Embed Size (px)
Citation preview
Aneurin Bevan Health Board
Medicines Management Policy, Code of Practice
As an interim agreement this document has been transferred from the former Gwent Healthcare NHS Trust to Aneurin Bevan Health Board. To the best of our knowledge the document is applicable across all areas of the Health Board. If however you believe it is not please contact [email protected] who will contact you and arrange formal review of the document.
N.B. Staff should be discouraged from printing this document. This is to avoid
the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the document
N.B. The Controlled Drugs and Non-Medical Prescribing Policies are currently
being developed and will be made available shortly, any questions in the interim should be directed to the Head of Pharmacy.
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011Owner: Chief Pharmacist Expiry date: 13 May 2012
Policy Number: ABHB/Clinical/0010

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date:13 May 2009Approved by: Clinical Forum Review date:13 May 2011 Expiry date: 13 May 2012
Page 2
Contents:
1 GLOSSARY OF TERMS AND ABBREVIATIONS ........................... 7
2 EXECUTIVE SUMMARY.................................................................... 11
3 POLICY STATEMENT ........................................................................ 11
4 POLICY AIM ......................................................................................... 11
4.1 Guidance on Safe and Appropriate Prescribing:.................................... 12 4.2 Classification of Drugs ........................................................................... 12
5 RESPONSIBILITIES ........................................................................... 13
5.1 Corporate Responsibilities..................................................................... 13 5.2 Operational Responsibilities .................................................................. 13
6 RISK MANAGEMENT......................................................................... 16
7 LEGISLATION AND GUIDANCE ON THE CONTROL OF MEDICINES..................................................................................................... 16
8 PRESCRIBING ..................................................................................... 17
8.1 Prescribing Medicinal Products – Who May Prescribe? ........................ 17 8.2 Prescriptions - Inpatients ....................................................................... 17 8.3 Discontinuing Medicines/Amendments to Prescriptions ........................ 20 8.4 Special additional charts........................................................................ 20 8.5 Discharge Notification and Prescription Forms...................................... 21
8.5.1 Discharge Prescriptions............................................................. 21 8.5.2 Out Patient Prescriptions ........................................................... 22 8.5.3 Discharge prescriptions transcribed by a pharmacist ............ 23 8.5.4 Dietetic Products ........................................................................ 24
8.6 Medicinal products issued other than by the pharmacy department ...... 24 8.7 Prescribers’ Specimen Signature........................................................... 24 8.8 Telephoned and Faxed Prescriptions .................................................... 25
8.8.1 Prescribing by Telephone – Verbal Prescriptions ................... 25 8.9 Regular Review of Prescriptions............................................................ 25 8.10 The Formulary ....................................................................................... 26

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 3
9 PATIENT GROUP DIRECTIONS (PGD) ......................................... 26
10 PATIENT SPECIFIC DIRECTION (PSD) ........................................ 27
10.1 Patient Specific Protocol........................................................................ 28
11 PHARMACY DEPARTMENTS .......................................................... 28
11.1 Responsibility......................................................................................... 28 11.2 Security.................................................................................................. 28 11.3 Purchasing of Medicinal (and other) Products ....................................... 29 11.4 Manufacture of Medicinal Products........................................................ 30 11.5 Storage of Medicinal Products within Pharmacy Departments .............. 30 11.6 Supply of Medicinal Products ................................................................ 31
11.6.1 Authorities under which a supply may be made:..................... 31 11.6.2 Telephoned and faxed orders .................................................... 32 11.6.3 Supply records............................................................................ 32
11.7 Dispensing quantities to be supplied ..................................................... 33 11.8 Labelling of Medicinal Products ............................................................. 34 11.9 When pharmacy departments are closed .............................................. 34 11.10 Ward Clinical Pharmacist Responsibilities............................................. 35 11.11 Controlled Stationery ............................................................................. 35
12 ORDERING STOCK DRUGS AND PHARMACEUTICALS (ACUTE AND COMMUNITY)....................................................................... 36
12.1 Responsibility......................................................................................... 36 12.2 Stock Medicines..................................................................................... 37
12.2.1 Revision of stockholding ........................................................... 37 12.2.2 Ordering stock drugs and pharmaceuticals ............................. 38 12.2.3 Top up by Pharmacy Staff.......................................................... 38 12.2.4 Delivery ........................................................................................ 38 12.2.5 Receipt of Medicines .................................................................. 39 12.2.6 Lending/borrowing medicines ................................................... 39
12.3 Ordering Controlled Drugs..................................................................... 40
13 STORAGE OF MEDICINAL PRODUCTS ........................................ 40
13.1 Stock holding ......................................................................................... 40 13.2 Inspection of drug stocks ....................................................................... 40 13.3 Medicinal Products ................................................................................ 41 13.4 Refrigerated Storage ............................................................................. 41 13.5 Medicine Trolleys................................................................................... 41 13.6 Emergency Medicines ........................................................................... 42 13.7 Patients Own Drugs............................................................................... 42 13.8 Unlawful Items – Drugs, etc................................................................... 42

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 4
14 GENERAL SECURITY ........................................................................ 44
14.1 Health and Safety .................................................................................. 44 14.2 Custody of Medicines Cupboard Keys................................................... 44 14.3 Bed Side Medicine Cabinet Keys........................................................... 45 14.4 GP Out of Hours .................................................................................... 45 14.5 Drug and Pharmaceutical Samples ....................................................... 45 14.6 Action to be taken in the Event of a Stock Discrepancy......................... 45
15 ADMINISTRATION ............................................................................. 46
15.1 Nurse Procedure.................................................................................... 47 15.2 Children and Neonates .......................................................................... 48 15.3 Emergency Administration..................................................................... 48 15.4 Measurement and administration of liquid medicines via oral and other enteral routes ..................................................................................................... 49 15.5 Administration Check-list of Medicines .................................................. 49 15.6 Administration of Controlled Drugs by Nurses ....................................... 50 15.7 Immunisation and Vaccination............................................................... 50 15.8 Administration Against Pharmacist Amended Prescriptions – Clarification of Roles and Responsibilities.......................................................... 51 15.9 Administration of Medicines to Patients at Home................................... 52 15.10 Patient Own Drugs (PODs).................................................................... 52 15.11 Incident Reporting.................................................................................. 52 15.12 Self Medication by Patients and Administration by Non Staff Carers..... 53 15.13 Aids to Support Concordance (compliance aids) ................................... 54 15.14 Complementary and Alternative Therapies............................................ 55 15.15 Administration of Drugs by Midwives ..................................................... 55
15.15.1 Supply of Pethidine for Home Confinements ........................... 55 15.15.2 Administration of Controlled Drugs by Midwives .................... 56 15.15.3 Prescription only Medicines ...................................................... 56 15.15.4 Inhalation Gases ......................................................................... 56 15.15.5 Audit of Records ......................................................................... 57
15.16 Management of Errors or Incidents in the Administration of Medicines . 57 15.17 Verbal Instructions to Administer ........................................................... 57 15.18 Patients Detained under the Mental Health Act 1983; Consent to Treatment ........................................................................................................... 58 15.19 Administration of medicines by the parenteral route .............................. 59
15.19.1 Parenteral medicines administration by nursing staff ............ 59 15.20 Administration Using Infusion Devices................................................... 60 15.21 Administration of Cytotoxic Drugs.......................................................... 61 15.22 Adverse Drug Reactions........................................................................ 61 15.23 Medical Gases....................................................................................... 62
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 5
16 NON AVAILABILITY OF A MEDICINE........................................... 62
17 DELAYED OR OMITTED MEDICINES ……………………………62
17.1 Action in the Event of a Delay or Omission ……………………………….63
18 ADMISSION AND DISCHARGE MEDICATION PROCEDURES 63
18.1 Medication on Admission....................................................................... 63 18.2 Patient’s Own Drugs (in use) ................................................................. 64 18.3 Patient’s Own Drugs for Disposal .......................................................... 64 18.4 Discharge on Wards where the PODS is in Place ................................. 64 18.5 Receipt of the Discharge Drugs from Pharmacy.................................... 64
19 DRUGS ON CLINICAL TRIAL .......................................................... 65
20 PATIENT’S HOLIDAYS...................................................................... 65
21 OCCUPATIONAL HEALTH DEPARTMENT .................................. 66
22 ACTION TO BE TAKEN IN THE EVENT OF A STOCK DISCREPANCY .............................................................................................. 66
23 DISPOSAL OF MEDICINAL PRODUCTS ....................................... 67
23.1 Medicinal Products Brought into Hospital by Patients............................ 67 23.2 Disposal of Cytotoxic Products .............................................................. 68 23.3 Disposal of Medicinal Products by the Pharmacy Department .............. 68 23.4 Disposal of Medicines in the Community ............................................... 69
24 REPORTING DEFECTS...................................................................... 69
25 HAZARD WARNINGS......................................................................... 70
26 TRANSPORT AND STORAGE OF MEDICINAL PRODUCTS .... 71
26.1 Outside hospitals and community based services ................................. 71 26.2 To Patient’s Home ................................................................................. 73 26.3 In the Hospital Setting............................................................................ 73 26.4 Required for Patients in Transit ............................................................. 73
27 UNLICENSED MEDICINES ............................................................... 73
27.1 Medicines used Outside their Product Licence...................................... 74

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 6
28 AMBULANCE SERVICE..................................................................... 75
29 APPENDICES ....................................................................................... 76
Appendix 1: Administration of parenteral prescription only medicines for the purpose of saving life in an emergency. ............................................................. 77 Appendix 2: Administration of parenteral prescription only medicines for the purpose of saving life in an emergency – crash call. .......................................... 78 29.1 Appendix 3: Aneurin Bevan Health Board – Drug and Dressing Defect Reporting Form for Wards and Departments...................................................... 79 Appendix 4: Prescribing for Members of the Health Board’s Staff and Families. 81 Appendix 5: Action to be Taken Outside of Pharmacy Opening Hours .............. 82 29.2 Appendix 6: Issues Relating to Drugs in Patients Homes...................... 83 Appendix 7: Drugs Carried by Community Midwives.......................................... 84 Appendix 8: Prescription-only medicines which can be administered parenterally by midwives in the course of their professional practice..................................... 85 Appendix 9: Disclaimer Form ............................................................................. 86 Appendix 10: Aneurin Bevan Health Board - Verbal Instructions to Administer a Medicinal Product............................................................................................... 87 Appendix 11: Gwent GP Out of Hours Service (GPOOH) .................................. 88 Appendix 12: Outpatient Department GP Medication Review Form................... 89
30 REFERENCES ...................................................................................... 90
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 7
1 GLOSSARY OF TERMS AND ABBREVIATIONS
Abbreviations The following common abbreviations may be used on prescriptions: ac Before food bd/bid Twice daily hrly Hourly od Daily mane/om In the morning nocte/on At night pc After food prn When required qds/qid Four times daily qqh Every four hours stat Immediately tds/tid Three times daily
Any abbreviation not readily understood must be clarified with the prescriber before either dispensing or administration
Accident An unplanned event, which may or may not lead to an injury.
Administer Administer to a human being or animal, whether orally, by injection or by introduction into the body in any other way, or by external application, a substance or article either in its existing state or after it has been dissolved or dispensed in, or diluted or mixed with, some other substance used as a vehicle
Adverse/Clinical Incident
Any occurrence, which is not consistent with the routine treatment or care of the patient or the routine operation of the Health Board.
Appropriate Nurse Practitioner
Means: a) a person who is (i) registered in the register maintained by the NMC
for Nursing, Midwifery and Health Visiting (the professional register); and (ii) has a district nursing qualification additionally recorded in the professional register or
b) a person registered in the professional register as a health visitor
Black Triangle Drugs
Newly introduced drugs, are subject to intensive monitoring for potential side effects by the Medicines Healthcare products Regulatory Agency and CSM (identified by in the British National Formulary)
Community Includes the non-hospital sites where drugs are stored supplied and administered.
Community Nurses
Includes all nurses working in the community setting; district nurses, health visitors, school nurses, midwives, community psychiatric nurses, learning disabilities and drug and alcohol services.
Complimentary Medicines
The principles outlined in this policy will apply to preparations that are generally considered to be alternative or complimentary medicines.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 8
Controlled Drug Includes those drugs classified under the Misuse of Drugs Act 1971 and its
associated regulations. Schedule 1 Controlled Drugs e.g. LSD and cannabis may only be
possessed or used by persons with a Home Office licence for research or other special purpose. Before anybody in the Health Board considers applying for such a licence they must first consult the Chief Pharmacist. (A pharmacist may be asked to deal with Schedule 1 drugs removed from patients on admission. A pharmacy cannot take possession of the drug other than for the purpose of destroying it or handing it to a police officer. The patient’s confidentiality should normally be maintained. A Schedule 1 drug must not be handed back to a patient at discharge)
Schedule 2 includes the opiates, the major stimulants such as amphetamine, and quinalbarbitone
Schedule 3 includes temazapam, the barbiturates, buprenorphine,
pentazocine, flunitrazepam, and diethylpropion Schedule 4 includes anabolic and androgenic steroids and most of the
benzodiazepines Schedule 5 includes preparations of certain Controlled Drugs e.g.
codeine, pholcodeine and morphine, which are exempt from full control when present in medicinal products of low strength.
Controlled Stationery
Controlled stationery is any stationery, which could be used to fraudulently obtain medicines including requisition or order books, prescription charts, Controlled Drug order books and particularly blank prescription forms.
Doctors Includes all doctors who are fully registered with the General Medical Council (GMC). Provisionally registered doctors (FP1’s and FP2’s) and doctors with limited registration (overseas qualified doctors) may only prescribe in connection with their employment.
Drug In this document means the same as “Medicinal Product”
GPMTC Gwent Partnership Medicines and Therapeutics Committee
GP OOH In this document means a GP (salaried or sessional) working in the Out of Hours Service.
GSL In this document, means General Sales List Medicines which can be sold over the counter at any establishment.
Hospital Includes acute, community and mental health inpatient units unless stated otherwise.
In-patient Is a patient who stays overnight in a hospital bed
Locum Consultant
Any consultant who is on a temporary contract.
Management of Medicines
(Medicines Management) refers to the policies, procedures and quality assurance for the safe and appropriate use of medicines.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 9
Medicinal Product /Medicines/ Drugs
Are all substances defined under the Medicines Act as being medicinal products.
(Note: For the purpose of this policy, items classified as medical devices but which are administered to patients e.g., bladder installations are to be regarded as medicinal products irrespective of whether they are controlled by the Medicine Devices Agency or the Medicines and Health Care Products Regulatory Authority).
Medicinal Purpose
Means any one or more of the following purposes: Treating or preventing disease Diagnosing disease or ascertaining the existence, degree or extent of a
physiologic condition Contraception Inducing anaesthesia Otherwise preventing or interfering with the normal operation of a
physiological function
MHRA Medicines and Healthcare Products Regulatory Agency.
Midwife Refers to issues pertaining directly to practising midwives in both acute and community settings.
Near Miss An occurrence which, but for luck or skilful management, would in all probability have become an adverse incident.
Non medical prescribers
In this document refers to nurses, pharmacists and other appropriate healthcare professionals who have undertaken additional training (Supplementary and/or Independent and have recorded this qualification with their professional body.
Nurse Includes nurses trained in general nursing, midwives and health visitors who are registered with the Nursing and Midwifery Council (NMC). Also those trained in Children’s, Mental Health and Nursing Disabilities Nursing. A first level nurse is a nurse registered on part 1, 3, 5, 8, 9, 10, 11, 12 (Pk2), 13 (Pk 2), 14 (Pk2), 15 (Pk2), of the register.
Nursing assistant Includes nursing auxiliaries and healthcare support workers.
Nurse in charge Means the Sister or Charge Nurse responsible for a ward, nursing team, department or clinic.
“Off label” use Drugs used outside the product licence: drugs used in a manner, in conditions, or in patient types which are outside the Summary of Product Characteristics (Data Sheet).
OOH Gwent OOH (urgent Primary Care) Service.
Out-patient Is a patient who attends a clinic, accident and emergency, or a ward but who does not stay overnight
ODP
In this document, means Operating Department Practitioner
P In this document, means pharmacy medicines – these may only be sold

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 10
under the supervision of a Pharmacist from a registered pharmacy.
PGDs
Patient Group Directions – this is a specific written instruction relating to the supply and administration or just administration of Prescription Only Medicines, by specified groups of NHS staff to patients who have not been identified prior to their arrival. The PGD is authorised by a Doctor, Chief Pharmacist and the Medical Director. They are only to be used when it is in the best interest of the patient (WHC: 2000:116 Patient Group Directions and Appendices). See Policy for the Use of Patient Group Directions .5
PSD Patient Specific Direction – See Section 10.
PSP
Patient Specific Protocol – A written statement defining the management of a named patient, which has been agreed by the clinician responsible for the patient and by other appropriate health professionals. See section 10.1.
Pharmacist In this document means a currently registered Member of the Royal Pharmaceutical Society of Great Britain employed by Aneurin Bevan Health Board
Pharmaceuticals Includes non-therapeutic items covered by the Code of Practice (e.g. disinfecting and sterilising agents).
Pharmacy Department
Means any Aneurin Bevan Health Board pharmacy department
PODs Patients own drugs.
POM’s Prescription only medicines
Prescriber In this document refers to a person who is legally entitled, and authorised by the Health Board to order medicinal products (including prescription only medicines) to be supplied or administered to a patient receiving medical services from the Health Board
Prescription In this document refers to a written order to supply (dispense) a medicinal product to a particular patient made to a professional who is legally authorised to dispense. Entries written on a patient’s prescription and administration record sheet are directions to administer but can be taken as an authority by the pharmacy to make a supply (including take-home medicines) provided the wording is clear
Senior Nurse Means Senior Nurse with professional and/or managerial responsibilities at higher level than the Nurse in Charge. The term covers clinical midwifery managers, clinical nurse managers, community service managers, nurse consultants and clinical nurse specialists.
SPC In this document, means Summary of Product Characteristics
Supply Refers to the provision of medicines for a patient to take away such as take home medication, out patient medication, or casualty pre-packs.
Health Board
In this document, means Aneurin Bevan Health Board
Unlicensed Medicines
Medicines with no UK Product License.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 11
Untoward Incident
Any event that has given or may give rise to actual or possible personal injury, compromised care, caused patient dissatisfaction or resulted in damage to property.
2 EXECUTIVE SUMMARY
The Aneurin Bevan Health Board Medicines Policy 2008, a Code of Practice for the Management of Medicines, updates and replaces previous Medicines Management Policy, Code of Practice, September 2003. It reflects current practice and incorporates new developments and changes in legislation The key principles that underpin the Code of Practice are legal, quality and safe practice. It applies to all doctors, dentists, nurses and other health care professionals across the Health Board, involved in the management of medicines. The Code of Practice sets out the framework that supports the Health Board’s commitment to the safe and secure handling of medicines to protect its patients, staff and visitors and its financial resources.
3 POLICY STATEMENT
The Aneurin Bevan Health Board is committed to the safe and secure handling of medicines to protect its patients, staff and visitors and its financial resources. The principles that underpin the Code of Practice – legal, quality and safe practice, apply to all doctors, nurses, dentists, pharmacists and other health care professionals across the Health Board, involved in the ordering, supply, storage, prescribing, administration and disposal of medicines. The medicines include Prescription Only Medicines (POMs), Pharmacy (P), General Sales List (GSL) and Controlled Drugs. Also included are Complementary Medicines and pharmaceuticals (non-therapeutic items). Controlled drugs are covered in detail in the Policy for the Management of Controlled Drugsi.
4 POLICY AIM
The purpose of the Code of Practice is to set out a framework to promote safe and secure systems for controlling and handling of medicinal products in the hospitals, clinics and community services operated by Aneurin Bevan Health Board as part of an overall medicines management process.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 12
4.1 Guidance on Safe and Appropriate Prescribing:
Guidance on safe and appropriate prescribing will be considered and disseminated by the Prescribing Advisory Group. In general:
• Medicines need to satisfy tests of clinical effectiveness.
• The use of medicines must be justifiable on safety grounds, accepting that this means a benefit/risk judgement will be needed.
