Embed Size (px)
Citation preview

Mel MattsonSTI/HIV/VH Branch Chief
Colorado Department of Public Health and Environment


S Objective 1: Promote access and adherence to prophylactic treatment, prioritizing those who are at greatest risk of becoming infected and facing economic or psychosocial barriers. Include both pre-exposure and post-exposure prophylaxis.
Objective 2: Promote access to clean injection equipment and treatment for substance use disorders, prioritizing those who are at greatest risk of becoming infected and facing economic or psychosocial barriers.
Objective 3: Promote access to vaccination, prioritizing those who are at greatest risk of becoming infected and facing economic or psychosocial barriers.
Objective 4: Promote access to expedited partner therapy, to intervene in disease transmission.
Objective 5: Maintain a surveillance system that identifies health care related infections and exposures, and respond to such incidents in coordination with other CDPHE programs.
Objective 6: Establish and monitor metrics that measure the effectiveness of efforts to prevent uninfected persons from becoming infected with HIV, STI, or viral hepatitis.
Objective 7: Build capacity of staff, contractors, and clinical providers to deliver evidence based biomedical interventions to prevent persons from acquiring STI/HIV/VH. (Tactics will include data, skills training, communication, and leadership development).
Objective 1: The STI/HIV/VH Branch will define and implement a protocol to link all persons reported for HIV, STI, or viral hepatitis to a medical home, prioritizing those who pose the greatest risk of transmitting HIV, STI, or viral hepatitis to their partners.
Objective 2: The STI/HIV/VH Branch will define and promote a supportive continuity of care pathway for people living with HIV, STI, viral hepatitis and comorbidities, prioritizing those who pose the greatest risk of transmitting their infection to their partners.
Objective 3: The STI/HIV/VH Branch will identify five key opportunities to improve evidence-based practices and health insurance coverage and will demonstrate success in achieving such improvements within <<NUMBER>> months .
Objective 4: The STI/HIV/VH Branch will establish and monitor metrics that measure the effectiveness of efforts to link people to a medical home, promote continuity of care, and increase availability of evidence-based practices and sufficient health insurance coverage for HIV, STI, viral hepatitis, and comorbidities, including:• Rates of reinfection • Number of persons named as partners of STI/HIV/VH • Number of persons at high risks who have insurance coverage who are not screened
for STI/HIV/VH by their health care providers
Objective 5: Build capacity of staff, contractors, and clinical providers to deliver comprehensive, evidence-based services to persons infected with STI/HIV/VH. (Tactics will include data, skills training, communication, and leadership development).
Objective 1: Advance evidence-based testing for HIV/STI/VH delivered by health care providers, tailored for client risk factors.
Objective 2: Deliver evidence-based testing for HIV/STI/VH, prioritizing those at highest risk of undiagnosed disease, tailored for client risk factors.
Objective 3: Assure comprehensive screening that includes issues that are highly associated with adherence and transmission, including substance use, mental illness, PrEP indicators, and destabilizing life situations.
Objective 4: Establish and monitor metrics that measure the effectiveness of testing and screening efforts.
Objective 5: Build capacity of staff, contractors, and clinical providers to deliver comprehensive, evidence-based testing and screening. (Tactics will include data, skills training, communication, and leadership development).
The integration of data systems is vital to the successful implementation of work plans throughout the branch .
Assure and continually improve the quality of services we deliver or fund.Make investments only when they are having a demonstrated impact on the epidemics
Strengthen internal and external communication
Leadership and staff development is vital for sustainable, highly functioning program implementationLeverage existing infrastructure when possible
Prioritize persons most likely to transmit an infection
Strategy 1: Interventions to prevent uninfected persons
from becoming infected
Strategy 3: Services for people who are infected
Strategy 2: Comprehensive Testing and Screening
Foundational Statements:
STI/HIV/VH Branch Strategic Map 2015 - 2020

Who remembers just a few years ago…..
Share my HIV data?
You have to be kidding me!

