Embed Size (px)
Citation preview
Helen Campbell
Meningcoccocal conjugate vaccines: epidemiological and
immunological perspective
Clinical Scientist (epidemiology)
Immunisation, Hepatitis and Blood Safety Department
HPA Centre
September 2010

o The contribution of high quality surveillance
to our understanding of how serogroup C
conjugate (MenC) vaccines work on an
individual and population basis.
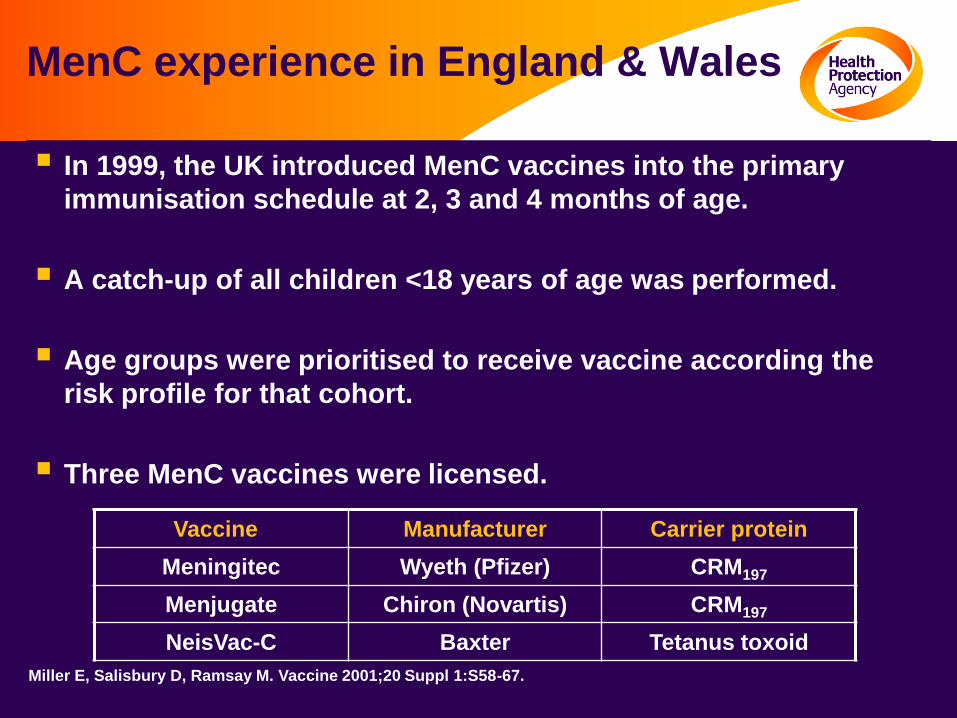
MenC experience in England & Wales
In 1999, the UK introduced MenC vaccines into the primary
immunisation schedule at 2, 3 and 4 months of age.
A catch-up of all children <18 years of age was performed.
Age groups were prioritised to receive vaccine according the
risk profile for that cohort.
Three MenC vaccines were licensed.
Vaccine Manufacturer Carrier protein
Meningitec Wyeth (Pfizer) CRM197
Menjugate Chiron (Novartis) CRM197
NeisVac-C Baxter Tetanus toxoid
Miller E, Salisbury D, Ramsay M. Vaccine 2001;20 Suppl 1:S58-67.
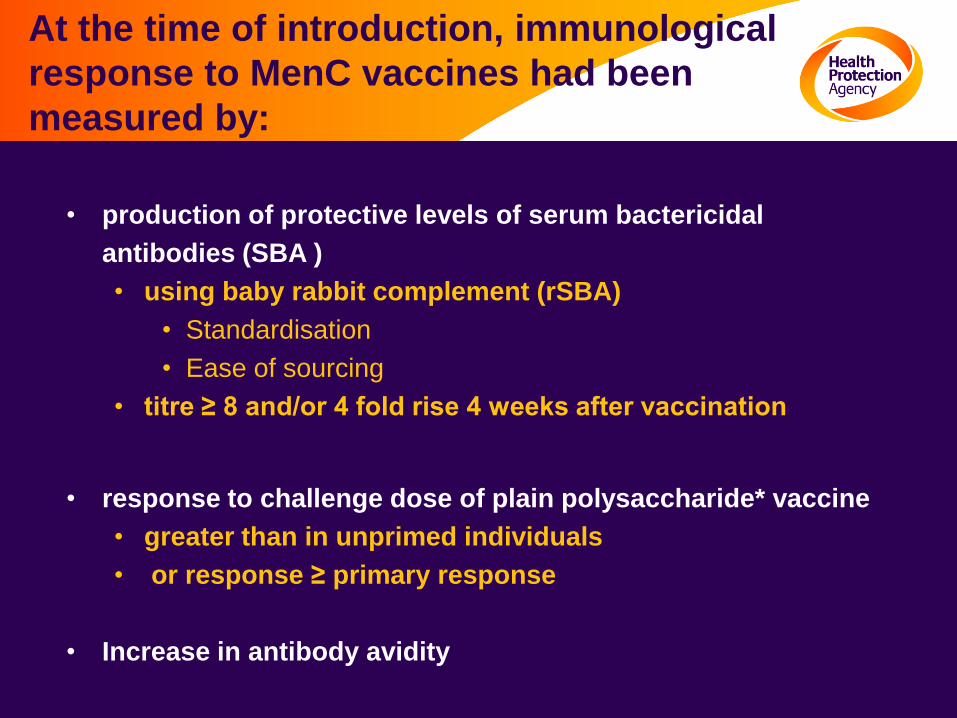
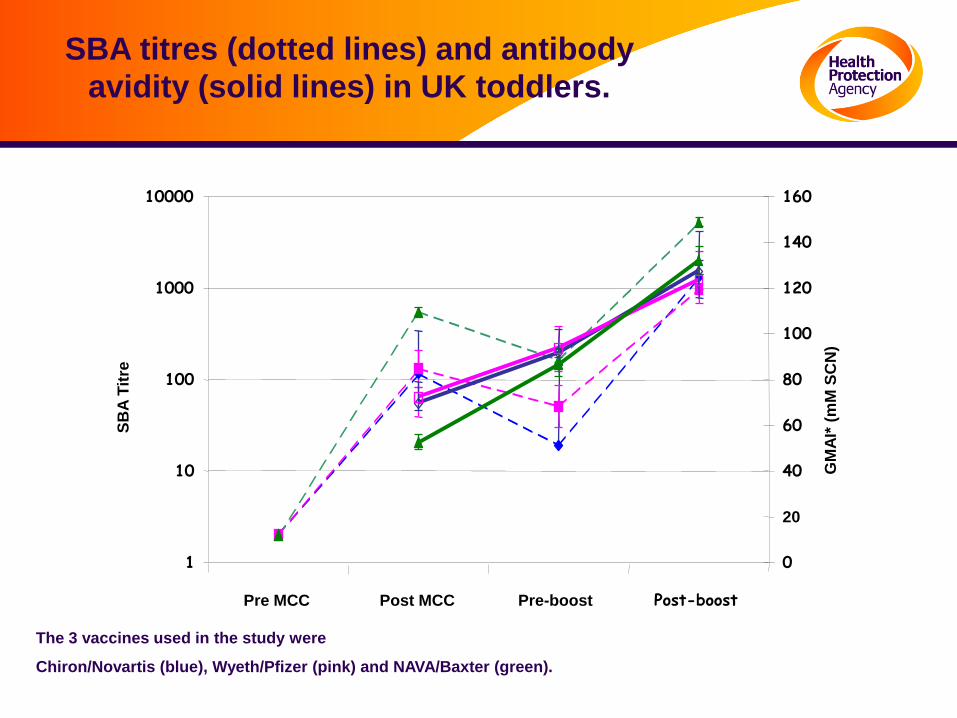
