Embed Size (px)
Citation preview

MEDICARE HOSPITAL OUTPATIENT CHANGES
EFFECTIVE JANUARY 1, 2017 (CY 2017)
CRHF Economics & Health PolicyNovember 30, 2016

DISCLAIMER This presentation is intended only for educational use. Any duplication is prohibited without
written consent of the authors. This information does not replace seeking coding advice from the payer and/or your coding staff. The ultimate responsibility for correct coding lies with the provider of services. Please contact your local payer for their interpretation of the appropriate codes to use for specific procedures.
Medtronic makes no guarantee that the use of this information will prevent differences of opinion or disputes with Medicare or other third party payers as to the correct form of billing or the amount that will be paid to providers of service.
CPT copyright 2016 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS/DFARS Restrictions Apply to Government Use. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for the data contained or not contained herein.
Note: CPT® code descriptions may be abbreviated and not listed in their entirety in all cases in this presentation. For full descriptions, please refer to your 2017 CPT code book.
2 CRHF ECONOMICS & HEALTH POLICY

CONTINUING EDUCATION UNITS
This program has prior approval of the American Academy ofProfessional Coders (AAPC) for one continuing education hour. Granting of this prior approval in no way constitutes endorsement by AAPC of the program content or the program sponsor.
The AAPC requires attendees to participate in the entire Web-Ex presentation in order to qualify for the CEU certificate.
This program has prior approval of the American Health Information Management Association (AHIMA) for one continuing education unit. Granting of this prior approval in no way constitutes endorsement by AHIMA of the program content or the program sponsor.
Registered attendees that qualify will receive an email that includes the AAPC and the AHIMA CEU certificates within a couple of weeks.
3 CRHF ECONOMICS & HEALTH POLICY

AGENDA
CY 2017 Updates
APC/C-APC Assignment Changes
OPPS Payment Rate Comparisons
CY 2017 OPPS Regulations
Device Intensive Procedures Site Neutral Payment: Provider-Based Designation
Medicare Coverage Policies
Appendix
Q&A
4 CRHF ECONOMICS & HEALTH POLICY

CY 2017 Updates
5 CRHF ECONOMICS & HEALTH POLICY

UPDATES OPPS payment rates are increasing by 1.7%.
The 7.1% rural adjustment to OPPS payments for Sole Community Hospitals will continue for CY 2017.
Twenty-five New Comprehensive Ambulatory Payment Classifications (C-APCs) added for CY 2017.
Hospitals that do not meet the outpatient quality reporting requirements will see a 2% payment rate reduction.
The CY 2020 payment year and subsequent years will include 2 claims based measures and 5 Outpatient Ambulatory Surgery Consumer Assessment of Healthcare Providers and Systems (OAS CAHPS) Survey-based measures.
The Comprehensive observation services (C-APC 8011) will remain “not applicable” when associated with a surgical procedure.
CMS Fact Sheet and Press Release dated November 1, 2016; Pages 79569, 79583-79585, 79755 of the Federal Register dated November 14, 2016. See Appendix for the links.
6 CRHF ECONOMICS & HEALTH POLICY

INPATIENT VERSUS OUTPATIENT PERCENTAGES1
1 2015 Medicare Physician Part B claims data file (Physician/Supplier Procedure Summary Master File).https://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/NonIdentifiableDataFiles/PhysicianSupplierProcedureSummaryMasterFile.html
7 CRHF ECONOMICS & HEALTH POLICY
CPT Code Brief Description Inpatient % Outpatient %(includes ASC)
33206-33208
Pacemaker system implants
59% 41%
33228 Dual chamber Pacemaker generator replacement
14% 86%
33249 ICD system implants 39% 61%
33263 Dual chamber ICD generator replacement
11% 89%
33282 ILR implant 25% 75%
93656 PVI catheter ablation 18% 72%

APC/C-APC Assignment Changes
8 CRHF ECONOMICS & HEALTH POLICY

APC / C-APC ASSIGNMENT CHANGES for CRHF RELATED PROCEDURE/SERVICES for CY 2017
CPT Code /HCPCS
Brief CPT Code / HCPCS Description
CY 2017 APC/ C-APC Assignment/National Payment1
CY 2016 APC/ C-APC Assignment/National Payment1
Leadless Pacemaker Implant
0387T Transcather insert/replace permanent. leadless pacer, ventricular
5194$14,776
(No CMS coverage yet)
5193$14,612
(No CMS coverage yet)
Transvenous lead repositioning
33215 Reposition previously implanted transvenous pacer or defibrillator lead
5181$2,360
5182$2,247
Removal of an implantable, patient-activated cardiac event recorder
33284 Remove implanted cardiac event recorder - if this is the only procedure performed
5071$539
5073$942
External mobile cardiovascular telemetry with electrocardiographic recording
93229 Up to 30 days technical support. connection and instructions
5733$55
5722$220
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.htmlSelect Hospital Outpatient Regulations and Notices and then CMS-1656 for CY 2017 and CMS-1633 for CY 2016.
9 CRHF ECONOMICS & HEALTH POLICY

APC / C-APC ASSIGNMENT CHANGES for CRHF RELATED PROCEDURE/SERVICES for CY 2017 - continued
CPT Code Brief CPT Code Description CY 2017 APC/ C-APC Assignment/National Payment1
CY 2016 APC/ C-APC Assignment/National Payment1
Echocardiography
93303 Transthoracic echo for congenital anomalies; complete
5524$449
5534$699
93304 Echo for congenital anomalies; follow-up or limited study
5533$417
93306 Echo, complete, w/spectral Doppler and color flow Doppler
5533$417
93307 Echo, complete, w/out spectral Doppler and color flow Doppler
5533$417
93308 Echo; follow-up or limited study 5523$226
5532$154
10 CRHF ECONOMICS & HEALTH POLICY
1 https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.htmlSelect Hospital Outpatient Regulations and Notices and then CMS-1656 for CY 2017 and CMS-1633 for CY 2016.

OPPS PAYMENT RATE COMPARISONS
11 CRHF ECONOMICS & HEALTH POLICY

National Medicare Hospital Outpatient Payment Rates forSignificant Medtronic Therapies1
Therapy and Applicable CPT Codes
CY2013APC
CY2014APC
CY 2015
C-APCs
CY 2016
C-APCs
CY2017
C-APCs
% change13-17
ICDs (33249) $30,680
composite
$32,145
composite
$30,818 $30,490 $30,514 (0.5%)
CRT-Ds(33249 and +33225)
$30,680
composite
$32,145
composite
$30,818 $30,490 $30,514 (0.5%)
Pacemakers (33208) $10,187 $10,588 $9,493 $9,273 $9,410 (7.6%)
CRT-Ps
(33208 and +33225)
$15,280 $15,883 $16,407 $16,914 $16,760 9.7%
PVI Ablations (93656) $11,146
composite
$13,115
composite
$14,362 $15,561 $16,778 50.5%
OUTPATIENT HOSPITAL APC / C-APC PAYMENTS 2013-2017SHOW VARIABILITY
1 Medicare national payment rates indicated are based on information included in the CMS Federal Registers for CY 2013 – 2017 available at:https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html
~ APC: Ambulatory Payment Classification; C-APC: Comprehensive Ambulatory Payment Classification
APC / C-APC payment rates reflect changes based on the Affordable Care Act.
12 CRHF ECONOMICS & HEALTH POLICY

