Embed Size (px)
Citation preview

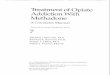
Methadone:You Don’t Prescribe it?
You Still Need to Know About it.
Karen Triandafyllis, NPOpiate Treatment Outpatient Program
San Francisco General Hospital
April 22, 2010

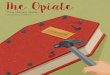
Methadone has many interactions with both prescribed medications and substances of abuse
These interactions, in turn, can significantly impact patient outcomes Medical Psychiatric Substance Abuse

Case Study #1 48-year old male with Opioid and Cocaine
Dependence, HIV, Hep C+, and Depressive disorder
On Methadone 70mg daily, no illicit opioid use x 6 mos, continues to use crack cocaine 3-4x/wk
On Sertraline 100mg qbedtime for depression PCP wants to start pt on HIV meds. Some
concerns re possible adherence, but thinks stable enough. Prescribes Atripla 1 tab daily
Pt misses initial f/u appt with PCP, returns 4 wks later. States he relapsed on heroin and has been off all his medications, except for Methadone, for the past 2 wks
What do you do to help him?

Case Study #2 35-year old female with Opioid and
Methamphetamine Dependence, Hep C+, HTN, OCD and Anxiety d/o NOS
On Methadone 50mg daily and HCTZ 25mg daily Enters residential tx, does well, stops using
any illicit drugs, engages in psychiatric care and is started on Fluvoxamine 100mg daily and Clonazepam 0.5mg BID
You receive a call from her program stating that she has been nodding off in groups and they are concerned she is abusing her benzos
What can you do to help her?

Methadone Pharmacology Opiate agonist High systemic bioavailability (90%) Peak plasma levels at 2-4 hours Long T ½ allows convenient dosing, but
T ½ is quite variable Relatively lipid soluble Duration of analgesia << expected with
T ½

Methadone Pharmacology (cont’d) Stored and accumulates in tissues (esp.
liver) which extend the apparent T ½ 90% protein bound (not eliminated by
dialysis) Biotransformation by P450 (3A4 and
2D6 mainly) Cleared by GI tract in patients with
significant renal disease

Methadone Safety: Black Box Warnings

QTc Prolongation and Torsade 2009 Clinical Guidelines for QTc Interval Screening in Methadone
Treatment: Consensus Recommendations Disclosure: Clinicians should inform patients of arrhythmia risk when
they prescribe methadone. Clinical History: Clinicians should ask patients about any history of
structural heart disease, arrhythmia, and syncope. Screening: Obtain a pretreatment electrocardiogram for all patients
to measure the QTc interval and then a follow-up electrocardiogram within 30 days and annually. Additional electrocardiography is recommended if the methadone dosage exceeds 100 mg/d or if patients have unexplained syncope or seizures.
Risk Stratification: If the QTc interval is greater than 450 ms but less than 500 ms, discuss potential risks and benefits with patients and monitor them more frequently. If the QTc interval exceeds 500 ms, consider discontinuing or reducing the methadone dose; eliminating contributing factors, such as drugs that promote hypokalemia; or using an alternative therapy.
Drug Interactions: Clinicians should be aware of interactions between methadone and other drugs that possess QT interval–prolonging properties or slow the elimination of methadone.
Krantz et al (2009). Ann Intern Med. 2009;150:387-395.

QTc Prolongation and Torsade (cont’d) Major risk factors include
Electrolyte abnormalities (hypomagnesemia, hypokalemia, hypocalcemia)
Hepatic dysfunction Other QT prolonging medications

Methadone-Drug Interactions CYP inhibitors
Slow Methadone metabolism, raise serum methadone levels, extend duration of its effects, possible cause Methadone-related toxicity (e.g., oversedation, respiratory depression, prolonged QTc)
Overmedication reactions develop within a few days after concurrent drug administration
CYP inducers Accelerate Methadone breakdown, abbreviate duration of Methadone effects, lower
serum methadone levels, possibly precipitate withdrawal May take a week or much longer to emerge, producing withdrawal sx
Not all interactions are related to altered drug metabolism Additive effects of Methadone with other CNS depressants, for example, causing
hypotension, sedation, respiratory depression or coma Other QTc prolonging medications
Methadone can also increase or decrease some concomitant drug levels, leading to toxicity or lack of efficacy
Also consider potential effects when discontinuing medications

Risks of Reduced Serum Methadone Levels
Potential relapse to illicit opioids
Non-adherence to prescribed medications

