Embed Size (px)
Citation preview

American Journal of Obstetrics and Gynecology (2005) 193, 1780–4
www.ajog.org
Medical students self-reported work hours: Perceptionversus reality
Colleen Casey, MD,a Sangeeta Senapati, MD,a Casey B. White, PhD,b
Larry D. Gruppen, PhD,c Maya M. Hammoud, MDa
Department of Obstetrics and Gynecology,a Office of Medical Education,b Department of Medical Education,c
University of Michigan Medical School, Ann Arbor, MI
Received for publication February 21, 2005; revised July 3, 2005; accepted August 8, 2005
KEY WORDSQuality of clerkshipMedical student
Work hoursObstetrics and
gynecology
clerkship
Objective: The objective of this study was to compare the students’ actual work hours with their
self-reported work hours during the obstetrics and gynecology clerkship, and to determinewhether the number of hours worked correlate with the amount of ‘‘scut’’ reported or students’rating of the quality of the clerkship.
Study design: Students self-reported work hours were compared against their actual scheduledhours over 2 different academic years. Pearson’s correlation was performed to correlate the actualhours with the amount of reported ‘‘scut’’ work and the overall rating of the quality of the clerkship.
Results: The actual hours per week worked by students averaged 59 hours in 2003 and 48 hours in2004. Students overestimated their work hours both years. Students who worked more hours ratedthe clerkship lower and the quality of the clerkship significantly improved from 2003 to 2004 (4.2 vs3.8 P ! .03).
Conclusion: The majority of third-year students overestimate their work hours in obstetrics andgynecology. The rating of the overall quality of the clerkship increase significantly with fewer hoursworked, and it is not affected by the amount of ‘‘scut’’ work.
� 2005 Mosby, Inc. All rights reserved.
The adoption of the 80-hour work week has resultedin major changes in residency programs in the UnitedStates. Although the airline, trucking, and railwayindustries have a longstanding history of having workhours regulated by the government,1 until recently workhour restrictions in the medical field were not mandated.However, on June 11, 2002, the Accreditation Councilfor Graduate Medical Education (ACGME) passeduniversal standards limiting resident work hours to 80hours per week. These new regulations became effectiveJuly 1, 2003.
Reprints not available from the authors.
0002-9378/$ - see front matter � 2005 Mosby, Inc. All rights reserved.
doi:10.1016/j.ajog.2005.08.017
In February 2004, the Liaison Committee on MedicalEducation (LCME) officials added an annotation re-garding student work hour regulations to its accredita-tion standards.2 They recommended that in addition tomonitoring the amount of classroom time and exami-nation frequency, medical schools should pay attentionto the hours that medical students work during theclinical years and the educational value of their clinicalactivities. Student duty hours should be set taking intoaccount the effects of fatigue and sleep deprivation onlearning and patient care, and medical students shouldnot be required to work longer hours than residents.Soon after this decision by the LCME, the Medical

Casey et al 1781
Student Section (MSS) of the American Medical Asso-ciation (AMA) passed a resolution (MSS Resolution 16:Medical Student Clinical Training and Education Con-dition),3 asking the AMA to encourage the LCME tofollow the lead of the ACGME and include specificlimits on the workload of students in its accreditationstandards. Namely, the resolution for medical studenteducation called for an 80-hour work week, a 24-hourlimit on shifts, and on call no more than once every3 nights.
As early as 2001, 17 of 124 US medical schoolsreported having formal policies on medical studentshours4; however, little is known about the number ofactual or reported student work hours. Burke et al5
published self-reported students’ work hours duringtheir third-year required clerkships; in that study stu-dents indicated an average between 47 to 87 hours perweek depending on the clerkship, with 2 clerkshipsreaching more than 80 hours. A study by Chen et al6
at Harvard Medical School, which asked medical stu-dents to track their daily hours for 1 week, indicatedthat students spent a mean of 74 hours per week in thehospital, with some reporting as many as 106 hours perweek. Mean work hours were dramatically higher oninpatient rotations (90 hours per week) than on outpa-tient rotations (45 hours per week). Students on surgeryrotations worked the longest hours, with a mean ofmore than 94 hours per week spent in the hospitalduring an inpatient rotation.