The use of medicines should also be justifiable based on appropriate criteria, i.e. is it the right therapy, right drug, right dose to treat this patient’s illness/problem. This should include a test of cost and clinical effectiveness, i.e. is it a cost effective choice given the alternative therapies available and the circumstances of the patient. In addition to this Code of Practice, healthcare professionals must abide with the current version of the relevant professional documents, (e.g., the Nursing and Midwifery Council document (NMC), “Code of Professional Conduct” June 1995, “Scope of Professional Practice” June 1992, “Midwives Rules and Code of Practice” 1998 and “Guidelines for Administration of Medicines”, October 2000).
4.2 Classification of Drugs
Drugs are considered as two main sub-groups, Controlled Drugs and Drugs.
i) Controlled Drugs Controlled drugs are those drugs classified under the ‘Misuse of Drugs Act 1971’, and its associated regulations.
ii) Drugs
Drugs will be taken to be all substances defined under the Medicines Act as being medicinal products. These include those restricted to supply on prescription (POM), those that can only be sold by a Pharmacist (P), and those that can be sold at any establishment, General Sales List medicines (GSL). iii) Complementary
The principles adopted for the use of drugs will also be followed for Complementary Medicines.
iv) Pharmaceuticals The term “pharmaceuticals” will be used to describe those non-therapeutic items covered by the Code of Practice (e.g. disinfecting and sterilising agents).
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 13
v) Black triangle drugs are newly introduced drugs, subject to intensive
monitoring for potential side effects by the Medicines and Healthcare products Regulatory Agency and CSM (identified by in the British National Formulary).
vi) Drugs used outside product licence are drugs used in a manner, in
conditions, or in patient types, which are outside the Summary of Product Characteristics.
5 RESPONSIBILITIES
5.1 Corporate Responsibilities
i) The Chief Executive has overall responsibility for the management of medicines in Aneurin Bevan Health Board.
ii) Medical Director This responsibility is delegated to the Health Board Medical Director, supported by the Clinical Forum and Prescribing Advisory Group.
iii) Chief Pharmacist
The Chief Pharmacist is responsible for organising, monitoring and reporting on the Medicines Management Policy, its systems and procedures.
5.2 Operational Responsibilities
i) Senior Nurses are responsible for ensuring that there are appropriate systems in place for the following:
• The ordering of drugs. • The storage (physical and environmental conditions of drugs). • The administration of drugs (other than that done by a Doctor). • The recording and administration. • The security of drugs and prescription forms. • The supply of drugs to patients in accordance with Patient Group
Directions/ Patient Specific Directions. • The reporting of drugs related incidents and errors via the Incident
Reporting System. • The safe and proper disposal of unused/unwanted drugs and
pharmaceuticals. • The retention of documents relating to the ordering, storage and
administration and supply of drugs.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 14
• The induction of new staff with respect to the Code of Practice. • The education and training required to enable nurses to comply with
this Code of Practice and for ensuring that a copy is readily available to staff.
The Nurse in Charge will have joint responsibility with the Chief Pharmacist for the ordering system where there is a pharmacy provided top-up service.
The Community Services Manager is responsible for ensuring that drug transport arrangements in the community are safe, secure and effective. The above nurse managers are responsible for ensuring that there are appropriate systems in place for the following:
• The investigation and reporting of drug related incidents and errors via the Incident Reporting System.
• The auditing of compliance with the Code of Practice and the implementation of remedial action.
ii) Nurses, Midwives and Health Visitors Each nurse is responsible for:
• Reading and understanding this Code of Practice. • Complying with this Code of Practice and the NMC guidance. Not
undertaking tasks beyond their qualifications, competency or authorisation.
iii) Doctors / Dentists Clinical Directors will devolve the operational management responsibility to Consultants who will ensure that doctors/ dentists are aware of and comply with the Code of Practice.
iv) Chief Pharmacist The Chief Pharmacist is responsible for ensuring that there are sufficient systems in place for the following:
• Providing a safe, effective, sufficient and secure system for drug stocks held within pharmacy.
• Providing a safe, effective, efficient and secure system for drug distribution.
• Providing a system for monitoring ward drug usage and advising on appropriate stock range and stock holding levels.
• Providing advice on drug security.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 15
• Providing advice on appropriate, environmental storage conditions. • Providing advice on safe and proper means of disposal of unused/
unwanted drugs. • Providing advice on safe and effective systems and arrangements for
drug administration. This includes commenting and advising on drug administration errors and near misses reported via the Incident Reporting system.
• Providing advice on transport of drugs and other pharmaceuticals. • Providing a system, when the pharmacy is closed, of access to
emergency drug stocks and the availability of a pharmacist for emergency duties.
• Where a pharmacy run top-up service is provided there will be a shared responsibility between the Nurse in Charge and the Chief Pharmacist.
In hospitals, each ward will have an assigned clinical pharmacist who has a delegated responsibility for routine implementation of the above. In the community, the senior pharmacists responsible for the community arm of the pharmacy services will be the delegated liaison pharmacist. The Chief Pharmacist is charged with the responsibility for medicines management throughout the Health Board.
As part of the responsibility of delivery of the medicines management process, the Chief Pharmacist will ensure that the following explicit, written, quality standards are prepared and audited:
• The process of prescribing of medicines in the Health Board. • The appropriateness of medicines prescribed for individual patients
including licence status and adherence to agreed therapeutic guidelines.
• The preparation of parenteral medicines. This will include all Health Board clinical areas as well as the main pharmacy department.
• The pharmacy reviewing of prescriptions and of dispensing medicines.
• The administration of medicines to patients. • The supplying of medicines to take home and the counselling of
patients about those medicines. • The reporting of medication errors. • Medicines administered for clinical research and drug trials.
These standards must be audited regularly. The Chief Pharmacist is responsible for organising, monitoring, and reporting on the Medicines Management Policy, its systems and procedures.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 16
All staff involved in medicines management have a professional responsibility to comply with Aneurin Bevan Health Board policy on Medicines Management, Code of Practice.
6 RISK MANAGEMENT
The Chief Pharmacist or a senior member of the Pharmacy Management Team will be a member of the Health Board’s Risk Management Committee. The Associate Director for Clinical Governance is a member of the Risk Management Committee and is responsible for leading the Health Board’s risk management process. The risks inherent in medicines management and the effectiveness of risk control measures must be monitored and reviewed on a continuous basis. Senior management (Pharmacy and Health Board as appropriate) must be informed of any significant risks and risk control measures via risk assessment and the Health Board’s Incident Reporting Policy and Procedure24. Trends in Incidents involving medicines are routinely reported to the Risk Management Group. The Medication Safety Group reviews and analyses themes in medication errors across the Health Board, indentifying good practice in strategies to minimise medication errors across directorates. All healthcare staff involved with medicines should undertake continuing professional development (CPD), which is aligned with clinical governance requirements, in order to keep up to date with changes in medicines management.
7 LEGISLATION AND GUIDANCE ON THE CONTROL OF MEDICINES
The prescribing, supply, administration, storage and disposal of medicinal products is governed by legislation e.g. Medicines Act 1968, (Amendment) Regulations 1995, Misuse of Drugs Act 1971, (Modification) Order 1996, as amendedii. The Department of Health and the National Assembly issue further guidance from time to time e.g. Guidelines for the Safe and Secure Handling of Medicines, A Team Approach, (Revised Duthie Report March 2005)iii. Anyone involved in any way with medicinal products in connection with the operation of Aneurin Bevan Health Board or its services must comply with current legislation, official guidance, and the Policy and Procedures contained within this document.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 17
If circumstances arise such that this Code of Practice cannot be applied then the prime consideration will be the safe and effective treatment of any patient concerned. However, those staff involved must document all alternative medicines taken in the appropriate records and inform senior professional staff.
8 PRESCRIBING
8.1 Prescribing Medicinal Products – Who May Prescribe?
Medicinal products may only be prescribed by persons who are legally qualified to do so. Prescribers must be currently registered with the appropriate professional body. They must be employed or sub-contracted (e.g. GP OOH) and authorised by the Health Board to prescribe and have the appropriate knowledge and experience to prescribe e.g. a doctor, a dentist, or an appropriately accredited practitioner e.g. a Nurse/Pharmacist. For further information also refer to the current Health Board Policy - Non Medical Prescribing Policy (Supplementary and Independent)iv. Prescribers may only prescribe from the appropriate list of medicinal products accorded to their profession. It is anticipated that the number of professionals authorised to prescribe will increase. Only doctors who are fully registered by the General Medical Council (GMC) may prescribe other than in connection with their employment. Provisionally registered doctors (Foundation Practitioners 1) and doctors with Limited Registration (overseas-qualified doctors) may only prescribe in connection with their employment (this means for example that they may not write prescriptions for patients who are not registered as Health Board patients and who they are not treating as part of their current employment). Persons supplying or administering medicines under a Patient Group Direction may only supply or administer the medicines in accordance with that particular direction. See Health Board Policy for the use of Patient Group Directionsv. All prescribers should comply with the GPMTC formulary requirements.
8.2 Prescriptions - Inpatients
Medicinal products may only be prescribed on an approved Health Board prescription or in-patient prescription and administration record sheet.
i) The following patient details must be entered:
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 18
• The patient’s name. • The patient’s address. • Unit number. • Date of birth. • Ward name. • Name of the Consultant. • Any known drug sensitivities. (Details of the nature of the sensitivity
should be given where possible, e.g. rash. Charts should also be endorsed with ‘None Known’ to indicate when No Known Allergies have been found).
• The weight of the patient should also be entered for all paediatric patients and for patients where dose adjustments by weight will be made.
• A pre-printed addressograph label should be used whenever possible and attached to the prescription chart or form before other details are added.
ii) The following medication details must be entered
• The name of the medicine should be written legibly using block capitals and approved names.
• Proprietary names (i.e. brand names) must not be used routinely. The use is acceptable for multi-ingredient preparations with no approved name or for products whose proprietary name defines a specific formulation (e.g. slow release Diltiazem preparations).
• The date on which the treatment is to commence must be entered on the prescription sheet.
• Dose must be expressed in SI units. Quantities less than 1 gram must be written as milligrams. Quantities less than 1mg must be written as micrograms (and where used, nanograms). The decimal point should be avoided – for example 500 mg not 0.5 g.
• Wherever a decimal point is necessary, the prescriber and the person administering the medicine must exercise great care in the writing of the prescription and/or administration of the medicine.
• The terms ‘microgram’ and ‘nanogram’ must not be abbreviated but must be printed in full and used for quantities of less than 1 milligram.
• The word ‘units’ (for example insulin) should be written in full. • The only abbreviations that are acceptable are:
mg milligram g gram kg kilogram l litre ml millilitre mmol millimole
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 19
• The dose required must not be expressed in the terms of dosage for a single ingredient preparation e.g. Atenolol “2 tablets” is not acceptable; it should be written as Atenolol “100mg”.
• Dose frequency. • For regular medication the prescriber must use either the 24-hour
clock or the pre-set drug round times to indicate administration time. • For “as required medicines”, the times of administration must be
written by the prescriber where relevant, e.g. hypnotics. The maximum frequency must be stated, as well as the maximum dose, within 24 hours. The frequency may be noted, e.g. prn 8 hourly and the reason for administration must be noted, e.g. for anxiety.
• For some medication it may be easier to define a maximum 24 hour dose (e.g. for nebulised salbutamol). In these situations the frequency of dosing must be prescribed but the time may be determined locally, in accordance with an agreed protocol or procedure.
iii) Pre- medication is medication prescribed prior to surgical procedures.
The anaesthetist usually prescribes pre-medication (before surgical procedures) if required by the patient. Should the patient not be seen prior to surgery by the anaesthetist then the junior doctor may prescribe the pre –medication.
iv) Route of administration - Only the following abbreviations are acceptable:
• IM for intramuscular • INH for inhalation • IV for intravenous • NEB for nebuliser • PO for oral • PR for rectal • SC for sub-cutaneous • PV for vaginal • S/L for sub-lingual • Top for Topical
Other routes of administration must be written in full.
v) Prescribers signature
All items on the main prescription chart or additional charts must bear the date and full signature of the authorised prescriber. In accordance with GMC guidance, registered doctors must use their registered name when signing statutory document, (including prescriptions). The signature of a medical student is not acceptable.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009
8.3 Discontinuing Medicines/Amendments to Prescriptions
The date when a medicine is discontinued must be entered in the administration box with the prescribers full signature. A diagonal line must de drawn through the prescription so that cancellation is obvious, but the prescription is not obliterated e.g. Incorrect entries must be scored through and the word ‘cancelled’ written against it by the prescriber. For regular medication it is possible to make one dose, frequency and route of administration change for each regular medication on the medication and administration record. If this dose change option is used the first dose column must be crossed through. The new dose, date and route must be entered in the second column and the prescriber must initial the change. If another change is required the whole prescription must be rewritten and the original entry cancelled. If an additional instruction is added by the original prescriber then this needs to be initialled and date added. If a minor amendment to clarify the prescription is required by a doctor or pharmacist then the change must be signed and dated. For any other change the medicines must be crossed out and rewritten. For dose or frequency changes for ‘when required’ medicines the original prescription must be crossed out by a diagonal line as above and the prescription rewritten.
8.4 Special additional charts
All medicines must be prescribed on the prescription sheet. When more than one chart exists then the front of the chart should state ‘1 of 2’, or ‘2 of 2’. Where separate charts are used, e.g. intravenous infusion (IV) charts, medicines should still be prescribed on the main chart with the words, “see additional charts” written across the medication boxes. The only exception to this is the Intensive Therapy Unit (ITU) when nearly all medicines are prescribed by intravenous infusion.
Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 20

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 21
8.5 Discharge Notification and Prescription Forms
8.5.1 Discharge Prescriptions The yellow copy of the combined discharge notification and prescription form is retained by pharmacy. The white copy is conveyed to the patient’s General Practitioner either by post or by fax to reach the patient’s GP within three days unless the patient or patient’s representative is responsible. If so they are instructed to take the copy to the GP as soon as possible during surgery hours. The pink copy of the prescription is retained in the patient’s notes. The blue copy is either given to the patient or shown/given to the community nurse/nursing home as required. If for any reason a prescriber does not wish a patient to read their form they must request the pharmacy to post it directly to the GP and not give the patient a copy. Discharge Notification and Prescription Forms must be sent to the pharmacy in a closed container or envelope to preserve confidentiality unless hand-delivered by a member of staff. An electronic discharge prescription system is being implemented throughout the Health Board and is available on many wards in place of the paper version. All medication on admission, medication prescribed during the inpatient stay and medication that is prescribed on discharge is added to the patient record. The resulting electronic record is used to produce the discharge prescription, which also records which medicines are new and which have been discontinued etc. Only if a controlled drug is prescribed, is there a need for a printed paper version to be signed by the prescriber. All other discharges can be processed electronically. The electronic prescription is printed out and retained by pharmacy and another sent to the GP by ward staff. Two copies are given to the patient, one for the patient to retain and one to give to their usual community pharmacy. A permanent record is available on CWS which can be accessed by GPs. For patients admitted using a monitored dosage system and requiring discharge on the same then the discharge prescription will be written on a WP10HP by a doctor or transcribed by a pharmacist for dispensing and supply by the patient’s usual community pharmacy. Community pharmacies usually require 24 – 24 hours notice. In working hours the pharmacist will normally be responsible for making this arrangement and out of hours the responsibility will be with the nurse in charge of the ward. The WP10HP pad must be stored securely at all times, the details of each prescription documented on the appropriate form. WP10HPs are not to be used for non monitored dosage system discharges.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 22
8.5.2 Out Patient Prescriptions The outpatient service enables senior hospital staff to carry out a medical or surgical review of a patient. At the time of writing this policy, Health Board senior hospital medical prescribers mainly use WP10HP prescription forms to prescribe. If the required medication is hospital only, unlicensed or there is an urgent clinical need then the Outpatient Triplicate Prescription Form HMR112(W) or other Health Board approved prescription form is used for writing outpatient prescriptions. Non medical prescribers use the following forms:
• WP10HIP Independent Nurse/Pharmacist Prescriber • WP10HSP Supplementary Nurse/Pharmacist Prescriber
For outpatient prescribing by non medical prescribers, see the Non-Medical Prescribing Policy (Supplementary and Independent)4. For the HMR112(W) form the top white copy is retained in pharmacy; the pink copy is given to the patient to give to his/her GP at their next appointment or posted to the GP by the outpatient department. The yellow copy must be retained in the patient’s medical record. A new protocol for outpatient prescribing (Protocol for the Prescribing of Medicines for Outpatientsvi) has been agreed with Gwent LHBs through the Gwent Partnership Medicines and Therapeutics Committee (GPMTC) and it is anticipated that the protocol will be in place from April 2009. In line with this protocol, following review of the patient, medication should only be provided where there is an urgent clinical need, or the medication required is a hospital only product or an unlicensed product. The senior medical prescriber or the authorised non-medical prescriber may request that the GP consider initiating alteration of dose of existing medication or discontinuing treatment. The senior medical prescriber or the authorised non-medical prescriber should notify the GP, in adequate time, of the patient’s diagnosis and drug therapy so that the patient’s treatment can be maintained. An Outpatient Department GP Medication Review form is included as page 6 in the protocol – see appendix 12. The prescription requirements for outpatients are the same as those indicated for inpatients (see 8.2). Under local agreement with Gwent LHBs, a system of patient pack dispensing is in place for outpatients. This enables up to one months supply to be given under normal circumstances. A larger supply may be appropriate for hospital
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 23
only medicines, clinical trial medicines etc. Consultants should personally authorise a request for more than 28 days supply. Only registered doctors and authorised non-medical prescribers may prescribe for outpatients. Therefore it is not permissible for Junior Foundation Practitioners to prescribe on an outpatient basis. Doctors and dentists using WP10(HP) prescriptions should also prescribe a maximum of 28 days medication except for finite courses such as antibiotics. GPs providing the Health Board GP OOH Service will prescribe on WP10 prescriptions. Medicines administered in outpatients should be recorded on a prescription chart and included in the notes to provide an accessible audit trail for drug therapy. Family Planning Doctors prescribe on the pre-printed sheet which is part of the patient file.
8.5.3 Discharge prescriptions transcribed by a pharmacist
i) Trained and competent pharmacists and pharmacy technicians may transcribe medication written on the drug chart onto a discharge prescription in order for it to be dispensed promptly (except for CDs and unlicensed medicines).
ii) When the doctor decides that the patient is ready for discharge the
medication will be reviewed and the doctor will write in the notes the phrase, “Home on medications as prescribed”. Any changes that are necessary to the patient’s medication, or any intended changes, must be made explicit in the medical notes and/or the necessary changes made to the inpatient prescription chart. Alternatively a sticker can be attached to the chart which states that the prescriber has reviewed the drug chart and all medication on the chart should be transcribed for discharge. The sticker must be signed, dated and a bleep number added. If there is any doubt on clarity of the intention of the prescriber then the pharmacist will contact the appropriate doctor.
iii) The pharmacist will review the prescription chart and medical notes. All
regular medication will be written on the discharge prescription with any changes to medication on admission highlighted for the benefit of the GP.
iv) PRN medication will be included on the take home prescription at the
discretion of the pharmacist, depending on the patient’s needs for these
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 24
items. Patients on regular inhaled steroids will always be prescribed rescue therapy and patients with angina will always be prescribed Glyceryl Trinitrate for sub lingual use.
v) A pharmacist or pharmacy technician will check that the patient understands
the prescribed medication regime and any changes that have been made.
vi) The pharmacist will date and sign the discharge form with the endorsement (Pharm) after the signature. No countersignature from the doctor will be required.
vii) Discharge prescriptions for controlled drugs however, must be prescribed
and signed by the doctor. See Policy for the Management of Controlled Drugs1.
8.5.4 Dietetic Products Dieticians are authorised to initiate the use of formulary dietetic products by writing them on the patient’s inpatient prescription chart. The same standards of prescribing as previously indicated apply. The dietician will endorse any items not for inclusion on the discharge prescription as “Not for TTO”. E.g. those products used for post-op “build up” use only. This helps to avoid inadvertent long term continuation.
