Embed Size (px)
DESCRIPTION
aricle or essay
Citation preview

PEDIATRIC DENTISTRY V 33 / NO 7 NOV I DEC I I
Microleakage of Stainless Steel Crowns Placed on Intact and Extensively DestroyedPrimary First Molars: An In Vitro StudyBahman Seraj, DDS. MSd • Mahdi Shahrabi, DDS, MSc • Pouria Motahari, DDS, MSc' • Rahil Ahmadi, DDS, MSC • Sara Ghadimi, DDS,Shahram Mosharalian, DDS, MSc' • Kaveh Mohammadi, DDS' • Mohammad Javad Kharazifard, DDS"
Abstract: Purpose: The purpose of this investigation was to evaluate the effect of residual tooth structure on the microieakage of stainiess steei crowns
cemented with giass ionomer on primary maxiiiary and mandibuiar first moiars. Methods: Thirty extracted primary moiars were divided into 2 groups:
group 1 induded intact teeth: and group 2 induded extensiveiy carious sampies. Each tooth received standard preparation, and each crown was
iuted with G-CEM on its specific specimen. Teeth were ioaded verticaiiy and transferred to distiiied water After thermoeyding and immersing in methy-
iene biue solution, the teeth were sectioned and examined microseopieaiiy for mieroieakage. Data were analyzed using Mann-Whitney U and Wiieoxon
signed-rank tests. Results: All specimens (intact and damaged teeth) had microieakage, aithough most of these presented oniy minimum microieakage.
No statisticaily significant differences were found in the microieakage of sound and extensiveiy carious teeth on either the buccal (P=.62) or iinguai (P'.65)
side. Bueeai (P=.73) and iinguai (P=.63) surfaces showed simiiar microieakage scores in primary maxillary and mandibuiar moiars. Conclusions: There was
no significant difference in the microieakage of sound or extensiveiy carious teeth and primary maxiiiary or mandibular first molars (Pediatr Dent 2011:
33:525-8) Received Aprii 7, 2010 I Last Revision November 8,2010 i Accepted November 16, 2010
KEYWORDS: STAINLESS STEEL CROWN, PRIMARY TEETH, MICROLEAKAGE
Dental caries is the most prevalent chronic childhood disease.'Rich carbohydrate diets, inadequate plaque control, low salivaryflow, and the presence of enamel defecrs lead to the developmentand progress of dental caries.'' Large carious lesions, early in-volvement of the pulp tissues, abscess formation, and pain arepredictable in the absence of any preventive or treatment pro-cedures. In this situation, particularly primary first molars areextracted to relieve pain and discomfort or prevent future treat-ment complications.''•^
Premature loss of primary molars causes supraeruption ofopposing teeth, space loss, unattractive appearance, and disrup-tion in jaw relationships.'' Therefore, preserving the primary teethis strongly recommended. It is advocated that, even in the con-dition of extensive destruction of the crown with pulp tissuesinvolved, if there is a proper pulp treatment prognosis, the pulptherapy should be performed''*'* Regardless of the pulp therapyemployed, long term success of this procedure is significantlyafl"ected by the integrity of the coronal seal; lack or loss of a co-ronal seal causes failure'*. Nevertheless, restoring multisurfacecarious posterior primary teeth, with or without pulpal involve-
Drs. 'Seraj and 'Mosharafian are assistant professors: ^Dr. Shahrabi is associate pro-
fessor. Department of Pédiatrie Dentistry: 'Dr. Ghadimi is an assistant professor. De-
partment of Pédiatrie Dentistry and Laser Research Center: 'Dr. Motahari is assistant
professor. Oral Pathology Department. 'Dr. Kharazifard is a researeh adnser. Dental
Research Center. 'Dr. Mohammadi is a graduate student. Pédiatrie Dentistry Depart-
ment, all at the Dental School. Tehran University of Medical .Sciences. Teham. Iran.
*Dr. Ahmadi is an assistant professor. Department of Pédiatrie Dentistry. Dental
School, Shahed University. Tehran. Iran.
