Embed Size (px)
DESCRIPTION
meth_info
Citation preview

What is methamphetamine?
Methamphetamine is apowerfully addictivestimulant that dramatical-
ly affects the central nervous
system. The drug is made easily in clandestine laboratories with relatively inexpensive over-the-counter ingredients. These factors combine to make meth-amphetamine a drug with highpotential for widespread abuse.
The abuse of methampheta-mine – a potent psychostimulant– is an extremely serious andgrowing problem. Although thedrug was first used primarily inselected urban areas in theSouthwestern part of the UnitedStates, we now are seeing high levels of methamphetamine abusein many areas of the Midwest, inboth urban and rural settings, andby very diverse segments of thepopulation.
As part of our Methamphet-amine Research Initiative, theNational Institute on Drug Abuse(NIDA) has developed this publi-cation to provide an overview ofthe latest scientific findings on thisdrug. Methamphetamine is a powerfully addictive stimulantassociated with serious health conditions, including memoryloss, aggression, psychotic behavior, and potential heart andbrain damage; it also contributesto increased transmission ofhepatitis and HIV/AIDS.
One of NIDA’s most impor-tant goals is to translate what scientists learn from research tohelp the public better understanddrug abuse and addiction and todevelop more effective strategiesfor their prevention and treat-ment. We hope this compilation ofscientific information on methamphetamine will helpinform readers about the harmfuleffects of methamphetamine abuseand will assist in prevention andtreatment efforts.
Alan I. Leshner, Ph.D.DirectorNational Institute on Drug Abusefr
om
th
e d
ire
cto
r
U . S . D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s ● N a t i o n a l I n s t i t u t e s o f H e a l t h
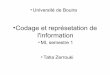
Methamphetamine and amphetamine use is on the rise.
Source: Drug Abuse Warning Network, SAMHSA, 1997
1994
Q10
1
2
3
4
5
6
Methamphetamine
Amphetamine
Q2 Q3 Q4
1995
Q1 Q2 Q3 Q4
1996
Q1 Q2 Q3 Q4
Quarterly emergency room episodes due to stimulant use weretracked from 1994 to 1996. A shortage of methamphetamine wasreported by epidemiologists during the last half of 1995 accountingfor the significant decrease in ER episodes.
Thou
sand
s
METHAMPHETAMINEAbuse and Addiction

Methamphetamine is com-monly known as “speed,” “meth,”and “chalk.” In its smoked formit is often referred to as “ice,”“crystal,” “crank,” and “glass.” Itis a white, odorless, bitter-tastingcrystalline powder that easily dis-solves in water or alcohol. Thedrug was developed early in thiscentury from its parent drug,amphetamine, and was used origi-nally in nasal decongestants andbronchial inhalers.Methamphetamine’s chemicalstructure is similar to that ofamphetamine, but it has morepronounced effects on the centralnervous system. Like ampheta-mine, it causes increased activity,decreased appetite, and a generalsense of well-being. The effectsof methamphetamine can last 6 to8 hours. After the initial “rush,”there is typically a state of highagitation that in some individualscan lead to violent behavior.
Methamphetamine is aSchedule II stimulant, whichmeans it has a high potential forabuse and is available onlythrough a prescription that can-not be refilled. There are a fewaccepted medical reasons for itsuse, such as the treatment of nar-colepsy, attention deficit disor-der, and––for short-termuse––obesity; but these medicaluses are limited.
What is the scope ofmethamphetamineabuse in the United States?
Methamphetamine abuse,long reported as the dom-inant drug problem in the
San Diego, CA, area, has become
a substantial drug problem inother sections of the West andSouthwest, as well. There areindications that it is spreading toother areas of the country,including both rural and urbansections of the South andMidwest. Methamphetamine, tra-ditionally associated with white,male, blue-collar workers, isbeing used by more diverse popu-lation groups that change overtime and differ by geographicarea.
According to the 1996National Household Survey onDrug Abuse, an estimated 4.9million people (2.3 percent of thepopulation) have tried metham-phetamine at some time in theirlives. In 1994, the estimate was3.8 million (1.8 percent), and in1995 it was 4.7 million (2.2 per-cent).