8.6 Medicinal products issued other than by the pharmacy department
Only a pharmacy department may issue medicinal products to outpatients unless a specific Protocol, Patient Group Direction or Patient Specific Direction has been officially agreed within the Health Board. The nurse in charge of the clinic must make a record of medicinal products issued or administered on the patient’s record within the clinic. There must be a secure system for recording and monitoring medicines use from which it should be possible to reconcile incoming and out goings on a patient by patient basis. Names of health professionals providing treatment, patient identifiers and medicine provided should all be recorded.
8.7 Prescribers’ Specimen Signature
A specimen signature and example of handwriting must be provided to the pharmacy department by anybody authorised by the Health Board to write prescriptions prior to commencing prescribing. This specimen signature must be held in the pharmacy department for reference purposes.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 25
8.8 Telephoned and Faxed Prescriptions
Prescriptions may only be telephoned to a pharmacy department in very exceptional circumstances and must be authorised by a pharmacist. Instead, a fax machine should be used to transmit the prescription. Under no circumstances can controlled drugs listed in Schedules 2 or 3 of the Misuse of Drugs Regulations 2001 be dispensed against a fax. Before telephoning a prescription the prescriber must write the prescription in full, then personally read the prescription over the telephone. A pharmacist must personally take the telephone call and record the telephoned prescription in the book kept for that purpose. The name of the prescriber and the date must be recorded together with the details of the prescription. The pharmacist is professionally responsible for accepting a telephoned prescription and must only do so if the instructions are clear and unambiguous. The written prescription must be sent to the pharmacy department as soon as possible and its receipt noted in the telephoned prescription book. For discharge prescriptions from community hospitals faxing the prescription and a copy of the prescription chart to the pharmacy department for request for discharge prescriptions is acceptable. The supply will then be made in the normal way and the faxed copy compared to the original prescription, upon its receipt, within the department. The original should be provided by the next postal delivery. Adequate safeguards must exist to ensure the integrity of faxed prescriptions is maintained.
8.8.1 Prescribing by Telephone – Verbal Prescriptions See 15.17 - Verbal instructions to administer.
8.9 Regular Review of Prescriptions
Drug therapy should be reviewed by prescribers at regular intervals and as a minimum when a drug chart needs to be rewritten. Patients who have been prescribed long term depot preparations must be reviewed at intervals not exceeding six months.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 26
8.10 The Formulary
The formulary is compiled for use by prescribers in primary and secondary care. It lists the medicinal products that may be prescribed. Requests for non-formulary drugs to be prescribed on an exceptional basis within the Health Board should be made to the chairman of the Prescribing Advisory Group. Applications for additions to the formulary may be made as follows:
• Application for drugs to be prescribed in primary and secondary care should be made to the Chairman of the Gwent Partnership Medicines and Therapeutics Committee (GPMTC).
• Applications for drugs to be prescribed solely in secondary care
should be made to the Chairman of the Prescribing Advisory Group.
• In both instances the application should be made on the formulary application form on the Torfaen LHB website under GPMTC: Link is:
www.wales.nhs.uk/sites3/home.cfm?ORGID=284
• GP OOH Formulary – medicines supplied from the GPOOH
pharmacy supplied stock may only be those listed in the Gwent GPOOH Medicines Formulary. Applications for additions to the formulary should be made to the Clinical Director GPOOH. GPs or nurses prescribing within the OOH service should prescribe from within the formulary.
9 PATIENT GROUP DIRECTIONS (PGD)
See the Health Board Policy for the Use of Patient Group Directions5. In most cases, the most appropriate clinical care will be provided on an individual basis by a specific prescriber to a specific individual patient. The Patient Group Direction (PGD) is a written direction relating to supply and/or administration, or just administration, of a prescription-only medicine (POM) to persons, not known at presentation and is signed by a doctor or dentist and by a pharmacist. It is then referred to the Medical Director for final approval by the Health Board. A PGD must not be confused with a written direction. Amendments made to Article 12 of the POM Order mean that a written direction must now be patient-specific. In addition, supply on the authority of a patient-specific written direction is now extended to apply to health authorities, Health Boards and other National Health Service bodies.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 27
A PGD for the supply and/or administration of medicines must only be considered where it would offer a benefit to patient care without compromising safety in any way. This is best achieved by involving representatives of all the relevant health care professions, including the professional group expected to supply or administer medicines under the direction. A senior representative of each profession will be responsible for ensuring the suitability and competence of the professionals operating within the scheme. Healthcare professionals involved with PGDs in any way must operate within all the legal requirements as well as the professional requirements of their Professional Code of Ethics.
10 PATIENT SPECIFIC DIRECTION (PSD)
Legislation allows a hospital to sell or supply a prescription only medicine in the course of its business, against a specific “written direction” of a doctor instead of a prescription. The written direction does not need to comply with the requirements specified for prescriptions, but does need to relate to a specific patient. The intention is to permit the sale or supply of medicines against the patient’s administration chart or patient notes. Entries on a patient’s administration chart are directions to administer. Providing the wording is clear, the entry can be taken as authority to make a supply as take home medication. In this Health Board the prescriber is required to state that the patient is to be discharged on the medication as written of the administration chart. Providing the entry fulfils the requirements the details can be transposed onto an order form, to be used in pharmacy to prepare the take home medication. It is good practice for the transposition to be carried out by a pharmacist. By carrying out this transcription the pharmacist is not prescribing as the original written direction to supply was made by a practitioner. For discharge prescriptions transcribed by a pharmacist see 8.6.3. A PSD can also be used in clinic settings where the patient is known prior to presentation. The assembly has not issued any further guidance on either of these patient specific documents. However, it is expected that the information contained in these documents to be sufficient to ensure that patient safety is not compromised. Until guidance is issued, it is considered that the information required for a PGD fulfils this criterion, in which case the addition of the patient’s details (i.e. name, address), the doctor’s signature and date of the PGD document may be sufficient to convert the document to a PSD. When a number of patients may be attending a practice for the same treatment e.g. travel vaccination clinic, then a list containing details of the patients expected, signed and dated by a doctor, could be attached to the appropriate PGD thus
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 28
converting the document to a PSD. Services wishing to draw up a PSD should contact the Pharmacy Department for advice and support.
10.1 Patient Specific Protocol
A written statement defining the management of a named patient, which has been agreed by the clinician responsible for the patient and by other appropriate health professionals.
11 PHARMACY DEPARTMENTS
11.1 Responsibility
The Chief Pharmacist for the Health Board has responsibility for establishing and maintaining systems for medicines management (including the safe and secure handling of medicines) and the operation of a suitable IT system in the Health Board in consultation with appropriate members of the medical, nursing and administrative staff. He or she may delegate certain duties but the responsibility will remain with the Chief Pharmacist. There must be written procedures for all aspects of handling medicines within the Health Board’s pharmacy departments. These must describe safe and secure systems of work and comply with standards issued by the Department of Health, the Welsh Assembly Government, all-Wales Chief Pharmacists’ Committee, Professional Bodies and the Health Board Policy “Medicines Management Code of Practice” Pharmacy department premises may be registered with the Royal Pharmaceutical Society. The Chief Pharmacist will be named as the superintendent pharmacist. All pharmacy staff must undertake continuing professional development and training that is aligned to clinical governance requirements and those of the relevant professional body. Records of training must be maintained.
11.2 Security
The physical security of each pharmacy department must comply with accepted standards. They must be intruder alarmed and doors must be fitted with security locks. All doors must be locked and windows shut except when the department is open for business. Intruder alarms must be kept in good working order, tested regularly and linked to the switchboard, police or agreed centre.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 29
Only pharmacy staff authorised by a department’s senior pharmacist may have access to a pharmacy department. A qualified pharmacist must be present whenever the pharmacy is open. Schedule 2 and 3 Controlled Drugs must be stored in locked secure cupboards or rooms to approved standards. Small working stocks will also be kept secure within the Aseptic Services area and Quality Control. Appropriate precautions (see COSHH reference data) must be taken by staff handling medicinal products especially those that are hazardous to health by any route (e.g. inhalation, ingestion, absorption).
11.3 Purchasing of Medicinal (and other) Products
All aspects of medicinal products, manufactured, purchased, used or supplied by the Health Board must comply with good manufacturing and laboratory practice. The purchasing of medicinal products must be under the control of a pharmacist. The range and quality of medicinal products held by a pharmacy department should reflect the current policy of Gwent Partnership Medicines and Therapeutics Committee (GPMTC) and Prescribing Advisory Group. Everything must be ordered in accordance with the Health Board Policy for Standing Orders, Tendering and Contract Procedures and Standing Financial Instructionsvii and the pharmacy department’s stores procedures, meeting the highest standards of accounting and stock handling practices. Orders of medicinal products must be in writing on a Health Board pharmaceutical computerised order form and signed by a pharmacist. Medicinal products must be received by an authorised person directly into a pharmacy department and checked against the delivery note. Any discrepancies must be promptly reported to the supplier for investigation. Invoices for medicinal and pharmaceutical products will be authorised for payment by pharmacy staff. Records of purchases, receipts and issues must be retained for the period necessary to comply with legislation including the Consumer Protection Act 1987viii. Delivery notes must be retained for two years.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 30
11.4 Manufacture of Medicinal Products
The standards set out in “Rules and Guidance for Pharmaceutical Manufacturers and Distributors, 2007 The Orange Guide updated”ix must be met whether medicinal products are prepared on a small or large scale. There must be written procedures for manufacturing and extemporaneously dispensing medicinal products. Procedures and processes must be regularly reviewed, updated and validated. Quality Assurance must be part of production processes and where appropriate there must be quality control testing. Staff engaged in manufacturing and dispensing must be appropriately qualified and trained. The manufacturing areas of the pharmacy department undertaking batch production will hold a special licence issued by the Medicines and Healthcare Products Regulatory Agency (MHRA).
11.5 Storage of Medicinal Products within Pharmacy Departments
Medicinal products within the pharmacy department must be stored under approved conditions under the control of a pharmacist. Schedule 2 and 3 Controlled Drugs must be stored in locked secure cupboards or rooms to approved standards. See Policy for the Management of Controlled Drugs1. Only authorised personnel will be allowed unaccompanied access to storage areas. Discrepancies in controlled drugs and other significant stock discrepancies must be reported immediately to the senior pharmacist on duty who will take appropriate action in accordance with the pharmacy department’s procedures and the Health Board’s Standing Financial Instructions7. The Chief Pharmacist must be notified at the earliest opportunity. Minor stock discrepancies must be reported in the first instance to the pharmacist or technician responsible for purchasing and any unresolved discrepancies reported to the pharmacy manager who will take appropriate action in accordance with the pharmacy department’s procedures and the Health Board’s Standing Financial Instructions8.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 31
Records must be maintained of all transactions involving the receipt and issue of medicinal and other products to enable reconciliation of stock. Stock checks should be carried out at intervals agreed with the Finance Department. (See also Section 25 - Storage and Transport of Medicinal Products)
11.6 Supply of Medicinal Products
11.6.1 Authorities under which a supply may be made:
• A written prescription of a medical or dental officer, or other authorised prescriber (see 8.1) for inpatients, outpatients attending a hospital or Health Board clinic. Patients cared for by the GPOOH service will be issued with WP10 prescriptions to be dispensed at community pharmacies. When the patient is unable to access a community pharmacy, e.g. late at night, then the prescription will be dispensed at the Out of Hours centre using overlabelled patient packs supplied by the hospital pharmacy.
• An order for discharge medication transposed by a pharmacist, or
under the direct supervision of a pharmacist, from a clearly written entry by a doctor on a patient’s prescription and administration sheet.
• A written requisition signed by a qualified nurse in charge of a ward or
department or signed by a member of the pharmacy team for use as stock for administering to patients on a ward or department. The requisition must only request the supply of a medicine on the approved stock list for that ward/department.
• An order generated at ward level by pharmacy staff, for the supply of
named patient medication for bedside lockers.
• A written requisition signed by a dentist, qualified nurse or midwife in community clinics for use within the clinic.
• A Midwife’s Supply Order (for use in the community) authorised by
the Supervisor of Midwives to be kept as stock securely stored for community midwives.
• A prescription written by a doctor or non medical prescriber for
administration to patients by Community Psychiatric Nurses.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 32
• A written requisition signed by a nurse in charge of a Primary care Centre (PCC) for use in the GP OOH Service.
• A requisition signed by an authorised person for items on an agreed
list of products for special areas e.g. Ambulance Service, Major Accident Kits, Emergency Cupboards and Emergency Kits.
• A written requisition signed by a physiotherapist, podiatrist or other
similar professional when the medicinal product requisitioned is one that they are entitled to possess under the regulations made under the Medicines Act 1968 (as amended)3.
• A signed order for the sale or supply to another person or institution
whose purpose in acquiring the medicinal product is to sell, supply or administer it to others in the course of their business or professional practice.
• A retail sale to a member of staff or the public of General Sales List
(GSL) and Pharmacy (P) medicines.
• WP10 and WP10 (HP) prescriptions are not to be dispensed by the hospital pharmacy unless prior authority is received from the senior pharmacist on duty. The appropriate community pharmacy must obtain the medicines for the patient even if it is via the hospital pharmacy in exceptional circumstances.
11.6.2 Telephoned and faxed orders Medicinal products must only be supplied against a telephoned order/requisition in exceptional circumstances and when it is not possible for the order to be transmitted by fax. Telephoned order/requisitions must be confirmed in writing without delay. Faxed requisitions for controlled drugs will be accepted when urgently required for the relief of pain but the requisition must comply with the Policy for the Management of Controlled Drugs. (CD orders for Temazepam are not considered urgent). The original order should be forwarded, within 24 hours to the pharmacy by first class post.
11.6.3 Supply records Orders/requisitions for medicinal products supplied by the pharmacy department must be retained in the pharmacy department for two years.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 33
Prescriptions must be retained for a period of two years and in the case of chemotherapy prescriptions should be retained for two years after the last chemotherapy treatment. Recommendation for the requisite time for retention of records pertaining to the pharmaceutical service will be attached as appendix when approved by the Welsh Chief Pharmacists Committee.
11.7 Dispensing quantities to be supplied
All dispensing activity within the pharmacy must be supervised by a pharmacist and under her/his personal control. Pharmacy accredited checking technicians may undertake checking procedures as stipulated in the standard operating procedures. Patients on wards receiving a Patient Orientated Medicines Service will, where appropriate, receive an original pack on admission labelled ready for discharge, which will be used on discharge. No patient should be discharged with less than seven days supply of medicine making additional allowances for intervening Bank Holidays or special circumstances of a patient. Where an original pack has not been supplied on admission labelled for a specific patient or less than seven days supply remains at discharge, then a patient pack – to last 28 days will be supplied at discharge. Patients in community hospitals will receive an original pack on discharge. Where monitored dosage systems are used, one weeks supply may be deemed appropriate. Patient packs will be supplied against outpatient prescriptions. A pharmacist may authorise the supply of a patient pack if it is appropriate. Prescriptions for a course of medication such as an antibiotic, infertility treatment, contraceptive or steroid reducing dose will be dispensed in full. A larger quantity may be authorised personally by a consultant but only in exceptional circumstances would a patients receive more than 28 days supply. To minimise the potential for waste, pharmacy departments will not usually supply more that 28 days supply of medicines at any one time. Doctors and dentists using WP10HP prescriptions should prescribe a maximum of 28 days medication except for courses such as antibiotics.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 34
11.8 Labelling of Medicinal Products
The containers and packages of medicinal products supplied or sold by the pharmacy department must be labelled in accordance with the Medicines (Labelling) Regulations 1976x, as amended. Those medicinal products that are also fully Controlled Drugs must be labelled in accordance with the Misuse of Drugs Regulations 1985, as amendedxi. The labels on containers of medicinal products must be computer generated or typed. Schedule 2 Controlled Drugs, plus temazepam, diethylpropion, buprenorphine, and flunitrazepam supplied for use within a hospital or clinic must be labelled “Store in a Controlled Drugs Cupboard” together with the name of the ward or department receiving the supply, and the date of the supply. Schedule 3 and 4 Controlled Drugs supplied for use within a hospital or clinic must be labelled “Store in Security Cupboard” except for temazepam, diethylpropion, buprenorphine and flunitrazepam, which must be labelled “Store in a Controlled Drug Cupboard”. In exceptional circumstances when it is necessary to refrigerate a Controlled Drug it should be labelled “Controlled Drug Store in a Refrigerator,” the refrigerator must be locked. Cytotoxic drugs supplied for use within a hospital or clinic must be labelled “Cytotoxic Handle with Care”.
11.9 When pharmacy departments are closed
Each pharmacy department has a locked Emergency Drug Supply Room/Cupboard separate from the department. Hospitals without pharmacy departments have Emergency Drug Cupboards. The senior nurse on duty in the hospital should be contacted to gain access to the Emergency Drug Supply Room/Cupboard. The keys should only leave the possession of the senior nurse in exceptional circumstances. The senior nurse on duty may enter or remove medicinal products from an Emergency Drug Supply Room/Cupboard.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 35
A record must be made of each visit to the Emergency Drug Supply Room/Cupboard in the record book kept in the room/cupboard, whether or not anything was removed. A record of all medicinal products taken (and any that are needed but not found) must be made in the record book. This is vital to ensure that the Emergency Drug Room/Cupboard is kept correctly stocked. The room or cupboard must be re-locked after obtaining the required supplies. (Also see Appendix 5 - Action to be taken outside of pharmacy hours.)
11.10 Ward Clinical Pharmacist Responsibilities
Each ward/patient area will have an allocated pharmacist responsible for the pharmaceutical care of patients. (Where a pharmacist is aligned with a medical team, then the pharmacist will be responsible for the pharmaceutical care of all patients under the care of that team irrespective of the ward area). They will undertake “rounds” on that ward at a frequency appropriate for the acute or long stay nature of the ward. The care will involve: i) Working through other health care professionals to ensure medication use is
both safe and effective by: • Ensuring patients medicines on admission are reconciled. • Ensuring doses and drugs are appropriate for the patient and
condition. • Ensuring drugs are supplied through safe and appropriate systems. • Ensuring appropriate information is available to aid the prescribing
and administration of medicines. • Being available via a bleep or through the pharmacy department to
deal with specific queries. • Documenting their care.
ii) Working with the patient to ensure understanding and concordance with their
medication.
11.11 Controlled Stationery
Controlled stationery is any stationery, which could be used to fraudulently obtain medicines including requisition or order books, prescription charts, controlled drug order books and in particular, blank prescription forms. Controlled stationery must be properly accounted for.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 36
Wherever controlled stationery is kept in the Health Board, it must be held in a secure location. Its receipt and issue must be controlled in a way that provides an audit trail. Once issued, controlled stationery is the responsibility of the authorised person to whom it is issued. This person must make appropriate arrangements for the secure storage of these items. Suspected or actual loss or theft of any controlled stationery must be reported immediately to the person in charge of the ward or department and to the senior pharmacist on duty. The latter will inform the Pharmacy Manager and Chief Pharmacist as soon as possible. Controlled stationery should be pre-printed and serially numbered where possible. An Incident Report form should be completed in the event of suspected or actual lost of any controlled stationery. Suspected or actual loss or theft of WP10 pads/prescriptions used by the GP OOHs Service should be reported to the Associate Medical Director, Primary Care or the Clinical Director of OOH.
12 ORDERING STOCK DRUGS AND PHARMACEUTICALS (ACUTE AND COMMUNITY)
12.1 Responsibility
The sister or acting sister of each ward, department, or theatre is responsible for all aspects of the control and security of medicines within their area and must ensure that this policy is followed. Duties may be delegated but accountability remains with the sister or acting sister. Dentists and podiatrists have similar responsibilities in their community clinics. Medicinal products may only be supplied or administered in accordance with this policy. Health Board employees must not take medicinal products supplied to wards, departments and theatres for their personal use, or another employee’s use, unless the product has been supplied in a first-aid kit for employee first aid. A medicinal product may only be issued to a patient to take out of the hospital it if has been supplied and labelled as a discharge medicine by the pharmacy department unless a written protocol has been agreed by the Chief Pharmacist to cover special circumstances.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 37
Samples of medicinal products must not be left in wards, departments, theatres or clinics. Appropriate precautions (see COSHH reference data) must be taken by staff handling medicinal products especially those that are hazardous to health by any route (e.g. inhalation, ingestion, absorption).
