-
8/12/2019 [MICROA - 2.1] Myeloid Tissue Histology
1/6
2.1 MYELOID TISSUE HISTOLOGY
LECTURER: Dennis Ivan U. Bravo, MD
DATE: 15 July 2014FEU-NRMF Institute of Medicine
Batch 2018
Outline:
Review of bone and BM histology
Erythropoiesis
Granulopoeisis
Platelet formation
Clinical Correlation
REVIEW OF BONE
FUNCTION OF BONE
Support for soft tissues and the attachment site
for tendons.
Because the bone is very hard, It protects the
soft internal organs like your brain. It is
protected from the external environment by the
very hard skull.
In combination with the muscle, it is responsible
for locomotion.
The bone also has a biochemical function. It
stores mineral (e.g. calcium and phosphates)and
is released whenever theres a need for them.
Blood cell production. It also has another
biological function, which is to produce the cells
that are found in the blood.
Triglyceride storage. It stores triglyceride in the
form of yellow marrow.
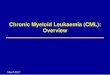
Explanation: This is a cross-section of a bone showing you
two types. The one in the surface is the CORTICAL
(Compact) BONE. So if its enlarged, you can see that its
made up of units known as OSTEON and in the center,
you will find the HAVERSIAN CANAL and the ones
concentrically arranged around it are the OSTECYTES.
Pointed above is the TRABECULAR (Spongy) BONE. The
trabecular bone itself is not in the picture but its
actually
the marrow which fills the spaces within the trabecular
bone.
HISTOLOGY OF BONE MARROW
TYPES OF BONE MARROW (OVERVIEW)
Red Marrow Actively involved in
hematopoeisis.
o
Contents: Stem Cells, Progenitor Cells
Developing Erythroblasts, Myeloblasts
and Megakaryoblasts.o Highly cellular. The spaces are filled
with
actively dividing hematopoietic cells.
Yellow Marrow storage site for adipocytes.
o
Contents: Adipose cells (varies with age
and activity)
Note: Both marrows contain a lot of dilated capillaries
Theres a wide network of capillaries present in the
marrow.
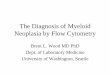
YELLOW MARROW
Located on long bonesof adults. (e.g. femur)
Highly infiltrated with
fat.
Not hematopoietic
under normal
conditions. But it has a
potential to become when theres a need fo
extra hematopoietic cell.
1 | P a g e M I C R O H S B A
-
8/12/2019 [MICROA - 2.1] Myeloid Tissue Histology
2/6
2.1 MYELOID TISSUE HISTOLOGY
LECTURER: Dennis Ivan U. Bravo, MD
DATE: 15 July 2014FEU-NRMF Institute of Medicine
Batch 2018
Explanation: This is how it looks like under a microscope.
The yellow marrow is composed of spaces between
trabecular bones and is filled with several adipose cells.
The adipose cells are filled with triglycerides.
RED MARROW
Located in the epiphysis of long bones, flat,
irregular, and short bones. (e.g. Sternum)
Highly vascular with large dilated venous sinuses
and surrounding them are the active
hematopoietic cells.
Explanation: The red marrow is filled with several venous
sinuses, arising from an artery. The green-colored objects
are the RETICULAR FIBERS, which provides support to the
hematopoietic cells.
Explanation: The clusters of solid blue cells are the
ERYTHROPOIETIC CELLS. The clusters of granulated blue
cells are the GRANULOPOIETIC CELLS. The white space
filled with RBCs is the VENOUS SINUS. It is normal to find
adipose cells. The distribution for adults is 50%
hematopoietic cells and the remaining 50% are adipose
cells.
Explanation: There is a prominent VENOUS SINUS filled
with RBCs. Surrounding them will be the
HEMATOPOIETIC CELLS, specifically ERYTHROPOIETIC
CELLS. A large cell is also present here known as the
MEGAKARYOCYTE.
Amount of red marrow varies according to the
patients age.
o
Childhood:
Virtually present in all bones o
the body.
