Embed Size (px)
Citation preview

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 1/66
Emergency Medicine
Emergency Medicine
MELANOTIC LESIONS OF
HEAD AND NECK REGION
PRESENTED BY:
ASHISH VYAS
PGT,ORAL AND MAXILLOFACIAL SURGERY
RDC,GUWAHATI
GUIDED BY:DR A.K.ADHYAPOK
PRINCIPAL AND H.O.D
DEPARTMENT OF ORAL AND MAXILLOFACIAL
SURGERY
RDC,GUWAHATI

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 2/66
INTRODUCTION
Human oral and head and neck mucosa is not
uniformly coloured and several degrees of chromatic
variegation may be observed in physiological and
pathological conditions.
Melanin-associated lesions represent the most
common pigmentations and include benign entities
as well as mucosal melanoma, an extremelyaggressive neoplasm.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 3/66
ORAL MUCOSAL MELANOCYTES• Melanocytes are dendritic cells located
mainly in the basal layer of the
epidermis and in some mucousmembranes.
• They are widely distributed and presentin large numbers in the oral mucosa.
• They are regularly interspersed betweenthe basal keratinocytes.
• Melanocytic dendrites reach a numberof keratinocytes in the close vicinity,and through these dendrites, melanin istransported and transmitted to theseepithelial cells.
• The main biochemical function of themature melanocyte is a process calledmelanogenesis through which the cellproduces and delivers melanin pigment.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 4/66

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 5/66
Emergency Medicine
Emergency Medicine
• Melanotic
macules
of the oral cavity are relatively
common lesions, caused by an increased production
and deposition of melanin within the basal cell layer,
the lamina
propria
, or both.
• Melanotic
macules
are usually single, well
-circumscribed blue or brown
-
to
-
black lesions
homogeneously colored, and less than 1 cm in
diameter.
• These
melanotic
macules
are idiopathic and may be
conceptualized as the rare mucosal corollary to the
much more common skin freckle (
ephelis
), althoughthe
melanotic
macule
does not darken in response
to sun exposure as does the skin freckle.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 6/66
Emergency Medicine
Emergency Medicine
• They are most
commonly seen on
the lower lip
vermilion or on the
attached
gingiva
,
but they can occur
on any oral site.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 7/66
Emergency Medicine Emergency Medicine
DIFFERENTIAL DIAGNOSIS
• The most important lesion todistinguish from a melanotic
macule is an early melanoma.
• Although most oral melanomas
will be black or blue and willmore characteristically have
varying shades of brown to black
within them, early melanomas
may appear as homogeneous as
melanotic macules.
• The most common lesion that
may appear similar to a
melanotic macule is an amalgam
tattoo.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 8/66
Emergency Medicine Emergency Medicine
TREATMENT
• Single lesions should undergo excisional biopsy torule out melanoma.
• The early identification of a small melanoma woulddramatically improve the prognosis in a case with an
otherwise poor prognosis.• When multiple lesions are present, it is often prudent
to biopsy one or two lesions.
• Choose the largest, darkest, most raised (if any are
raised), and most irregularly bordered ones toundergo biopsy.
• If the biopsy confirms more than one melanoticmacule, a screening work‐up for Peutz ‐ Jeghers
syndrome and Addison disease is required.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 9/66
Emergency Medicine Emergency Medicine
SMOKER‟S MELANOSIS
• Smokers' melanosis is a focal increase inmelanin pigmentation in the oral mucosa found
in cigarette, pipe, and cigar smokers who
smoke frequently.
• The melanosis is either a diffuse patch of
brownish discolored mucosa or numbers of small melanotic macules.
• The lesion is not dysplastic or premalignant,
but its presence indicates a continual and
frequent smoking habit that places the patient
at an increased risk for oral carcinoma.
• Most lesions are seen on the labial mucosa
and floor of the mouth, but the tongue, gingiva,
and buccal mucosa may also be involved.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 10/66
Emergency Medicine Emergency Medicine
TREATMENT
• Only lesions suggestive of melanomaby virtue of induration, thickening,ulceration, or darkening in color requirebiopsy.
• Because these lesions are notthemselves dangerous, no specifictreatment is required.
• However, smoking reduction or cessation is strongly advised, which, inturn, will often result in a lightening of the pigmentation and in some caseselimination of it.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 11/66
Emergency Medicine Emergency Medicine

