Medicare and Medical Technology Policy Sean Tunis MD, MSc Chief Medical Officer, CMS February 11,...
45
Medicare and Medical Medicare and Medical Technology Policy Technology Policy Sean Tunis MD, MSc Sean Tunis MD, MSc Chief Medical Officer, Chief Medical Officer, CMS CMS February 11, 2005 February 11, 2005
Medicare and Medical Technology Policy Sean Tunis MD, MSc Chief Medical Officer, CMS February 11, 2005
Medicare and Medical Technology Policy Sean Tunis MD, MSc Chief
Medical Officer, CMS February 11, 2005
Slide 2
Overview Improved health, technology, spending Improved health,
technology, spending Is technological change worth it? Is
technological change worth it? Moving toward transparent, rational
technology policy Moving toward transparent, rational technology
policy Medicare coverage Medicare coverage Linking coverage to
clinical research Linking coverage to clinical research Economic
factors in technology policy Economic factors in technology
policy
Slide 3
Mortality in the 20 th Century Better treatment of
cardiovascular disease, low birth weight infants Reduced infectious
disease mortality (clean water, sewers, antibiotics, better
nutrition)
Slide 4
U.S. Iceland Canada Australi a Netherlands Switzerland Germany
France U.K. Japan Sweden HEALTH SPENDING AND AGING: SELECTED OECD
COUNTRIES 2000 SOURCE: OECD Data, 2002 Now over 15%
Slide 5
Looking Ahead: Expected Cost Increases Estimated cost of family
coverage: $9,160 for 2003 Estimated cost of family coverage: $9,160
for 2003 Figure will rise to $14,545 in 2006 Figure will rise to
$14,545 in 2006 Number of uninsured Americans projected to reach
51.2 to 53.7 mil in 2006, from 41.2 in 2001 (US Census Bureau)
Number of uninsured Americans projected to reach 51.2 to 53.7 mil
in 2006, from 41.2 in 2001 (US Census Bureau) Projected. Source:
Kaiser/HRET Employer Health Benefits, 2001-2003; Towers Perrin 2003
Health Care Cost Survey, Report of Key Findings, 2003; Mercer US
Health Care Survey Results, Mercer HR Consulting, December 9 2002;
Health Care Cost Increases Expected to Continue Double-Digit Pace
in 2003, Hewitt Associates, Oct. 14, 2002. National Business Group
on Health
Slide 6
Technology and Spending David Cutler (1995) estimated 50% David
Cutler (1995) estimated 50% 81% of economists identify technology
as primary cost driver (Fuchs 1996) 81% of economists identify
technology as primary cost driver (Fuchs 1996) Project Hope (March
2001) estimates 25-33% of growth is technology Project Hope (March
2001) estimates 25-33% of growth is technology BCBSA report (Oct
2002) estimates 18% of growth is technology BCBSA report (Oct 2002)
estimates 18% of growth is technology
Slide 7
Health Affairs, Sept/Oct 2001 Is Technological Change in
Medicine Worth It? Cutler and McClellan studied costs and benefits
of technology for 5 conditions Cutler and McClellan studied costs
and benefits of technology for 5 conditions Technological change is
bad only if the cost increases are greater than the benefits.
