Embed Size (px)
DESCRIPTION
Tratamento do cancer atraves do metabolismo e nutriçao
Citation preview

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
Cell Cycle 12:8, 1166–1179; April 15, 2013; © 2013 Landes Bioscience
PersPeCtive
1166 Cell Cycle volume 12 issue 8
Keywords: Warburg effect, reprogram-ming, cancer stem cells, metabolism, stemness, pluripotency
Submitted: 03/20/13
Accepted: 03/27/13
http://dx.doi.org/10.4161/cc.24479
*Correspondence to: Javier A. Menendez and Alejandro Vazquez-Martin; Email: [email protected] or [email protected] and [email protected] or [email protected]
When fighting cancer, knowledge on metabolism has always been
important. Today, it matters more than ever. The restricted cataloging of can-cer genomes is quite unlikely to achieve the task of curing cancer, unless it is integrated into metabolic networks that respond to and influence the constantly evolving cancer stem cell (CSC) cellu-lar states. Once the genomic era of car-cinogenesis had pushed the 1920s Otto Warburg’s metabolic cancer hypoth-esis into obscurity for decades, the most recent studies begin to support a new developing paradigm, in which the molecular logic behind the conversion of non-CSCs into CSCs can be better understood in terms of the “metabolic facilitators” and “metabolic impedi-ments” that operate as proximate open-ings and roadblocks, respectively, for the transcriptional events and signal transduction programs that ultimately orchestrate the intrinsic and/or microen-vironmental paths to CSC cellular states. Here we propose that a profound under-standing of how human carcinomas install a proper “Warburg effect version 2.0” allowing them to “run” the CSCs’ “software” programs should guide a new era of metabolo-genomic-personalized cancer medicine. By viewing metabolic reprogramming of CSCs as an essen-tial characteristic that allows dynamic,
The Warburg effect version 2.0Metabolic reprogramming of cancer stem cells
Javier A. Menendez,1,2,†,‡,* Jorge Joven,3,† Sílvia Cufí,1,2 Bruna Corominas-Faja,1,2 Cristina Oliveras-Ferraros,1,2 Elisabet Cuyàs,1,2 Begoña Martin-Castillo,2,4 Eugeni Lopez-Bonet,2,5 Tomás Alarcón6 and Alejandro Vazquez-Martin1,2,‡,*1Metabolism & Cancer Group; Translational Research Laboratory; Catalan Institute of Oncology-Girona (ICO-Girona); Girona, Spain; 2Molecular
Oncology; Girona Biomedical Research Institute (IDIBGi); Girona, Spain; 3Unitat de Recerca Biomèdica (URB-CRB); Institut d’Investigació Sanitaria
Pere i Virgili (IISPV); Universitat Rovira i Virgili; Reus, Spain; 4Clinical Research Unit; Catalan Institute of Oncology-Girona (ICO-Girona); Girona, Spain; 5Department of Anatomical Pathology; Dr. Josep Trueta University Hospital; Girona, Spain; 6Computational & Mathematical Biology Research Group; Centre
de Recerca Matemàtica (CRM); Barcelona, Spain†These authors contributed equally to this work.‡These authors share co-senior authorship.
multidimensional and evolving cancer populations to compete successfully for their expansion on the organism, we now argue that CSCs bioenerget-ics might be another cancer hallmark. A definitive understanding of metabolic reprogramming in CSCs may comple-ment or to some extent replace, the 30-y-old paradigm of targeting oncogenes to treat human carcinomas, because it can be possible to metabolically create non-permissive or “hostile” metabotypes to prevent the occurrence of CSC cellular states with tumor- and metastasis-initi-ating capacity.
Over the past 30 y, oncology research has been dominated by a genocentric view of discovery. Information is no longer a bottleneck to understanding the ultimate genetic complexity of cancer diseases, because we have not yet reached a plateau in the advances in genome sequencing and editing. However, the process of discovery and the approval of new oncology drugs have stagnated during the past decade. Today, although a large catalog of human cancer genomes exists, the success rate of new drugs reaching cancer patients is extremely low, with the regulatory agen-cies approving only a small proportion of the drugs entering phase I clinical tri-als.1-3 Cancer remains one of the leading causes of death in Europe and the US, and

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1167
PersPeCtive PersPeCtive
approved a single novel oncology therapy agent in the last two years reflects our inability to discover and develop magic-bullet therapies against the thousands of genes that can be mutated in every can-cer type. More than 100,000 point cancer mutations have been identified to date, and more than 350 of these mutations are thought to influence the cancer phe-notype.7-12 Targeted therapies, i.e., drugs developed to interfere with specific can-cer gene products, have been a dominant research focus in cancer biology over the past 30 y but have translated into few novel oncology treatments. Several expla-nations may support the current state of cancer research. First, most cancer genes are tumor suppressors, which are either inactivated or completely lost in tumor cells; tumor suppressors are not drug-gable targets for the easily designed small molecules that are commonly devel-oped to block oncoprotein hyperactivity. Second, many oncogenic gains-of-func-tion, including those for the commonly deregulated non-enzymatic transcription factors, are also difficult to target. Third, most newly identified candidate cancer genes, including genes that represent good drug targets, exhibit very low mutation frequencies, indicating that these genes may represent passenger noise in geneti-cally unstable tumors. Indeed, part of the difficulty in identifying appropriate drug targets is that passenger mutations greatly outnumber the bona fide mutations that are required for cancer development, called driver mutations. For example, recent genome analyses of 500 primary breast cancer samples revealed 27,000 point mutations; however, less than 0.01% of these mutations are thought to repre-sent potential drivers.12 The development of most common cancers requires multiple driver mutations; therefore, these can-cers generally develop slowly over many years. Thus, the mutations that facilitate an essential malignant function early in cancer development may no longer be required at the relatively late stage when the tumor is clinically detected.13 These results may compromise the current efforts of the International Cancer Genome Consortium in coordinating a global gen-otype assessment of 500 tumor samples from 50 cancer types.14 The genotyping
that cancer solutions will be generated exclusively by large, expensively managed projects rather than simple approaches.6 Complementary, we hypothesize that it is time to revisit the 1920s and remember Otto Warburg’s original, simple meta-bolic hypothesis for cancer, which states that “the prime cause of cancer is the replacement of the respiration of oxygen (oxidation of sugar) in normal body cells by fermentation of sugar.”
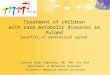
This thinking might unexpectedly clarify the modern hypotheses in cancer pathophysiology, one of which states that the molecularly distinct subpopulation of so-called cancer stem cells (hereafter CSCs) are responsible for many, if not all, aspects of tumorigenesis, including the clinical failure of the majority of avail-able oncology therapies and the existence of persistent, deadly metastases. We now propose a new version 2.0 of the Warburg effect that incorporates bioenergetics to the operational properties of CSCs (Fig. 1).
The End of a 30-Year-Old Paradigm for Targeting Cancer
Genes to Cure Cancer
Current cancer drug discovery: The genome scenario. The fact that regulatory agencies such as the US FDA have not
as a consequence of the aging population, the incidence of cancer is rising (as dem-onstrated in the cancer fact sheet4 pub-lished on the World Health Organization website). Although the US Food and Drug Administration (FDA)’s Critical Path Initiative5 was launched in 2004 to streamline the development process of new drugs, the US FDA has not approved a single novel agent in oncology in the last two years, and the success rate of major oncology-pharma and -biotechs is lower than ever. The lack of success in the cur-rent cancer drug-discovery progress is fur-ther exacerbated by the typical cytostatic, transient response to novel single-path-way-targeting drugs, which has resulted in an unacceptable situation, wherein we are progressing into more personalized approaches for providing effective cancer therapy in a post-genomics world. Rather than recurrently boosting genomics and other human “cancer-omics”-project-like approaches, such as cancer proteomics and cancer epigenomics, “to drive innovation in the scientific processes through which oncology products are developed […],”5 perhaps we should consider that the 30-y-old paradigm of targeting cancer genes to treat human carcinomas is reaching its end.
Because cancer is a very complex, mul-tifactorial disease, it has been assumed
Figure 1. the Warburg effect version 2.0: Coloring an old, black and white picture. Because cancer is a very complex, multifactorial disease, it has been erroneously assumed that cancer solutions will be generated exclusively by large, expensive managed projects rather than simple approaches. instead, it is time to revisit the 1920s and remember Otto Warburg’s original, simple metabolic hypothesis for cancer, which states “the prime cause of cancer is the replacement of the respiration of oxygen (oxidation of sugar) in normal body cells by fermentation of sugar.” this thinking would now clarify the modern hypotheses in cancer pathophysiology, one of which states that the molecularly distinct subpopulation of so-called CsCs are responsible for many, if not all, aspects of tumorigenesis, including the clinical failure of the majority of available oncol-ogy therapies and the existence of persistent, deadly metastases.

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
1168 Cell Cycle volume 12 issue 8
Stochastic transitions of drug-responsive CSCs may also produce non-CSCs that lack the major CSC attributes and that can therefore remain hidden from drugs that are aimed to attack the CSC self-renewing machinery.
