Embed Size (px)
Citation preview
Introduction
I have always had an interest in traveling and havebeen to most parts of the United States, but I hadnever been out of the country before my trip to WestAfrica. When I learned of the study tour to TheGambia, I was mainly int r igued by the t ravelopportunity and not so much by the anthropologycredits I would earn by writing this paper. But, itwas a package deal, so when I got to The Gambia, Ihad to find a research topic. I am a student ofchemistry but did not want a project that would putme in a laboratory; I didn�t cross the Atlantic Oceanto research a topic that I could at home. Medicalresearch is my primary interest, and when our groupstarted touring hospitals and learning about the dualhealth system of The Gambia, traditional medicinepresented itself as an intriguing field that was acombination of my interests in medicine as well asAfrican culture.
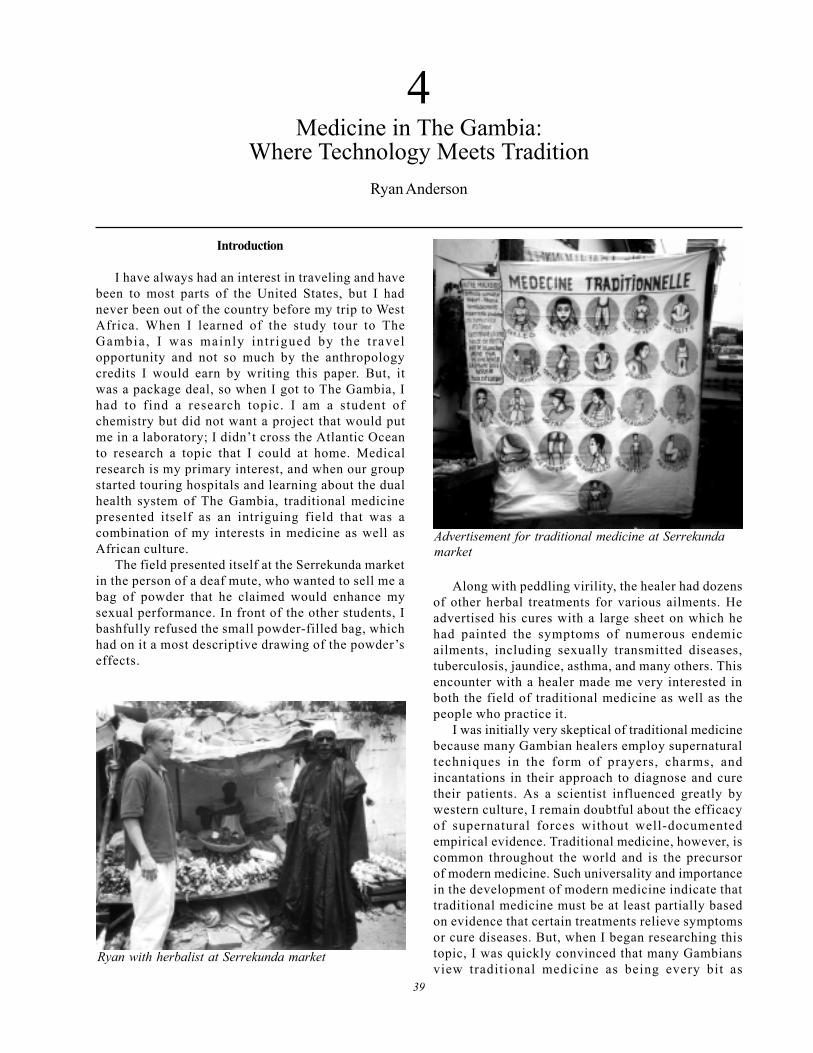
The field presented itself at the Serrekunda marketin the person of a deaf mute, who wanted to sell me abag of powder that he claimed would enhance mysexual performance. In front of the other students, Ibashfully refused the small powder-filled bag, whichhad on it a most descriptive drawing of the powder�seffects.
Along with peddling virility, the healer had dozensof other herbal treatments for various ailments. Headvertised his cures with a large sheet on which hehad painted the symptoms of numerous endemicailments, including sexually transmitted diseases,tuberculosis, jaundice, asthma, and many others. Thisencounter with a healer made me very interested inboth the field of traditional medicine as well as thepeople who practice it.
