Embed Size (px)
Citation preview

MethodsMethods
ResultsResults
Abstract No H-77
10th CROI, Boston MA
Contact information:
Carlos del Rio MD* [email protected]
David Rimland MD** [email protected]
Jodie L. Guest PhD** [email protected]
Ngoc-Anh Le PhD† [email protected]
Virgil Brown MD‡ [email protected]
Phone*: 404-616-7025 Fax*: 404-880-9305
Phone**: 404-728-7748 Fax**: 404-728-7782
Phone † : 404-321-6111 ext. 6899 Fax †: 404-728-4716
Lipid Abnormalities among PI-treated Women may be due to Excess Production of ApoC-III Lipid Abnormalities among PI-treated Women may be due to Excess Production of ApoC-III Isabel Hernández, Carlos del Rio, Erik Folch, Jeffrey Lennox, Ngoc-Anh Le, David Rimland, Jodie L. Guest, Virgil Brown.
Emory University Center for AIDS Research, Emory Lipid Research Laboratory, & VA Medical Center. Atlanta, Georgia, USA
Variable N Percentage
Race: African-American 180 89
White or Hispanic 22 11
Age > 40 years 106 52
Tobacco + 86 43
High Blood Pressure* 54 27
Diabetes Mellitus 16 8
BMI Normal 61 30
Overweight 136 67
Lipid-lowering drugs 20 10
Family history of: DM 98 48.5
Stroke 81 40.1
CVD 78 48.6
CD4 >200 cells/ mL 150 74
VL <10,000 copies/ mL 132 65
VL < 400 copies/ mL 91 45
Table 1. Patient Characteristics (N=202).
AbstractAbstractBackground: Mortality from AIDS has been reduced with the availability of HIV-protease inhibitors (PI); however, lipid abnormalities have become common among PI-treated patients and may lead to premature atherosclerosis and its complications. The pathogenesis of these abnormalities is not well understood. We studied the prevalence of lipid abnormalities as well as apolipoproteins (new markers of coronary artery disease) among HIV-infected women in an inner city clinic in the US.
Methods: Cross-sectional study of HIV-infected women who had: 1) >3 months of stable ARV therapy; 2) no ARV therapy in the last 3 months or, 3) who were treatment naïve. A questionnaire and a complete fasting lipid profile were performed. Laboratory and medical records were reviewed. Comparisons were made using Chi-Square, Fisher’s Exact test or t test as appropriate.
Results: 202 HIV-infected women were included between 3/02 and 10/02. The majority were African American (90%), with median age of 41 years (range 21-72); 8% were diabetic, 43% smoked, 10% were on anti-lipid drugs, and 67% were overweight. Mean CD4 count was 371 cells/µL (median 323, range 11-1123) and mean viral load was 61,153 copies/mL (median 1,070, range 30- >750000). Half of the patients had a viral load <10,000 but > 50 copies/mL. Two thirds (131/202) had received ARVs for at least 3 months, 26% (52) had no ARV therapy in the last 3 months and 9% (19) were naïve. Among those receiving ARVs (131), 66% (86) were on a PI (NFV 55%, LPV/rtv 30%, IDV 12%, RTV 8%) and 35% were on an NNRTI together with reverse transcriptase inhibitors (d4T in 30% and ddI in 26%).
See tables 2 and 3.
Conclusions: Our data suggest that among PI-treated women, lipid abnormalities seem to be related to excess of ApoC-III in VLDL which can interfere with normal triglyceride hydrolysis. These drugs may be causing an increased production of ApoC-III which can lead to all of the observed lipoprotein abnormalities described.
BackgroundBackground ConclusionsConclusionsGroup N (%)
Chol>240
TG>200
HDL<35
LDL>160
Apo A-I < 80
Apo B>120
ApoC-III >25
Apo E<4
Overall 202 13.0 16.8 22.3 9.4 8.4 25.7 30.2 13.4
PI 86 (42.6) 20.9 † 18.6 11.6 ‡ 16.3* 8.1 34.9 † 41.9 ‡ 3.5 †
No PI 45 (22.3) 13.3 20.0 13.3 † 2.2 2.2 28.9 * 35.6 † 15.6
No ARV/ naïve
71 (35.1) 2.8 12.7 40.8 5.6 12.7 12.7 12.7 23.9
* p<0.05 † p≤0.01 ‡ p≤0.0001 Statistical significance is based on comparisons with the “No ARV/ naïve” group.