12.2 Stock Medicines
In hospitals, stock medicines are those that are in routine and sufficiently frequent use to warrant being available prior to being prescribed. Nursing staff should be familiar with their use. Stock medicines will reflect the speciality of the ward. The nurse in charge of each ward/department and the clinical pharmacist/pharmacy technician for that area will agree a list of items to be kept in stock by the ward/department. Dentists and podiatrists have similar responsibilities in their community clinics. The ward/department/clinic and the pharmacy department must each keep a copy of this list. Adequate stocks should be ordered and kept for the day to day running of the ward/department/clinics. Medicinal products with the earliest expiry date must be used first.
12.2.1 Revision of stockholding The stock holding should be subject to continuous assessment and evaluation by the clinical pharmacist, pharmacy assistant technical officer with responsibility for that ward and the nurse in charge. The nurse in charge, the clinical pharmacist and the pharmacy technician should review and agree the total stock holding on a regular basis. This should be not less than twice a year. The revised stock holding should be based on the computer-generated data of drugs issued to the ward. In the community, medicines may be held as stock at community bases and in clinics. Community nurses may hold a very small working stock. The arrangements for clinics will be the same as for wards except that the community services pharmacy technician/ATO will carry out the stock review in conjunction with the pharmacist responsible for community clinics. This review will need to be done annually.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 38
12.2.2 Ordering stock drugs and pharmaceuticals Medicinal products (including Schedule 4 and 5 Controlled Drugs) and other items supplied by the pharmacy department may be ordered by the nurse in charge of a ward/department/clinic from the pharmacy department or supplied as part of the pharmacy department’s “topping-up” service. a) Orders by nursing staff
• Stocks for controlled drugs must be ordered using the Controlled Drug requisition book. See Policy for the Management of Controlled Drugs1.
• If a top-up service is not in place then an order for stock medicines must be made using the ward requisition book. Any spare space on the order should be crossed out to prevent unauthorised additions and the order signed by a nurse.
• In the community and in some acute hospital departments, stock medicines obtained from pharmacy must be ordered using the approved, pre-printed stock list. Any additional orders must be written in the ward requisition book.
• Telephone orders: - These are only accepted in an emergency. - They must be given by the nurse in charge. - They must give full details of the stock medicine required. - They must be followed up by a written confirmation order
endorsed “Confirmation Order”.
12.2.3 Top up by Pharmacy Staff The pharmacy will provide each ward/department or primary care centre in the GPOOH service, with the details of the servicing arrangements applicable to that ward. These details will include the frequency of the top-up service (e.g. the usual service days and times) and the names of the usual pharmacy staff member assigned to service that ward. There will be an annual review of the servicing arrangements. A signature from the nurse will not be required where a top up service is in place. In most instances there will be no requisition to sign, as bar code and data pens will collate the ordering data.
12.2.4 Delivery Medicines may be carried for delivery by any authorised hospital employee. They must never be given to patients to deliver.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 39
12.2.5 Receipt of Medicines All areas receiving medicines should have a designated place for the receipt of stock and where applicable, dispensed medicines.
i) Medicines requiring refrigeration - medicines requiring refrigeration will have their outer transport containers suitably labelled. These must be unpacked immediately and placed in the locked medicine storage refrigerator.
ii) Receipt of stock via Pharmacy top-up - A member of nursing staff will
check the stock issued through the pharmacy top-up system onto the ward
iii) Issue note - All stock issues made by pharmacy will be accompanied by a
copy order or issue note, which will include details of the quantities of items issued and the date of issue.
iv) Receipt of Stock ordered by nurses - Where nurses order stock issues
separately the receiving nurse must check the supply against the copy order or issue note.
v) Discrepancies - Any discrepancies must be reported immediately to
pharmacy. This report should be made to the pharmacy technician who is responsible for stock issues from the pharmacy store area.
If a stock issue matches with the copy order or issue note then the checking nurse should sign and date the issue note. This issue note, which is part of the Ward Order Book, must be retained for 12 months, i.e. the Ward Order Book must be retained on the ward for 12 months after its last entry.
vi) If medicinal products are damaged upon receipt contact the pharmacy,
who will advise on their safe handling and return.
12.2.6 Lending/borrowing medicines
i) Medicines must be obtained from the appropriate hospital pharmacy department when pharmacy is open. Medicines must not be lent/borrowed from other wards other than in an emergency or under exceptional circumstances and with the agreement of the pharmacy.
ii) When the pharmacy is closed it may be appropriate to lend/borrow
medicines. If the drug is not available in the emergency room/cupboard.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 40
iii) When lending and borrowing takes place the details of the medicine transfer should be recorded in the donor ward medicine order book and countersigned by a nurse on the receiving ward.
iv) If a ward is unable to locate a medicine outside pharmacy opening hours,
the emergency duty pharmacist should be consulted. They may know about stock shortages, know the best place to borrow from and then will be able to rectify stock balances on the next working day. The emergency duty pharmacist becomes part of an audit trail. This can protect the lending ward in the event of discrepancies and an investigation.
v) Only in exceptional circumstances can Controlled Drugs be lent or
borrowed. See Policy for the Management of Controlled Drugs.
12.3 Ordering Controlled Drugs
See policy – Policy for the Management of Controlled Drugs1.
13 STORAGE OF MEDICINAL PRODUCTS
(See also Section 25 - Storage and Transport of Medicinal Products.)
13.1 Stock holding
The range and level of drugs held as stock should reflect current prescribing and usage trends. The stock holding should be the minimum for safe and effective patient treatment and efficient service provision. Storage of drugs no long in use increases risk of error. Medicinal products received by wards and departments must immediately be placed in the appropriate locked cupboard, locked patient’s own medicines locker, locked trolley or locked refrigerator (with the exception of emergency drug boxes).
13.2 Inspection of drug stocks
A pharmacist may inspect all drug stocks on any Health Board premises at any time.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 41
13.3 Medicinal Products
Medicinal products must be stored in a designated locked cupboard (which may be an individual patient’s medicine locker) or locked refrigerator. All these storage areas must be adequately maintained, kept clean, well ordered and comply with current legislation. It is good practice, where possible, to store preparations for internal and external use in separate cupboards. If it is not possible to use separate cupboards then discretely separated parts of the same cupboard may be used with external medications being stored below internal medications. Large volume infusion fluids, irrigation fluids and sterile topical fluids should be stored in safe locations that are as secure as practicable. Flammable material must be stored in locations approved by the fire officer, preferably locked. Disinfectants must be stored separately, preferably in locked cupboards.
13.4 Refrigerated Storage
Medicines must be stored under suitable environmental conditions. Medicines requiring to be kept in refrigerators or freezers will be labelled accordingly. Refrigerators and freezers used for storing medicines must be lockable, kept locked and be exclusively used for that purpose. Medicine refrigerators and freezers must be hard wired to the electrical supply to prevent accidental switching off. The use of fridges with temperature chart recorders is preferred. Medicine refrigerators and freezers must have the temperature monitored daily and recorded. The nurse in charge is responsible for ensuring that there are arrangements for monitoring and these are subject to regular audits.
13.5 Medicine Trolleys
Medicinal products in current use, except for Schedule 2 Controlled Drugs, and temazepam, buprenorphine, diethylpropion and flunitrazepam, may be kept in a medicine trolley.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 42
The trolley must be kept in a locked cupboard or room, secured to a solid surface by means of an anti-theft device, when not in use.
13.6 Emergency Medicines
Emergency drug boxes should not be stored in locked receptacles and must be located in areas known to all who may be required to use them, but secure from patients and others. Each container must be sealed and once the seal is broken, it must be exchanged as soon as possible for a new sealed container from the pharmacy department or the hospital’s emergency drug supplies room/cupboard.
13.7 Patients Own Drugs
In hospital the term “patients own drugs” refers to either, prescribed medicines and medicines brought in from outside by the patient, or dispensed for the patient by the Health Board pharmacy as part of Patients Own Drugs System (PODS). Patients’ own drugs, which have been used as part of the PODS are normally stored in lockable bedside medicine cabinets used exclusively for this purpose. The storage and use of patient’s own drugs are covered by procedures that have been approved by the Health Boards Clinical Forum.
Where a PODS service is not in use the patient’s own drugs are normally returned to the patients’ relative or carer.
Hospital staff should discuss with patients on admission the possibility that their medication needs may change during their hospital stay. This may result in some current medication being no longer required. Staff should inform the patient of the potential risks and that the hospital has facilities for the safe disposal of medicines no longer required, see section 17.3.
13.8 Unlawful Items – Drugs, etc
The Health Board has a duty under the Misuse of Drugs Act 198511 as amended, to ensure its premises are not used for the illegal supply, use or possession of any controlled drug or illicit substance. If a patient is suspected of being in possession of illegal substances the nurse-in-charge should ask the patient to surrender the items voluntarily.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 43
For safety of staff, patients should not be confronted in a side room away from the main part of the ward but neither should they be confronted in the main part of the ward at visiting time; if they are in bed then the curtains should be drawn around to afford them some privacy. Other members of staff should be aware of the situation and be on hand to assist if required. The patient should be advised that if they have a drug problem then the appropriate help can be accessed. If possession is denied but the nurse-in-charge is sure of possession they should ask the patients permission to check their property. This should be done with another member of staff as witness. Care should be taken in case the patient becomes aggressive and to avoid needle stick injuries from hidden syringes. If the patient refuses permission to have property checked, staff should:
• Inform the patient that the Health Board under the Misuse of Drugs Act does not allow the possession or use of illegal substances on hospital premises.
• Consult with their Nurse/Unit Manager with reasons for suspicion and patients response.
• Note in clinical file staff suspicion and advice given to the patient. • If agreed with the Nurse Manager and/or Medical staff, the police may
be contacted with their suspicion that the patient possesses and/or is using suspected illegal substances.
If the patient is unconscious or otherwise unable to hand the item over, the staff should remove the item and complete a disclaimer form with a note that the patient was unconscious at the time of removal. (See appendix 9). Any suspected illegal substances handed to or found by staff should be noted in the clinical file. The substance should be disposed of by flushing down the toilet in the presence of a witness and noted in the clinical file. Nursing staff should refer to the Health Board policy, Searching of Patients and their Property within Mental Health and Learning Disability Settingsxii. School nurses, presented with a similar situation, should work to local school policy, report the incident to the Community Services Manager and complete an incident report form. The nurse must not personally take unidentifiable/possibly illegal substances to a police station.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 44
14 GENERAL SECURITY
All medicines and pharmaceuticals must always be stored in a locked cupboard, locked bedside locker or a locked trolley. The nurse in charge will hold the keys. The patient may hold the key to their own individual bedside medicines cabinet, where they have been assessed as appropriate and have agreed to participate in the self medication programme. Certain pharmaceuticals, such as bulk sterile fluids, may be stored in areas other than locked cupboards. In the case of community staff, drugs must be stored in a secure, lockable bag. If the key of a medicines cupboard of fridge in which medicines are stored goes missing then the senior manager should ensure an incident form is completed and consider if necessary the option of changing locks. The senior pharmacist on duty should be informed.
14.1 Health and Safety
The storage of some pharmaceuticals has Health & Safety considerations that must be met (e.g. medical gas cylinders). Flammable material must be stored in locations approved by the Fire Officer and preferably locked. Disinfectants should be stored separately, preferably in locked cupboards.
14.2 Custody of Medicines Cupboard Keys
Medicine cupboard and refrigerator keys must be kept in a safe place separate from other ward or department keys. The keys for the controlled drug cupboard are the responsibility of the nurse in charge (in theatres, this may be the operating department practitioner (ODP) in charge). They may be passed to a registered nurse (or ODP) in order for them to carry out their duties and returned to the nurse in charge. If the keys for the controlled drug cupboard go missing the locks must be changed and pharmacy informed and an incident form completed. See Policy for the Management of Controlled Drugs1. The controlled drug cupboard keys should be kept separately from the main body of keys. Except in exceptional circumstances medicine cupboard keys should not leave the ward or department if it is necessary the nurse in charge should arrange for the keys to be held in a neighbouring ward or department by the nurse in charge.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 45
A second set of keys must be kept in a secure place but accessible to a senior nurse on duty 24 hours a day. In dental clinics a second set of keys must be held in a suitable safe accessible to the senior manager 24 hours a day.
14.3 Bed Side Medicine Cabinet Keys
Keys for individual bedside medicine cabinets should be stored with medicine cupboard and refrigerator keys. A master key for bedside medicine cabinets is held by each team on the ward and handed back to the nurse in charge at the end of the shift. Individual patients who have been approved for self-medication may hold the individual key for their bedside medicine cabinet. The secure holding of a bedside cabinet master key is essential. If one is lost or stolen it must be reported immediately and the appropriate incident form completed. Appropriate pharmacy staff also hold a master key when they are working on the ward which is returned to pharmacy when their ward work is completed.
14.4 GP Out of Hours
For GPOOH PCCs the keys to medicines cupboards will be held by the sister/nurse in charge on designated wards at designated hospitals. Hand over of keys must be supported by a signature and audit trail for the movement of keys between the ward and the GPOOH PC.
14.5 Drug and Pharmaceutical Samples
It is imperative that the Health Board knows what products are being used within the organisation and that they comply with all legislation. The policy of the Prescribing Advisory Group is that medicine samples or samples of other pharmaceuticals must not be left for use in the Health Board by representatives of manufacturers or suppliers.
14.6 Action to be taken in the Event of a Stock Discrepancy
For controlled drugs see the Policy for the Management of Controlled Drugs1. Any apparent discrepancies in the stock of medicines including controlled drugs must be reported to the nurse in charge and the senior pharmacist on duty for the hospital. When pharmacy is closed any discrepancy must be reported to the emergency duty pharmacist.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 46
The Chief Pharmacist must be informed at the earliest opportunity. All discrepancies must be reported to and investigated by the nurse in charge, senior nurse and Chief Pharmacist or nominated member of pharmacy staff.
15 ADMINISTRATION
Only registered nurses, midwives, health visitors, doctors, dentists and other healthcare professionals with appropriate and valid dispensations may administer drugs. All employees administering medicines to patients will be held individually accountable for their actions/omissions. When administering medical products nurse, midwives and health visitors act within the framework of current legislation and in accordance with the NMC, Code of Professional Conduct: Standards for conduct, performance and ethics, 2004, and the NMC Guidelines for the Administration of Medicines, Aug 2004xiii. She/ he also acts in accordance with the relevant policies of the Health Board. Other healthcare staff, e.g., health care assistants and student nurses may have a support role in the administration of medicines, under direct supervision of a nurse who is accountable for the administration process. If an error occurs in the administration of medication to a patient the consultant/ dentist who has responsibility for the care of the patient, the nurse in charge of the ward/department and the Senior Nurse must be informed immediately. An incident form must be completed and, at an appropriate time, the patient must be informed. Only medicinal products that have been issued or dispensed by a Health Board pharmacy department or a patient’s own medicine may be administered or supplied to a patient. A doctor, nurse or pharmacist must positively identify a patient’s own medicines before they may be administered. Medicinal products may only be administered to a patient:
• In accordance with the prescription written on an approved in-patient form, signed and dated by an authorised prescriber.
• On the verbal instruction of a doctor or dentist who is present with a
patient in the case of a cardiac arrest or similar emergency.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 47
• By a person working under a Patient Group Direction.
• On the verbal instruction of a doctor for a medicine previously
prescribed for that specific patient. See 15.17 – Verbal instructions to administer.
• In exceptional chases in community hospitals where a medicine is
required urgently and the on call doctor is unable to attend (and the criteria for a verbal order does not apply) the on call doctor may fax an administration chart to the appropriate ward. The medicine prescribed on this additional administration chart should be crossed off and rewritten on the main administration chart (B) by the next visiting doctor to avoid confusion and errors with the use of two charts. The original additional administration chart should be sent as soon as possible in the internal mail and matched with the faxed administration chart (A). If the prescribed medicine is transferred to the original chart (B) then both the faxed chart (A) and the original copy (C) should be filed in the patients notes.
• Patients or carers may administer medicines under the self-
medication arrangements. A record of all medicinal products administered to a patient must be made on the appropriate, approved prescription and administration record sheet. In clinics patients’ records are used as the prescription and administration record sheet.
15.1 Nurse Procedure
In hospitals other than the procedures listed below as a being a two nurse procedure, drug administration is normally a single nurse procedures, with the exception of paediatrics.
• The reconstitution of dry injectable powders into an injectable solution.
• The selection and mixing of drugs in syringes or infusion bags. • All parenteral drug administration (IV, IM, SC, epidural). • All administrations to neonatal/paediatric patients. • All cytotoxic drug administrations (by any routes of administration). • All Controlled Drug administrations. • Insulin Injections. • The setting up of pumps for IV administration. • The replacement of drug containing syringes or bags in IV pumps
already set up and use. • Where a calculation is required.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 48
It is best practice that when administering a medicine in a single nurse procedure, that the nurse seeks a check when dealing with medicines they are not familiar with and medicines with complex administration requirements or calculations. IN THE COMMUNITY, the requirement for certain medication administrations to be two nurse procedures does not apply. Controlled drugs and insulin administrations are a one registered nurse procedure, however where a second nurse is available the checking procedure should be undertaken by both. IN DENTAL CLINICS Midazolam for sedation is a single operator procedure given by a dentist trained to give IV sedation.
15.2 Children and Neonates
Any medicines administered to children and neonates must be checked and witnessed by two nurses, one must be a first level nurse. In a dental clinic the administration is a one-person procedure undertaken by a dentist or by a PCD (Professional Complimentary to Dentistry).
15.3 Emergency Administration
The legislation provides that no one may administer a parenteral prescription-only medicine (POM) otherwise than to himself/herself unless he/she is an appropriate practitioner or is acting in accordance with the directions of an appropriate practitioner. There is a list of prescription only injections that are exempt from the POM Regulations for the purpose of saving life in an emergency. The list authorised under the Medicines Act is shown in Appendix 1. Nurses administering Epinephrine/Atropine Intravenously under the scope of this policy (without authorisation from a medical practitioner) must be a current Resuscitation Council (UK) Advanced Life Support Provider. In addition they should have successfully completed the Health Board Intravenous Medication Administration Course or a similar course transferable from another Health Board. See Health Board Policy for the Administration of Intravenous Medicationxiv. The administration of IM Epinephrine for the treatment of anaphylaxis requires nurses/doctors to update themselves routinely in recognition and treatment of anaphylaxis for first responders.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 49
The list shown in Appendix 2 is for a “crash call” situation to save a life. These have been authorised by the Health Board’s Prescribing Advisory Group.
15.4 Measurement and administration of liquid medicines via oral and other enteral routes
In line with NPSA guidelines, an appropriate oral/enteral syringe should be used to measure oral medicines where the use of a medicine spoon or graduated measure cannot ensure accurate measurement and dosing. Medicines spoons (5ml) are appropriate for doses of 5ml or multiples of 5ml. Medicine cups are appropriate for doses equating to 2.5ml, 5ml or more than 5ml in multiples of no less than 1ml. Oral/enteral syringes are appropriate for all doses including doses less than 5ml or doses that include multiples of 0.1ml. Liquid medicines requiring administration via a syringe must only be measured using an oral/enteral syringe. If the administration of the medicine is not one uninterrupted process then the oral/enteral syringe should be labelled with the name and strength of the medicine, the patients name and the date and time it was prepared.- Press-in bottle adaptors or medicines quills should also be used to facilitate the use of oral/enteral syringes for the administration of liquid medicines. Within inpatient areas oral/enteral syringes are for single use only. Any patients discharged from hospital or outpatients requiring liquid medicines should be issued with a 5ml medicine spoon or appropriate oral/enteral syringe, complete with cleaning instructions and a bottle adaptor.
15.5 Administration Check-list of Medicines
Before any medicinal product is administered the following must be checked:
• The patient’s identity: - The person administering the medication must confirm the identity
of the patient before administering the medication. In hospitals, confirmation is undertaken by checking the patient’s wrist band for name, date of birth, address and hospital number.