At the time of introduction, immunological
response to MenC vaccines had been
measured by:
• production of protective levels of serum bactericidal
• antibodies (SBA )
• using baby rabbit complement (rSBA)
• Standardisation
• Ease of sourcing
• titre ≥ 8 and/or 4 fold rise 4 weeks after vaccination
• response to challenge dose of plain polysaccharide* vaccine
• greater than in unprimed individuals
• or response ≥ primary response
• Increase in antibody avidity
1
10
100
1000
Pre MCC Post MCC Pre-boost Post-boost
SB
A T
itre
0
20
40
60
80
100
120
GM
AI*
(m
M S
CN
)
10000
140
160
SBA titres (dotted lines) and antibody
avidity (solid lines) in UK toddlers.
The 3 vaccines used in the study were
Chiron/Novartis (blue), Wyeth/Pfizer (pink) and NAVA/Baxter (green).
Surveillance of MenC vaccines post introduction in E&W
• Post-marketing surveillance involved follow up for vaccination history of all laboratory confirmed MenC cases
–Vaccination status of >99% of all MenC cases ascertained
• Vaccine coverage data collected nationally against individual immunisation records
Effectiveness estimates using screening method.
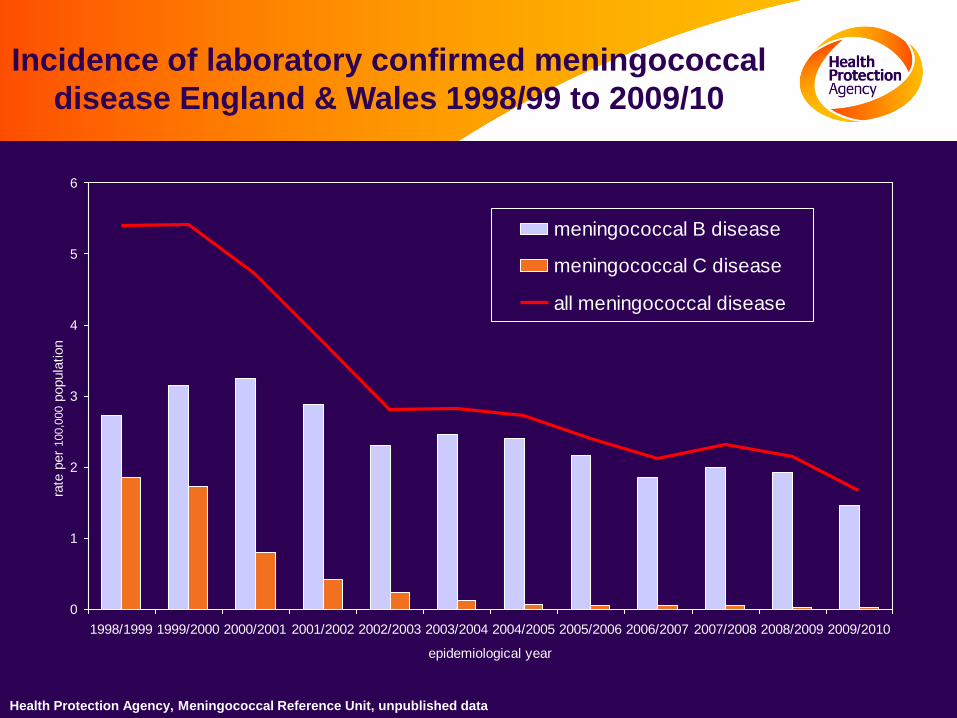
Incidence of laboratory confirmed meningococcal
disease England & Wales 1998/99 to 2009/10
Health Protection Agency, Meningococcal Reference Unit, unpublished data
0
1
2
3
4
5
6
1998/1999 1999/2000 2000/2001 2001/2002 2002/2003 2003/2004 2004/2005 2005/2006 2006/2007 2007/2008 2008/2009 2009/2010
epidemiological year
rate
per
100,0
00 p
opula
tion
meningococcal B disease
meningococcal C disease
all meningococcal disease
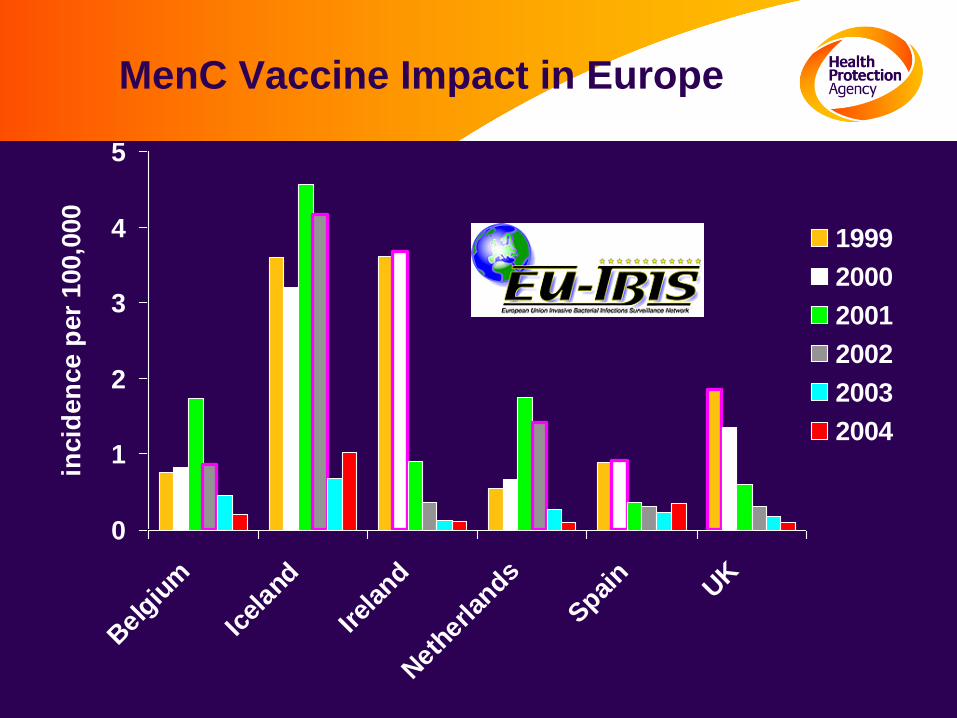
MenC Vaccine Impact in Europe
0
1
2
3
4
5
Bel
gium
Icel
and
Irel
and
Net
herlan
ds
Spai
n UK
incid
en
ce p
er
100,0
00
1999
2000
2001
2002
2003
2004
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
>= 1:4 >= 1:8 >= 1:16 >= 1:32 >= 1:64 >= 1:128
Protective threshold
Va
cc
ine
Eff
ica
cy
(%
)
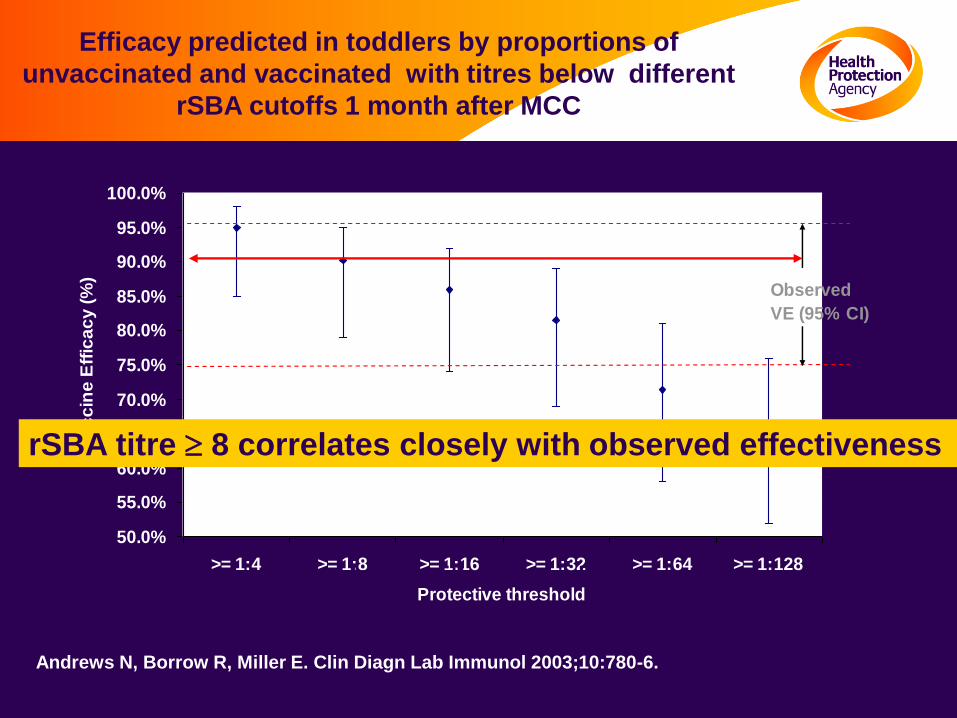
Observed
VE (95% CI)
Andrews N, Borrow R, Miller E. Clin Diagn Lab Immunol 2003;10:780-6.