I was initially very skeptical of traditional medicinebecause many Gambian healers employ supernaturaltechniques in the form of prayers, charms, andincantations in their approach to diagnose and curetheir patients. As a scientist influenced greatly bywestern culture, I remain doubtful about the efficacyof supernatural forces without well-documentedempirical evidence. Traditional medicine, however, iscommon throughout the world and is the precursorof modern medicine. Such universality and importancein the development of modern medicine indicate thattraditional medicine must be at least partially basedon evidence that certain treatments relieve symptomsor cure diseases. But, when I began researching thistopic, I was quickly convinced that many Gambiansview traditional medicine as being every bit as
4Medicine in The Gambia:
Where Technology Meets TraditionRyan Anderson
Advertisement for traditional medicine at Serrekundamarket
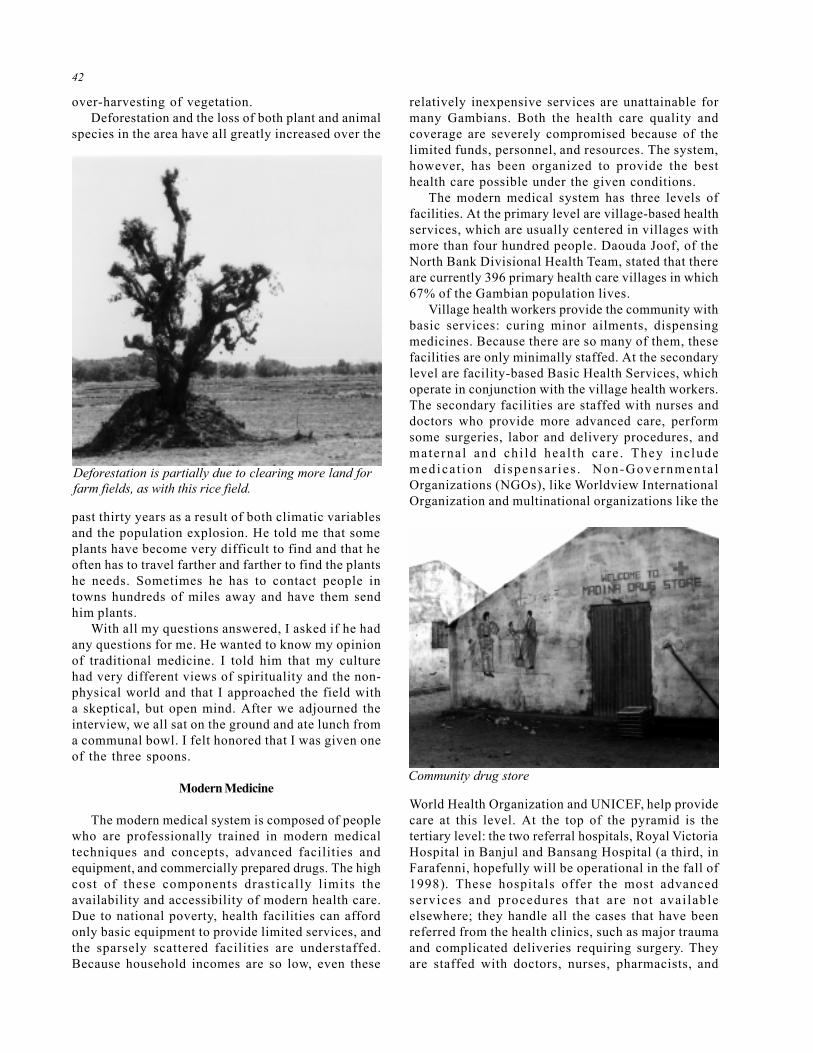
Ryan with herbalist at Serrekunda market
39

40
effective as modern medicine. Practically every time Itold someone that I was studying traditional medicine,he/she would tell me anecdotes about marabouts(people with spiritual powers) healing people whomdoctors could not. Then they would tell me about thetraditional remedies they knew. One evening, I cameback to the hotel with three bundles of sticks that Ihad bought from an herbalist in the Serrekunda market.A Gambian saw what I had and told me how to usethem to cure a long list of ailments (his directionswere identical to those I got from the herbalist) andthen asked if he could have some of the concoctionbecause he wanted to be more powerful.
After having researched the field more extensively,I have found that traditional medicine is common allover the world. For thousands of years, cultureseverywhere have been developing their own uniquehealth care, employing the supernatural as well asthe natural world that surrounds them. While I was in
The Gambia, I studied the full spectrum of traditionalmedicine and healers, but as a chemist I am mostinterested in herbalism, the field of traditional medicinethat employs the use of plants and plant products totreat medical conditions. The reason for this is that Iam interested in medicinal chemistry, and plants arethe foundation of modern medicine; plant chemicalsand synthetic mimics are the active ingredients of one-fourth of all prescription drugs in the U.S. (Plotkin1993:7).
I set out to study traditional medicine, specifically,how it contributes to health care in The Gambia, whatobstacles have prevented the integration of modernand traditional health care sectors in The Gambia, andhow these obstacles might be overcome so that healthcare can be optimized. The goals of this paper are tocontribute to the discussion about what changes canbe implemented to better the health care system and
to provide non-Gambians with educational informa-tion about Gambian health care, culture, and currenthealth issues.
Traditional Medicine
Like many aspects of society in The Gambia, thehealth care system has two primary influences:African culture and European culture. The Africanculture has been developing since humans originated.It has been affected by such movements as thewestward migration of Islam across northern Africaand the dominance of the Malian Empire in thethirteenth century. Western or European culture didnot make its entrance in the area until relativelyrecently, only a few hundred years ago, when thePortuguese first colonized the coastal area in 1455. Inthe late seventeenth century, the Portuguese soldtrading rights to the British and the French, and in1783, the British took sole trading rights. The Gambiawas a British colony until it gained its independencein 1965, but after hundreds of years of occupation byforeign countries, numerous aspects of Europeanculture are prominent but clearly distinct from thenative Gambian ways.
On the roads in the cities, German-made Mercedes Benztaxis speed past hand-made donkey carts; most Gambiansspeak the mother language of their ethnic group (e.g.