Targeting CSCs: We aim for hid-den and moving targets. Although recent breakthroughs have highlighted the importance of some subsets of non-druggable transcription factors and epi-genetic modifiers in the establishment, maintenance and reprogramming of CSC-like cellular identities, few anti-CSC drugs have been identified, and none have been approved for clinical use. Virtually all CSC-related drug discovery studies have genocentrically focused on ultimate causes, which generally involve the molec-ular mechanisms by which some cells elicit all of the unique properties that are commonly associated with the CSC cellu-lar phenotype, such as immortality, self-renewal and cross-resistance to multiple treatments. However, because normal and non-CSC tumor cells can spontaneously convert to CSCs, i.e., CSCs are also made and not just born, an emerging consensus in the field is that the cellular state rather than the cellular phenotype is crucial to defining and investigating CSCs. This model indicates that, whereas CSCs can likewise differentiate into non-CSCs, non-CSCs may also be reprogrammed and converted to CSCs, suggesting the existence of a dynamic intercon-version between CSCs and non-CSCs cellular states that is controlled by cell-autonomous and non-cell autonomous mechanisms (Fig. 2). The balance of the CSCs/non-CSCs interconversion could be shifted in one direction or another in response to intrinsic and/or microenviron-mental signals, which may in part account for the frequency of CSC representation between different tumor types or within a tumor progressing through different stages. Such plasticity of the CSC cellular state is absent in the conventional depic-tion of the stem/progenitor cell hierarchy within a normal tissue being transformed into one-way CSCs hierarchy, and has revolutionary changed our current percep-tion of CSCs biology. Finally, but still cru-cially important, a subset of CSCs appears to be exclusively responsible for metastatic
conventional therapies with hormones, radiation, chemotherapeutic agents and also to molecularly targeted drugs; the differential behavior of CSCs in their responsiveness to treatment may largely explain the differences in the efficacy of therapy among cancer patients with com-parable tumors by histopathological anal-ysis. Together with their ability to colonize distant organs, CSCs have been therefore proposed to be ultimately responsible for the clinical failure of the majority of cur-rently available oncology therapies and for metastases that appear after surgical treat-ment and/or systemic therapy of primary tumors.21-25
CSCs are also made not just born. Carcinogenesis involves the accumulation of numerous oncogenic events over long periods of time. In tumors that originate from tissues with high epithelial cellular turnover, only normal SCs, with their innate self-renewal capacity, remain in the tissue long enough to accumulate the oncogenic alterations necessary to support a complete transformation. Accordingly, adult SCs have been hypothesized to represent the cells-of-origin in cancer, because they can be directly targeted with CSC initiation events. Progenitor cells may similarly gain the ability to self-renew through oncogenic transformation. In this traditional view of a one-way CSC hierarchy, all of the cancer cells within a tumor arise from special self-renewing CSCs. However, although CSCs obvi-ously exhibit the SC properties of self-renewal and differentiation, they do not necessarily originate from the transforma-tion of normal tissue SCs or progenitor cells. Individual tumors generally harbor multiple phenotypically or genetically dis-tinct CSCs because differentiated, either normal or non-SC tumor cells can gain CSC cellular properties, e.g. drug refrac-toriness via the activation of still par-tially known paths to stemness.26-31 The unstable CSC phenotype continuously evolves and can be switched on or off in response to cell-intrinsic or microenviron-mental cues including therapeutics. The inherent plasticity of the CSC phenotype implies that eliminating CSCs alone may not effectively cure tumors, as they can be regenerated from non-CSCs, calling for dual targeting therapeutic regiments.
for each set of tumor samples is estimated to cost 20 million dollars, which totals over 1 billion dollars for all 50 cancer types, and will facilitate the identification of driver mutations that occur at frequen-cies as low as 3%.15 With the identifica-tion of new genetic cancer subtypes, up to 1,000 tumor samples from each cancer type should be genotyped to identify all of the clinically relevant driver mutations.16 From a cancer drug discovery perspective, it is not surprising that heavy operational bias exists toward targeting signaling pathway kinases; however, because onco-genic networks maintain essential features for robustness, such as modularity and redundancy,16 signaling pathway kinases are subject to the rapid onset of resistance phenomena via compensatory pathways. In this regard, the approximately 10 y and 1 billion dollars required to bring an oncology therapy to Phase III (at which point the therapies often fail) raise ques-tions regarding the value of the hundreds of potential new therapies we are accumu-lating through our ever-growing integra-tive capacity to distinguish driver from passenger genetic mutations. The devel-opment of additional molecular therapies could place an immense strain on our healthcare systems.
The wrong scenario: We are miss-ing the target. In the 1970s, a new para-digm emerged with respect to the origin of epithelial malignancies. In a manner similar to hematological tumors, malig-nant stem cells, with their aberrant capac-ity for auto-renewal and differentiation, were implicated as the drivers of the ori-gin, growth and metastatic dissemina-tion of most epithelial carcinomas. Since then, an ever-growing number of studies have repeatedly suggested the existence of molecularly distinct subpopulations of cancer cells that have been termed tumor-initiating cells, tumor-propagating cells or CSCs. This subset of cancer cells are exclusively able to propagate tumor growth, and they have the ability of self-renewal and differentiate into multiple cell lineages, the two hallmark characteristics of normal stem cells (hereafter SCs), thus crucially contributing to the phenotypic and functional heterogeneity of a diverse array of cancer types.17-20 CSCs have been shown to be more resistant to a variety of

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1169
itself would be the sole credible target in CSCs, we propose that Warburg’s think-ing that reprogramming of the bioener-getic cancer cell state should be considered the metabolic switch defining the “root of cancer”36,37 almost a century ago might now clarify the immediate cause(s) through which the cells-of-origin in can-cer appropriate the core machinery to sup-port self-renewing cell divisions that are generally restricted to normal SCs and, as a result, become CSCs. Previously, sci-entists believed that metabolic changes were a mere consequence of the aberrant cancer cell growth. However, the most recent experimental approaches from our laboratory begin to indirectly suggest that metabolic reprogramming of CSCs may have cancer-causing activity.38-48 By view-ing metabolic reprogramming of CSCs as an essential characteristic that allows dynamic, multidimensional and evolving cancer populations to compete success-fully for their expansion on the organism, we now argue that CSCs bioenergetics might be another cancer hallmark.
Metabolic reprogramming and can-cer: Chutes and ladders. The Canadian scientist Tak W. Mak, a world authority on the use of transgenic mice for cancer research, has recently stated that the “time has come to look at cancer in a differ-ent way, concentrating on processes that affect all tumor cells, or at least a majority, rather than an individual molecule […] treatments that target common features of cancer such as the metabolic abnor-malities that have been known for nearly 80 years definitely hold the possibility of helping more patients less expensively”.49,50 To better understand Professor Mak’s assertions, we must revisit the advance-ments and setbacks that have occurred along the time path of cell metabolism and cancer investigation, which certainly resembles the ancient Indian board game Chutes and Ladders. If the arrival at the end of the board at the hundredth square means achieving a definitive understand-ing of the true molecular nature and clinical relevance of the unique CSCs’ metabolic infrastructure and functioning, the previous journey is full of scientific breakthroughs representative of a “lad-der,” and bad deeds (ironically, just from a metabolic perspective!) representative
differentiation capabilities are acquired traits, it might seem unwise to attack mark-ers of the CSC phenotype either alone or in combination with debulking standard-of-care agents. Directly targeting the CSC machinery, wherever is located, could be a promising strategy. Counterintuitively, therefore, the existence of a unique, shared molecular hallmark that would be amena-ble to drug therapy among the CSCs of all carcinomas and/or the distinct sub-types of a single type of tumor should be inves-tigated. In this regard, CSC-driven malig-nant progression might be envisioned as an evolving spatiotemporal heterogeneous structure that cannot be driven solely by irreversible genetic alterations;32-35 instead, CSC-driven malignant progression must be additionally determined by novel, non-genetic dimensions that operate as the proximate causes of the CSC cellular states (Fig. 2).
Under the assumption that the molecu-lar biology of the stemness transformation
spread, which is the final step in 90% of all fatal solid tumors. If an initial genetic defect in multi-potent adult SCs is not the sole mechanism for the generation of dynamically evolving CSC reservoirs, it follows that primary CSCs are not neces-sarily identical to metastatic CSCs.
A Metabolic Causation of CSC-like Cellular States: A New Paradigm
in Cancer Research
If normal, non-CSC tumor cells, CSCs and metastatic CSCs are flexible entities that can change state, how can we resolve the apparently impossible problem of dis-covering cancer drugs that specifically target CSC cellular states? Although it has been largely assumed that chemother-apy enriches residual cancer with CSCs, an accelerated production of new CSC populations from mature, differentiated cancer cell origins would also be concor-dant with the data. As self-renewal and
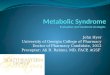
Figure 2. Metabolic reprogramming: A new parameter in the plasticity of the tumor cell differentiation-state that dictates the transition rates between non-CsC and CsC cellular states. Bidirectional interconversion exists between non-CsC and CsC cellular states. Any convergence toward phenotypic equilibrium in cancer cell state proportions likely occurs due to specific cancer cell state interconversion within tumors. Although the ultimate mechanisms stabilizing phenotypic proportions remain unclear, the transition rates between cell states, which vary across distinct cancer cell populations, have been suggested to largely depend on the intrinsic degree of differentiation-state plasticity dictated by genetic, epigenetic and/or microenvironmental (cell niche) parameters. indeed, current descriptions of cancer cell states, i.e., the set of charac-teristics that are informative for the transition between two cell states of interest, consist mostly of the levels of gene expression or the levels of epigenetic methylation or acetylation of DNA or chromatin. the final dimension of the non-CsC/CsC transitions is therefore mostly “hard-wired” by the genome. Our current model hypothesizes that the metabotype is an additional character-istic that, in addition to genetic determinants, epigenetics and extrinsic factors (niche), causally determines either “permissive” (P) or “non-permissive” (NP) features that lastly determine the number of additional requirements to gain the self-renewal capacity, potency and tumorigenicity possessed by CsC cellular states.

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
1170 Cell Cycle volume 12 issue 8
necessary, because carcinogenesis itself takes advantage of the elevated production of toxic glycolysis by-products, such as lactate. Increased glucose consumption in invasive and metastatic lesions is not used for substantial energy production (ATP) as is commonly assumed; rather, the glu-cose is used to produce acid, which gives the cancer cells a competitive advantage for invasion. Warburg aerobic glycolysis is elevated in tumors, because it invariably produces a toxic, acidic environment that, given that the acidic environment is more toxic to adjacent tissue compared than to the cancer cells themselves, represents an evolutionary advantage to cancer cells vis-à-vis the normal stroma into which they invade (ladder!). The recent milestone proposal by Vander Heiden, Cantley and Thompson emphatically rekindled inter-est in the Warburg effect in cancer.56 By answering the question “does aerobic gly-colysis arise in cancer cells merely because it is the most favorable metabotype for all rapidly proliferating cells with high glu-cose uptake capacity?”, the authors illu-minated how tumor cell metabolism is apparently adapted to facilitate the uptake and incorporation of nutrients into the biomass needed to produce a new cell. Because that cell division phenomenon requires substantial levels of cellular mac-romolecules, the bulk of the glucose can-not be committed to carbon metabolism for ATP production via mitochondrial OXPHOS. As most of the carbon, nitro-gen, free energy and reducing equivalents required to support cell growth and divi-sion are supplied by only two molecules, glucose and glutamine, and because the synthesis of nucleotides, amino acids and lipids consumes more equivalents of car-bon and NADPH (nicotinamide adenine dinucleotide phosphate, reduced) than ATP, the conversion of all of the glucose to CO
2 via mitochondrial OXPHOS to
maximize ATP production will drastically impair the needs of a proliferating cell.