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 12/66
Emergency Medicine Emergency Medicine
MELANOYTIC NEVI
• Nevi, also called moles, are benign collections of nevus cells that are derived either from melanocytesor from the same neural crest precursors asmelanocytes.
• Nevi on skin are very common; nearly every person
has at least one.• Nevi on the oral mucosa are very uncommon, withless than 1% of individuals possessing a truemucosal nevus.
• About 1% of newborns have a nevus.
• The number of individuals with nevi increases andthe number of nevi on each individual increases to apeak at puberty.
• Although nevi can occur on any skin surface, greater numbers appear on sun‐exposed surfaces.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 13/66
Emergency Medicine Emergency Medicine
MELANOCYTIC NEVI
• Melanocytic naevi constitute benign neoplasms of • cutaneous melanocytes, which frequently harbour oncogenic BRAF or, less commonly, NRAS or HRAS mutations .
• Probably, oncogenic mutations drive the initial
hyperproliferation that results in the formation of thenaevus, while a subsequent growth-arrest responsewith the features of oncogene-induced cellular senescence accounts for the cessation of further growth .
• Different from normal melanocytes which areregularly interspersed as single cells among basalkeratinocytes, forming the so-called “epidermal-melanin unit”, nevomelanocytes tend to cluster incompact so-called theques

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 14/66
Emergency Medicine Emergency Medicine
TYPES OF NEVI
JUNCTIONAL COMPOUND DERMAL

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 15/66
Emergency Medicine Emergency Medicine
JUNCTIONAL NEVUS
• Junctional nevi are flat or onlyslightly elevated.
• Nevus cells (nests) at the DEJ.
• Most are hairless and small,varying in size from 1 to 10 mm .
• They are only rarely seen as acongenital nevus.
• Most arise at about age 2 yearsand evolve into compound nevi inthe teen years.
• Junctional nevi on the palms,soles, and genital areas remain junctional and never seem toconvert to a compound nevus.
• Transformation into a melanoma
is very rare.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 16/66
Emergency Medicine Emergency Medicine
COMPOUND NEVUS
•Compound nevi tend to beelevated with a uniformlyround or oval shape.
• Many are natural skin color,others are somewhat darker.
•Light brown, dome-shapedpapule
• Nevus cells at the DEJ anddermis
• Hair is often present arising
around a compound nevus.• With increasing age, nevibecome more elevated andmay develop a wartyappearance.
• Melanoma transformation isalso rare.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 17/66
Emergency Medicine Emergency Medicine
DERMAL NEVUS
• Nests of nevus cells in the dermiswith no component at the DEJ.
• Dermal nevi may also be of naturalskin color or darker.
• All are elevated nodules and become
firm as fibrous tissue replacesdegenerated nevus cells.
• Most are described as domeshaped, but others may be warty.
• The warty surface is regular and
symmetric throughout the lesion.• Some dermal nevi will also develop a
stalk and produce a pedunculatedlesion resembling a skin tag,particularly in the groin, axilla, and
neck.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 18/66
Emergency Medicine Emergency Medicine
TREATMENT
• Any skin nevus with signs suggestive of a melanoma requires excision down toand including the subcutaneous level.
• All mucosal nevi require excision downto and including the submucosal level.
• Excision of such nevi eradicates thelesion and may lead to diagnosis of an
early melanoma.• Static nevi without features suggestive
of a melanoma do not require excision
and may be followed.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 19/66
Emergency Medicine Emergency Medicine
BLUE NEVUS
• The blue nevus, a blue dermal nevus, isusually small (less than 5 mm) and appearsas a regular, round elevated nodule. Itappears blue because the melanin pigment,which is naturally brown, is located deepwithin the dermis.
• The brown pigment and the thickness of
skin absorb the longer wavelengths of light(eg, reds, oranges, yellows) and reflect themore penetrating, shorter wavelengths, suchas blue (ie, the Tyndall effect).
• The blue nevus will appear in childhood onthe dorsum of hands, extremities, and scalp.
• It has a low potential for malignanttransformation.
• However, a larger, rare variant, called thecellular blue nevus, has a higher melanomatransformation rate. It is frequently larger than 1 cm and most often located on the
buttocks.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 20/66
Emergency Medicine Emergency Medicine
HALO NEVUS
• AKA Sutton‟s nevus, perinevoidvitilgo, & leukodermaacquisitum centrifugum
• A pigmented nevus withsurrounding depigmented zone
• Nevus is usually compound or
intradermal• May be single or multiple• Usually on the trunk• Mostly develop in teenagers
• The nevus architecture is
obscured by a denselymphocytic infiltrate
• Lymphocytes infiltrate amongthe dermal nevus cells, whicheventually degenerate and
disappear.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 21/66
Emergency Medicine Emergency Medicine
SPITZ NEVUS
•A variant of the compound nevus.
• A smooth-surfaced, raised, round,slightly scaly, firm papule withdistinctive pink, brownish red, or purplish red color.
• Typically, firm,rosy papule on the
face, especially on the cheek.• 3 – 10 mm in diameter.• Female predominance.• Epidermal irregular acanthosis,
pseudoepitheliomatous
hyperplasia, and thinning of theepidermis• Nevus cells are pleomorphic, but
mostly spindle-shaped (fusiform),or polygonal (epithelioid) cells