At the University of Michigan Medical School, whenthe 80-hour work week regulation was adopted forresidents, medical students began to report anecdotallyan increase in their work hours. In addition, curriculumleaders considered adopting similar restrictions on med-ical students work hours, so starting in 2003, students onall required clerkships (internal medicine, surgery, ob-stetrics and gynecology, pediatrics, family medicine,neurology, psychiatry) were asked at the end of therotation to report how many hours they were requiredto be in the hospital per week. When we reviewed thenumber of hours students reported working during theirthird-year obstetric and gynecologic (Ob-Gyn) clerk-ship, we found a sizeable discrepancy between theirreports and the hours they were scheduled to work. Weundertook this study to compare the students’ scheduledor actual hours versus their perceived or self-reportedwork hours in 2003 and 2004. In addition, we wanted todetermine whether the number of work hours correlatedwith the amount of academically unproductive (‘‘scut’’)work they performed, as well as their overall rating ofthe quality of the clerkship.
Methods
At the beginning of the 6-week Ob-Gyn clerkship, allstudents rotating at the University Hospital were given a
work schedule. The schedule specified their daily assign-ments including clinics, inpatient services, and on-callresponsibilities. At the end of the clerkship, all studentscompleted a confidential online survey rating the qualityof their experiences on a 5-point Likert scale from 1 to 5(1 = poor; 5 = excellent). The questionnaire coveredseveral areas of their experiences including the overallquality of the clerkship. They were also asked toestimate the amount of time spent in academicallyunproductive work on a scale of 1 to 5 (1 = too little;3 = just right; 5 = too much), and the average numberof hours per week they were required to be in thehospital or clinics on a 4-point categorical scale asfollows: 1 = less than 60 hours; 2 = 61 to 70 hours; 3 =71 to 80 hours; 4 = more than 80 hours.
To reduce the number of medical student work hours,a student ‘‘night float’’ system was initiated in 2004,where students’ on-call responsibilities consisted of 3consecutive 12-hour night shifts and a 12-hour shift onthe weekend. This replaced the regular once-a-week callfrom the previous year. For the purposes of this study,we considered each year separately because of thecurriculum change. After institutional review boardexemption was obtained, all the students rotating atthe University Hospital (70 in 2003 and 65 in 2004) wereconsidered for the study. Although data were availableon the reported work hours for most of the studentsbecause more than 95% filled out a clerkship survey, wewere unable to retrieve all the actual work schedules thatresulted in available data for 35 students from 2003 and42 students from 2004. In calculating the actual hours,we added the number of hours scheduled each day tocompute the hours per week. The hours per week werethen combined and divided by 6 to calculate averagehours per week worked.
To compare students’ scheduled or actual work hourswith their reported or perceived work hours, the stu-dents were separated into 4 groups on the basis of theirreported work hours category 1 to 4 (1 = !60 hours;2 = 61-70 hours; 3 = 71-80 hours; 4 = 80 hours). Thesewere compared against the actual work hours we calcu-lated for them. In addition, Pearson’s correlation wasperformed to correlate the actual hours with the amountof reported scut work and the overall rating of thequality of the clerkship. The c2 analysis was performedto check if the amount of scut work was differentbetween 2003 and 2004, and an analysis of variancewas performed to compare the overall quality of theclerkship between the 2 years.
Results
The actual hours per week worked by students werehigher in 2003 (59 hours, range: 52-68) than in 2004(48 hours, range: 43-52). The estimated hours workedper week were also much higher in 2003 than 2004 as

1782 Casey et al
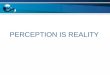
shown in Table I. At least 71% of the students over-estimated their work hours in 2003 compared with 53%of the students in 2004. More interestingly, although theactual hours worked was only about 10 more hours in2003 than it was in 2004, 71% of the students reportedworking more than 70 hours per week in 2003 and only12% reported working that many hours in 2004. Stu-dents reporting less than 60 hours per week were themost accurate, whereas those reporting more than 80hours were the least accurate (Figure).
The actual hours worked correlated negatively withthe overall rating of the quality of the clerkship for 2004and for both years combined. Students who workedmore hours rated the clerkship lower (Table II). Inaddition, the actual number of hours worked correlatedwith the amount of scut work for both years combined.This relationship did not hold true when consideringeach year separately. There was no significant correla-tion between the rating of the overall quality of theclerkship and the amount of scut work. There was nosignificant distribution difference in the amount of scutwork reported between 2003 and 2004; however, theoverall quality of the clerkship did significantly improvein 2004 (4.2 vs 3.8 P ! .03).