OPPS MEDICARE PAYMENT COMPARISONS - PACEMAKERS:CY 2015 – CY 2017 Comprehensive APCs
Medicare CY 2015-CY 2017 OPPS final rule National Payments from Addendum B, see Appendix for links.
$9,493
$9,273
$9,410
$9,150$9,200$9,250$9,300$9,350$9,400$9,450$9,500$9,550
2015 2016 2017
Initial System Pacemaker Implants: Single Chamber and Dual
Chamber
$16,407
$16,914
$16,760
$16,100$16,200$16,300$16,400$16,500$16,600$16,700$16,800$16,900$17,000
2015 2016 2017
Cardiac ResynchronizationTherapy - Pacemaker (CRT-P)
13 CRHF ECONOMICS & HEALTH POLICY
% increase (decrease) from prior year
• 2016 to 2015: (2.3%)
• 2017 to 2016: 1.5%
% increase (decrease) from prior year
• 2016 to 2015: 3.1%
• 2017 to 2016: (0.9%)

OPPS MEDICARE PAYMENT COMPARISONS - DEFIBRILLATORS:CY 2015 – CY 2017 Comprehensive APCs
$30,818
$30,490$30,514
$30,300
$30,400
$30,500
$30,600
$30,700
$30,800
$30,900
2015 2016 2017
Defibrillator and Cardiac Resynchronization Therapy - Defibrillator (CRT-D)
14 CRHF ECONOMICS & HEALTH POLICY
Medicare CY 2015-CY 2017 OPPS final rule National Payments from Addendum B, see Appendix for links.
% increase (decrease) from prior year
• 2016 to 2015: (1.1%)
• 2017 to 2016: 0.1%

APC/C-APC PAYMENT RATE COMPARISONS
Selected Cardiac Rhythm and Heart Failure (CRHF) National Medicare Payment rates are included in the following table.
These CY 2017 and CY 2016 national payment rates have not been adjusted by any factors (wage index, 2% sequestration adjustment, etc.).
See Appendix for an expansive list of CRHF procedures.
SI: Status Indicator. See Appendix for a detailed description of selected Status Indicators.
15 CRHF ECONOMICS & HEALTH POLICY

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
0387T Insert pacer system; leadless 5194$14,776 (J1)
5193$14,612 (J1)
33208 Insert pacer system; A and V 5223 $9,410 (J1)
5223 $9,273 (J1)
33228 Remove pacer and replace pacer gen.; dual lead system
5223 $9,410 (J1)
5223 $9,273 (J1)
33249 Insert or replace ICD system w/ transvenous leads, single or dual chamber
5232$30,514 (J1)
5232$30,490 (J1)
33263 Remove ICD and replace ICD gen.; dual lead system
5231$22,991 (J1)
5231$21,491 (J1)
33282 Insert patient-activated cardiac event recorder (ILR)
APC 5222$6,974 (J1)
APC 5222$6,697 (J1)
33284 Remove ILR - if this is the only procedure performed
APC 5071$539 (Q2)
APC 5073$942 (Q2)
93656 PVI ablation APC 5213$16,778 (J1)
APC 5213$15,561 (J1)
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B
SELECTED APC/C-APC PAYMENT RATE COMPARISONS1
16 CRHF ECONOMICS & HEALTH POLICY

CY 2017 AMBULATORY SURGICAL CENTER (ASC) FINAL RULEPAYMENT COMPARISON: OPPS VS. ASC:
CPT Code®
Short Description 2017 Final OPPS
Payment1
2017 FinalASC
Payment2
33208 Implant DC PM System $9,410 $7,84833228 Remove/replace dual lead PM
generator$9,410 $7,700
33249 Implant ICD/CRT-D system $30,514 $26,77233263 Remove/replace dual lead ICD
generator$21,991 $19,473
33282 Insert ILR $6,974 $ 6,15233284 Explant ILR – if this is the only
procedure performed$539 $291
1 See Appendix for the link to the CY 2017 OPPS Addendum B2 See Appendix for the link to the CY 2017 ASC Addendum AA
17 CRHF ECONOMICS & HEALTH POLICY

CY 2017 OPPS Regulations
18 CRHF ECONOMICS & HEALTH POLICY

DEVICE INTENSIVE PROCEDURES - CHANGES
Device Intensive calculation and the device offset will be determined at the HCPCS (Healthcare Common Procedure Coding System) level and not at the APC level.
When a device intensive procedure is assigned to an APC that has less than 100 total claims, the payment rate will be based on the “mean cost” instead of the geometric mean cost.
When the device offset table by HCPCS code includes at least a 40% device offset amount, then this procedure is defined as including a costly device.
19 CRHF ECONOMICS & HEALTH POLICY
CMS Fact Sheet dated November 1, 2016; Page 79569 of the Federal Register dated November 14, 2016.See Appendix for the links.

DEVICE INTENSIVE PROCEDURES - CHANGES
New HCPCS C1889: Implantable/insertable device for device intensive procedure not other classified. This C-code should be reported for a device intensive procedure that does
not have any associated claims data at this point in time because it is new.
The device offset percentage for this new device is 41%.
CY 2016 Table 42: Listed applicable APC along with the associated procedure codes that identified “Device Intensive Procedures” where the hospital payment would be adjusted if the hospital receives a credit for the replaced device that is >50% of the replacement device cost. Only these “Device Intensive Procedures” require a HCPCS C-code.
CY 2017: Hospitals should continue to follow correct coding guidelines and include the applicable C-code (device code) when billing.
20 CRHF ECONOMICS & HEALTH POLICY
CMS Fact Sheet dated November 1, 2016; Page 79658-79659 of the Federal Register dated November 14, 2016.See Appendix for the links.

Site Neutral PaymentsProvider-Based Designation
21 CRHF ECONOMICS & HEALTH POLICY

PLACE OF SERVICE (POS) FOR PROVIDER-BASED PHYSICIANS
A Practice designated as office-based reports “POS 11 Office “on the Professional claim form.
Provider-Based Off-Campus or On-Campus professional claim submission1 for:diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services to sick or injured persons who do not require hospitalization or institutionalization. POS 19: Off-Campus Outpatient Hospital POS 22: On-Campus Outpatient Hospital
For On-campus and existing Off-Campus Provider-Based practices (as of November 2, 2015), the hospital portion of the facility claim is paid separately (under OPPS) and the physician portion (professional claim) is reimbursed based on the Medicare Physician Fee Schedule (MPFS) facility rate.
1 Pub 100-04 Medicare Claims Processing, Transmittal 3315 dated August 6, 2015, effective on January 1, 2016 is available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R3315CP.pdfProvider Based CMS Transmittal A-03-030 dated 4.18.2003 is at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/a03030.pdfPub 100-02 Medicare Benefit Policy Manual Chapter 6 Hospital Services Covered Under Part B can be found at:https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c06.pdf
22 CRHF ECONOMICS & HEALTH POLICY
Page 79699-79719 of the Federal Register dated November 14, 2016. See Appendix for the link.