VA VA
Medical Medical
CenterCenter
Group N (%)Chol>240
TG>200
HDL<35
LDL>160
Apo A-I <80
Apo B>120
Apo C-III >25
Apo E<4
PI with hyperlipidemia
26 (30)
69.2 ‡ 61.5 ‡ 7.7 42.3 ‡ 15.4 61.5 † 80.8 ‡ 0.0
PI with normal lipid profile
60 (70)
0.0 0.0 13.3 5.0 5.0 23.3 25 5.0
GroupN (%)
Chol>240
TG>200
HDL<35
LDL>160
Apo A-I <80
Apo B>120
Apo CIII >25
Apo E<4
PI 72
(35.6)19.4† 19.4 12.5† 15.3 8.3 36.1† 43.1‡ 4.2†
PI and NNRTI 14 (6.9)
28.6† 14.3 7.1* 21.4 7.1 28.6 35.7* 0
NNRTI32
(15.8)15.6* 25.0 6.2† 0.0 3.1 34.4* 43.7† 15.6
Only NRTI13
(6.4)7.7 7.7 30.8 7.7 0.0 15.4 15.4 15.4
No ARV in last 3 months or naïve
71 (35.1)
2.8 12.7 40.8 5.6 12.7 12.7 12.7 23.9
Study design: Cross-sectional studyPatient population: HIV infected patients with
advanced disease, divided in 3 groups1) Three months of stable ARV therapy2) No ARV therapy in the last 3 months3) Treatment naïve
Setting: Infectious Diseases Program (IDP) at Grady Memorial Hospital (GMH) in Atlanta GA, USA.
Enrollment: Between 3/02 and 10/02, at routine blood drawn, if the patient was fasting and willing to participate.
Procedure: Questionnaire and fasting lipid profile. Medical and laboratory records were reviewed.
Hyperlipidemia: Cholesterol >= 240 and / or Triglicerides >= 200
(according to the high risk categories of the National Cholesterol Education Program III Guidelines).
Biomarkers assessed: Basic lipid profile (TG, total, HDL, and direct LDL cholesterol); Apo-lipoprotein risk profile (Apo A-I, B, C-III, E, Lp(a)); Composition of TG-rich lipoproteins isolated at density <1.020 gm/mL by ultracentrifuge; and LDL phenotype by non-denaturating Gradient Gel Electrophoresis.
Statistical analysis: Comparisons made with Chi-square, Fisher’s Exact test, t test, or Wilcoxon, using SAS software v.8.2.
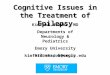
Previous studies using conventional lipid profile have not been consistent and potential abnormal pathways have not been identified. ApoC-III, which is present in Chylomicrons, VLDL (TG rich lipoproteins TRL), inhibits lipoprotein lipase in vitro and reduces VLDL and Chylo remnant clearance. Its over-expression would increase the TG concentrations and decrease TG clearance as demonstrated in mice transgenic for ApoCIII.
Among PI-treated women, lipid abnormalities seem to be related to excess ApoC-III content of VLDL which can interfere with normal TG hydrolysis.
Both, patients with PI or NNRTI therapy had Elevated levels of total cholesterol, Higher Apo C-III and Apo B levels Higher levels of TG, however the percentage of
patients with levels >200 mg/dL was not significantly different from patients with no ARV therapy.
These findings suggest impaired metabolism of TG-rich lipoproteins. Additional risk factors of smoking and DM, in an aging population might increase the likelihood of future atherosclerotic events. Kinetic studies of apoC-III, apoB and triglycerides are planned to determine if the hypothetical physiologic alteration due to PI and NNRTI treatment is enhanced apoC-III synthesis.
LPL LDL
VLDL
Cholesterol EsterTransport Protein
TG
CholesterolEsters
Fatty Acids
LDLReceptor
RemnantReceptor
Excess apoC-IIIChylomicrons Remnants
Lipoprotein lipase LPL
HDL
Excess apoC-III
Excess apoC-III
Figure1. Potential Inhibitory Effects of the Excess Production of Apolipoprotein C-III.
Two hundred and two HIV-infected women were included between 3/02 and 10/02. The median age was 41 years (range 21-72), mean CD4 count was 371 cells/mL (median 323), and mean VL was 61,153 copies/mL. Demographic and laboratory characteristics are shown in Table 1.
Fig. 2. Patient Population. ARV Exposure.
