Embed Size (px)
Citation preview

Medical Mycology Case Reports 1 (2012) 107–111
Contents lists available at SciVerse ScienceDirect
Medical Mycology Case Reports
2211-75
http://d
n Corr
E-m
journal homepage: www.elsevier.com/locate/mmcr
Granulomatous invasive fungal rhinosinusitis extending into thepterygopalatine fossa and orbital floor: A case report
Tae Hoon Kim, Hyun Uk Jang, Yun Young Jung, Jung Soo Kim n
Department of Otorhinolaryngology—Head and Neck Surgery, School of Medicine, Kyungpook National University, Daegu, Korea
a r t i c l e i n f o
Article history:
Received 1 September 2012
Received in revised form
5 October 2012
Accepted 12 October 2012
Keywords:
Fungi
Sinusitis
Aspergillosis
39/$ - see front matter & 2012 International
x.doi.org/10.1016/j.mmcr.2012.10.004
esponding author. Tel.: þ82 53 200 5777; fax
ail address: [email protected] (J.S. Kim).
a b s t r a c t
Invasive fungal rhinosinusitis is a rare and life-threatening disease. Granulomatous invasive fungal
rhinosinusitis has a time course exceeding 12 weeks, and the destruction of bone progresses slowly.
This disease has been reported primarily in Sudan, India, Pakistan, and the USA; however, it is very rare
in Korea. In this study, we present the case of a 69-year-old man with granulomatous invasive fungal
rhinosinusitis. He was successfully treated with a combination of surgery and itraconazole.
& 2012 International Society for Human and Animal Mycology. Published by Elsevier B.V. All rights
reserved.
1. Introduction
Invasive fungal rhinosinusitis is rare; however, there hasrecently been an increase in the prevalence of invasive fungalrhinosinusitis due to the development of diagnostic techniquesand an increase in the prevalence of diabetes and immunosup-pressive conditions. Invasive fungal rhinosinusitis is a potentiallylife-threatening disease that has high mortality and morbidityrates. Several organisms are known to cause fungal rhinosinusitis,of which Aspergillus is the most common [1].
Fungal rhinosinusitis can be classified as invasive and non-invasive on the basis of the histopathological findings of theinvaded tissue. Invasive fungal rhinosinusitis is further classifiedinto 3 groups: (1) acute invasive (fulminant) fungal rhinosinusitis,(2) granulomatous invasive fungal rhinosinusitis, and (3) chronicinvasive fungal rhinosinusitis [2,3]. Of these, granulomatousinvasive fungal rhinosinusitis has been primarily reported inSudan, but it is also prevalent in India, Pakistan, and the UnitedStates [2,3]. Invasive fungal rhinosinusitis, excluding granuloma-tous invasive fungal rhinosinusitis, mostly occurs in diabetics andother immunosuppressed patients.
In Korea and Japan, several cases of invasive fungal rhinosinu-sitis have been reported [4,5]; however, no case of granulomatousinvasive fungal rhinosinusitis has been reported. In this study, wereport the clinical case of a patient with granulomatous invasivefungal rhinosinusitis involving the pterygopalatine fossa andorbital floor and review the associated literature.
Society for Human and Animal M
: þ82 53 423 4524.
2. Case
A 69-year-old man with a history of hypertension and HBVcarriage was referred to our hospital (Day 0) because of headache,which had persisted for 6 months (Day–180), and left cheeknumbness and pain, which had persisted for 2 months (Day–60).
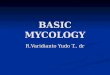
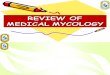
Brain magnetic resonance imaging (MRI) was performed at alocal medical center 3 months (Day–90) before he visited ourhospital; however, the MRI findings were nonspecific. Afterward,he remained under observation without any specific treatment.His headache persisted, and he developed left cheek numbnessand pain. He visited our hospital and underwent MRI andcomputed tomography (CT) serially (Day 0). T2-weighted MRimages revealed hypointense signal opacity that extended intothe posterior wall of the left maxillary sinus. T1-weighted MRimages with gadolinium-enhancement revealed enhanced signalopacity in the left maxillary sinus that extended into the posteriorwall (Fig. 1). CT showed opacity of the left maxillary sinus thatextended into the pterygopalatine fossa, orbital floor, and lateralmaxillary sinus wall (Figs. 2a and b). We performed endoscopicbiopsy and partial debridement under local anesthesia to rule outmalignant disease or mucocele (Day 43). Histological examinationconfirmed tissue invasion by Aspergillus with the formation ofgranuloma and fibrosis (Fig. 3). Granulomatous invasive fungalrhinosinusitis was diagnosed on the basis of clinical and histo-pathologic findings. Follow-up CT (Day 83) revealed exacerbationof the disease condition in comparison to the previous CT (Figs. 2cand d). We performed left partial maxillectomy without orbitalexenteration under general anesthesia because of the relativeease of separating pathologic tissues from the periorbitum(Day 88). The maxillary sinus was filled with granulation and
ycology. Published by Elsevier B.V. All rights reserved.