- In some units, e.g. A & E and Psychiatry, wrist bands may not be used and in such circumstances therefore, other means of patient
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 50
identification must be used to confirm the patient’s identity prior to administration. Details should be specified in a local policy.
- In the case of paediatrics, the identity of the child should be confirmed with the accompanying adult prior to the application of an identity wrist band and then the wrist band checked prior to administering the medication.
• That the patient is not sensitive or allergic to the medicinal product (in hospital patients with a known allergy should wear a red wrist band bearing the patients name, identification number and date of birth).
• That the correct medicine has been selected against the prescription. • The expiry date of the medicine. • The suitability of the route of administration. • Any special instructions are being followed. • Whether any further information is required about the medicine or if
detailed calculations need to be checked. If so the pharmacy department should be contacted.
• The correct medicine must be given in the prescribed dose by the prescribed route and at the required time.
• That the patient has taken the medication and that an appropriate record has been made on the prescription form. The prescription chart should be marked to indicate non-administration as per medication record guidelines. A Clinical Incident form should be completed for non-administration of a medication for more than one dose.
• In the community, prior to administration of medicines the nurse or carer must confirm the patient’s identity. Reasons for non-administration of a drug must be fully documented in the patient’s notes and the GP informed.
If there is any doubt about the legibility of the prescription or any other particulars such as the dose, route, mix of drugs or gases, allergies, time or frequency of administration, the person administering the medicinal product must contact the prescriber or responsible doctor/dentist, prior to administration.
15.6 Administration of Controlled Drugs by Nurses
See separate policy, Policy for the Management of Controlled Drugs1.
15.7 Immunisation and Vaccination
Doctors and Nurses who administer vaccines must ensure they are familiar and competent with the procedure for administration of vaccines and the management for anaphylactic shock.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 51
15.8 Administration Against Pharmacist Amended Prescriptions – Clarification of Roles and Responsibilities
For practical and safety reasons Pharmacists rewrite prescription charts, amend individual prescriptions or transcribe GP treatments onto prescription charts for elective admissions. Any pharmacy alteration will be legible, dated, and identify the amending pharmacist by their initials and / or bleep number. It will specify when appropriate which clinician the amendment was agreed with. Where amendments would decrease readability, the prescription will be rewritten and signed by the pharmacist. The nurse administering the medicine in these situations is authorised to do so without a medical countersignature. A countersignature is no longer needed within 24 hours. Specific examples of acceptable situations include when:
• Telephoned queries produce changes better actioned immediately, rather than leaving a note for later amendment e.g. reducing a high dose.
• An ambiguous prescription is clarified. • Alternative treatment is agreed with prescriber after discussing an
interacting drug. • Prescription chart is rewritten. When this is done the medicines will be
reviewed at same time and any queries discussed with appropriate clinician. Controlled Drugs will be transcribed, but any ambiguities must be discussed with the appropriate clinician.
• Implementing Clinical Forum and Prescribing Advisory Group approved substitution policies.
• Regular medication or strengths are accidentally omitted e.g. eye drops, inhalers, inhaler strengths, topical treatments, clerking omissions due to lack of accurate drug history.
Where actual or potential clinical reasons exist for missing items the item will not be added to chart. If the reason for omission is not documented a note will be left or contact made with the prescriber, depending on the urgency. New items for new needs will not be prescribed, unless done within a locally agreed procedure such as addition of antibiotic or DVT prophylaxis. The pharmacist will not amend anything beyond their experience or competence.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 52
Communication with the prescriber is essential to maintain safety and ensure correct treatment.
15.9 Administration of Medicines to Patients at Home
In the community, patients receiving medication at home should be given their medicines in accordance with the labelled directions and/or documentation provided by the patient’s GP and or community pharmacy. Details of the medicine to be given should be confirmed with the patient/carer before administration.
15.10 Patient Own Drugs (PODs)
In hospitals the Patient Own Drugs (PODS) for medicines’ management offers benefits over the traditional system of mixed stock and dispensed medicines being used by the patient. The Health Board has approved the implementation of PODS. Once the PODS have been assessed at admission by suitably qualified technicians, pharmacists or trained nurses, the patient’s medicines should be stored in lockable bedside locker or drawers used exclusively for this purpose. (In community hospitals PODs can be stored on a medicines trolley suitable for the purpose of segregating medicines for individual patients). The administration of medicines to patients is made in the traditional manner but from the individual supply rather than from the medicine trolley. The procedure for PODS must be followed. Community hospitals will use appropriate agreed procedures which should maintain safe standards of practice. The directions on the prescription chart take precedence over the label on the medication. If there is a discrepancy, nursing staff must inform the ward clinical pharmacist.
15.11 Incident Reporting
It is important that both ‘near misses’ and ‘incidents’ are reported in accordance with the Health Board Policy – Incident Reporting Policy and Procedure24. a) Whenever an incident is discovered or suspected, the first duty of the person
discovering it is to prompt instigation of any remedial action. b) In the acute hospital, if at any time during or following the administration of
medication, it is suspected that an incident has occurred, it must be immediately reported to the nurse in charge and the duty doctor in charge of the patient.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 53
c) In the community, be it in the patient’s home, clinic or community or continuing care hospital, the same standard applies and the event or a suspected incident reported to the Community Services Manager, Hospital Manager and either the Community Doctor or the GP, whichever is appropriate.
Clinical incidents involving medicines should be reported to the Chief Pharmacist either directly or through the ward/team pharmacist.
15.12 Self Medication by Patients and Administration by Non Staff Carers
Certain patients may administer their own medication within the Health Board in order to:
• Help them learn to take their own medication correctly. • Enable them to retain their independence or become more
independent. • Confirm the patient’s understanding and compliance with their
medication regime. When there is any doubt an assessment of the suitability of self-medication programmes for individual patients should be made collectively by the doctor, nurse and pharmacist. If a patient is going to hold and administer his or her own medication, it must be written in the patient’s Care Plan. The prescriber must write the administration instruction on the Prescription and Administration Record Sheet. It is good practice to write “Self-medication” next to the item where appropriate. The ward pharmacist must be involved so that the medication can be dispensed in containers clearly labelled with the patient’s name, the name and strength of the medication, the dose and any other instructions for use. If necessary the patient can be instructed by the pharmacist on the use of their medication. Medicines for self administration will be stored in the patient’s bedside medicine cabinet and the key held by the patient. In certain circumstances e.g. glyceryl trinitrate, the patient may be requested to keep the medication with him/her at all times. During formal drug rounds a nurse will check with the patient that the prescribed medication has been taken and make the appropriate entry on the Prescription and Administration Record Sheet.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 54
When arrangements are made in special care baby units and paediatric wards for other persons e.g. mothers to administer oral medication to patients, the professional staff must provide clear instruction and training and the system must be monitored to ensure that correct doses are administered. Self-medication procedures must be based on a process designed specifically for the circumstances for which they apply (i.e. a procedure for one speciality may not apply in another). Clinical Forum must approve all self-medication procedures. Self-medication procedures must provide for safe, effective treatment for the self-medicating patient and protection for other patients and staff. The procedure must pay particular regard to storage, administration, the documentation of administration and the avoidance of errors arising from incomplete communication.
15.13 Aids to Support Concordance (compliance aids)
The Disability Discrimination Act 1995 requires service providers to make reasonable adjustments to their service so that people with disabilities are able to use it. The Act described a disabled person as “A person has a disability for the purpose of the Act if he has a physical or mental impairment which has a substantial and long term adverse effect on his ability to carry out normal day to day activities”. Long term is defined as at least one year or for the rest of the person’s life. Several adjustments can be made ranging from adjustments to labelling and packaging, providing reminder charts or providing medicines in a compliance aid. If the Health Board is unable to dispense in a compliance aid, a WP10HP may be provided to the patient’s community pharmacist. Contact the ward pharmacist for further information. Self-administration from dispensed containers may not always be possible for some patients. If an aid to concordance is considered necessary, careful attention should be given to the assessment of the patient’s suitability and understanding of how to use an appropriate aid safely. However, all patients will need to be regularly assessed for continued appropriateness of the aid. Ideally, any concordance aid, such as a monitored dose container or a daily/weekly dosing aid, should be dispensed, labelled and sealed by a pharmacist. Where it is not possible to get a concordance aid filled by pharmacy staff, you should ensure that you are able to account for its use. The patient has a right to expect that the same standard of skill and care will be applied by non pharmacy staff in dispensing into a concordance aid as would be applied if the patient were receiving the medication from a pharmacist. This includes the same standard of labelling and record keeping. Compliance aids, which can be purchased by patients for their own use, are aids that are filled from containers of dispensed

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 55
medicines. If nursing choose to repackage dispensed medicines into compliance aids, they should be aware that their use carries a risk of error.
15.14 Complementary and Alternative Therapies
Complementary and alternative therapies are increasingly used in the treatment of patients. Registered nurses and midwives who practise the use of such therapies must have successfully undertaken training and be competent in this area. An authorised prescriber must prescribe homeopathic medicines and treatment must be discussed with the multi disciplinary team prior to commencement. (Please refer to the Code of Professional Conduct). You must have considered the appropriateness of the therapy to both the condition of the patient and any co-existing treatments. It is essential that the patient is aware of the therapy and gives informed consent.
15.15 Administration of Drugs by Midwives
Midwives shall observe, in addition to all current legislation, the rules set out in the current NMC Midwives Rules and Standards, the current NMC Code of Professional Conduct: standards for conduct, performance and ethics, 200413 and any local policies and procedures specified by the Local Supervising Authority or the Supervisor of Midwives. Irrespective of their qualifications/rights to practice in the community, midwives must abide by the Health Board’s policies, procedures, standing orders, patient group directions, and protocols for the administration of medicinal products by midwives when in the Health Board’s hospitals/community. When midwives administer Controlled Drugs in hospital the whole process must be witnessed by a second person. See Policy for the Management of Controlled Drugs1. The administration of medicines to neonates must always be a two-nurse procedure. In the community a practising midwife is authorised to administer certain medicines for their practice according to the regulations of the NMC, Midwives Rules and Standards. For an agreed list of medicines that midwives may carry see (Appendix 7)
15.15.1 Supply of Pethidine for Home Confinements See Policy for the Management of Controlled Drugs1.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 56
(Also refer to Appendix 6 “Issues Relating to Drugs in Patients Homes”).
15.15.2 Administration of Controlled Drugs by Midwives See Policy for the Management of Controlled Drugs1.
15.15.3 Prescription only Medicines The Gwent Local Supervising Authority has agreed a list of Prescription Only Medicines and other medicines to be carried by community midwives (See Appendix 8). The community midwife can order these medicines from a nominated hospital pharmacy on a written requisition. To obtain the medicines, the Supervisor of Midwives must have notified the Pharmacy Department that the midwife is authorised to practice in the area. Midwives working on hospital wards must use the drugs ordered by the ward or department from the Pharmacy Department, not his or her own supplies. Registered midwives may administer parenterally in the course of their professional practice prescription-only medicines containing any of the substances listed in Appendix 8, but no other prescription-only medicines except in accordance with the written instructions of a prescriber or under a Patient Group Direction.
15.15.4 Inhalation Gases All medical gases are to be prescribed individually or an appropriate PGD in operation except for midwives. A practising midwife shall only administer those medicines, including analgesics, in which she has been trained as to use, dosage and methods of administration. A practising midwife shall only administer medicines including inhalation analgesics by means of apparatus if s/he is satisfied that the apparatus has been properly maintained and: • The apparatus is for the time being approved by the Council on a
recommendation of the Board, to enable a particular hospital to investigate a new method of administration.
• The midwife has ensured that the apparatus has been properly maintained. A midwife may administer an inhalation analgesic using other apparatus if instructed to do so and directly supervised by a Registered Medical Practitioner.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 57
To avoid separation of the gases, Entonox cylinders should be kept at a temperature above 10°c and stored horizontally for a period of 24 hours before use. If this is not practicable Entonox cylinders must be maintained at a temperature above 10°c for at least two hours then completely inverted, or place in warm water at body temperature for five minutes and then completely inverted three times.
15.15.5 Audit of Records The supervisors of Midwives should, as part of their duties, periodically audit and reconcile the records of controlled drugs and prescription only medicines kept by each midwife. Any discrepancy should be investigated.
15.16 Management of Errors or Incidents in the Administration of Medicines
Refer to Health Board policy – Incident Reporting Policy and Procedure24.
15.17 Verbal Instructions to Administer
• Medicines should not be administered on telephoned instructions except in exceptional circumstances and then only if the medicine has previously been prescribed for the patient.
• Verbal instructions must not be used for either controlled drugs or intravenous
medicines. • In any circumstance where there is doubt or professional disagreement
regarding a verbal order an appropriate senior nurse or senior member of the clinical team must be consulted.
• The telephoned instructions must be given personally by a doctor or dentist
and must be recorded on a verbal order form by a registered nurse and read back to the medical or dental officer as a double check. The verbal order form must be attached to the patient's prescription and administration sheet until the doctor/dentist has fully endorsed the sheet.
• Ideally a fax or e-mail should be sent to the nurse administering the
medication from the prescriber and this must be attached to the patients prescription chart.
• The nurse taking the verbal order must administer the medicine.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 58
• The nurse taking the verbal message must be familiar with the medicine. • Whenever possible a second nurse should be present when verbal
instructions are received to witness the signature of the registered nurse receiving the instructions.
• The nurse in charge of the ward/department must ensure that the
prescription and administration sheet is fully completed and signed by the doctor/dentist within twenty-four hours in the acute hospital setting.
• In the community hospital setting the doctor giving the verbal order may not
be able to attend the hospital to sign the prescription chart. In these circumstances the doctor giving the verbal order will also complete and sign a verbal order form and send to the ward in the next post. The nurse in charge of the ward must ensure that this signed form is received and attached to the patient’s prescription and administration sheet along with the form completed by the nurse. The next attending doctor, must review the patient’s requirements for this medicine and if appropriate rewrite and sign the medication on the prescription and administration chart within 72 hours of the verbal order being given.
For Verbal Order Form - See Appendix 10
15.18 Patients Detained under the Mental Health Act 1983; Consent to Treatment
Section 58 of the Mental Health Act 1983xv requires that detained patients subject to Section(s) 3, 37, or 48 must after 3 months from the start of drug treatment for mental disorder have given consent to its continuation. This must be affirmed by ensuring that Form 38, or a Certificate of Second Opinion Form 39 is in effect. Nurses administering medicines for the treatment of mental disorder to such patients must ensure that a Form 38 or Form 39 is in effect. This should be checked every time medicines are given, and the nurse gives only those medicines in dosages that accord with the regimen of medication set out in the Form 38 or Form 39 (usually attached to the drug sheet). Emergency drug treatment(s) that may be needed can be prescribed and administered in accordance with the need for emergency care. medicines prescribed for concurrent physical disorders would not be specified on Forms 38 or 39, and although it would not be proper for such medicines to be pressed on an unwilling patient, except in accordance with Section 62 of the Act, it would be improper for such medicines to be withheld because they are not specified on Forms 38 or 39.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 59
15.19 Administration of medicines by the parenteral route
The parenteral route refers to intravenous, intramuscular, subcutaneous and epidural injections. Before giving medicines by the parenteral route, the staff must have the required skills and competence.
15.19.1 Parenteral medicines administration by nursing staff
i) Registered nurses who have undertaken the Health Board’s training programme and achieved satisfactory competence in the administration of parenteral medicines are permitted to administer the first and subsequent doses of a prescribed medicine by this route. Nurses employed from other Health Boards must either provide evidence that they have undertaken and satisfactorily completed an appropriate training programme or they must undertake the Health Board’s training programme and assessment before giving medicines by these routes.
ii) Doctors must administer the first dose of all epidural injections in
neonates and children.
iii) Only registered nurses who have been certificated to administer intravenous medicines and have attended a further course in the administration of cytotoxic drugs will be allowed to administer cytotoxic drugs parenterally. See Health Board policy on Safe Handling of Cytotoxic Drugs, Dec 200816.
iv) Drugs may be administered by either peripheral or central intravenous
lines, by a nurse who has completed the Health Board’s Training Course – Administration of Intravenous Medication. See Health Board Policy for the Administration of Intravenous Medication14. The Doctor must prescribe the most appropriate route when more than one line is present.
v) Drug administration must be signed for on the patient’s prescription chart
by the nurse administering the drug and checked by a second trained registered nurse in accordance with the Aneurin Bevan Health Board Medicines Management Policy
vi) It is the responsibility of the individual nurse to maintain and improve
professional knowledge and competence in relation to the actions and potential complications of the drugs he/she administers.
vii) The nurse must acknowledge any limitations of competence and refuse,
in such cases, to accept delegated functions without having first received sufficient instruction and information to ensure safe practice. Nurses
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 60
should not administer any drug which they do not feel confident in giving but should ask a more experienced colleague or doctor to perform the administration.
viii) The method of drug administration must comply with either the:
• Manufacturer’s instructions as described in the Summary of
Product Characteristics, or; • Current edition of “Medicines for Children”, or: • Any specific drug administration guidelines produced by
pharmacy. Any administration deviating from one of these defined methods should be specifically prescribed and carried out by medical staff.
i) Reconstituted drugs supplied by the pharmacy CIVAS unit should be used wherever possible.
j) The administration of BOLUS injections of controlled drugs by nursing
staff is restricted to specialist areas where continuous monitoring is possible, e.g. SCBU.
k) The guidelines are not exhaustive but are to be followed in conjunction
with the:
• NMC Code of Professional Conduct, June 2002. • NMC Guidelines for the Administration of Medicines (Revised),
April 2002. • Manufacturer’s Instructions.
Nominated radiographers trained in accordance with the Health Boards radiological procedures may administer intravenous Frusemide for diagnostic purposes when it has been prescribed. Doctors must administer the first dose of all intravenous injections in neonates and children and the first doses of all epidural injections. In all other administrations of parenteral injections the nurse can administer the first dose. Appropriately trained dentists may administer IV Midazolam for dental patients undergoing sedation in community clinics.
15.20 Administration Using Infusion Devices
Before using any infusion device the nurse must be confident that they have the required knowledge skills and competence in the selection and use of the
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 61
pumps and syringe drivers. All nurses who have not covered the theory during a pre registration course will be expected to undertake specific training and be able to demonstrate their competence. Newly qualified nurses and nurses who use infusion devices infrequently must maintain their familiarity with infusion devices and associated equipment. In the event of a doctor using infusion devices they must also work to the standards and guidance set out above.
15.21 Administration of Cytotoxic Drugs
The preparation, handling, administration and disposal of cytotoxic products must comply with recommendations issued by the WAG and the Health Board’s policy on Safe Handling of Cytotoxic Drugs, Dec 2008xvi. A further procedure deals specifically with the safe administration of Intrathecal Cytotoxic Drugs because this route is associated with exceptional risk. (Safe Prescribing, Dispensing and Administration of Intrathecal Chemotherapy Policy, Dec 2008xvii.
For parenteral therapy specially designed prescription forms for each individual treatment regimen are the preferred option in the Health Board, each being approved by the Prescribing Advisory Group. If regimen specific forms have not been developed for a particular treatment, then a standard cytotoxic prescription form can be used as an alternative. Oral cytotoxic therapy can be prescribed on the standard inpatient or outpatient prescription forms but only in the context of a written protocol and treatment plan. The Pharmacy Department Cytotoxic Reconstitution Service should always be used in preference of reconstituting cytotoxic products in wards or departments.