Mandinka, Wolof, Fula, Jola and Serahulie), but the nationalofficial language is English. In the hospitals, people take x-rays for broken bones or chloroquine for malaria, yet rightdown the street from the hospital, one may go to a tradi-tional healer such as a bone setter to mend a broken limb.Many people wear jujus, a protective charm prepared by amarabout, to keep away evil spirits, bad luck, and even con-tagious diseases such as malaria.
This co-existence of divergent cultural traditionsis exemplified in The Gambia�s health care system.
Stone circles at Wassu
Horse-drawn cart

41
There are two distinct systems of health care in TheGambia: modern or westernized medicine andtraditional medicine. Traditional medicine refers to thehealth care system that is based on a set of beliefsand associated practices, incorporated to heal the sickand injured, that each generation adopts from theprev ious genera t ion . This sys tem has beendeveloping in The Gambia ever since people firstinhabi ted the region. Most of my exposure totraditional medicine was through meetings with peopleon the street at the markets in Banjul and Serrekunda.In these areas, the population is large enough that itcan suppor t the job of hea l ing as a fu l l - t imeprofession.
Most of the healers I saw were herbalists who saton the side of the street displaying their collectionsof sticks, barks, roots, and leaves, which had medicinalpurposes. I was never able to find one who spokeEnglish, but Dr. Roberts and the occasional friendlypasser-by were able to help me when I wanted to speakwith these healers. I would describe symptoms ofsome diseases for which I wanted cures, and theywould gather different bundles of herbs and explainto me exactly what I had to do with them in order tocure the described illnesses.
Some of the other healers I saw at the markets weremarabouts, who have spiritual powers to heal as wellas to perform other services. One afternoon inSerrekunda, I had a marabout tell me my future.Marabouts say prayers or make jujus for people towear for protection from harm or disease or to helpthem find a job or a spouse. They also use thesepowers to heal the sick.
Most of the healers I met in the Kombo area werefull-time healers, but the majority of healers live inmore rural areas, where there are not enough patientsto necessitate full-time healers. In the small townsand v i l l ages , hea le rs usua l ly had a p r imaryprofession, such as farming or serving as the villagechief. Medicine men are often highly respectedmembers of the communi ty because of the i rsupernatural powers and often have many moreresponsibilities than just healing the ill.
Traditional medicine is not really organized as asystem; there are no records or patient histories, notechnology or collaboration of health care workers.When people get sick or have broken bones, theyconsult a local healer. In some communities there mayonly be a single healer, so healers have to be trainedto handle many types of health problems. However,most healers have a specialty, such as the ability tocure mala r ia o r b roken bones , dysen te ry, o rtuberculosis. If these healers are good enough, theirreputations spread among neighboring villages, andwhen people have ailments in the specialties of a
nearby healer, they may seek out that healer to curethem. The best healers have reputations spanninghundreds of miles, throughout The Gambia and intoSenegal and Mali; patients sometimes travel for daysto find a certain healer.
Healers work in a variety of ways. Some are ableto take care of in-patients for a few days, others treatonly on an out-patient basis. Patients often go to thehealers, and sometimes healers will travel to theirpatients. How they work depends on a variety offactors: how many patients need them, what kind ofhealer they are, where they live, how busy the healersmay be with their other jobs, and other variables aswel l . They a l l have d i ffe ren t spec ia l t i e s andremedies, were trained differently, get their powersfrom different sources, and wil l pass on theirknowledge in a unique way.
One of the healers I interviewed lived in the villageof Njaba Kunda, near Farafenni. Daouda Joof, of theNorth Bank Divisional Health Team (DHT), took meto the healer�s home. I sat down in the shade with thehealer and a couple of Mr. Joof �s co-workers, whoserved as translators. I had not prepared interviewquestions, so I just got basic information about thehealer.
He told me that he inherited his powers and skillsfrom his father and has been working as a healer forover thirty years, but he is also a farmer. He sometimestreats more than ten patients a day and can keep asmall number of patients in his home while he healsthem. His son recently started learning the trade butwill not work alone until his father can no longer work.I have found this to be a common method of passingdown these skills. Many believe that the descendantsof those with supernatural powers will possess thesame gift. This method insures that the number ofhealers remains constant and that this respectedprofession stays in the family. This healer is the fifthgeneration of healers in his family; the profession ispassed from father to son.
I wanted to know if healers ever worked together:collaborate to cure people or share knowledge to makeeach other better healers. My informant had workedwith other healers, and sometimes doctors of modernmedicine, to heal people, but he never shared hisknowledge or learned from other healers. He told methat all healers have confidential practices and keepit that way to protect their family tradition.
I also asked him a few questions about his herb-collecting techniques. He explained that he hadgathered and stored a variety of medicinal herbs andcould give them to pat ients immediately upondiagnosis, but he often had to go out and find theplants that patients needed after he diagnosed them.A major problem currently facing The Gambia is the
42
over-harvesting of vegetation.Deforestation and the loss of both plant and animal
species in the area have all greatly increased over the
past thirty years as a result of both climatic variablesand the population explosion. He told me that someplants have become very difficult to find and that heoften has to travel farther and farther to find the plantshe needs. Sometimes he has to contact people intowns hundreds of miles away and have them sendhim plants.
