Embed Size (px)
DESCRIPTION
Microcirculation: introduction. 1) Capillaries are the site of diffusion of nutrients and waste between blood and tissue 2) Transcapillary exchange of fluid Maintains p lasma & interstitial flluid Volume Opposes edema formation ( Capillary Starling forces) Lymphatic structure & function - PowerPoint PPT Presentation
Citation preview

Microcirculation: introduction
1) Capillaries are the site of diffusion of
nutrients and waste between blood and tissue
2) Transcapillary exchange of fluid
Maintains plasma & interstitial flluid
Volume
Opposes edema formation ( Capillary
Starling forces)
Lymphatic structure & function
Edema formation

Microvascular unit
Arteriole
Venule
Metarteriole
Capillaries Arteriovenous shunt (S)
Pre-capillary sphincters exist at the origin of each capillary

Structures in the microcirculation
StructureSmooth Muscle Innervated Function Control
Arteriole Yes Yes Resistance Local & neural
Metarteriole Sparse Occasionally Resistance Local
Precapillary sphincter Yes No Resistance Local
Capillary No No Exchange None (passive)
Venule Yes Yes Capacitance Neural

Capillary Structure
Capillaries:
Site of exchange by diffusion (some diffusion occurs in venules also).
Capillary walls are porous to small molecules:
Intercellular clefts
Fused vesicle channels

The Permeability Surface area term for diffusion across a capillary wall
The rate of diffusion of a molecule is proportional to area & concentration gradient, &
inversely proportional to distance:
n = amount, t = time, D = diffusion coefficient, A = area, dC = concentration gradient,
dx = distance.
dx
dCAD
dt
dn
Applied to the circulation, the equation for diffusion of molecules across the capillary
wall is:
Where P is permeability of the capillary & S is surface area. Under most conditions P
is constant & determined by the structure of the capillary wall.
Physiologically, the area S available for diffusion can be increased by recruiting more
capillaries, which also decreases the distance (shorter intercapillary distance).
dx
dCSP
dt
dn

Transcapillary exchange of lipid soluble substances
Lipid soluble substances such as CO2, O2 & many anesthetics penetrate the capillary
wall by diffusing via the lipid component of the endothelial cell membranes.
Capillary area for diffusion of lipid soluble molecules is maximal.
Transcapillary movement of macromolecules & cells
Molecules > 40 A can be transported across the endothelium by pinocytosis.
Leucocytes & lymphocytes migrate through intercellular clefts by ameboid movement.

Transcapillary exchange of water soluble substances
H2O, monosaccharides, amino acids, small peptides & organic acids and inorganic ions (Na+, K+, Ca++, etc) diffuse rapidly through intercellular clefts.
The area for diffusion of water soluble molecules is less than for lipid soluble molecules.
Capillaries have two types of endothelium:
Discontinuous endothelium capillaries have large clefts & gaps in basement membrane, relatively high permeability.
Continuous endothelium: basement membrane is continuous, intercellular clefts are ~ 40 angstroms diameter & have tight junctions. Molecules larger than 40 A, like proteins, cannot cross the wall by diffusion.
Continuous endothelium (muscle, skin, lung, CNS)
Discontinuous endothelium (liver, spleen, glomerulus, small intestine, endocrine glands, bone marrow)

Flow & diffusion limits on exchange`
Flow limited exchange: exchange of molecules that diffuse rapidly is limited by the rate of blood flow (examples: H2O and small molecules)
Diffusion limited exchange: exchange limited by diffusion because either
The molecules diffuse slowly (macromolecules) or
Diffusion distances are large
flowFlow-limited; Diffusion is rapid
flowDiffusion limited;
Diffusion is slow
With edema increased diffusion distance may limit supply of nutrients to tissues
Transcapillary exchange of fluid impacts plasma & interstitial fluid volumes
Total body water content is maintained nearly constant by control mechanisms that operate through thirst (input) and kidney function (output)
Total body water can be divided into
Extracellular fluid (ECF)
Plasma
Interstitial fluid including lymph
Intracellular fluid (ICF)
The distribution of fluid between plasma and interstitium depends on:
1. Osmotic pressure due to plasma proteins
2. Capillary hydrostatic pressure
3.Osmotic pressure due to proteins in interstitial fluid
4. Interstitial fluid hydrostatic pressure
(These are the Starling Forces)
Imbalances in these factors may produce edema & decrease blood volume.
Edema is “a palpable swelling produced by expansion of the interstitial fluid volume.”

