotreported)or
no
treatm
entfor7days
after
hemorrhoidectom
y
Observer-blind
RCT
N=112
MPF
F:n=56
Notreatm
ent:
n=56
Medianage*
41–4
5years
40–4
3%
wom
en
Inclusioncriteria:patientswithsymptom
aticthird-
orfourth-degree
hemorrhoids
who
underwenthemorrhoidectom
y
Exclusion
criteria:p
atientswithconcom
itantanaldiseasesuch
asfissure,abscess,
fistula,C
ohn’sor
ulcerative
colitis,o
rrectalcancer,and
thosetaking
oral
anticoagulants
Pain
(0–1
0scale)
25(2–7
)6(5–7
)Y
33.5(0–5
.5)
5(3.5–7
)Y
72(0–3
)3.5(2–4
)Y
Analgesicconsum
ption
738/56(67.9%
)48/56(85.7%
)Y
Analgesicconsum
ption
duration
(days)
2(0–3
)3(1.5–3
)Y
Overallsatisfaction
by
patient(‘‘moderate’’,
‘‘good’’and
‘‘excellent’’)h
725/28(89.3%
)21/28(75.0%
)Y
Dim
itropoulos
(2005)
[24]
Greece
MPF
F3000
mg/dayor
no
treatm
entfor5days
afterIRP
Observer-blind
RCT
N=351
MPF
F?
IRP:
n=117
IRP:
n=117
Meanage
49.2
years
51%
wom
en
Inclusioncriteria:ambulatory
maleandfemalepatients,over18
yearswithrectal
bleeding
dueto
grades
I,II,and
IIIacuteinternalhemorrhoids,w
ithno
previous
treatm
entforHD
withinthe6monthsprecedingthestudyand
without
coexistent
colondiseases
Exclusion
criteria:pregnancy,historyof
acuteHD
attacks,concom
itantlarge-
bowelandanalcanald
iseases,historyof
pelvicradiation,
useof
anticoagulant
andantiplatelet
agentsor
nonsteroidalanti-in
flammatorydrugs
Bleedingcessation
583/111
(74.8%
)
65/117
(55.6%
)
Y
Bleedingrecurrence
904/83
(4.8%)
9/65
(13.8%
)N
Ho(1995)
[27]
Singapore
MPF
F3000
mg/dayfor3daysthen
1500
mg/dayfor4days,o
rno
treatm
entafterhemorrhoidectom
y
Observer-blind
RCT
N=228
MPF
F:
n=114
Notreatm
ent:
n=114
Meanage
39.5
years
46%
wom
en
Inclusioncriteria:patientswiththreecolumns
ofsymptom
aticirreducible
prolapsedhemorrhoids
Bleeding(secondary)
6–15
1/114(0.9%)
7/114(6.1%)
Y
2802 Adv Ther (2020) 37:2792–2812

Table2
continued
Stud
y,year,coun
try/intervention
sStud
ydesign/
Nparticipants
Participants:
inclusionandexclusioncriteria
Outcomes
analyzed
(MPFF
vscontrol)
Param
eter
Day
MPFF
Con
trol
Significant
(Y/N
)
LaTorre
(2004)
[28]
Italy
MPF
F2000
mg/dayfor10
days
and1000
mg/dayfor20
days,o
r
notreatm
entafter
hemorrhoidectom
y
RCT
N=50
MPF
F:n=25
Notreatm
ent:
n=25
Meanage*
56–5
7years
37%
wom
en
Inclusioncriteria:patients[
18yearsoldwithan
indication
for
hemorrhoidectom
y,apasthistoryof
HDlongerthan
6months,symptom
atic
irreducibleprolapsedhemorrhoids
Exclusion
criteria:fistulaor
chronicanalfissure,infl
ammatoryboweldisease,
diabetes
orothermetabolicor
endocrinedisorders,alcoholism,d
rugabuse,
coagulationdisorders,andprevious
anorectalsurgery
Pain
i3
3.48
6.16
Y
603.88
±2.28
8.32
±2.88
Y
Pruritus
31.84
4.04
Y
601.96
±1.54
5.04
±2.49
Y
Tenesmus
31.48
5.36
Y
601.68
±1.82
7.21
±3.13
Y
Bleeding
32
4.4
Y
602.00
±1.29
5.24
±2.8
Y
Lee
(1998)
[29]
Korea
MPF
F3000
mg/dayfor4days,
then
2000
mg/dayfor3days,o
r
placeboafterhemorrhoidectom
y
RCT
N=54
MPF
F:n=27
Placebo:
n=27
Meanage*
41–4
3years
51–5
6%
wom
en
Inclusioncriteria:maleor
female,over
18yearsold,
hadun
dergonesurgeryfor
hemorrhoids
ofatleastgrade2atSamsung
MedicalCenter’s
GeneralSurgery
departmentfrom
Janu
ary1,
1997
toJanu
ary1,
1998
Exclusion
criteria:patientswho
werepregnant
ornu
rsing;sufferingfrom
rectal
orcoloncancer,gastrointestinalinfl
ammationor
infection,analdiseasesother
than
HD;patientstaking
anyothervasoactive
agent,anticoagulants,
adrenocorticalhorm
ones,n
onsteroidalanti-in
flammatorydrugs,antiplatelet
agentsor
otherpharmaceuticalHD
treatm
ent,andpatientswithcompliance
of\
80%
or[
120%
withthestudydrug
Pain
j18
18/27(66.7%
)7/27
(25.9%
)Y
Analdiscom
fort
1811/27(40.7%
)5/27
(18.5%
)N
Postoperativebleeding
1824/27(88.9%
)6/27
(22.2%
)Y
Postoperativepusdischarge
1823/27(85.2%
)10/27(37.0%
)Y
CQ
Cissus
quadrangularisL.,IRPinfrared
photocoagulation,MPF
Fmicronizedpurifiedflavonoid
fraction
*Meanagewas
calculated
bytreatm
entgroup
aAllsignsandsymptom
sgraded
ona4-pointscale:0=none;1=mild;2=significant;3=severe.P
ercentages
arepercentagesof
patientswithno
symptom
sat
day7
bThree-item
assessment:‘‘verysatisfied’’,‘‘satisfied’’,‘‘not
satisfied’’