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 22/66
Emergency Medicine Emergency Medicine
SPITZ NEVUS
• The Spitz nevus has clinical and histologicfeatures mimicking those of a melanoma.
• The nevi present as red or reddish‐brown,smooth‐surfaced nodules, usually between 0.5and 1.5 cm.
• Clinically, Spitz nevi may suggest a melanomabecause they emerge suddenly, unlike other nevi that develop slowly as macular lesionsand evolve into nodular dermal nevi.
• They may also be suggestive of a melanomabecause of their vascular nature, which maylead to bleeding following minor trauma.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 23/66
Emergency Medicine Emergency Medicine
TREATMENT
•Spitz nevi usually require excision to rule outmelanoma and other diseases on the differential list.
• Excision is accomplished with 1‐ to 2‐mm marginsand includes the entire subcutaneous level.
• If the pathologist identifies the lesion as a Spitz
nevus, no further excision or treatment is required.• The Spitz nevus does not recur, not even in thecase of incomplete excision.
• Therefore, in equivocal cases in which thehistopathologic distinction between melanoma and a
Spitz nevus is uncertain, follow‐up is recommended. Any evidence of clinical recurrence is interpreted as
evidence of melanoma.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 24/66
Emergency Medicine Emergency Medicine
NEVUS OF OTA
• The nevus of Ota is a unique nevus that
represents a melanocytic disorder following the distribution of one or moredivisions of the trigeminal nerve .
• About 48% are congenital or appear within a few weeks of birth, and 36% ariseat puberty, thereby creating a bimodal
incidence peak.• The nevus will appear as a diffuse
brownish discoloration or a cluster of small, blue‐black, well‐demarcated spots.
• The skin over the maxillary division of thetrigeminal nerve seems to be involved
more frequently than the other divisions,and corresponding nevi simultaneouslyappear on the oral mucosa, nasalmucosa, and sometimes on theconjunctiva of the ipsilateral eye.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 25/66
Emergency Medicine Emergency Medicine
NEVUS OF OTA
• Neither the cutaneous component nor theoral mucosa membrane component of thenevus of Ota is associated withmelanoma.
• The nevus of Ota is thought to representa developmental anomaly of excessmelanocytes residual from neural crestcells that migrated along a trigeminalnerve distribution.
• In those arising during puberty, it may bea hamartomatous proliferation of theseresidual cells stimulated by hormonalincreases.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 26/66
Emergency Medicine Emergency Medicine
TREATMENT
• The nevus of Ota is merely a matter of cosmetic concern; rarely does it undergotransformation to melanoma, nor does thenevus usually progress throughout life.
• However, patients with ocular involvement
have a high incidence of secondaryopen‐angle glaucoma due to melanocytescollecting at the angle, causing obstruction of drainage.
• They also have a higher incidence of retinal,iridic, and cerebral melanomas.
• Therefore, patients with cutaneous lesionssuggestive of nevus of Ota should undergo anophthalmologic evaluation.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 27/66
Emergency Medicine Emergency Medicine
NEVUS OF ITO
• The nevus of Ito is similar to the nevus of
Ota; however, it mostly occurs in thedeltoid region.
• It may be seen on the upper chest, back,or supraclavicular area as well.
• Like the nevus of Ota, this nevus formsalong peripheral nerve fibers.
• Clinically, it will present as a bluishhyperpigmentation, which on fine sensorytesting may be associated with a localparesthesia.
• On occasion, the nevus has beenassociated with reduced sweating
presumably because of its associationwith small sympathetic fibers, whichinnervate facial sweat glands.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 28/66
Emergency Medicine Emergency Medicine
DYSPLASTIC NEVUS
• The dysplastic nevus is a clinicallyand histologically atypical nevusrepresenting the single mostimportant precursor to a cutaneousmelanoma.
• More than the congenital nevus, itis the primary pigmented lesion thattransforms into a melanoma.
• Dysplastic nevi appear either
sporadically or in aautosomal‐dominant inheritedcondition called dysplastic nevussyndrome (DNS).