A metabolic rewriting of the Hanahan and Weinberg cancer hallmarks. Cancer cells definitely possess requirements that extend beyond ATP. The Warburg effect, a necessary part of the glucose- and glu-tamine-addicted metabolism in tumor cells, can be correctly redefined in terms of the obligatory dependence of the tumor
formal molecular-cancer disease model. Because Vogelstein’s multistep model of human tumor pathogenesis was used to define the cancer hallmark capabili-ties, all of the cancer cell attributes, i.e., self-sufficiency in growth signals, insen-sitivity to anti-growth signals, apoptosis evasion, limitless replicative potential, sustained angiogenesis and tissue inva-sion and metastasis, were thought to be necessary “in order for a cell to become cancerous.” A metabolic understanding of cancer was regarded as an out-of-date reductionist perspective of the one-size-fits-all approach; it was therefore rejected (chute!). Indeed, under the assumption that all aspects of tumor biology, from proliferative progression to invasion and metastasis, should be the result of a con-tinuous optimization process governed by Darwinian dynamics (i.e., the Warburg effect must impart a selective advantage on the cells that possess such a pheno-type), it may seem an evolutionary and bioenergetic conundrum to state that it is significantly advantageous for cancer cells to utilize glycolysis when oxygen is abundantly present. The use of glycoly-sis would not seem advantageous in these conditions, because aerobic glycolysis is 18-fold less efficient than mitochondrial OXPHOS in producing ATP.
Understanding cancer’s unorthodox metabolism within cancer orthodoxy. If cancer progression occurs via Darwinian somatic evolution, the inefficient, toxic glycolytic phenotype should be selected against after cancer cells secure access to blood vessels and normoxic environments. However, this result has not been observed; metastatic cancer cells are commonly found to express the glycolytic phenotype and to produce copious lactic acid irre-spective of oxygen accessibility. Moreover, metabolic reprogramming occurs in a fully oxygenated state for leukemia. Renewed interest in Warburg’s metabolic model of cancer has occurred in the last decade due to the realization that the adop-tion of a less-efficient cancer metabotype by tumor cells is counterintuitive when solely explained in terms of ATP produc-tion. The elegant mathematical models and empirical observations of Gillies and Gatenby52-55 have established that tumor cells’ elevated glucose consumption is
of a “chute.” The game movements began almost 100 y ago.
The Otto Warburg hypothesis: Cancer is a metabolic disease. At the end of the 1920s, Otto Warburg first described the anoma-lous character of energy metabolism in tumor cells.36,37 Cancer cells were found to reprogram glucose metabolism and to display an intrinsic method of producing energy or ATP, by activating a bioener-getic state called aerobic glycolysis. In this process, the glycolytic pathway is favored over mitochondrial oxidative phosphory-lation (OXPHOS) as the primary form of energetic metabolism even in the presence of oxygen. The Otto Warburg hypothesis, which states that the endogenous respira-tion defects of cancer cells, accompanied by the development of enhanced aerobic glycolysis during carcinogenesis, are a metabolic switch defining the “root of cancer” (Fig. 3), has persisted for many years (ladder!). However, when radioac-tive tracer techniques were employed to study the metabolism of radioactively labeled glucose into carbon dioxide in the 1950s, it became apparent that tumor tissues could also oxidize glucose at rates comparable with those observed in normal tissues. In addition, mutant mitochondrial proteins did not play pivotal functional roles, because most tumor tissues were found to contain functional respiratory enzymes and coenzymes, a functional citric acid cycle and a normal coupling of oxidation with ATP formation (chute!).
Hanahan and Weinberg’s cancer hall-marks: Moving metabolism from the cause of cancer to the consequence of cancer. The arrival of the molecular era in the 1990s rapidly emphasized that changes in energy metabolism, although universally recog-nizable in tumors from different tissue types, should no longer be regarded as the major root of cancer. In the former version of the 2000s landmark article in which Hanahan and Weinberg synthesized a large amount of information and con-densed the molecular characteristics of a cancer cell into a single conceptual frame-work,51 the metabolic transformation that generally accompanies tumorigenesis was not among the six selected hallmarks of cancer. The tumor genetics and transduc-tion pathway signatures were the exclusive parameters considered in producing their

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1171
proliferating cancer cells.57-60 Considering that the Warburg effect involves a major replacement of the metabolic program that operates in most normal tissues to fuel the physiological operations of cancer cells, it might be tempting to suggest that
allows for the diversion of key metabo-lites into the major cellular biosynthetic pathways (amino acid synthesis, nucleic acid synthesis and de novo fatty acid bio-genesis), thus maximizing the produc-tion of macromolecules and organelles in
cells to rapidly produce other metabolic end products in an unrestricted man-ner; therefore, the cancer cells are self-autonomous within the generally starved microenvironmental conditions in grow-ing solid tumors.57-60 The Warburg effect
Figure 3. For figure legend, see page 1172.

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
1172 Cell Cycle volume 12 issue 8
behind the conversion of cells-of-origin into CSCs can be better understood in terms of the “metabolic facilitators” and “metabolic impediments” that operate as openings and roadblocks, respectively, for the transcriptional events and signal transduction programs that ultimately orchestrate the intrinsic and/or microen-vironmental paths to CSC-like cellular states (Fig. 3). If this scenario proves true, we should be able to delineate the self-autonomous cell metabotype that is com-patible with the operational properties exclusively owned by CSCs. Subsequently, we should be able to pharmacologically impose a normalized metabolic environ-ment for the required pro-immortalizing metabotype that fuels the induction of cancer stemness, pluripotency and differ-entiation, thus endowing non-CSCs with an energetic infrastructure that is pro-tected against the reprogramming events that lead to CSC cellular states.
Nobel Prize-winning iPSCs: The paradox and paradigm of cancer metabo-stemness. The most recent Nobel Prize in Medicine, which was awarded to Gurdon and Yamanaka for their genial contri-bution to somatic cell reprogramming to produce SCs, has underlined revolu-tionary consequences for regenerative medicine and provided alternative strate-gies in cancer research. Yamanaka-like reprogramming technologies have been developed to revert normal somatic differ-entiated cells into patient-specific iPSCs that can be differentiated into different
functional independence from the core hallmarks (chute!).
Metabolic reprogramming of CSCs: Engineering a new-dimensional cancer hallmark. To resolve the worst-case sce-nario in cancer biology research and oncol-ogy drug discovery, we must reconsider our current genocentric guidelines regard-ing the molecular classification and treat-ment of human carcinomas. In light of the recent cluster analyses of driver mutations showing that several of these mutations converge on metabolic pathways58,63 and considering the aforementioned findings revealing that bona fide cancer hallmarks can indeed impinge on cancer metabolism, Professor Mak’s statement is relevant in that, in cancer research, we are erroneously “putting the carts (driver gene mutations) before the horses (aberrant metabolism).” However, if we target specific alterations in cell metabolism as part of the mere development of the cancer phenotype, like radiation and chemotherapies do with the proliferative rate, should we not expect an analogous failure on the way to success-fully treating cancer?
Beyond the increasingly recognized capability of cancer-associated meta-bolic reprogramming to contribute to the acquisition of the six bona fide cancer hall-marks, the a priori energetic infrastruc-ture of the cells-of-origin in cancer may represent a key feature for optimal routing to CSC cellular states. The most recent studies begin to support a new developing paradigm in which the molecular logic
aerobic glycolysis should gain the status of a cancer hallmark (ladder!). However, proteins that are somehow involved in pro-gramming the bona fide core hallmarks of cancer can also orchestrate the redirec-tion of energy metabolism. As a result of oncogenic gain-of-function events or the loss of tumor suppressors primarily affect-ing the PI3K/AKT/mTOR/HIF axis and the p53 system, respectively, a stereo-typed pattern of metabolic changes can be induced, including glucose transport, glycolysis, lactate production, reduced OXPHOS and lipid synthesis.61 Viewed in this way, the Warburg effect is simply an evolutionarily conserved target that is programmed by most common prolifera-tion-inducing “metabolic oncogenes” and “metabolic tumor-suppressors,” thus rais-ing the question of whether the deregula-tion of cellular energy metabolism is a core hallmark capability of cancer cells that is as fundamental as the six well-established core hallmarks (Fig. 3). When Hanahan and Weinberg revisited the hallmarks of cancer in 2011,62 they added the two following categories: “enabling charac-teristics,” which do not necessarily cause cancer but at least assist cells in acquir-ing cancer hallmarks in a transition from normal to malignant status (like tumor-promoting inflammation), and “emerging hallmarks,” which may not be pervasive in all cancers. Metabolism reprogramming was designated as an emerging hallmark to highlight both its evident importance and the unresolved issues surrounding its
Figure 3 (See previous page). the Warburg effect: An evolutionary perspective. exogenous microenvironmental factors (e.g., hypoxia, oxidative stress, extracellular matrix detachment and nutrient starvation) and intrinsic genetic determinants (e.g., oncogenes, tumor suppressor genes and epigenetics) converge to coordinately determine the induced and/or inherent activation status of the Warburg phenotype in tumor tissues. Once cancer cells reach the oxygen diffusion limit, they become hypoxic, and they can be directed either to cell death or adaptation to a glycolytic phe-notype. in this state, tumor cells may adapt a Warburg phenotype as the need for complementary bioenergetic resources is satisfied by the ability of the glycolysis to generate not only energy but also building blocks for anabolic (biosynthetic) metabolism. As a consequence of glycolysis, lesions become acidotic and may require additional adaptation through resistance to apoptosis by upregulation of cellular anabolism (e.g., lipogenesis). the constitutive stimulation of regulatory cascades leading to the switch from mitochondrial OXPHOs to aerobic glycolysis (Warburg effect) can also be driven in response to early changes in certain metabolic oncogenes and tumor-suppressor genes (e.g., K-ras, p53, Pi3K, AKt, Myc), which have evolved to regulate cancer cell metabolism, as they ensure the activation and maintenance of the cancer-associated bioenergetics and biosynthetic metabolic pathways, including the Warburg effect. CsC cellular states emerging from these extrinsic/intrinsic convergent sequences should have a powerful growth and survival advantage, as the metabolic reprogramming of CsCs chronically exposed to an unstable oxic-hypoxic and nutrient- and growth factor-starved environment in pre-malignant and/or early stages of carcinogenesis is later maintained and likely enhanced in primary and metastatic malignancies with the appearance of the integrated circuits, in which aberrant metabolic activity reinforces the gene networks and transcriptional signatures, thereby driving a distinct bioenergetic/biosynthetic CsC cell state. We now propose that the Warburg effect is a/the “permitted” cell metabotype possessing the necessary plasticity to reprogram the tumor cell of origin so that it can acquire the cellular state of a CsC. Conversely, the intrinsic and extrinsic genetic/epigenetic factors that control the paths-to-CsC properties cannot operate in non-Warburg “protected” cell metabo-types. Previously, scientists believed that commonly observed Warburg-like metabolic changes were a mere consequence of the aberrant cancer cell growth within tumor tissues. We now propose for the first time that metabolic reprogramming of CsCs has cancer-causing activity. such a new definition of the Warburg effect would make it possible to metabolically create non-permissive (or “hostile”) metabotypes to prevent the occurrence of cellular states with tumor- and metastasis-initiating capacities.

