Embed Size (px)
Citation preview
I-MOVE Norway, V3 last updated 10.09.2018
1
Population-level impact of
Pneumococcal Conjugate Vaccines in older adults in Norway
using data provided by routine surveillance systems for Invasive Pneumococcal Disease
October 2015, revised September 2018
I-MOVE Norway, V3 last updated 10.09.2018
2
Original document prepared by I-MOVE+ partners involved in pneumococcal vaccines’ studies from WP3 and WP4, coordinated by EpiConcept and THL.
Partly adapted from the SpIDnet Generic Protocol to measure PCV impact in children developed under the European Centre for Disease Prevention and Control – funded project “Assessing the impact of vaccination with the conjugate vaccines on the epidemiology of the invasive pneumococcal disease in Europe”, ECDC/2012/038, and discussions during SpIDnet expert meetings (Madrid 2012, Paris 2013, Prague 2013).
The revised I-MOVE Norway protocol is based on the generic I-MOVE+ protocol and amended to include extended analyses on Norwegian data in Norway (IMOVE+ Norway). The generic I-MOVE+ protocol has been approved and the study is completed. The I-MOVE+ Norway protocol has been approved, but we apply for some changes.
Funding
The Generic protocol was developed for the Work Package 3 of I-MOVE+ project: Measuring the effects of pneumococcal vaccines in the elderly
I-MOVE+ has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 634446.
The revised I-MOVE+ Norway activities are not part of I-MOVE+ and will be funded by the Norwegian Institute of Public Health.
I-MOVE Norway, V3 last updated 10.09.2018
3
Contents
Innhold Introduction ............................................................................................................................................ 4 1. Background of the protocol ................................................................................................................ 9 2. Objectives ......................................................................................................................................... 10
2.1. Overall objective ........................................................................................................................ 10 2.2. Specific objectives ...................................................................................................................... 10
3. Methods ............................................................................................................................................ 11 3.1. Study design ............................................................................................................................... 11 3.2. Study setting .............................................................................................................................. 11 3.3. Study population ........................................................................................................................ 11 3.4. Study period ............................................................................................................................... 11 3.5. Outcomes ................................................................................................................................... 12 3.6. Laboratory methods................................................................................................................... 13 3.7. Data source and collection......................................................................................................... 13 3.8. Data management ..................................................................................................................... 13
4. Analysis ............................................................................................................................................. 13 4.1. Descriptive analysis ............................................................................................................... 14 4.2. Measure of impact ................................................................................................................ 14 4.3. Adjustments .......................................................................................................................... 15
5. Limitations..................................................................................................................................... 15 5.1. Study design related ............................................................................................................. 15 5.2. Pre-existing vaccination ........................................................................................................ 15 5.3. Case identification and serotyping ....................................................................................... 15
6. Ethical approval ............................................................................................................................. 15 7. Human resources .......................................................................................................................... 16 References ............................................................................................................................................ 17 Attachments .......................................................................................................................................... 18
Attachment 1. Invasive pneumococcal disease (IPD) – Linkage of NPR data for research. ............. 18 Attachment 2 Overview of the included data, its data sources and the percentage of cases with available data .................................................................................................................................... 20 Attachement 3: MSIS variables included in the analysis .................................................................. 22 Attachement 4: data gathered under the generic I-MOVE+ project that will be included for I-MOVE+ Norway ................................................................................................................................. 23

I-MOVE Norway, V3 last updated 10.09.2018
4
Introduction Streptococcus pneumoniae is a Gram-positive diplococcus bacterium causing a wide spectrum of illness either by invading the bloodstream or by mucosal contiguity. Based on capsule polysaccharide composition, more than ninety serotypes of Streptococcus pneumoniae have been identified. These serotypes differ not only in prevalence by area and over time but also in pathogenicity and age distribution. Invasive pneumococcal disease (IPD), defined as the isolation of Streptococcus pneumoniae or the detection of nucleic acid or antigen of Streptococcus pneumoniae from a normally sterile fluid, may present different clinical conditions such as meningitis, bacteraemic pneumonia, bacteraemia without focus, septic shock, and other less frequent conditions such as arthritis, peritonitis, etc. Transmitted by contiguity to middle ear, sinuses or other locations of the respiratory tract, Streptococcus pneumoniae can also cause non-invasive diseases such as acute otitis media, sinusitis or pneumonia. Streptococcus pneumoniae nasopharyngeal colonization, particularly in young children, represent the main reservoir of pneumococci and the primary means of transmission to susceptible individuals. As recent acquisition of Streptococcus pneumoniae in nasopharynx is thought to precede episodes of pneumococcal disease, carriage plays a key role in the epidemiology of pneumococcus. Two major groups of vaccines are currently available to protect against Streptococcus pneumoniae: polysaccharide vaccine (23-valent vaccine - PPV23) and more recently pneumococcal conjugate vaccines (PCVs). PPV23, licensed in 1983, is generally recommended for use in the elderly as well as adults and children ≥2 years with underlying medical conditions (risk groups)1. Pneumococcal conjugate vaccines2 (PCV7, PCV10 and PCV13) covering the 7, 10 and 13 serotypes most frequently causing IPD in developed countries during pre-vaccine era, were licensed in the European Union (EU) in 2001 (PCV7), and in 2009 (PCV10 and PCV13) for the use in children under five years old, with PCV10 and PCV13 replacing PCV7. PCV13 was approved for use in adults in 2011, and in children up to 17 years in November 2012. Currently, PCV13 is licensed for prevention of invasive disease, pneumonia and acute otitis media caused by Streptococcus pneumoniae in infants, children and adolescents from 6 weeks to 17 years of age, as well as for the prevention of invasive disease and pneumonia caused by Streptococcus pneumoniae in adults ≥18 years of age and the elderly3. In Norway, PCV7 was introduced in the childhood vaccination programme in 2006 and was changed to PCV13 in 2011. PCV23 has been recommended for risk groups and elderly for decades. Since 2013, PCV13 is recommended in addition to PPV23 only for a few very high risk groups.
Definition of vaccination effects In epidemiology, effect is the amount of change in a population‘s disease frequency caused by a specific factor. Absolute effects are differences in incidences rates, incidence proportions, prevalences, or incidence time. Relative effects involve ratios of these measures4. Effects in vaccinology measure various absolute or relative changes in incidences observed between populations exposed and not exposed to an intervention (vaccination).