Efficacy predicted in toddlers by proportions of
unvaccinated and vaccinated with titres below different
rSBA cutoffs 1 month after MCC
rSBA titre 8 correlates closely with observed efficacy
rSBA titre 8 correlates closely with observed effectiveness
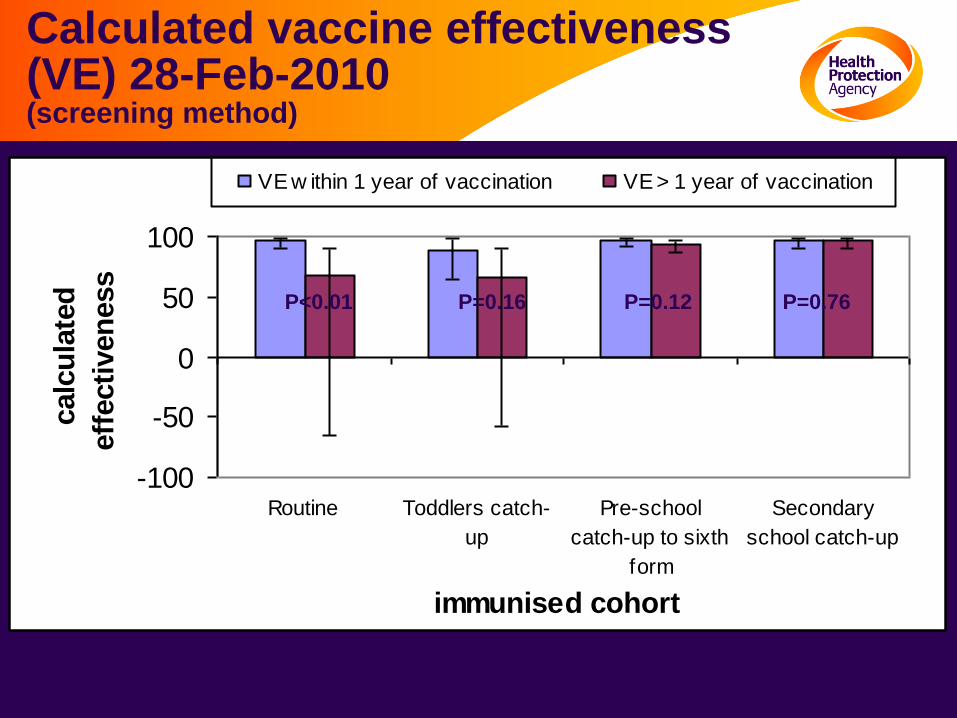
Calculated vaccine effectiveness (VE) 28-Feb-2010 (screening method)
-100
-50
0
50
100
Routine Toddlers catch-
up
Pre-school
catch-up to sixth
form
Secondary
school catch-up
immunised cohort
calc
ula
ted
eff
ecti
ven
ess
VE w ithin 1 year of vaccination VE > 1 year of vaccination
P<0.01 P=0.16 P=0.12 P=0.76
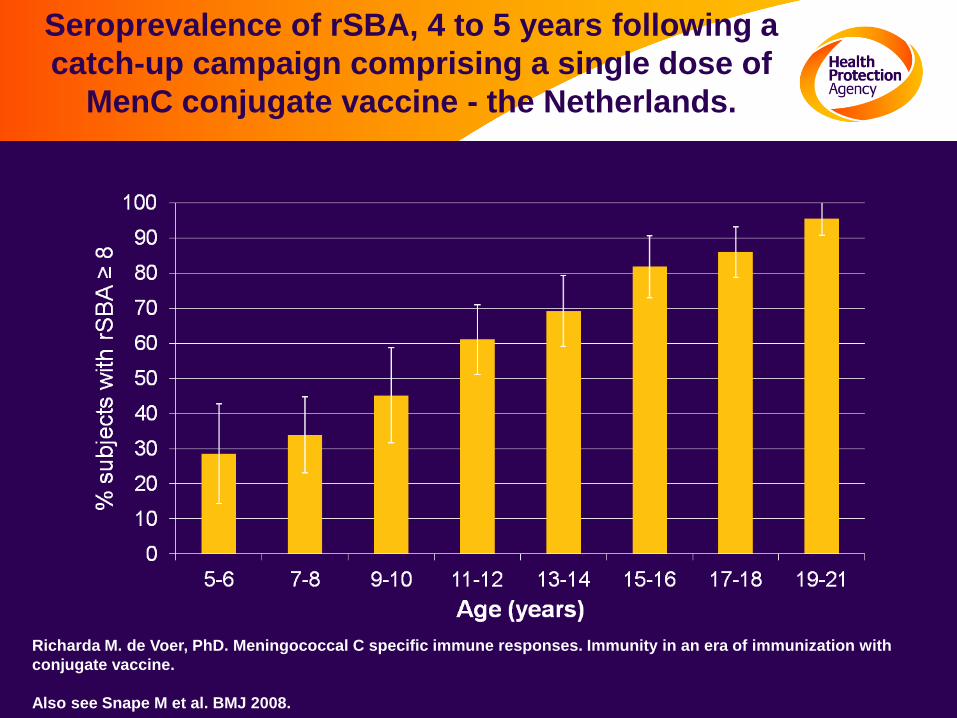
Richarda M. de Voer, PhD. Meningococcal C specific immune responses. Immunity in an era of immunization with
conjugate vaccine.
Also see Snape M et al. BMJ 2008.
Seroprevalence of rSBA, 4 to 5 years following a
catch-up campaign comprising a single dose of
MenC conjugate vaccine - the Netherlands.