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1173
with greater potentials for self-renewal and pluripotency will also have a higher probability of causing tumors, much research in the field has focused on the tumorigenic traits of iPSCs to facilitate the development of safe, tumorigenic-free iPSCs-based therapies.67-69 Indeed, due to the fact that remarkable similarities exist between the processes that lead to the acquisition of oncogenic CSC cellular states and the reprogramming of somatic cells to induced pluripotency,70,71 an improved understanding of the molecular details underlying the pluripotency repro-gramming process has provided crucial insights into the mechanisms by which CSCs might arise.
Oncogenesis and iPSCs generation are closely related processes. During tumori-genesis, both the activation of cancer-pro-moting oncogenes and the loss of tumor suppressor genes destabilize the normal transcriptome of the target cell, which, coupled with epigenetic alterations that directly depend on oncogenic changes or secondary to tumor progression, leads to the partial or total loss of the cell’s original identity. One or several permissive/selec-tive steps are also required to permit the cell to bypass the safety mechanisms that prevent survival in the presence of unfavor-able conditions, such as DNA damage and uncontrolled growth. The generation of a CSC cellular state additionally requires the re-acquisition of self-renewal and asymmetric division capacities. Induced
reprogramming factors, which can “reset” the epigenetic status of the cells and allow them to adopt a new plethora of possible fates,64-66 were previously known for their oncogenic activity. Because a fundamen-tal principle of cell biology is that the SCs
lineages. Yamanaka’s method involves the transient expression of a set of four transcription factors (Oct4, Sox2, Klf4 and c-Myc) into cells; these factors have been demonstrated as critical for stemness and cell differentiation. Several of these
Figure 4. the metabo-CsC attribute might uncouple tumorigenesis from normal pluri-potency. the close affinity of normal tissue sCs and CsCs is expected to be problematic for the increased possibility of off-target effects of CsC-based anticancer therapies. in this regard, the CsC metabotype (infra-structure and functioning) appears to show unique features that are pivotal for sC-related tumorigenesis but are dispensable for adult sC development in mature tissues. Our recent discovery of the specific, efficient elimination of the malignant teratoma-initiating iPsCs47 that are responsible for the teratocarcinoma growth strongly suggest that the metabo-CsC attribute is a previously unrecognized, indispensable component of the CsC ma-chinery that differentiates between the spe-cific characteristics of normal tissue sCs and CsCs, thus providing an essential requisite for assessing the best treatment targets for CsCs while minimizing undesirable sequelae.

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
1174 Cell Cycle volume 12 issue 8
CSCs. Intriguingly, the latest discover-ies in the field have revealed that iPSCs appear to share all of the core compo-nents of metabolic reprogramming that have been commonly observed in human tumors.
The enforced aerobic glycolysis (the Warburg effect) that typically accompanies the metabolic reprogramming of tumor tis-sues is a fundamental iPSC phenotypic trait. Somatic mitochondria within iPSCs dras-tically alter their morphology and func-tionality to acquire an immature organelle shape with underdeveloped cristae and low oxidative stress levels. These changes directly affect the cellular bioenergetic profile, which is shifted from OXPHOS to glycolysis upon reprogramming and returns to OXPHOS during the subse-quent redirection of iPSC differentiation into defined lineages. Importantly, the glycolytic phenotype is necessary for and promotes the optimal routing of somatic cells to pluripotency; the stimulation of aerobic glycolysis favors, while the block-ade of glycolytic enzymes blunts, repro-gramming phenomena.84-90 These findings appear to establish cell bioenergetics as a
Thus, one of the primary assays of stem-ness is also a tumor assay, which clearly illustrates the strong link between CSCs, reprogramming and tumorigenicity.
Metabolic reprogramming enables the generation of induced pluripotency. iPSCs certainly offer a unique system for study-ing the molecular and cellular mechanisms underlying the process of de novo genera-tion of CSC cellular states. This process is initiated when committed cells overcome certain cellular barriers, such as tumor sup-pressor pathways, e.g., oncogene-induced senescence (OIS), which also act as criti-cal roadblocks against reprogramming, e.g., reprogramming-induced senescence (RIS), to acquire an indefinite self-renewal capacity and a certain degree of pluripo-tent plasticity. If CSC-driven tumorigene-sis is closely associated with the acquisition of SC-like properties in induced pluri-potency, determining the mechanisms that positively regulate the efficiency and kinetics of somatic reprogramming to iPSCs may provide a proof-of-concept val-idation for the novel self-renewing tumor-initiating mechanisms that regulate both the number and aberrant functionality of
pluripotency similarly requires specific combinations of collaborating oncogenes/tumor suppressor genes that can efficiently produce a less-differentiated cell that can proliferate and self-renew indefinitely. The generation of iPSCs by the expression of stem cell-specific genes is negatively regu-lated by the activation of cell-intrinsic, cancer-protective programs such as p53- and p16INK4a-driven senescence, i.e., the major tumor-suppressive mechanism that must be also overcome during malig-nant transformation of normal epithelial cells.72-80 Escaping senescence or acquiring immortality is a crucial, rate-limiting step toward the establishment of iPSCs, fur-ther underscoring the similarities between tumorigenesis and induced pluripotency. Both oncogenesis and induced pluripo-tency are similarly more efficient when the cell of origin is closer to the SC state. When oncogenes, transcription factors or onco-microRNAs induce differentiated cells to reprogram into iPSCs, these cells spon-taneously form teratocarcinomas when transplanted into nude mice due to the presence of an undifferentiated compart-ment of “teratoma-initiating” iPSCs.81-83
Figure 5. the metabo-CsC paradigm in cancer therapeutics. identifying the metabotypic infrastructure of CsCs will add a novel dynamic dimension to well-recognized cancer hallmarks. in the clinic, the cancer metabo-CsC attribute will be the basis to rapidly pursue unique therapeutic approaches that target the addiction of CsCs to certain metabolic infrastructures and metabolic fluxes, i.e., the CsC metabotype. the opportunities and chal-lenges for targeting the CsC metabolic infrastructure can be rapidly achieved, because existing metabolic drugs currently used for treatment of diabetes, obesity or cardiovascular diseases might be easily repositioned from the evolutionary pre-clinical stages to revolutionary clinical approaches in cancer.

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1175
novel pre-requisite of acquired stemness. Accordingly, an experimental model com-paring oncogenic transformation and cellular reprogramming has recently con-firmed that somatic cells must first acquire changes that lead to the downregulation of cell differentiation machinery combined with the upregulation of glycolysis and other glycolysis-related metabolic path-ways.91 Only then do the oncogenic trans-formation/induced pluripotency pathways diverge, which depends on other factors, such as the activity of pluripotency genes.
iPSCs couple the Warburg effect to ana-bolic metabolism to fully mimic metabolic reprogramming in cancer cells. As above-mentioned, the Warburg effect has been correctly redefined in terms of the obliga-tory dependence of the tumor cells to max-imize the production of macromolecules and organelles, because aerobic glycolysis, but not OXPHOS, allows for the rapid and efficient diversion of key metabolites into the major cellular biosynthetic pathways in proliferating cancer cells.56-59 Similar to biologically aggressive carcinomas and CSCs,92-95 we have recently demonstrated that iPSCs supercharge lipogenesis by trig-gering regulatory circuits that activate and provide substrates for the key lipogenic enzymes, fatty acid synthase (FASN),48 a highly NADPH-consuming metabolic strategy that facilitates the Warburg effect by rapidly generating NAD+ and avoid-ing low NAD+/NADH ratios that would eventually inhibit glycolysis. Like cancer cells, iPSCs may also evoke a high rate of lipid synthesis to overcome the detrimen-tal effects of toxic free radical generation, because the de novo synthesized monoun-saturated lipids are less susceptible to lipid peroxidation, thus cooperating with the suppression of the mitochondria-related oxidative stress pathway.