23 CRHF ECONOMICS & HEALTH POLICY
Medicare Regulation: Section 603 of the Bipartisan Budget Act of 2015: Off-campus Provider-based departments that began furnishing services on or after November 2, 2015 are not eligible to be paid under OPPS for services provided effective January 1, 2017.
Medicare classifies these Off-campus Provider-based services as “Non-Excepted.”An Off-campus Provider-based department is still considered a department of the hospital and will be included in the Hospital’s Medicare cost report with this type of designation.
CMS determined that the Medicare payment source for “Non-Excepted” Off-campus departments should be based on the Medicare Physician Fee Schedule (MPFS), however, it is impossible to create a payment structure and claims processing rules in time for CY 2017.The final rule provided an “interim rule” with a comment period that ends on December 31, 2016. CMS plans to review these comments and this may result in changes.
On Campus Provider-based departments or those Off-Campus that were certified by CMS before November 2, 2015 are considered to be “Excepted.”This means the technical component for services provided in these provider-based departments will continue to be paid under OPPS.
SITE NEUTRAL PAYMENT BACKGROUND
Pages 79699-79719 of the Federal Register dated November 14, 2016.See Appendix for the links.

PO MODIFIER FOR OFF-CAMPUS “EXCEPTED” SERVICES
PO Modifier implemented January 1, 2016: Used to designate Services, procedures and/or surgeries furnished at off-campus, provider-based outpatient departments
– PO designated services are excepted.
Reporting the PO modifier1:
Implemented January 1, 2016, and claims submitted with this modifier have been and will continue to be monitored by CMS.
Required to be reported with every code for excepted OP hospital services provided at an off-campus Provider-Based Department (PBD)
Not required for: (see Appendix for definitions of Remote locations and Satellite facilities)
• Remote locations of a hospital• Satellite facilities of a hospital• Emergency department
1PO modifier information: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9097.pdf
24 CRHF ECONOMICS & HEALTH POLICY
Page 79699-79718 of the Federal Register dated November 14, 2016. See Appendix for the link.

NEW: HOSPITAL PN MODIFIER FOR “NON-EXCEPTED SERVICES
The PN Modifier is used by Off-Campus PBDs whose payment is defined as not payable under OPPS, and thus these services are defined as “non-excepted”.
– Non-excepted services performed in these off-campus PBDs are reported with the PN on each claim line of the UB-04, using Bill type 131.
– The modifier will trigger applicable payment for “non-excepted” items and services.
CMS finalized that the MPFS will be the mechanism by which PN identified services will be paid.
The Medicare payment rate for services billed with a PN modifier is an interim final rule and the comment period ends on December 31, 2016. This payment:
– Represents the technical component of Physician Services
– Is adjusted by the Hospital wage index
– Includes OPPS packaging
– For 2017 will be 50% of the OPPS rate, with some exceptions
– Will be included in hospital cost reporting
– May change after CMS reviews the comments
25 CRHF ECONOMICS & HEALTH POLICY
Page 79699-79718 of the Federal Register dated November 14, 2016. See Appendix for the link.

PHYSICIAN OWNED and PROVIDER-BASED “EXCEPTED” ON-CAMPUS EXAMPLES
CPT®
codeCPT Brief Description CY 2017
Medicare National Payment
Physician owned practice and Place of Service 11 “Office”
93283 Dual lead ICD in person programming $82.901 Global
Provider-Based Physician practice and Place of Service 22 “On-Campus Outpatient Hospital” – Modifier PO and Modifier PN are not applicable – “Excepted Service”
93283-26 Dual lead ICD in person programming $58.861 PC
93283 Dual lead ICD in person programming (Technical Component)
$35.132 TCHospital Outpatient APC*
Total Provider-Based On-Campus Payment for an “Excepted Service”
$93.99
Physician Global: PC (Professional Component) plus TC (Technical Component)* Hospital APC: Ambulatory Payment Classification1 Physician payment rate: http://www.cms.gov/apps/physician-fee-schedule/overview.aspx2 Hospital payment rate: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html
26 CRHF ECONOMICS & HEALTH POLICY
Page 79699-79719 of the Federal Register dated November 14, 2016. See Appendix for the link.

PHYSICIAN OWNED and PROVIDER-BASED “NON-EXCEPTED” OFF-CAMPUS EXAMPLES
CPT®
codeCPT Brief Description CY 2017
Medicare National Payment
Physician owned practice and Place of Service 11 “Office”
93283 Dual lead ICD in person programming $82.901 Global
Provider-Based Physician practice and Place of Service 19 “Off-Campus Outpatient Hospital” – Modifier PN is applicable for non-excepted services
93283-26 Dual lead ICD in person programming $58.861 PC
93283 Dual lead ICD in person programming (Technical Component)
$17.562 TC (@ 50%)Hospital Outpatient APC*
Total Provider-Based Off-Campus Payment for a “Non-Excepted Service”
$76.42
Physician Global: PC (Professional Component) plus TC (Technical Component)* Hospital APC: Ambulatory Payment Classification1 Physician payment rate: http://www.cms.gov/apps/physician-fee-schedule/overview.aspx2 Hospital payment rate: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.html
27 CRHF ECONOMICS & HEALTH POLICY
Page 79699-79719 of the Federal Register dated November 14, 2016. See Appendix for the link.

Medicare Coverage Policies
28 CRHF ECONOMICS & HEALTH POLICY

CMS NATIONAL COVERAGE ANALYSISTIMELINE for LEADLESS PACEMAKERS
National Coverage Analysis (NCA) Initiated
Public Comments Due
CMS Staff Review
Draft Decision Memo Posted
Public Comments Due
Final Decision Memo Posted(NCD)
May 18, 2016 June 17, 2016
Maximum 6 Months
Nov. 14, 2016 with a 30-day Comment period
30 Days 30 Days 60 Days Max
By Approximately Feb. 12, 2017
Maximum 9 Months
29 CRHF ECONOMICS & HEALTH POLICY

MEDICARE NCD FOR PACEMAKER IMPLANTS August13, 2013:
Revised NCD in effect for DOS on or after 8/13/2013; NCD 20.8.3
July 6, 2015:Implementation – Claims Processing Rules; Change Request CR 9078, MLN Matters® MM9078 Revised
July 7, 2015:Implementation – Claims Processing rules – Rescinded and Delayed
October 26, 2015:MLN Matters MM9078 article revised
Due to claims processing issues brought to the attention of CMS, MACs will implement this NCD at the local level.
CMS has not published revised claims processing instruction and edits so be sure to contact your local MAC.
See Appendix for links to Transmittal 187 (Includes NCD 20.8.3) and MM9078 RevisedNCD: National Coverage Determination
30 CRHF ECONOMICS & HEALTH POLICY

MAC LOCAL PACEMAKER POLICIES1
State MAC (Medicare Administrative Contractor)
Number
AL, GA, TN Cahaba GBA A54949
KY, OH Cigna Government Services A54961
FL, PR, VI First Coast Service Options A54926
CT, IL, MA, ME, MN, NH, NY, RI, VT, WI
National Government Services(NGS)
A54909
CA, HI, NV Noridian A54929
AK, AZ, ID, MT, ND, OR, SD, UT, WA, WY
Noridian A54931
AR, CO, DE, DC, LA, MD, MS, NJ, NM, OK, PA, TX
Novitas L34833
NC, SC, VA, WV Palmetto GBA A54831
IA, IN, KS, MI, MO, NE Wisconsin Physician Services A54958
1 CMS website: https://www.cms.gov/medicare-coverage-database/search/advanced-search.aspx
31 CRHF ECONOMICS & HEALTH POLICY