Evidence that priming of immune memory did not protect against disease
• Compared SBA titres, IgG levels and avidity indices (AI) in acute and convalescent samples in vaccine failures (n=56) and non-vaccine failures (n=55)
• No evidence of immunodeficiency in vaccine failures.
• AIs in acute serum samples were significantly higher in subjects with vaccine failure than in unvaccinated subjects 3.2-fold higher for AIs [P=.001].
• SBA titers in convalescent serum samples were significantly higher in subjects with vaccine failure than in unvaccinated subjects 6.1-fold higher for SBA titers [P=.03]
Auckland C et al. The Journal of Infectious Disease 2006; 194:1745–52
CONCLUSION:
“The antibody response in the subjects with vaccine
failure was consistent with an anamnestic response,
suggesting that MenC disease occurred despite the
MCC vaccine priming for immune memory…”
Antibody decay post-booster
•UK changed the MenC
routine schedule on 4
September 2006 to 2
doses in infancy (at 3,4
months) and 1 dose at 12
months as MenC-Hib
(Menitorix)
•Meningococcal SBA decay pattern
post booster is very similar (-1.59) to
that post primary (-1.55).
•Thus as time doubles, SBA titres go
down by two thirds.
•MenC IgG decay pattern was -0.95,
thus as time doubles, IgG goes
down by half.
Borrow R, Andrews N, Findlow H, Waight P, Southern J, Crowley-Luke A, Stapley L, England A,
Findlow J, Miller E. Clin Vaccine Immunol. 2010;17:154-9.
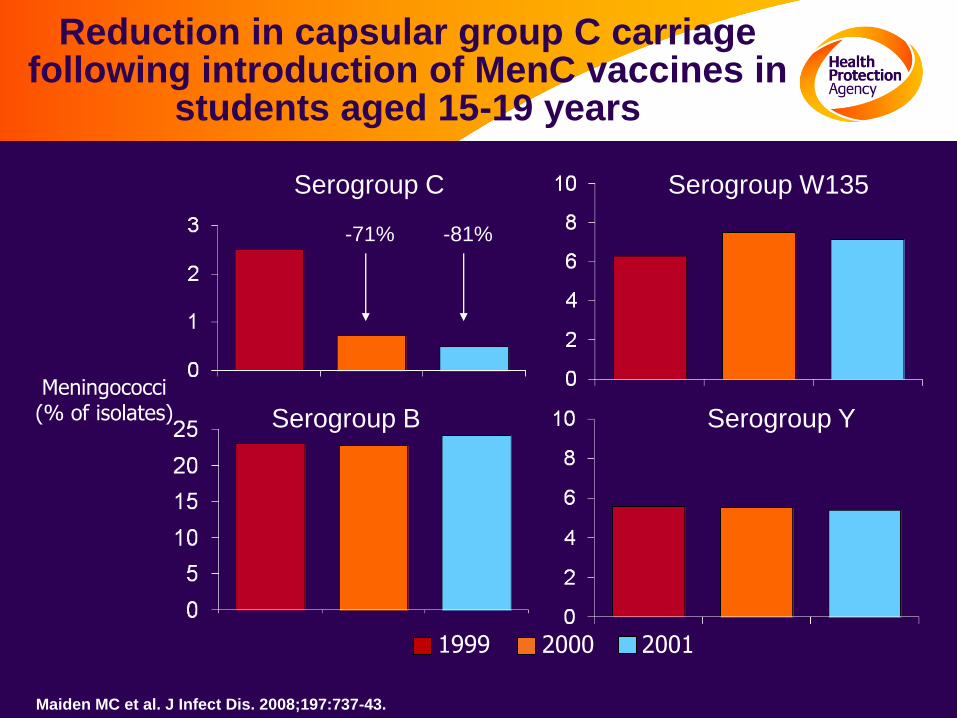
Reduction in capsular group C carriage following introduction of MenC vaccines in
students aged 15-19 years
Meningococci(% of isolates)
1999 2000 2001
Maiden MC et al. J Infect Dis. 2008;197:737-43.
Serogroup C
Serogroup YSerogroup B
Serogroup W135
-71% -81%
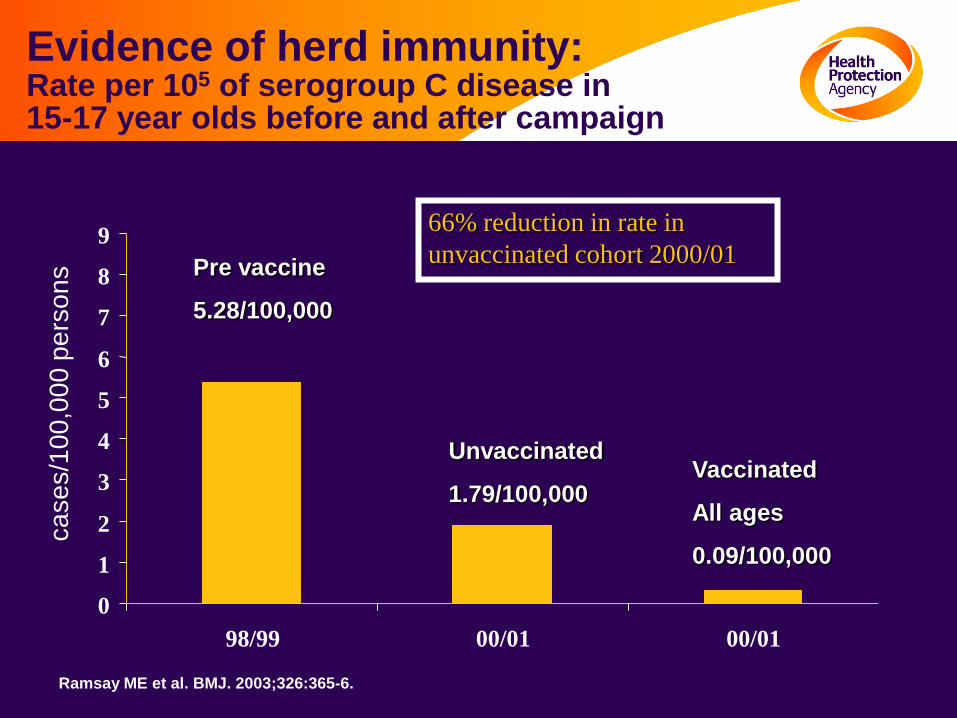
Evidence of herd immunity:Rate per 105 of serogroup C disease in 15-17 year olds before and after campaign
Pre vaccine
5.28/100,000
Unvaccinated
1.79/100,000Vaccinated
All ages
0.09/100,000
66% reduction in rate in
unvaccinated cohort 2000/01
0
1
2
3
4
5
6
7
8
9
98/99 00/01 00/01
Ramsay ME et al. BMJ. 2003;326:365-6.