The a priori bioenergetics of somatic cells correlates with the reprogramming efficien-cies. A bioenergetic shift from somatic oxidative mitochondria toward an alterna-tive glycolytic phenotype maximizes the efficiency of iPSCs generation. Somatic cells that demonstrate oxidative:glycolytic energy production ratios that are closer to those of pluripotent SCs reprogram more rapidly and efficiently.88-90 Crucially, iPSCs glycolytic capacity relate to their intrinsic tumorigenic and differentiation
potential. The inclusion of the c-Myc oncogene potentiates the pluripotent glycolytic behavior and the tumorigenic incidence of derived iPSCs;96 conversely, c-Myc removal decreases the tumorige-nicity of iPSCs and facilitates OXPHOS-dependent lineage commitment and terminal differentiation.97
The reprogramming-competent metabo-type of iPSCs involves the sole two-primum movens that account for OXPHOS inhibition and promote the acquisition of the Warburg effect in human carcinomas without requir-ing mutations in cancer genes. First, iPSCs notably downregulate the expression of the catalytic subunit of the AMP-activated protein kinase (AMPK),86,98 a master met-abolic switch that senses and decodes intra-cellular changes in the energy status.99-101 iPSCs suppress the activation of AMPK to avoid anabolic inhibition and escape the growth-arresting effects of AMPK, which is similar to phenomena com-monly observed in cancer cells. AMPK underexpression is frequently observed in human carcinomas, and AMPK inac-tivation promotes epithelial cell carcino-genesis. AMPK activity opposes tumor development, and the loss of AMPK activ-ity fosters tumor progression, in part, by regulating the cellular metabolic pathways that support cell growth and proliferation. Crucially, AMPK has recently been shown to suppress tumor growth in vivo by nega-tively regulating the Warburg effect.102 Second, the H+-ATPase synthase-geared metabolism switch, a mitochondria-medi-ated energy adaptation that is sufficient to promote the acquisition of the Warburg effect in tumor cells,103-108 is employed during somatic reprogramming to limit the bioenergetic activity of mitochondria and shifting the metabotype to enhanced aerobic glycolysis. Somatic cell repro-gramming involves a significant increase in the expression of the ATPase inhibitor factor 1 (IF1) accompanied by extremely low expression levels of the catalytic β1-F1-ATPase subunit.48 Mitochondrial H+-ATPase is repressed at both the activ-ity and protein levels in human carcino-mas. IF1, which limits the activity of the H+-ATPase, is negligibly expressed in normal tissues and highly overexpressed in numerous carcinomas. The cellular content of the H+-ATPase, which directly
correlates with mitochondrial OXPHOS activity and inversely correlates with the rate of glucose utilization by aerobic gly-colysis, is transcriptionally and transla-tionally limited in cancer cells. In iPSCs, AMPK activity has been found to regu-late the same mechanisms that limit the activity and level of the mitochondrial H+-ATPase in cancer cells,48 thus linking the two-primum movens that establish the Warburg effect in the absence of genetic alterations.
Pharmacological prevention of meta-bolic reprogramming eliminates tumori-genic traits in iPSCs. If the Warburg effect is a reversible trait, because it can be acquired without any genetic alteration, as repeatedly hypothesized for cancer cells, the cancer-like metabolic reprogramming of iPSCs could be pharmacologically tar-geted to impede the undesirable stemness-tumorigenicity coupling. Accordingly, direct and indirect AMPK activators have been shown to impose a normalized meta-bolic effect that differs from the required pro-immortalizing glycolysis that fuels the induction of stemness and pluripotency, endowing somatic cells with an energetic infrastructure that is protected against reprogramming.45 The metabolic barrier imposed by AMPK-activating strategies cannot be bypassed even through p53 deficiency, a fundamental mechanism that greatly improves the efficiency of stem cell-production. The activation of an anabolic metabolism like de novo fatty acid biogenesis is also an instrumental event that enables the reprogramming of somatic cells to iPSCs, because the phar-macological inhibition of FASN activity is sufficient to markedly decrease repro-gramming efficiency.48 The activation of AMPK alone, which drastically impacts the OXPHOS:aerobic glycolysis ratio, fully reverses the high IF1/β-F1-ATPase ratio and suppresses the anabolic phe-notype in iPSCs.48 Perhaps more impor-tantly, AMPK activation is sufficient to fully recapitulate the ability of an increased dosage of tumor suppressors (like p53 and Ink4a/ARF) to prevent the occurrence or drastically reduce the size and weight of teratoma-like masses following the trans-plantation of iPSCs into immunodeficient mice.47,83 The pharmacological prevention of Warburg-like metabotypes therefore

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
1176 Cell Cycle volume 12 issue 8
to clinical approaches. The drugs that would arise from the knowledge-based drug repositioning strategies selected to metabolically suppress the frequency and/or functionality of CSCs could silently operate as “cancer tissue sweepers” of dys-functional cells capable of initiating and propagating tumors while sparing their normal counterparts.
In “The Prime Cause and Prevention of Cancer,” a lecture delivered at the 1966 annual meeting of Nobelists at Lindau, Germany, Otto Warburg stated, “Cancer, above all other diseases, has countless sec-ondary causes. But, even for cancer, there is only one prime cause […]. During the cancer development, the oxygen-respira-tion always falls, fermentation appears, and the highly differentiated cells are transformed to fermenting anaerobes, which have lost their body functions and retain only the now useless property of growth.” If Otto Warburg were alive today, he would be surely lecturing on “CSCs that turn back the clock, in meta-bolic terms, to share some properties with embryonic SCs, notably self-renewal and differentiation capacities, which are aber-rantly utilized both in the acquisition of pluripotency and in tumorigenesis,” i.e., the Warburg effect version 2.0.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
This work was financially supported by the Instituto de Salud Carlos III (Ministerio de Sanidad y Consumo, Fondo de Investigación Sanitaria (FIS), Spain, grants CP05-00090, PI06-0778 and RD06-0020-0028), the Fundación Científica de la Asociación Española Contra el Cáncer (AECC, Spain) and the Ministerio de Ciencia e Innovación (SAF2012-38914, SAF2009-11579, Plan Nacional de I+D+I, MICINN, Spain). Alejandro Vazquez-Martin received a Sara Borrell post-doctoral contract (CD08/00283, Ministerio de Sanidad y Consumo, Fondo de Investigación Sanitaria -FIS-, Spain). Sílvia Cufí received a research fellowship (Formación de Personal Investigador, FPI) from the Ministerio de Ciencia e Innovación (MICINN, Spain).
cell of origin to enter reprogramming at different time points after reprogramming induction and the length of time required to complete the reprogramming sequence could be affected by the a priori bioener-getic and anabolic status. With the lack of an appropriate metabotype, fewer cells would undergo the required stochastic genetic and epigenetic events to proceed to a fully reprogrammed state of acquired self-renewal and pluripotency. The pos-session or intrinsic ability to develop a Warburg-like/anabolic metabotype repre-sents a very early, crucial molecular event that imposes an a priori barrier on the path of transformation from somatic differen-tiated cells to CSCs. This process does not necessarily require the participation of oncogene-driven metabolic changes (Fig. 3). In this scenario, the remodelling of bioenergetic and biosynthetic metabo-lism is an active component (rather than a consequence) that defines cell fate, and both the intrinsic flexibility and reversibil-ity may have revolutionary implications for the pharmacological manipulation of the self-renewal and pluripotent capabili-ties fuelling CSC-driven tumorigenesis.
Metabolic reprogramming of CSC cellular states: A therapeutic corollary. In the past, cancer genomics theories had pushed Warburg’s metabolic hypothesis of cancer into obscurity. We now propose the possibility of delineating a metabolic roadmap for malignant stemness that might not require pre-existing mutations or rearrangements of proto-oncogenes or tumor suppressor genes. Identifying the metabotypic infrastructure and the metabotype functioning of CSCs will add a novel dynamic dimension to well-rec-ognized cancer hallmarks. In the clinic, the metabo-CSC attribute will be the basis to rapidly pursue unique therapeu-tic approaches that target the addiction of CSCs to certain metabolic infrastruc-tures and metabolic fluxes, i.e., the CSC metabotype (Fig. 5). This novel approach might generate a shift in the theory of oncology, resulting in a new era of metab-olo-genomic-personalized cancer medi-cine. The opportunities and challenges for targeting the metabolic infrastruc-ture of CSCs might be rapidly achieved, because existing metabolic drugs may be easily repositioned from pre-clinical stages
facilitates the specific elimination of ter-atoma-initiating pluripotent stem cells that are intermixed with the desired, non-tumorigenic iPSC derivatives that termi-nally differentiate into multiple lineages (Fig. 4).47,109 The close affinity of normal tissue SCs and CSCs can be problematic for the increased possibility of off-target effects of CSC-based anticancer therapies. Differentiating between the specific char-acteristics of normal tissue SCs and CSCs may be an essential requisite for assessing the best treatment targets for CSCs while minimizing sequelae. The specific, effi-cient elimination of the malignant iPSCs that are responsible for the teratocarci-noma growth strongly supports the pro-posal that the metabo-stemness hallmark is a previously unrecognized, indispens-able component of the CSC machinery.