cFour-item
assessment:‘‘verygood’’,‘‘good’’,‘‘useful’’,‘‘null’’
dIllsignsandsymptom
sgraded
ona4-pointscalefrom
0(nil)
to3(severe).P
ercentages
arepercentagesof
patientswithadecrease
inscore(improvem
ent)aftertreatm
ent
eAllsignsandsymptom
sgraded
ona4-pointscale:0=absent,1
=mild,2
=moderate,3=severe
fAllsignsandsymptom
sgraded
ona4-pointscale:0=absent,1
=mild,2
=moderate,3=severe.P
ercentages
arepercentagesof
patientswithadecrease
inscore(improvem
ent)aftertreatm
ent
gAllsignsandsymptom
sgraded
ona4-pointscale:0=nil,1=notableim
provem
ent,2=significant
improvem
ent,3=disappearanceor
cure.P
ercentages
arepercentagesof
patientswithim
provem
ent(scored1,
2,or
3)after
treatm
ent
hFour-item
assessment:‘‘excellent’’,‘‘good’’,‘‘m
oderate’’,‘‘poor’’.D
istributions
werecomparedusingWilcoxon
signed-ranktest
iAllsignsandsymptom
sgraded
ona4-pointscalefrom
0to
3:0=no
symptom
s,1=mild,2
=moderate,3=severe
intensity.The
values
aretheglobalscores
which
werecalculated
byadding
upmeansymptom
scores
over
the
observationperiod.V
aluesat
day60
aretabulatedwithstandard
deviations,w
hich
werenotprovided
forday3data
jAllsignsandsymptom
sgraded
ona4-pointscale:0=no
symptom
s,1=mild,2
=moderate,3=severe
intensity.Percentagesarepercentagesof
patientswithno
symptom
sat
day18
Adv Ther (2020) 37:2792–2812 2803

Effects of Intervention
BleedingFour studies reported significant effects of MPFFon bleeding in acute HD. One study showedthat the proportion of patients with bleeding atday 7 was significantly lower (P = 0.006) in theMPFF-treated group compared to the placebogroup [22, 23]. Another study showed thatbleeding scores (assessed using a 4-point scale)at day 4 and day 7 were significantly lower(P\0.05) [19] in the MPFF-treated group com-pared to the control group. In addition, theproportion of patients in whom bleeding hadimproved at day 60 was significantly higher(91% vs 59%, respectively; P\ 0.01) [25, 26]with MPFF treatment than with placebo treat-ment. In another study, significantly morepatients had ceased bleeding at day 3 through 7(P\0.01) with MPFF treatment than with pla-cebo, and bleeding duration was also signifi-cantly shorter by 2.1 (95% CI 1.2–2.9) days withMPFF treatment (P\0.01) [30]. Two studiesreported that neither patient- nor physician-assessed bleeding was significantly improvedwith MPFF treatment [31, 32].
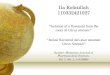
A pooled meta-analysis of two studies for thepresence/absence of bleeding after 7 days ofMPFF or placebo treatment for acute HD yieldedan OR of 0.082 (95% CI 0.027–0.250; P\ 0.001)in favor of MPFF treatment (Fig. 2a) [22, 23, 30].These results were confirmed in a sensitivityanalysis that included a third study (OR 0.101,95% CI 0.037–0.272; P\0.001) [19] (Fig. 2b). Inthis third study, the results for bleeding and theother binary endpoints excluded the modality‘‘mild’’ in contrast to the other studies, whichconsidered ‘‘mild’’, ‘‘moderate’’, or ‘‘severe’’events. Because this exclusion introduced a biasin the results, this study was added as a sensi-tivity analysis even though heterogeneity waslow (I2 = 0).
Four studies reported that bleeding after asurgical or outpatient procedure improved sig-nificantly with MPFF treatment. MPFF treat-ment was significantly better than no treatmentfor complete cessation of bleeding at day 5 afteran infrared photocoagulation (IRP) procedure(P = 0.004) [24], secondary bleeding at 7–-14 days (P = 0.03) [27] and 18 days (P\ 0.005)
[29] after hemorrhoidectomy, and for bleedingscores on days 1–3 (P\0.0001) and at day 60(P\0.0001) after hemorrhoidectomy [28].
PainFive studies investigated the effects of MPFFtreatment on pain in acute HD. Three studiesreported statistically significant improvementsin pain with MPFF treatment compared to pla-cebo, by pain score at day 7 (P\0.001 [22, 23];and P = 0.001 [19]), and by the proportion ofpatients in whom pain had improved at day 60(98% vs 47%; P\ 0.01) [25, 26]. Two studiesreported no significant improvement in pain atday 7 with MPFF compared to placebo [31, 32].