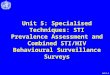
100% of PLWH
80% of PLWH
73% of PLWH
65% of PLWH
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
People who have lived with
diagnosed HIV infection for at least
12 months in Colorado with
laboratory evidence of medical
care in the last 5 years*
At least one care visit past year Engaged in care or virologically
suppressed past year**
Virologic suppression***
HIV Care Continuum as of December 31, 2013, Colorado
7,689
4,968
5,6106,188
Of those individuals, # who are
virologicallysuppressed.
Of those individuals, # who have had at least one care visit in the past year.
Of those individuals, # who have engaged
in care OR virologically
suppressed in the past year.
People who have lived with Diagnosed HIV
infection in Colorado for at least 12 months
with laboratory evidence of medical
care in the last 5 years*
100% of PLWH
80% of PLWH65% of PLWH73% of PLWH
HIV Care Continuum as of December 31, 2013

◦ It is so much more than responding to the Care Continuum
◦ Creating “not in care” lists – developing procedures to respond
◦ Partnering with healthcare providers and other HIV stakeholders – data sharing, expedited treatment, linkage to other services
◦ Rapidly identifying persons most at risk for acquiring an infection
◦ Determining most current address
◦ Must integrate all of our data systems across STI/HIV/VH

Opportunity to communicate benefits of a Data to Care program to the community
Allows for important issues related to privacy and confidentiality to be openly discussed and addressed
Many topical areas to discuss including program purpose, proposed program activities, security and confidentiality of data

If we are not using our data…why are we collecting it?
If you are not integrating STI/HIV/HCV data –you are missing key opportunities to ID persons most at risk to ……(fill in the blank).


SBIRT- Substance Abuse Screening
ILI delivery
Health insurance navigation
Linking to medical home
PrEP referrals
Rectal/pharyngeal GC/CT testing

DIS routinely interact with high-risk individuals who are often ideal candidates for PrEP:
◦ STI diagnosis◦ Contact to newly dx HIV positive◦ Needle-sharing partners ◦ Other high-risk activities (substance abuse, mental
health, transactional sex)
• DIS are in a unique position to identify these individuals at a pivotal moment: when clients are most at risk for HIV infection but have not yet acquired the virus.
• DIS offer full STI and HIV screening to all clients: including urethral and extragential GC/CT testing (pharyngeal/rectal) and syphilis.

Internal Operational PrEP Workgroup convened monthly during development stages to determine next steps and feasibility
One of our more senior staff DIS indentified as the Biomedical Intervention Program Coordinator
Drafted implementation plans, counseling tools, referral forms and created a known PrEP prescriber inventory.
Convened a broad based community PrEP Workgroup to begin providing community input and recommendations for moving forward.
CDPHE worked with community stakeholders to enact SB 247, which could bring an estimated $1 million to support biomedical interventions, including covering the costs of PrEP for the uninsured or underinsured.


Strong OIT support allows for the customization of PRISM to fit business and programmatic need.
Field Record “960” – PrEP Initiation Referral
This field record tracks DIS and PrEP Coordinator initial screening and referral activities◦ PrEP Screening◦ PrEP Counseling◦ Financial Screening & Healthcare Access Troubleshooting◦ Provider Referral and Placement◦ Final Outcome/Disposition

550 PRISM FR Workflow Algorithm
HIV(+) Client
Client Financially Able to Receive PrEP Clinical Services & Medication
PrEP Initiation
960 PRISM Referral FR
Created
Field DIS
Workflow Algorithm & 960 PRISM Field Record Outcomes HIV Pre-Exposure Prophylaxis (PrEP) Initiation Referral
Healthcare Access 550 PRISM FR Created
Disposition AC
Administratively Closed
Client Enrolled in Payer Source
CO Medicaid, Medicare, ACA Insurance or Other
960 PRISM Referral FR Assigned
to PrEPCoordinator
(or retained by Advanced Field
DIS)
Disposition MC
Medication Contraindicated
Disposition FU
Unable to Afford Medication
Disposition H
Unable to Locate
Disposition DM
Attended Intake & Declined Medication
Disposition J
Located, Did Not Respond
Disposition OM
Already on Medication, No Referral Provided
Disposition SC
Seroconverted, Referral Terminated
Disposition PR
Located, Passive Referral Provided
960 PRISM FR Worked
PrEPCoordinator
(or Advanced Field DIS)
Healthcare Access 550 PRISM FR Worked
PrEP Coordinator
(or Advanced Field DIS)
Initial PrEPCounseling Provided &
Client Accepted Referral
Field DIS
Client Evaluated for PrEP
Indicators & Motivation
Field DIS
Client Evaluated for Acute
HIV Infection
Field DIS
HIV(-) Client
Reinforce Other High Impact HIV Risk Reduction Strategies
Client Not Indicated or
Motivated for PrEP Referral
Initial PrEPCounseling Provided &
Client Declined Referral
Field DIS
Client NOT Financially Able to Receive PrEPClinical Services &
Medication
Un-Insured or Underinsured
Client Screened for Drug Assistance Program (DAP)
PrEP Coordinator
(or Advanced Field DIS)
Disposition SM
Attended Intake & Started Taking Medication
Client Enrolled in DAP
Client Not Enrolled in DAP
Screening Counseling Referral Healthcare Access & Provider
Placement Outcome
Disposition K
Moved Out of Jurisdiction