Data from the 1996 DrugAbuse Warning Network(DAWN), which collects infor-mation on drug-related episodesfrom hospital emergency depart-ments in 21 metropolitan areas,reported that methamphetamine-related episodes decreased by 39percent between 1994 and 1996,after a 237 percent increasebetween 1990 and 1994. Therewas a statistically significantdecrease in methamphetamine-related episodes between 1995(16,200) and 1996 (10,800).However, there was a significantincrease of 71 percent betweenthe first half of 1996 and the sec-ond half of 1996 (from 4,000 to6,800).
NIDA’s CommunityEpidemiology Work Group(CEWG), an early warning net-work of researchers that provides
2 NIDA RESEARCH REPORT SERIES
100
80
60
40
20
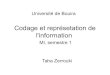
0Hawaii San Diego San Francisco
96
36
11
1
38
27
<1
23
57
Smoking
Sniffing
Injecting
Area
The preferred method of taking methamphetamine varies among geographical regions.
Note: Calendar year in Hawaii and San Diego; State fiscal year in San FranciscoSource: Community Epidemiology Work Group, NIDA 1997
Perc
ent

information about the nature andpatterns of drug use in majorcities, reported in its June 1997publication that methampheta-mine continues to be a problemin Hawaii and in major Westerncities, such as San Francisco,Denver, and Los Angeles.Increased methamphetamineavailability and production arebeing reported in diverse areas ofthe country, particularly ruralareas, prompting concern aboutmore widespread use.
Drug abuse treatment admis-sions reported by the CEWG inDecember 1996 showed thatmethamphetamine remained theleading drug of abuse amongtreatment clients in the SanDiego area and was second onlyto marijuana in Hawaii.Stimulants, including metham-phetamine, accounted for smallerpercentages of treatment admis-
sions in other states and metro-politan areas of the West (e.g., 5percent in Los Angeles andSeattle and 4 percent in Texas andSan Francisco). By comparison,stimulants were the primarydrugs of abuse in less than 1 per-cent of treatment admissions inmost Eastern and Midwesternmetropolitan areas, except inMinneapolis-St. Paul and St.Louis, where they accounted forapproximately 2 percent of totaladmissions.
How is methamphetamineused?
Methamphetamine comes inmany forms and can besmoked, snorted, orally
ingested, or injected. The drug
alters moods in different ways,depending on how it is taken.
Immediately after smokingthe drug or injecting it intra-venously, the user experiences anintense rush or “flash” that lastsonly a few minutes and isdescribed as extremely pleasur-able. Snorting or oral ingestionproduces euphoria––a high butnot an intense rush. Snortingproduces effects within 3 to 5minutes, and oral ingestion pro-duces effects within 15 to 20minutes.
As with similar stimulants,methamphetamine most often isused in a “binge and crash” pat-tern. Because tolerance formethamphetamine occurs withinminutes––meaning that the plea-surable effects disappear evenbefore the drug concentration inthe blood falls significantly––users try to maintain the high by
NIDA RESEARCH REPORT SERIES 3
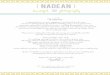
The brain – Dopamine plays an important role in the regulation of pleasure. In addition to otherregions, dopamine is manufactured in nerve cells within the ventral tegmental area and is released in the nucleus accumbens and the frontal cortex.
MethamphetamineDopamine
Methamphetamine stimulatesexcess release of dopamine.

binging on the drug. In the 1980’s, “ice,” a smok-
able form of methamphetamine,came into use. Ice is a large, usu-ally clear crystal of high puritythat is smoked in a glass pipe likecrack cocaine. The smoke is odor-less, leaves a residue that can beresmoked, and produces effectsthat may continue for 12 hours ormore.
What are the immediate(short-term) effects of methamphetamineabuse?