With all my questions answered, I asked if he hadany questions for me. He wanted to know my opinionof traditional medicine. I told him that my culturehad very different views of spirituality and the non-physical world and that I approached the field witha skeptical, but open mind. After we adjourned theinterview, we all sat on the ground and ate lunch froma communal bowl. I felt honored that I was given oneof the three spoons.
Modern Medicine
The modern medical system is composed of peoplewho are professionally trained in modern medicaltechniques and concepts, advanced facilities andequipment, and commercially prepared drugs. The highcost of these components drastically limits theavailability and accessibility of modern health care.Due to national poverty, health facilities can affordonly basic equipment to provide limited services, andthe sparsely scattered facilities are understaffed.Because household incomes are so low, even these
relatively inexpensive services are unattainable formany Gambians. Both the health care quality andcoverage are severely compromised because of thelimited funds, personnel, and resources. The system,however, has been organized to provide the besthealth care possible under the given conditions.
The modern medical system has three levels offacilities. At the primary level are village-based healthservices, which are usually centered in villages withmore than four hundred people. Daouda Joof, of theNorth Bank Divisional Health Team, stated that thereare currently 396 primary health care villages in which67% of the Gambian population lives.
Village health workers provide the community withbasic services: curing minor ailments, dispensingmedicines. Because there are so many of them, thesefacilities are only minimally staffed. At the secondarylevel are facility-based Basic Health Services, whichoperate in conjunction with the village health workers.The secondary facilities are staffed with nurses anddoctors who provide more advanced care, performsome surgeries, labor and delivery procedures, andmaterna l and chi ld hea l th care . They inc ludemedica t ion d i spensar ies . Non-Governmenta lOrganizations (NGOs), like Worldview InternationalOrganization and multinational organizations like the
World Health Organization and UNICEF, help providecare at this level. At the top of the pyramid is thetertiary level: the two referral hospitals, Royal VictoriaHospital in Banjul and Bansang Hospital (a third, inFarafenni, hopefully will be operational in the fall of1998). These hospitals offer the most advancedservices and procedures that are not avai lableelsewhere; they handle all the cases that have beenreferred from the health clinics, such as major traumaand complicated deliveries requiring surgery. Theyare staffed with doctors, nurses, pharmacists, and
Deforestation is partially due to clearing more land forfarm fields, as with this rice field.
Community drug store

43
laboratory specialists (Grant 1998:1-3).My first exposure to modern health care in The
Gambia was a tour of Royal Victoria Hospital (RVH) inBanjul. This is the larger of two hospitals in thecountry. As we walked through the various wards, Iwas struck by the conditions; there was a thick smellof blood in every room, a few screen doors werefalling off their hinges, and the heat was stifling. Theadult wards consisted of single rooms, in whichtwenty to thirty beds were lined up side by side,scarcely with room for a single visitor. The children�sward was even more crowded. Into small, windowless,poorly ventilated rooms were crammed dozens ofmothers with children in their arms. Most sat or layon the small beds; they looked exhausted from theheat, the waiting, and the anxiety that accompaniesillness.
The main cause for such conditions seems to be alack of resources. RVH is the largest hospital in thecountry, but it is one of only two, which means itmust service more than half the country. The facilitiesare simply not large enough to accommodate all thepatients. The beds are packed into the wards astightly as possible, and there are still too few of them.The health facilities are severely understaffed; thereare not enough trained personnel to take care ofeveryone. One reason for this is that The Gambia doesnot have any institutions for training doctors. Of thedozen or so doctors I met, not one of them was nativeto The Gambia. Most come from Nigeria, Cuba,England, and the U.S.A.
The health care system is also in desperate needof funds. Medical services are heavily subsidized bythe government, and patients are charged to pay fora small portion of the costs. The patient�s cost forstaying in a bed in RVH for a week, including anyservices rendered and medications, is fifty dalasis(D50 = $5 U.S.). The government cannot afford tocontinue to pay the ever-increasing costs of healthcare; Daouda Joof said that patients are being chargedincreasing amounts for medical care in efforts torecover costs. Unfortunately, many Gambians have a
difficult time paying for medical care, even at thepreviously lower rates, and cost-recovery attemptsare reducing the number of people who can affordmodern medical attention.
Problems with Modern Medicine
There are many inherent problems with modernmedic ine in The Gambia tha t prevent i t f romcompletely replacing traditional medicine. Along withthe prohibi t ively high costs of care that weredescribed above, there are several other factorsmaking care inaccessible to much of the population.Due to the very limited funds, personnel, and facilities,those that are available are scattered quite sparinglyacross the country. With only two hospitals in thecount ry, mos t o f the popula t ion mus t t rave lsubstantial distances to get to these tertiary healthfacilities. Someone can travel a hundred miles in theU.S. in less than two hours, but for Gambians, such atrip may take days. Not everyone owns a car or amotorcycle, and very few of the roads are paved.
Unfortunately, those who need to get to a hospitalare usually suffering from the most severe illnesses,which may only be complicated by traveling. The endresult is that the hospitals are not an option for agreat many Gambians.