15.22 Adverse Drug Reactions
All untoward reactions must be reported to the doctor and ward clinical pharmacist and a note made in the Nursing Record and Medical Record and on the prescription chart. The doctor or ward clinical pharmacist should initiate a Committee for Safety of Medicines (CSM) Yellow card report, when appropriate. Nurse Prescribing – If a patient reports a severe or unexpected reaction to a prescribed medicine it should be reported immediately to the GP by the nurse. The Yellow Card Adverse Reaction Reporting Scheme is a voluntary scheme through which doctors notify suspected adverse reactions to medicines. It is for the GP to decide, following discussion with the nurse, whether to submit a Yellow Card to the Medicines and Healthcare Products Regulatory Agency (MHRA)/Committee on Safety of Medicines.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 62
15.23 Medical Gases
All medical gases used in the Health Board are licensed medicines. They are subject to the Medicine Act and must be treated in the same way as any other medicines. Before a medical gas is administered to a patient, written authority from a prescriber must be obtained. This authority must include the name and concentration of the medical gas (where appropriate), the method of administration and the rate of flow. This can be achieved by:
• An in patient prescription for an individual patient. • A PGD authorising the administration of a medical gas in an
emergency. A practitioner administering a medical gas to a patient must make a written record that treatment with the particular medical gas has been initiated on the prescription chart (or in the patient’s notes for dental patients). In dental clinics Nitrous Oxide and Oxygen are only administered by a dentist who has undertaken further specific training and continue to undertake a recognised minimum number of procedures per annum. The storage of medical gases should follow the advice of the Health Board’s Quality Control Pharmacist and the Health Boards Health and Safety Department. All cylinders and regulators should be routinely tested.
16 NON AVAILABILITY OF A MEDICINE
The Pharmacy department will inform the ward and where possible the prescriber if a medicine can not be supplied by pharmacy.
17 DELAYED OR OMITTED MEDICINES
On some occasions medicine doses are omitted or delayed in hospital for a variety of reasons. While often these events may not seem serious, for some critical medicines or conditions, delays or omissions can cause serious harm or death. The NPSA, in consultation with stakeholders have produced the following lists of drugs whose timely (plus or minus two hours of the prescribed time on the inpatient chart) administration is considered to be critical. They are as follows:

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 63
Group one: • Resuscitation medicines including colloid or crystalloid IV fluids. • First doses of injected anti-infectives. • First doses of injected anticoagulants or thrombolytics. • First dose of injected anticonvulsants including benzodiazepines. • “Stat” doses of any medicine if the prescriber requires the dose to be
administered before the next regular medicine administration round. Group two:
• Insulin - linked to when food will be actually eaten. • Strong analgesics. • Bronchodilators. • Glyceryl trinitrate. • Parkinson’s disease medicines.
For some of the medicines in the second group, enabling inpatients to self-administer their own medicines at the most appropriate time is a practical approach, but may not be appropriate for all patients. A full copy of the alert can be found via http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=66780&type=full&servicetype=Attachment 17.1 Action in the Event of a Delay or Omission The nurse making the discovery will contact the prescriber. The dose will be given as a matter of urgency. The delay or omission will be noted in the patient records and an entry made onto Datix.
18 ADMISSION AND DISCHARGE MEDICATION PROCEDURES
18.1 Medication on Admission
On admission patients (or carers) should bring the medicines currently being used into the hospital. The patient’s own medicines are important in gaining a complete and accurate medication history. A full drug and allergy history should be undertaken by the admitting doctor reconciling any changes to the medication taken prior to admission. This should be completed using the Medicines Reconciliation Form. Pharmacy will take a full medication and allergy history during the working week and sign and date the Medicines Reconciliation Form to confirm that the medicines have been reconciled.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 64
18.2 Patient’s Own Drugs (in use)
On some wards PODS is in place (See section13.7). On these wards patients own medicines may be used during their hospital stay provided the criteria laid down in the PODS assessment list are met. If the Pharmacy assesses the PODS as being suitable for use it will bear a signed and dated green sticker. The lack of a sticker does not preclude the use of PODS, but means the administering nurse needs to make their assessment using the PODS assessment checklist. Patient’s own medication must not be used for any other patient. If a patient’s own drugs are Controlled Drugs then refer to the Policy for the Management of Controlled Drugs.
18.3 Patient’s Own Drugs for Disposal
Patient’s drugs should only be sent to pharmacy for disposal:
• If they are date expired. • In an unacceptable condition for safe, further use, e.g. drugs mixed in
one container. • If patient prescription is changed and the drug is no longer needed.
• Under normal circumstances the patient’s agreement is required
before disposing of the patient’s own drugs. In the case of psychiatric patients, children and patients too ill to comply the legal guardians may give authority for the disposal of unwanted medication.
18.4 Discharge on Wards where the PODS is in Place
The procedure allows for ward based checking of discharge medication against the discharge prescription. Clinical pharmacists and pharmacy technicians usually undertake this when Pharmacy is open. When the pharmacist is not available a Pharmacy accredited nurse can undertake this task following the Protocol for the Supply of Take Home Medicines by Nurses and Midwives, as prescribed by Medical Practitionersxviii.
18.5 Receipt of the Discharge Drugs from Pharmacy
On wards where patient’s own drugs are not used, the nurse or pharmacist should check the medication against a copy of the prescription prior to giving
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 65
the discharge medication to the patient or relative/carer. They should then counsel the patient concerning the drugs. If there are drugs on the ward that were brought in by the patient on admission these may be returned to the patient/carer provided that the nurse or pharmacy confirms that there is a continuing need for each drug, that the dose and directions are still appropriate.
19 DRUGS ON CLINICAL TRIAL
The investigator must submit the protocol for any clinical trial of medicinal products to the Gwent Research Ethics Committee, Research Scrutiny Committee, and the Research Committee for Approval. Clinical trials of medicines may not be undertaken before the Ethics Committee has issued its approval in writing. All trial material must be stored in the pharmacy department unless this would seriously impair the process of the trial. A Chief Pharmacist or clinical trials pharmacist must approve alternative storage. Clinical trial material must be issued in accordance with the agreed protocol and the pharmacy department’s clinical trial procedures. A prescription for Clinical Trial material must be written and signed by the investigator on a standard prescription form unless a Chief Pharmacist and the Ethics Committee has agreed an alternative. The prescription must be retained within the pharmacy department. A copy of the trial information and randomisation codes must be lodged within the pharmacy before any trial commences. The pharmacy department must retain information and randomisation codes for 2 years after the trial is completed.
20 PATIENT’S HOLIDAYS
When patients leave long-stay units for holidays but remain under hospital care, their medication for the holiday period must be dispensed for them individually by the pharmacy department. Responsibility for the custody of the medicines rests with the senior nurse in overall charge of the patients. A locked container must be used for the storage
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 66
of medicines and this container must be located securely with no access to patients or unauthorised persons. The patients’ Prescription and Administration Record Sheets must accompany the medicines and nursing staff must record all administration on these sheets. Any medicines not used during the holiday must be returned to the pharmacy department when the patient returns to the hospital. If patients from long stay units leave the hospital for short periods e.g. weekend leave at home, an individual prescription must be written and dispensed for them on each occasion. (Also see Appendix 6 “Issues relating to Drugs in Patients Homes” and section 17 Admission and Discharge Medication Procedures).
21 OCCUPATIONAL HEALTH DEPARTMENT
Medicinal products required by Occupational Health Departments may be ordered by the Occupational Health Service doctor or a registered nurse in the department following the same procedures as for hospital wards and departments. Medicinal products may only be administered within Occupational Health Departments in accordance with the written instructions of a doctor or under a Patient Group Direction. The medication administration procedures for wards and departments should be followed except that the record must be kept in the patient’s medical record instead of on a prescription sheet.
22 ACTION TO BE TAKEN IN THE EVENT OF A STOCK DISCREPANCY
In the event of an apparent discrepancy in the stock of controlled drugs or other drugs, the nurse in charge must immediately inform the senior nurse/dentist on duty. Any discrepancies in controlled drugs within the GPOOH service must be reported immediately by the doctor to the shift lead at the OOH Control Centre and if appropriate by the sister/nurse in charge of the ward to the senior nurse for the hospital. An investigation must take place immediately to establish whether or not the discrepancy is valid.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 67
If the discrepancy cannot be reconciled, the senior pharmacist on duty responsible for the hospital/clinic must be contacted for an independent investigation. The senior nurse or senior member of dental staff must be informed. If the discrepancy can be accounted for as other than theft or fraud, the senior nurse or dentist and pharmacist may amend the appropriate records accordingly, both signing the appropriate record book annotating the reason for the discrepancy. If this discrepancy reoccurs within 6 months on the same ward/department/clinic, further action should be considered. If, after these investigations, theft or fraud is suspected the nurse manager/senior nurse or senior member of dental staff in conjunction with the senior pharmacist for the hospital must take the action laid down by the Health Board’s Standing Financial Instructions8 for the reporting of a loss of theft. If the discrepancy is reported outside of the normal pharmacy opening hours the senior nurse/senior staff member must refer it to the on-call pharmacist if it remains unresolved following their investigation. A decision is then to be made whether or not to investigate further immediately, or defer until the following day. The Chief Pharmacist should be informed at the earliest opportunity. Only in extreme cases, where discrepancies cannot be reconciled, should the formal Health Board procedures in the event of fraud or theft be initiated.
23 DISPOSAL OF MEDICINAL PRODUCTS
Controlled drugs must be destroyed in accordance with the requirements laid down in the Misuse of Drugs Regulations 198511 and the Health Board Policy for the Management of Controlled Drugs1. Medicinal products must be disposed of in accordance with the Health Board’s Waste Management Policyxix.
23.1 Medicinal Products Brought into Hospital by Patients
Patients own medications see section 17.3. Medicines obtained for a patient on a GP or Dentist’s prescription are the property of the patient. If they are no longer required (or the patient has died) the patient or patient’s agent should be encouraged to dispose of them by returning with the patient’s permission to the pharmacy from which they were
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 68
obtained. If this is not practicable they should be returned to the pharmacy department accompanied by a list of the returns.
23.2 Disposal of Cytotoxic Products
Arrangements for the disposal should be in accordance with the recommendations contained in the current policy on the Safe Handling of Cytotoxic Drugs16 and the Waste Management Policy19. Residual contents of cytotoxic injections should be sent back to pharmacy for disposal, in suitable leak proof containers labelled cytotoxic waste. Ideally the containers should be covered with a yellow bag clearly labelled ‘Cytotoxic Waste’ with the appropriate yellow labels.
23.3 Disposal of Medicinal Products by the Pharmacy Department
• All medicinal products for destruction will be placed in the appropriate destruction containers. Separate containers exist for aerosols, cytotoxic waste and for other medication.
• Controlled Drugs should be destroyed in accordance with
departmental policy that renders then unsalvageable. They should then by placed within the appropriate containers for destruction. See Policy for the Management of Controlled Drugs1.
• All of the containers for destruction must be accounted for at the time
of collection and a signature obtained for the dispatcher. All containers will be incinerated in accordance with the Health Board’s Waste Management Policy19.
When medicinal products supplied for patients while they are in hospital are no longer required, the label on the container must be crossed with a Z to indicate they are no longer required. On acute wards they should be retained on the ward in a locked cupboard for the pharmacy staff to sort. On community hospital wards they should be returned to pharmacy. The ward pharmacist must be informed by the nurse in charge if stock items are no longer required at ward level so that adjustments can be made to the stock lists at ward and pharmacy level. A written list of medicinal products being returned to the pharmacy department must be prepared and sent with the items to the pharmacy in a locked or sealed container or handed to a pharmacist or pharmacy technician. A copy of the list must be kept in the ward or department.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 69
Medicinal products that are out of date or no longer required must be returned to the pharmacy department in a locked or sealed container. Expired items must be marked “Expired”. When small volume injections, infusion solutions and other products have been opened at ward or department level and it is not practical to return them to the pharmacy, the remaining contents of the container must be disposed of via the ward or department’s sluice system or other direct sewage access point. The residual contents of opened live vaccine containers must be returned for disposal in YELLOW sharps bins in accordance with the Waste Management Policy19 for the Health Board. Community Psychiatric Nurses must keep a record of any drugs returned to the pharmacy department and obtain a receipt. Medicinal products must be disposed of in accordance with current legislation and the Health Board’s Waste Management Policy19.
23.4 Disposal of Medicines in the Community
Community nurses are required to advise patients about safe disposal of out of date medicines and medicines no longer prescribed. Patients, or the estate in event of the patient’s death, are advised to return such medicines to the local community pharmacy (chemist).
24 REPORTING DEFECTS
When a defect in a medicinal product or dressing is discovered or suspected, medical, nursing or other professional staff must immediately report the defect to a senior pharmacist (or the on-call pharmacist) and the senior nurse in the unit. All suspect material must be identified and quarantined in a safe place for analysis. A “Drug and Dressing Defect Reporting Form for Wards and Departments” (Appendix 3) must be completed at a ward or department level by a pharmacist and the medical and nursing staff who discover or suspect the defect. The Principal Pharmacist, Quality Assurance will normally be the senior pharmacist responsible for completing the documentation but this will be delegated to a senior pharmacist in their absence. The report must fully identify the product, the precise reason for suspecting the defect, the incident and the person discovering the defect and any other important information.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 70
The Principal Pharmacist, Quality Assurance or in their absence, the senior pharmacist on duty will follow the current procedure for Reporting Accidents With and Serious Defects in Drugs and Dressings and the WAG Guidance on Defective Medicinal Products. Instructions will be issued to all concerned regarding further use of the drug or dressing. On completion of the investigation the pharmacy department will report back to the staff concerned at ward or departmental level. In the event of a suspected or discovered defect in an IV product then the administration apparatus, including the infusion bag and giving set should also be retained. Details of defects in medicinal products will be notified by the Pharmacy to the All Wales Quality Control Pharmacist who will inform the MHRA and National Assembly for Wales where a product recall is deemed necessary.
25 HAZARD WARNINGS
During working hours, Hazard Warnings relating to defective medicinal products will be faxed to the pharmacy department at the Royal Gwent Hospital (RGH) by the National Assembly for Wales. 1. The Public Health Link system is used when information needs to reach
health professionals quickly. Categories describe the degree of urgency of the message and how quickly the message needs to be read and cascaded by health professionals.
2. Categories for Public Health Link messages are; Immediate: Cascade within 6 hours. To be used infrequently in
exceptional cases where potentially serious health risks are implicated.
Urgent: Cascade within 24 hours - the most common category. Non-urgent: Cascade within 48 hours For information: This is used in circumstances where there is no
need to cascade the information and only those who receive the message directly need to be aware of its content.
3. Public Health Links are used to inform health professionals of drug alerts,
drug recalls, medicine defects, and other appropriate information or guidance.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 71
4. Public Health Links are received from the Welsh Assembly usually by email,
but other routes such as fax, letter or telephone may also be used. 5. The Secretary, RGH will check Chief Pharmacist’s emails/fax/post for PHLs. 6. If received, the Secretary will attach form PHL1 to the PHL and give to
Pharmacy Manager RGH, or nominated deputy. 7. The Secretary will immediately fax the PHL to Pharmacy Managers at NHH
and CDMH for action and will phone them to alert them of the fax. 8. The Chief Pharmacist or nominated deputy must record details onto Form
PHL1, attach the Public Health Link to Form PHL1, and follow the ACTION stipulated in Form PHL1.
9. If the Public Health Link concerns a Drug Recall and the defective batch(s)
have been stocked at any time, then all possible locations on wards, departments and clinics must be checked and/or informed of the recall/defect.
10. Any defective batch(s) must be quarantined until it can either be destroyed
or returned as instructed. 11. If the PHL involves a CD, then the CD Return procedure must be followed. 12. Stock held/not held is to be reported verbally within 6 hours of notification
and confirmed in writing using form PHL2 within 48 hours (from RGH, NHH and CDMH).
13. The Secretary RGH must check that the appropriate forms have been
returned, and in the case of a Medical Device alert will report back by email to the clinical governance facilitator of the division whether or not the device is stocked .
26 TRANSPORT AND STORAGE OF MEDICINAL PRODUCTS
26.1 Outside hospitals and community based services
Staff involved directly with the transport of medicines must be trained to ensure that they understand the procedures and the need for security. This should include instruction in the action to be taken in the event of physical threats.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 72
Lockable cupboards that comply with British Standards are to be used for the storage of all medicines. The medicines must be located in a secure location and only authorised nurses/ODPs, (doctors in the GPOOH service) will hold the keys. The appropriate records must be completed when medicines are received or returned to the cupboards. A second nurse must witness any transfer of medicines. Medicinal products must be transported between the pharmacy department and storage cupboards in an appropriate locked or tamper evident container. An authorised person must receive medicinal products and the delivery must be signed for including items delivered by taxi. Medicinal products must not be left unsupervised. Each sealed delivery box will contain a note itemising the products enclosed. Any discrepancies must be reported to the pharmacy department immediately. In the interests of safety, Nurses, Midwives and Health Visitors are not encouraged to carry medicinal products albeit on occasions it is recognised that this will be necessary. Community Nurses and Midwives must take all possible precautions to ensure the safe custody of medicinal products in their possession e.g. carry any medicines with them on visits in a locked container and restrict the quantity carried to that required until their next visit to the storage cupboard. If it is necessary to leave the locked container in a vehicle it must be placed out of sight in the locked boot of the car. The Community Midwife must possess an authenticated identification card authorising her to carry medicines. The card must bear the name of the midwife and her date of authorisation. Vaccines and other heat-sensitive products for community hospitals or clinics must be transported in cool-boxes with ice packs and clearly labelled “STORE IN A REFRIGERATOR” and/or “VACCINES – STORE COOL”. Order books/pads, WP10 (HP) prescriptions and other controlled stationery must travel to and from the pharmacy in locked or sealed containers, or be carried by an authorised person. Transport staff are responsible for the security of medicines during transport until the medicines are delivered to and signed for by an authorised person. Once issued to nursing, midwifery, medical staff or other professional staff, medicinal products, including controlled drugs, become the responsibility of the person to whom they have been issued.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 73
When controlled drugs are carried they must always be kept on the person of the authorised carrier and not left in cars, other than the brief period when a transport driver is delivering to a number of hospitals. Medicinal products being returned to the pharmacy must be returned in locked or sealed containers with the destination clearly shown. No unauthorised passengers my travel in hospital vehicles carrying drugs to hospitals or clinics.
26.2 To Patient’s Home
i) Medicines for treatment of patients at home, for example patients with psychiatric illness, are prescribed by the appropriate Doctor or GP. In some instances these are collected by the community nurse and conveyed in a secure manner to the patient’s home (see par. 25.1 c). In this instance the nurse acts as the patient’s agent, the medicines being the patient’s property.
ii) Occasionally it may be inadvisable for the medicines to be kept in the patient’s home. The medicines must be kept in a secure place, in a suitable locked cupboard, with the keys in the possession of authorised nursing staff.
iii) When the patient’s medicines are not stored in the patient’s home, the nurse will inform the appropriate nurse /team manger and GP. The nurse must also enter the necessary information in the relevant nursing notes.
26.3 In the Hospital Setting
Only authorised hospital employees may carry medicines. Patients or relatives are not permitted to carry anything other than their own or their relatives’ medicines’.
26.4 Required for Patients in Transit
The safe custody and administration of these drugs will be the responsibility of the accompanying nurse/doctor.
27 UNLICENSED MEDICINES
Prescribing of unlicensed medicines has occurred for many years and is recognised as necessary under the Medicines Act 1968 (Amendment) Regulations 19952.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 74
However, the Medicines Act makes it quite clear that if clinicians prescribe medicines without a product licence that they take clinical responsibility. In 1993 all NHS hospitals lost Crown Immunity and many Health Boards looked at prescribing of unlicensed medicines as a potential for litigation and set up policies accordingly. The NHS White Paper ‘Putting Patient’s First’ (enacted 1999)xx led to the introduction of the concept of Clinical Governance. Risk management is a key component of the Clinical Governance agenda. The management of medicines is high priority. The Health Board has introduced systems and protocols to monitor the use of unlicensed medicines. The MHRA Guidance Note Number 14 (MAL 14) (February 2000)xxi states ‘’Hospital Health Boards should have clear policies on the use of unlicensed medicines which reflect the differences in liability which may exist”. The Prescribing Advisory Group, on behalf of the Aneurin Bevan Health Board, should support therapeutic practices that are advocated by respectable, responsible bodies of opinion. However, there is a responsibility to monitor prescribing practices in order to protect the patients and clinicians and limit liability. For use of medicines not covered by a product see the Health Board’s Use of Unlicensed Medicines and Medicines Used Outside their Produce License policyxxii. Nurse and pharmacist prescribers are not allowed to prescribe unlicensed medication.