As a powerful stimulant,methamphetamine, even in small doses, can increase
wakefulness and physical activityand decrease appetite. A brief,intense sensation, or rush, isreported by those who smoke orinject methamphetamine. Oralingestion or snorting produces along-lasting high instead of arush, which reportedly can con-tinue for as long as half a day.Both the rush and the high arebelieved to result from the releaseof very high levels of the neuro-transmitter dopamine into areasof the brain that regulate feelingsof pleasure.
Methamphetamine has toxiceffects. In animals, a single highdose of the drug has been shownto damage nerve terminals in thedopamine-containing regions ofthe brain. The large release ofdopamine produced by metham-phetamine is thought to con-
tribute to the drug’s toxic effectson nerve terminals in the brain.High doses can elevate body tem-perature to dangerous, sometimeslethal, levels, as well as cause con-vulsions.
What are the long-termeffects of methamphetamineabuse?
Long-term methamphetamineabuse results in many damag-ing effects, including addic-
tion. Addiction is a chronic,relapsing disease, characterized bycompulsive drug-seeking and druguse which is accompanied byfunctional and molecular changesin the brain. In addition to beingaddicted to methamphetamine,chronic methamphetamineabusers exhibit symptoms thatcan include violent behavior, anxi-ety, confusion, and insomnia.They also can display a number ofpsychotic features, including
paranoia, auditory hallucinations,mood disturbances, and delusions(for example, the sensation ofinsects creeping on the skin,called “formication”). The para-noia can result in homicidal aswell as suicidal thoughts.
With chronic use, tolerancefor methamphetamine can devel-op. In an effort to intensify thedesired effects, users may takehigher doses of the drug, take itmore frequently, or change theirmethod of drug intake. In some
cases, abusers forego food andsleep while indulging in a form ofbinging known as a “run,” inject-ing as much as a gram of the drugevery 2 to 3 hours over severaldays until the user runs out of thedrug or is too disorganized tocontinue. Chronic abuse can leadto psychotic behavior, character-ized by intense paranoia, visualand auditory hallucinations, andout-of-control rages that can becoupled with extremely violentbehavior.
Although there are no physi-cal manifestations of a withdrawal
4 NIDA RESEARCH REPORT SERIES
Long-term effects can include:
Dependence and addiction psychosis
– paranoia– hallucinations– mood
disturbances– repetitive motor
activityStrokeWeight loss
Short-term effects can include:
Increased attention and decreased fatigue
Increased activity
Decreased appetite
Euphoria and rush
Increased respiration
Hyperthermia

syndrome when methampheta-mine use is stopped, there areseveral symptoms that occurwhen a chronic user stops takingthe drug. These include depres-sion, anxiety, fatigue, paranoia,aggression, and an intense cravingfor the drug.
In scientific studies examiningthe consequences of long-termmethamphetamine exposure inanimals, concern has arisen overits toxic effects on the brain.Researchers have reported that asmuch as 50 percent of thedopamine-producing cells in thebrain can be damaged after pro-longed exposure to relatively lowlevels of methamphetamine.Researchers also have found thatserotonin-containing nerve cellsmay be damaged even moreextensively. Whether this toxicityis related to the psychosis seen insome long-term methampheta-mine abusers is still an openquestion.
How is methamphetaminedifferent fromother stimulants,like cocaine?
Methamphetamine is classi-fied as a psychostimulant as are such other drugs
of abuse as amphetamine andcocaine. We know that metham-phetamine is structurally similarto amphetamine and the neuro-transmitter dopamine, but it isquite different from cocaine.Although these stimulants havesimilar behavioral and physiologi-cal effects, there are some majordifferences in the basic mecha-nisms of how they work at thelevel of the nerve cell. However,the bottom line is that metham-phetamine, like cocaine, results inan accumulation of the neuro-transmitter dopamine, and thisexcessive dopamine concentrationappears to produce the stimula-
tion and feelings of euphoriaexperienced by the user. In con-trast to cocaine, which is quicklyremoved and almost completelymetabolized in the body,methamphetamine has a muchlonger duration of action and alarger percentage of the drugremains unchanged in the body.This results in methamphetaminebeing present in the brain longer,which ultimately leads to pro-longed stimulant effects.