Correspond with Dr. Rahil Ahmadi ot [email protected]
ment, is a challenging task in pédiatrie dentistry. The restorationshould adequately protect the remaining tooth and prevent theseepage of oral fluids through its margins.''''''''
In 1950, Humphrey described the use of a stainless steelcrown (SSC) to serve as a definitive restoration in primary mo-lars."'•''" These prefabricated, preformed crowns are the idealchoice in managing extensive carious lesions, particularly multi-surface decay of primary first and second molars, fractured teeth,restoring primary molars following pulp therapy, poor oralhygiene conditions, and the treatment of hereditary and develop-mental anomalies.''^''°'"
Currently, SSCs are widely used in the restorative treatmentof primary teeth.'•^•'" Advantages which make these restorationsinevitable in everyday practice include: low cost; less chair time;saving the tooth from future caries attacks; lack of mercury; andpreserving normal vertical dimensions.'"" Retrospective studieshave shown that SSCs are superior in durability and lifespan com-pared to multisurface amalgam and composite restorations.''^'"
Despite all the benefits mentioned above, similar to any otherrestoration, microleakage through the SSC margin is the majordeterrent to the development of a durable, successful restoration.'"•'''The clinically undetectable passage of bacterial toxins and oralfluids may lead to some complications and, consequently, failurewithin a few years."" Tooth hypersensitivity, pulpal irritation, pe-riodontal disease, and deterioration of restorative or luting ma-terials may be associated with this phenomenon.'''''^'
Because of the destructive complications associated withmicroleakage, it is essential to assess the influence of differentclinical methods and factors in restoring teeth with SSCs in orderto understand how these parameters might affect microleakage
MICROLEAKAGE OF SSC ON INTACT AND DAMAGED PRIMARY MOLARS 525
PEDIATRIC DENTISTRY V 33 I NO 7 NOV I DEC 11
and, thus, the survival and success rate of the restoration. Asstated by many investigators, the success rate and longevity of thecrown restorations are related to numerous factors. These includequality of tooth preparation, crown size selection, and cementa-tion.'-"'''"^^' There is some evidence that occluso-gingival lengthof the prepared tooth is an important factor regarding retentionand, thus, microleakage of the crowns.'"•'''•" By contrast, Myerset al. and Full et al. described that retention of the crown is main-ly attained when the tooth's cervical area is intact, and the re-maining tooth structure has limited influence on the restoration'ssuccess.-"'^ Despite these controversial outcomes about the re-maining tooth structure following tooth preparation, little hasbeen done to evaluate the influence of the residual tooth structure,in grossly destroyed teeth, on the microleakage of the SSCs.~"