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 29/66
Emergency Medicine Emergency Medicine
DYSPLASTIC NEVUS
• Clinically, the dysplastic nevus differs from theordinary nevus. It is usually larger, and manyare greater than 1 cm, whereas the commonnevus rarely exceeds 0.6 cm.
• Its borders are irregular, with the color fading
gradually into the surrounding skin, in contrastto the well‐demarcated and regular borders of the ordinary nevus .
• It is variegated in color, usually a mixture of
brown, black, and red, whereas common neviare uniform in color .
• Common nevi have a site preference for sun‐exposed areas, while dysplastic nevi tendto occur at unusual sites such as the scalp,
buttocks, and breast.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 30/66
Emergency Medicine Emergency Medicine
DYSPLASTIC NEVUS
• Dysplastic nevi associated with dysplasticnevus syndrome have an exceedingly highmelanoma potential.
• Dysplastic nevi are found concomitantly on theskin of 90% of melanoma patients who have a
family history of melanoma.• Dysplastic nevi of either the sporadic type or
the familial DNS are not congenital but appear in midchildhood as a common mole.
• They begin to take on the clinical features of dysplastic nevi in the early teens, and newnevi continue to appear even past the age of 40 years.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 31/66
Emergency Medicine Emergency Medicine
TREATMENT
• The general approach is to excise two to four of themost suspicious nevi to establish a histopathologicdiagnosis.
• The excision uses 2‐ to 5‐mm margins to andinclusive of the subcutaneous level.
• If the diagnosis confirms dysplastic nevi, thegeneral rule is to excise all new nevi that arisethereafter and all of those in the scalp because of the difficulty of monitoring scalp lesions.
• Prophylactic excision of all remaining nevi is neither
practical nor indicated if there are more than 10.• Such lesions should be followed with serialexaminations and compared to baselinephotographs.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 32/66
Emergency Medicine Emergency Medicine