Coupled with the low availability of modernmedicine is the inability to provide the best carepossible. While many Gambians never get to thehospitals, a very large number still do. The limitedspace cannot always accommodate all the patients.People often have to wait for beds, and they may haveto wait to get medical attention because the hospitalsare understaffed. This shortage of personnel is theresul t of very few people get t ing the t ra iningnecessary to function in hospitals. The few who arequalified are often drastically over-worked but stillonly earn meager salaries because of the limited fundsfor health care. These factors cause a great manyprofessionals to quit their government jobs and openprivate practices or work for NGOs, where they willwork fewer hours and earn better salaries. Those whodo stay must be admired for their devotion to caringfor their fellow Gambians. Coupled with the scarcityof personnel is the shortage of equipment andsupplies. Many patients may not get the medications,operations or other services they need because ofthese shortages caused by a lack of funding. All ofthese shortcomings equate to an unreliable medicalsystem; even if patients travel to the facilities andpay the increasingly high costs of service, there isstill a good chance that they will not receive the carethey need.
With all these problems, it should come as no
The new hospital at Farafenni is not yet operational.

44
surprise that Gambians more often than not choosethe alternative: traditional medicine. During my stayin Bakau, I was out walking one night and cut myhand on the broken glass that looms atop manycompound fences as a security measure. The cut wasvery deep, and Dr. Roberts suggested that he takeme to RVH for stitches. Even though this is the besthealth facility in the country, and stitches are arelatively simple procedure, I was still very reticentto go to the hospital that night. I was paranoid ofgetting diseases from dirty equipment, a painfulsurgery due to a lack of anesthetic, a scarred fingerfrom an incompetent doctor. I probably would havebeen fine to go to the hospital, but these fears werevery real at the time. I chose to dress the woundmyself, partly due to the lack of severity, but largelydue to my lack of confidence in the facilities.
Predominance of Traditional Medicine
After centuries of scientific research contributionsfrom around the world toward the advancement ofmodern medicine, it seems clear that it has thepotential for being a highly effective system. Despitethe superiority of modern medicine, traditionalmedicine is the prevailing system in The Gambia; Mr.Sarr, from the School of Nursing, estimated that sixtypercent of Gambians will go to a traditional healerbefore a modern health facility. Modern medicine hasfailed to replace traditional medicine for severalreasons, not only because of the limitations withmodern medicine in The Gambia, but also becausecer ta in character is t ics of t radi t ional medicinepreclude its extinction from the area.
There are many qualities of traditional medicinethat contribute to its continued popularity in TheGambia. It is much more accessible, both financiallyand in terms of convenience. When people need tosee a healer, they need only to walk down the streetor maybe travel to the next village to find one. Incertain circumstances, people with severe or unusualcases may need to go farther, but these situations arerelatively rare. Also, the cost of traditional medicineis quite low compared to that of modern medicine,and because the government is charging more fortreatment to recover costs, traditional medicine isbecoming even more relatively inexpensive. The feesthat healers charge are usually reasonable. Sincehealers oftentimes have other means of income, theydo not rely on their patients for a steady income;healing practices may not even be profitable. Healersare rarely paid with money, but rather they are givenfood� chickens, bags of rice� or promised servicesas payment for their work.
There are also cultural influences that help
maintain traditional medicine in West African society.There are still Americans who believe in supernaturalpowers, but spiritualism in the U.S. has, for the mostpart, been put to death by the hand of modern science.While the scientific method is the new religion ofwestern cultures, it has not yet thoroughly infiltratedWest Africa. Most Gambians are religious and dobelieve in supernatural powers. For example, manyGambians believe that evil spirits can make a personill, and some healers have mystical powers of prayers,charms, and special plants that can drive away thespirits that bring sickness. Traditional healers employmethods that address what the patients believe to bethe cause of sickness; modern doctors address whatmodern science dictates the causes to be. ThoseGambians who have not been educated about germtheory hold perceptions of diseases that are largelyshared by traditional healers. Such people maydisagree with doctors� explanations for disease andwill be much more likely to seek out traditional healers.Even after years of public health education, manyGambians a re unaware of germ theory andexplanations of contagion.
Not only is the Gambian culture very spiritual, buti t i s a l so t rad i t ional . Through a l l the fore igninfluences� colonialism, imperialism, slave trading,religious missionaries� Gambians have strongly heldand perpe tua ted the i r ind igenous t rad i t ions .Traditional medicine is a prime example of this.Healers, who are usually male, pass down theirknowledge and skills to a single apprentice, usuallythe healer�s son. The strong family bond that existsin The Gambia leads to generation after generation ofhealers in the same family. A healer will take care of acertain region or village, and when he is too old towork, his apprentice takes over his patients. Thehea l ing prac t ice i s passed down to the nex tgeneration, and patients and their children continue
Remains of famous slave factory/fortress on James Island

45
to seek out the same practice and get care from thenew healer. This cycle makes it very difficult formodern medicine to gain acceptance.
This concept of tradition was very apparent in thevillages I visited. I had the opportunity to observevillage life and the role of healers in the communitywhen I t raveled up-country. Since the vi l lagecommunities are small, everyone is close. The healersare highly respected and trusted members of thevillage, and people have faith in their powers. It wouldbe an insult not to go to the local healer.