Fig. 2 Forest plot comparisons of MPFF versus placebofor bleeding in acute HD after 7 days of treatment. In apooled analysis of two studies using the fixed-effect(Mantel–Haenszel) method, micronized purified flavonoidfraction (MPFF) treatment was associated with a beneficialand statistically significant effect for bleeding in acutehemorrhoidal disease (odds ratio [OR] 0.08, 95% confi-dence interval [CI] 0.03–0.25; P\ 0.001) with nostatistical heterogeneity (I2 = 0%) (a). Results were similarin a sensitivity analysis that included a third study (Jiang2006) in which the bleeding endpoint was heterogeneous(OR 0.10, 95% CI 0.04–0.27; P\ 0.001) (b)
2804 Adv Ther (2020) 37:2792–2812

A pooled meta-analysis of two studies for thepresence/absence of pain after 7 days of MPFF orplacebo treatment yielded an OR of 0.11 (95%CI 0.01–1.11; P = 0.06) indicating that MPFFtreatment is associated with a nearly statisticallysignificant benefit for pain (Fig. 3). This resultshould be viewed in the context of high statis-tical heterogeneity (I2 = 85%) since the study byJiang and Cao [19] did not include ‘‘mild’’ as apain modality.
Three studies reported that MPFF signifi-cantly improved pain following hemorrhoidec-tomy. Patients treated with MPFF compared tothose receiving placebo or no treatment,respectively, had significant differences in:
• Median pain scores at day 2 (P = 0.033),day 3 (P = 0.011), and day 7 (P = 0.001) [21]
• Mean global pain scores over days 1–3 and atday 60 (P\0.0001) [28]
• Number of patients with no pain (18/27 vs7/27), mild pain (9/27 vs 16/27), or moderatepain (0/27 vs 4/27) at day 18 (P\0.005overall) [29]
PruritusIn acute HD, two studies reported significantimprovement in pruritus with MPFF, whereasone reported no improvement. Improvement inpruritus was observed at day 60 in 86% of
patients who received MPFF and in 58% ofpatients who received placebo (P\ 0.01)[25, 26]. A slight but statistically significantdifference in mean pruritus score was observedat day 7 (P\ 0.05) but not at day 4 [19]. Incontrast, patient-assessed pruritus was not sig-nificantly improved with MPFF treatment atday 7 compared to placebo (OR 1.24, 95% CI0.62–2.49; P = 0.539) [31].
One study reported significant improvementin pruritus after hemorrhoidectomy. Meanpruritus scores were significantly better withMPFF treatment than with no treatment overdays 1–3 and at day 60 (P\0.0001) after sur-gery [28].
Anal DiscomfortOne study reported significant improvement inanal discomfort with MPFF compared to pla-cebo (P\ 0.001) at day 7 [22, 23], whereas asecond study found no significant improvement[32]. After hemorrhoidectomy, one studyreported no significant improvement in analdiscomfort with MPFF compared to placebo atdays 7 and 18 [29].
TenesmusIn acute HD, tenesmus at day 60 was improvedin significantly more patients treated with MPFFthan with placebo (98% vs 50%; P\ 0.01)[25, 26]. After hemorrhoidectomy, tenesmusscores were significantly lower with MPFF thanwith no treatment over days 1–3 and at day 60(P\0.0001) [28].
Anal Discharge or LeakageThree studies reported that anal discharge,defined as an intermittent or continuousexpression of liquid from the anus, in acute HDsignificantly improved with MPFF compared toplacebo. The proportion of patients withoutdischarge or mild discharge was higher at day 7(P\0.001) [22, 23]. The proportion of patientswho had improved by day 60 (97% vs 54%;P\ 0.01) [25, 26] was significantly greater withMPFF than with placebo. Discharge improve-ment by patient assessment was significantlybetter at day 2 (P = 0.038) and discharge inten-sity by investigator assessment was significantly
Fig. 3 Forest plot comparison of MPFF versus placebo forpain in acute hemorrhoidal disease after 7 days oftreatment. In a pooled analysis of two studies, micronizedpurified flavonoid fraction (MPFF) treatment was associ-ated with a beneficial but not statistically significant effectfor pain in acute hemorrhoidal disease (odds ratio [OR]0.11 95% confidence interval [CI] 0.01–1.11, P = 0.06)with high statistical heterogeneity (I2 = 84.6%)
Adv Ther (2020) 37:2792–2812 2805

lower at day 7 (P = 0.001) [32]. In contrast, dis-charge was not significantly improved withMPFF in terms of leakage scores at day 4 or 7[19] or in the number of patients who reportedimprovement at day 7 (OR 1.35, 95% CI0.79–3.17; P = 0.473) [31].
A pooled meta-analysis of two studies for thepresence/absence of discharge or leakage aftertreatment for acute HD yielded an OR of 0.12(95% CI 0.04–0.42; P\ 0.001) in favor of MPFF,without statistical heterogeneity (I2 = 0) (Fig. 4)[19, 22, 23]. This result indicates that MPFFtreatment is associated with a statistically sig-nificant benefit of reducing discharge andleakage.
Following hemorrhoidectomy, one studyreported that the proportion of patients withdischarge at day 18 was lower with MPFF treat-ment than with placebo (14.8% vs 63.0%;P\ 0.005) [29].
