Embed Size (px)
Citation preview
Khalil Fattouch, Roberta Sampognaro, Giuseppe Speziale, Khalil Fattouch, Roberta Sampognaro, Giuseppe Speziale, Marco Caruso, Pietro Dioguardi, Salvatore Novo, Giovanni Marco Caruso, Pietro Dioguardi, Salvatore Novo, Giovanni
Ruvolo. Ruvolo.
Disclosures: NoneDisclosures: None
Aortic Symposium 2010 Sheraton Hotel and Towers, New York, USA.
Results of aortic valve repair according to valve morphology and surgical
techniques.
Background
• In the last decade, results of aortic valve repair were dramaticaly improved in term of mortality and freedom from aortic valve regurgitation and reoperation
•Several techniques were used for aortic valve repair in bicuspid and tricuspid aortic valve.
Study endpoints To assess postoperative outcome of aortic valve repair according to:
1.Valve morphology (tricuspid or bicuspid)
2.Surgical techniques: plication, free edge reinforcement with Gore-Tex, “chordae technique” (described by us)
Study EndpointsStudy Endpoints
Evaluate the impact of AV repair on 6-year freedom:
• from overall and cardiac-related death • from reoperation on aortic valve• from reccurrent aortic valve
regurgitation grade ≥ II Valve-related events were as follows:
reccurent AR, reoperation, endocarditis, stenosis, trombo-embolism.
Patients and Patients and MethodsMethods
• Since February 2003, 216 patients with aortic regurgitation underwent valve repair in our institution.
• Patients were classified preoperatively according to functional classification: Type I in 55 pts (25.5%), Type II in 126 (58.3%) and Type III in 35 (16.2%).
