CASE PRESENTATION
MGT OF PNEUMONIAby
DR TASIE OBINNANATIONAL ASSEMBLY CLINIC, ABUJA.7 SEPT
2015.OVERVIEWIntroductionEpidemiologyClassificationCausesPathophysiologySymptoms
and signsDiagnosisInvestigationTreatmentComplicationDifferential
diagnosisConclusionINTRODUCTIONInflammatory condition affecting the
lung parenchyma due to acute microbial infection with at least one
opacity on chest radiograph. ORAcute respiratory illness associated
with recently developed radiological pulmonary shadowing which may
be segmental, lobar or multilobar.EPIDEMIOLOGYCommon illness seen
in general outpatient clinic. Pneumonia is the second major killer
of Nigerian children with 17% infant mortality per year, yet our
fathers and mothers are ignorant of its causes and prevention.In a
prospective cohort study in Ilorin, the rate of pneumonia was 2
episodes per child per year as compared with South East Asia( 0.36
episodes/ child/ year), European regions ( 0.06 episodes/ child
/year).In Bronchopneumonia, rates are greatest in children less
than 5yrs and adults older than 65yrs, occuring frequently in
developing world than in developed world.Rudan et al calculated and
published the 1st global estimate of incidence of clinical
pneumonia. More than half of the world annual new pneumonia cases
are concentrated in just five countries: India, China, Pakistan,
Bangledesh and Nigeria.CLASSIFICATIONSITE: lobar or
bronchopneumoniaAETIOLOGY: infective , chemical, allergic, PREVIOUS
HEALTH: CAP, Nosocomial pneumonia , immunocompromised.CLINICAL
PRESENTATION: typical or atypical.ATYPICAL PNEUMONIAaka
Interstitial pneumonitis.Inflammation is in the alveolar septa and
interstitium, there is no exudate in the alveolar space.caused by
viruses and mycoplasma pneumonia in majority of cases.Symptoms are
milder and longer lasting than typical pneumonia.Histology: chronic
inflammatory cells in the alveolar wall and interstituim with pink
hyaline membrane lining the alveolar walls.COMMUNITY ACQUIRED
PNEUMONIAInfectious lung disease involving the alveoli, distal
airways and the interstituim of the lungs , contracted outside the
hospital setting.Affects 4 million adults yearly.Severity is
determined by host factor , not pathogen type and virulence.Most
gram negative bacteria that cause CAP are enterobacteria [
S.pneumonia, H.influenza] and enter the lungs via inhalation of
vomits.HOSPITAL ACQUIRED PNEUMONIAaka nosocomial infection.Refers
to new episode of pneumonia occurring at least 2days after
admission to hospital and not incubating at the time of
admission.Highest rates among ICU patients undergoing mechanical
ventilation.The most important distinction between hospital and
community acquired pneumonia is the difference in the spectrum of
the pathogenic organism.CAUSESBACTERIA eg : Strep pneumonia,
Chlamydia pneumonia, Mycoplasma pneumonia, Legionella pneumophilia,
H. influenza, Staph aureus, Klebsella etc.VIRUSES eg : Rhinovirus,
Coronavirus, Adenovirus, Parainfluenza, Human simplex virus. Human
simplex virus rarely causes pneumonia except in groups such as
newborn, person with cancer, transplant recipients and significant
burns patients.3. FUNGI eg Histoplasma capsalatum, C.immitis,
C.neoformans, Aspergilloses, Candidiasis( rare), Sporotrichosis.4.
PARASITIC causesT.gondii, Ascaris lumbricoides, Hookworm and
S.stercoralis.PREDISPOSING FACTORS Smoking.Chronic
alcoholism.Asthma.Chronic obstructive airway disease.Old age.Recent
cold or flu.Immunodeficiency state.Male gender.Use of acid
suppressing medications like proton pump inhibitor/ H2 blocker,
steroid therapy10. Contaminated ventilator system or equipments.11.
