Embed Size (px)
Citation preview

Methicillin Resistant Staphylococcus aureus
Catherine D. Bacheller, MDInfectious Diseases
Medical Director, Infection Prevention and Control KMCAssistant Professor of Medicine, WSU



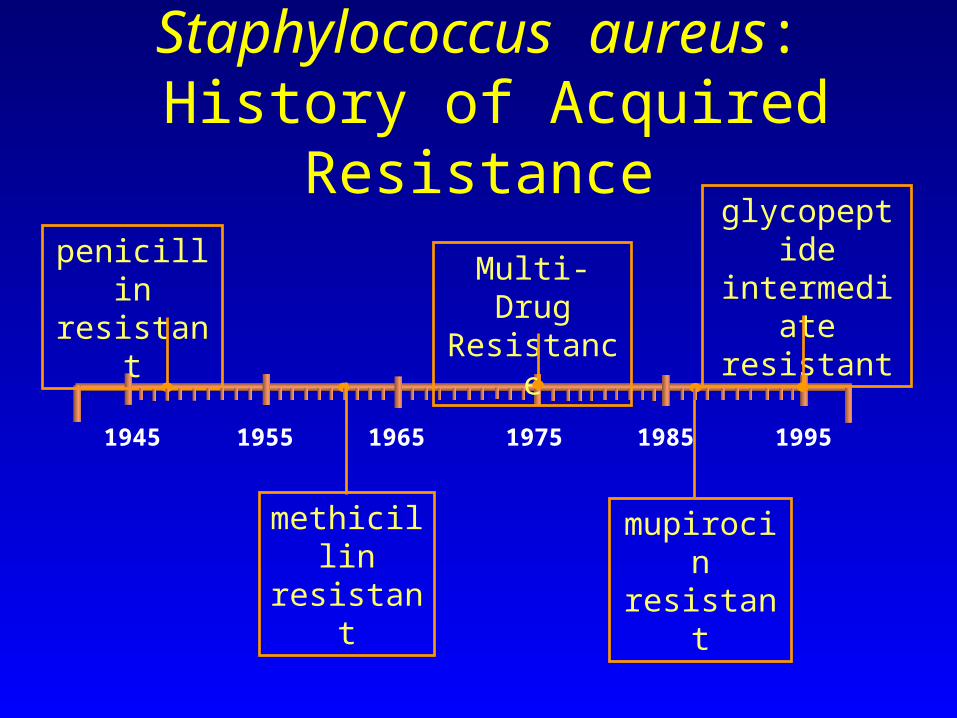
Staphylococcus aureus: History of Acquired Resistance
1945 1955 1965 1975 1985 1995
methicillin resistant
Multi-Drug Resistance
mupirocin resistant
glycopeptideintermediate
resistantpenicillinresistant

Mechanisms of MRSA Antibiotic Resistance
Mayer et al. Principles and Practice of Infectious Diseases. 1995;
Eliopoulos. Infectious Diseases. 1992.
• Activated B-lactamase• Reduced PBP capacity• Chromosomal mecA gene
Altered PBP
Low affinity for B-lactams
Causes resistance to all beta lactam antibiotics

Nosocomial Bloodstream Infections
Fungi (8%)
Edmond MB et al. Clin Infect Dis, 1999; 29: 239-244
Gram Negative (27%)
Gram Positive (64%)

Nosocomial Bloodstream Pathogens
Coagulase Negative Staphylococcus (32%)
Staphylococcus aureus (16%)
Enterococci (11%)
Candida (8%)
ViridansStreptococci (1%)
All Gram Negative (21%)
Other (11%)
Edmond MB et al. Clin Infect Dis, 1999; 29: 239-244