1 WHO, 23-valent pneumococcal polysaccharide vaccine WHO position paper – 2008, WER 2008; 83: 373–384
2 WHO, Pneumococcal vaccines – WHO position paper -2012, WER 2012; 14; 87:, 129–144
3 European Medicines Agency. Prevenar 13: EPAR – Product information. Annex I - Summary of product
characteristics. 12/05/2015.
4 Rothman KJ, Epidemiology – An introduction; Oxford University Press, 2002

I-MOVE Norway, V3 last updated 10.09.2018
5
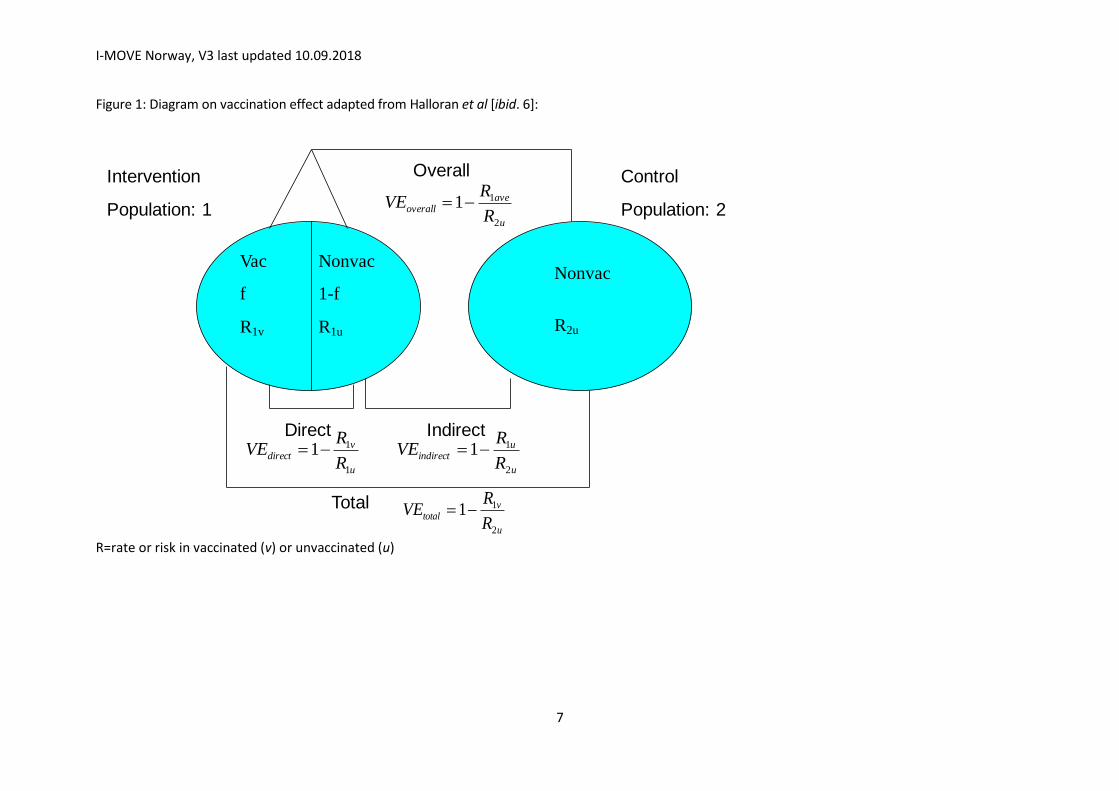
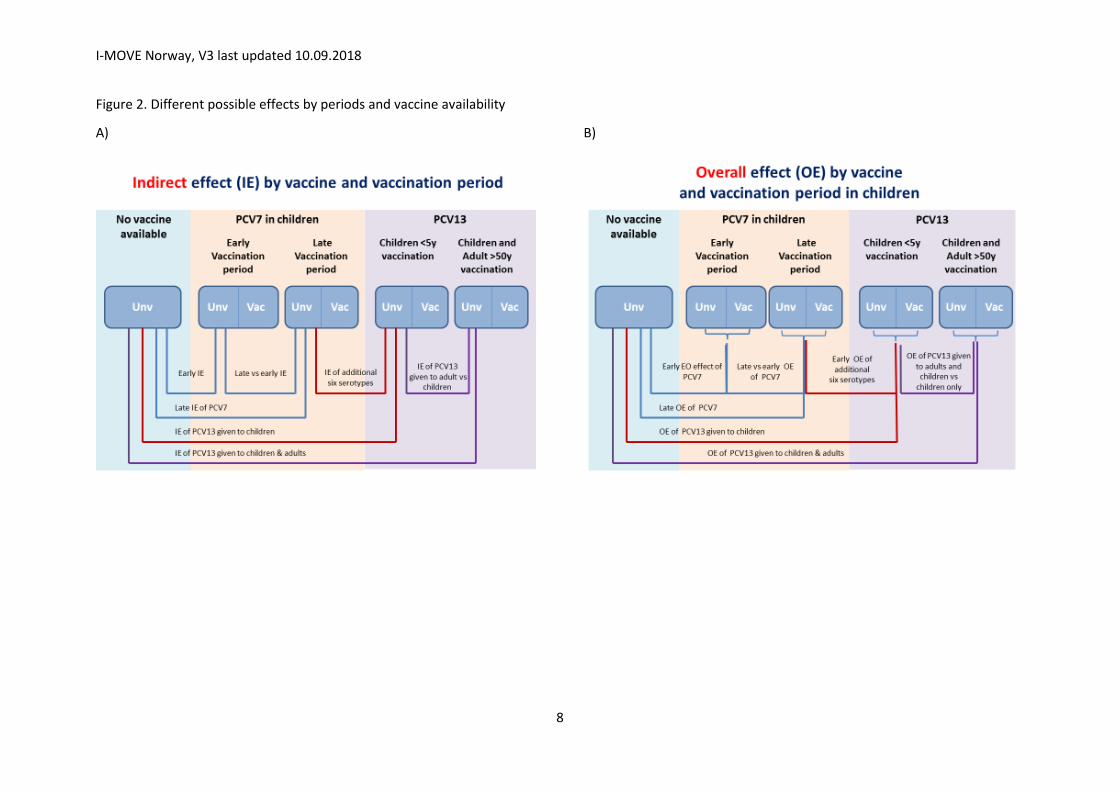
For the purpose of this document, the following terms will be used, based on Halloran5 description of vaccination effects (Figure 1). Overall effect The overall effect is the effect of the vaccination programme in the entire population, including vaccinated and unvaccinated. To measure the overall effect, the overall (average) incidence of disease (or other outcome) of the population in which there is a vaccination programme is compared to the incidence of disease (or other outcome) in a completely unvaccinated population (Figure 1). Indirect effect The indirect effect is the population-level effect on the unvaccinated portion within a population with a vaccination programme. This type of effect is usually estimated by comparing the incidence of disease (or other outcomes) in the unvaccinated portion of a population in which some individuals have been vaccinated, with the incidence of disease (or other outcomes) in a completely unvaccinated population (Figure 1). The indirect effect can be measured by comparing the incidence rates of disease (outcome) in a group never targeted for vaccination before and after the introduction of the vaccination programme. For age-group-specific estimates, the age-groups of interest can vary according to time since introduction of vaccination. For example, unless a catch up campaign is conducted, two years after vaccination, the indirect effect can be measured by comparing outcome rates in those older than two years before and after the introduction of the vaccination programme. Three years after vaccination, the comparison can be made among those aged more than three years; and so on. Total effect The total effect of a vaccination programme measures the population-level effect of vaccination on the vaccinated portion of a population. This can be estimated by comparing the incidence of disease (or other outcome) in the vaccinated portion of a population in which some individuals have been vaccinated, with the incidence of disease (or other outcomes) in a completely unvaccinated population (Figure 1). For the purpose of this document, the term “impact” refers to overall, indirect and total effect of vaccination as the term “effectiveness” refers only to the direct effect of vaccination under field conditions6. An attempt to present the types of effects according to the availability of the childhood and adult vaccination is presented in the Figure 2.
