Embed Size (px)
Citation preview


Apa yang anda ukur



Penilaian hasil rekaman EKG: Frekuensi (rate) dihitung / menit Irama (rythm): regular / irregular Zona transisi V1-V6 Axis Elektrik: sumbu (derajat), posisi (normal, left, right, indeterminate / right superior / northwest) Interval PR, QRS, dan QT dalam detik Lain-lain

Berapa kecepatan kertas ECG bergerak: 25 mm/detik
1 mv beda potensial antara kedua elektrodaakan terekam setinggi berapa cm ?
1 cm

Berapa Frekuensinya:
Bila jarak R ke R dalam kotak besar (5 mm) hitung 300/jarak R-R (150-100-75-60-50)Bila jarak R ke R dalam mm 1500/jarak R-R dlm mm
Bila tidak teratur hitung jumlah kompleks QRS dlm rekaman sepanjang 15 cm (6 detik) kemudian hasilnya dikalikan 10

Penilaian hasil rekaman EKG: Frekuensi (rate) dihitung / menit Irama (rythm): regular / irregular Zona transisi V1-V6 Axis Elektrik: sumbu (derajat), posisi (normal, left, right, indeterminate / right superior / northwest) Interval PR, QRS, dan QT dalam detik Lain-lain

Beats and Rhythms




normal ("sinus") beats
sinus node doesn't fire leading to a period of asystole p-wave has different shape
indicating it did not originate in the sinus node, but somewhere in the atria. It is therefore an "atrial" beat
Atrial Escape Beat








there is no p wave, indicating that it did not originate anywhere in the atria, but since the QRS complex is still thin and normal looking, we can conclude that the beat originated somewhere near the AV junction. The beat is therefore called a "junctional" beat
QRS is slightly different but still narrow, indicating that conduction through the ventricle is relatively normal
Junctional Escape Beat

there is no p wave, indicating that the beat did not originate anywhere in the atria
actually a "retrograde p-wave may sometimes be seen on the right hand side of beats that originate in the ventricles, indicating that depolarization has spread back up through the atria from the ventricles
QRS is wide and much different ("bizzare") looking than the normal beats. This indicates that the beat originated somewhere in the ventricles
Ventricular Escape Beat

Ectopic Beats or Rhythms
• beats or rhythms that originate in places other than the SA node
• the ectopic focus may cause single beats or take over and pace the heart, dictating its entire rhythm
• they may or may not be dangerous depending on how they affect the cardiac output














Penilaian hasil rekaman EKG: Frekuensi (rate) dihitung / menit Irama (rythm): regular / irregular Zona transisi V1-V6 Axis Elektrik: sumbu (derajat), posisi (normal, left, right, indeterminate / right superior / northwest) Interval PR, QRS, dan QT dalam detik Lain-laian


Penilaian hasil rekaman EKG: Frekuensi (rate) dihitung / menit Irama (rythm): regular / irregular Zona transisi V1-V6 Axis Elektrik: sumbu (derajat), posisi (normal, left, right, indeterminate / right superior / northwest) Interval PR, QRS, dan QT dalam detik Lain-lain


Na+
K+ Na+ K+Na+ K+
Na+
K+
Na+
K+
++++ ---- ++++
P o la rizedC e ll
R e po la riz ingC e ll
( )K +
efflux
D e po la rizedC e ll
D e po la riz ingC e ll
( in flu x )Na+
P o la rizedC e ll
“Wave of Depolarization“ or ”P ropigation of Action Potentia l” m oving from left to right
T he need le o f th is reco rd ing e lectrode inscribes a to ta lly
com plex because the w ave o f depola riz tion is m ov ing from it du ring the entire tim e the strip is depoariz ing
nega tive
aw ay
T he need le o f th is reco rd ing e lectrode is because ha lf o f the tim e the w ave o f depo lariza tion is m ov ing it w h ile the o the r ha lf o f the tim e it is m ov ing from it
b iphasic
tow ards
aw ay
T he need le o f th is reco rd ing e lec trode inscribes a to ta lly com p lex because the w ave o f depo lariz tion is m ov ing it during the en tire tim e the strip is depoariz ing
pos itive
tow ards
Depolarization Wave of a Strip of Nerve Cells (or Myocardial Muscle Cells m inus the depiction of Ca influx)
+ +
---- ----++++