Personal and public health benefit when PLWH/A are engaged in care, taking their medications, and
achieving viral suppression.
• The clients least likely to achieve viral suppression have multiple issues going on in their lives
• Some of these clients could stabilize if they had sufficient resources delivered during a short period with a high degree of “motivational support”
• There is funding available due to ACA and Medicaid expansion

• CDPHE has engaged stakeholders in brainstorming a list of “critical events” commonly experienced by clients that result in serious health care access issues. The list is now part of the CO HIV AIDS Strategy (COHAS)
• Nominations for CE funding may come from either community organizations or CDPHE staff
• The “Data Sharing and Privacy Task Force” has been addressing confidentiality implications

• The support is meant to be short-term and moving toward stabilization. The client will have tasks to complete.
• The client will need intensive case management during the period of CE support, either from community agencies or CDPHE
• There will likely be a “team approach” with coordination through the ARIES data system

• No maximum amount per client, but all requests must be justified
• The standard CE support period will be up to 6 months, with some extensions possible
• Requests will go through two levels of approval at CDPHE
• Quick turnaround” will be the expectation

• CE is meant to move clients toward stability.
• It is NOT meant to temporarily meet emergency needs and leave clients “as-is” six months later
• Every agency and staff person involved in a client’s treatment plan must share this vision and philosophy
• Documenting client progress and issues, for all the collaborators to see, is critical.

Complete CDPHE’s Acuity Tool to identify other needs and/or barriers to medical care
Eligibility Screening for Medical Insurance
Medicaid, LTMH completes enrollment
Ryan White enrollment (ADAP, HIAP, SWAP)
If Qualified for ACA Marketplace-LTMH discusses case with Health Care Access Unit Staff
Discuss options for medical care, sign proper ROIs
Facilitation of first medical Visit
Share any Behavioral Medical Care needs with provider
Make other referrals as appropriate(Build a support network for client)

• Recently homeless or pending eviction
• Recently unemployed• Diagnosed with a
gonorrhea, syphilis, or chlamydia
• Worsening health status due to hepatitis C
• Named as a partner to a person recently diagnosed with HIV
• Intimate partner violence and sexual assault
• Diagnosed with another acute illness requiring complex medical treatment or hospitalization
• Evidence based screening shows potentially severe addiction or drug dependence.
• Evidence based screening shows potentially severe mental illness.

Any service that is allowable under HRSA guidelines can be paid for with Critical Event
funding.
The most common types of services will be:
Emergency Financial Assistance Housing Substance Use Treatment (outpatient and residential) Mental Health Services.

• Are clients satisfied with the services they receive through Critical Events?
• Do Critical Events services make a difference?
• Do Critical Events clients experience increased positive health outcomes?
• Are participating agencies able to implement the Critical Events protocol?
• Can a web-based client level data collection system be used across agencies for a support services program successfully?
• What was the level of satisfaction with the Critical Events project from the perspective of the agencies?
Client Level Agency Level

• CDPHE is developing a funding base for a similar CE system for HIV negative clients
• So far, CHAPP has allocated some funding
• Eligibility criteria and the list of “critical events” is under development
• Projected implementation is July 2015
• CDPHE is developing a funding base for a similar CE system for HIV negative clients
• So far, CHAPP has allocated some funding
• Eligibility criteria and the list of “critical events” is under development
• Projected implementation is July 2015

Comprehensive - Consider the entire medical and psychosocial situation of the client.
Short term - The standard period of CE Assistance is six months, with a case-by-case decision about extensions.
Motivational - Payments tied to client progress on tasks. A pattern of failing to make progress on assigned tasks will result in a cancellation of CE Assistance.

Task: Client will maintain non-use of alcohol while residing at the Serenity Sober Living Facility during March.
Assigned to: Client
Target date: March 22, 2015
Follow up date: March 31, 2015
As documented by: Marge Smith at the Serenity Sober Living Facility will fax the UA results to the CE Sponsor at 303-555-5555 by 3/22/15.
Outcome: In Process
Budget: $750 rent payment to Serenity Sober Living Facility for April is contingent on the clean UA being faxed by target date.

• Ideally, clients will move to self-sufficiency
• If still needing assistance, they will need to transition to other, ongoing sources:
Ryan White Part A funded housing, EFA, etc.
Ryan White Part B funded housing, EFA, etc.
Assistance provided outside the Ryan White system

We are living “the future”, right here, right now.
Five years ago, who would have thought that we would have the tools to virtually end this epidemic?
Ending AIDS initiatives – NY, Washington, LA….what do we need to do to all move towards this goal?