A Multi-Center Economic Analysis of MRSA Bacteremia
MSSA(n=148)
13.1 7.2 24% 19.5k
MRSA(n=148)
15.8 13.9* 34%† 23.1k
Welch KE, et al. 39th ICAAC. 1999, abstract
LOS ICU LOS Mortality Cost (Days) (Days) ($)
*P = 0.03; †P = 0.07
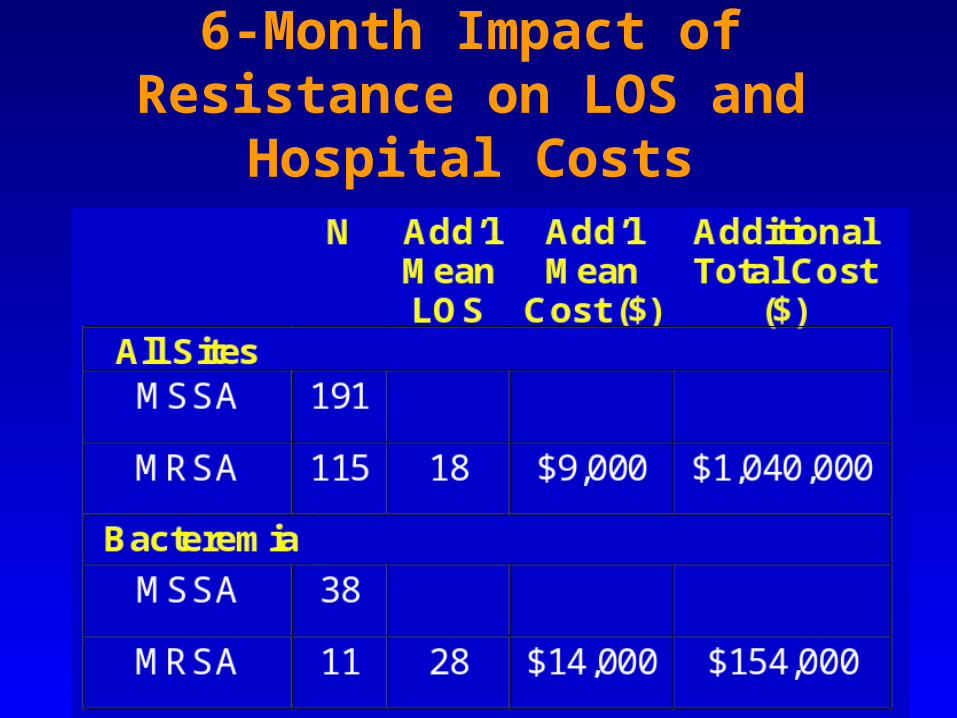
6-Month Impact of Resistance on LOS and Hospital Costs

Nosocomial Infections
with MRSA
Panlilio et al. Infect Control Hosp Epidemiol. 1992.
6060

Staphylococcus aureusICU Nosocomial Infections
05
101520253035404550
1987 1989 1991 1993 1995 1997
Per
cen
t R
esis
tan
t% Sens Vanc only % MRSA
Lowy, NEJM 1998; 339:520-32

The issue about trying to contain MRSA is also very much about:
1. Cost to the hospital in vancomycin use (to treat MRSA infections and for empiric treatment in units where MRSA is endemic)
2. Microbial cost - potential for VRSA, emergence or selection of VRE and other vancomycin-resistant organisms.
[email protected] Subject: PROMED: Infection Control: MRSA (3) Date: Thu, 6 Jun 1996 17:43:27 -0400

S aureus Is Most Common Bacterial Pathogen Isolated From SSTIs of Hospitalized Patients
Adapted from Doern GV et al. Diagn Microbiol Infect Dis. 1999;34:67.
• Other organisms (320/1,562) represented 20.5% of the total bacteria recovered