27.1 Medicines used Outside their Product Licence
For a medicine to be marketed in the United Kingdom, it must receive a product licence, now called a marketing authorisation. It is then said to be licensed. Many medicines used within specialist areas in the hospital such as paediatrics, intensive care unit and psychiatry are not licensed for a particular indication, age group, dosage or route of administration. This position arises when a pharmaceutical company has made an application to the licensing authority for a marketing authorisation for use of the medicine for a specific indication, etc. It may, however, not make an application to use the medicine in other ways, which are safe and legitimate. See the Health Board Policy for Use of Unlicensed Medicines and Medicines Used Outside their Product License as above.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 75
28 AMBULANCE SERVICE
Medicinal products on a list agreed by the Health Board and the Ambulance Trust will be issued to ambulance officers who have completed the extended training in ambulance aid and hold a certificate of proficiency in ambulance paramedic skills. The list of prescription-only medicines allowed is limited to those currently on the statutory list. The Chief Ambulance Officer will have responsibility for ensuring that this system is followed and that the security of medicines handled by ambulance staff is maintained. The Chief Ambulance Officer may decide to delegate some of the duties but the accountability will always remain with the Chief Ambulance Officer. When medicines are carried on an ambulance the Chief Ambulance Officer will ensure that the written protocol for the Procurement, Storage, Administration and Handling of Medicinal Productsxxiii is given to each authorised Ambulance Officer and that he or she is made aware of his or her responsibilities. Staff who have undergone the Extended Training Programme and who have been authorised, will be personally responsible for the security of the medicines in their possession. Appropriate precautions (see COSHH reference data) must be taken by staff handling medicinal products especially those that are hazardous to health by any route (e.g. inhalation, ingestion, absorption) The medicinal products listed apart from large volume infusion fluids will be issued in Emergency Ambulance Drug Boxes appropriately labelled with instructions for the replacement of their contents and numbered for identification. Large volume infusion fluids and any extra supplies of listed items may only be supplied against an officially written order (bearing an order number) signed by the station manager. The Ambulance Trust is responsible to send appropriate staff to collect a replacement ambulance box, which will be replaced on a one to one basis. Used boxes will be re-filled by pharmacy. Pharmacy departments will keep records of the numbered Emergency Boxes issued to individual sites.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 76
It will be the duty of the Chief Pharmacist to ensure that medicines are only supplied in accordance with the agreed procedures. Whilst in the possession of the Ambulance Service the responsibility for the safe keeping and control of the medicines rests with the Chief Ambulance Officer. Persons who hold a certificate of proficiency in ambulance paramedic skills issued by or with the approval of the Secretary of State may administer certain parenteral prescription-only medicines. The administration will be only for the immediate, necessary treatment of sick or injured persons and, in the case of a prescription-only medicine containing heparin sodium, will only before the purpose of cannula flushing. The Ambulance Officer administering a medicine must record the administration in the approved administration records. Medicines refused, wasted or disposed of must be recorded. Any problems that arise with medicinal products, including loss or theft, must be reported immediately to a pharmacy department.
29 APPENDICES
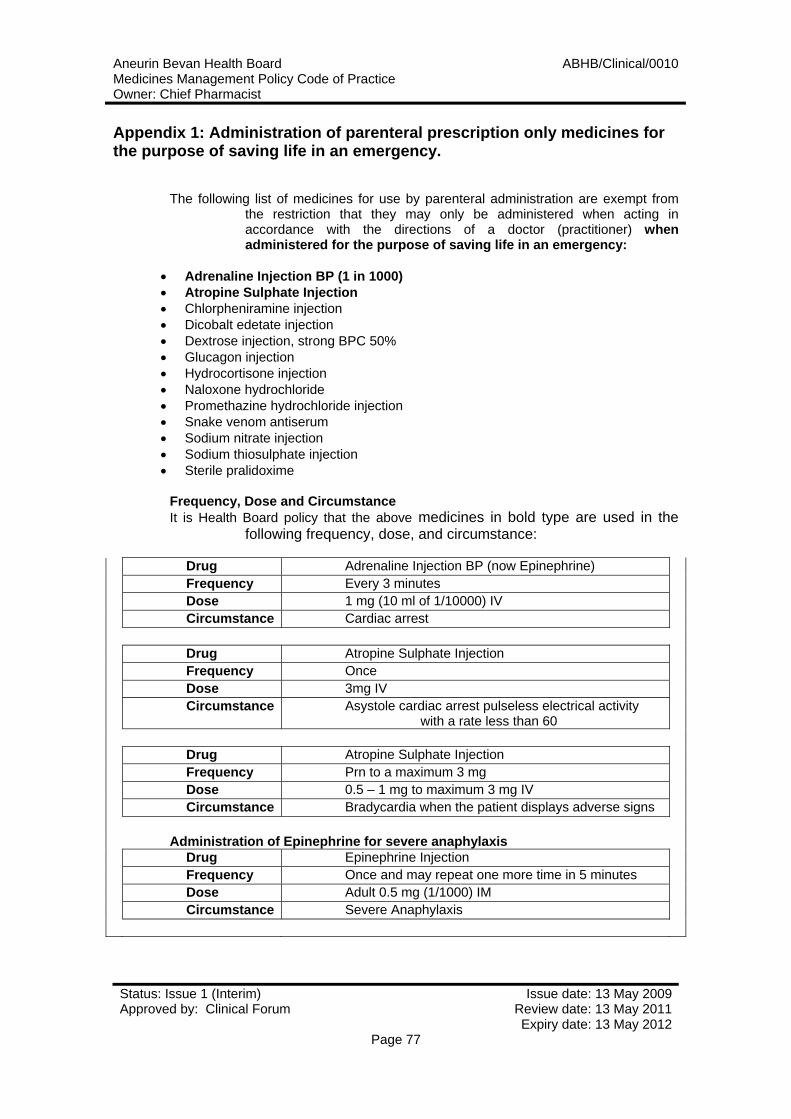
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 77
Appendix 1: Administration of parenteral prescription only medicines for the purpose of saving life in an emergency.
The following list of medicines for use by parenteral administration are exempt from
the restriction that they may only be administered when acting in accordance with the directions of a doctor (practitioner) when administered for the purpose of saving life in an emergency:
• Adrenaline Injection BP (1 in 1000) • Atropine Sulphate Injection • Chlorpheniramine injection • Dicobalt edetate injection • Dextrose injection, strong BPC 50% • Glucagon injection • Hydrocortisone injection • Naloxone hydrochloride • Promethazine hydrochloride injection • Snake venom antiserum • Sodium nitrate injection • Sodium thiosulphate injection • Sterile pralidoxime
Frequency, Dose and Circumstance It is Health Board policy that the above medicines in bold type are used in the
following frequency, dose, and circumstance:
Drug Adrenaline Injection BP (now Epinephrine) Frequency Every 3 minutes Dose 1 mg (10 ml of 1/10000) IV Circumstance Cardiac arrest Drug Atropine Sulphate Injection Frequency Once Dose 3mg IV Circumstance Asystole cardiac arrest pulseless electrical activity
with a rate less than 60 Drug Atropine Sulphate Injection Frequency Prn to a maximum 3 mg Dose 0.5 – 1 mg to maximum 3 mg IV Circumstance Bradycardia when the patient displays adverse signs
Administration of Epinephrine for severe anaphylaxis Drug Epinephrine Injection Frequency Once and may repeat one more time in 5 minutes Dose Adult 0.5 mg (1/1000) IM Circumstance Severe Anaphylaxis
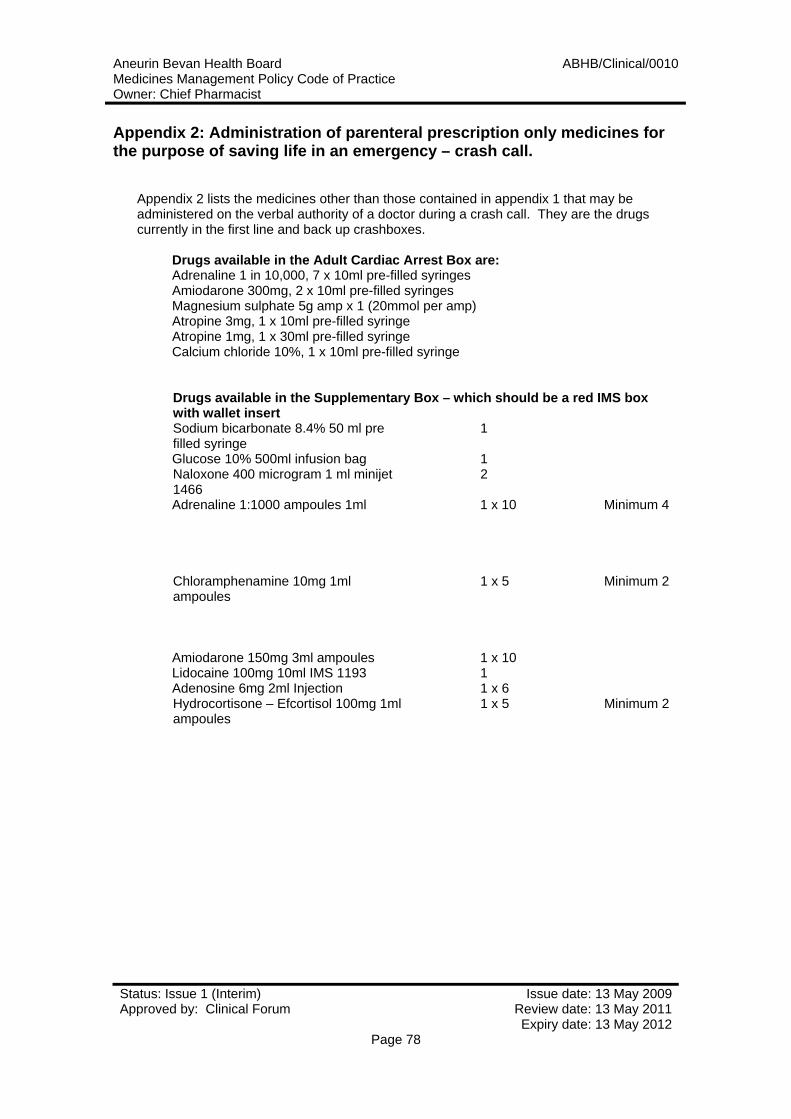
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 78
Appendix 2: Administration of parenteral prescription only medicines for the purpose of saving life in an emergency – crash call.
Appendix 2 lists the medicines other than those contained in appendix 1 that may be administered on the verbal authority of a doctor during a crash call. They are the drugs currently in the first line and back up crashboxes.
Drugs available in the Adult Cardiac Arrest Box are: Adrenaline 1 in 10,000, 7 x 10ml pre-filled syringes Amiodarone 300mg, 2 x 10ml pre-filled syringes Magnesium sulphate 5g amp x 1 (20mmol per amp) Atropine 3mg, 1 x 10ml pre-filled syringe Atropine 1mg, 1 x 30ml pre-filled syringe Calcium chloride 10%, 1 x 10ml pre-filled syringe
Drugs available in the Supplementary Box – which should be a red IMS box with wallet insert Sodium bicarbonate 8.4% 50 ml pre filled syringe
1
Glucose 10% 500ml infusion bag 1 Naloxone 400 microgram 1 ml minijet 1466
2
Adrenaline 1:1000 ampoules 1ml 1 x 10 Minimum 4
Chloramphenamine 10mg 1ml ampoules
1 x 5 Minimum 2
Amiodarone 150mg 3ml ampoules 1 x 10 Lidocaine 100mg 10ml IMS 1193 1 Adenosine 6mg 2ml Injection 1 x 6 Hydrocortisone – Efcortisol 100mg 1ml ampoules
1 x 5 Minimum 2
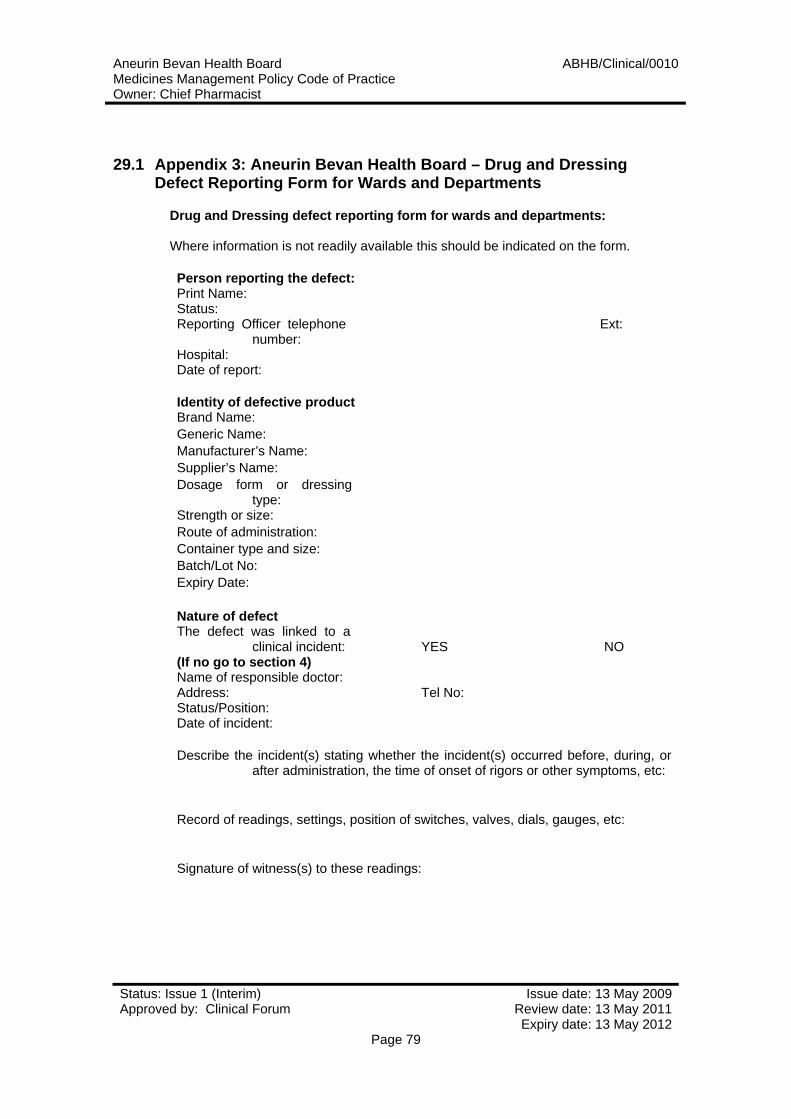
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 79
29.1 Appendix 3: Aneurin Bevan Health Board – Drug and Dressing Defect Reporting Form for Wards and Departments
Drug and Dressing defect reporting form for wards and departments: Where information is not readily available this should be indicated on the form. Person reporting the defect: Print Name: Status: Reporting Officer telephone
number: Ext:
Hospital: Date of report:
Identity of defective product Brand Name: Generic Name: Manufacturer’s Name: Supplier’s Name: Dosage form or dressing
type:
Strength or size: Route of administration: Container type and size: Batch/Lot No: Expiry Date:
Nature of defect The defect was linked to a
clinical incident: (If no go to section 4)
YES NO
Name of responsible doctor: Address: Tel No: Status/Position: Date of incident:
Describe the incident(s) stating whether the incident(s) occurred before, during, or
after administration, the time of onset of rigors or other symptoms, etc: Record of readings, settings, position of switches, valves, dials, gauges, etc: Signature of witness(s) to these readings:
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 80
Recollections of those present at the incident (attach separate sheet if necessary): Details of other therapy if relevant (other infusions, drugs etc.): Details of action
taken (specimens for blood culture, culture of catheter tip, urine samples taken, use of batch stopped locally, etc.):
Pharmaceutical Observations: Name of pharmacist: Tel No: Address: Described the defect: This report refers to: ISOLATED CONTAINERS ALL CONTAINERS Date the batch was introduced onto the Market: Estimated date when the batch was introduced into stock locally: Estimated amount of batch used locally todate: Manufacturer’s telephone number: Name of person contacted: Manufacturer’s comments: Details of samples and IV giving sets, etc sent for analysis (number, reference
number, where sent etc): Result of analysis: Signature of pharmacist: Date: ALL DEFECT/INCIDENTS MUST BE REPORTED IN ACCORDANCE WITH WHC
(89) 26 or later amendment WITHOUT DELAY.
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 81
Appendix 4: Prescribing for Members of the Health Board’s Staff and Families
Policy for Doctors Self-Prescribing This policy was formulated and agreed by a meeting of the Clinical Policy
Board on 1st March 2000. It is an attempt to allow some emergency prescribing but ensure that good clinical practice is maintained. It is based on the premise that, in general, self-medication represents sub-optimal practice and can, on occasions, represent bad clinical practice. (Note that unless doctors have FULL registration with the GMC they may only prescribe prescription-only medicines (POMs) in connection with their work for the Health Board i.e. they may not prescribe POMs for themselves).
Doctors Prescribing for Themselves Doctors who experience minor ill health whilst on duty or who forget simple
but regular medications may obtain prescriptions for such medications from the hospital pharmacy free of charge. These include classes of drugs such as inhaler devices for asthma, antibiotics and simple non-steroidal anti-inflammatory agents. Sufficient for while the doctor is on duty (or an unbreakable pack like an inhaler) may be supplied free of charge. Other drugs can be prescribed but there are limitations. The dispensing of these drugs will require payment consisting of a private prescription fee and handling costs:
(i) Simple medicines may be dispensed at the discretion of a pharmacist. E.g.:
Gaviscon, skin preparations, etc.
(ii) Other drugs (including antihypertensives, proton pump inhibitors etc), may be dispensed by the pharmacist no more than 2 days supply will be dispensed – allowing work to continue but time to consult a general practitioner for a repeat prescription.
Prescriptions for any drugs that significantly affect performance will
not be allowed through the hospital pharmacy. This includes opiates, benzodiazepines, antidepressants and other mood altering formulae or recreational medications.
Doctors Prescribing for Their Family or Other Relatives There will be a moratorium on dispensing prescriptions for doctors’ family
members who should be registered under a local general practitioner.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 82
Appendix 5: Action to be Taken Outside of Pharmacy Opening Hours
Action to be Taken Outside of Pharmacy Opening Hours
All medication must be requested from the appropriate pharmacy during their normal working hours.
If medication is unavailable and required immediately the senior nurse on
duty must be contacted. He/she will have access to the pharmacy departments emergency drug cupboard. The list of contents will be available on the Intranet and/or via regularly updated hard copies.
The senior nurse, who will have keys to access the emergency drug
cupboard, must obtain the supply, making an entry in the issue book available. This will enable restocking when the pharmacy reopens. (A note should be left if the required medication is not available to bring this to the attention of the Pharmacy the following day).
If the medication required is not available in the emergency cupboard the
on call pharmacist may be contacted via the hospital switchboard. Calls will only be accepted from the senior nurse or the prescriber if the request is for information.
The on call pharmacist and the senior nurse/prescriber will agree
appropriate action.

Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 83
29.2 Appendix 6: Issues Relating to Drugs in Patients Homes
Issues relating to medicines in patient homes Medicines required for patients or clients being cared for in their own
homes should be obtained by prescription from the patient’s General Practitioner, or from the take home medicines prescribed for the patient before discharge. The patient or their next of kin should collect these medicines.
Midwives attending a home birth, or CPN, can obtain drugs for
administration at the home by order from the pharmacy, however, the preferred method of managing these events is for the General Practitioner, or identified Doctor, to prescribe individually for the client.
Nurses, Midwives and Health Visitors who care for patients and clients in
their own homes have a moral and ethical duty to ensure that the patient is fully aware of the safest way to store and dispose of medicines in the home. Practitioners must draw the patients attention to the extra care required where children form part of the family.
Medicines not required after treatment is complete or has been changed
must be returned to the pharmacy by the patient or his/her next of kin. The community practitioner will not be involved in disposal or return of drugs. In the case of midwives in attendance at home births, the Misuse of Drugs Regulations contains a procedure for witnessing the destruction of Pethidine (or other controlled drugs approved in accordance with the Medicines Act 1968) which have been supplied to the midwife but are no longer required. (Midwives rules and code of practice 1998 Section 17).