What are the medical complications ofmethamphetamineabuse?
Methamphetamine cancause a variety of cardio-vascular problems. These
include rapid heart rate, irregularheartbeat, increased blood pres-sure, and irreversible, stroke-pro-ducing damage to small bloodvessels in the brain.Hyperthermia (elevated bodytemperature) and convulsionsoccur with methamphetamineoverdoses, and if not treatedimmediately, can result in death.
Chronic methamphetamineabuse can result in inflammationof the heart lining, and amongusers who inject the drug, dam-aged blood vessels and skinabscesses. Methamphetamineabusers also can have episodes ofviolent behavior, paranoia, anxi-ety, confusion, and insomnia.Heavy users also show progres-sive social and occupational dete-rioration. Psychotic symptoms
NIDA RESEARCH REPORT SERIES 5
Although both methamphetamine and cocaine are psychostimulants, there are differences between them.
Methamphetamine vs.
Man-made
Smoking produces a highthat lasts 8-24 hours
50% of the drug is removed from the body in 12 hours
Limited medical use
Cocaine
Plant-derived
Smoking produces a highthat lasts 20-30 minutes
50% of the drug is removedfrom the body in 1 hour
Used as a local anesthetic insome surgical procedures

can sometimes persist for monthsor years after use has ceased.
Acute lead poisoning isanother potential risk formethamphetamine abusers. Acommon method of illegalmethamphetamine productionuses lead acetate as a reagent.Production errors may thereforeresult in methamphetamine contaminated with lead. Therehave been documented cases ofacute lead poisoning in intra-venous methamphetamineabusers.
Fetal exposure to metham-phetamine also is a significantproblem in the United States. Atpresent, research indicates thatmethamphetamine abuse duringpregnancy may result in prenatalcomplications, increased rates ofpremature delivery, and alteredneonatal behavioral patterns, suchas abnormal reflexes and extremeirritability. Methamphetamineabuse during pregnancy may belinked also to congenital deformi-ties.
Are methamphetamineabusers at risk for contractingHIV/AIDS andhepatitis B and C?
Increased HIV and hepatitis Band C transmission are likelyconsequences of increased
methamphetamine abuse, particu-larly in individuals who inject thedrug and share injection equip-ment. Infection with HIV andother infectious diseases is spread
among injection drug users pri-marily through the reuse of cont-aminated syringes, needles, orother paraphernalia by more thanone person. In nearly one-thirdof Americans infected with HIV,injection drug use is a risk factor,making drug abuse the fastestgrowing vector for the spread ofHIV in the nation.
Research also indicates thatmethamphetamine and relatedpsychomotor stimulants canincrease the libido in users, incontrast to opiates which actuallydecrease the libido. However,long-term methamphetamine usemay be associated with decreasedsexual functioning, at least inmen. Additionally, methampheta-mine seems to be associated withrougher sex which may lead tobleeding and abrasions. The com-bination of injection and sexualrisks may result in HIV becom-ing a greater problem amongmethamphetamine abusers thanamong opiate and other drugabusers, something that alreadyseems to be occurring inCalifornia.
NIDA-funded research hasfound that, through drug abusetreatment, prevention, and com-munity-based outreach programs,drug abusers can change theirHIV risk behaviors. Drug use canbe eliminated and drug-relatedrisk behaviors, such as needle-sharing and unsafe sexual prac-tices, can be reduced significantlythus decreasing the risk of expo-sure. Therefore, drug abuse treat-ment is also highly effective inpreventing the spread of HIV,hepatitis B, and hepatitis C.
What treatmentsare effective formethamphetamineabusers?
At this time the most effec-tive treatments formethamphetamine addic-
tion are cognitive behavioralinterventions. These approachesare designed to help modify thepatient’s thinking, expectancies,and behaviors and to increaseskills in coping with various lifestressors. Methamphetaminerecovery support groups alsoappear to be effective adjuncts tobehavioral interventions that canlead to long-term drug-freerecovery.