It is composed of hematopoietic
cells. Virtually no adipose cells
are found.
o
Adults:
Reduced to 50%
Present in the sternum, ribs
pelvis and skull.
o 70 years:
Reduced to 30%
ERYTHROPOIESIS
Pluripotent Stem Cell Blast Cells Proerythroblast
Basophilic Erythroblast Polychromatic Erythroblast
Orthochromatic Erythroblast Reticulocyte
Erythrocyte
2 | P a g e M I C R O H S B A
-
8/12/2019 [MICROA - 2.1] Myeloid Tissue Histology
3/6
2.1 MYELOID TISSUE HISTOLOGY
LECTURER: Dennis Ivan U. Bravo, MD
DATE: 15 July 2014FEU-NRMF Institute of Medicine
Batch 2018
HOW DO WE DISTINGUISH ERYTHROPOIETIC CELLS?
FROM OTHER HEMATOPOIETIC CELLS
o As a group, they do not have any
prominent granules in contrast to the
developing myelocytes.
o
The nucleus, whether small or large, is
consistently round when its still present.
In contrast to the developing WBCs
where the shape of the nucleus varies
according to stage of its development.
FROM EACH STAGE
o
Cell sizeo Subtle differences in the nucleus
o Color of the cytoplasm
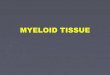
TREND IN THE DEVELOPMENT OF RBCs
Explanation: If the cell develops from young to mature,
youll notice a change in the nucleus. Initially, it is big
it
becomes smaller until eventually disappears. There is a
PROGRESSIVE CONDENSATION of the nucleus.
Another trend is that there is a change from Basophilic to
Eosinophilic. Initially, there is no haemoglobin. But
eventually, an accumulation of haemoglobin will be
present as the cell progress thereby giving it its
eosinophilic quality. Since there is absence ofhaemoglobin
during the early stage of erythropoiesis,
there is a production of RNA present. These RNA will
contribute to the production of RIBOSOMES. This gives
the cell its basophilic characteristics. The RNA and
ribosome are the ones involved in protein synthesis,
namely haemoglobin.
There is also a progressive reduction in the size of the
cell. It initially starts with a large cell and as it
matures,
the cell is now smaller.
STAGES OF ERYTHROPOIESIS
BLAST CELL
o The origin of erythropoietic cells.
o Cannot be distinguished from the blas
cells of myelocytes series.
o
Mitotically active (It divides).
o No granules.
PROERYTHROBLAST
o
Cell is large.
o Mitotic.
o Positive nucleoli (w/c means that its
actively involved in synthesis of RNA).o Basophilic
cytoplasm.
BASOPHILIC ERYTHROBLAST
o
The nucleolus has disappeared (w/c
means the synthesis of RNA has
stopped).
o
Intensely basophilic because o
ribosomes.
POLYCHROMATIC ERYTHROBLAST
o
Smaller than its precursor.o The nucleus is starting to
condense
thats why it has a checkerboard
appearance (Writes stain).
o
Gray-green cytoplasm because o
haemoglobin accumulation.
ORTHOCHROMATIC ERYTHROBLAST
o Aka Normoblast
o Smaller pyknotic nucleus (about to be
extruded)
o
Pink cytoplasm due to haemoglobin
accumulation.
RETICULOCYTE
o No nucleus (already extruded)
o Pink/orange color (because of the
haemoglobin) with bluish hue (due to
remaining ribosomes).
o
Named such because of cresyl blue
They seem to have a network-like
appearance.
3 | P a g e M I C R O H S B A
-
8/12/2019 [MICROA - 2.1] Myeloid Tissue Histology
4/6
2.1 MYELOID TISSUE HISTOLOGY
LECTURER: Dennis Ivan U. Bravo, MD
DATE: 15 July 2014FEU-NRMF Institute of Medicine
Batch 2018
IN SUMMARY:
Decrease in basophilia
Increase in haemoglobin concentration
Decrease in cell volume
Increase in chromatin condensation, followed by
extrusion of a pyknotic nucleus
GRANULOPOIESIS
All granulocytes arise from a single MYELOBLAST which
came from a UNIPOTENT STEM CELL. The development of
all types of myelocytes follows the same stages.