Thus, the purpose of this study was to assess the effect ofthe remaining tooth structure on the microleakage of SSCs lutedwith glass ionomer cement (GIC) placed on extensively de-stroyed primary maxillary and mandibular first molars.
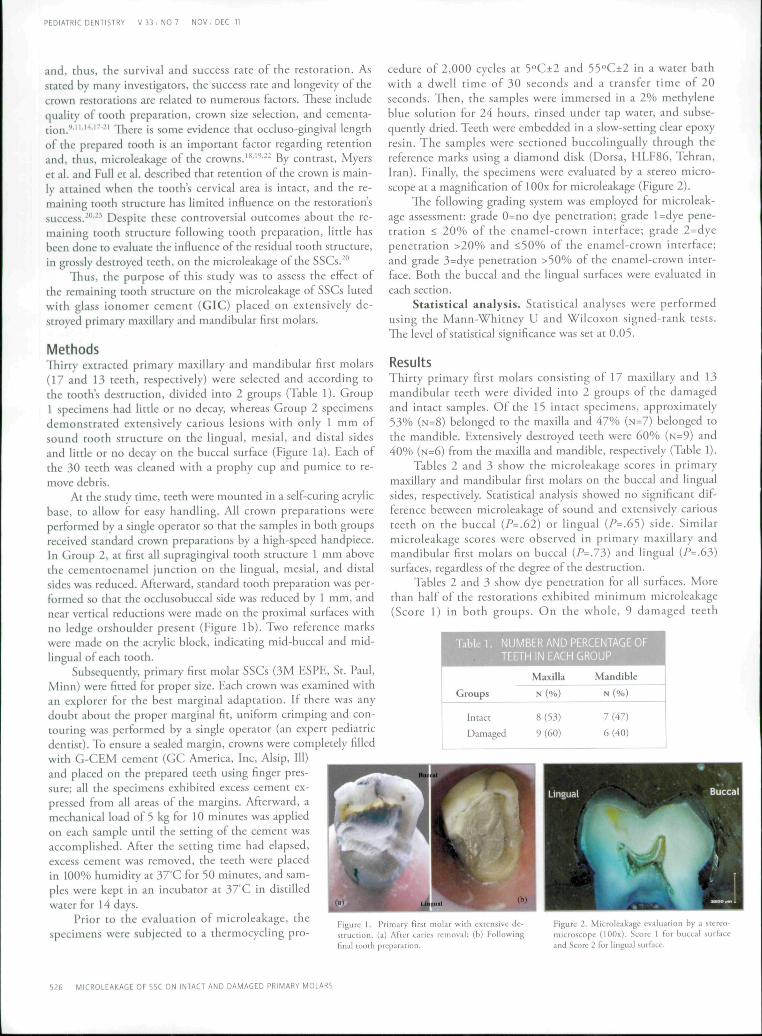
MethodsTliirty extracted primary maxillary and mandibular first molars(17 and 13 teeth, respectively) were selected and according tothe tooth's destruction, divided into 2 groups (Table 1). Group1 specimens had little or no decay, whereas Group 2 specimensdemonstrated extensively carious lesions with only 1 mm ofsound tooth structure on the lingual, mesial, and distal sidesand little or no decay on the buccal surface (Figure la). Each ofthe 30 teeth was cleaned with a prophy cup and pumice to re-move debris.
At the study time, teeth were mounted in a self-curing acrylicbase, to allow for easy handling. All crown preparations wereperformed by a single operator so that the samples in both groupsreceived standard crown preparations by a high-speed handpiece.In Group 2, at first all supragingival tooth structure 1 mm abovethe cementoenamel junction on the lingual, mesial, and distalsides was reduced. Afterward, standard tooth preparation was per-formed so that the occlusobuccal side was reduced by 1 mm, andnear vertical reductions were made on the proximal surfaces withno ledge orshoulder present (Figure lb). Two reference markswere made on the acrylic block, indicating mid-buccal and mid-lingual of each tooth.
Subsequently, primary first molar SSCs (3M ESPE, St. Paul,Minn) were fitted for proper size. Each crown was examined withan explorer for the best marginal adaptation. If there was anydoubt about the proper marginal fit, uniform crimping and con-touring was performed by a single operator (an expert pédiatriedentist). To ensure a sealed margin, crowns were completely filledwith G-CEM cement (GC America, Inc, Alsip, 111)and placed on the prepared teeth using finger pres-sure; all the specimens exhibited excess cement ex-pressed from all areas of the margins. Afterward, amechanical load of 5 kg for 10 minutes was appliedon each sample until the setting of the cement wasaccomplished. After the setting time had elapsed,excess cement was removed, the teeth were placedin 100% humidity at 37'C for 50 minutes, and sam-ples were kept in an incubator at 37 C in distilledwater tor 14 days.