Prescribing Medications that Interact with Methadone Use alternative, non-interacting drugs if
possible Adjust concomitant drug as appropriate if
Methadone affects its levels Advise pts in advance of physical symptoms of
overmedication or withdrawal that may occur Encourage pts to let their Methadone Clinic
know about initiation or discontinuation of interacting medications
Inform Methadone Clinic about changes For W93 pts, call 206-8412 and ask for the NP on call

Methadone-Drug Interactions: HIV medications
Drug Effects
Didanosine (ddl) Significant ↓ in ddl concentration
Stavudine (d4T) Significant ↓ in d4T concentration
Zidovudine (AZT) AZT concentration increased 40%
Abacavir (ABC) ↓ Methadone level; ↓ ABC peak concentration
Efavirenz ↓ Methadone level, withdrawal common
Lopinavir+Ritonavir ↓ Methadone level, withdrawal common
Darunavir ↓ Methadone level, withdrawal may occur
Nevirapine ↓ Methadone level, may precipitate withdrawal

Methadone-Drug Interactions: Psychotropic medications
Drug Effects
Benzodiazepines Additive CNS depression
MAOIs Contraindicated due to potential adverse reactions
TCAs (amitriptyline, desipramine, imipramine, nortriptyline)
↑ TCA toxicity (desipramine level doubles), proarrhythmic effects
SSRIs/SNRIs (fluoxetine, fluvoxamine, paroxetine, sertraline, venlafaxine)
fluvoxamine: Potentially dangerous ↑ in Methadone levels. Moderate Methadone ↑: fluoxetineMild Methadone ↑: paroxetine, venlafaxineQTc: fluoxetine, sertraline, venlafaxine
Antipsychotics (haloperidol, quetiapine, ziprasidone)
QTc prolongationQuetiapine: ↑ Methadone levels
Carbamazepine Strong CYP3A4 induction, opioid withdrawal common

Methadone-Drug Interactions: Other medications
Drug Effects
Barbituates Particularly phenobarbital, sharp ↓ in Methadone levels and opioid withdrawal
Phenytoin and Carbamazepine Sharp ↓ in Methadone levels
Rifampin Severe opioid withdrawal
Fluconazole (possible other azoles)
↑ Methadone levels
Macrolides (Erythromycin, Clarithromycin)
↑ Methadone levels
St. John’s Wort Significant ↓ in Methadone levels (47% in one study)
Grapefruit juice ↑ Methadone levels
Omeprazole May inhibit Methadone absorption
Cimetidine CYP450 enzyme inhibitor

Methadone-Drug Interactions: Substances of Abuse ETOH and Sedatives: additive effects,
risk for overdose
Cocaine: accelerates Methadone elimination
Methamphetamine: not studied in human pharmacokinetics studies
Tobacco: mixed reports, most indicate reduced effectiveness of Methadone

Case Study #1 48-year old male with Opioid and Cocaine
Dependence, HIV, Hep C+, and Depressive disorder
On Methadone 70mg daily, no illicit opioid use x 6 mos, continues to use crack cocaine 3-4x/wk
On Sertraline 100mg qbedtime for depression PCP wants to start pt on HIV meds. Some
concerns re possible adherence, but thinks stable enough. Prescribes Atripla 1 tab daily
Pt misses initial f/u appt with PCP, returns 4 wks later. States he relapsed on heroin and has been off all his medications, except for Methadone, for the past 2 wks
What do you do to help him?

Case Study #2 35-year old female with Opioid and
Methamphetamine Dependence, Hep C+, HTN, OCD and Anxiety d/o NOS
On Methadone 50mg daily and HCTZ 25mg daily Enters residential tx, does well, stops using
any illicit drugs, engages in psychiatric care and is started on Fluvoxamine 100mg daily and Clonazepam 0.5mg BID
You receive a call from her program stating that she has been nodding off in groups and they are concerned she is abusing her benzos
What can you do to help her?

Ward 93 Contact Information Referrals
Referral forms available at most clinics, ED, Wound Clinic, and Urgent Care
Fax referral form to Bryan Jackson at 206-6875 or call at 206-4288
Most pts admitted to 30-day or 90-day detox Direct admission to MMTP for pregnant pts or
Forensic AIDS Program (FAP) pts
To discuss medical concerns and coordinate care, phone 206-8412 and ask for the NP on call

Questions?