There are currently no partic-ular pharmacological treatmentsfor dependence on amphetamineor amphetamine-like drugs suchas methamphetamine. The cur-rent pharmacological approach isborrowed from experience withtreatment of cocaine dependence.Unfortunately, this approach hasnot met with much success sinceno single agent has proven effica-cious in controlled clinical stud-ies. Antidepressant medicationsare helpful in combating thedepressive symptoms frequentlyseen in methamphetamine userswho recently have become absti-nent.
There are some establishedprotocols that emergency roomphysicians use to treat individualswho have had a methampheta-mine overdose. Because hyper-thermia and convulsions are com-mon and often fatal complica-tions of such overdoses, emer-
6 NIDA RESEARCH REPORT SERIES

gency room treatment focuses onthe immediate physical symp-toms. Overdose patients arecooled off in ice baths, and anti-convulsant drugs may be admin-istered also.
Acute methamphetamineintoxication can often be handledby observation in a safe, quietenvironment. In cases of extremeexcitement or panic, treatmentwith antianxiety agents such asbenzodiazepines has been helpful,and in cases of methampheta-mine-induced psychoses, short-term use of neueptics has provensuccessful.
Where can I getfurther scientificinformation aboutmethamphetamineabuse?
To learn more about metham-phetamine and other drugsof abuse, contact the
National Clearinghouse forAlcohol and Drug Information(NCADI) at 1-800-729-6686.Information specialists are avail-able to assist you in locatingneeded information andresources. Information can beaccessed also through the NIDAWorld Wide Web site(http://www.nida.nih.gov) or theNCADI Web site(http://www.health.org).
Fact sheets on health effectsof drug abuse and other topicscan be ordered free of charge, inEnglish and Spanish, by callingNIDA INFOFAX at 1-800-NIH-NIDA (1-800-644-6432) or
1-888-TTY-NIDA (1-888-889-6432)for the hearing impaired.
A list of fact sheet topics follows:HHeeaalltthh EEffffeeccttss ooff SSppeecciiffiicc DDrruuggss
•Cigarettes and other tobacco products
•Crack and cocaine•Ecstasy•Heroin•Inhalants•LSD•Marijuana•Methamphetamine•Pain medications•PCP•Ritalin•Rohypnol and GHB•Steroids (anabolic)
DDrruugg AAbbuussee aanndd AAIIDDSSLLeessssoonnss ffrroomm PPrreevveennttiioonn
RReesseeaarrcchhTTrreeaattmmeenntt RReesseeaarrcchh
•Treatment methods•Treatment medications•Treatment methods for women
•Behavior change through treatment
TTrreennddss aanndd SSuurrvveeyyss•Costs to society from drug abuse
•High school and youth trends
•Hospital visits and deaths•Nationwide trends•Pregnancy and drug abuse trends
•Treatment trends•Workplace trends
NNeewwss RReelleeaasseess oonn RReesseeaarrcchh FFiinnddiinnggss
IInnffoorrmmaattiioonn aabboouutt NNIIDDAA•Home page on the WorldWide Web
•Mission and structure
•Opportunities for special populations
•Funding opportunities•Upcoming events and conferences
OOtthheerr DDrruugg AAbbuussee IInnffoorrmmaattiioonn SSeerrvviicceess
NIDA web sitehttp://www.nida.nih.gov
Access information on the internet
• What’s new on the NIDA web site
• Information on drugs of abuse
• Publications and communications (including NIDA Notes)
• Calendar of events• Links to NIDA
organizational units• Funding information
(including program announcements and deadlines)
• International activities• Links to related
web sites (access to web sites of many other organizations in the field)
NCADI web sitehttp://www.health.org
NIDA RESEARCH REPORT SERIES 7

8NIDA RESEARCH REPORT SERIES
GlossaryAAddddiiccttiioonn:: a chronic, relapsingdisease, characterized by compul-sive drug-seeking and drug useand by neurochemical and molec-ular changes in the brain.
AAnnaalloogg:: a chemical compoundthat is similar to another drug inits effects but differs slightly in itschemical structure.