• 66 pts (27.7%) had bicuspid valve
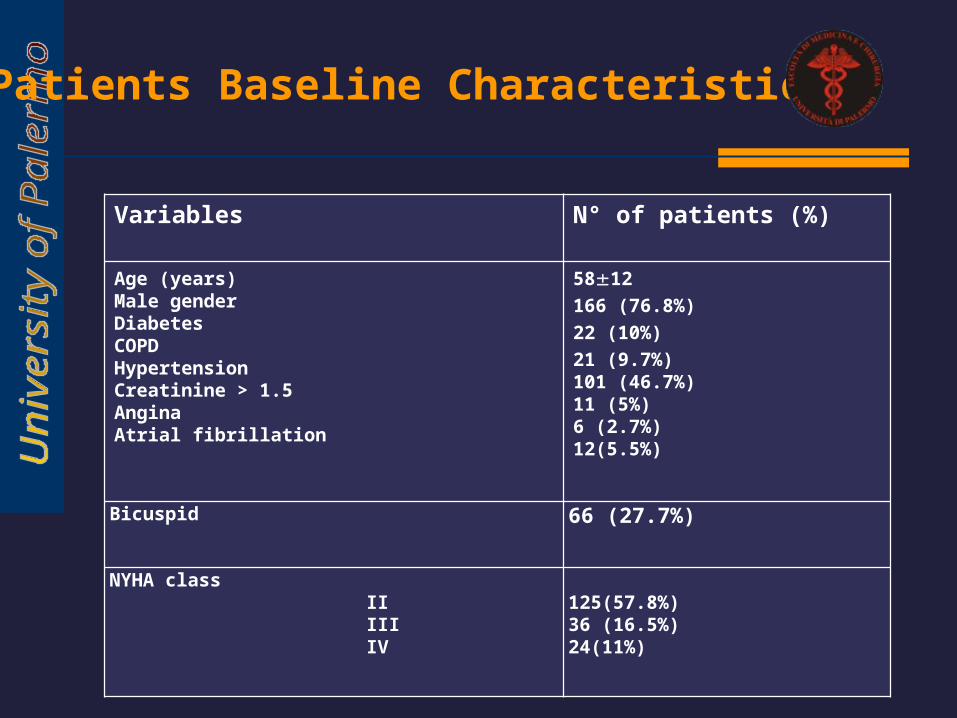
Variables N° of patients (%)
Age (years)Male gender DiabetesCOPDHypertensionCreatinine > 1.5AnginaAtrial fibrillation
5812 166 (76.8%)22 (10%)21 (9.7%) 101 (46.7%)11 (5%)6 (2.7%)12(5.5%)
Bicuspid 66 (27.7%)
NYHA class II III IV
125(57.8%)36 (16.5%)24(11%)
Patients Baseline Characteristics
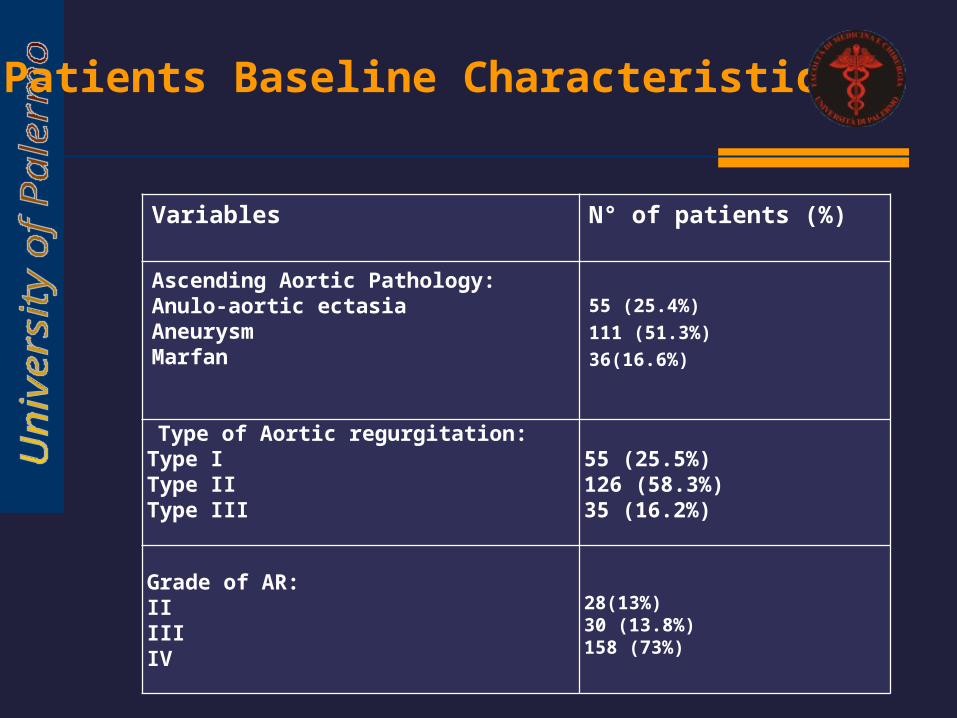
Variables
N° of patients (%)
Ascending Aortic Pathology:Anulo-aortic ectasia AneurysmMarfan
55 (25.4%)111 (51.3%)36(16.6%)
Type of Aortic regurgitation:Type IType IIType III
55 (25.5%)126 (58.3%)35 (16.2%)
Grade of AR:IIIIIIV
28(13%)30 (13.8%)158 (73%)
Patients Baseline Characteristics
Intraoperative Characteristics