Comment
The reported hours and the actual hours worked bymedical students decreased in 2004, which reflected arestructuring of the clerkship. Students no longer hadregular on-call duties, which eliminated 24- to 36-hourshifts, so the actual number of hours worked per weekdecreased from 59 hours in 2003 to 48 hours in 2004.Although a large number of students were still over-estimating their hours in 2004, they represented asmaller percentage than the students who overestimatedtheir hours in 2003. These findings indicate that studentstend to overestimate their work hours more when theyare actually working more. In addition, the more hoursstudents worked, the more scut they reported. This
Table I The reported number of hours and the actual numberof hours worked by third-year medical students during theobstetrics and gynecology clerkship
YearNumber ofstudents
Studentpercent
Reportedhours
Actual hours(range)
2003 1 3 !60 602003 9 26 61-70 59 (53-68)2003 21 60 71-80 59 (52-64)2003 4 11 O80 59 (56-61)
2004 20 48 !60 47 (44-50)2004 17 41 61-70 49 (43-52)2004 5 12 71-80 49 (48-51)2004 0 0 O80 n/a
could indicate that with longer hours, students are eitherspending more time in academically unproductive activ-ities or the students potentially perceive less quality totheir learning experience because they are tired.
Our data show that decreasing the number of workhours and providing a structured schedule contributedto higher student ratings of the Ob/Gyn clerkship.Several studies support the notion that a structuredwork schedule results in increased student satisfactionwith the clerkship.7-10 Considering that the Ob/Gynclerkship has been the lowest rated clerkship by medicalstudents,11 these findings support the importance ofdeveloping a structured clerkship with reasonable hoursto improve the quality of the educational experience forthird-year medical students.
Figure Differences between perceived and actual hoursworked.
Table II Correlations between the overall quality of theclerkship, actual work hours, and amount of scut work
YearActualhours
Amount ofscut work
2003Overall quality of clerkship R = 0.0312* R = 0.0437
P = .859y P = .80Amount of scut work R = 0.2789
P = .105
2004Overall quality of clerkship R = �0.3452 R = �0.0313
P = .025 P = .844Amount of scut work R = 0.0993
P = .531
2003 and 2004Overall quality of clerkship R = �0.2685 R = �0.0488
P = .018 P = .67Amount of scut work R = 0.3004
P = .008
* R = Correlation coefficient.y P = P value.

Casey et al 1783
It is interesting that third-year medical studentsreported spending more hours at the hospital thanwhat they were scheduled to work. We thought oneexplanation for this might be that some students electedto stay and work beyond their scheduled hours. How-ever, a discussion with students and residents indicatedthis was not the case. Although there were occasionalinstances where a student stayed late for an interestingcase, students on gynecology call were also often senthome ahead of schedule. Students were also oftenexcused early and they were not expected to be presentfor gynecology afternoon rounds. In addition, when wecalculated their hours, we tried to err on the side ofoverestimating. For example, we added extra hours forstudents on gynecologic oncology, assuming they stayedlate every day although this only happened on average2 times a week. We also assumed students were at thehospital 1 hour before rounds, which is often not true.In any case, even if there were instances where a studentmight have worked more hours than scheduled, it wasimpossible to account for all of the extra reported hours,which in some cases reached more than 20 hours perweek.
A second possibility might be that students simply arenot able to estimate their work hours accurately. It hasbeen suggested that medical students’ estimations oftheir work hours may actually be a reflection of resi-dents’ work hours observed by the students.12 In addi-tion, previous studies in medical and higher educationhave shown that students are not very accurate in self-assessing their performance.13 When looking specificallyat medical student self-assessment, investigators havefound that the less experience a student has (ie,transitioning from the familiarity of the classroom tothe clinical clerkships), the more self-assessment accur-acy and performance suffers.14 Student work hours canpotentially fall into this category where third-year med-ical students are simply not experienced enough toaccurately assess their hours.
A third possibility for these findings might be thatstudents think they are working more hours becausethey are working hard or because of the many variationsin their daily schedule. The Ob-Gyn clerkship is achallenging clerkship. Students rotate through so manydifferent services including the operating room, laborand delivery, clinic, or night float. Some of these servicescan be very demanding and stressful and students mighttend to recall these experiences more than others. Thismakes it difficult for students to accurately recall thehours by simple reflection. It would be interesting toperform similar analyses for other clerkships, specifi-cally, some of the less demanding ones with moreoutpatient setting and no on-call duties to check if therewould be similar findings.