EdemaTwo studies reported significant improvement inedema with MPFF treatment in acute HD. Clini-cal findings including edema were improved insignificantly more patients treated with MPFFthan in those treated with placebo after 7 days oftreatment (94% vs 58%; P\ 0.001) [23] and after60 days of treatment (98% vs 47%; P\ 0.01)[25, 26]. However, in one study, the proportion
of patients in whom edema improved after7 days of treatment with MPFF or with placebowas not significantly different (P = 0.43) [31].Similarly, mean edema score in patients was notsignificantly different after 4 or 7 days of treat-ment with MPFF or placebo [19].
Overall ImprovementIn acute HD, patient-assessed overall improve-ment or satisfaction in five studies was consis-tently greater with MPFF treatment than withplacebo. Improvement scores were significantlygreater withMPFF on all days from day 2 to day 7(P\0.001) [22, 23]. More patients were satisfiedor very satisfied with MPFF than with placeboafter 7 days of treatment (P = 0.023) [32] andafter 60 days of treatment (P\0.01) [25, 26].Overall efficacy was assessed as good or excellentby significantly more patients treated withMPFF(75.6%) than with placebo (39.0%; P = 0.007)[19]. Similarly, significantly more patientsreported day-to-day improvement with MPFF(73.5%) than with placebo (41.5%; P = 0.012)[19]. Patient satisfaction after hemorrhoidec-tomy was also significantly greater with MPFFtreatment than with no treatment (P = 0.001)[21].
A pooled meta-analysis of three studies forpatient-assessed overall improvement at day 7in acute HD or after hemorrhoidectomy yieldedan OR of 5.25 (95% CI 2.58–10.68; P\ 0.001) infavor of MPFF treatment (Fig. 5a) [19, 21–23].
In four studies of acute HD, investigators alsoconsidered treatment efficacy to be greater withMPFF than with placebo. After 7 days of treat-ment, physician investigators in two studiesconsidered therapeutic activity to be good orexcellent for significantly more patients treatedwith MPFF (75.5% versus 39.0%, respectively)than with placebo (32% and, respectively;P\ 0.001 and P\0.006) [19]. Overall activityevaluated by the investigator at day 7 was alsosignificantly better with MPFF than with pla-cebo in two other studies (P\0.001 andP = 0.009, respectively) [22, 23, 32]. Resultswere similar after 60 days of treatment, withoverall efficacy being considered good or verygood for 83% of patients treated with MPFFcompared to 37% of those treated with placebo(P\0.01) [25, 26].
Fig. 4 Forest plot comparison of MPFF versus placebo fordischarge or leakage after 7 days of treatment. In a pooledanalysis of two studies using the fixed-effect (Man-tel–Haenszel) method, micronized purified flavonoidfraction (MPFF) treatment was associated with a beneficialand statistically significant effect for discharge or leakage inacute hemorrhoidal disease (odds ratio [OR] 0.12, 95%confidence interval [CI] 0.04–0.42; P\ 0.001) with nostatistical heterogeneity (I2 = 0%)
2806 Adv Ther (2020) 37:2792–2812

A pooled meta-analysis of two studies forinvestigator-assessed overall improvement inacute HD at day 7 yielded an OR of 5.51 (95% CI2.76–11.0; P\ 0.001) in favor of MPFF treat-ment, with no statistical heterogeneity (I2 = 0)(Fig. 5b) [19, 22, 23].
Other OutcomesTwo studies investigated the effect of MPFFtreatment on prolapse [19, 31]; however, therewere no significant differences between theMPFF arm and the control placebo groups withrespect to this outcome.
Two out of three studies that investigatedconcomitant use of topical and systemic anal-gesics found statistically significant beneficialeffects associated with MPFF treatment. Onestudy found that MPFF treatment significantlyreduced the use of topical and systemic anal-gesics in acute HD from day 3 (P = 0.041 andP = 0.013, respectively) through day 7(P\0.001 and P\ 0.001, respectively) [22, 23].One study found that uptake of intramuscularanalgesic at 2 and 3 days (P = 0.022 andP = 0.007) after hemorrhoidectomy and overall(P = 0.021) was significantly less with MPFFtreatment [21].One study reportedno significantdifference in analgesic consumption after hem-orrhoidectomy between the MPFF and no treat-ment groups [27].
Two studies investigated the effects of MPFFtreatment on hospital length-of-stay (LOS). Onestudy reported that hospital LOS after hemor-rhoidectomy was significantly shorter withMPFF than with no treatment (2 vs 2.5 days,P = 0.001) [21]. One study reported no signifi-cant difference in hospital LOS after hemor-rhoidectomy between groups receiving MPFFtreatment or no treatment [27].
Of the three studies that investigated theeffects of MPFF treatment on recurrence ofacute episodes of HD, two studies reported sta-tistically significant beneficial effects of MPFFtreatment and one study was associated with abeneficial but not statistically significant effect.The proportion of patients who presented withan acute HD episode during 60 days of treat-ment was significantly smaller with MPFFtreatment than with placebo (40% vs 76%;P\ 0.05) [25, 26]. The frequency of bleedingrelapse in acute HD was reduced by 24% (95%CI 2–46) with MPFF taken as preventive treat-ment over 90 days compared to placebo treat-ment (P\0.05) [30]. In the third study, thebleeding relapse rate within 90 days after IRPtended to be lower with 5 days of MPFF post-procedure treatment (4.8%) than with notreatment (13.8%), but the difference was notstatistically significant (P = 0.12) [24].