Prior to the evaluation of microleakage, thespecimens were subjected to a thermocycling pro-
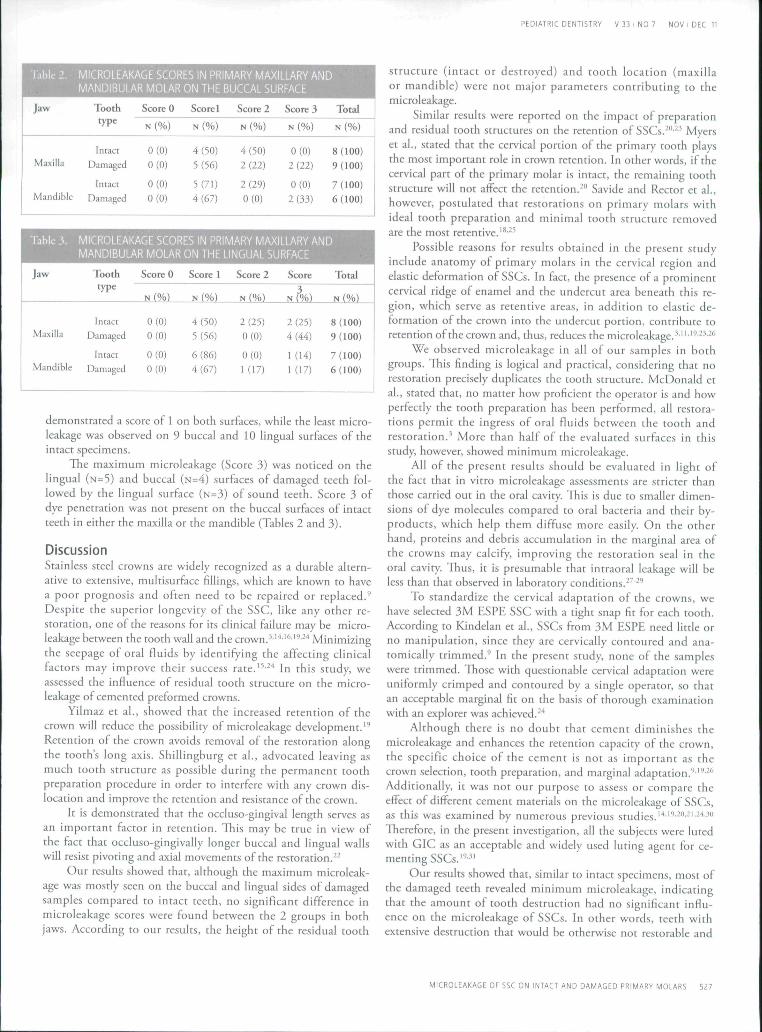
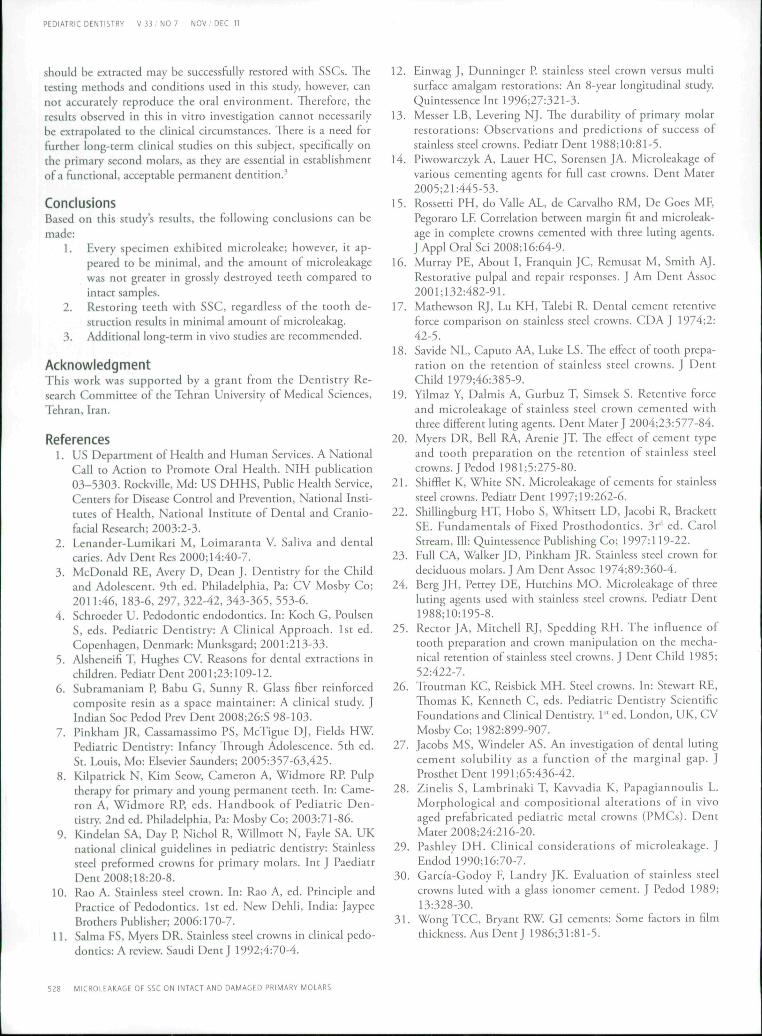
cedure of 2,000 cycles at 5°C±2 and 55°C±2 in a water bathwith a dwell time of 30 seconds and a transfer time of 20seconds. Then, the samples were immersed in a 2% méthylèneblue solution for 24 hours, rinsed under tap water, and subse-quently dried. Teeth were embedded in a slow-setting clear epoxyresin. The samples were sectioned buccolingually through thereference marks using a diamond disk (Dorsa, HLF86, Tehran,Iran). Finally, the specimens were evaluated by a stereo micro-scope at a magnification of lOOx for microleakage (Figure 2).