The Concept of a "Lead"
+-
G
• Right arm (RA) negative, left arm (LA) positive, right leg (RL) ground……this arrangement of electrodes enables a "directional view" recording of the heart's electrical potentials as they are sequentially activated throughout the entire cardiac cycle
Electrocardiograph
Lead I

The Concept of a "Lead"Lead I
+-
• The directional flow of electricity from Lead I can be viewed as flowing from the RA toward the LA and passing through the heart. Also, it is useful to imagine a camera lens taking an "electrical picture" of the heart with the lead as its line of sight



The Concept of a "Lead"The Limb Leads
0o
LEAD AVR LEAD AVL
LEAD AVF
LEAD II
LEAD I
LEAD III
60o
90o120o
-30o-150o
• Each of the limb leads (I, II, III, AVR, AVL, AVF) can be assigned an angle of clockwise or counterclockwise rotation to describe its position in the frontal plane

The Concept of a "Lead"Leads I II III
+-
• By changing the arrangement of which arms or legs are positive or negative, two other leads ( II & III ) can be created and we have two more "pictures" of the heart's electrical activity from different angles
RA
RA
LL+
+
--LA
LL
LA
LEAD II
LEAD I
LEAD III
Remember, the RLis always the ground




The Concept of a "Lead"Leads AVR AVL AVF
+
-
• By combining certain limb leads into a central terminal, which served as the negative electrode, other leads could be formed to "fill in the gaps" in terms of the angles of directional recording. These leads required augmentation of voltage to be read and are thus labeled.
RA
RA & RL LL & LA
+
+
-
LL
RA & LA
LA
LEAD AVR
-
LEAD AVL
LEAD AVF




The Concept of a "Lead"The Precordial Leads
V1 V2
V4 V5V3
V6
• Each of the precordial leads is unipolar (1 electrode constitutes a lead) and is designed to view the electrical activity of the heart in the horizontal or transverse plane






aVR aVL
aVF

Hexaxial Array for Axis Determination
determination of the angle of the main cardiac vector in the frontal plain

If lead I is mostly positive, theaxis must lie in the right half ofof the coordinate system
Lead I Example 1

If lead AVF is mostly positive, theaxis must lie in the bottom half ofof the coordinate system
Lead AVF

Combining the two plots, we seethat the axis must lie in the bottomright hand quadrant
I AVF

Once the quadrant has been determined, find the most equiphasic or smallest limb lead. The axis will lie about 90o away from this lead. Given that AVL is the most equiphasic lead, the axis here is at approximately 60o.
I AVF AVL

Since QRS complex in AVL is a slightly more positive, the true axis will lie a little closer to AVL (the depolarization vector is moving a little more towards AVL than away from it). A better estimate would be about 50o.
I AVF AVL

If lead I is mostly negative, theaxis must lie in the left half ofof the coordinate systemLead I
Example 2

If lead AVF is mostly positive, theaxis must lie in the bottom half ofof the coordinate system
Lead AVF

Combining the two plots, we seethat the axis must lie in the bottomleft hand quadrant (Right Axis Deviation)
I AVF

Once the quadrant has been determined, find the most equiphasic or smallest limb lead. The axis will lie about 90o away from this lead. Given that II is the most equiphasic lead, the axis here is at approximately 150o.
I AVF II

I AVF IISince the QRS in II is a slightly more negative, the true axis will lie a little farther away from lead II than just 90o (the depolarization vector is moving a little more away from lead II than toward it). A better estimate would be 160o.

Precise calculation of the axis can be done using the coordinate system to plot net voltages of perpendicular leads, drawing a resultant rectangle, then connecting the origin of the coordinate system with the opposite corner of the rectangle. A protractor can then be used to measure the deflection from 0. Consider the example:
Since Lead III is the most equiphasic lead and it is slightly more positive than negative, this axis could be estimated at about 40o.



Penilaian hasil rekaman EKG: Frekuensi (rate) dihitung / menit Irama (rythm): regular / irregular Zona transisi V1-V6 Axis Elektrik: sumbu (derajat), posisi (normal, left, right, indeterminate / right superior / northwest) Interval PR, QRS, dan QT dalam detik Lain-lain




Penilaian hasil rekaman EKG: Frekuensi (rate) dihitung / menit Irama (rythm): regular / irregular Zona transisi V1-V6 Axis Elektrik: sumbu (derajat), posisi (normal, left, right, indeterminate / right superior / northwest) Interval PR, QRS, dan QT dalam detik Lain-lain









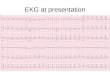
ECG diagnosis