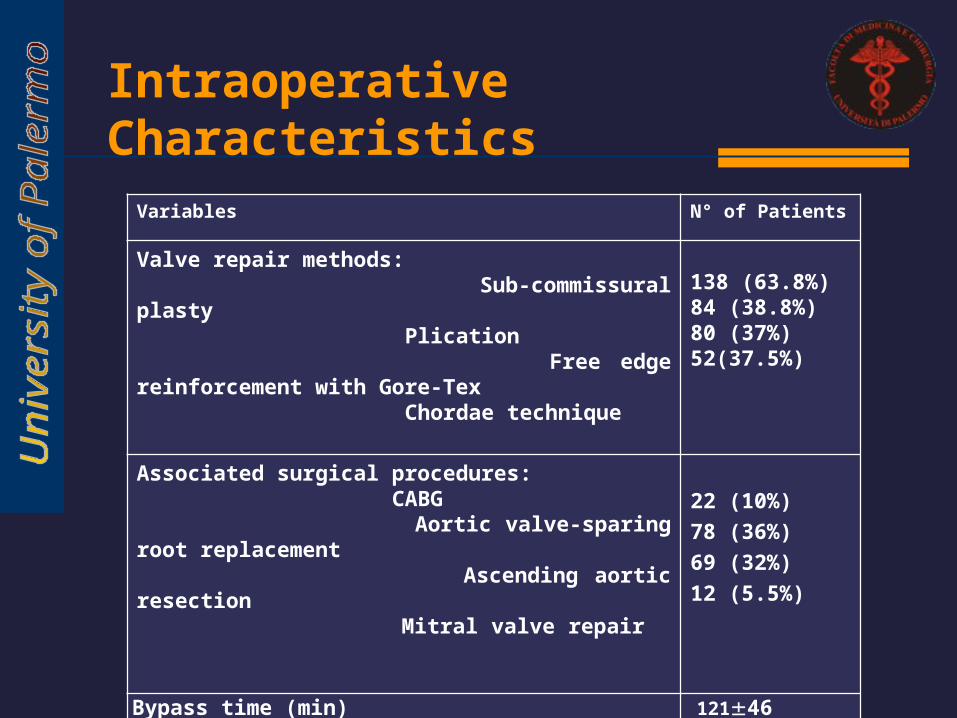
Variables N° of Patients
Valve repair methods: Sub-commissural plasty Plication Free edge reinforcement with Gore-Tex Chordae technique
138 (63.8%) 84 (38.8%) 80 (37%)52(37.5%)
Associated surgical procedures: CABG Aortic valve-sparing root replacement Ascending aortic resection Mitral valve repair
22 (10%)78 (36%)69 (32%)12 (5.5%)
Bypass time (min)Cross-clamp time (min)Logistic EuroSCORE
Early Mortality
12146 8732 5.23.1
6 (2.7%)
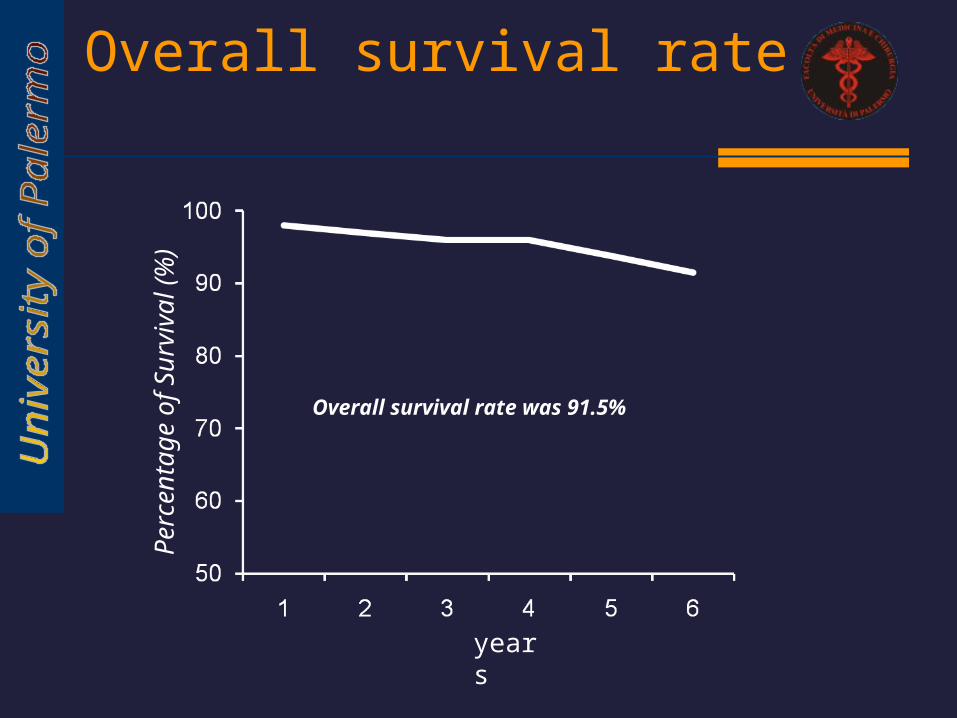
Overall survival rate P
erce
ntag
e of
Sur
viva
l (%
)
years
Overall survival rate was 91.5%
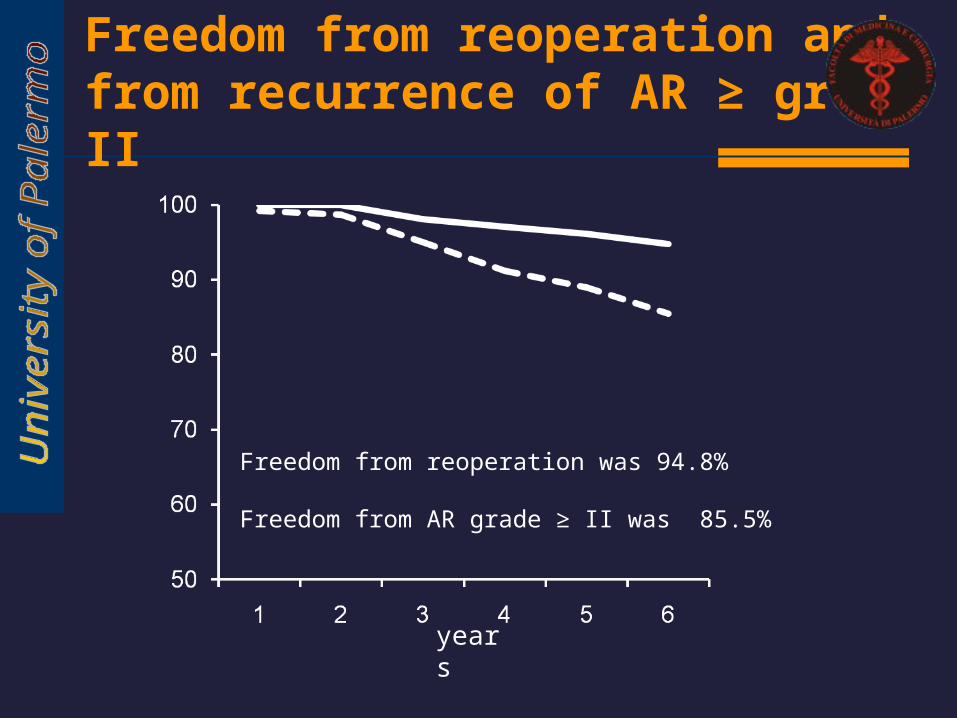
Freedom from reoperation and from recurrence of AR ≥ grade II
years
Freedom from reoperation was 94.8%
Freedom from AR grade ≥ II was 85.5%