The following grading system was employed for microleak-age assessment: grade 0=no dye penetration; grade l=dye pene-tration < 20% of the enamel-crown interface; grade 2 = dyepenetration >20% and <50% of the enamel-crown interface;and grade 3=dye penetration >50% of the enamel-crown inter-face. Both the buccal and the lingual surfaces were evaluated ineach section.
Statistical analysis. Statistical analyses were performedusing the Mann-Whitney U and Wilcoxon signed-rank tests.The level of statistical significance was set at 0.05.
ResultsThitty primary first molars consisting of 17 maxillary and 13mandibular teeth were divided into 2 groups of the damagedand intact samples. Of the 15 intact specimens, approximately53% (N=8) belonged to the maxilla and 47% (N=7) belonged tothe mandible. Extensively destroyed teeth were 60% (N=9) and40% (N=6) from the maxilla and mandible, respectively (Table 1).
Tables 2 and 3 show the microleakage scores in primarymaxillary and mandibular first molars on the buccal and lingualsides, respectively. Statistical analysis showed no significant dif-ference between microleakage of sound and extensively cariousteeth on the buccal (^=.62) or lingual {P=.65) side. Similarmicroleakage scores were observed in primary maxillary andmandibular first molars on buccal {P=.73) and lingual (P=.63)surfaces, regardless of the degree of the desrruction.
Tables 2 and 3 show dye penetration for all surfaces. Morethan half of the restorations exhibited minimum microleakage(Score 1) in both groups. On the whole, 9 damaged teeth
Table 1 . :: NUMBER AND PERCENTAGE OF= ==;;;; ,= TEETH IN EACH GROUP
Groups
Intact
Damaged
Maxilla
N (%)
8(53)
9(60)
Mandible
N(%)
7(47)
6 (40)
struction. (a) After carfinal rooth prepararion.
mh extensive de-¡cs removal; (b) Following
Figure 2. Microleakage evaluation by a stereo-microscope (lOOx). Score 1 for buccal surfaceand Score 2 for lingual surface.
526 MICROLEAKAGE OF SSC ON INTACT AND DAMAGED PRIMARY MOLARS
PEDIATRIC DENTISTRY V 33 / NO 7 NOV I DEC 11
ÍVirtROLEAKAGE SCORES IN PRIMARY MAklLlÄRY ANDMANDIBULAR MOLAR ON THE BUCCAL SURFACE
Jaw
Maxilla
Mandible
Tooth
type
IntactDamaged
IntactDamaged
Score 0
N (%)
0(0)0(0)
0(0)0(0)
Score 1
N (%)
4(50)5(56)
5(71)4(67)
Score 2
N (%)
4(50)2(22)
2(29)0(0)
Score 3
N (%)
0(0)2(22)
0(0)
2(33)
Total
N (%)
8(100)9 (100)
7 (100)6 (100)
MICROLEAKAGE SCORES IN PRIMARY MAXILLARY ANDMANDIBULAR MOLAR ON THE LINGUAL SURFACE
Jaw
Maxilla
Mandible
Tooth
type
IntactDamaged
IntactDamaged
Score 0
N (%)
0(0)0(0)
0(0)0(0)
Score 1
N (%)
4(50)5(56)
6(86)4(67)
Score 2
N (%)
2(25)0(0)
0(0)
1 (17)
Score
2(25)4(44)
1(14)1(17)
Total
N (%)
8 (100)9(100)
7(100)6 (100)
demonstrated a scote of 1 on both surfaces, while the least micro-leakage was observed on 9 buccal and 10 lingual surfaces of theintact specimens.