The Pathogenic Potential of S. aureus(associated sites)
SKIN AND WOUND INFECTIONSImpetigoEcthymaFolliculitisFurunculosisCarbunclesCellulitisAbscessParonychiaSurgical sites infectionsBurn infectionsHidradentitis supprativascalded skin syndrome
BONEOsteomylelitis
HEARTEndocarditisMyocarditis
LUNGPneumonia
JOINTSSeptic arthritis
BLOODSepticemiaBacteremia
INTESTINAL TRACTFood poisoning
EYEEndophthalmitis
VAGINAToxic shock syndrome
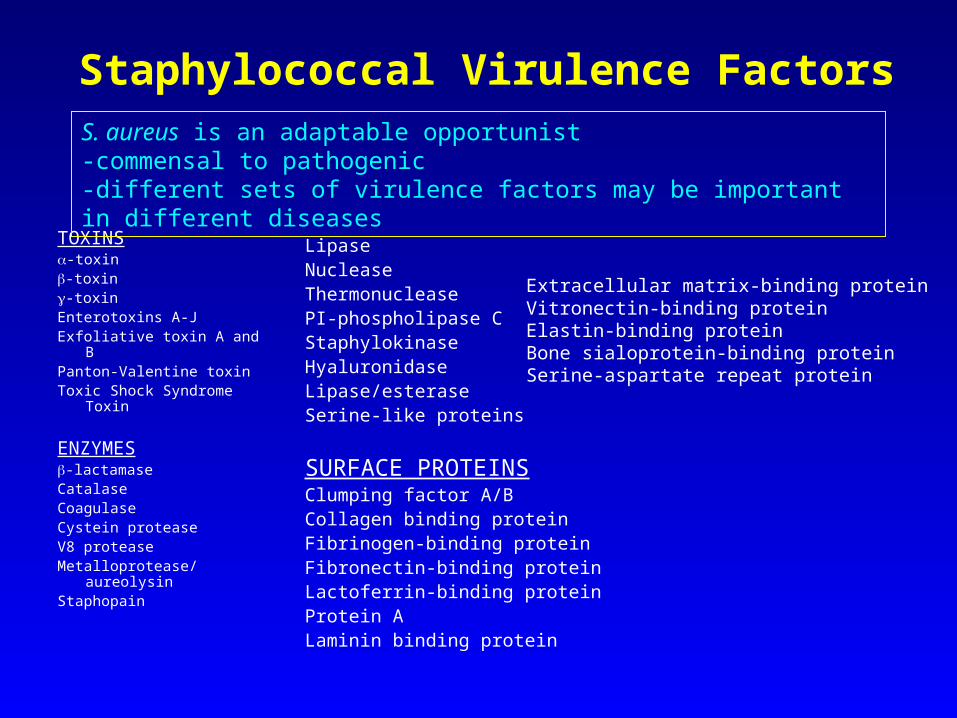
Staphylococcal Virulence Factors
TOXINS-toxin-toxin-toxinEnterotoxins A-JExfoliative toxin A and BPanton-Valentine toxinToxic Shock Syndrome
Toxin
ENZYMES-lactamaseCatalaseCoagulaseCystein proteaseV8 proteaseMetalloprotease/aureolysinStaphopain
LipaseNucleaseThermonucleasePI-phospholipase CStaphylokinaseHyaluronidaseLipase/esteraseSerine-like proteins
SURFACE PROTEINSClumping factor A/BCollagen binding proteinFibrinogen-binding proteinFibronectin-binding proteinLactoferrin-binding proteinProtein ALaminin binding protein
Extracellular matrix-binding proteinVitronectin-binding proteinElastin-binding proteinBone sialoprotein-binding proteinSerine-aspartate repeat protein
S. aureus is an adaptable opportunist -commensal to pathogenic -different sets of virulence factors may be important in different diseases

Staphylococcal Infections
Preventing Spread of MRSA Outbreak Among Hospitalized Patients
• Timely ID of epidemic strain• Culture surveillance of patients and staff• Barrier precautions• Staff carriers to non-clinical duties• HANDWASHING !!!!!!!!!• Discharge of patients infected with epidemic
strain• Flagging infected patients records
National Clean Hands Week at Kettering Hospital September 18-24, 2005