CARDIAC PACEMAKER EVALUATION SERVICES NCD §20.8.1 and 20.8.1.1 of CMS PUB. 100-03 The decision as to how often any patient's pacemaker should be monitored is
the responsibility of the patient's physician who is best able to take into account the condition and circumstances of the individual patient.
Transtelephonic monitoring (TTM) Guidelines I and II are for both single and dual chamber pacemakers and are included in this NCD.
Pacemaker clinic* service frequency guidelines for routine monitoring are:
Single chamber: Twice in the first 6 months following implant, then once every 12 months
Dual chamber: Twice in the first 6 months following implant, then once every 6 months
Increased frequency of monitoring must be supported by documented medical necessity.
* Please note that “Pacemaker clinic” also includes “Physician practice” and “Hospital device monitoring departments.” Rev. 182, 05-22-15 is available at:http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/ncd103c1_Part1.pdf
32 CRHF ECONOMICS & HEALTH POLICY

33 CRHF ECONOMICS & HEALTH POLICY
OUTPATIENT HOSPITAL NATIONAL PAYMENT AMOUNTS CARDIAC DEVICE MONITORING
CPT code Assigned Outpatient APC
January-December 2017 Medicare National Payment1
Pacemakers
93279-93281, 93288, 93293, 93296
5741 $35.13
ICDs
93282-93284, 93289, 93296 5741 $35.13
Implantable Cardiovascular Monitor (ICM)
93290, 93299 5741 $35.13
Implantable Loop Recorder (ILR)
93285, 93299 5741 $35.13
93291 5732 $28.37
1 Calendar Year 2017 Hospital APC payments are available at:http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.htmlSee Addendix for CPT code descriptions.

CARDIAC RHYTHM AND HEART FAILURE (CRHF) INFORMATIONCARDIAC RHYTHM AND HEART FAILURE (CRHF) RESOURCES
Join our E-mail ListSubscribe to receive news and updates
www.medtronic.com/crdmreimbursement
CRHF
Economics and Health Policy
Visit our website:www.Medtronic.com/CRDMreimbursement
www.medtronicacademy.com
Email us:[email protected]
CRHF ECONOMICS & HEALTH POLICY34
Call our Coding Hotline:1 (866) 877-4102

CARDIAC RHYTHM AND HEART FAILURE (CRHF) INFORMATION
CRHF ECONOMICS & HEALTH POLICY35
OUR CCP TEAM
Joanne Groenewold Carol Male Laurie Desjardins
CCP: Coding, Coverage and Payment

APPENDIX
36 CRHF ECONOMICS & HEALTH POLICY
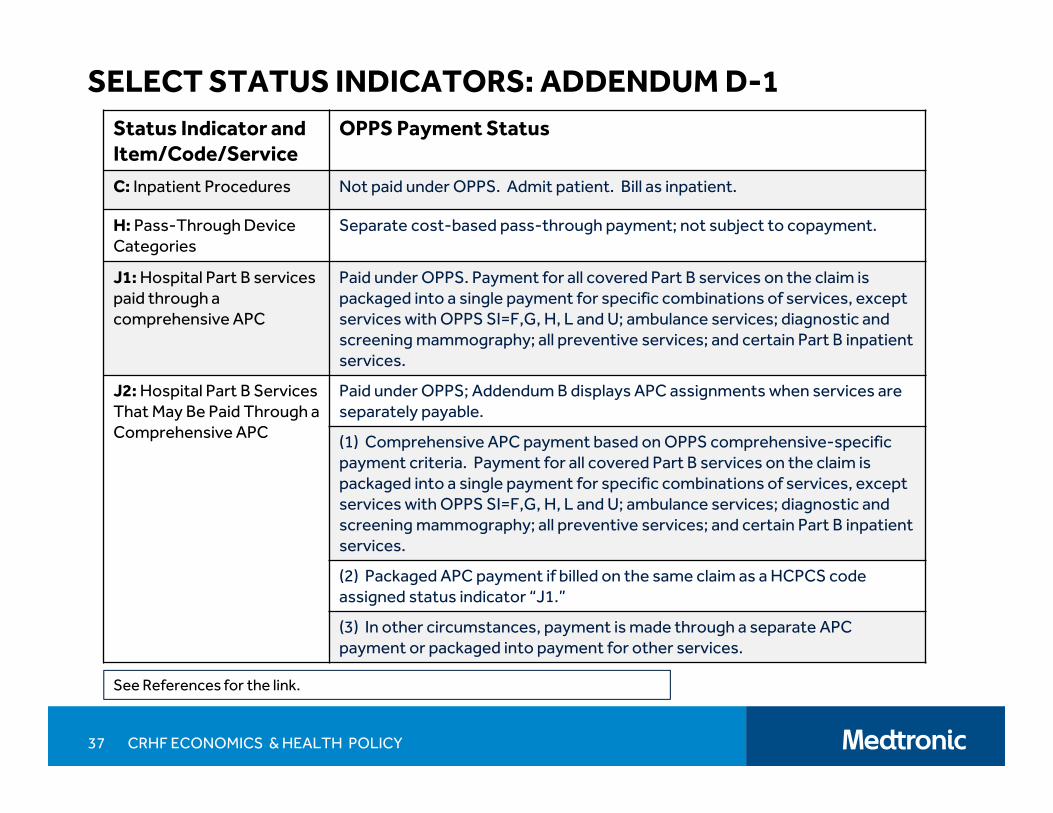
SELECT STATUS INDICATORS: ADDENDUM D-1Status Indicator and Item/Code/Service
OPPS Payment Status
C: Inpatient Procedures Not paid under OPPS. Admit patient. Bill as inpatient.
H: Pass-Through Device Categories
Separate cost-based pass-through payment; not subject to copayment.
J1: Hospital Part B services paid through a comprehensive APC
Paid under OPPS. Payment for all covered Part B services on the claim is packaged into a single payment for specific combinations of services, except services with OPPS SI=F,G, H, L and U; ambulance services; diagnostic and screening mammography; all preventive services; and certain Part B inpatient services.
J2: Hospital Part B Services That May Be Paid Through a Comprehensive APC
Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
(1) Comprehensive APC payment based on OPPS comprehensive-specific payment criteria. Payment for all covered Part B services on the claim is packaged into a single payment for specific combinations of services, except services with OPPS SI=F,G, H, L and U; ambulance services; diagnostic and screening mammography; all preventive services; and certain Part B inpatient services.
(2) Packaged APC payment if billed on the same claim as a HCPCS code assigned status indicator “J1.”
(3) In other circumstances, payment is made through a separate APC payment or packaged into payment for other services.
37 CRHF ECONOMICS & HEALTH POLICY
See References for the link.
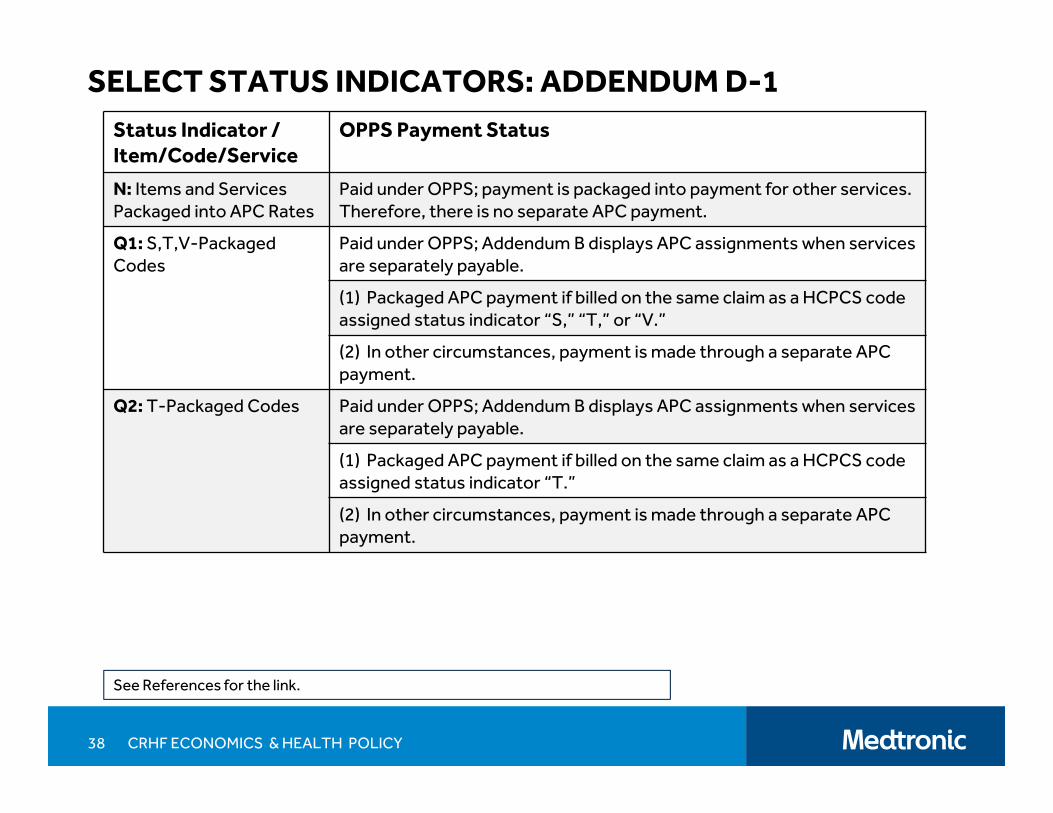
SELECT STATUS INDICATORS: ADDENDUM D-1Status Indicator / Item/Code/Service
OPPS Payment Status
N: Items and Services Packaged into APC Rates
Paid under OPPS; payment is packaged into payment for other services. Therefore, there is no separate APC payment.
Q1: S,T,V-Packaged Codes
Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
(1) Packaged APC payment if billed on the same claim as a HCPCS code assigned status indicator “S,” “T,” or “V.”
(2) In other circumstances, payment is made through a separate APC payment.
Q2: T-Packaged Codes Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
(1) Packaged APC payment if billed on the same claim as a HCPCS code assigned status indicator “T.”
(2) In other circumstances, payment is made through a separate APC payment.
38 CRHF ECONOMICS & HEALTH POLICY
See References for the link.