The maximum microleakage (Score 3) was noticed on thelingual (N=5) and buccal (N=4) sutfaces of damaged teeth fol-lowed by the lingual surface (N=3) of sound teeth. Score 3 ofdye penettation was not present on the buccal surfaces of intactteeth in either the maxilla ot the mandible (Tables 2 and 3).
DiscussionStainless steel crowns are widely recognized as a durable altern-ative to extensive, multisutface fillings, which ate known to havea poot prognosis and often need to be repaired or replaced.''Despite the superior longevity of the SSC, like any other re-storation, one of the reasons for its clinical failure may be micro-leakage between the tooth wall and the ctown.''''•'^' '''•''' Minimizingthe seepage of otal fluids by identifying the affecting clinicalfactots may imptove their success rate.'^''' In this study, weassessed the influence of residual tooth structute on the micro-leakage of cemented preformed ctowns.
Yilmaz et al., showed that the incteased retention of thectown will reduce the possibility of microleakage development.'''Retention of the crown avoids removal of the restoration alongthe tooth's long axis. Shillingbutg et al., advocated leaving asmuch tooth structure as possible during the petmanent toothpreparation procedure in order to interfere with any crown dis-location and improve the retention and resistance of the crown.
It is demonsttated that the occluso-gingival length serves asan important factor in retention. This may be true in view ofthe fact that occluso-gingivally longer buccal and lingual wallswill resist pivoting and axial movements of the testoration."
Our results showed that, although the maximum mictoleak-age was mostly seen on the buccal and lingual sides of damagedsamples compared to intact teeth, no significant difference inmicroleakage scores were found between the 2 gtoups in bothjaws. According to out results, the height of the residual tooth
structute (intact or desttoyed) and tooth location (maxillaor mandible) were not major parametets conttibuting to themicroleakage.
Similar results were reported on the impact of preparationand residual tooth structures on the tetention of SSCs.- "' ^ Myerset al., stated that the cervical portion of the ptimary tooth playsthe most impottant tole in crown tetention. In othet words, if thecervical patt of the primary molar is intact, the remaining toothstructure will not affect the retention.*" Savide and Rector et al.,howevet, postulated that restorations on primary molars withideal tooth pteparation and minimal tooth sttuctute temovedare the most retentive.'*"
Possible teasons for results obtained in the present studyinclude anatomy of primary molars in the cervical region andelastic deformation of SSCs. In fact, the presence of a prominentcetvical tidge of enamel and the undercut atea beneath this re-gion, which serve as retentive areas, in addition to elastic de-formation of the crown into the undercut portion, contribute toretention of the crown and, thus, reduces the microleakage.'"'''•-^'•^''
We observed microleakage in all of our samples in bothgroups. This finding is logical and practical, considering that notestotation precisely duplicates the tooth sttucture. McDonald etal., stated that, no matter how proficient the operator is and howperfectly the tooth preparation has been performed, all restora-tions petmit the ingtess of oral fluids between the tooth andrestotation.' More than half of the evaluated sutfaces in thisstudy, howevet, showed minimum microleakage.