Elimination of nasal carriage of methicillin-resistant Staphylococcus aureus with mupirocin during a hospital outbreak.
During a hospital outbreak of methicillin-resistant S. aureus (MRSA), involving more than 200 patients, 40 patients and 32 hospital staff who were stable nasal carriers of MRSA received topical application of 2% mupirocin, formulated in a white soft paraffin and lanolin ointment, to their anterior nares for five days. ...
… The elimination of nasal MRSA by mupirocin, and the introduction of isolation facilities, were associated with the control of the outbreak.
Hill RL; Duckworth GJ; Casewell MW J Antimicrob Chemother 1988;22:377 - 84.
[email protected] Subject: PROMED: Infection Control: MRSA (3) Date: Thu, 6 Jun 1996 17:43:27 -0400
My personal impression is that there is probably a critical limit of MRSA prevalence beyond which control measures are largely futile (I hope to be proved wrong, perhaps by a case-control study of wards with and without control measures), and that control measures are most beneficial in hospitals which have a near-zero rate of MRSA.

MRSA: No Longer Limited toNosocomial Infections in the USA
Moreno et al. Clin Infect Dis. 1995.
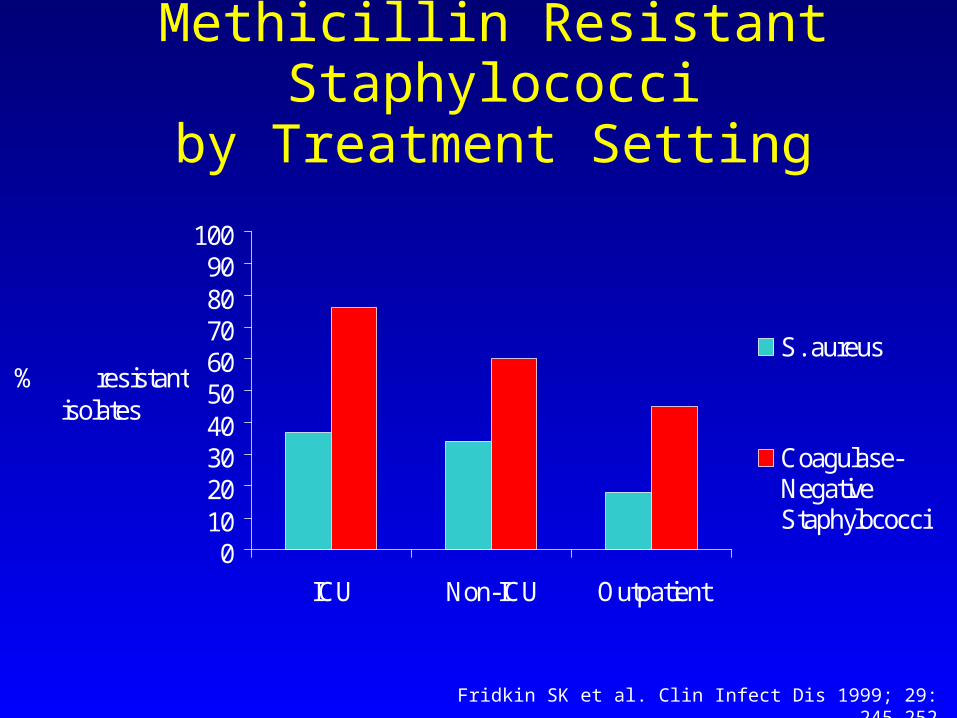
Methicillin Resistant Staphylococciby Treatment Setting
0102030405060708090
100
ICU Non-ICU Outpatient
% resistant isolates
S. aureus
Coagulase-NegativeStaphylococci
Fridkin SK et al. Clin Infect Dis 1999; 29: 245-252