Rationale A total of 1.6 million deaths due to pneumococcal disease occur annually worldwide among all ages7. Despite the decreases in vaccine type IPD rates due to herd effects from routine infant PCV introduction, substantial burden of pneumococcal disease remains in older adults.
5 Halloran ME, Longini Jr IM, Struchiner CJ. Design and Analysis of Vaccine Studies. Series: Statistics for Biology
and Health 2010, XVIII, 389 p. Hardcover, ISBN 978-0-387-40313-7
6 Hanquet G, Valenciano M, Simondon F, Moren A. Vaccine effects and impact of vaccination programmes in
post-licensure studies. Vaccine 2013; doi:10.1016/j.vaccine.2013.07.006
7 WHO. The global burden of disease: 2004 update. Geneva: World Health Organization; 2008.
I-MOVE Norway, V3 last updated 10.09.2018
6
ECDC/Venice II latest estimate of PCV introduction in the 29 EU/EEA MS reported that 24/29 countries had already included PCV in the immunisation programme: 13 (54%) universally recommended, five (21%) recommended to risk groups and six (25%) recommended both universally in children<2 years and in risk groups ≥2 years, and 10 countries included a catch-up campaign. In addition 23/25 respondents to the ECDC/Venice II survey acknowledged the presence in the country of at least an IPD surveillance system and the report presented data on 27 surveillance systems. Of these, 24 are organised at the national level and 25 are comprehensive8. This protocol presents the approach to determine the PCV impact among the older adult population in Norway by using the before and after design with data provided by the Norwegian Surveillance System for Communicable Diseases (MSIS). These data will be linked to hospital discharge data from the Norwegian Patient Registry, date of death form the Population Registry and data on vaccine history from the generic I-MOVE+ study.
8 ECDC and Venice II, Impact of childhood pneumococcal vaccination programmes and activities for
pneumococcal vaccines in the EU and EEA \EFTA countries. Available from
http://venice.cineca.org/VENICE_Survey_PNC_1_2012-02-24.pdf
I-MOVE Norway, V3 last updated 10.09.2018
7
Figure 1: Diagram on vaccination effect adapted from Halloran et al [ibid. 6]:
R=rate or risk in vaccinated (v) or unvaccinated (u)
u
uindirect
R
RVE
2
11
u
aveoverall
R
RVE
2
11
Intervention
Population: 1
Control
Population: 2
Vac
f
R1v
Nonvac
1-f
R1u
Overall
Nonvac
R2u
IndirectDirect
u
vdirect
R
RVE
1
11
Total
u
vtotal
R
RVE
2
11
I-MOVE Norway, V3 last updated 10.09.2018
8
Figure 2. Different possible effects by periods and vaccine availability
A)
B)
I-MOVE Norway, V3 last updated 10.09.2018
9
1. Background of the protocol I-MOVE+ project was part of the work programme PHC 17 – 2014: “Personalising health and care”, “Comparing the effectiveness of existing healthcare interventions in the elderly”. The objectives of the I-MOVE+ network were to identify, pilot test, use, and disseminate in and beyond the EU the best study designs to measure, in near real time the effectiveness and impact of vaccines used in the elderly population to prevent influenza and pneumococcal infections. I-MOVE+ measured the impact of available pneumococcal vaccines against IPD and community acquired pneumonia (CAP) in the elderly population in order to determine the best study designs and data sources needed to be used to provide evidence for informing public health actions at regional, national and supranational levels. The current I-MOVE+ Norway study will measure the impact of the 7- and 13-valent pneumococcal vaccines against IPD and mortality in the elderly Norwegian population over a longer period than originally included in the I-MOVE+ study. Furthermore, I-MOVE+ Norway aims to determine whether the population falling ill and the clinical presentation of IPD has changed during the study period. In Norway, PCV7 was introduced in the childhood immunisation programme in July 2006. Immunisation is provided free of charge at healthy baby clinics in a 2+1 schedule with doses administered at 3, 5 and 12 months of age. In April 2011, PCV7 was replaced with PCV13. Immunisations administered in the childhood immunisation programme are mandatorily recorded in the national immunisation registry (SYSVAK), and the vaccine uptake for the complete schedule is approximately 92%. PPV23 has been available in Norway since 1983. In 1996 a recommendation for use of PPV23 for risk groups and elderly (age ≥ 65 years) was published by the Norwegian Institute of Public Health (NIPH) (1). The recommendations were substantially revised in 2013 (2). The revision included a new description of risk groups, recommendation for revaccination, recommendation for when to perform antibody measurement, and recommendation to use PCV13 for immunisation of the groups with the highest risk for IPD. Pneumococcal vaccination to elderly and risk groups are not reimbursed as a rule, although individuals with certain immunodeficiency conditions can have the costs reimbursed. Immunisations to risk groups, including the elderly, are administered by medical specialists, GPs or at municipal health clinics. Immunisations can be voluntarily recorded in SYSVAK, but presumably the majority of immunisations are not entered in the database. The uptake of PPV23 in risk groups and the elderly has been estimated by sales statistics. In the past decade, approximately 27,000 doses have been distributed annually, and an estimated 15-25% of risk groups are immunized. Surveillance of IPD is performed by NIPH, using the European case definition. Cases are notified by laboratories and clinicians to the Surveillance System for Communicable Diseases (MSIS). Notification from the clinician is missing for up to 25% of notified cases. Isolates of S. pneumoniae are forwarded to the National Reference Laboratory (NRL) at NIPH for serotyping and antimicrobial susceptibility testing. Isolates are received from more than 95 % of notified cases. Data from MSIS, SYSVAK, the National Registry and NRL can be merged by the unique 11-digit personal identification number. The population wide impact of the introduction of PCV7 and the subsequent switch to PCV13 in the childhood immunization program in Norway has been described in cohort studies focusing on the direct and indirect effect, and on antimicrobial resistance (3-6). The impact of pneumococcal
I-MOVE Norway, V3 last updated 10.09.2018
10
carriage has been assessed in cross-sectional studies (7-9). One study has investigated the impact of the indirect effect on iatrogenically-immunosuppressed individuals (10), but studies on the impact in other medical risk groups are lacking.