SELECT STATUS INDICATORS: ADDENDUM D-1
Status Indicator / Item/Code/Service
OPPS Payment Status
S: Procedure or Service, Not Discounted When Multiple
Paid under OPPS; separate APC payment.
T: Procedure or Service, Multiple Procedure Reduction Applies
Paid under OPPS; separate APC payment.
39 CRHF ECONOMICS & HEALTH POLICY
See References for the link.

2017 MEDICARE BENEFICIARY RESPONSIBILITY ORIGINAL MEDICARE
Part B – includes Physician and Outpatient Hospital Services Annual deductible: 2017 $183 vs 2016 $166
Coinsurance: 20% of allowable
Outpatient hospital coinsurance limited to inpatient deductible (per service)
Part A – includes Inpatient Hospital services Per benefit period deductible: 2017 $1,316 vs 2016 $1,288
Co-insurance: none for first 60 days of an admission
For more information about the 2017 Medicare Parts A and B premiums and deductibles access the Federal Register publications dated November 15, 2016:https://www.gpo.gov/fdsys/pkg/FR-2016-11-15/pdf/2016-27389.pdfhttps://www.gpo.gov/fdsys/pkg/FR-2016-11-15/pdf/2016-27388.pdfhttps://www.gpo.gov/fdsys/pkg/FR-2016-11-15/pdf/2016-27425.pdf
40 CRHF ECONOMICS & HEALTH POLICY

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
0387T Insert pacer system; leadless 5194$14,776 (J1)
5193$14,612 (J1)
0388T Remove pacer system; leadless 5182$2,360 (T)
5182$2,247 (T)
33206 Insert pacer system; atrial 5223 $9,410 (J1)
5223 $9,273 (J1)
33207 Insert pacer system; ventricle 5223 $9,410 (J1)
5223 $9,273 (J1)
33208 Insert pacer system; A and V 5223 $9,410 (J1)
5223 $9,273 (J1)
33210 Insert temporary lead, single 5222$6,974 (J1)
5222$6,697 (J1)
33211 Insert temporary leads, dual 5222$6,974 (J1)
5222$6,697 (J1)
33212 Insert pacer gen. only; w/ single lead 5222$6,974 (J1)
5222$6,697 (J1)
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B
APC/C-APC PAYMENT RATE COMPARISONS1
41 CRHF ECONOMICS & HEALTH POLICY