ca
se
s/1
00
,00
0 p
ers
on
s
0
100
200
300
400
500
600
700
800
1998/
1999
1999/
2000
2000/
2001
2001/
2002
2002/
2003
2003/
2004
2004/
2005
2005/
2006
2006/
2007
2007/
2008
2008/
2009
2009/
2010
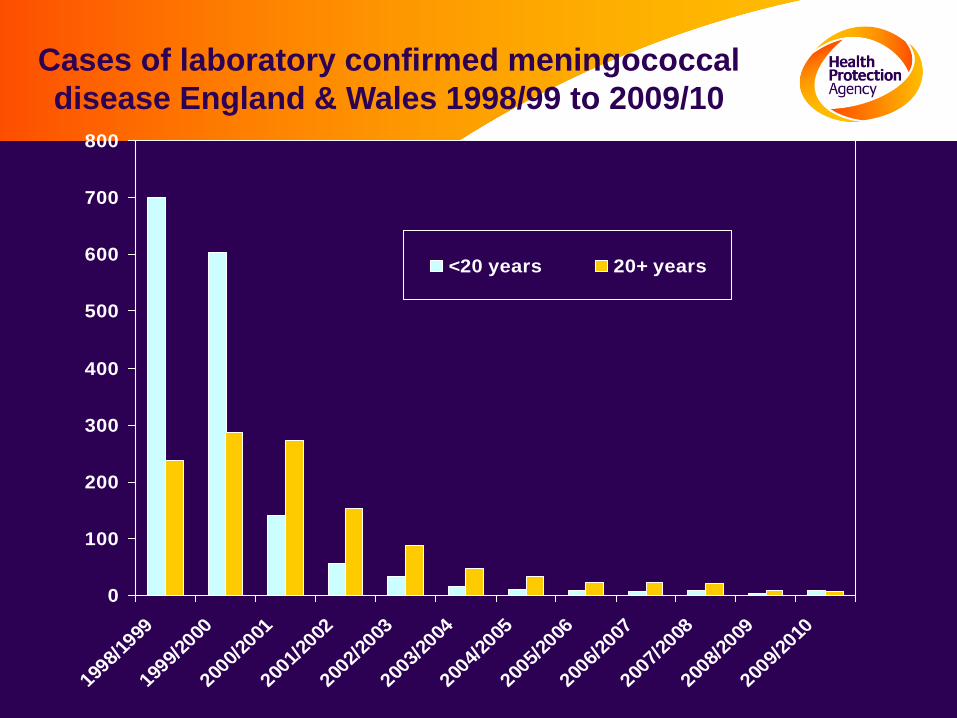
<20 years 20+ years
Cases of laboratory confirmed meningococcal
disease England & Wales 1998/99 to 2009/10
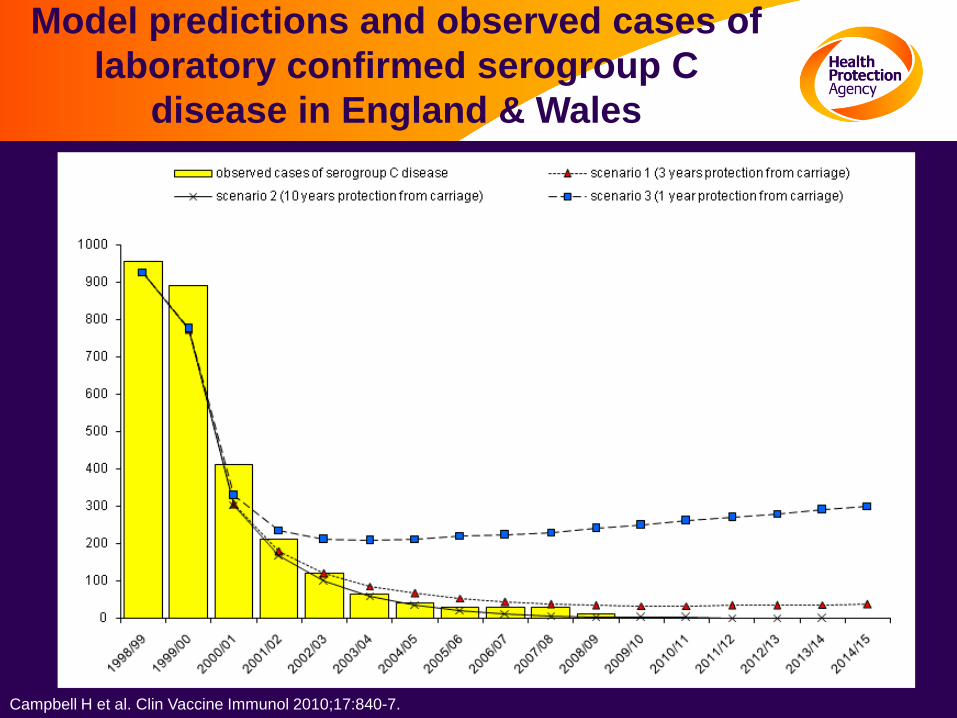
Model predictions and observed cases of
laboratory confirmed serogroup C
disease in England & Wales
Campbell H et al. Clin Vaccine Immunol 2010;17:840-7.