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 33/66
Emergency Medicine Emergency Medicine
MNTI
• Melanotic neuroectodermal tumor of infancy (MNTI) is arelatively uncommon osteolytic-pigmented neoplasm thatprimarily affects the jaws of newborn infants.
• The MNTI, which originates from neural crest cells,represents an overgrowth of these cells rather than their usual involution.
• Normally, neural crest cells originate from a mantlearound the developing spinal cord and project out to theperiphery along sympathetic nerves.
• In other parts of the body, they populate the primordia of sympathetic ganglia and the adrenal medulla to become
neurosecretory cells of these respective structures.• In the maxilla and most peripheral sympathetic neuralpathways, they involute.
• Those that develop into the MNTI are the rare failures of involution, which instead proliferate into a tumor.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 34/66
Emergency Medicine Emergency Medicine
MNTI
• Although melanotic neuroectodermal tumor
of infancy (MNTI) is classified as a benignlesion, it is often clinically worrisomebecause of its rapid onset and alarming localgrowth rate.
• Often, sucking and feeding are impairedsecondary to the swelling.
• The patient is usually asymptomatic.• The typical melanotic
neuroectodermal tumor of infancy(MNTI) begins as a nonulcerated,lightly pigmented, blue or black
lesion on the anterior aspect of themaxilla and rapidly expands to forma swelling or a tumescence that iscosmetically obvious to the parentsof the infant.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 35/66
Emergency Medicine Emergency Medicine
MNTI
• The intraoral lesion appears as a sessile,lobulated mass, often reaching 2-4 cm indiameter by the time of diagnosis.
• Bone destruction and displacement of teethoften occur because of the intraosseous
location in the maxilla.• No thrill or pulse can be elicited from the
MNTI.
• Although the lesion expands rapidly, the
overlying mucosa remains intact.• More than 90% of MNTI occur in the head and
neck region, with most on the anterior part of the maxillary ridge. Other common sitesinclude the skull, the mandible, the epididymis,and the brain.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 36/66
Emergency Medicine Emergency Medicine
DIAGNOSTIC WORK UP
• The most important diagnostic step is aconfirmatory incisional biopsy.
• However, an occlusal radiograph that showsthe central incisor displaced to the peripheryof a mass that itself shows destruction of the
anterior maxilla is pathognomonic.• About 10% to 15% of MNTI will elaborate
vanillylmandelic acid (VMA or 3‐methoxy‐4‐hydroxy mandelic acid), which is
a soluble metabolic breakdown product of norepinephrine.
• It is indicative of the neuroectodermal cellorigin of this tumor.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 37/66
Emergency Medicine Emergency Medicine
TREATMENT
• The MNTI should be treated by a peripheral
• excision with 2‐ to 5‐mm margins .
• Although the destructive nature of this tumor and itsgrowth rate are significant, total maxillectomies andmaxillary resections with margins greater than 5 mm
are unnecessary.• Early excision is of great value. Limiting thedestruction that the tumor causes in the anterior maxilla will lessen the deformity and preservedeveloping teeth.
• The excision should include the overlying mucosa.The resultant wound may be packed with a tie‐over pressure dressing for 5 to 7 days to reduce oozing.
• The wound itself heals rapidly by granulation tissueand secondary epithelialization.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 38/66
Emergency Medicine Emergency Medicine

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 39/66
Emergency Medicine Emergency Medicine
MELANOMA
• Melanoma is a potentially deadlyand aggressive neoplasm resulting
from the malignant transformation of
melanocytes.• The incidence of melanoma is
increasing faster than any other
cancer.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 40/66
Emergency Medicine Emergency Medicine
• Treatment of melanoma of head and neck is a

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 41/66
Emergency Medicine Emergency Medicine
Treatment of melanoma of head and neck is a
complex issue.
• The behaviour of this malignancy is aggressive, and it
has overall worst prognosis than that of other skinsites.
• Histological involvement ofregional lymph nodes by
metastases of malignant melanoma in the head and
neck region is very poor prognostic sign.
• Accurate localization of pathologically involved
cervical lymph nodes is crucial in the treatment of
these patients.
LYMPHATIC REGIONS OF

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 42/66
Emergency Medicine Emergency Medicine
LYMPHATIC REGIONS OF
NECK
• Lymphatic tissue in the neck accounts for one-third of all nodal tissue in the entire body.
• Most cervical lymph nodes are located in the
anterior triangle traversing the carotid sheath
from the skull base to the thoracic inlet.
• Most head and neck surgeons, radiologists,
and oncologists refer to „„nodal levels‟‟ to
describe nodal groups involved by diseaseand encompassed by neck dissections.
• The six cervical lymph node levels are as
follows:

