Michael W Rich, MD Professor of Medicine Washington University School of Medicine St. Louis,...
75
Heart Rhythm Disorders in Older Adults Michael W Rich, MD Professor of Medicine Washington University School of Medicine St. Louis, Missouri Disclosures: None
Michael W Rich, MD Professor of Medicine Washington University School of Medicine St. Louis, Missouri Disclosures: None
Michael W Rich, MD Professor of Medicine Washington University
School of Medicine St. Louis, Missouri Disclosures: None
Slide 2
Outline Effects of aging on the cardiac conduction system
Bradyarrhythmias and pacemakers Supraventricular arrhythmias: Focus
on atrial fibrillation Ventricular arrhythmias: Focus on ICDs
Research directions: Unmet needs
Slide 3
Effects of Aging on the Cardiac Conduction System Sinus node
Progressive decline in number of pacemaker cells (
Criteria for ICD Implantation Class I indications: NYHA class
II-III symptoms LVEF 30-35% Life expectancy > 1 year Good
functional status ACC/AHA/HRS Guidelines for Device-Based Therapy J
Am Coll Cardiol 2008;51:e1-e62
Slide 42
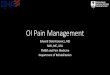
ICDs in Patients 75 Years: Pooled Results from AVID, CASH, and
CIDS Eur Heart J 2007;28:1746-9 N=252
Slide 43
Age and Effectiveness of ICDs for Primary Prevention of SCD:
Meta-analysis of RCTs 5783 pts from 5 RCTs (MADIT-II, DINAMIT,
DEFINITE, SCD-HeFT, IRIS) 44% elderly (defined as age 60-65 yrs)
Mean follow-up: 32 months Impact of ICD therapy on all-cause
mortality: Younger pts: HR 0.65 (95% CI 0.50-0.83, p < 0.001)
Older pts: HR 0.81 (95% CI 0.62-1.05, p = 0.11) Exclusion of
DINAMIT and IRIS did not change results Ann Intern Med 2010;
153:592-9
Slide 44
ICD Considerations in Older Adults With increasing age, the
relative likelihood of dying from VT/VF decreases, while the
likelihood of dying from worsening HF, MI, or other non-cardiac
causes increases The risk for inappropriate shocks may be higher in
older adults due to increasing incidence of AF/RVR Procedural
complications increase with age, esp. after 80 yrs Therefore, the
benefit/risk ratio of ICD implantation decreases with age Routine
generator replacement at end of battery life is not warranted and
must be considered on an individual basis
Slide 45
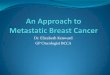
ICDs Implanted in US: 1995-2008 Age at ImplantNumber% of total
Under 201,2900.6 20-292,2501.0 30-395,4502.4 40-4916,5007.2
50-5939,10017.0 60-6963,15027.6 70-7974,35032.4 80-8924,60010.7
90-996650.3 100 and over100.0 Unknown1,8500.8 Total229,215100.0
43.4%
Slide 46
ICDs and End-of-Life Care Terminally ill patients with
previously implanted ICDs often receive 1 or more shocks in the
last 30 days of life Given the choice, many patients and families
prefer disabling the ICD to allow a natural death rather than
suffering unwanted shocks (but this almost never happens!) Device
disablement is consistent with patient autonomy (the right to
refuse treatment) and is considered legal and ethical in all states
All patients with ICDs should be asked about preferences for device
disablement in the event of terminal illness Heart Rhythm
2010;7:1008-26
Slide 47
Research Directions: Unmet Needs Effects of aging on the
conduction system Elucidate mechanisms Develop interventions for
attenuating age-related effects Bradyarrhythmias and pacemakers
Prevention of age-associated bradyarrhythmias Pacemaker selection
and mode optimization Novel therapies (e.g. stem cells, other
devices) Atrial fibrillation Primary prevention Develop safer and
more effective anti-thrombotic and anti-arrhythmic agents Define
role of AF ablation and other interventions (e.g. LAA occluders)
Ventricular arrhythmias and ICDs Patient selection (i.e. improved
risk stratification) Refine criteria for generator replacement
Enhance communication about risks/benefits Incorporate patient
preferences and goals of care into decision-making
Slide 48
Question 1 All of the following changes in the cardiac
conduction system occur with normal aging EXCEPT: A.Marked decrease
in the number of functioning sinus node pacemaker cells B.Impaired
conduction from the sinus node to the atrial conduction system C.