Week 4
During the fourth week of the trip, all the studentswent their separate ways to work on our projects. OnMonday morning, I took a taxi to the Serrekunda taxipark and found the van that was to take me toFarafenni at some time that day. I waited during thehottest part of the day in a van that had twenty otherpeople in it. My water had to last me all day, so I tooksmall sips to keep from getting dehydrated. There wasa metal bar in my seat back that was making its waythrough my spine and a gas jug at my feet making medizzy from the fumes. There were children crying nextto me or crawling over me to get to their seats whilevenders milled around outside the van and pesteredme through the window. Most of the people were justlooking at me and wondering, I suppose, what a tubabwas doing on a bus by himself headed half way upthe country. I wondered the same thing.
After driving for six hours and waiting anotherhour for the ferry to cross the river, I arrived inFarafenni late that evening. I began wandering aroundthe taxi park asking i f anyone spoke English.Eventually I found where the DHT was located andwalked there to find Daouda Joof. I was extremelyrelieved when I finally found him because it meant Ihad arrived where I had set out to go. I got cleanedup in the room that Mr. Joof gave me and then haddinner and watched a World Cup game with a groupof people who lived at the DHT.
That night I walked around Farafenni to get a latesnack and some water. As I walked back to the DHTthat night, I was amazed at how dark and quiet thetown was. The night sky was perfectly clear, and Icould not hear a sound until I was startled by a dogfight that erupted thirty feet from me. Disturbed bywhat I could make out of the fight with my flashlight,I quickly walked back to my room.
In the morning I interviewed Mr. Joof about healthcare in The Gambia, and then we drove to someneighboring villages to drop off health supplies.Later, we drove to Njaba Kunda, where I conductedan interview with a healer, which I already described.
In the afternoon, I walked around the DHT to seewhat went on there. I ate dinner and watched theWorld Cup with Mr. Joof again and then went to bedvery early, as I was exhausted from the heat and thetraveling.
I got a ride in a DHT vehicle to Kerewan the nextday. I was to meet Momodou Conteh (the Information,Communication and Education Officer for WorldviewVision) there, but he had not yet gotten back fromBanjul, so his colleague, Haruna Kuyateh, showedme around and found a room for me. I got cleaned upin the room, which was as nice as any other place Istayed the whole month. I went to bed having no ideaI was in for a long night. The electricity shut offaround midnight, and the fan, providing a refreshinglycool breeze in which I slept, stopped. When I hadgone to sleep, I thought that the absence of amosquito net would not be a problem because of thefan. The breeze no longer protected me from themosquitoes, and I awoke, shortly thereafter, in a coldsweat to the roar of hungry mosquitoes swarmingaround me. I spent the next six hours huddled beneathmy sheet clutching my bottle of 95% DEET mosquitorepellant. Every few minutes I would peek out fromunder my sweat- and DEET-soaked sheet at thewindow, hoping for a glimpse of sunlight, indicatingthat the night would soon end.
I had breakfast with Mr. Kuyateh, and then wedrove to a few nearby villages. He had to distributeeducational supplies. Then we met with the traditionalhealer Ma Lagi Conteh whom Mr. Kuyateh hadarranged for me to interview. He led us into hiscompound, and we al l sa t down. Mr. Kuyatehintroduced me in Mandinka and explained the natureof our visit to the healer.
Ma Lagi Conteh had been a village herbalist forthe past fifteen years. He told me about his gift as a
Kids watching the World Cup in the compound atFarafenni

46
healer; by looking into a patient�s eye or by holdingthe patient�s hand, he can tell what disease the patienthas. After diagnosing a patient, Ma Lagi goes intothe bush looking for plant remedies. He says thatplants are like people, that they have different statesof mind, sometimes sleeping or relaxing, and he mustwake them up so he can communicate with them. Hesays that a plant will tell him if it will help the patientand if the patient can be treated at all.
These powers were a gift that he learned to usewith the help of his father. Ma Lagi did not have anapprentice at the time of the interview, but his sonoften accompanies him when he collects plants. Heonly has space in his house for one patient at a timeand often takes care of patients for several days. Iasked him about the number of patients he hastreated, and he pulled out a small booklet that had allhis records. He had figures on how many people hehad treated from his village, nearby Farafenni andKerewan, the Kombo area, and southern Senegal.Most of his patients had come to him, but he said hetook regular trips around the country to treat people.
I was curious about his opinion of modernmedicine. He explained that modern medicine is oftenbetter than traditional medicine but that many people,especially in villages, go to healers just because it iseasier. He also said that traditional medicine was fasterand more effective for certain diseases. He did,however, express confidence in modern medicine;when he is unable to treat patients, he refers them tomodern health facilities because he recognizes thatthey have the capacity to treat a larger number ofailments.
After I had asked all my questions, I thanked himprofusely for taking time away from his fields to speakwith me. We exchanged addresses because he wantedto keep in contact with me so that we could maintaina collaborative relationship between healers. Hewanted to teach me more and wanted to learn moreabout western methods of healing. He said that thenext time I was in The Gambia, he would take me intothe bush and show me how he communicated withthe plants and found the right ones.