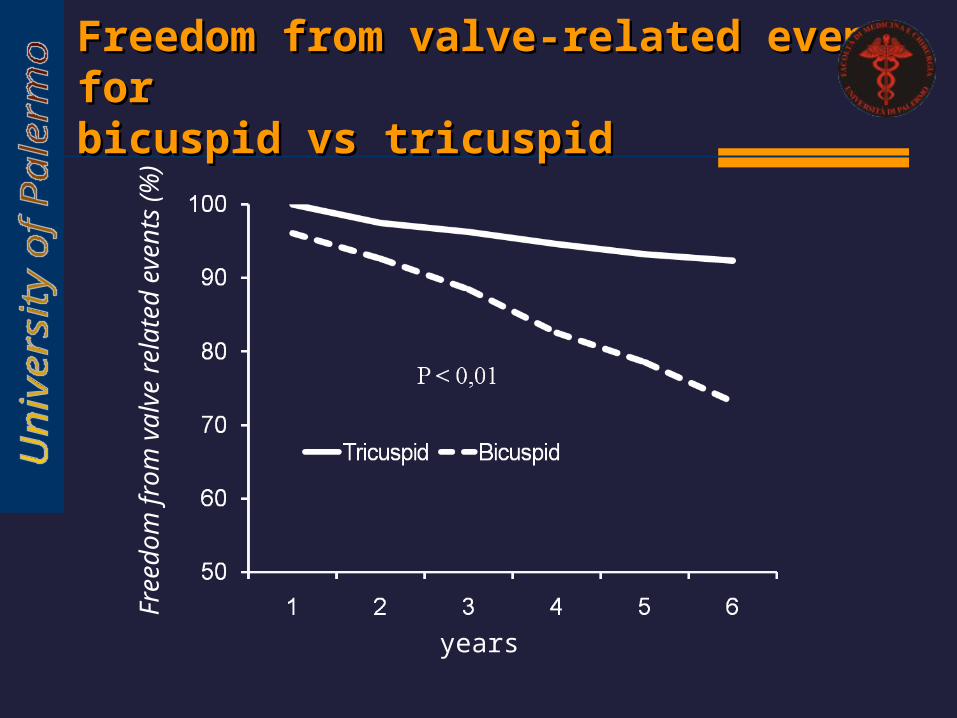
Freedom from valve-related events for Freedom from valve-related events for bicuspid vs tricuspidbicuspid vs tricuspid
years
Fre
edom
from
val
ve r
elat
ed e
vent
s (%
)
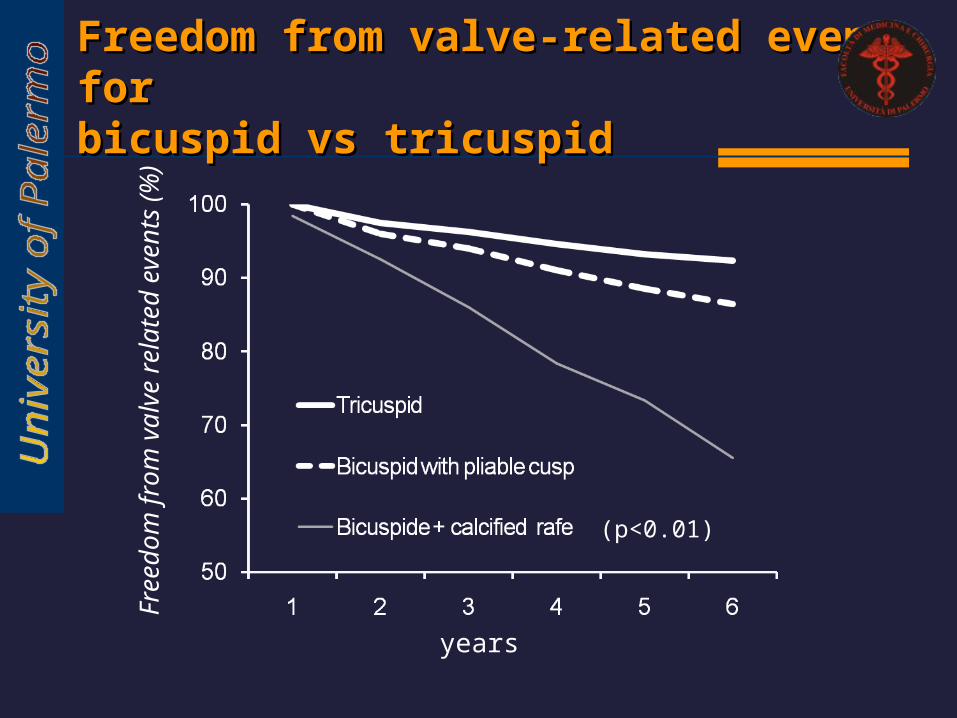
Freedom from valve-related events for Freedom from valve-related events for bicuspid vs tricuspidbicuspid vs tricuspid
years
Fre
edom
from
val
ve r
elat
ed e
vent
s (%
)
(p<0.01)
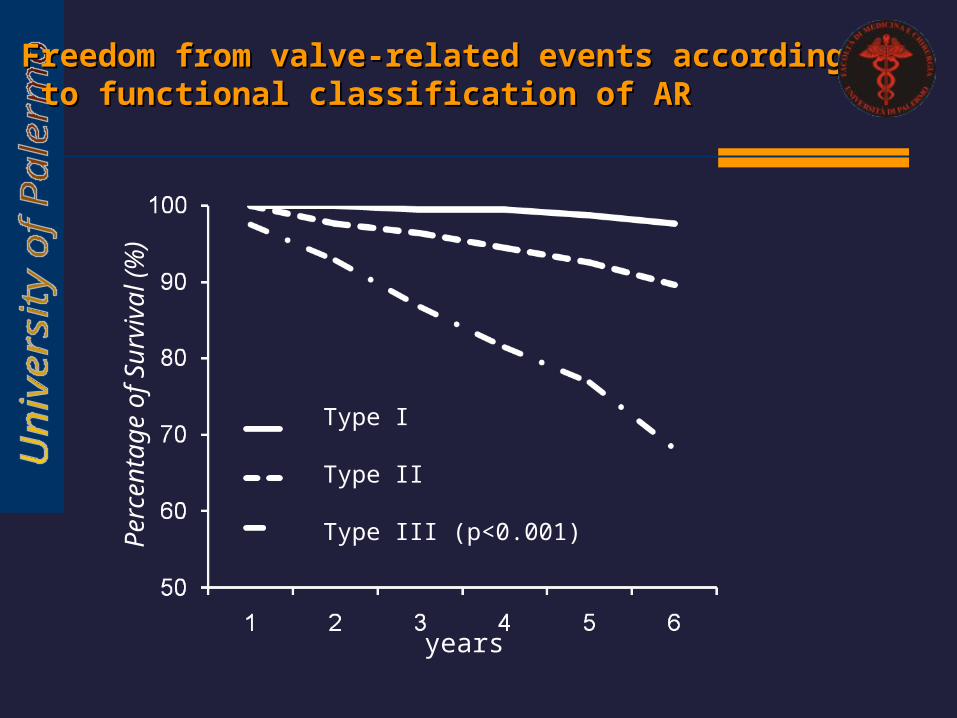
Type I
Type II
Type III (p<0.001)Per
cent
age
of S
urvi
val (
%)
years
Freedom from valve-related events accordingFreedom from valve-related events according to functional classification of AR to functional classification of AR
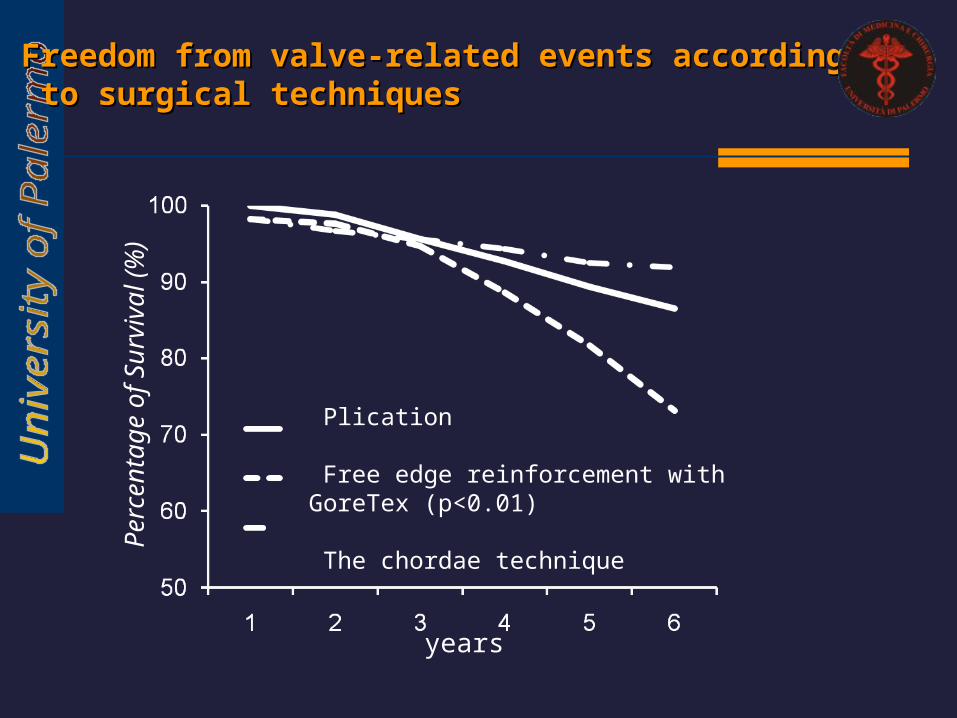
Plication
Free edge reinforcement with GoreTex (p<0.01)
The chordae technique
Per
cent
age
of S
urvi
val (
%)
years
Freedom from valve-related events accordingFreedom from valve-related events according to surgical techniques to surgical techniques
Conclusions
Aortic valve repair can be performed
with low early (2.7%) and late mortality.
Late survival rate was 91.5% and late cardiac related death was 6%.
Overall 6-year aortic regurgitation recurrence (grade≥2) was 14.5%
Overall incidence of aortic valve reoperation after valve repair was 5.2%.
Conclusions
Optimal results was observed for tricuspid and pliable bicuspid valve
Optimal results was observed for Type I and II.
Better results for plicatio and The chordae technique respect to only free
edge reinforcement





