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 84
Appendix 7: Drugs Carried by Community Midwives
• Ergometrine maleate 500mcg in 1ml (2 ampoules)
• Syntometrine injection 1ml ampoules (5 ampoules)
• Naloxone Hydrochloride 400mcg per 1ml (3 ampoules)
• Lignocaine Hydrochloride 1% (3x 5ml ampoules)
• Glycerin suppositories 4g (1 box of 12)
• Lubricating jelly 1 x 150mg (5g)
• Paracetamol tablets 500mg
• Konakion injection 1mg in 0.5ml (2 ampoules)
• Senna tablets 7.5mg
• Sodium chloride single use eye drops 0.9% minims
• Phosphate retention enema
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 85
Appendix 8: Prescription-only medicines which can be administered parenterally by midwives in the course of their professional practice
• Diamorphine
• Ergometrine maleate
• Lignocaine
• Lignocaine hydrochloride
• Morphine
• Naloxone hydrochloride
• Oxytocins (natural and synthetic)
• Pentazocine lactate
• Pethidine hydrochloride
• Phytomenadione
• Promazine hydrochloride
(In the case of lignocaine, lignocaine hydrochloride and promazine
hydrochloride only while attending on a woman in childbirth).
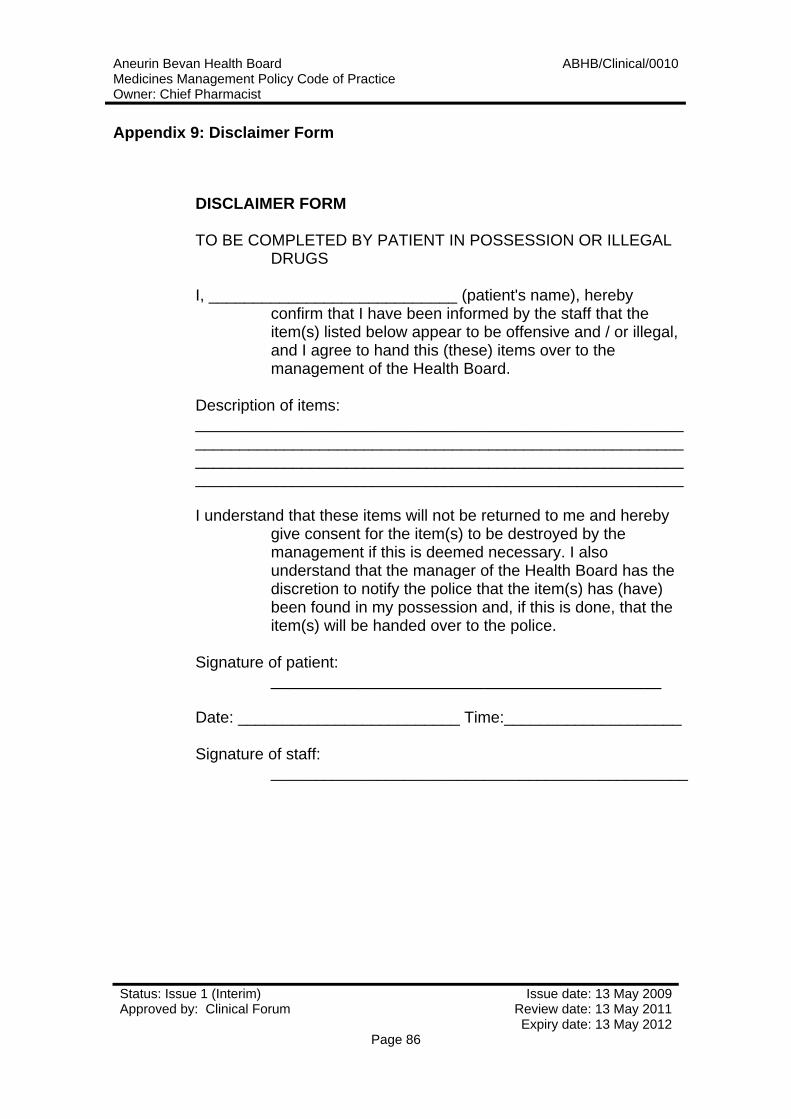
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 86
Appendix 9: Disclaimer Form
DISCLAIMER FORM TO BE COMPLETED BY PATIENT IN POSSESSION OR ILLEGAL
DRUGS I, ____________________________ (patient's name), hereby
confirm that I have been informed by the staff that the item(s) listed below appear to be offensive and / or illegal, and I agree to hand this (these) items over to the management of the Health Board.
Description of items: _______________________________________________________ _______________________________________________________ _______________________________________________________ _______________________________________________________ I understand that these items will not be returned to me and hereby
give consent for the item(s) to be destroyed by the management if this is deemed necessary. I also understand that the manager of the Health Board has the discretion to notify the police that the item(s) has (have) been found in my possession and, if this is done, that the item(s) will be handed over to the police.
Signature of patient:
____________________________________________ Date: _________________________ Time:____________________ Signature of staff:
_______________________________________________
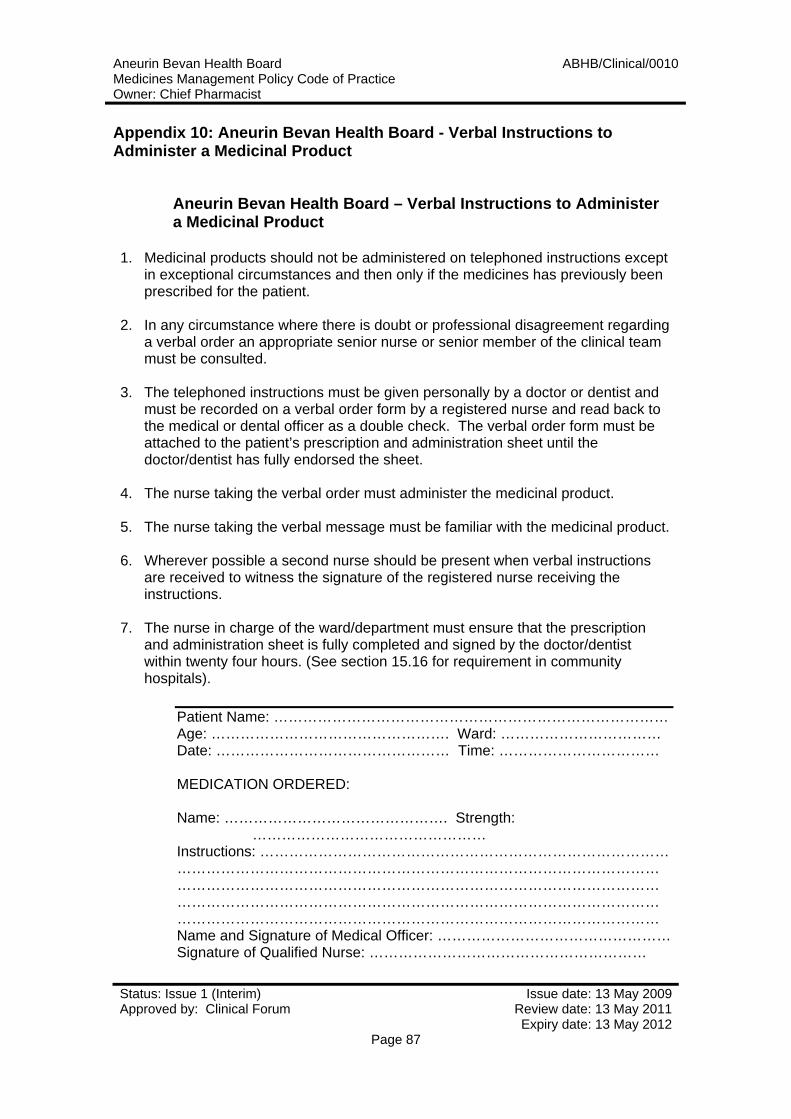
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 87
Appendix 10: Aneurin Bevan Health Board - Verbal Instructions to Administer a Medicinal Product
Aneurin Bevan Health Board – Verbal Instructions to Administer a Medicinal Product
1. Medicinal products should not be administered on telephoned instructions except in exceptional circumstances and then only if the medicines has previously been prescribed for the patient.
2. In any circumstance where there is doubt or professional disagreement regarding
a verbal order an appropriate senior nurse or senior member of the clinical team must be consulted.
3. The telephoned instructions must be given personally by a doctor or dentist and
must be recorded on a verbal order form by a registered nurse and read back to the medical or dental officer as a double check. The verbal order form must be attached to the patient’s prescription and administration sheet until the doctor/dentist has fully endorsed the sheet.
4. The nurse taking the verbal order must administer the medicinal product.
5. The nurse taking the verbal message must be familiar with the medicinal product.
6. Wherever possible a second nurse should be present when verbal instructions
are received to witness the signature of the registered nurse receiving the instructions.
7. The nurse in charge of the ward/department must ensure that the prescription
and administration sheet is fully completed and signed by the doctor/dentist within twenty four hours. (See section 15.16 for requirement in community hospitals).
Patient Name: ……………………………………………………………………… Age: …………………………………………. Ward: …………………………… Date: ………………………………………… Time: …………………………… MEDICATION ORDERED: Name: ………………………………………. Strength:
………………………………………… Instructions: ………………………………………………………………………… ……………………………………………………………………………………… ……………………………………………………………………………………… ……………………………………………………………………………………… ……………………………………………………………………………………… Name and Signature of Medical Officer: …………………………………………Signature of Qualified Nurse: …………………………………………………
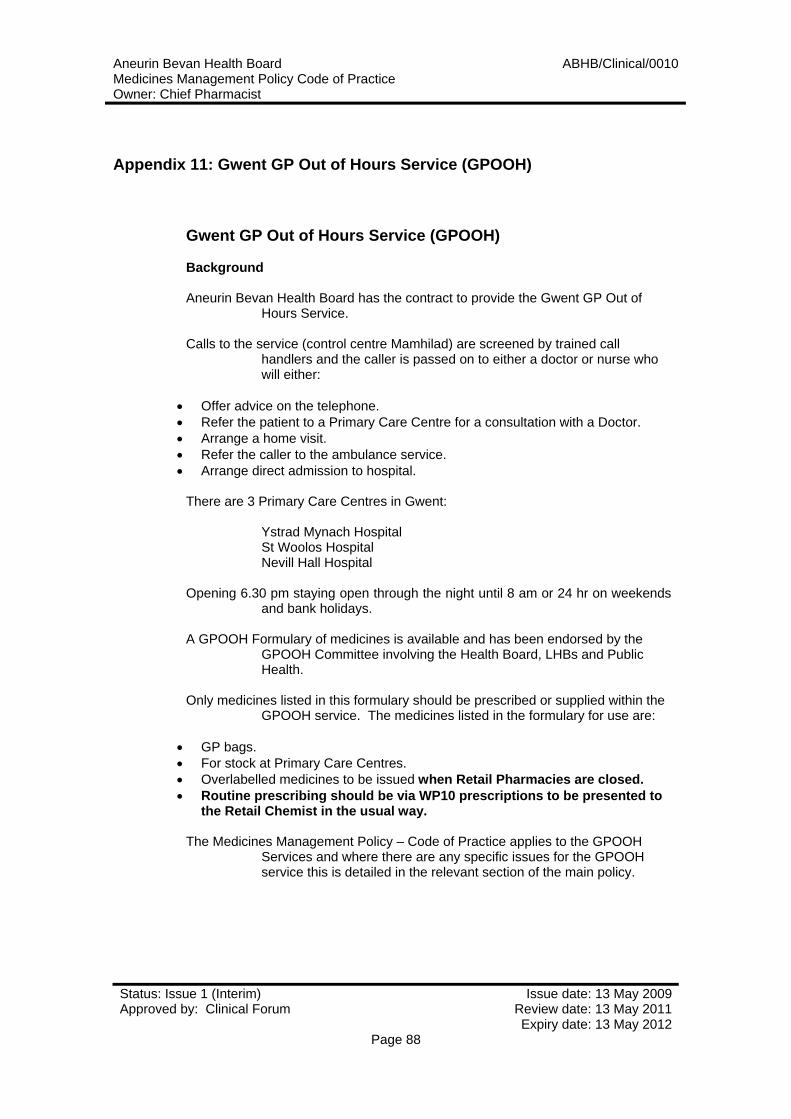
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 88
Appendix 11: Gwent GP Out of Hours Service (GPOOH)
Gwent GP Out of Hours Service (GPOOH) Background Aneurin Bevan Health Board has the contract to provide the Gwent GP Out of
Hours Service. Calls to the service (control centre Mamhilad) are screened by trained call
handlers and the caller is passed on to either a doctor or nurse who will either:
• Offer advice on the telephone. • Refer the patient to a Primary Care Centre for a consultation with a Doctor. • Arrange a home visit. • Refer the caller to the ambulance service. • Arrange direct admission to hospital.
There are 3 Primary Care Centres in Gwent: Ystrad Mynach Hospital St Woolos Hospital Nevill Hall Hospital Opening 6.30 pm staying open through the night until 8 am or 24 hr on weekends
and bank holidays. A GPOOH Formulary of medicines is available and has been endorsed by the
GPOOH Committee involving the Health Board, LHBs and Public Health.
Only medicines listed in this formulary should be prescribed or supplied within the
GPOOH service. The medicines listed in the formulary for use are:
• GP bags. • For stock at Primary Care Centres. • Overlabelled medicines to be issued when Retail Pharmacies are closed. • Routine prescribing should be via WP10 prescriptions to be presented to
the Retail Chemist in the usual way. The Medicines Management Policy – Code of Practice applies to the GPOOH
Services and where there are any specific issues for the GPOOH service this is detailed in the relevant section of the main policy.
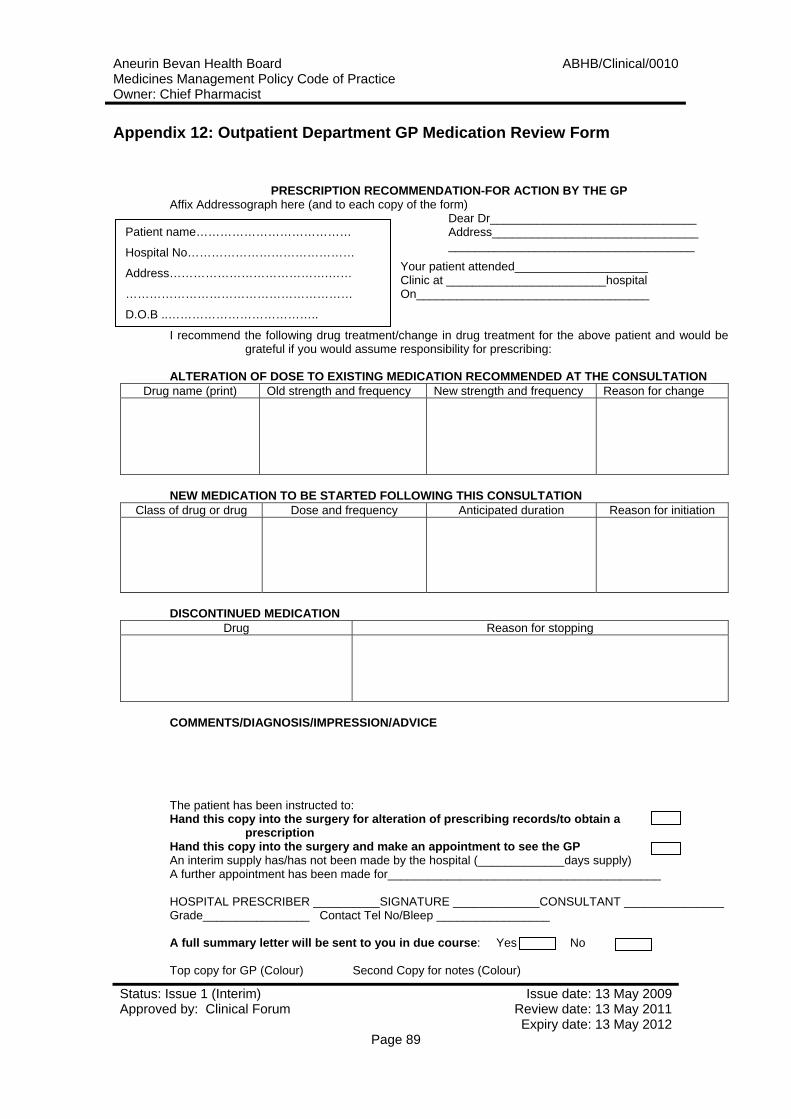
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009
Appendix 12: Outpatient Department GP Medication Review Form
PRESCRIPTION RECOMMENDATION-FOR ACTION BY THE GP
Affix Addressograph here (and to each copy of the form) Dear Dr_______________________________ Address_______________________________ _____________________________________
Your patient attended____________________ Clinic at ________________________hospital On___________________________________
I recommend the following drug treatment/change in drug treatment for the above patient and would be grateful if you would assume responsibility for prescribing:
ALTERATION OF DOSE TO EXISTING MEDICATION RECOMMENDED AT THE CONSULTATION
Drug name (print) Old strength and frequency New strength and frequency Reason for change
NEW MEDICATION TO BE STARTED FOLLOWING THIS CONSULTATION
Class of drug or drug Dose and frequency Anticipated duration Reason for initiation
DISCONTINUED MEDICATION
Drug Reason for stopping
COMMENTS/DIAGNOSIS/IMPRESSION/ADVICE
The patient has been instructed to: Hand this copy into the surgery for alteration of prescribing records/to obtain a
prescription Hand this copy into the surgery and make an appointment to see the GP An interim supply has/has not been made by the hospital (_____________days supply) A further appointment has been made for_________________________________________ HOSPITAL PRESCRIBER __________SIGNATURE _____________CONSULTANT _______________ Grade________________ Contact Tel No/Bleep _________________ A full summary letter will be sent to you in due course: Yes No Top copy for GP (Colour) Second Copy for notes (Colour)
Patient name…………………………………
Hospital No……………………………………
Address………………………………….……
…………………………………………………
D.O.B ..………………………………..
Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 89
Aneurin Bevan Health Board ABHB/Clinical/0010Medicines Management Policy Code of Practice Owner: Chief Pharmacist
Status: Issue 1 (Interim) Issue date: 13 May 2009Approved by: Clinical Forum Review date: 13 May 2011 Expiry date: 13 May 2012
Page 90
30 REFERENCES
i GHT Policy for the Management of Controlled Drugs ii Medicines Act 1968, (Amendment) Regulations 1995, Misuse of Drugs Act 1971, Modification) Order 1996, as amended iii Guidelines for the Safe and Secure Handling of Medicines, A Team Approach, (Revised Duthie Report March 2005) iv GHT Non Medical Prescribing Policy (Supplementary and Independent) v GHT Policy for the Use of Patient Group Directions vi GHT Protocol for the Prescribing of Medicines for Outpatients vii GHT Standing Orders, Tendering, Contract Procedures and Financial Instructions viii Consumer Protection Act 1987 ix Rules and Guidance for Pharmaceutical Manufacturers and Distributors, 2007 The Orange Guide updated x Medicines (Labelling) Regulations 1976 xi Misuse of Drugs Regulations 1985, as amended xii GHT Searching of Patients and their Property within Mental Health and Learning Disability Settings xiii NMC, Code of Professional Conduct: Standards of conduct, performance and ethics, for Nurses and Midwives, 2008 NMC Standards for Medicines Management, Aug 2008 xiv GHT Policy for the Administration of Intravenous Medication xv Mental Health Act 1983 xvi GHT Safe Handling of Cytotoxic Drugs, April 2006 xvii GHT Safe Prescribing, Dispensing and Administration of Intrathecal Chemotherapy Policy, April 2006). xviii GHT - Protocol for the Supply of Take Home Medicines by Nurses and Midwives, as prescribed by Medical Practitioners. xix GHT Waste Management Policy xx NHS White Paper ‘Putting Patient’s First’ (enacted 1999) xxi MHRA Guidance Note Number 14 (MAL 14) (February 2000) xxii GHT Use of Unlicensed Medicines and Medicines Used Outside their Produce License policy xxiii Procurement, Storage, Administration and Handling of Medicinal Products xx1v GHT Incident Reporting Policy and Procedure