HOW DO WE DISTINGUISH GRANULOPOIETIC CELLS?
FROM OTHER HEMATOPOIETIC CELLS
o
Consistently contain granules
o
When clustered as a group, they appear
DIRTY together.
FROM EACH STAGES
o Type of granule present
o Appearance of the nucleus
STAGES OF GRANULOPOIESIS
PROMYELOCYTE
o
First identifiable WBC precursor.
o Contains purple-staining azurophilic
nonspecific granules.
o Cell is large.
o
Nucleus is large.
o Nucleolus is prominent.
MYELOCYTE
o
Distinguished once the lilac-staining
specific granules start appearing ove
the purple-staining azurophilic
nonspecific granules.o Wide range in cell size.
o Frequently indented round nucleus.
METAMYELOCYTE
o The primary granules will start to
disappear and the secondary granules
will predominate.
o Nucleus becomes flattened.
BAND
o
The nucleus will become morecondensed. Eventually, it will
become
U-shaped or horseshoe-shaped.
GRANULOCYTE
o The nucleus becomes segmented into
lobes.
IN SUMMARY:
4 | P a g e M I C R O H S B A
-
8/12/2019 [MICROA - 2.1] Myeloid Tissue Histology
5/6
2.1 MYELOID TISSUE HISTOLOGY
LECTURER: Dennis Ivan U. Bravo, MD
DATE: 15 July 2014FEU-NRMF Institute of Medicine
Batch 2018
Myeloblast = No cytoplasmic granules
Promyelocyte = appearance of Primary Granules
Myelocyte = appearance of Secondary granules
Metamyelocyte = Abundance of Secondary
granules and dispersed Primary Granules
Band = Nucleus will become horseshoe-shaped
Granulocyte = Nucleus is segmented
PLATELET FORMATION
OVERVIEW: Consist of 3 stages and it arose from the
Unipotent Stem Cell. It will divide to form the
MEGAKARYOBLAST. The megakaryoblast will undergo
ENDOMITOSIS to form MEGAKARYOCYTE. And the
megakaryocyte will fragment to form the platelet.
STAGES OF PLATELET FORMATION
MEGAKARYOBLAST
o
Large cell with single large-lobed
nucleus.
o Basophilic non-granular cytoplasm.
o
It will undergo ENDOMITOSIS (nucleusis doubled up but doesnt
undergo
division).
o RARE
MEGAKARYOCYTE
o Extremely large cell with single, large
POLYPLOID nucleus.
o
Lies just outside the sinusoids.
o Fragments to platelets.
o Sheds platelets.
o
They are found near the sinusoidsbecause they form PSEUDOPODS
that
fragments to form platelets goes
directly to the sinusoids to join the
bloodstream or circulation right away.
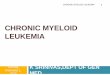
CLINICAL CORRELATION
ACUTE MYELOGENOUS LEUKEMIA
LEUKEMIA the uncontrolled proliferation of the
myelocyte.
ACUTE MYELOGENOUS LEUKEMIA the uncontrolled
proliferation of UNDIFFERENTIATED MYELOBLAST.
COMPARISON:
Bone Marrow w/ AML
o
Highly cellular
o
Everythings obliteratedo Absence of erythropoietic cells
o Abundance of myeloblastic cells
o
Absence of fats
o Absence of platelet forming cells
o
Obliteration of marrow space with tumor
cells
SYMPTOMS (Purely based on the slides):
Increased WBC
o
Caused by the abundance in myeloblast
but are immature and non-functional.
Infection
o WBCs are non-functional
Anemia
o
Obliteration of erythropoietic cells
Bleeding
o
Obliteration of platelet forming cells
Pain
o
Since it is growing in the confined space
of the bone
5 | P a g e M I C R O H S B A
-
8/12/2019 [MICROA - 2.1] Myeloid Tissue Histology
6/6
2.1 MYELOID TISSUE HISTOLOGY
LECTURER: Dennis Ivan U. Bravo, MD
DATE: 15 July 2014FEU-NRMF Institute of Medicine
Batch 2018
John Henry Caas, ECT
07-20-14
6 | P a g e M I C R O H S B A