CPT/ HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
33213 Insert pacer gen. only; w/ dual leads 5223 $9,410 (J1)
5223 $9,273 (J1)
33214 Upgrade single pacer to dual pacer 5223 $9,410 (J1)
5223 $9,273 (J1)
33215 Reposition previously placed RA or RV lead 5182$2,360 (T)
5181$863 (T)
33216 Insert single lead, pacer/ICD 5222$6,974 (J1)
5222$6,697 (J1)
33217 Insert 2 leads, pacer/ICD 5222$6,974 (J1)
5222$6,697 (J1)
33218 Repair single lead, pacer/ICD 5221$2,559 (T)
5221$2,490 (T)
33220 Repair 2 leads, pacer/ICD 5221$2,559 (T)
5221$2,490 (T)
33221 Insert pacer gen, only; w/ multiple leads 5224 $16,760 (J1)
5224 $16,914 (J1)
42 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
33222 Relocate skin pocket for pacemaker 5054$1,427 (T)
5054$1,411 (T)
33223 Relocate skin pocket for cardioverter-defibrillator
5054$1,427 (T)
5054$1,411 (T)
33224 Insert LV lead, attach to existing pacer/ICD 5223 $9,410 (J1)
5223 $9,273 (J1)
+33225 Insert LV lead at time of pacer/ICD generator implant
Status N Status N
CRT-P Dual chamber pacemaker and LV lead(33208 and +33225) (Complexity Adjusted)
5224$16,760 (J1)
5224$16,914 (J1)
33226 Reposition previously placed LV lead 5182$2,360 (T)
5182$2,247 (T)
33227 Remove pacer gen. and replace pacer gen.;single lead system
5222 $6,974 (J1)
5222 $6,697 (J1)
43 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
33228 Remove pacer and replace pacer gen.; dual lead system
5223 $9,410 (J1)
5223 $9,273 (J1)
33229 Remove pacer and replace pacer gen.; multiple lead system
5224$16,760 (J1)
5224$16,914 (J1)
33230 Insert ICD gen. only; w/ existing dual leads 5231$22,991 (J1)
5231$21,930 (J1)
33231 Insert ICD gen. only; w/ multiple leads 5232$30,514 (J1)
5232$30,490 (J1)
33233 Remove pacemaker gen. only 5222$6,974 (Q2)
5222$6,697 (Q2)
33234 Remove pacer lead; single 5221$2,559 (Q2)
5221$2,490 (Q2)
33235 Remove pacer leads; dual 5221$2,559 (Q2)
5221$2,490 (Q2)
44 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
33240 Insert ICD gen. only; w/ single lead 5231$22,991 (J1)
5231$21,930 (J1)
33241 Remove ICD gen. only 5221$2,559 (Q2)
5221$2,490 (Q2)
33244 Remove ICD leads; by transvenous extraction 5221$2,559 (Q2)
5221$2,490 (Q2)
33249 Insert or replace ICD system w/ transvenousleads, single or dual chamber
5232$30,514 (J1)
5232$30,490 (J1)
CRT-D Dual chamber ICD and LV lead (33249 and 33225)
5231$30,514 (J1)
5232$30,490(J1)
33262 Remove ICD and replace ICD gen.; single lead system
5231$22,991 (J1)
5231$21,491 (J1)
33263 Remove ICD and replace ICD gen.; dual lead system
5231$22,991 (J1)
5231$21,491 (J1)
33264 Remove ICD and replace ICD gen.; multiple lead system
APC 5232$30,514 (J1)
APC 5232$30,490 (J1)
45 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
33270 Insert/replace subcutaneous defibrillator APC 5232$30,514 (J1)
APC 5232$30,490 (J1)
33271 Insert subcutaneous defibrillator lead APC 5222$6,974 (J1)
APC 5222$6,697 (J1)
33272 Remove subcutaneous defibrillator lead APC 5221$2,559 (J1)
APC 5221$2,490 (J1)
33273 Reposition subcutaneous defibrillator lead APC 5221$2,559 (T)
APC 5221$2,490 (J1)
33282 Insert patient-activated cardiac event recorder (ILR)
APC 5222$6,974 (J1)
APC 5222$6,697 (J1)
33284 Remove ILR APC 5071$539 (Q2)
APC 5073$942 (Q2)
0389T Program device eval; leadless pacemaker APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
0391T Interrogation device eval, leadless pacemaker APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B. The Red font identifies a payment decrease.
46 CRHF ECONOMICS & HEALTH POLICY
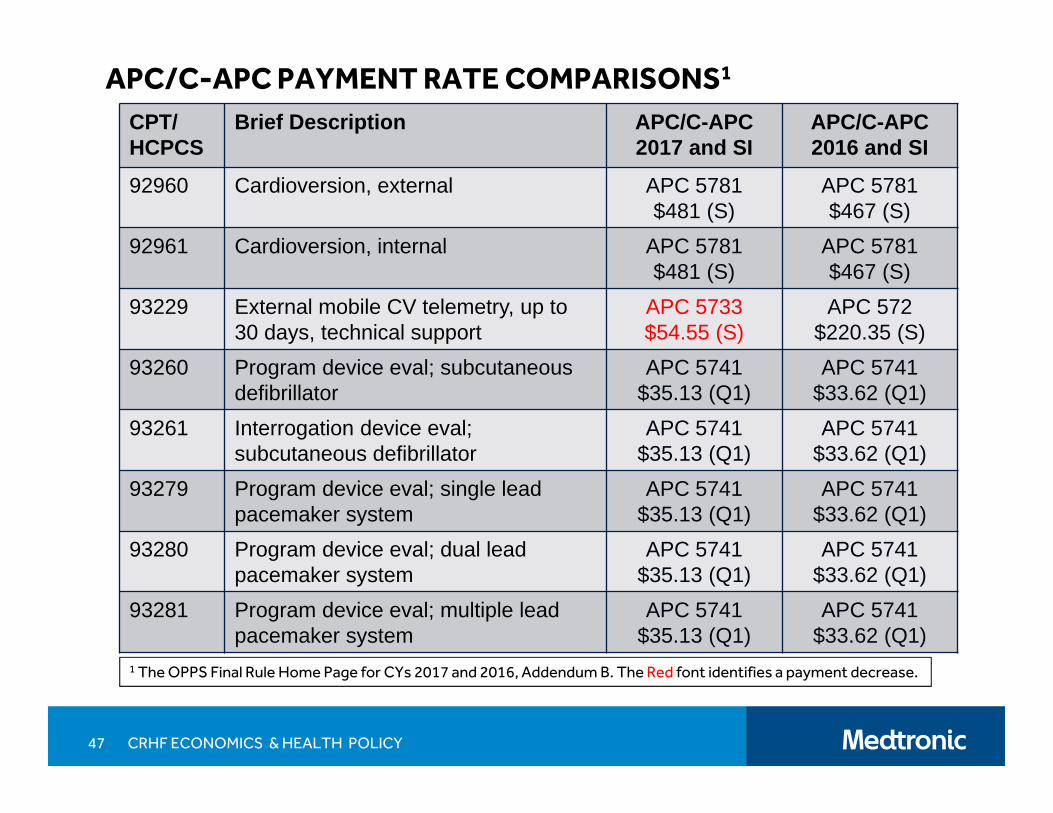
CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
92960 Cardioversion, external APC 5781$481 (S)
APC 5781$467 (S)
92961 Cardioversion, internal APC 5781$481 (S)
APC 5781$467 (S)
93229 External mobile CV telemetry, up to 30 days, technical support
APC 5733$54.55 (S)
APC 572$220.35 (S)
93260 Program device eval; subcutaneous defibrillator
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93261 Interrogation device eval; subcutaneous defibrillator
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93279 Program device eval; single lead pacemaker system
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93280 Program device eval; dual lead pacemaker system
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93281 Program device eval; multiple lead pacemaker system
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
47 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B. The Red font identifies a payment decrease.

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
93282 Program device eval; single lead ICD system APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93283 Program device eval; dual lead ICD system APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93284 Program device eval; multiple lead ICD system
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93285 Program device eval; ILR APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93286 Peri-procedural device eval, pacer Status N Status N
93287 Peri-procedural device eval, ICD Status N Status N
0390T Peri-procedural device eval. leadless pacemaker
Status N Status N
93288 Interrogation device eval; all pacemaker systems
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93289 Interrogation device eval; all ICD systems APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
48 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
93290 Interrogation device eval; implantable CV monitor (ICM)
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93291 Interrogation device eval, ILR APC 5732$28.37 (Q1)
APC 5732$30.51 (Q1)
93292 Interrogation; wearable ICD system APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93293 Transtelephonic pacemaker eval(s), up to 90 days
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93296 Interrogation device eval(s), up to 90 days; pacemaker system or ICD system
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93299 Interrogation device eval(s), (remote), up to 30 days; ILR or ICM
APC 5741$35.13 (Q1)
APC 5741$33.62 (Q1)
93306 Echo, transthoracic, 2D, complete, with spectral and color flow Doppler
APC 5524$449 (S)
APC 5533$417 (Q1)
49 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B. The Red font identifies a payment decrease.