2. Objectives
2.1. Overall objective
To estimate the impact of the pneumococcal conjugate vaccination programme on the invasive pneumococcal disease (IPD) burden among different risk groups of ≥65 years of age and older. This will be accomplished by comparing incidence rates of IPD before and after changes in the conjugate vaccination programme (PCV7 periods vs. PCV13 period). In Norway, the PCV7 period is from 2006-2010, and the PC13 period from 2011.
2.2. Specific objectives
• Estimate the reduction in the burden among older adults ≥65 years of age, by IPD related outcome such as mortality due to routine infant PCV programmes (herd protection, i.e. indirect effect);
• Estimate the direct effect of adult vaccination on invasive pneumococcal disease. • Understand the timing and magnitude of potential increase in disease from non-vaccine
serotypes (replacement disease). • Describe the changes in IPD incidence, the serotype distribution and whether a change
in the clinical characteristics of the IPD cases has occurred during the seven years since the switch from PCV7 to PCV13
We will use the number of IPD reported to MSIS among the elderly age groups. Denominator data (aggregated data on the size of the risk groups) will be used to calculate IPD incidences; And by:
Serotype category (all serotypes, vaccine serotypes (PCV7, PCV10 non7, PCV13non10, PPV23nonPCV13), vaccine-related, non-vaccine (nonPPV23), specific serotypes); (See Table 1 – Serotypes contained in different pneumococcal vaccines)
Clinical manifestation including fatality;
Comorbidity risk-groups Table 1: Streptococcus pneumoniae serotypes by outcome
Vaccine Serotypes
PCV7 4, 6B, 9V, 14, 18C, 19F, 23F
PCV10non7 1, 5, 7F
PCV13non10 3, 6A, 19A
PPV23nonPCV13 2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F, 33F
I-MOVE Norway, V3 last updated 10.09.2018
11
PPV23 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20,
22F, 23F, 33F
3. Methods
3.1. Study design
Population-based before and after study, comparing IPD rates during the PCV7 period with the period post-PCV13 introduction. The periods before introduction of PCV13 vaccination (PCV7 period) is considered the reference period.
3.2. Study setting
The study is embedded in the routine IPD surveillance system, using the same data sources and databases. MSIS is a nationwide infectious disease registry, and notification of IPD is mandatory. Information about serotype is available for approximately 95% of cases in the PCV7 and PCV13 periods. The surveillance system has not been changed over the past 20 years. MSIS contains variables on clinical presentation and outcome, but the completeness is limited and the validity has not been assessed.
3.3. Study population
The study population comprises all community dwelling individuals ≥65 years of age who are residents of the catchment area of the laboratory / hospitals participating in the already set up surveillance system, for whom information is collected for surveillance purposes.
The population aged ≥65 years in Norway in the period 2009-2017 has been 700 000 and almost
900 000.
3.4. Study period
The study period is 2009-2017. The switch from PCV7 to PCV13 was in 2011. Hospital discharge data (ICD-10 codes) from the Norwegian Patient Register (NPR) will be used to define clinical manifestation and comorbidity risk groups in the IPD population. NPR-data are available for linkage on individual level starting in 2008. To allow for some history in hospitalization the IPD population included in this study starts in 2009. This will allow for a two year reference period before switching from PCV7 to PCV13, and account for changes in medical and diagnostic practices and surveillance activities.
Definitions of periods before and after the PCV introduction PCV7 period: 2009-2010 will be used as PCV7 period.
I-MOVE Norway, V3 last updated 10.09.2018
12
Post-13 period: 2012-2017 will be used as PCV13 period. 2011 is regarded a transition year; PCV13 replaced PCV7 in April 2011.
3.5. Outcomes
The primary outcome of interest is laboratory confirmed IPD (isolation or detection of Streptococcus pneumoniae from a normally sterile site).
Secondary outcomes include:
1. IPD cases due to vaccine, vaccine-related, non-vaccine related or specific serotypes. The following categories will be considered: PCV7, PCV10non7, PCV13non10, PPV23nonPCV13, nonPPV23 (Table 1)
2. Clinical manifestation in IPD-cases, by serotype and co-morbidity 3. Fatality by clinical presentation, co-morbidity risk, serotypes and age 4. Vaccine-type IPD by vaccine history for the period 2015-2017
Case definitions IPD is defined according to the ECDC case definition used for surveillance purposes9 :
PNEUMOCOCCAL INVASIVE DISEASE(S) (Streptococcus pneumoniae) Clinical criteria Not relevant for surveillance purposes Laboratory criteria At least one of the following three: — Isolation of Streptococcus pneumoniae from a normally sterile site — Detection of Streptococcus pneumoniae nucleic acid from a normally sterile site — Detection of Streptococcus pneumoniae antigen from a normally sterile site Epidemiological criteria NA Case classification A. Possible case NA B. Probable case NA C. Confirmed case Any person meeting the laboratory criteria
For the primary outcome (all type IPD), a case is defined as a patient with laboratory confirmed IPD according to the ECDC case definition. For secondary outcomes, a case is defined as above for the primary outcome, and if:
1. Pneumococcal serotype is determined 2. Clinical presentation is available (defined by ICD-codes from NPR and as reported in MSIS) 3. Information on co-morbidities is available (defined by ICD-codes from NPR) 4. 30 days case fatality (defined by date of death from the Population Registry)
9 European Commission, Commission Decision 2008/426/EC of 28 April 2008 amending Decision 2002/253/EC laying down
case definitions for reporting communicable diseases to the Community network under Decision No 2119/98/EC of the European Parliament and of the Council (notified under document number C(2008) 1589)
I-MOVE Norway, V3 last updated 10.09.2018
13
5. By vaccine history for cases notified in 2015-2017 (data obtained during the generic I-MOVE+ study)
3.6. Laboratory methods
To fulfil the IPD case definition, cases should be laboratory confirmed by culture or PCR/Ag testing. In addition, for the secondary outcomes, serotyping is needed.