Whatever the causes are, this perception by medicalstudents that they are working longer hours than they
actually are can have serious implications. The perceivedwork hours required in surgical residencies play a part ina decreased interest in those specialties.12,15,16 Forexample, Miller et al17 surveyed 134 third- and fourth-year medical students to determine factors that influ-enced their decision in choosing a specialty. They foundthat 38% would not consider a residency program witha reputation for long work hours. In a separate study,Miller et al18 looked at how students entering surgicalfields developed their personal rank list. They found that40% of the applicants ranked higher those programsthat strictly adhered to work hour limitations. Thus, asstudents estimate long working long hours in obstetricsand gynecology they might also consider those hoursnegatively as they consider their residency choices. Thisis of special importance to the Ob-Gyn specialty becauseof the decreased number of students choosing to enterthe field.19
The adoption of the 80-hour work week regulationmandated by the ACGME has resulted in a restructur-ing of several residency programs nationwide. Muchdiscussion has been generated about its impact onresidents’ experience and job satisfaction.20,21 Whenconsidering restricted work hours for medical studentswe must remind ourselves of the role of the medicalstudent in the hospitaldmedical students are in thehospital to learn. It is our duty to create an idealenvironment for them to learn by maximizing goodeducational opportunities and minimizing ‘‘scut’’ work.Furthermore, we have to consider how those percep-tions of long hours might be impacting students’ careerchoices especially in obstetrics and gynecology.
References
1. Leach DC. Resident duty hours. The ACGME perspective.
Neurology 2004;62:E1-2.
2. Current LCME Accreditation Standards. Available at: http:
//www.lcme.org/standard.htm. Accessed on February 21, 2005.
3. Student Work Hours. Available at: http://www.ama-assn.org/
ama/pub/category/12141.html. Accessed on February 21, 2005.
4. Barzansky B, Etzel SI. Educational programs in US medical
schools, 2001-2002 [see comment] JAMA 2002;288:1067-72.
5. Burke W, Williams JA, Fenner DE, Hammoud MM. The obstet-
rics and gynecology clerkship: building a better model from past
experience. Am J Obstet Gynecol 2004;191:1772-6.
6. Chen J, Kamath R, Lam A, Litrovnik B, Leight K, Miller S, et al.
How will changes in resident work hours affect medical students?
Curr Surg 2003;60:268-70.
7. Ko CY, Escarce JJ, Baker L, Klein D, Guarino C. Predictors for
medical students entering a general surgery residency: national
survey results. Surgery 2004;136:567-72.
8. Sumit KD, Henke PK, Ailawadi G, Dimick JB, Colleti LM.
Attending, house officer, and medical student perceptions about
teaching in the third-year medical school general surgery clerkship.
J Am Coll Surg 2004;199:932-42.
9. Pogacnik M, Juznic P, Kosorok-Drobnic M, Pogacnik A, Cestnik
V, Kogovsek J, et al. An attempt to estimate student workload.
J Vet Med Educ 2004;31:255-60.

1784 Casey et al
10. Dunn TS, Wolf D, Beuler J, Coddington CC. Increasing recruit-
ment of quality students to obstetrics and gynecology: impact
of a structured clerkship. Am Coll Obstet Gynecol 2004;103:
339-41.
11. AAMC Medical School Graduation Questionnaire, 1978-2003.
Washington (DC): Association of American Medical Colleges;
2003.
12. O’Herrin JK, Lewis BJ, Rikkers LF, Chen H. Why do students
choose careers in surgery? J Surg Res 2004;119:124-9.
13. Ward M, Gruppen L, Regehr G. Measuring self-assessment:
current state of the art. Adv Health Sci Educ 2002;7:63-80.
14. Fitzgerald JT, White CB, Gruppen LD. A longitudinal study of
self-assessment accuracy. Med Educ 2003;37:645-9.
15. Azizzadeh H, McCollum CH, Miller CC 3rd, Holliday KM,
Shilstone HC, Lucci A Jr. Factors influencing career choice
among medical students interested in surgery. Curr Surg 2003;60:
210-3.
16. Gelfand DV, Podnos YD, Wilson SE, Cooke J, Williams RA.
Choosing general surgery: insights into career choices of current
medical students. Arch Surg 2002;137:941-7.
17. Miller G, Bamboat ZM, Allen F, Biernacki P, Hopkins MA,
Gouge TH, et al. Impact of mandatory resident work hour
limitations on medical students’ interest in surgery. J Am Coll
Surg 2004;199:615-9.
18. Miller G, Bamboat ZM, Allen F, Hopkins MA, Gouge TH, Riles
TS, et al. Attitudes of applicants for surgical residency toward
work hour limitations. Am J Surg 2004;188:131-5.
19. National Resident Matching Program Match Data. Advanced
data tables 2004. Available at: http://www.nrmp.org/res_match/
tables/table5_04.pdf. Accessed on February 21, 2005.
20. Killelea BK, Chao L, Scarpinato V. The 80 hour workweek. Surg
Clin N Am 2004;84:1557-72.
21. Lund KJ, Alvero R, Teal SB. Resident job satisfaction: will 80
hours make a difference? Am J Obstet Gynecol 2004;191:1805-10.