Here comes community-acquired MRSA…

MMWR, 48(32); 707-710. Aug 20, 1999

Methicillin-resistant Staphylococcus aureus


CA MRSA

CA MRSA
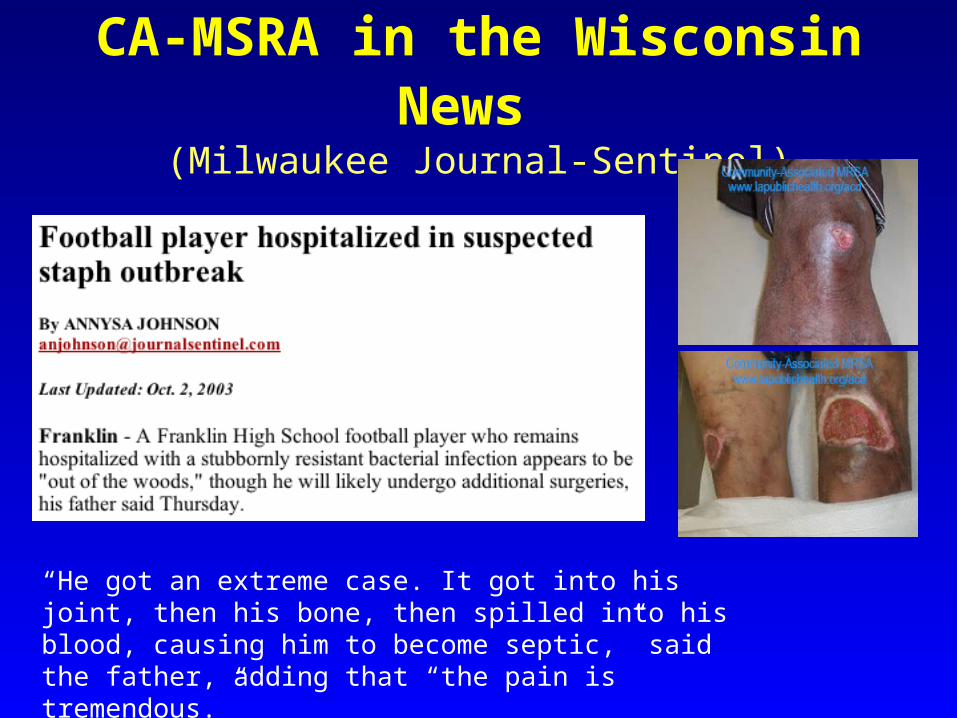
CA-MSRA in the Wisconsin News (Milwaukee Journal-Sentinel)
“He got an extreme case. It got into his joint, then his bone, then spilled into his blood, causing him to become septic,” said the father, adding that “the pain is tremendous.”

Subject: Tibia - MRSA osteomyelitis Vanderbilt University Date: Wed, 24 Dec 2003 06:11:14 -0600


Characteristics of CA-MRSA
• Community-acquired MRSA differs from HA-MRSA in that CA-MRSA is not multidrug-resistant and can usually be treated with clindamycin, trimethoprim/sulfamethoxazole, minocycline, or linezolid.
• Both organisms carry the staphylococcal cassette chromosome mecA (SCCmecA)
gene that encodes resistance to the ß-lactams

Emerging Infectious Diseases • Vol. 9, No. 8, August 2003
We assessed whether any common genetic markers existed among 117 CA-MRSA isolates from the United States, France, Switzerland, Australia, New Zealand, and Western Samoa by performing polymerase chain reaction for 24 virulence factors and the methicillin resistance determinant.
Although the selective advantage conferred by the combination of genetic traits (i.e., PVL locus and SSCmec IV in an agr3 background) is not clear, the spread of a limited number of clones in each continent suggests that these CA-MRSA strains are particularly suited to be successful community-based pathogens.
Limited number of clones found
Involvement of Panton-Valentine Leukocidin Producing Staphylococcus aureus in
Primary Skin Infections and Pneumonia.1. Panton-Valentine leukocidin (PVL) is a cytotoxin that causes
leukocyte destruction and tissue necrosis. It is produced by fewer than 5% of Staphylococcus aureus strains.
2. A collection of 172 S. aureus strains were screened for PVL genes by polymerase chain reaction amplification.
3. PVL genes were detected in 93% of strains associated with furunculosis and in 85% of those associated with severe necrotic hemorrhagic pneumonia (all community-acquired). They were detected in 55% of cellulitis strains, 50% of cutaneous abscess strains, 23% of osteomyelitis strains, and 13% of finger-pulp infection strains.
4. PVL genes were not detected in strains responsible for other infections, such as infective endocarditis, mediastinitis, hospital-acquired pneumonia, urinary tract infection, and enterocolitis, or in those associated with toxic-shock syndrome. It thus appears that PVL is mainly associated with necrotic lesions involving the skin or mucosa.
Gerard Lina, et al. Clinical Infectious Diseases 1999;29:1128-1132..