● During the study period, serotyping of isolates was performed at the reference laboratory using capsular reaction testing (Quellung test)(Statens Serum Institut, Denmark).
Specimen from normally sterile body sites have been collected at hospitals and processed at hospital diagnostic laboratories. Isolates have been forwarded to the NRL at NIPH on transport media.
3.7. Data source and collection
Cases (numerator) Case based IPD data will be extracted from MSIS 2009-2017. Data on serotype will be extracted from the NRL laboratory database.
Denominator Annual population data will be retrieved from Statistics Norway. Aggregated data on the size of the comorbidity groups will be obtained from NPR.
Vaccination coverage We will use vaccine information for IPD cases notified to MSIS in 2015-2017. This information is available from the completed I-MOVE effectiveness study.
Case fatality We will calculate 30 days case fatality based on information on date of death from the Population registry in Norway and the date of the IPD diagnosis from MSIS.
3.8. Data management
Extraction of IPD data and from MSIS and storage of key file with personally identifiable data will be
managed by a dedicated data-manager, Department of Infectious Disease Registries at NIPH.
Identifiable data will be stored separate from study data in a secured server for research data
according to NIPH routines. Each individuals’ 11 digit ID number will be replaced with a study ID for
data-linkage.
De-identified data from MSIS, NPR and the National Registry will be linked through the study ID
number. Data will be analysed by Brita A. Winje, Didrik F. Vestrheim and Anneke Steens from the
Department of Vaccine Preventable Diseases, and Richard White from the Department of Infectious
Disease Epidemiology and Modelling at NIPH. We will use Excel, SPSS and Stata. De-identified data
will be stored in a password protected server area.
4. Analysis
I-MOVE Norway, V3 last updated 10.09.2018
14
4.1. Descriptive analysis
IPD cases will be described by time period, age group, serotype categories, clinical presentation, co-morbidities and outcome.
The (disease-, age group- and vaccine-specific) incidences of IPD will be calculated by dividing the number of cases by the size of the subgroups in the Norwegian population and will be presented per 100,000 inhabitants.
We will categorise cases into medical risk groups using ICD-10 codes (see attachment 1, table 2). We include ICD-10 codes for co-morbidity only if registered within the last two years before the date of diagnosis. In Norway, hospital discharge data are only available on individual level for registry linkage since 2008. For IPD-cases reported in 2009, we included all available data from January 2008 up to the date of testing. Those with no registered medical risk condition in the two years prior to the sampling date will be assumed not to have a medical risk condition. We include ICD-10 codes for clinical presentation only if registered 30 days before or after the date of the IPD diagnosis. Relevant ICD-10 codes and the classification is presented in full in attachment 1, table 1a-c.We will further apply to NPR for aggregated data on risk conditions for the total population as a population denominator and to explore the role of shifts in the population during the study period.
4.2. Measure of impact
The impact (see also 10) is computed as:
the reduction in the number of cases in the post-PCV13 period compared with the reference period, expressed as absolute numbers or percentage change in the number of cases;
the reduction in the cumulative incidence or rate in the post-PCV13 period compared with the reference period, expressed as rate/risk difference;
the relative reduction in the incidence proportion or rate during the post-PCV13 period, expressed as the annual change in incidence rate ratio with the corresponding 95% CI.
A change in the serotype distribution and vaccine-type / non-vaccine type IPD incidence
A change in the incidence and proportion of the different clinical presentations (meningitis, invasive pneumonia, bacteraemia without focus, pyogenic arthritis and others) and fatality
A change in the prevalence of comorbidities in the population falling ill
The impact will be analysed separately for the different comorbidity groups.
On the basis of estimates of pneumococcal vaccination uptake among individuals 65 years of age and older, we can describe:
an overall effect: the measure of impact in the age group >65 years of age in a population where a proportion of people in this age group and in the paediatric age group is vaccinated compared with the same population before the introduction of the vaccination programmes;
indirect effect: the measure of impact of infant conjugate vaccination programme among persons >65 years of age in the absence of direct PCV13 vaccination programme in older adults, compared to the same population before the introduction of the infant vaccination programme;
10 Hanquet G, Valenciano M, Simondon F, Moren A. Vaccine effects and impact of vaccination programmes in post-licensure studies. Vaccine 2013; doi:10.1016/j.vaccine.2013.07.006
I-MOVE Norway, V3 last updated 10.09.2018
15
4.3. Adjustments
Adjustment for missing data on serotype will be done by assuming similar distribution of serotypes/cases with information to serotypes/cases without information. The proportion of cases missing serotype data is limited in the post-PCV era.
5. Limitations
5.1. Study design related
In studies comparing pre and post intervention, the main limitation is that the effect measured can be due to other factors not related to vaccination.. Therefore, different factors should be considered, such as:
changes in case detection and ascertainment
changes in sensitivity of the surveillance system
secular trends
changes in medical practices and in health seeking behaviour
other factors that may influence IPD incidence
The surveillance system in Norway has remained unchanged throughout the study period, with no known changes to sensitivity of laboratory methods or guidelines for clinical diagnosis.
5.2. Pre-existing vaccination
In Norway, PCV7 was licensed in 2001, but the use was limited until introduction in the childhood immunisation programme in 2006. PPV23 has been available since 1983, and recommended to risk groups and adults aged 65 years and more since 1996. The use of PPV23 has been limited and stable over the last ten years, according to sales statistics.
5.3. Case identification and serotyping
Laboratory-based case identification implies good specificity and sensitivity of the case definition. Moving from the culture-based case confirmation (low sensitivity, high specificity) to PCR (higher sensitivity, high specificity) will increase the number of IPD cases identified and underestimates the impact estimate. In addition increase in testing and serotyping will also underestimate impact. However it can also help identify new or emerging serotypes causing IPD. This has a high importance in identifying replacement.