MPFF was well tolerated and none of thesestudies showed any serious side effect and themajority of the studies had no secondary effect.Only in a few cases were mild, known secondary
Fig. 5 Forest plot comparisons of MPFF versus placebofor overall improvement according to patient and toinvestigator after 7 days of treatment. In a pooled analysisof three studies using the fixed-effect (Mantel–Haenszel)method, micronized purified flavonoid fraction (MPFF)treatment was associated with a beneficial and statisticallysignificant effect for overall improvement according topatients (odds ratio [OR] 5.25, 95% confidence interval[CI] 2.58–10.68; P\ 0.001) with no statistical hetero-geneity (I2 = 0%) (a). In a pooled analysis of two studiesusing the fixed-effect (Mantel–Haenszel) method, MPFFtreatment was associated with a beneficial and statisticallysignificant effect for overall improvement according toinvestigators (OR 5.51, 95% CI 2.76–11.00; P\ 0.001)with no statistical heterogeneity (I2 = 0%) (b)
Adv Ther (2020) 37:2792–2812 2807

effects like gastralgia, diarrhea, and abdominalpain declared.
DISCUSSION
MPFF has a variety of significant anti-inflam-matory, antioxidant, and venoprotectiveactions, which form the basis of its beneficialclinical effects [10, 12, 33]. In a number ofexperimental models, it reduced venousinflammation by inhibiting leukocyte rolling,adhesion, and migration, and inhibited thesynthesis of inflammatory mediators[10, 34–36]. It improves venous tone and lym-phatic drainage by modulating noradrenergicsignalling and reducing norepinephrine meta-bolism [37, 38]. MPFF significantly reducescapillary hyperpermeability and improves thecapillary resistance in patients with abnormalcapillary fragility leading to further improve-ment of microcirculation [39, 40]. As venouspathologies and diminished venous return playprominent roles in HD, these actions of MPFFprovide the rationale for its use in treating HD.
To study the efficacy of MPFF across abroader spectrum of signs and symptoms inpatients with HD, we examined data from 11studies that compared MPFF to placebo or notreatment for the treatment of acute HD orsymptoms after a medical or surgical procedureto remove prolapsed hemorrhoids. In morethan half of the studies, there was some risk ofbias due to incomplete descriptions of ran-domization, allocation concealment, or blind-ing of participants to the treatment forsubjective patient-determined endpoints suchas pain or overall improvement and selectivereporting. As a result of heterogeneity in studydesign, only selected endpoints could be used inpooled meta-analyses to assess the magnitude ofeffects across the different studies. Quantitativeanalysis of pooled results indicated that 7 daysof MPFF treatment in patients with acute HDwas associated with statistically significantbeneficial effects for reducing bleeding(P\0.001), reducing discharge and leakage(P\0.001), and overall improvement accord-ing to patients (P = 0.002) and investigators(P\0.001). Quantitative analysis also indicated
that MPFF treatment tended to decrease pain(P = 0.06). In general, qualitative analysis of thestudies indicated that MPFF treatment wasbeneficial for the most important signs andsymptoms of acute HD and for post-hemor-rhoidectomy patients.
Four studies in this systematic review repor-ted significant reductions in bleeding comparedto placebo after MPFF treatment[19, 22, 23, 25, 26, 30] versus two that reportedno significant benefit [31, 32]. Only two of thesestudies could be combined for meta-analysis[22, 23, 30], with the result showing a signifi-cant benefit in favor of MPFF treatment byreducing the risk of bleeding by over 90% (OR0.08, P\ 0.001). Four studies also reported thatMPFF treatment showed an apparent benefit inreducing post-procedure bleeding [24, 27–29].
Similar benefits of MPFF treatment inreducing bleeding were reported in two previ-ous meta-analyses. In a Cochrane meta-analysisof the studies by Jiang and Misra [19, 30], Pereraet al. found an OR of 0.12 (95% CI 0.04–0.37;P\ 0.001) in favor of MPFF over placebo [13].Whereas in a more recent meta-analysis of thestudies by Jiang, Cospite, and Misra, which waspublished while our study was being conducted,Aziz et al. found a relative risk (RR) of 1.46 (95%CI 1.10–1.93; P = 0.008) in favor of MPFFtreatment for reducing bleeding [41]. Our find-ings confirm these results, indicating that MPFFreduces bleeding effectively and quickly.
Qualitative analysis of MPFF treatment forreducing pain associated with acute HD inclu-ded three studies reporting significant benefitafter treatment [19, 22, 23, 25, 26] and twostudies reporting no significant benefit [31, 32].Pooled meta-analysis indicated that MPFFtreatment is associated with a nearly statisticallysignificant benefit for pain (P = 0.06). Resultsfrom three previous meta-analyses are varied,with one reporting significant reduction in painwith MPFF or flavonoid (RR 0.35, 95% CI0.18–0.69) treatment [8], one a nearly signifi-cant benefit (P = 0.06) [13], and one no signifi-cant benefit (P = 0.47) [41]. The reason for thisvariability may be that pain is not a universalsymptom in internal HD and, if present, it isoften at a low level. Thus it may be difficult todemonstrate a statistically significant benefit in
2808 Adv Ther (2020) 37:2792–2812

studies lacking enough patients to provide suf-ficient statistical power.