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
93307 Echo, transthoracic, 2D, complete, w/o spectral and color flow Doppler
APC 5524$449 (S)
APC 5533$416 (Q1)
93308 Echo, transthoracic, 2D, follow-up or limited study
APC 5523$226 (S)
APC 5532$154 (Q1)
93350 Stress TTE APC 5524$449 (S)
APC 5533$417 (Q1)
93351 Stress TTE complete APC 5524$449 (S)
APC 5533$417 (Q1)
+93462 Transseptal puncture Status N Status N
93600 Bundle of His recording APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
50 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
93602 Intra-atrial recording APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
93603 Right ventricular recording APC 5211$866 (J1)
APC 5211$845 (J1)
93609 Mapping of tachycardia site(s) Status N Status N
93610 Intra-atrial pacing APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
93612 Intraventricular pacing APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
+93613 3-Dimensional mapping Status N Status N
93615 Esophageal pacing of atrial electrogram APC 5211$866 (J1)
APC 5211$845 (J1)
93616 Esophageal pacing of atrial electrogram; w/recording
APC 5211$866 (J1)
APC 5211$845 (J1)
51 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
93618 Induction of arrhythmia by electrical pacing
APC 5211$866 (J1)
APC 5211$845 (J1)
93619 Comprehensive EP study; without induction of arrhythmia
APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
93620 Comprehensive EP study; with induction of arrhythmia
APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
93624 EP follow-up study with pacing and recording to test effectiveness
APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
93641 EP evaluation of implantable defibrillatorgen. and leads at implant
Status N Status N
93642 EP evaluation of implantable defibrillator, not at implant
APC 5211$866 (J1)
APC 5211$845 (J1)
93644 EP evaluation of subcutaneous implantable defibrillator
Status N Status N
52 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

CPT/HCPCS
Brief Description APC/C-APC 2017 and SI
APC/C-APC 2016 and SI
93650 AV Node ablation APC 5212$5,004 (J1)
APC 5212$4,698 (J1)
93653 VT ablation APC 5213$16,778 (J1)
APC 5213$15,561 (J1)
93654 SVT ablation APC 5213$16,778 (J1)
APC 5213$15,561 (J1)
93656 PVI ablation APC 5213$16,778 (J1)
APC 5213$15,561 (J1)
93660 Tilt table evaluation APC 5723$416 (S)
APC 5723$397 (S)
93724 Electronic analysis of antitachycardiapacemaker system
APC 5743$253 (S)
APC 5743$241 (S)
93745 Set up wearable ICD APC 5743$253 (S)
APC 5743$241 (S)
53 CRHF ECONOMICS & HEALTH POLICY
APC/C-APC PAYMENT RATE COMPARISONS1
1 The OPPS Final Rule Home Page for CYs 2017 and 2016, Addendum B

DEVICE MONITORING
2017 CPT code book
CPT®
Code Description
93279
Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report by a physician or other qualified health care professional; single lead pacemaker system
93280 dual lead pacemaker system
93281 multiple lead pacemaker system
93282
Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report by a physician or other qualified health care professional; single lead transvenous implantable defibrillator system
93283 dual lead transvenous implantable defibrillator system
93284 multiple lead transvenous implantable defibrillator system
54 CRHF ECONOMICS & HEALTH POLICY

DEVICE MONITORING - CONTINUED
CPT®
Code Description
93285
Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, review and report by a physician or other qualified health care professional; implantable loop recorder system
93288Interrogation device evaluation (in person) with analysis, review and report by a physician or other qualified health care professional, includes connection, recording and disconnection per patient encounter; single, dual, or multiple lead pacemaker system
93289single, dual, or multiple lead transvenous implantable defibrillator system, including analysis of heart rhythm derived data elements
93290implantable cardiovascular monitor system, including analysis of 1 or more recorded physiologic cardiovascular data elements from all internal and external sensors
93291implantable loop recorder system, including heart rhythm derived data analysis
93293Transtelephonic rhythm strip pacemaker evaluation(s) single, dual, or multiple lead pacemaker system, includes recording with and without magnet application with analysis, review and report(s) by a physician or other qualified health care professional, up to 90 days
2017 CPT code book
55 CRHF ECONOMICS & HEALTH POLICY
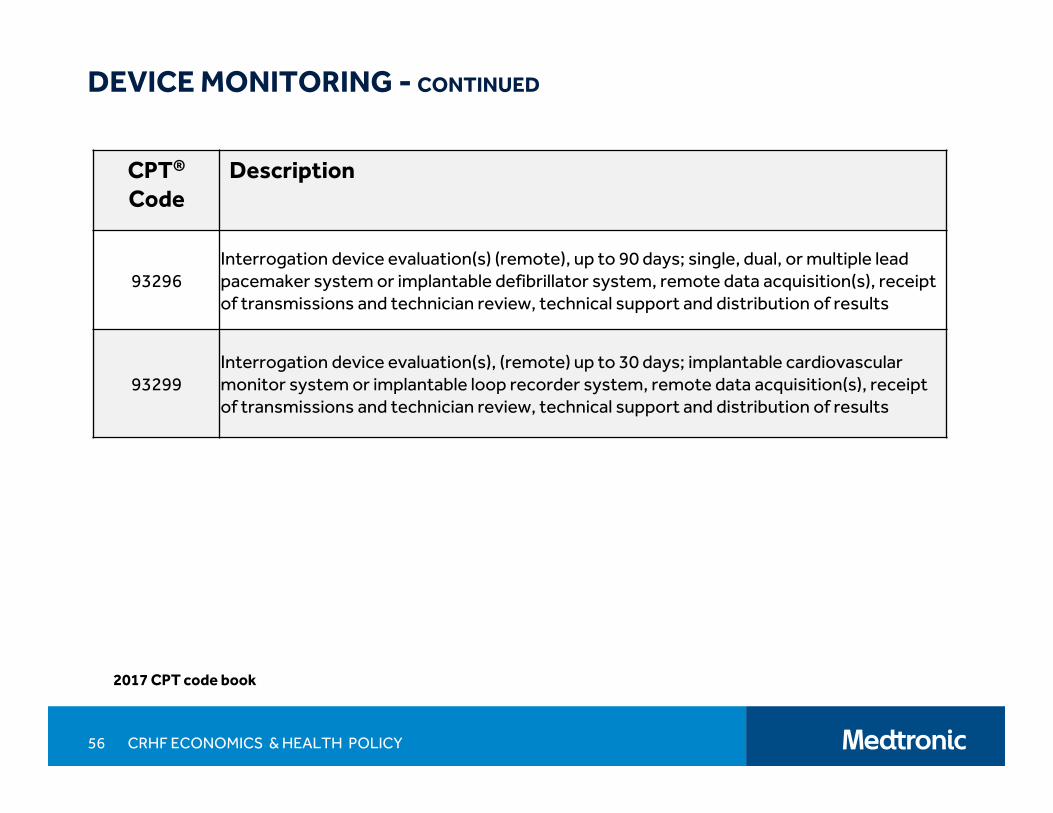
CPT®
Code Description
93296Interrogation device evaluation(s) (remote), up to 90 days; single, dual, or multiple lead pacemaker system or implantable defibrillator system, remote data acquisition(s), receipt of transmissions and technician review, technical support and distribution of results
93299Interrogation device evaluation(s), (remote) up to 30 days; implantable cardiovascular monitor system or implantable loop recorder system, remote data acquisition(s), receipt of transmissions and technician review, technical support and distribution of results
2017 CPT code book
DEVICE MONITORING - CONTINUED
56 CRHF ECONOMICS & HEALTH POLICY

SEVEN MEASURES for PAYMENT YEAR 2020
Claims Based Measures:
OP-35: Admissions and Emergency Department Visits for Patients Receiving Outpatient Chemotherapy; and
OP-36: Hospital Visits after Hospital Outpatient Surgery (NQF #2687)
Survey Based Measures (OAS CAHPS =Outpatient andAmbulatory Surgery Consumer Assessment of Healthcare Providers and Systems) :
OP-37a: OAS CAHPS - About Facilities and Staff;
OP-37b: OAS CAHPS - Communication About Procedure;
OP-37c: OAS CAHPS - Preparation for Discharge and Recovery;
OP-37d: OAS CAHPS - Overall Rating of Facility; and
OP-37e: OAS CAHPS - Recommendation of Facility
57 CRHF ECONOMICS & HEALTH POLICY
Page 79570 of the Federal Register dated November 14, 2016. See Appendix for the link.