No major changes have been made to laboratory diagnostics in Norway during the study period. PCR is used by some laboratories for identification of pneumococci from CSF, but is not used for identification in blood/serum. The proportion of isolates from notified cases of IPD received at the NRL increased following introduction of PCV7. However, this is reflecting a change in isolate referral and intensified prompting by the NRL, and not a change in diagnostic routines.
6. Ethical approval
We will apply for a change in the obtained ethical clearance from the Committee of Research Ethics
I-MOVE Norway, V3 last updated 10.09.2018
16
in Norway for the following amendments:
Extension of study end date from Dec 31.2018 to Dec 31 2021 for I-MOVE+ Norway. This will only include data management and data analysis in Norway. The European I-MOVE+ project will be finalized 31.12.2018 as previously planned
Linkage with date of death from the National Registry
7. Human resources
The roles and responsibilities of the members of the investigation team should be described: principal investigator, assistant, data manager, etc.
Brita A. Winje: principal investigator epidemiology, researcher
Kirsten Konsmo: data management.
Anneke Steens: researcher epidemiology
Didrik F. Vestrheim: principal investigator laboratory, researcher
Richard A White: researcher, statistics
I-MOVE Norway, V3 last updated 10.09.2018
17
References 1. Høiby EA, Aaberge IS, Froholm LO, Hareide B, Lystad A, Nokleby H. 1996. Utvidet bruk av
pneumokokkvaksine i Norge. folkehelse Sif, Oslo, Norway. 2. Furuseth E, Rønning K, Steens A, Aaberge IS, Vestrheim DF, Bergsaker MA, Storsaeter J,
Wiklund BS. 2013. Anbefalinger for bruk av pneumokokkvaksine utfenfor barnevaksinasjonsprogram i Norge. Norwegian Institute of Public Health, Oslo.
3. Vestrheim DF, Lovoll O, Aaberge IS, Caugant DA, Hoiby EA, Bakke H, Bergsaker MR. 2008. Effectiveness of a 2+1 dose schedule pneumococcal conjugate vaccination programme on invasive pneumococcal disease among children in Norway. Vaccine 26:3277-3281.
4. Vestrheim DF, Høiby EA, Bergsaker MR, Rønning K, Aaberge IS, Caugant DA. 2010. Indirect effect of conjugate pneumococcal vaccination in a 2+1 dose schedule. Vaccine 28:2214-2221.
5. Steens A, Bergsaker MA, Aaberge IS, Ronning K, Vestrheim DF. 2013. Prompt effect of replacing the 7-valent pneumococcal conjugate vaccine with the 13-valent vaccine on the epidemiology of invasive pneumococcal disease in Norway. Vaccine 31:6232-6238.
6. Vestrheim DF, Steinbakk M, Aaberge IS, Caugant DA. 2012. Postvaccination Increase in Serotype 19A Pneumococcal Disease in Norway Is Driven by Expansion of Penicillin-Susceptible Strains of the ST199 Complex. Clinical and Vaccine Immunology 19:443-445.
7. Vestrheim DF, Hoiby EA, Aaberge IS, Caugant DA. 2008. Phenotypic and genotypic characterization of Streptococcus pneumoniae strains colonizing children attending day-care centers in Norway. Journal of Clinical Microbiology 46:2508-2518.
8. Vestrheim DF, iby EA, Aaberge IS, Caugant DA. 2010. Impact of a pneumococcal conjugate vaccination program on carriage among children in Norway. Clinical and Vaccine Immunology: CVI 17:325-334.
9. Steens A, Caugant DA, Aaberge IS, Vestrheim DF. 2015. Decreased carriage and genetic shifts in the Streptococcus pneumoniae population after changing the 7-valent to the 13-valent pneumococcal vaccine in Norway. Pediatr Infect Dis J doi:10.1097/INF.0000000000000751.
10. Steens A, Winje BA, White RA, Odsbu I, Brantsaeter AB, Vestrheim DF. 2018. Indirect effects of pneumococcal childhood vaccination in individuals treated with immunosuppressants in ambulatory care: a case-cohort study. Clinical Infectious Diseases.
I-MOVE Norway, V3 last updated 10.09.2018
18
Attachments
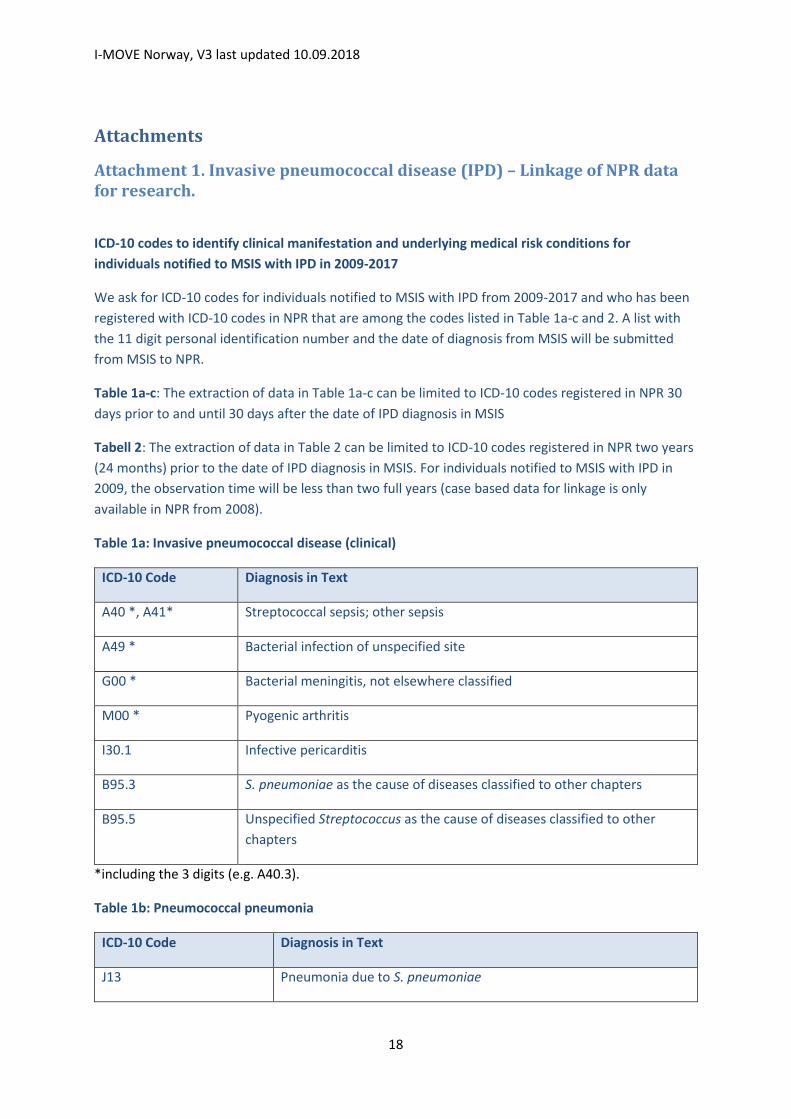
Attachment 1. Invasive pneumococcal disease (IPD) – Linkage of NPR data for research.