0
10
20
30
40
50
60
70
80
90
100
% w
ith
SB
A t
itre
s ≥
8
Age
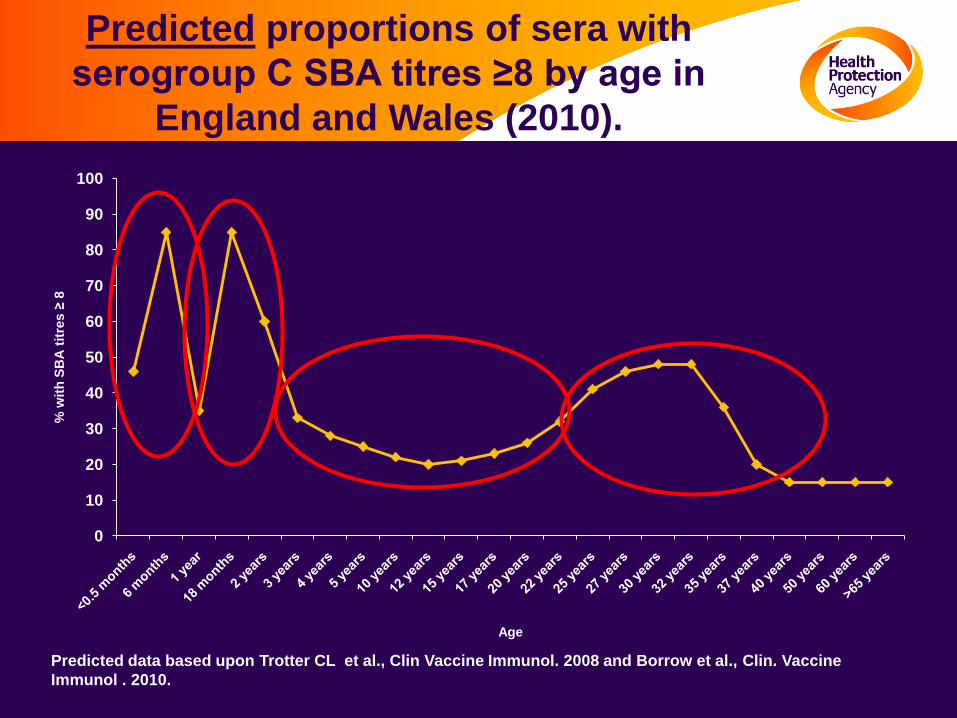
Predicted proportions of sera with
serogroup C SBA titres ≥8 by age in
England and Wales (2010).
Predicted data based upon Trotter CL et al., Clin Vaccine Immunol. 2008 and Borrow et al., Clin. Vaccine
Immunol . 2010.
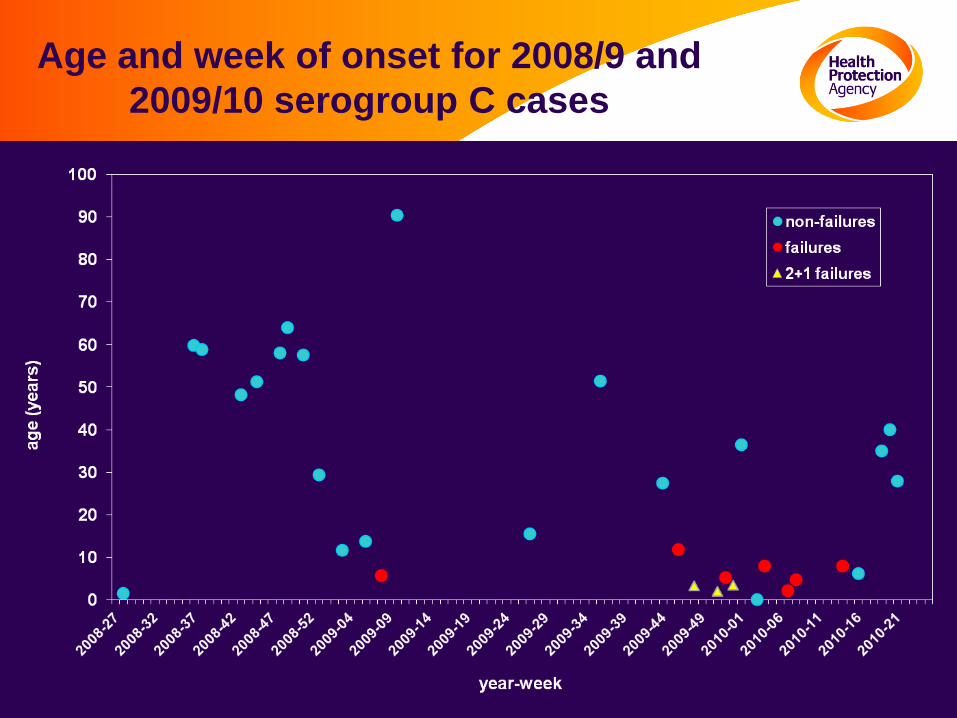
Age and week of onset for 2008/9 and
2009/10 serogroup C cases
Conclusions - MenC
•Ongoing, high quality surveillance with timely analysis
and dissemination of data generated are key.