In contrast, MPFF treatment after hemor-rhoidectomy demonstrated consistent and sta-tistically significant benefits in pain relief[21, 28, 29]. It is possible that the higher level ofpain associated with hemorrhoidectomy allowsthe pain relief benefit of MPFF to be demon-strated more consistently than with acute HD.
Qualitative analyses suggest that MPFFtreatment may provide some benefits for pruri-tus. Two studies reported significant improve-ments in anal itching in acute HD [19, 25, 26],although the treatment period in the Gode-berge study was long (60 days) and the itchingscore improvement at day 7 in the Jiang studywas small (1.1 vs 1.3). In contrast, a third studyreported no significant improvement after7 days of MPFF treatment [31]. In the one studythat investigated pruritus after hemorrhoidec-tomy, significant benefits were observed inglobal itching scores [28]. Similarly, meta-anal-yses conducted by Perera et al. [13] and byAlonso-Coello et al. [8] found significant bene-fits for pruritus with flavonoid treatment in HD.
Among the five studies that investigated analdischarge or leakage in acute HD, three reporteda significant benefit with MPFF treatment[22, 23, 25, 26, 32], whereas two did not [19, 31].However, quantitative analysis of the results thatcould be pooled indicated a statistically signifi-cant benefit in favor ofMPFF. This result was alsofound in a previous meta-analysis [13] thatincluded the same studies by Jiang and Cospite[19, 22]. Significant benefits of MPFF in leakageor discharge were also observed in the recoveryperiod after hemorrhoidectomy [29]. Takentogether, these results could suggest a likelybenefit for MPFF treatment in reducing leakagein HD.
There was some evidence for a positive effectof MPFF treatment on tenesmus from twostudies [25, 26, 28] but the evidence forimprovement of anal discomfort or edema waslimited with only one of three studies reportinga significant benefit for each symptom[22, 23, 25, 26]. Such symptoms may be difficultto assess consistently if anal discomfort is notprecisely defined and edema is difficult tomeasure.
Consistent benefits were reported for MPFFtreatment in patient-assessed overall improve-ment and satisfaction either in acute HD[19, 22, 23, 25, 26, 32] or after hemorrhoidec-tomy [21]. The meta-analysis of three of thesestudies [19, 21–23] yielded a significant OR of5.25 in favor of MPFF treatment. These resultsstrongly suggest that patients consider MPFF tobe an effective treatment providing quick relieffor acute HD and in improving the quality ofthe recovery period after hemorrhoidectomy.Similarly, investigators in four studies alsoconsistently considered MPFF an effectivetreatment [19, 22, 23, 25, 26, 32], and this wassupported by the accompanying meta-analysis.
Reduction in the need for concomitantanalgesic use, shorter hospital stays after hem-orrhoidectomy, and prevention of relapses havebeen identified as indirect benefits of treatmentwith MPFF in some studies [21–23, 25, 26, 30].
Compared to our meta-analysis, the previ-ously published meta-analyses by Perera et al.[13] and Alonso-Coello et al. [8] did not targetany particular venoactive drug. On the otherhand, the meta-analysis by Aziz et al. [41]specifically examined the effects of MPFF butexcluded trials in patients who underwent sur-gery/procedures for HD. Moreover, Aziz et al.assessed only pain, bleeding, and itchingwhereas, in our meta-analysis, a wide range ofparameters were investigated. As far as we canascertain, the initial scope of our literaturesearch was therefore broader than for the othermeta-analyses and assessed more parameterswhich provided further added value.
The chief limitation in this study is that only11 studies could be included in the systematicreview and there was considerable heterogene-ity among the endpoints reported in thesestudies. This heterogeneity limited our ability topool the studies for meta-analysis. In addition,variability in the results for some of the end-points, which may have been the consequenceof differences in patient populations andassessment methods, made it difficult to drawfirm conclusions from the qualitative analyses.Another limitation is that the risk of bias washigh or unclear in seven of the 11 studies.Despite the fact that no limit for treatmentduration was set, all of the studies which met
Adv Ther (2020) 37:2792–2812 2809

the selection criteria treatment were of shortduration or, if of longer duration, only short-term assessments were performed. One studyperformed by Godeberge and collaborators[25, 26] measured longer-term efficacy, but inan open-label follow-up. Consequently, nostudies assessing the long-term benefit of MPFFversus placebo under blinded conditions havebeen identified. Lastly, none of the studiesevaluated potential benefits of treatment withMPFF on hard clinical endpoints (e.g., less needfor transfusions, fewer hospital admissions)after hemorrhoidectomy.
Despite these limitations, findings fromqualitative analysis were consistent in suggest-ing benefits of MPFF treatment in reducingbleeding in acute HD and in patients afterhemorrhoidectomy. Quantitative analyses alsoindicated that MPFF treatment was associatedwith a significant benefit in reducing dischargeand leakage, and a benefit in reducing pain thatwas nearly statistically significant. Consistentand statistically significant quantitative evi-dence was also found for the overall improve-ment in symptoms as assessed by patients andinvestigators.
CONCLUSIONS
The aim of our review was to assess all publishedrandomized placebo-controlled trials investi-gating the effect of MPFF in relieving the signsand symptoms in patients with acute HD as wellas RCTs with patients who underwent medicalor surgical procedures. We thus performed anextensive search of several different databases toidentify these studies.