ICD-10 codes to identify clinical manifestation and underlying medical risk conditions for
individuals notified to MSIS with IPD in 2009-2017
We ask for ICD-10 codes for individuals notified to MSIS with IPD from 2009-2017 and who has been
registered with ICD-10 codes in NPR that are among the codes listed in Table 1a-c and 2. A list with
the 11 digit personal identification number and the date of diagnosis from MSIS will be submitted
from MSIS to NPR.
Table 1a-c: The extraction of data in Table 1a-c can be limited to ICD-10 codes registered in NPR 30
days prior to and until 30 days after the date of IPD diagnosis in MSIS
Tabell 2: The extraction of data in Table 2 can be limited to ICD-10 codes registered in NPR two years
(24 months) prior to the date of IPD diagnosis in MSIS. For individuals notified to MSIS with IPD in
2009, the observation time will be less than two full years (case based data for linkage is only
available in NPR from 2008).
Table 1a: Invasive pneumococcal disease (clinical)
ICD-10 Code Diagnosis in Text
A40 *, A41* Streptococcal sepsis; other sepsis
A49 * Bacterial infection of unspecified site
G00 * Bacterial meningitis, not elsewhere classified
M00 * Pyogenic arthritis
I30.1 Infective pericarditis
B95.3 S. pneumoniae as the cause of diseases classified to other chapters
B95.5 Unspecified Streptococcus as the cause of diseases classified to other
chapters
*including the 3 digits (e.g. A40.3).
Table 1b: Pneumococcal pneumonia
ICD-10 Code Diagnosis in Text
J13 Pneumonia due to S. pneumoniae
I-MOVE Norway, V3 last updated 10.09.2018
19
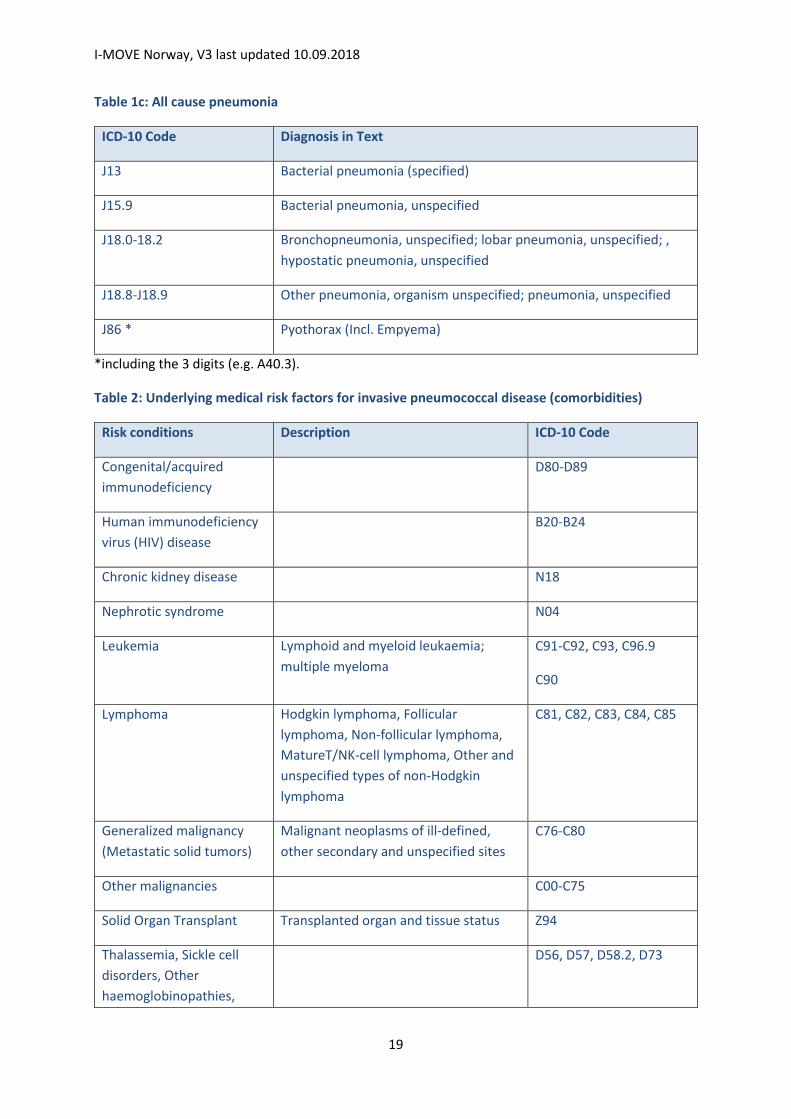
Table 1c: All cause pneumonia
ICD-10 Code Diagnosis in Text
J13 Bacterial pneumonia (specified)
J15.9 Bacterial pneumonia, unspecified
J18.0-18.2 Bronchopneumonia, unspecified; lobar pneumonia, unspecified; ,
hypostatic pneumonia, unspecified
J18.8-J18.9 Other pneumonia, organism unspecified; pneumonia, unspecified
J86 * Pyothorax (Incl. Empyema)
*including the 3 digits (e.g. A40.3).