On the ride back to Kerewan, the bike that Mr.Kuyateh and I were on ran out of gas, and we walkedabout three miles back to town. After the walk in thesweltering afternoon heat, I was ready for my dailyafternoon nap, which I grew to rely on to replenishmy strength, especially up-country where the heat isunrelenting. I left for Banjul later that afternoon. Mr.Kuyateh took me to the taxi park, and I boarded a vanheaded for Barra. The travel was slow for the firsthour because the road was not paved, but we finallygot to the paved section. I got to Barra right as theferry to Banjul was pulling out, so I had to wait two
hours for the next one. I walked around town and metsome people. A local showed me around Fort Bullenand introduced me to a man who had been living in a
tree for the past three decades. I also met somechildren who were very eager to get my address andto give me theirs so we could stay in contact.
I boarded the ferry as the sun was setting. I didn�thave any warm clothes with me, so I shivered as thetemperature dropped and the ocean wind blew. I washappy to be a little cold after being in the desert heatfor the past several days. We finally docked in Banjul,and I caught a taxi to Bakau. By the time I got back tothe hotel, it was nighttime, and I was exhausted. As Ilook back, this was my favorite week of the trip, butat the time, I was happy to be back in Bakau and withthe rest of the group again.
Initiative to Integrate the Medical Systems
Currently the two systems of health care functionrelatively independently of one another, each with itsown advantages as well as disadvantages. There hasbeen a trend in some of Gambia�s neighboring WestAfrican countries to combine these two systems sothat the advantages of each are preserved and theshortcomings of each are eliminated by the presenceof the other. Mr. Joof told me that both Ghana andNiger have worked toward this integration and, as aresult, have two of the best health care systems inWest Africa. Very little has been done in The Gambiato combine the two systems, but, given the currenthealth care needs of a rapidly growing population,integration may be a difficult but essential step toimproving health care.
Though complete integration is a distant goal, The
Out of gas on the Kerewan road

47
Gambia has made efforts with certain programs tocombine traditional and modern medicine. TheTraditional Birth Attendant (TBA) program is anexample of such attempts. TBAs are usually localvillage women who help other village women to delivertheir babies at home. They are nominated for theprogram by the other villagers and are trained bymodern health educators for six to eight weeks todeliver babies in a rural setting and to dispense certainmedications. Aseptic techniques, a pillar of modernmedicine, are also an integral part of the training; manyGambians are not familiar with modern germ theory,and it is very important to teach TBAs how to avoidinfections, which are a significant cause of death inThe Gambia. TBAs are also trained to refer patientsto modern hea l th fac i l i t i e s in the even t o fcomplications during deliveries. Since the TBAs arevillagers, they usually have close relationships withtheir patients and have their trust and confidence.The reasoning behind the TBA program is that theyhave enough training to handle most deliveries andreduce the number of infections, which often lead tocomplications or death, and there are sufficientnumbers of TBAs who are spread across the countrythat most Gambians have access to their services.
By establishing TBAs as one of the links betweenvillagers and health services, health coverage hasimproved through education, communication, andinformation efforts (Use of Village... 1975:78). TheTBA program has met with much success; DaoudaJoof gave me some statistics on the improvement ofheal th care over the past twenty years . Infantmortality has dropped from 267 to 93 per 1000 livebirths. Deaths of children under five years old havedropped from 365 to 123 per 1000. Maternal mortalityhas dropped from 30 to 10 per 1000 births since theinstallation of the TBA program and decentralizationfrom the hospitals to the primary and secondaryhealth services.
This system is a very good example of how thelimited resources available for health care can bedelegated effectively. Since neither the fundingnor the personnel is available to construct healthfac i l i t i e s in every v i l l age , the re mus t becompromises, and the TBA program, where themodern medical system has been able to reach outto virtually every village, has been a success.TBAs are serving as a model whereby the healthcare providers who are already in place, traditionalhealers, are trained by modern medical educatorson how to provide the best care in the rural setting.
Three-Day Workshop
While our group was in Bansang, we visited
the Divisional Health Team based there and met withMargaret Grant, a Peace Corps volunteer stationedthere. When she found out that I was researchingtraditional medicine, she invited me to attend aworkshop for t radi t ional healers organized bymembers of the DHT. I went to the workshop thefollowing day, which was the third and final day ofthis UNICEF-sponsored event. Eleven healers from allover the Central River Division had come to thisworkshop, which focussed on the rapid diagnosis andtreatment of malaria, acute respiratory infection(ARI), and diarrhea.
The session started at 10:00 a.m. as healers slowlycame into the classroom. There were two instructorsin charge. I sat beside one who had offered totranslate for me. There was no single common languageamong the eleven healers at the conference, so theinstructors spoke in Mandinka and then repeatedthemselves in Wolof and Fula.
The goal of the conference was to provide healerswith the information that modern health practitionersuse to diagnose and treat these diseases, three of themost common in The Gambia. The ability of healers todiagnose these diseases is a key step to treating them.There are no effective traditional cures for malariaand ARI, so it is imperative that healers refer patientswho present the symptoms of these diseases tomodern health services. Diarrhea is more complex; thedifficulty is not in diagnosing it but rather determininghow severe the case is and treating it accordingly.Severe diarrhea can be fatal, especially for children,because the body becomes dehydrated very quickly,especially in the tropics. Healers are trained todiagnose cases as either mild or severe and treat mildcases with an oral rehydration mixture of sugar, saltand water. Because this treatment is ineffective withsevere diarrhea, healers are told to refer these cases
Figure 4.1 Home recipe for oral rehydration solution totreat diarrhea

48
to health facilities immediately.After two hours of teaching, there was a question
and answer session. The healers were getting restless,explaining to the instructors that they had been atthe conference for three days and had to get back totheir villages. All had families to care for, many hadfields to work in, and others had civic duties becausethey were village leaders.