Osmosis
Osmotic pressure is pressure created by a difference in solute
concentration across a semi-permeable membrane.
Osmosis is the passive diffusion of water from a region of low solute
concentration (dilute solution, low osmotic pressure) to a region of high
solute concentration (concentrated solution, high osmotic pressure).
Osmotic pressure due to protein molecules is called oncotic pressure.
Definition of an osmole
Osmotic Pressure depends on the concentration of particles in a solution..
An osmole is a unit that refers to the total number of particles dissolved in a solution. One osmole = 6.02 x 1023 particles (Avogadro’s number).
One gram molecular weight of glucose dissolved in water will liberate one osmole of particles.
One mole of NaCl dissolved in water will yield two osmoles (Na+ and Cl-) of particles.
One osmole of glucose in one liter of water will yield a one osmolar solution.
Osmolarity is the number of osmoles/liter of solution.
Osmolality is the number of osmoles/kilogram of solvent.
The difference between osmolarity & osmolality for biological solutions is insignificant.

Normal plasma osmolality
Plasma solutes, millimoles/liter
Cations Anions
Na+ 135 Cl- 108
K+ 3.5 HCO3- 24
Ca++ 2 Lactate 1
Sum 140.5 Albumin 0.6
Sum 133.6
Glucose 5
Urea 5
Grand total 284.1
mM = millimole = 1/1000th of a molemOsm = milliosmole = 1/1000th of an osmoleNormal plasma osmolality = 280 to 296 mOsm/liter

Starling forces in capillaries
OUT IN
F = K [(Pcap + i) – (Pi + cap)]
F = net movement of fluid across the capillary wall (ml/min)
Pc ap = capillary hydrostatic pressure (mmHg)
cap = capillary oncotic pressure* (mmHg)
Pi = interstitial fluid hydrostatic pressure (mmHg)
I = interstitial fluid oncotic pressure (mmHg)
K = filtration constant: (determined by capillary surface area and permeability to water (ml/min)/mmHg)
*oncotic pressure = osmotic pressure due to proteins

Calculation of net filtration pressure
F = K [(Pcap + i) – (Pi + cap)]
net filtration pressure
F ~ Pcap – cap
Blood flow
Pc ap = 37 mm Hg
i= 0 Pi = 1 mm Hg
cap = 25 mm Hg
Arterial end: Pcap > cap
Net filtration pressure = (37 + 0) - (1 + 25) = 11 mm Hg
Venous end: Pcap < cap
Net filtration pressure = (17 + 0) - (1 + 25) = - 9 mm Hg
Pcap =17 mm Hg
cap = 25 mm Hg
i= 0 Pi = 1 mm Hg
Negative value for net filtration pressure indicates net force favors absorption
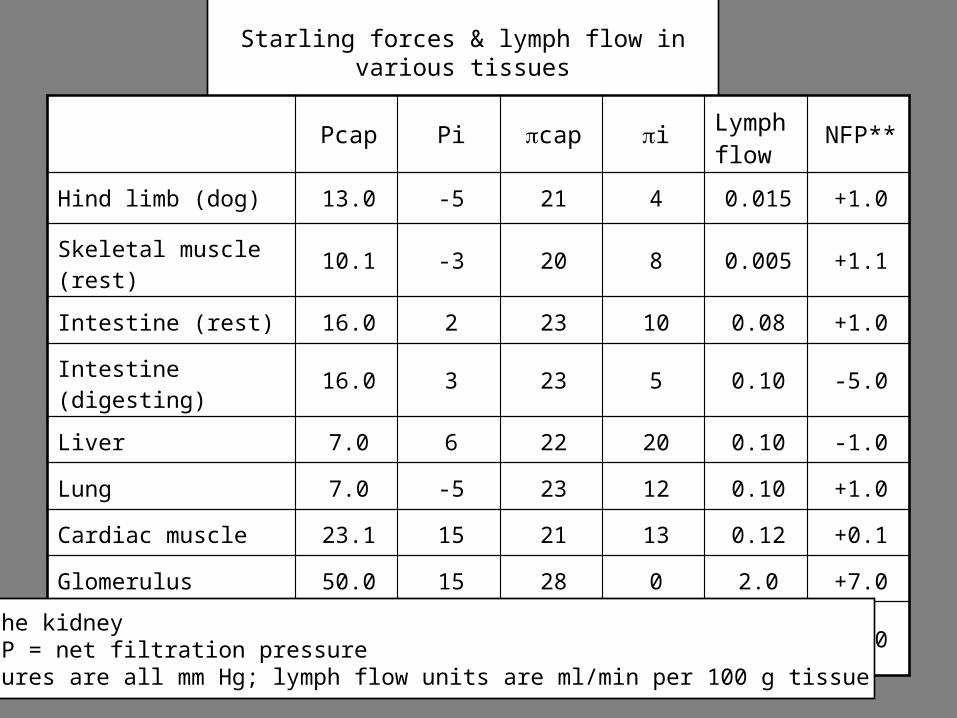
Starling forces & lymph flow in various tissues
Pcap Pi cap i Lymph flow
NFP**
Hind limb (dog) 13.0 -5 21 4 0.015 +1.0
Skeletal muscle (rest) 10.1 -3 20 8 0.005 +1.1
Intestine (rest) 16.0 2 23 10 0.08 +1.0
Intestine (digesting) 16.0 3 23 5 0.10 -5.0
Liver 7.0 6 22 20 0.10 -1.0
Lung 7.0 -5 23 12 0.10 +1.0
Cardiac muscle 23.1 15 21 13 0.12 +0.1
Glomerulus 50.0 15 28 0 2.0 +7.0
Peritubular capillary* 25.0 7 32 7 2.0 -7.0
*in the kidney** NFP = net filtration pressurePressures are all mm Hg; lymph flow units are ml/min per 100 g tissue