Table 2: Underlying medical risk factors for invasive pneumococcal disease (comorbidities)
Risk conditions Description ICD-10 Code
Congenital/acquired
immunodeficiency
D80-D89
Human immunodeficiency
virus (HIV) disease
B20-B24
Chronic kidney disease N18
Nephrotic syndrome N04
Leukemia Lymphoid and myeloid leukaemia;
multiple myeloma
C91-C92, C93, C96.9
C90
Lymphoma Hodgkin lymphoma, Follicular
lymphoma, Non-follicular lymphoma,
MatureT/NK-cell lymphoma, Other and
unspecified types of non-Hodgkin
lymphoma
C81, C82, C83, C84, C85
Generalized malignancy
(Metastatic solid tumors)
Malignant neoplasms of ill-defined,
other secondary and unspecified sites
C76-C80
Other malignancies C00-C75
Solid Organ Transplant Transplanted organ and tissue status Z94
Thalassemia, Sickle cell
disorders, Other
haemoglobinopathies,
D56, D57, D58.2, D73

I-MOVE Norway, V3 last updated 10.09.2018
20
Diseases of the spleen
(including anatomical
asplenia)
Cerebrospinal fluid (CSF)
leak
G96.0
Cochlear implant Z96.2
Chronic heart disease Chronic ischemic heart disease,
Cardiomyopathy, Heart failure
I25, I42, I50
Chronic lung disease Emphysema, Other COPD, Asthma J43, J44, J45
Diabetes mellitus Type 1 Diabetes, Type 2 Diabetes,
Malnutrition-related diabetes, Other
specified diabetes, Unspecified diabetes
E10, E11, E12, E13, E14
Alcoholism Mental and behavioural disorders due
to use of alcohol, Degeneration of
nervous system due to alcohol,
Alcoholic polyneuropathy, Alcoholic
myopathy, Alcoholic cardiomyopathy,
Alcoholic gastritis, Alcoholic liver
disease, Alcohol-induced acute
pancreatitis, Alcohol-induced chronic
pancreatitis, Maternal care for
(suspected) damage to fetus from
alcohol,
F10, G31.2, G62.1, G72.1,
I42.6, K29.2, K70, K85.2,
K86.0, O35.4
Chronic liver disease,
cirrhosis
Hepatic failure, NES, Chronic hepatitis,
NES, Fibrosis and cirrhosis, Other
diseases of liver, Malignancy of liver
K72, K73, K74, K76, K76.9,
C22
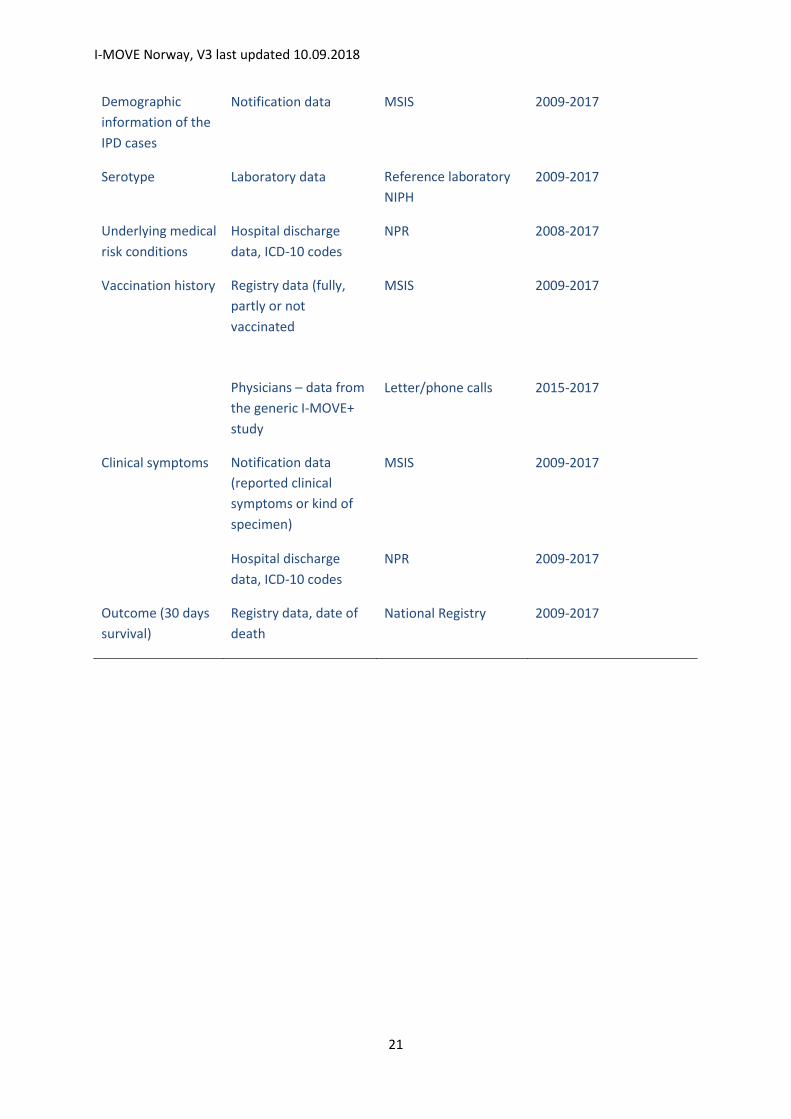
Attachment 2 Overview of the included data and its data sources
Variable Kind of data Data source Years included
Index date / year Notification data, date
of sampling of material
for pneumococcal
identification
MSIS 2009-2017
I-MOVE Norway, V3 last updated 10.09.2018
21
Demographic
information of the
IPD cases
Notification data MSIS 2009-2017
Serotype Laboratory data Reference laboratory
NIPH
2009-2017
Underlying medical
risk conditions
Hospital discharge
data, ICD-10 codes
NPR 2008-2017
Vaccination history Registry data (fully,
partly or not
vaccinated
MSIS 2009-2017
Physicians – data from
the generic I-MOVE+
study
Letter/phone calls 2015-2017
Clinical symptoms Notification data
(reported clinical
symptoms or kind of
specimen)
MSIS 2009-2017
Hospital discharge
data, ICD-10 codes
NPR 2009-2017
Outcome (30 days
survival)
Registry data, date of
death
National Registry 2009-2017

I-MOVE Norway, V3 last updated 10.09.2018
22
Attachment 3: MSIS variables included in the analysis
Variable from MSIS Use in this study
Age in years
Sex
Date of testing Used as index date
Material used for testing Used in the definition of clinical picture
Method used for testing To determine the proportion that has been
cultured
Pneumococcal serotype
Clinical picture Combined with the ICD-10 codes
(supplementary table 2) to define clinical
picture
Outcome (healthy, still ill, died) Intra hospital death
Vaccine history Fully / partially / un-vaccinated

I-MOVE Norway, V3 last updated 10.09.2018
23
Attachment 4: data gathered under the generic I-MOVE+ project that will be included for I-MOVE+ Norway
Date of each PPV23 dose Used to define yes/no vaccinated with PPV23
the last 10 years, up to 14 days before the
index date; used to define “vaccine failure”.
2015-2017
Date of each PCV dose
Kind of PCV (PCV7/PCV10/PCV13)
Used to define yes/no vaccinated with PCV
up to 14 days before the index date; used to
define “vaccine failure”. 2015-2017