Metabolic reprogramming of the CSC cellular states: A working model for a new cancer hallmark. Within an individual tumor, a bidirectional conversion exists between the non-CSC and CSC cellular states. Therefore, a convergence toward a phenotypic equilibrium, such as the het-erogeneous tumor tissue that a pathologist would classify and an oncologist would treat, likely occurs due to highly dynamic cancer cell-state interconversions. The transition rates between the cell states, which can vary across distinct cancer cell populations, has been considered to largely depend on the degree of the differenti-ation-state plasticity dictated by genetic and epigenetic parameters. Cancer, cellu-lar plasticity and cell fate reprogramming are tightly intertwined processes, because not all cancer cells possess the necessary plasticity to permit their reprogramming to CSC cellular states, and only some can-cer genes possess, in the right cellular con-text, the required capacity to fully elicit the reprogramming process. Because the occurrence of parallel metabolic changes in oncogenesis and the induction of plu-ripotency support the notion that cell reprogramming is a naturally occurring phenomenon and not just a technology, it is reasonable to suggest that (as observed with iPSCs) cell bioenergetics can operate as the pivotal decision-making parameter during the reprogramming acquisition of SC properties in normal and non-CSC tumor cells. The individual ability of the

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1177
37. Warburg O. On the origin of cancer cells. Science 1956; 123:309-14; PMID:13298683; http://dx.doi.org/10.1126/science.123.3191.309
38. Vazquez-Martin A, Oliveras-Ferraros C, Del Barco S, Martin-Castillo B, Menendez JA. The anti-diabetic drug metformin suppresses self-renewal and pro-liferation of trastuzumab-resistant tumor-initiating breast cancer stem cells. Breast Cancer Res Treat 2011; 126:355-64; PMID:20458531; http://dx.doi.org/10.1007/s10549-010-0924-x
39. Vazquez-Martin A, Oliveras-Ferraros C, Cufí S, Martin-Castillo B, Menendez JA. Metformin and energy metabolism in breast cancer: from insulin physiology to tumor-initiating stem cells. Curr Mol Med 2010; 10:674-91; PMID:20712585; http://dx.doi.org/10.2174/156652410792630625
40. Vazquez-Martin A, Oliveras-Ferraros C, Cufí S, Del Barco S, Martin-Castillo B, Menendez JA. Metformin regulates breast cancer stem cell ontog-eny by transcriptional regulation of the epithelial-mesenchymal transition (EMT) status. Cell Cycle 2010; 9:3807-14; PMID:20890129; http://dx.doi.org/10.4161/cc.9.18.13131
41. Cufí S, Vazquez-Martin A, Oliveras-Ferraros C, Martin-Castillo B, Joven J, Menendez JA. Metformin against TGFβ-induced epithelial-to-mesenchymal transition (EMT): from cancer stem cells to aging-associated fibrosis. Cell Cycle 2010; 9:4461-8; PMID:21088486; http://dx.doi.org/10.4161/cc.9.22.14048
42. Oliveras-Ferraros C, Cufí S, Vazquez-Martin A, Torres-Garcia VZ, Del Barco S, Martin-Castillo B, et al. Micro(mi)RNA expression profile of breast cancer epithelial cells treated with the anti-diabetic drug metformin: induction of the tumor suppressor miRNA let-7a and suppression of the TGFβ-induced oncomiR miRNA-181a. Cell Cycle 2011; 10:1144-51; PMID:21368581; http://dx.doi.org/10.4161/cc.10.7.15210
43. Vazquez-Martin A, López-Bonetc E, Cufí S, Oliveras-Ferraros C, Del Barco S, Martin-Castillo B, et al. Repositioning chloroquine and metformin to eliminate cancer stem cell traits in pre-malig-nant lesions. Drug Resist Updat 2011; 14:212-23; PMID:21600837
44. Menendez JA, Vellon L, Oliveras-Ferraros C, Cufí S, Vazquez-Martin A. mTOR-regulated senescence and autophagy during reprogramming of somatic cells to pluripotency: a roadmap from energy metabo-lism to stem cell renewal and aging. Cell Cycle 2011; 10:3658-77; PMID:22052357; http://dx.doi.org/10.4161/cc.10.21.18128
45. Vazquez-Martin A, Vellon L, Quirós PM, Cufí S, Ruiz de Galarreta E, Oliveras-Ferraros C, et al. Activation of AMP-activated protein kinase (AMPK) provides a metabolic barrier to reprogramming somatic cells into stem cells. Cell Cycle 2012; 11:974-89; PMID:22333578; http://dx.doi.org/10.4161/cc.11.5.19450
46. Vazquez-Martin A, Cufi S, Corominas-Faja B, Oliveras-Ferraros C, Vellon L, Menendez JA. Mitochondrial fusion by pharmacological manipula-tion impedes somatic cell reprogramming to pluri-potency: new insight into the role of mitophagy in cell stemness. Aging (Albany NY) 2012; 4:393-401; PMID:22713507
47. Vazquez-Martin A, Cufi S, Lopez-Bonet E, Corominas-Faja B, Oliveras-Ferraros C, Martin-Castillo B, et al. Metformin limits the tumorigenicity of iPS cells without affecting their pluripotency. Sci Rep 2012; 2:964; PMID:23236586; http://dx.doi.org/10.1038/srep00964
48. Vazquez-Martin A, Corominas-Faja B, Cufi S, Vellon L, Oliveras-Ferraros C, Menendez OJ, et al. The mitochondrial H(+)-ATP synthase and the lipogenic switch: new core components of metabolic reprogramming in induced pluripotent stem (iPS) cells. Cell Cycle 2013; 12:207-18; PMID:23287468; http://dx.doi.org/10.4161/cc.23352
20. Creighton CJ, Li X, Landis M, Dixon JM, Neumeister VM, Sjolund A, et al. Residual breast cancers after conventional therapy display mesenchymal as well as tumor-initiating features. Proc Natl Acad Sci USA 2009; 106:13820-5; PMID:19666588; http://dx.doi.org/10.1073/pnas.0905718106
21. Kakarala M, Wicha MS. Implications of the can-cer stem-cell hypothesis for breast cancer preven-tion and therapy. J Clin Oncol 2008; 26:2813-20; PMID:18539959; http://dx.doi.org/10.1200/JCO.2008.16.3931
22. Liu S, Wicha MS. Targeting breast cancer stem cells. J Clin Oncol 2010; 28:4006-12; PMID:20498387; http://dx.doi.org/10.1200/JCO.2009.27.5388
23. Liu S, Dontu G, Wicha MS. Mammary stem cells, self-renewal pathways, and carcinogenesis. Breast Cancer Res 2005; 7:86-95; PMID:15987436; http://dx.doi.org/10.1186/bcr1021
24. Kakarala M, Wicha MS. Implications of the can-cer stem-cell hypothesis for breast cancer preven-tion and therapy. J Clin Oncol 2008; 26:2813-20; PMID:18539959; http://dx.doi.org/10.1200/JCO.2008.16.3931
25. Alison MR, Islam S, Wright NA. Stem cells in cancer: instigators and propagators? J Cell Sci 2010; 123:2357-68; PMID:20592182; http://dx.doi.org/10.1242/jcs.054296
26. Michor F, Polyak K. The origins and implications of intratumor heterogeneity. Cancer Prev Res (Phila) 2010; 3:1361-4; PMID:20959519; http://dx.doi.org/10.1158/1940-6207.CAPR-10-0234
27. Alison MR, Lim SM, Nicholson LJ. Cancer stem cells: problems for therapy? J Pathol 2011; 223:147-61; PMID:21125672; http://dx.doi.org/10.1002/path.2793
28. Magee JA, Piskounova E, Morrison SJ. Cancer stem cells: impact, heterogeneity, and uncertainty. Cancer Cell 2012; 21:283-96; PMID:22439924; http://dx.doi.org/10.1016/j.ccr.2012.03.003
29. Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan A, Zhou AY, et al. The epithelial-mesenchymal transi-tion generates cells with properties of stem cells. Cell 2008; 133:704-15; PMID:18485877; http://dx.doi.org/10.1016/j.cell.2008.03.027
30. Iliopoulos D, Hirsch HA, Struhl K. An epigen-etic switch involving NF-kappaB, Lin28, Let-7 MicroRNA, and IL6 links inf lammation to cell transformation. Cell 2009; 139:693-706; PMID:19878981; http://dx.doi.org/10.1016/j.cell.2009.10.014
31. Gupta PB, Fillmore CM, Jiang G, Shapira SD, Tao K, Kuperwasser C, et al. Stochastic state transitions give rise to phenotypic equilibrium in populations of can-cer cells. Cell 2011; 146:633-44; PMID:21854987; http://dx.doi.org/10.1016/j.cell.2011.07.026
32. Chaffer CL, Brueckmann I, Scheel C, Kaestli AJ, Wiggins PA, Rodrigues LO, et al. Normal and neoplastic nonstem cells can spontaneously con-vert to a stem-like state. Proc Natl Acad Sci USA 2011; 108:7950-5; PMID:21498687; http://dx.doi.org/10.1073/pnas.1102454108
33. Iliopoulos D, Hirsch HA, Wang G, Struhl K. Inducible formation of breast cancer stem cells and their dynamic equilibrium with non-stem cancer cells via IL6 secretion. Proc Natl Acad Sci USA 2011; 108:1397-402; PMID:21220315; http://dx.doi.org/10.1073/pnas.1018898108
34. Polytarchou C, Iliopoulos D, Struhl K. An integrated transcriptional regulatory circuit that reinforces the breast cancer stem cell state. Proc Natl Acad Sci USA 2012; 109:14470-5; PMID:22908280; http://dx.doi.org/10.1073/pnas.1212811109