Technological change is bad only if the cost increases are greater
than the benefits. Heart attack and low birth weight benefits equal
all health spending 1950 1990 Heart attack and low birth weight
benefits equal all health spending 1950 1990 Implication policies
to reduce spending, eliminate waste must consider impact on
innovation Implication policies to reduce spending, eliminate waste
must consider impact on innovation
Slide 8
MedTAP Jan 2003 MedTAP report: Value of Innovation in Health
Care Looked at health spending and outcomes 1980 to 2000 Looked at
health spending and outcomes 1980 to 2000 Diabetes, stroke, MI, and
one other Diabetes, stroke, MI, and one other Annual health
spending increased by 102% over the 20 year period Annual health
spending increased by 102% over the 20 year period Health gains of
$2.40 to $3.00 for each $1 spent Health gains of $2.40 to $3.00 for
each $1 spent Assumes all gains result from spending on health care
Assumes all gains result from spending on health care
Slide 9
CP1027346-1 Percutaneous Coronary Interventions
Slide 10
Percent of Medicare Decedents Admitted to ICU During their
Final Hospitalization (1995-96)
Desirable new/improved Medicare benefits Fast, appropriate
payment for innovation Fast, appropriate payment for innovation
Better screening / prevention Better screening / prevention Improve
safety and quality of care Improve safety and quality of care Avoid
cuts in provider payments Avoid cuts in provider payments Invest in
health IT infrastructure Invest in health IT infrastructure
telemedicine, remote monitoring, e-visits telemedicine, remote
monitoring, e-visits
Slide 13
Slide 14
In need of coherent technology policy framework Technology will
continue to be focus since widely felt to increase costs Technology
will continue to be focus since widely felt to increase costs
Policy framework must: Policy framework must: Ensure quality and
safety of care Obtain good value for health care dollars spent
Provide incentives to use technology appropritely and efficiently
Support informed decision making Support robust environment for
innovation
Slide 15
Today more than ever, we must get more for what we spend on
health care. Weve got to generate valuable innovation in medical
products to reduce errors, complications, and unnecessary care
while improving quality. All thats necessary to understand how
urgent this is to consider the alternative: crude forms of cost
cutting, in ways that reduce the incentives for medical progress
while doing nothing to make our fragmented system work better. We
owe it to the patients we serve to be more clinically sophisticated
than that. Mark McClellan, September 2004
Slide 16
Steps to Medicare Reimbursement Regulatory approval (if
applicable) Regulatory approval (if applicable) Benefit
determination Benefit determination Coverage Coverage Reasonable
and Necessary local vs national Coding Coding Payment Payment
separately billable things bundled payment systems
Slide 17
While I can explain the meaning of life, I dont dare try to
explain Medicare reimbursement.
Slide 18
Major Coverage Issues ICD for primary prevention of SCD ICD for
primary prevention of SCD LVAD LVAD Carotid stents Carotid stents
FDG-PET and other molecular imaging FDG-PET and other molecular
imaging Zevalin, Bexxar, Eloxatin, Erbitux, Avastin, and
anti-cancer pipeline Zevalin, Bexxar, Eloxatin, Erbitux, Avastin,
and anti-cancer pipeline Bariatric surgery Bariatric surgery
Lifestyle interventions Lifestyle interventions Genetic testing
Genetic testing
Slide 19
Improvements since 2000 Coverage process described Coverage
process described With specified timeframes for review Explicit
adoption of rules of evidence Explicit adoption of rules of
evidence Increased technical sophistication Increased transparency
Increased transparency Public advisory committee (MCAC) Decision
memos Highly interactive with stakeholders MMA changes: timeframes,
proposed decisions, guidance docs. MMA changes: timeframes,
proposed decisions, guidance docs.
Slide 20
MEDICARE NATIONAL COVERAGE PROCESS Staff Review Draft Decision
Memorandum Posted National Coverage Request Medicare Coverage
Advisory Committee External Technology Assessment 6 months
Reconsideration Staff Review Public Comments Final Decision
Memorandum and Implementation Instructions 30 days60 days 9 months
Preliminary Meeting Benefit Category Department Appeals Board
Slide 21
Statutory Basis for Coverage Sect. 1862 (a)(1)(A), Title 18,
SSA Sect. 1862 (a)(1)(A), Title 18, SSA ...no payment may be
made... For expenses incurred for items or services.. [which] are
not reasonable and necessary for the diagnosis or treatment of
illness or injury or to improve the functioning of a malformed body
member. ...no payment may be made... For expenses incurred for
items or services.. [which] are not reasonable and necessary for
the diagnosis or treatment of illness or injury or to improve the
functioning of a malformed body member.
Slide 22
Brief History of R&N 1977 Intermediary letters defined
R&N 1977 Intermediary letters defined R&N Safe, effective,
appropriate, not experimental 1989: NPRM issued (legal settlement)
1989: NPRM issued (legal settlement) Safe, effective, appropriate,
cost-effective 1990s: no consensus, no reg 1990s: no consensus, no
reg May 2000: Notice of Intent May 2000: Notice of Intent 1989 NPRM
withdrawn Demonstrated medical benefit, added value Strong
stakeholder opposition Dec 2003: guidance documents (MMA) Dec 2003:
guidance documents (MMA)
Slide 23
Reasonable and Necessary Safe and effective (per FDA, if
applicable) Safe and effective (per FDA, if applicable) Adequate
evidence to conclude that the item or service improves net health
outcomes Adequate evidence to conclude that the item or service
improves net health outcomes emphasis of outcomes experienced by
patients generalizable to the Medicare population as good or better
than current covered alternatives Guidance documents will provide
greater detail on producing adequate evidence Guidance documents
will provide greater detail on producing adequate evidence Open
door call Sept 30
Slide 24
Role of costs in R&N Legislative language and history mute
Legislative language and history mute 1989 NPRM proposed CEA as
criterion 1989 NPRM proposed CEA as criterion Long practice to
ignore costs Long practice to ignore costs In practice high cost
and/or small benefit receive greater scrutiny In practice high cost
and/or small benefit receive greater scrutiny
Slide 25
EBM: Definition ...Evidence-based medicine de-emphasizes
intuition, unsystematic clinical experience, and patho-physiologic
rationale as sufficient grounds for clinical decision making and
stresses the examination of evidence from clinical research.