BBeennzzooddiiaazzeeppiinneess:: drugs thatrelieve anxiety or are prescribedas sedatives; among the mostwidely prescribed medications,including valium and librium.
CCeennttrraall nneerrvvoouuss ssyysstteemm ((CCNNSS))::the brain and spinal cord.
CCrraavviinngg:: a powerful, oftenuncontrollable desire for drugs.
DDeessiiggnneerr ddrruugg:: an analog of arestricted drug that has psychoac-tive properties.
DDeettooxxiiffiiccaattiioonn:: a process ofallowing the body to rid itself of adrug while managing the symp-toms of withdrawal; often the firststep in a drug treatment program.
DDooppaammiinnee:: a neurotransmitterpresent in regions of the brainthat regulate movement, emotion,motivation, and feelings of plea-sure.
NNaarrccoolleeppssyy:: a disorder character-ized by uncontrollable attacks ofdeep sleep.
PPhhyyssiiccaall ddeeppeennddeennccee:: an adap-tive physiological state that occurswith regular drug use and resultsin a withdrawal syndrome whendrug use stops.
PPssyycchhoossiiss:: a mental disordercharacterized by symptoms suchas delusions or hallucinations thatindicate an impaired conceptionof reality.
RRuusshh:: a surge of euphoric plea-sure that rapidly follows adminis-tration of a drug.
SSeerroottoonniinn:: a neurotransmitter thathas been implicated in states ofconsciousness, mood, depression,and anxiety.
TToolleerraannccee:: a condition in whichhigher doses of a drug arerequired to produce the sameeffect as experienced initially;often leads to physical depen-dence.
TTooxxiicc:: temporary or permanentdrug effects that are detrimentalto the functioning of an organ orgroup of organs.
WWiitthhddrraawwaall:: a variety of symp-toms that occur after use of anaddictive drug is reduced orstopped.
Resources"Blood Level of Intravenous Drug Users," by R.L.
Norton, B.T. Burton, and J. McGirr. Journal of Clinical Toxicology 34(4):425-30, 1996.
Epidemiologic Trends in Drug Abuse: Vol. 1. Highlights and Executive Summary of the Community Epidemiology Work Group, June 1997. NIH Pub. No. 98-4207. National Institute on Drug Abuse, 1997.
Epidemiologic Trends in Drug Abuse: Vol. 1. Highlights and Executive Summary of the Community Epidemiology Work Group, December 1996. NIH Pub. No. 97-4204. National Institute on Drug Abuse, 1997.
"Integrating Treatments for Methamphetamine Abuse:A Psychosocial Perspective," by A. Huber, W. Ling, S. Shoptaw, V. Gulati, P. Brethen, and R. Rawson.Journal of Addictive Diseases, 16(4):41-50, 1997.
"Like Methamphetamine, Ecstacy May Cause Long-Term Brain Damage," by R. Mathias. NIDA Notes 11:7, 1996.
Methamphetamine Abuse (NIDA Capsules). National Institute on Drug Abuse, September 1997.
National Methamphetamine Strategy. U.S. Department of Justice, 1996.
National Survey Results on Drug Use From the Monitoring the Future Study, 1975-1994, Vol. I: Secondary School Students. NIH Pub. No. 93-3498. National Institute on Drug Abuse, 1995.
National Survey Results on Drug Use From the Monitoring the Future Study, 1975-1994, Vol. II: College Students and Young Adults. NIH Pub. No. 96-4027. National Institute on Drug Abuse, 1995.
"NIDA Survey Provides First National Data on Drug Abuse During Pregnancy," by R. Mathias. NIDA Notes 10:6-7, 1995.
“Preliminary Results from the 1996 National Household Survey on Drug Abuse”. Substance Abuse and Mental Health Services Administration, 1997.
Year-End Preliminary Estimates from the 1996 Drug Abuse Warning Network. Substance Abuse and Mental Health Services Administration, November 1997.
NIH Publication Number 98-4210.Printed April 1998.Feel free to reprint this publication.