35. Floor SL, Dumont JE, Maenhaut C, Raspe E. Hallmarks of cancer: of all cancer cells, all the time? Trends Mol Med 2012; 18:509-15; PMID:22795735; http://dx.doi.org/10.1016/j.molmed.2012.06.005
36. Warburg O, Posener K, Negelein E. Uber den stoff-wechsel der carcinomzelle. Biochem Z 1924; 152:309
References1. Stratton MR. Exploring the genomes of cancer cells:
progress and promise. Science 2011; 331:1553-8; PMID:21436442; http://dx.doi.org/10.1126/sci-ence.1204040
2. Al-Lazikani B, Banerji U, Workman P. Combinatorial drug therapy for cancer in the post-genomic era. Nat Biotechnol 2012; 30:679-92; PMID:22781697; http://dx.doi.org/10.1038/nbt.2284
3. Patel MN, Halling-Brown MD, Tym JE, Workman P, Al-Lazikani B. Objective assessment of cancer genes for drug discovery. Nat Rev Drug Discov 2013; 12:35-50; PMID:23274470; http://dx.doi.org/10.1038/nrd3913
4. http://www.who.int/mediacentre/factsheets/fs297/en/index.html
5. http://www.fda.gov/scienceresearch/specialtopics/criticalpathinitiative/default.htm
6. Rees J. Complex disease and the new clinical scienc-es. Science 2002; 296:698-700; PMID:11976444; http://dx.doi.org/10.1126/science.296.5568.698
7. Greenman C, Stephens P, Smith R, Dalgliesh GL, Hunter C, Bignell G, et al. Patterns of somat-ic mutation in human cancer genomes. Nature 2007; 446:153-8; PMID:17344846; http://dx.doi.org/10.1038/nature05610
8. Sjöblom T, Jones S, Wood LD, Parsons DW, Lin J, Barber TD, et al. The consensus coding sequences of human breast and colorectal cancers. Science 2006; 314:268-74; PMID:16959974; http://dx.doi.org/10.1126/science.1133427
9. Wood LD, Parsons DW, Jones S, Lin J, Sjöblom T, Leary RJ, et al. The genomic landscapes of human breast and colorectal cancers. Science 2007; 318:1108-13; PMID:17932254; http://dx.doi.org/10.1126/science.1145720
10. Stratton MR, Campbell PJ, Futreal PA. The cancer genome. Nature 2009; 458:719-24; PMID:19360079; http://dx.doi.org/10.1038/nature07943
11. Curtis C, Shah SP, Chin SF, Turashvili G, Rueda OM, Dunning MJ, et al.; METABRIC Group. The genomic and transcriptomic architecture of 2,000 breast tumors reveals novel subgroups. Nature 2012; 486:346-52; PMID:22522925
12. Ledford H. Big science: The cancer genome chal-lenge. Nature 2010; 464:972-4; PMID:20393534; http://dx.doi.org/10.1038/464972a
13. Macconaill LE, Garraway LA. Clinical implications of the cancer genome. J Clin Oncol 2010; 28:5219-28; PMID:20975063; http://dx.doi.org/10.1200/JCO.2009.27.4944
14. Chin L, Andersen JN, Futreal PA. Cancer genomics: from discovery science to personalized medicine. Nat Med 2011; 17:297-303; PMID:21383744; http://dx.doi.org/10.1038/nm.2323
15. Arteaga CL, Baselga J. Impact of genomics on personalized cancer medicine. Clin Cancer Res 2012; 18:612-8; PMID:22298893; http://dx.doi.org/10.1158/1078-0432.CCR-11-2019
16. Ashfaq R. Molecular profiling for personalized cancer care. Clin Exp Metastasis 2012; 29:653-5; PMID:22678423; http://dx.doi.org/10.1007/s10585-012-9483-3
17. Wicha MS, Liu S, Dontu G. Cancer stem cells: an old idea--a paradigm shift. Cancer Res 2006; 66:1883-90, discussion 1895-6; PMID:16488983; http://dx.doi.org/10.1158/0008-5472.CAN-05-3153
18. Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF. Prospective identification of tumorigenic breast cancer cells. Proc Natl Acad Sci USA 2003; 100:3983-8; PMID:12629218; http://dx.doi.org/10.1073/pnas.0530291100
19. Li X, Lewis MT, Huang J, Gutierrez C, Osborne CK, Wu MF, et al. Intrinsic resistance of tumorigenic breast cancer cells to chemotherapy. J Natl Cancer Inst 2008; 100:672-9; PMID:18445819; http://dx.doi.org/10.1093/jnci/djn123

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
1178 Cell Cycle volume 12 issue 8
84. Prigione A, Fauler B, Lurz R, Lehrach H, Adjaye J. The senescence-related mitochondrial/oxida-tive stress pathway is repressed in human induced pluripotent stem cells. Stem Cells 2010; 28:721-33; PMID:20201066; http://dx.doi.org/10.1002/stem.404
85. Varum S, Rodrigues AS, Moura MB, Momcilovic O, Easley CA 4th, Ramalho-Santos J, et al. Energy metabolism in human pluripotent stem cells and their differentiated counterparts. PLoS ONE 2011; 6:e20914; PMID:21698063; http://dx.doi.org/10.1371/journal.pone.0020914
86. Prigione A, Lichtner B, Kuhl H, Struys EA, Wamelink M, Lehrach H, et al. Human induced pluripotent stem cells harbor homoplasmic and het-eroplasmic mitochondrial DNA mutations while maintaining human embryonic stem cell-like meta-bolic reprogramming. Stem Cells 2011; 29:1338-48; PMID:21732474
87. Panopoulos AD, Yanes O, Ruiz S, Kida YS, Diep D, Tautenhahn R, et al. The metabolome of induced pluripotent stem cells reveals metabolic changes occurring in somatic cell reprogramming. Cell Res 2012; 22:168-77; PMID:22064701; http://dx.doi.org/10.1038/cr.2011.177
88. Folmes CD, Nelson TJ, Martinez-Fernandez A, Arrell DK, Lindor JZ, Dzeja PP, et al. Somatic oxidative bioenergetics transitions into pluripotency-depen-dent glycolysis to facilitate nuclear reprogramming. Cell Metab 2011; 14:264-71; PMID:21803296; http://dx.doi.org/10.1016/j.cmet.2011.06.011
89. Folmes CD, Nelson TJ, Terzic A. Energy metab-olism in nuclear reprogramming. Biomark Med 2011; 5:715-29; PMID:22103608; http://dx.doi.org/10.2217/bmm.11.87
90. Folmes CD, Nelson TJ, Dzeja PP, Terzic A. Energy metabolism plasticity enables stemness programs. Ann N Y Acad Sci 2012; 1254:82-9; PMID:22548573; http://dx.doi.org/10.1111/j.1749-6632.2012.06487.x
91. Riggs JW, Barrilleaux BL, Varlakhanova N, Bush KM, Chan V, Knoepfler PS. Induced pluripotency and oncogenic transformation are related processes. Stem Cells Dev 2013; 22:37-50; PMID:22998387; http://dx.doi.org/10.1089/scd.2012.0375
92. Menendez JA, Lupu R. Fatty acid synthase and the lipogenic phenotype in cancer pathogenesis. Nat Rev Cancer 2007; 7:763-77; PMID:17882277; http://dx.doi.org/10.1038/nrc2222
93. Pandey PR, Okuda H, Watabe M, Pai SK, Liu W, Kobayashi A, et al. Resveratrol suppresses growth of cancer stem-like cells by inhibiting fatty acid synthase. Breast Cancer Res Treat 2011; 130:387-98; PMID:21188630; http://dx.doi.org/10.1007/s10549-010-1300-6
94. Pandey PR, Xing F, Sharma S, Watabe M, Pai SK, Iiizumi-Gairani M, et al. Elevated lipogenesis in epithelial stem-like cell confers survival advantage in ductal carcinoma in situ of breast cancer. Oncogene 2012; Epub Ahead of Print; PMID:23208501; http://dx.doi.org/10.1038/onc.2012.519
95. Li G, Zhao F, Cui Y. Proteomics using mammo-spheres as a model system to identify proteins deregu-lated in breast cancer stem cells. Curr Mol Med 2013; 13:459-63; PMID:23331018
96. Folmes CD, Martinez-Fernandez A, Faustino RS, Yamada S, Perez-Terzic C, Nelson TJ, et al. Nuclear reprogramming with c-Myc potentiates glycolytic capacity of derived induced pluripotent stem cells. J Cardiovasc Transl Res 2013; 6:10-21; PMID:23247633; http://dx.doi.org/10.1007/s12265-012-9431-2
97. Martinez-Fernandez A, Nelson TJ, Ikeda Y, Terzic A. c-MYC independent nuclear reprogramming favors cardiogenic potential of induced pluripotent stem cells. J Cardiovasc Transl Res 2010; 3:13-23; PMID:20221419; http://dx.doi.org/10.1007/s12265-009-9150-5
68. Knoepfler PS. Deconstructing stem cell tumorigenic-ity: a roadmap to safe regenerative medicine. Stem Cells 2009; 27:1050-6; PMID:19415771; http://dx.doi.org/10.1002/stem.37
69. Ben-David U, Benvenisty N. The tumorigenicity of human embryonic and induced pluripotent stem cells. Nat Rev Cancer 2011; 11:268-77; PMID:21390058; http://dx.doi.org/10.1038/nrc3034
70. Abollo-Jiménez F, Jiménez R, Cobaleda C. Physiological cellular reprogramming and can-cer. Semin Cancer Biol 2010; 20:98-106; PMID:20188173; http://dx.doi.org/10.1016/j.sem-cancer.2010.02.002
71. Castellanos A, Vicente-Dueñas C, Campos-Sánchez E, Cruz JJ, García-Criado FJ, García-Cenador MB, et al. Cancer as a reprogramming-like disease: impli-cations in tumor development and treatment. Semin Cancer Biol 2010; 20:93-7; PMID:20188174; http://dx.doi.org/10.1016/j.semcancer.2010.02.001
72. Kawamura T, Suzuki J, Wang YV, Menendez S, Morera LB, Raya A, et al. Linking the p53 tumor suppressor pathway to somatic cell reprogramming. Nature 2009; 460:1140-4; PMID:19668186; http://dx.doi.org/10.1038/nature08311
73. Marión RM, Strati K, Li H, Murga M, Blanco R, Ortega S, et al. A p53-mediated DNA dam-age response limits reprogramming to ensure iPS cell genomic integrity. Nature 2009; 460:1149-53; PMID:19668189; http://dx.doi.org/10.1038/nature08287