TABLE 1: NEW C-APCS FOR CALENDAR YEAR 20171
C-APC CY 2017 C-APC Title Clinical Family
5072 Level 2 Excision/ Biopsy/ Incision and Drainage EBIDX
5073 Level 3 Excision/ Biopsy/ Incision and Drainage EBIDX
5091 Level 1 Breast/Lymphatic Surgery and RelatedProcedures
BREAS
5092 Level 2 Breast/Lymphatic Surgery and RelatedProcedures
BREAS
5112 Level 2 Musculoskeletal Procedures ORTHO
5113 Level 3 Musculoskeletal Procedures ORTHO
5153 Level 3 Airway Endoscopy AENDO
5154 Level 4 Airway Endoscopy AENDO
5155 Level 5 Airway Endoscopy AENDO
EBIDX = Excision/ Biopsy/ Incision and DrainageBREAS = Breast SurgeryORTHO = Orthopedic SurgeryAENDO= Airway Endoscopy
58 CRHF ECONOMICS & HEALTH POLICY
Table 1 is referenced but the text states Table 2. Page 79583-79585 of the Federal Register dated November 14, 2016. See Appendix for the links.

TABLE 1: NEW C-APCS FOR CALENDAR YEAR 2017C-APC CY 2017 APC Title Clinical Family
5164 Level 4 ENT Procedures ENTXX
5191 Level 1 Endovascular Procedures VASCX
5200 Implantation Wireless PA Pressure Monitor WPMXX
5244 Level 4 Blood Product Exchange and RelatedServices
SCTXX
5302 Level 2 Upper GI Procedures GIXXX
5303 Level 3 Upper GI Procedures GIXXX
5313 Level 3 Lower GI Procedures GIXXX
5341 Abdominal/Peritoneal/Biliary and RelatedProcedures
GIXXX
ENTXX = ENT ProceduresVASCX = Vascular ProceduresWPMXX = Wireless PA Pressure MonitorSCTXX = Stem Cell TransplantGIXXX = Gastrointestinal Procedures
59 CRHF ECONOMICS & HEALTH POLICY
Table 1 is referenced but the text states Table 2. Page 79583-79585 of the Federal Register dated November 14, 2016. See Appendix for the links.

TABLE 1: NEW C-APCS FOR CALENDAR YEAR 2017C-APC CY 2017 APC Title Clinical Family
5373 Level 3 Urology & Related Services UROXX
5374 Level 4 Urology & Related Services UROXX
5414 Level 4 Gynecologic Procedures GYNXX
5431 Level 1 Nerve Procedures NERVE
5432 Level 2 Nerve Procedures NERVE
5491 Level 1 Intraocular Procedures INEYE
5503 Level 3 Extraocular, Repair, and Plastic EyeProcedures
EXEYE
5504 Level 4 Extraocular, Repair, and Plastic EyeProcedures
EXEYE
UROXX = Urologic Procedures GYNXX = Gynecologic ProceduresNERVE = Nerve ProceduresINEYE = Intraocular SurgeryEYEYE = Extraocular Ophthalmic Surgery
60 CRHF ECONOMICS & HEALTH POLICY
Table 1 is referenced but the text states Table 2. Page 79583-79585 of the Federal Register dated November 14, 2016. See Appendix for the link.

APPENDIX: REFERENCES
Calendar Year 2017OPPS CY 2017 Federal Register dated November 14, 2016 is available at: https://www.gpo.gov/fdsys/pkg/FR-2016-11-14/pdf/2016-26515.pdf
Data files released with the CY 2017 final rule are available at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.htmlClick on Hospital Outpatient Regulations and Notices, then Regulation No. CMS-1656-FC. The “2017 Final Rule OPPS Addenda” zip file includes: Addendum A (APC payment), Addendum B (HCPCS listing and APC assignment), Addendum C (APC assignment and every HCPCS assigned to that APC), Addendum D-1 (Status Indicators), Addendum J (Complexity Adjusted APC details) and other files.
Press Release:CMS Finalizes Hospital Outpatient Prospective Payment System Changes to Better Support Hospitals and Physicians and Improve Patient Carehttps://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2016-Press-releases-items/2016-11-01.html
Fact Sheet:CMS Finalizes Hospital Outpatient Prospective Payment Changes for 2017https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-11-01-3.html
2017 OPPS HCPCS Offset File (can be found by accessing the CMS Home page, next Medicare, then Hospital Outpatient OPPS, next Annual Policy File and then click on Year 2017:https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Annual-Policy-Files-Items/2017-Annual-Policy-Files.html?DLPage=1&DLEntries=10&DLSort=0&DLSortDir=descending
ASC Addendum AA for CY 2017 can be found at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ASCPayment/index.htmlFirst click on “ASC Regulations and Notices” and then CMS-1656-FC. Scroll down to Related Links and open the Addendum file.
61 CRHF ECONOMICS & HEALTH POLICY

APPENDIX: REFERENCES
Calendar Years 2016 and 2015CY 2016 final rule publication in the Federal Register dated November 13, 2016:https://www.gpo.gov/fdsys/pkg/FR-2015-11-13/pdf/2015-27943.pdf
CY 2016 Addendum B:https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.htmlClick on “Addendum A and Addendum B Updates” and select October 2016 (Release Date), Addendum B (Subject) and 2016 (Year).
CY 2015 final rule publication in the Federal Register dated November 10, 2014:https://www.gpo.gov/fdsys/pkg/FR-2014-11-10/pdf/2014-26146.pdf
CY 2015 Addendum B:https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/index.htmlClick on “Addendum A and Addendum B Updates” and select October 2015 (Release Date), Addendum B (Subject) and 2015 (Year).
Definitions of Remote locations and Satellite locations: Page 66913 of the November 10, 2014 Federal Register publicationof the CY 2015 Final Rule. This file is available at: https://www.gpo.gov/fdsys/pkg/FR-2014-11-10/pdf/2014-26146.pdf
Remote locations of a hospital:hospital campus other than the main hospital campus; facility or an organization that is either created by, or acquired by, a hospital thatis a main provider for the purpose of furnishing Inpatient hospital services under the name, ownership, and financial and administrative control of the main provider.
Satellite locations of a hospital: provides inpatient services in a building also used by another hospital, or in one or more entire buildings located on the same campus as buildings used by another hospital, or in one or more entire buildings located on the same campus as buildings used by another hospital
62 CRHF ECONOMICS & HEALTH POLICY

APPENDIX: REFERENCESOther CMS Links:Proposed Decision Memo for Leadless Pacemakers (CAG-00448N) released on Monday November 14, 2016. This decisionhas a 30-day comment period.https://www.cms.gov/medicare-coverage-database/details/nca-proposed-decision-memo.aspx?NCAId=285
NCD – Transmittal No. 187: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R187NCD.pdf
MM9078 Revised:https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM9078.pdf
63 CRHF ECONOMICS & HEALTH POLICY





