Training programs such as this one are verydifficult to organize. Community health educatorshave a hard time getting healers to attend suchprograms. Those who do participate are forced toneglect other responsibilities to their families andcommuni t ies . Funding f rom UNICEF paid fortransportation to and from the workshop, food andlodging for three days for all the healers, instructors�salaries, and materials used. Since resources werelimited, the most famous and respected healers weresolicited for the workshop. The reasoning behind thiswas that these healers would most likely treat thegreatest number of patients. Also, other healers, whoare lesser known, may follow the lead of these healersand become more receptive to future opportunitiesfor similar training. By finding these prominentindividuals, the health educators can hopefullymaximize the benefits derived from training this smallnumber of healers.
Not only is it difficult to convince healers toparticipate, but it is a major task just to find them.There is no licensing or registration of traditionalhealers, so organizers cannot thumb through theyellow pages to find all the healers in a certain region.They often have to travel to the villages and findhealers personally, which is a task complicated bythe fact that many healers are hesitant to come forwardto health officials.
Educators must realize that many healers may see
no personal benefits to modernizing. The majority ofGambians, including those who work in the modernmedical health sector, already go to traditional healersfirst, and many people have faith in the curativepowers of healers, so they will not think a healerincompetent if he fails to cure a disease. Healers mustbe driven by the knowledge that working with modernhealth services is in the best interest of their patients.
Conclusion
With continued efforts, The Gambia can furtherthe integration of modern and traditional medicine.Programs like the training workshop in Bansang areaimed at spreading modern medical techniques andinformation across the country to all health careprov iders . There a re s t i l l many bar r ie r s todisseminating such information. As discussed above,finding healers who are willing to learn is oftendifficult. Many healers are very reluctant to letoutsiders alter healing practices that have beenpassed down through the generations. Also, becausehealers have traditional views about disease beingcaused by spirits or other supernatural powers, theymay be skeptical that modern techniques are moreeffective than their family practices. Even the peoplewho attended the conference in Bansang may decidenot to get involved in the system and not follow anyof the instructions they received. Unfortunately,without fol low-up monitor ing, which requiresadditional resources and personnel, there is no wayof knowing how beneficial the efforts have been.
To remedy this attitude barrier and bridge the gap,the government must take the initiative. Healtheducators must s t ress that healers wil l not bereplaced, that the two systems will work together, witheach doing its part. The modern health system canprovide the training, resources, and technical supportfor local healers. Funding, which is already scarce,will be needed for such increased efforts. Dependingon the success of health system reformations, theymay prove to be cost effective. Preventive health careand education must increase because avoiding diseasesis much cheaper than treating them.
Overcoming barriers created by different attitudes,traditional ideologies, and severe funding shortageswill be very difficult. Gambians strongly cling to theirtraditions, but if they are to improve their health care,this transformation must be everyone�s priority. Whilethese obstacles exist, The Gambia may look toneighboring countries for guidance. The healthsystems in Ghana, Niger, and Nigeria had the sameobstacles but underwent similar changes and havemet with great success.Traditional healer who participated in the UNICEF
workshop in Bansang

49
Acknowledgements
I would like to thank Daouda Joof, of the NorthBank Divisional Health Team in Farafenni for takingcare of me for a few days and for providing a wealth
of information on modern health care in The Gambia.Haruna Kuyateh, of Worldview Vision in Kerewan,was a great guide. I had fun riding around the bushon his motorcycle. Unfortunately, I never got to meetwi th Momodou Conteh , the Informat ion ,Communication and Education Officer for WorldviewVision, in Kerewan, but I did speak with him at lengthin Bakau one morning. Ismaila Njie, the Acting ChiefNursing officer in Banjul, spent several afternoons
The mosque is a central symbol for the country�sspiritual life.
with the group and showed us around the healthfacilities in Banjul. Mr. Sarr and Mrs. Isatou, from theSchool of Nursing in Banjul, also helped to provideinformation. I also want to thank all the healers withwhom I met. I expected them to be protective of theirpractices, but they were all very willing to teach meabout their skills and knowledge, and most wereinterested in my thoughts on the health care in TheGambia. I would like to see them again.
Works Cited
Grant, Margaret. 1998 A Brief and Incomplete Descriptionof the Health Care System in The Gambia. Un-published manuscript.
Plotkin, Mark. 1993 Tales of a Shaman�s Apprentice.Harmondsworth, New York: Penguin Books.
Djukanovic, V. and E.P. Mach (editors) Use of village healthworkers and trained traditional birth attendants in theDepartment of Maradi, Niger. In AlternativeApproaches to Meeting Basic Health Needs inDeveloping Countries. Geneva: World HealthOrganization.
Conteh, Momodou. Personal Interview. 21 June 1998.
Joof, Daouda. Personal Interview. 25 June 1998.
Sarr, Mr. Personal Interview. 11 June 1998.
Some of Ryan�s friends at a drumming session in Bakau
50
Mural of President Yahya Jammeh at Wassu museum
Women�s museum on Goree Island, Senegal