74. Utikal J, Polo JM, Stadtfeld M, Maherali N, Kulalert W, Walsh RM, et al. Immortalization eliminates a roadblock during cellular reprogramming into iPS cells. Nature 2009; 460:1145-8; PMID:19668190; http://dx.doi.org/10.1038/nature08285
75. Liu Y, Hoya-Arias R, Nimer SD. The role of p53 in limiting somatic cell reprogramming. Cell Res 2009; 19:1227-8; PMID:19881523; http://dx.doi.org/10.1038/cr.2009.121
76. Li H, Collado M, Villasante A, Strati K, Ortega S, Cañamero M, et al. The Ink4/Arf locus is a barrier for iPS cell reprogramming. Nature 2009; 460:1136-9; PMID:19668188; http://dx.doi.org/10.1038/nature08290
77. Banito A, Rashid ST, Acosta JC, Li S, Pereira CF, Geti I, et al. Senescence impairs successful repro-gramming to pluripotent stem cells. Genes Dev 2009; 23:2134-9; PMID:19696146; http://dx.doi.org/10.1101/gad.1811609
78. Liu Y, Clem B, Zuba-Surma EK, El-Naggar S, Telang S, Jenson AB, et al. Mouse fibroblasts lacking RB1 function form spheres and undergo reprogramming to a cancer stem cell phenotype. Cell Stem Cell 2009; 4:336-47; PMID:19341623; http://dx.doi.org/10.1016/j.stem.2009.02.015
79. Collado M, Blasco MA, Serrano M. Cellular senes-cence in cancer and aging. Cell 2007; 130:223-33; PMID:17662938; http://dx.doi.org/10.1016/j.cell.2007.07.003
80. Collado M, Serrano M. Senescence in tumors: evi-dence from mice and humans. Nat Rev Cancer 2010; 10:51-7; PMID:20029423; http://dx.doi.org/10.1038/nrc2772
81. Blum B, Bar-Nur O, Golan-Lev T, Benvenisty N. The anti-apoptotic gene survivin contributes to tera-toma formation by human embryonic stem cells. Nat Biotechnol 2009; 27:281-7; PMID:19252483; http://dx.doi.org/10.1038/nbt.1527
82. Barrilleaux B, Knoepfler PS. Inducing iPSCs to escape the dish. Cell Stem Cell 2011; 9:103-11; PMID:21816362; http://dx.doi.org/10.1016/j.stem.2011.07.006
83. Menendez S, Camus S, Herreria A, Paramonov I, Morera LB, Collado M, et al. Increased dosage of tumor suppressors limits the tumorigenicity of iPS cells without affecting their pluripotency. Aging Cell 2012; 11:41-50; PMID:21981310; http://dx.doi.org/10.1111/j.1474-9726.2011.00754.x
49. http://www.cnio.es/es/news/docs/tak-mak-cnio-1jun12-en.pdf
50. http://utmj.org/ojs/index.php/UTMJ/article/view-File/1265/1143
51. Hanahan D, Weinberg RA. The hallmarks of cancer. Cell 2000; 100:57-70; PMID:10647931; http://dx.doi.org/10.1016/S0092-8674(00)81683-9
52. Gatenby RA, Gillies RJ. Why do cancers have high aerobic glycolysis? Nat Rev Cancer 2004; 4:891-9; PMID:15516961; http://dx.doi.org/10.1038/nrc1478
53. Gatenby RA, Gawlinski ET, Gmitro AF, Kaylor B, Gillies RJ. Acid-mediated tumor invasion: a multi-disciplinary study. Cancer Res 2006; 66:5216-23; PMID:16707446; http://dx.doi.org/10.1158/0008-5472.CAN-05-4193
54. Gatenby RA, Gillies RJ, Brown JS. Evolutionary dynamics of cancer prevention. Nat Rev Cancer 2010; 10:526-7; PMID:21137109; http://dx.doi.org/10.1038/nrc2892
55. Estrella V, Chen T, Lloyd M, Wojtkowiak J, Cornnell HH, Ibrahim-Hashim A, et al. Acidity generated by the tumor microenvironment drives local invasion. Cancer Res 2013; 73:1524-35; PMID:23288510; http://dx.doi.org/10.1158/0008-5472.CAN-12-2796
56. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science 2009; 324:1029-33; PMID:19460998; http://dx.doi.org/10.1126/science.1160809
57. DeBerardinis RJ, Lum JJ, Hatzivassiliou G, Thompson CB. The biology of cancer: metabolic reprogramming fuels cell growth and proliferation. Cell Metab 2008; 7:11-20; PMID:18177721; http://dx.doi.org/10.1016/j.cmet.2007.10.002
58. Jones RG, Thompson CB. Tumor suppressors and cell metabolism: a recipe for cancer growth. Genes Dev 2009; 23:537-48; PMID:19270154; http://dx.doi.org/10.1101/gad.1756509
59. Thompson CB. Rethinking the regulation of cel-lular metabolism. Cold Spring Harb Symp Quant Biol 2011; 76:23-9; PMID:22429931; http://dx.doi.org/10.1101/sqb.2012.76.010496
60. Daye D, Wellen KE. Metabolic reprogramming in cancer: unraveling the role of glutamine in tumor-igenesis. Semin Cell Dev Biol 2012; 23:362-9; PMID:22349059; http://dx.doi.org/10.1016/j.semcdb.2012.02.002
61. Kroemer G, Pouyssegur J. Tumor cell metabolism: cancer’s Achilles’ heel. Cancer Cell 2008; 13:472-82; PMID:18538731; http://dx.doi.org/10.1016/j.ccr.2008.05.005
62. Hanahan D, Weinberg RA. Hallmarks of can-cer: the next generation. Cell 2011; 144:646-74; PMID:21376230; http://dx.doi.org/10.1016/j.cell.2011.02.013
63. Vogelstein B, Kinzler KW. Cancer genes and the pathways they control. Nat Med 2004; 10:789-99; PMID:15286780; http://dx.doi.org/10.1038/nm1087
64. Hanna JH, Saha K, Jaenisch R. Pluripotency and cel-lular reprogramming: facts, hypotheses, unresolved issues. Cell 2010; 143:508-25; PMID:21074044; http://dx.doi.org/10.1016/j.cell.2010.10.008
65. Papp B, Plath K. Reprogramming to pluripotency: stepwise resetting of the epigenetic landscape. Cell Res 2011; 21:486-501; PMID:21321600; http://dx.doi.org/10.1038/cr.2011.28
66. Carey BW, Markoulaki S, Hanna JH, Faddah DA, Buganim Y, Kim J, et al. Reprogramming factor stoi-chiometry influences the epigenetic state and biologi-cal properties of induced pluripotent stem cells. Cell Stem Cell 2011; 9:588-98; PMID:22136932; http://dx.doi.org/10.1016/j.stem.2011.11.003
67. Blum B, Benvenisty N. The tumorigenicity of human embryonic stem cells. Adv Cancer Res 2008; 100:133-58; PMID:18620095; http://dx.doi.org/10.1016/S0065-230X(08)00005-5

©20
13 L
ande
s B
iosc
ienc
e. D
o no
t dis
tribu
te.
www.landesbioscience.com Cell Cycle 1179
108. Sánchez-Aragó M, Formentini L, Cuezva JM. Mitochondria-Mediated Energy Adaption in Cancer: The H(+)-ATP Synthase-Geared Switch of Metabolism in Human Tumors. Antioxid Redox Signal 2012; (Epub ahead of print); PMID:22901241; http://dx.doi.org/10.1089/ars.2012.4883
109. Menendez JA, Vazquez-Martin A. Rejuvenating regeneration: metformin activates endogenous adult stem cells. Cell Cycle 2012; 11:3521-2; PMID:22935702; http://dx.doi.org/10.4161/cc.21878
104. Sánchez-Cenizo L, Formentini L, Aldea M, Ortega AD, García-Huerta P, Sánchez-Aragó M, et al. Up-regulation of the ATPase inhibitory factor 1 (IF1) of the mitochondrial H+-ATP synthase in human tumors mediates the metabolic shift of cancer cells to a Warburg phenotype. J Biol Chem 2010; 285:25308-13; PMID:20538613; http://dx.doi.org/10.1074/jbc.M110.146480
105. Sánchez-Aragó M, Formentini L, García-Bermúdez J, Cuezva JM. IF1 reprograms energy metabolism and signals the oncogenic phenotype in cancer. Cell Cycle 2012; 11:2963-4; PMID:22871729; http://dx.doi.org/10.4161/cc.21387
106. Sánchez-Aragó M, Chamorro M, Cuezva JM. Selection of cancer cells with repressed mitochondria triggers colon cancer progression. Carcinogenesis 2010; 31:567-76; PMID:20080835; http://dx.doi.org/10.1093/carcin/bgq012
107. Willers IM, Cuezva JM. Post-transcriptional regula-tion of the mitochondrial H(+)-ATP synthase: a key regulator of the metabolic phenotype in can-cer. Biochim Biophys Acta 2011; 1807:543-51; PMID:21035425; http://dx.doi.org/10.1016/j.bba-bio.2010.10.016
98. Prigione A, Adjaye J. Modulation of mitochondrial biogenesis and bioenergetic metabolism upon in vitro and in vivo differentiation of human ES and iPS cells. Int J Dev Biol 2010; 54:1729-41; PMID:21305470; http://dx.doi.org/10.1387/ijdb.103198ap
99. Hardie DG. AMP-activated protein kinase: an ener-gy sensor that regulates all aspects of cell function. Genes Dev 2011; 25:1895-908; PMID:21937710; http://dx.doi.org/10.1101/gad.17420111
100. Hardie DG. Adenosine monophosphate-activated protein kinase: a central regulator of metabolism with roles in diabetes, cancer, and viral infection. Cold Spring Harb Symp Quant Biol 2011; 76:155-64; PMID:22071265; http://dx.doi.org/10.1101/sqb.2011.76.010819
101. Hardie DG. Sensing of energy and nutrients by AMP-activated protein kinase. Am J Clin Nutr 2011; 93:891S-6; PMID:21325438; http://dx.doi.org/10.3945/ajcn.110.001925
102. Faubert B, Boily G, Izreig S, Griss T, Samborska B, Dong Z, et al. AMPK is a negative regulator of the Warburg effect and suppresses tumor growth in vivo. Cell Metab 2013; 17:113-24; PMID:23274086; http://dx.doi.org/10.1016/j.cmet.2012.12.001
103. Cuezva JM, Sánchez-Aragó M, Sala S, Blanco-Rivero A, Ortega AD. A message emerging from devel-opment: the repression of mitochondrial beta-F1-ATPase expression in cancer. J Bioenerg Biomembr 2007; 39:259-65; PMID:17712532; http://dx.doi.org/10.1007/s10863-007-9087-9