Gradual decline in resting heart rate D. Slowing of conduction
through the AV node E.Increased prevalence of both left bundle
branch block and right bundle branch block
Slide 49
Question 2 All of the following statements about atrial
fibrillation in older adults are true EXCEPT: A.More than 50% of
all patients in the U.S. with atrial fibrillation are 75 years of
age B.The incidence of atrial fibrillation is higher in older women
than in older men C.The proportion of ischemic strokes attributable
to atrial fibrillation increases exponentially with age D.In older
patients with atrial fibrillation, the risk of stroke is higher in
women than in men E.In most cases, high fall risk is not a
contraindication to warfarin in older adults with atrial
fibrillation
Slide 50
Question 3 All of the following statements about implantable
cardioverter- defibrillators (ICDs) in patients 80 years of age or
older are true EXCEPT: A.The efficacy of ICDs in terminating
life-threatening ventricular tachyarrhythmias declines with
increasing age (esp. after age 80) B.Compared to younger patients,
older patients with ICDs are at increased risk for inappropriate
shocks (i.e. in the absence of a life-threatening ventricular
tachyarrhythmia) C.ICDs have been shown to reduce mortality in
appropriately selected octogenarians D.It is legal and ethical for
a physician to disable an ICD in an older patient approaching the
end-of-life E.In the absence of shocks (appropriate or
inappropriate), ICDs have minimal impact on quality of life in
older adults
Slide 51
Slide 52
Am J Cardiol 1996;77:1185-90
Slide 53
Epidemiology of AF in the U.S. Most common arrhythmia in
clinical practice Estimated 2.5 million Americans affected Accounts
for ~ 1/3 of hospitalizations for heart rhythm disorders 66%
increase in hospitalizations for AF over the past 20 yrs Annual
cost/pt ~ $3600 (total cost ~ $9 billion) AF is associated with ~
10-15% increase in mortality in men, ~ 20-25% increase in women
Median age 75 yrs, ~ 50% women (60% after age 75)
Slide 54
Epidemiology of AF in the U.S. Prevalence: 2.7 million, with
projected increase to 5.5-6 million by 2050 due to population aging
Incidence > 75,000 new cases per year Incidence & prevalence
increase progressively with age Incidence is higher in men than in
women, but women comprise over 50% of cases 66% increase in
hospitalizations for AF over the past 20 yrs Annual cost/pt ~ $3600
(total cost ~ $9 billion) AF is associated with ~ 10-15% increase
in mortality in men, ~ 20-25% increase in women Circulation
2011;123:e18-e209
Slide 55
Incidence of Atrial Fibrillation: The Framingham Heart Study Am
J Cardiol 1998;82(8A):2N-9N
Slide 56
Age-Related CV Changes that Increase AF Risk Increased arterial
stiffness ( systolic BP) Increased myocardial stiffness and
impaired relaxation (altered diastolic filling, LVEDP) Increased LA
size and fibrosis Degenerative changes in the conduction system,
esp. SA node (sick sinus; tachy-brady)
Slide 57
Co-existing Conditions that Increase AF Risk Hypertension
Coronary artery disease Valve disease (esp. AS & MR) Pulmonary
disease Subclinical hyperthyroidism
Slide 58
Warfarin vs. Aspirin: SPAF-II Subgroup Analysis by Age Lancet
1994;343:687-691 P=0.39 Among patients > 75 yrs (N=385)
all-cause CVA with residual deficit occurred in 4.6% of pts on
warfarin vs. 4.3% of pts on aspirin.
Slide 59
BAFTA: Subgroup Analysis Lancet 2007;370:493-503
Slide 60
Incidence of Major Extracranial Bleeding in 13,559 Patients
with Atrial Fibrillation J Am Geriatr Soc 2006;54:1231-1236
Slide 61
Incidence of Intracranial Hemorrhage in 13,559 Patients with
Atrial Fibrillation J Am Geriatr Soc 2006;54:1231-1236
Slide 62
Risk of Major Bleeding Events in Patients at High vs. Low Risk
for Falls Am J Med 2012;125:773-8 Prospective study of 515 pts on
oral anticoagulants Median 71.2 yrs, 64% male High fall risk: 59.8%
Follow-up: 12 mo Incidence of major bleeds: 7.5 per 100 pt-yrs
Predictors of major bleeds: female, # of medications AHR: 1.09
(o.54-2.21)
Slide 63
In NVAF, what may matter most to patients is not the risk of
stroke or bleeding but rather the risks of functional and cognitive
disability. Arch Intern Med 2010;170:566-569
Slide 64
Emerging Therapies for Atrial Fibrillation Dronedarone -
ATHENA: N Engl J Med 2009;360:668-78 - Similar results in pts <
75 and 75 Dabigatron (direct thrombin inhibitor) - RE-LY: N Engl J
Med 2009;361:1139-51 - No subgroup analysis by age Aspirin +
clopidogrel (vs. aspirin alone) - ACTIVE-A: N Engl J Med 2009;
360:2066-78 - No benefit in pts 75
Slide 65
ACTIVE-A Study Design 7554 pts with AF, increased stroke risk,
and contraindications to vitamin K antagonists Mean age 71 yrs, 42%
female, mean CHADS2 score 2.0 Randomized to ASA 75-100 mg/day plus
either clopidogrel 75 mg/day or placebo (double-blind) Primary
endpoint: CV death, stroke, MI, systemic embolism Median follow-up
3.6 years NEJM 2009;360:2066-78
* Also no benefit in diabetics, NYHA class III patients, or
patients with LVEF > 30% NEJM 2005;352:225-37 ICD vs. Placebo in
Selected Subgroups: SCD-HeFT
Slide 74
All-Cause Mortality: SCD-HeFT ICD vs. Amiodarone vs. Placebo
NEJM 2005;352:225-37 ICD Placebo Amio