•Persistence of SBA is recognised as a more appropriate
correlate of long-term protection for MenC vaccines than
immune memory.
•Catch-up campaigns and herd immunity of paramount
importance.
• duration of protection against carriage is not known and
correlates of protection against carriage are lacking.
Acknowledgements
HPA Meningococcal Reference UnitRay Borrow
Steve Gray
Ed Kaczmarski
HPA Immunisation, Hepatitis and Blood Safety DepartmentMary Ramsay
Nick Andrews
Jessica Flood
Shamez Ladhani
University of BristolCaroline Trotter
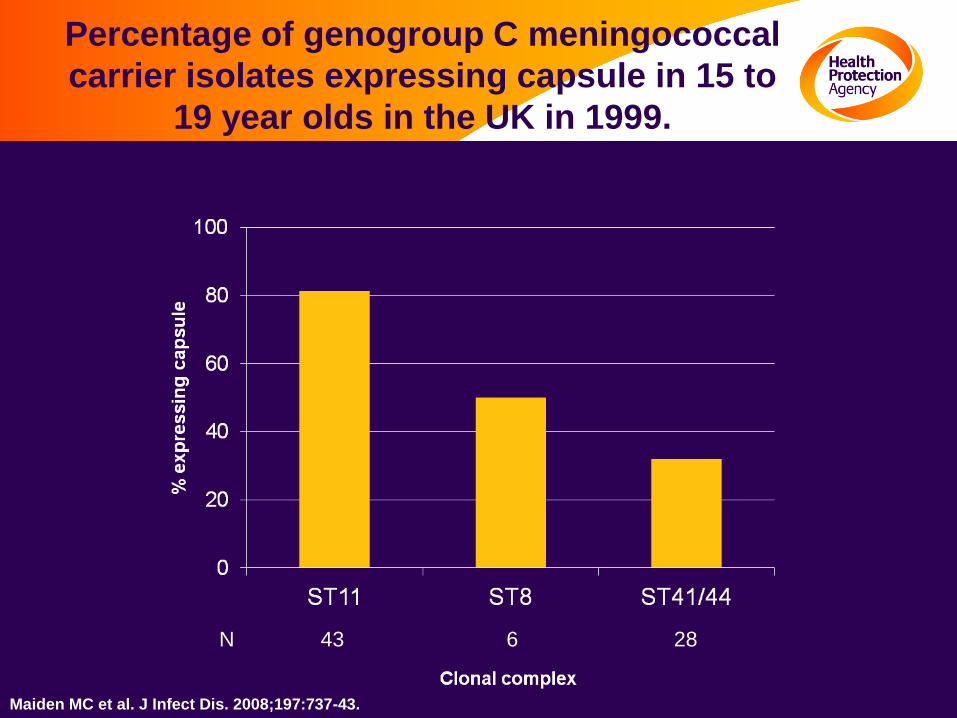
Percentage of genogroup C meningococcal
carrier isolates expressing capsule in 15 to
19 year olds in the UK in 1999.
N 43 6 28
Maiden MC et al. J Infect Dis. 2008;197:737-43.
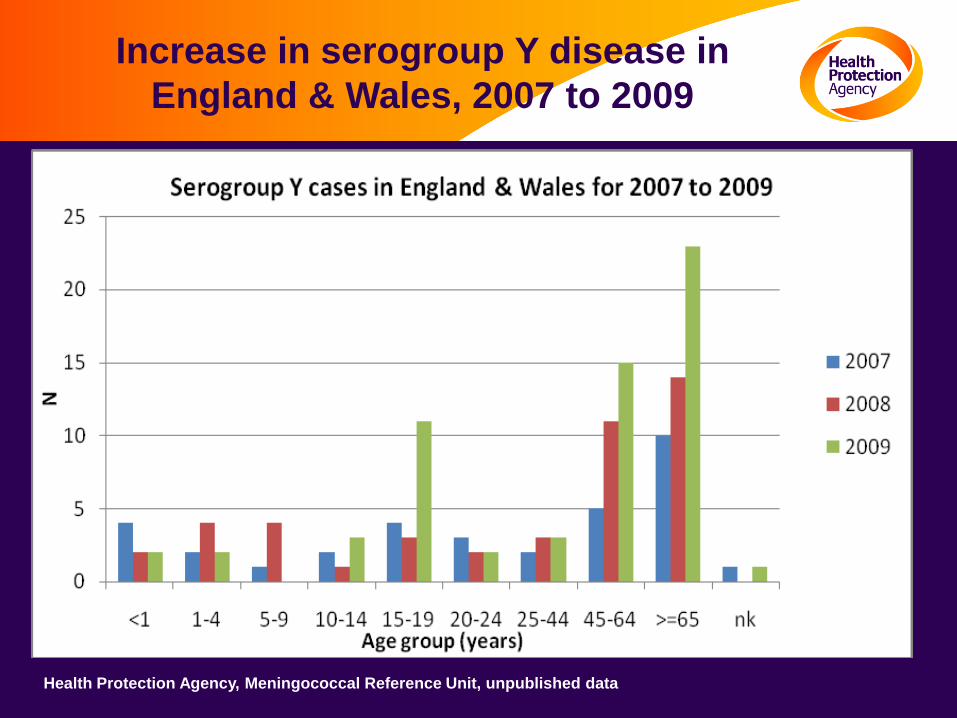
Increase in serogroup Y disease in
England & Wales, 2007 to 2009
Health Protection Agency, Meningococcal Reference Unit, unpublished data