Aspiration of oropharyngeal contents into the lower respiratory
tract.12. SepsisPATHOPHYSIOLOGYBacteria typically enter the lungs
with inhalation, though they can reach the lung via the blood
stream if other part of the body are infected.Often bacteria live
in the upper respiratory tract and are continually being inhaled
into the alveoli. Once inside the alveoli, bacteria travel into the
spaces between the cells and also between adjacent alveoli through
connecting pores.BACTERIA AND FUNGIInvasion of the lungs by
bacteria and fungi causes cellular death and triggering of the
immune system leading to phagocytosis of the bacteria by
neutrophils.Cytokines released by neutrophils causes exudation of
fluid inside the alveoli.The neutrophil, bacteria debris and the
exudates in the alveoli result in impaired oxygen
transportation.Sepsis may occur from bacteremia.Septic shock may
occur and leads to damage in multiple parts of the
body.PATHOPHYSIOLOGY contd.Viral infections occur when contaminated
airborne droplets are inhaled through the mouth or nose. Some
viruses such as measles and Human simplex virus may reach the lung
via the blood. The invasion of the lungs may lead to varying
degrees of cell death. When the immune system responds to the
infection , even more lung damage may occur.PARASITEEnters the body
through skin or swallowing.Migrates to the lungs most often through
the blood.Both mechanism of cellular destruction and immune
response result in disruption of oxygen transportation.Immune
response is mediated by eosinophil.STAGES 1. CongestionThe affected
lung parenchyma is partially consolidated and red purple. Occurs on
Day1/2. On microscopy, there is vascular engorgement, few
neutrophils and bacteria in the alveoli. 2. Red hepatization seen
on Day 3/4The pulmonary lobe appears consolidate, red brown, dry,
firm with liver like consistency. Microscopically, there is
accumulation in the alveolar space of exudate rich in fibrin mainly
with leucocytes, erythrocytes and bacteria.contd of STAGES. 3. Gray
hepatization occur on Day 5-7The affected lungs have a liver like
consistency with uniform gray color. On cut surface, you would see
grayish purulent liquid drains. 4. Resolutionbegins on Day 8 and
continues for 3weeks while the exudates within the alveolar spaces
will be drained through lymphocytes and airways.SYMPTOMS/
SIGNSCough: productive or non productive. sputum may be whitish ,
yellowish or greenish.Fever: moderate/ high grade.
Fatigue.Pleuritic chest pain: stabbing pain aggravated or worse on
deep inspiration or coughing.Difficulty in
breathing.Confusion.Headache.Loss of appetite.DIAGNOSIS1) History2)
Physical Examinationa) Respiratory examTachypnea i.e. respiratory
rate> 18c/mDecreased chest expansion on the affected side.
Increased vocal resonance. Dull percussion note. Bronchial breath
sounds. Fine / coarse crepitation on the affected
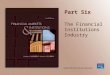
side.INVESTIGATION.Chest Xray38yr old patient with M.pneumonia
chest xray film showing vague ill defined opacity in the left lower
lobe.
XRAY FINDINGS IN LEGIONELLA PNEUMONIA
LOBAR PNEUMONIA XRAY FILM
Legionella pneumonia is implicated in 2- 15% of Community
acquired pneumonia. Mild infection may manifest with bilateral
involvement but in severe infection , lung agitation and bulging of
the fissure have been reported.INVESTIGATIONS2. Sputum M/C/S3. Full
blood count. increased WBC is noted> 11,000 cells/ microliter.4.
Urine ELISA : legionella5. Pleural fluid M/C/S: mycoplasma,
chlamydia, coxiella.6. Blood culture.7. Pulse oximetry: simple non
invasive method of measuring arterial oxygen saturation, and assist
in monitoring oxygen therapy response.Rare lab testHigh resolution
computed tomograghy [ HRCT] can pick up opacities even if chest
xray is normalPCR Amplification of the DNA or RNA of micro organism
can be used to detect legionella, mycoplasma, and chlamydia
pneumonia.OBJECTIVES The main objectives of investigating patients
with a clinically based diagnosis of pneumonia are: Obtain
radiological confirmation of diagnosis. Obtain a microbiological
diagnosis. Assess the severity Identify the development of
complications.INDICATION FOR ADMISSIONCURB 65C- confusionU- blood
urea nitrogen >7mmol/lR- respiratory rate> 30cycles/minB-
diastolic blood pressure 65years.TREATMENTAntibiotics is the drug
of choice for treating pneumonia. They include : PARENTERAL
INFUSION.IV Ceftriazone 1g dailyIV Erythromycin 500mg qds [ if
mycoplasma or legionella is suspected].IV Augmentin 1.2g bdIV
Flucloxacillin 1g tds [ if staph is implicated] IV antibiotics can
be changed to oral therapy when : WBC is returning toward
normalThere are two normal temperature readings [