Factors that influence lymph flow
Lymph flow is increased by
Interstitial hydrostatic pressure
Lymphatic contractions (smooth muscle) & valves
Sympathetic stimulation of lymph vessels
Skeletal muscle pump

Lymphatic circulation
systemic capillaries
Venous system
Interstitial fluid
Filtration 20 liters/day
Absorption 16 to 18 liters/day
Lymph flow2 to 4 liters/day
systemic arteries
Right heartPulmonary circulation
Left heart
2 to 4 liters of fluid per day is filtered out of the capillaries, taken up by the lymphatics and returned to the systemic circulation.
Terminal lymphatics are highly permeable to protein
Lymphatics are the only route for return to circulation of protein that leaves capillaries

Arteriolar Tone and Capillary Hydrostatic Pressure
Arteriolar constriction decreases Pcap
Arteriolar dilation increases Pcap
Changes in PCap will affect filtration & absorption
Effect on mean arterial pressure:
MAP = CO x TPR
Constriction of arterioles in one organ or tissue may be offset by dilation elsewhere, without causing a change in TPR and MAP
Widespread arteriolar constriction in many tissues will increase TPR and MAP (if CO doesn’t change).
Arterial pressure Capillary hydrostatic pressure
dilation
constriction
CapillaryArtery Arteriole

Absorption of interstitial fluid into the circulation compensates in hemorrhage
MAP = CO x TPR
Hemorrhage
sympathetic nerve activity
heart rate cardiac contractility
Restore MAP
TPR
Cardiovascular reflexes
hypotension
absorption of fluid into capillaries
Restore blood volume
CO
Vasoconstriction(skin, kidney, GI tract)
capillary hydrostatic pressure
hematocrit

Three physiological roles of arteriolar tone
Support arterial blood pressure
Direct distribution of flow between organs & tissues
Influence capillary filtration & absorption

Edema safety factors
Capillary hydrostatic pressure, mm Hg
30
Lym
ph
flow
B
30
Pi,
mm
Hg
C
30
(c
ap -
i)
, mm
H
g
A
A: As capillary hydrostatic pressure & filtration increase, tissue protein is diluted, i decreases, so cap - i increases, limiting further filtration.(The y-axis in panel A is cap - I, the oncotic pressure gradient influencing filtration)
B: As filtration increases, lymph flow increases, limiting accumulation of fluid in the interstitium.
C: As filtration increases, fluid added to the interstitium increases Pi, decreasing the hydrostatic pressure gradient favoring filtration (Pcap – Pi)

Edema formation
Edema is a pathological accumulation of excess fluid in the interstitial space
Causes of edema:
Decreased plasma oncotic pressure
Kidney disease urinary excretion of plasma protein
Liver disease inadequate albumin synthesis
Increased capillary permeability to proteins
Tissue trauma
Anaphylactic shock
Increased venous & capillary hydrostatic pressure
Congestive heart failure
Blockage of lymphatics
Tumors
Parasites