Taken together, the results of our qualitativeand quantitative analyses suggest that MPFFtreatment can improve themost important signsand symptoms of HD including bleeding, pain,pruritus, tenesmus, and anal discharge/leakage.
ACKNOWLEDGEMENTS
Funding. Financial support for this study,Rapid Service Fee and Open Access Fees was
provided by the Institut de Recherches Inter-nationales Servier (Suresnes, France). Thesponsor provided support for the literaturesearch, data acquisition, statistical analysis, andmedical writing assistance. The sponsor alsoreviewed the manuscript prior to submission forpublication.
Medical Writing and Editorial Assis-tance. Medical writing and editorial assistancewas provided by Dr. Kurt Liittschwager (4Clin-ics, France) and paid for by the sponsor (Servier,France). Statistical analysis was performed bystatisticians employed by the sponsor.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Disclosures. Parvez Sheikh, Varut Lohsiri-wat, and Yury Shelygin have received speakerfees from the study sponsor Servier.
Compliance with Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not contain any studies with humanparticipants or animals performed by any of theauthors.
Data Availability. The datasets generatedduring and/or analyzed during the currentstudy are available from the correspondingauthor on reasonable request.
Open Access. This article is licensed under aCreative Commons Attribution-Non-Commercial 4.0 International License, whichpermits any non-commercial use, sharing,adaptation, distribution and reproduction inany medium or format, as long as you giveappropriate credit to the original author(s) andthe source, provide a link to the CreativeCommons licence, and indicate if changes weremade. The images or other third party materialin this article are included in the article’sCreative Commons licence, unless indicatedotherwise in a credit line to the material. Ifmaterial is not included in the article’s Creative
2810 Adv Ther (2020) 37:2792–2812

Commons licence and your intended use is notpermitted by statutory regulation or exceeds thepermitted use, you will need to obtain permis-sion directly from the copyright holder. To viewa copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
REFERENCES
1. Haas PA, Haas GP, Schmaltz S, Fox TA Jr. Theprevalence of hemorrhoids. Dis Colon Rectum.1983;26(7):435–9.
2. Johanson JF, Sonnenberg A. The prevalence ofhemorrhoids and chronic constipation. An epi-demiologic study. Gastroenterology. 1990;98(2):380–6.
3. Riss S, Weiser FA, Schwameis K, et al. The preva-lence of hemorrhoids in adults. Int J Colorectal Dis.2012;27(2):215–20.
4. Sun Z, Migaly J. Review of hemorrhoid disease:presentation and management. Clin Colon RectalSurg. 2016;29(1):22–9.
5. Madoff RD, Fleshman JW. American Gastroentero-logical Association technical review on the diag-nosis and treatment of hemorrhoids.Gastroenterology. 2004;126(5):1463–73.
6. Cristea C, Lewis CR. Hemorrhoidectomy. StatPearls.Treasure Island (FL). 2019. https://www.ncbi.nlm.nih.gov/books/NBK549864.
7. Misra MC. Drug treatment of haemorrhoids. Drugs.2005;65(11):1481–91.
8. Alonso-Coello P, Zhou Q, Martinez-Zapata MJ, et al.Meta-analysis of flavonoids for the treatment ofhaemorrhoids. Br J Surg. 2006;93(8):909–20.
9. Kakkos SK, Nicolaides AN. Efficacy of micronizedpurified flavonoid fraction (Daflon�) on improvingindividual symptoms, signs and quality of life inpatients with chronic venous disease: a systematicreview and meta-analysis of randomized double-blind placebo-controlled trials. Int Angiol.2018;37(2):143–54.
10. Mansilha A, Sousa J. Pathophysiological mecha-nisms of chronic venous disease and implicationsfor venoactive drug therapy. Int J Mol Sci.2018;19(6):1669.
11. Johanson JF. Nonsurgical treatment of hemor-rhoids. J Gastrointest Surg. 2002;6(3):290–4.
12. Lyseng-Williamson KA, Perry CM. Micronisedpurified flavonoid fraction: a review of its use inchronic venous insufficiency, venous ulcers andhaemorrhoids. Drugs. 2003;63(1):71–100.
13. Perera N, Liolitsa D, Iype S, et al. Phlebotonics forhaemorrhoids. Cochrane Database Syst Rev.2012(8):CD004322.
14. Moher D, Liberati A, Tetzlaff J, Altman DG. Reprint-preferred reporting items for systematic reviews andmeta-analyses: the PRISMA statement. Phys Ther.2009;89(9):873–80.
15. DerSimonian R, Laird N. Meta-analysis in clinicaltrials. Control Clin Trials. 1986;7(3):177–88.
16. Mantel N, Haenszel W. Statistical aspects of theanalysis of data from retrospective studies of dis-ease. J Natl Cancer Inst. 1959;22(4):719–48.
17. Cochran WG. The combination of estimates fromdifferent experiments. Biometrics. 1954;10(1):101–29.
18. Higgins JP, Thompson SG, Deeks JJ, Altman DG.Measuring inconsistency in meta-analyses. BMJ.2003;327(7414):557–60.
19. Jiang ZM, Cao JD. The impact of micronized puri-fied flavonoid fraction on the treatment of acutehaemorrhoidal episodes. Curr Med Res Opin.2006;22(6):1141–7.
20. Higgins JPT, Altman DG, Sterne JAC. Chapter 8:Assessing risk of bias in included studies. In: Hig-gins JPT, Green S, editors. Cochrane Handbook forSystematic Reviews of Interventions Version 510[updated March 2011]. London: The CochraneCollaboration; 2011.