Pneumonia

CA MRSA Inpatient Therapy
Bacteremia• Vancomycin 1gm q 12hr (target trough 10-20)• Daptomycin 6mg/kg q 24hr• Quinupristin-dalfopristin 7.5mg/kg q 8hr via CVP
Ventilator Associated Pneumonia• Linezolid 600mg q 12hr (?superior)• Vancomycin 1gm q 12hr• (DO NOT USE Daptomycin)

CA MRSA Outpatient Therapy
I & D of abscess and Culture of fluid
Oral antibiotics for 2 weeks:• Clindamycin 300mg q 6hr (inducible resistance)• TMP/SMZ DS q 12hr (not active in pus)
?plus Rifampin 300mg q 12hr• Minocycline or Doxycycline 100mg q 12hr• Linezolid 600mg q 12hr ($$$$)
If recurrent infection, repeat above plus: Nasal & Nails: Mupirocin BID x 5days
Skin: Chlorhexidine (CHG) bath daily

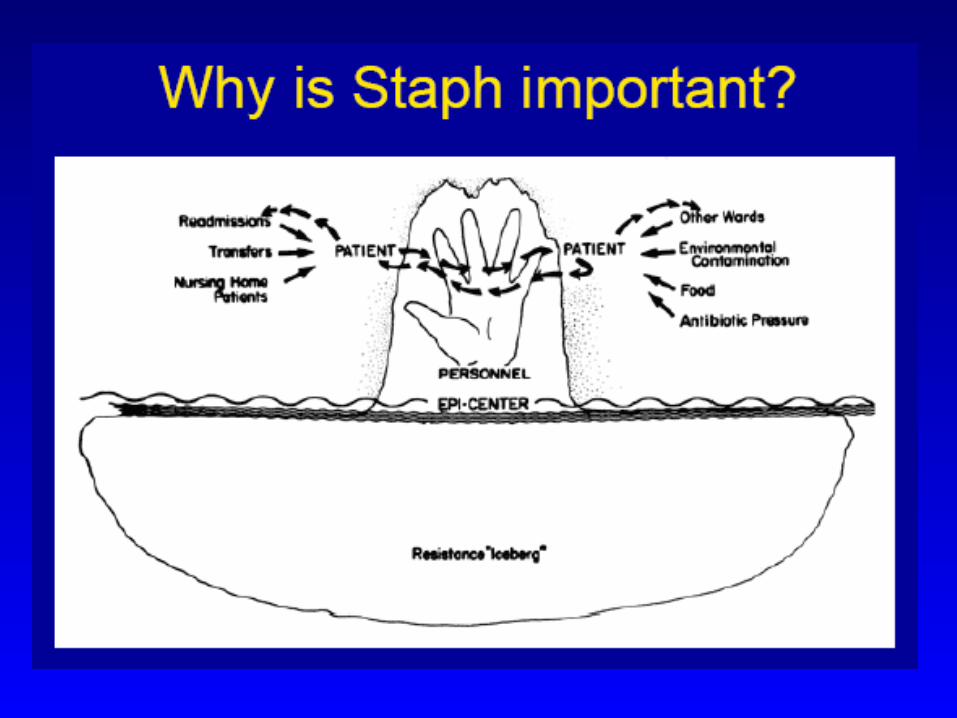
Methicillin-resistant Staphylococcus aureus: a consensus review of the microbiology, pathogenesis, and epidemiology with implications for prevention and management.
... MRSA colonization precedes infection. A major reservoir is the anterior nares. MRSA is usually introduced into an institution by a colonized or infected patient or health care worker. The principal mode of transmission is via the transiently colonized hands of hospital personnel...
Mulligan ME; Murray-Leisure KA; Ribner BS; Standiford HC; John JF; Korvick JA; Kauffman CA; Yu VL. Am J Med 1993;94:313

Handwashing is the single most important means of preventing
the spread of infections