All of the present results should be evaluated in light ofthe fact that in vitro microleakage assessments are stricter thanthose cattied out in the oral cavity. This is due to smaller dimen-sions of dye molecules compared to otal bactetia and their by-products, which help them diffuse more easily. On the otherhand, proteins and debris accumulation in the matginal atea ofthe crowns may calcify, improving the testoration seal in theoral cavity. Thus, it is ptesumable that inttaotal leakage will beless than that observed in laboratory conditions.'"" '''
To standardize the cervical adaptation of the crowns, wehave selected 3M ESPE SSC with a tight snap fit for each tooth.Accotding to Kindelan et al, SSCs from 3M ESPE need litde orno manipulation, since they are cervically contotited and ana-tomically ttimmed.'' In the ptesent study, none of the sampleswere ttimmed. Those with questionable cervical adaptation wereuniformly crimped and contoured by a single operatot, so thatan acceptable marginal fit on the basis of thotough examinationwith an explorer was achieved.''*
Although there is no doubt that cement diminishes themicroleakage and enhances the tetention capacity of the ctown,the specific choice of the cement is not as important as thectown selection, tooth preparation, and marginal adaptation.''•'''••'''Additionally, it was not our purpose to assess or compare theeffect of different cement materials on the microleakage of SSCs,as this was examined by numerous previous studies.''*''-''''- '- '*™Therefore, in the present investigation, all the subjects were lutedwith GIC as an acceptable and widely used luting agent fot ce-menting SSCs.'"-"
Our results showed that, similar to intact specimens, most ofthe damaged teeth revealed minimum microleakage, indicatingthat the amount of tooth destruction had no significant influ-ence on the mictoleakage of SSCs. In other words, teeth withextensive desttuction that would be othetwise not restorable and
MICROLEAKAGE OF SSC ON INTACT AND DAMAGED PRIMARY MOLARS 527
PEDIATRIC DENTISTRY V 33 I NO 7 NOV I DEC 11
should be extracted may be successfully restored with SSCs. Thetesting methods and conditions used in this study, however, cannot accurately reproduce the oral environment. Therefore, theresults observed in this in vitro investigation cannot necessarilybe extrapolated to the clinical circumstances. There is a need forfurther long-term clinical studies on this subject, specifically onthe primary second molars, as they are essential in establishmentof a functional, acceptable permanent dentition.^
ConclusionsBased on this study's results, the following conclusions can bemade:
1. Every specimen exhibited microleake; however, it ap-peared to be minimal, and the amount of microleakagewas not greater in grossly destroyed teeth compared tointact samples.
2. Restoting teeth with SSC, regardless of the tooth de-struction results in minimal amount of microleakag.
3. Additional long-term in vivo studies are recommended.
Acknowledgmentrhis work was supported by a grant from the Dentistry Re-search Committee of the Tehran University of Medical Sciences,Tehran, Iran.
References1. u s Department of Health and Human Services. A National
Call to Action to Promote Oral Health. NIH publication03-5303. Rockville, Md: US DHHS, Public Health Service,Centers for Disease Control and Prevention, National Insti-tutes of Health, National Institute of Dental and Cranio-facial Research; 2003:2-3.
2. Lenander-Lumikari M, Loimaranta V. Saliva and dentalcaries. Adv Dent Res 2000; 14:40-7.
3. McDonald RE, Avery D, Dean J. Dentistry for the Childand Adolescent. 9th ed. Philadelphia, Pa: CV Mosby Co;2011:46, 183-6, 297, 322-42, 343-365, 553-6.
4. Schroeder U. Pedodontic endodontics. In: Koch C, PoulsenS, eds. Pédiatrie Dentistry: A Clinical Approach. 1st ed.Copenhagen, Denmark: Munksgard; 2001:213-33.
5. Alsheneifi T, Hughes CV. Reasons for dental extractions inchildren. Pediatr Dent 2001;23:109-12.
6. Subramaniam P, Babu G, Sunny R. Glass fiber reinforcedcomposite resin as a space maintainer: A clinical study. JIndian Soc Pedod Ptev Dent 2008;26:S 98-103.
7. Pinkham JR, Cassamassimo PS, McTigue DJ, Fields HW.Pédiatrie Dentistry: Infancy Through Adolescence. 5th ed.St. Louis, Mo: Elsevier Saunders; 2005:357-63,425.
8. Kilpatrick N, Kim Seow, Cameron A, Widmore RP Pulptherapy for primary and young permanent teeth. In: Came-ron A, Widmore RP, eds. Handbook of Pédiatrie Den-tistry 2nd ed. Philadelphia, Pa: Mosby Co; 2003:71-86.
9. Kindelan SA, Day P, Nichol R, Willmott N, Fayle SA. UKnational clinical guidelines in pédiatrie dentistry: Stainlesssteel preformed crowns for primary molars. Int J PaediatrDent 2008; 18:20-8.