21. Colak T, Akca T, Dirlik M, Kanik A, Dag A, Aydin S.Micronized flavonoids in pain control after hem-orrhoidectomy: a prospective randomized con-trolled study. Surg Today. 2003;33(11):828–32.
22. Cospite M. Double-blind, placebo-controlled eval-uation of clinical activity and safety of Daflon500 mg in the treatment of acute hemorrhoids.Angiology. 1994;45(6 Pt 2):566–73.
23. Cospite M. Double blind placebo controlled evalu-ation of clinical activity and safety of Daflon500 mg in the treatment of acute haemorrhoids.Phlebology. 1994;9(Suppl 1):40–3.
24. Dimitroulopoulos D, Tsamakidis K, Xinopoulos D,Karaitianos I, Fotopoulou A, Paraskevas E. Prospec-tive, randomized, controlled, observer-blinded trialof combined infrared photocoagulation andmicronized purified flavonoid fraction versus each
Adv Ther (2020) 37:2792–2812 2811

alone for the treatment of hemorrhoidal disease.Clin Ther. 2005;27(6):746–54.
25. Godeberge P. Daflon 500 mg is significantly moreeffective than placebo in the treatment of haem-orrhoids. Phlebology. 1992;7(Suppl. 2):61–3.
26. Godeberge P. Daflon 500 mg in the treatment ofhemorrhoidal disease: a demonstrated efficacy incomparison with placebo. Angiology. 1994;45(6 Pt2):574–8.
27. Ho YH, Foo CL, Seow-Choen F, Goh HS. Prospectiverandomized controlled trial of a micronizedflavonidic fraction to reduce bleeding after haem-orrhoidectomy. Br J Surg. 1995;82(8):1034–5.
28. La Torre F, Nicolai AP. Clinical use of micronizedpurified flavonoid fraction for treatment of symp-toms after hemorrhoidectomy: results of a ran-domized, controlled, clinical trial. Dis ColonRectum. 2004;47(5):704–10.
29. Lee HW, Lee WY, Chun HK. Clinical effects ofVenitol� on complications after hemorrhoidec-tomy prospective randomized and placebo-con-trolled trial. J Korean Soc Coloproctol. 1998;14(4):761–6.
30. Misra MC, Parshad R. Randomized clinical trial ofmicronized flavonoids in the early control ofbleeding from acute internal haemorrhoids. Br JSurg. 2000;87(7):868–72.
31. Panpimanmas S, Sithipongsri S, Sukdanon C,Manmee C. Experimental comparative study of theefficacy and side effects of Cissus quadrangularis L.(Vitaceae) to Daflon (Servier) and placebo in thetreatment of acute hemorrhoids. J Med Assoc Thai.2010;93(12):1360–7.
32. Vajrabukka T, Rojanasakul A, Vathanophas V, et al.Therapeutic activity of Daflon 500 mg� in acuteepisodes of hemorrhoids. Chula Med J. 1994;38(2):77–83.
33. Katsenis K. Micronized purified flavonoid fraction(MPFF): a review of its pharmacological effects,
therapeutic efficacy and benefits in the manage-ment of chronic venous insufficiency. Curr VascPharmacol. 2005;3(1):1–9.
34. das Gracas CSM, Cyrino FZ, de Carvalho JJ, Blanc-Guillemaud V, Bouskela E. Protective effects ofmicronized purified flavonoid fraction (MPFF) on anovel experimental model of chronic venoushypertension. Eur J Vasc Endovasc Surg. 2018;55(5):694–702.
35. Friesenecker B, Tsai AG, Allegra C, Intaglietta M.Oral administration of purified micronized flavo-noid fraction suppresses leukocyte adhesion inischemia-reperfusion injury: in vivo observations inthe hamster skin fold. Int J Microcirc Clin Exp.1994;14(1–2):50–5.
36. Korthuis RJ, Gute DC. Postischemic leukocyte/en-dothelial cell interactions and microvascular barrierdysfunction in skeletal muscle: cellular mecha-nisms and effect of Daflon 500 mg. Int J MicrocircClin Exp. 1997;17(Suppl 1):11–7.
37. Cotonat A, Cotonat J. Lymphagogue and pulsatileactivities of Daflon 500 mg on canine thoraciclymph duct. Int Angiol. 1989;8(4 Suppl):15–8.
38. McHale NG, Hollywood MA. Control of lymphaticpumping: interest of Daflon 500 mg. Phlebology.1994;9:23–5.
39. Behar A, Lagrue G, Cohen-Boulakia F, Baillet J.Study of capillary filtration by double labellingI131-albumin and Tc99m red cells. Application tothe pharmacodynamic activity of Daflon 500 mg.Int Angiol. 1988;7(2 Suppl):35–8.
40. Galley P, Thiollet M. A double-blind, placebo-con-trolled trial of a new veno-active flavonoid fraction(S 5682) in the treatment of symptomatic capillaryfragility. Int Angiol. 1993;12(1):69–72.
41. Aziz Z, Huin WK, Badrul Hisham MD, Tang WL,Yaacob S. Efficacy and tolerability of micronizedpurified flavonoid fractions (MPFF) for haemor-rhoids: a systematic review and meta-analysis.Complement Ther Med. 2018;39:49–55.
2812 Adv Ther (2020) 37:2792–2812