Evidence-Based Medicine Working Group, JAMA (1992)
Slide 26
Alternatives to EBM Eminence-based medicine Confidence-based
medicine Eloquence-based medicine Vehemence-based medicine
Providence-based medicine Diffidence-based medicine
Nervousness-based medicine Isaacs D, Fitzgerald D. Br Med J
1999;319:1618.
Slide 27
EBM according to Dilbert
Slide 28
Problems with EB coverage Viewed as interference with pt/doc
decisions Viewed as interference with pt/doc decisions Payers
appear to impede innovation in order to control spending / protect
profits Payers appear to impede innovation in order to control
spending / protect profits Insensitive to real barriers to doing
adequate trials, and different challenges by technology Insensitive
to real barriers to doing adequate trials, and different challenges
by technology When evidence limited, may still be strong demand for
technology When evidence limited, may still be strong demand for
technology Does not promote promising but unproven high value
technologies Does not promote promising but unproven high value
technologies
Slide 29
Improving Evidence for Decisions: core concept Links coverage
with prospective data collection Links coverage with prospective
data collection Build on concept of medical necessity Build on
concept of medical necessity Adequate evidence of benefit Adequate
evidence of potential value and provided in appropriately designed
study i.e. promising, important, potentially high value, and under
careful investigation i.e. promising, important, potentially high
value, and under careful investigation Retains EBM as conceptual
framework for coverage and payment Retains EBM as conceptual
framework for coverage and payment
Slide 30
PET for suspected AD Evidence supports clinical utility in
limited context, but not broadly Evidence supports clinical utility
in limited context, but not broadly Non-coverage difficult to
sustain Non-coverage difficult to sustain covers for sx progressive
for 6 months; diagnostic uncertainty (AD vs FTD) covers for sx
progressive for 6 months; diagnostic uncertainty (AD vs FTD)
Broader coverage for use in a large, community-based, practical
clinical trial Broader coverage for use in a large,
community-based, practical clinical trial established precedent for
R&N in trials CMS, AHRQ, Alz Ass, industry, academics have
developed protocols CMS, AHRQ, Alz Ass, industry, academics have
developed protocols
Slide 31
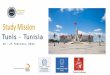
Hazard Ratio = 0.69 Kaplan-Meier Survival by Treatment Group
Adjusted P=0.016 31% reduction in risk of all-cause mortality Total
Mortality CONV: 19.8% ICD: 14.2%
Slide 32
Patients with pacemakers were excluded. CMS analysis of the
MADIT II dataset supplied by Guidant. Kaplan-Meier Estimates of the
Survival Probability in MADIT II for Patients with QRS 120 ms
p-value=0.25
Slide 33
CMS ICD policy ICD June 03 ACC/AHA/NASPE gave this IIa
recommendation ACC/AHA/NASPE gave this IIa recommendation single
trial, possible selection bias need for risk-stratification MCAC
voted 7-0 (evidence adquate) MCAC voted 7-0 (evidence adquate)
MADIT-II prevalence pool 600k (about half >65 - $9B potential
spending) MADIT-II prevalence pool 600k (about half >65 - $9B
potential spending) CMS decided to cover wide-QRS subgroup,
revaluate after SCD-HeFT results CMS decided to cover wide-QRS
subgroup, revaluate after SCD-HeFT results Widely viewed as driven
by economic factors
Slide 34
HR97.5% CIP-Value Amiodarone vs. Placebo1.060.86, 1.300.529 ICD
Therapy vs. Placebo0.770.62, 0.960.007 Sudden Cardiac Death
SCD-HeFT Heart Failure Trial Mortality by Intention-to- treat
Slide 35
Meta-Analysis Results: ICD Therapy for Primary Prevention of
SCD (DCRI, 2004) QRS >= 120
Slide 36
Meta-Analysis Results: ICD Therapy for Primary Prevention of
SCD (DCRI, 2004) QRS < 120ms
Slide 37
CMS ICD policy Jan 2005 Medicare proposed decision to cover
most pts with EF