10. Rao A. Stainless steel crown. In: Rao A, ed. Principle andPractice of Pedodontics. 1st ed. New Dehli, India: JaypeeBrothers Publisher; 2006:170-7.
11. Salma FS, Myers DR. Stainless steel crowns in clinical pedo-dontics: A review. Saudi DentJ 1992;4:70-4.
12. Einwag J, Dunninget P. stainless steel crown versus multisurface amalgam restorations: An 8-year longitudinal study.Quintessence Int 1996;27:321-3.
13. Messer LB, Levering NJ. The durability of primary molarrestorations: Observations and predictions of success ofstainless steel crowns. Pediatr Dent 1988;10:81-5.
14. Piwowarczyk A, Lauer HC, Sorensen JA. Microleakage ofvarious cementing agents for full cast crowns. Dent Mater2005;21:445-53.
15. Rossetti PH, do Valle AL, de Carvalho RM, De Goes MF,Pegoraro LF. Correlation between margin fit and microleak-age in complete crowns cemented with three luting agents.J Appl Oral Sei 2008; 16:64-9.
16. Murray PE, About I, Franquin JC, Remusat M, Smith AJ.Restorative pulpal and repair responses. J Am Dent Assoc2001;132:482-91.
17. Mathewson RJ, Lu KH, Talebi R. Dental cement retentiveforce comparison on stainless steel crowns. CDA J 1974;2:42-5.
18. Savide NL, Caputo AA, Luke LS. The effect of tooth prepa-ration on the retention of stainless steel crowns. J DentChild 1979;46:385-9.
19. Yilmaz Y, Dalmis A, Gurbuz T, Simsek S. Retentive forceand microleakage of stainless steel crown cemented withthree different luting agents. Dent Mater J 2004;23:577-84.
20. Myers DR, Bell RA, Arenie JT. The effect of cement typeand tooth preparation on the retention of stainless steelcrowns. J Pedod 1981;5:275-80.
21. Shifflet K, White SN. Mictoleakage of cements for stainlesssteel crowns. Pediatr Dent 1997; 19:262-6.
22. Shillingburg HT, Hobo S, Whitsett LD, Jacobi R, BrackettSE. Fundamentals of Fixed Prosthodontics. 3r'' ed. CarolStream, 111: Quintessence Publishing Co; 1997:119-22.
23. Full CA, Walker JD, Pinkham JR. Stainless steel crown fordeciduous molars. J Am Dent Assoc 1974;89:360-4.
24. Berg JH, Pettey DE, Hutchins MO. Microleakage of threeluting agents used with stainless steel crowns. Pediatr Dent1988;10:195-8.
25. Rector JA, Mitchell RJ, Spedding RH. The influence oftooth preparation and crown manipulation on the mecha-nical retention of stainless steel crowns. J Dent Child 1985;52:422-7.
26. Troutman KC, Reisbick MH. Steel crowns. In: Stewart RE,Thomas K, Kenneth C, eds. Pédiatrie Dentistry ScientificFoundations and Clinical Dentistry. 1" ed. London, UK, CVMosby Co; 1982:899-907.
27. Jacobs MS, Windeier AS. An investigation of dental lutingcement solubility as a function of the marginal gap. JProsthet Dent 1991;65:436-42.
28. Zinelis S, Lambrinaki T, Kavvadia K, Papagiannoulis L.Morphological and compositional alterations of in vivoaged prefabricated pédiatrie metal crowns (PMCs). DentMater 2008;24:216-20.
29. Pashley DH. Clinical considerations of mictoleakage. JEndod 1990; 16:70-7.
30. Garcia-Godoy F, Landry JK. Evaluation of stainless steelcrowns luted with a glass ionomet cement. J Pedod 1989;13:328-30.
31. WongTCC, Bryant RW. GI cements: Some factors in filmthickness. Aus DentJ 1986;31:81-5.
528 MICROLEAKAGE OF SSC ON INTACT AND DAMAGED PRIMARY MOLARS

Copyright of Pediatric Dentistry is the property of American Society of Dentistry for Children and its content
may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express
written permission. However, users may print, download, or email articles for individual use.





