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 43/66
Emergency Medicine Emergency Medicine
CLASSIFICATION OF NECK

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 44/66
Emergency Medicine Emergency Medicine
CLASSIFICATION OF NECK
DISSECTIONS
MODIFICATIONS IN NEW

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 45/66
Emergency Medicine Emergency Medicine
MODIFICATIONS IN NEW
CLASSIFICATION
•The three most significant changes in therevised classification were
• (i) the way in which various SNDs aredescribed,
• (ii) the use of radiologically depicted anatomic
structures to define boundaries betweenvarious neck levels and sublevels toaccurately designate imaged nodes, and
• (iii) the introduction of sublevels into the
classification system, since certain zoneshave been identified within the six levels thatmay have biologic significance independent of the large zone in which they lie.
• These three modifications comprise

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 46/66
Emergency Medicine Emergency Medicine
These three modifications comprise
• sublevel IA (submental nodes) and IB(submandibular nodes),
• sublevel IIA and IIB (together comprisingthe upper jugular nodes), and
• sublevel VA (spinal accessory nervenodes) and VB (transverse cervical andsupraclavicular nodes).
• Each variant is depicted by SND and theuse of parentheses to denote the level or sublevel of nodes removed, e.g., SND (I –III).

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 47/66
Emergency Medicine Emergency Medicine
RADICAL NECK DISSECTION
• consists of the removal of all fivelymph node levels of one side of the
neck (levels I –V) and removal of the
sternocleidomastoid muscle, theinternal jugular vein, and the spinal
accessory nerve.
MODIFIED RADICAL NECK

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 48/66
Emergency Medicine Emergency Medicine
MODIFIED RADICAL NECK
DISSECTION
• Modified radical neck dissectioninvolves the excision of all lymphnodes routinely removed during
radical neck dissection but withpreservation of one or more of thenonlymphatic structures (e.g., spinalaccessory nerve, internal jugular
vein, sternocleidomastoid muscle)routinely removed during a radicalneck dissection.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 49/66
Emergency Medicine Emergency Medicine
SELECTIVE NECK DISSECTION
• SND is any type of cervical lymphadenectomyin which one or more of the lymph node
groups that are routinely removed in a radical
neck dissection are preserved.
• Determining which lymph node groups toremove is based on the pattern of metastases,
which is predictable relative to the location of
the primary site of the neoplasm.
• Each variant is depicted by „„SND‟‟ as well as
parentheses to denote the levels or sublevels
of removed nodes, e.g., SND (I –III), SND (II –
IV), or SND (VI).
EXTENDED RADICAL NECK

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 50/66
Emergency Medicine Emergency Medicine
EXTENDED RADICAL NECK
DISSECTION
• Extended radical neck dissectionincludes either lymph node groups
or nonlymphatic structures that are
not routinely removed in standardradical neck dissection.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 51/66
Emergency Medicine Emergency Medicine

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 52/66
Emergency Medicine Emergency Medicine
ELECTIVE NECK DISSECTION
•Tumor thickness is the most important factor in
determining whether or not to perform END.
• All patients with histologically confirmed melanoma
thicker than 0.7mm with Clark level of 4 are
candidates for END.
EXTENT OF PAROTID GLAND SURGERY
Patients with thick melanomas (>4mm) are likely to
undergo total parotidectomy.
ANATOMICAL SITES

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 53/66
Emergency Medicine Emergency Medicine
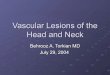
ANATOMICAL SITES
•The skin of head and neck can
be divided into 6 anatomical
sites as management of
melanoma is site specific.
1. Forehead, Upper Face &
Lower Face
2. Coronal Preauricular Scalp
3. Posterior Scalp
4. Upper Neck5. Inferior Anterior Neck
6. Upper & Lower Posterior neck