ARV >3m
N=131 (65%)
Median VL <400
No ARV last 3m
N=52 (26%)
Median VL 32,440
Naïve
N=19 (9%)
Median VL 59,350
Patient population N=202
Median viral load 1,070 copies/mL
2.3
3
9.9
25.2
4.6
19.8
35.9
21.4
26.7
30.5 52.7
71.8
0 20 40 60 80
3TC
AZT
d4T
ddI
ABC
NFV
LPV/r
IDV
RTV
IDV + RTV
EFV
NVP
% of patients
Figure 3. Current ARV exposure among patients with >3 months of therapy (n=131).
Among those patients receiving ARVs (131), 86 (65.6%) were on a PI (NFV 54.6%, LPV/r 30.2%, IDV 11.6%, RTV 8.1%), and 35% were on NNRTI together with reverse transcriptase inhibitors. Simultaneous exposure to PI and NNRTIs occurred in 14 patients (10.7%). Median time of exposure to PI were 16 months and for NNRTIs 10 months. The most frequent regimens had AZT and 3TC with NFV (22/131 patients, 17%), with EFV (11, 8.4%), or with ABC (11, 8.4%).
Parameter PI
N=72
PI + NNRTI
N=14NNRTI
N=32
Only NRTI
N=13
No ARV/ naïve
N=71
Mean Median
Mean Median
Mean Median
Mean Median
Mean Median
Cholesterol206.6 ‡
201
212.9 †
197.5
198.8 †
190.5
161.5
153
161.1
163
TG136.8 *
123
147.5
127
163.7 *
112
117.5
115
111.7
90
HDL53.7 ‡
51
55.9 †
53
52.4 ‡
48
39.7
38
40.4
40
LDL117.9 †
112
118.6 *
111
102.1
101.5
98.4
93
97.6
95
Apo A-I151.9 ‡
148
136.1 *
141
144.8 †
138
105.5
106
115.8
106
Apo B109.7 †
96.5
102.9
91
105.6 *
107.5
73.6
67
85.6
77
Apo C-III24.2 ‡
24.2
23.6 †
23.1
23.7 †
21.2
19.5
18.9
19
17.8
Apo E6.7 ‡
6.4
7.3 †
6.3
6.0
5.4
4.9
4.3
5.2
5.0
We studied the prevalence of lipid abnormalities as well as apolipoproteins (new markers of coronary artery disease) among HIV-infected women in an inner city clinic in the US.
* High blood pressure at the moment of the visit
Table 2. Percentage of Women with Lipid Abnormalities.
Table 3. Percentage of Women Exposed to PI (n=86) with and without Hyperlipidemia (cholesterol >240 and / or TG > 200 mg/dL).
Table 4. Percentage of Women with Lipid Abnormalities by ARV Group Exposure.
Comparisons made using Wilcoxon Rank sum test or t test.* p<0.05 † p<0.01 ‡ p<0.0001 Statistical significance is based on comparisons with the “No ARV/ naïve” group.
Table 5. Mean Values of Lipids and Apolipoproteins by ARV Exposure Group.
* p<0.05 † p<0.01 ‡ p<0.0001Statistical significance is based on comparisons with the “No ARV/ naïve” group.
In comparison with HIV + patients without treatment or treatment naïve, those patients being treated with ARV in the last 3 months had significant higher mean levels of cholesterol (199 vs 161 mg/dL), TG (143 vs 112), HDL, LDL and all the apolipoproteins tested (A-I, B, C-III, and E).
BackgroundBackground
An increase in LDL cholesterol and triglycerides (TG), as well as a decrease in HDL cholesterol are the lipid abnormalities associated with HIV infection and HAART. Other cardiovascular risk factors in HIV infected patients with HAART include: Increased visceral fat, insulin resistance, chronic inflammation and endothelial dysfunction / atherosclerosis.Acknowledgment: Partial support provided by the Emory CFAR (P30-AI50409).
PI
Lipid abnormalities
Accelerated atherosclerosis and other complications
Pathogenesis?
* p<0.05 † p<0.01 ‡ p<0.0001 Statistical significance is based on comparisons with the “PI with normal lipid profile” group.
Patients being treated with a PI were 7 times more likely to have total cholesterol >240 mg/dL (RR 6.9; 95%CI 1.6-29.3) in comparison with patients with no ARV. However, neither patients with PI, NNRTI nor both were more likely to have TG >200 mg/dL in comparison with patients with no ARV therapy (all 95%CI included the null value). Tables 4 and 5 shown the percentage of patients with lipid abnormalities, and the mean values by ARV treatment group.
PI treated patients had higher levels of HDL, LDL and total cholesterol, and apoB, C-III and E (Table 2). The increase in Apo C - III levels was mainly present among patients with hyperlipidemia (Table 3).