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 54/66

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 55/66

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 56/66
SLNB has certain limitations in management of head & neck
melanomas:
Increased incidence of nodal recurrence in SLN negative
patients.
Possibility of false negative results.
Difficult identification of SLN if they are located close to the
primary site
SLN found in multiple node fields in contrast to melanomas
located on extremities which usually drain to only one field.
SLN in parotid region, which are often very small may be
difficult to find and their removal may put the facial nerve at
risk.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 57/66

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 58/66
INTRODUCTION
Primary oral malignant melanoma (OMM)is a rare neoplasm, accounting for 0.5% ofall oral malignancies.
The most frequently affected oral sites arethe palate and the maxillary gingiva.
CLINICAL FEATURES

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 59/66
Emergency Medicine Emergency Medicine
CLINICAL FEATURES
• According to Tanaka et al, oral melanomas could beclassified into five types, based on their clinicalappearance: pigmented nodular, nonpigmented nodular, pigmented macular, pigmented mixed and nonpigmented mixed
• The clinical coloration of oral melanomas has a widerange, which can appear as black, gray, purple, andeven reddish.
• While some lesions are uniform in color, others exhibitmarked variations.
• The tumors are asymmetric, irregular in outline, andoccasionally multiple.
• Their surface architecture ranges from macular toulcerated and nodular.
• Pain is present in advance cases.
HISTOLOGIC FEATURES

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 60/66
Emergency Medicine Emergency Medicine
HISTOLOGIC FEATURES
• The 1995 WESTOP (Western Society of Teachers of Oral
Pathology) Banff Workshop on OMM drew attention to the
fact that most OMMs are discovered and biopsied in an
advanced stage, which probably contributes to the
heterogeneity of microscopic patterns.
• Like cutaneous melanoma, OMM probably has in manycases an initial phase characterized by radial growth
followed by a phase of invasion of the underlying tissues
(the so-called „vertical growth phase‟).
• OMMs can be histologically subclassified into:
(1) in situ melanoma
(2) melanomas with an invasive pattern.
(3) melanomas with a combined pattern of invasive melanoma
with in situ componen.t

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 61/66
Emergency Medicine Emergency Medicine
• OMM does not fit well into any of the classicalcutaneous melanoma categories like
superficial spreading melanoma (SSM),
nodular melanoma (NM) and acral lentiginous
melanoma (ALM).• There is, however, often some similarity to
ALMand NM.
DIAGNOSIS

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 62/66
Emergency Medicine Emergency Medicine
DIAGNOSIS
• The so called ABCDE checklist that is commonly used
in the identification process of cutaneous melanoma
could also be of some help in the diagnosis of oral
melanoma .
• When an oral pigmentation cannot be confidently
diagnosed as benign on clinical grounds, a biopsy ismandatory in order to exclude OMM.
• Sentinel-node biopsy or lymphoscintigraphy, which is
beneficial in staging of cutaneous melanoma, has less
value in staging or treating oral melanoma. Complexand ambiguous drainage patterns may result in the
bypass of some first-order nodes and in the
occurrence of metastasis in contralateral nodes.
STAGING SYSTEM

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 63/66
Emergency Medicine Emergency Medicine
STAGING SYSTEM
• The histological microstaging system of Clark, used in
cutaneous melanoma, cannot be applied to oral
mucosa because of the lack of histologic landmarks
analogous to papillary and reticular dermis.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 64/66
Emergency Medicine Emergency Medicine
• The American Joint Committee onCancer (AJCC) does not have
published guidelines for the staging
of oral malignant melanomas.
MANAGEMENT

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 65/66
Emergency Medicine Emergency Medicine
MANAGEMENT
• Ablative surgery with tumor -free margins remains the
treatment of choice. Early surgical intervention when
local recurrence is detected enhances survival,
because the dismal outcomes are associated with
distant metastasis.
• Prophylactic neck dissection (ie, elective neckdissection) is not advocated as a treatment for oral
melanoma.

7/31/2019 Melanotic Lesions of Head and Neck Region
http://slidepdf.com/reader/full/melanotic-lesions-of-head-and-neck-region 66/66