Fig. 1. (a) Gadolinium-enhanced T1-weighted magnetic resonance (MR) image
showing enhanced opacity with extension into the posterior wall of the left
maxillary sinus. (b) T2-weighted MR image showing hypointensity signal opacity
with extension into the posterior wall of the left maxillary sinus along with the
findings of (a).
T. Hoon Kim et al. / Medical Mycology Case Reports 1 (2012) 107–111108
necrotic tissue. A biopsy specimen confirmed invasion of thesurrounding tissue by Aspergillus.
Systemic amphotericin B (50 mg/day) was intravenously admi-nistered for 10 days after the operation. The patient experiencedintermittent fever (maximum body temperature: 39.2 1C) andchilling sensations during the amphotericin B therapy. Therefore,the antifungal agent was changed to itraconazole. The patientreceived intravenous itraconazole (250 mg/day) for 10 days andoral itraconazole (400 mg/day) for 70 days. Administration of theantifungal agent was stopped after 3 months (Day 180).
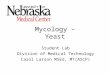
At the 6-month follow-up visit (Day 250), endoscopic findingsrevealed no recurrence and confirmed the healing of the surgical
site (Fig. 4). To date (Day 530), the patient has successfullymanaged postsurgery with amphotericin B followed by itracona-zole, without clinical symptoms or recurrence.
3. Discussion
Three types of fungal rhinosinusitis were identified by McGillin 1980: indolent aspergillosis, aspergilloma, and fulminantaspergillosis [6]. Since the late 1990s, a new type of fungalrhinosinusitis has been reported [2,3]. Fungal rhinosinusitis isclassified as noninvasive and invasive. Invasive fungal rhinosinu-sitis is further classified into 3 types: acute invasive (fulminant)fungal rhinosinusitis, chronic invasive fungal rhinosinusitis, andgranulomatous invasive fungal rhinosinusitis.
Acute invasive (fulminant) fungal rhinosinusitis occurs pre-dominantly in immunocompromised and rarely in immunocom-petent patients, and it has a time course of less than 4 weeks. Itshistopathology includes vascular invasion, inclusion of the carotidarteries and cavernous sinus, vasculitis with thrombosis, hemor-rhage, and tissue infarction [2,3]. Aspergillus fumigatus and sapro-phytic fungi of the order Mucorales are the most commoncausative agents. Chronic invasive fungal rhinosinusitis andgranulomatous invasive fungal rhinosinusitis have a time courseexceeding 12 weeks. The most important differences betweenchronic and granulomatous invasive fungal rhinosinusitis are thehistopathological characteristics. Chronic invasive fungal rhinosi-nusitis is characterized by the dense accumulation of the hyphae,occasional invasion of the blood vessels, and the involvement ofadjacent tissues, whereas granulomatous invasive fungal rhinosi-nusitis is characterized by noncaseating granuloma with foreignbodies or Langhans-type giant cells, occasional vasculitis, vascularproliferation, and perivascular fibrosis [2,3]. The former usuallydevelops in immunocompromised patients who are infected withA. fumigatus, whereas the latter develops in immunocompetentpatients, most commonly in association with Aspergillus flavus
infection.Radiological findings associated with fungal rhinosinusitis gen-
erally include hyperattenuating soft-tissue collection and calcifica-tions in the paranasal sinus on CT scans. Iso or hypointense signalsare observed on T1-weighted MR images, and marked hypointensesignals are observed on T2-weighted MR images. It is known thatCT is superior to MRI for evaluating the sinonasal anatomy andidentifying the surgical landmark. The imaging findings of chronicinvasive fungal rhinosinusitis are similar to those of granulomatousinvasive fungal rhinosinusitis. These findings are analogous tothose of malignant lesions and include bony destruction andextension beyond the sinus. By contrast, acute invasive fungalrhinosinusitis is occasionally associated with very subtle andnonsignificant bone destruction and mucosal thickening comparedto the other types of invasive fungal rhinosinusitis [7].
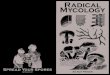
In our case, the patient complained of a headache for 6 monthsand left cheek numbness and pain that had persisted for 2 months.Although 3 months elapsed before a diagnosis of granulomatousinvasive fungal rhinosinusitis was made, this was not consideredconsequential for a chronic disease. The patient was in animmunocompetent state and histological examination withGomori methenamine silver staining revealed tissue invasion bynarrow septate hyphae and 451 dichotomous branching hyphae,which are consistent with Aspergillus; moreover, histologicalexamination with hematoxylin and eosin staining (H&E stain)revealed granuloma and giant cells (Fig. 3). Hence, granulomatousinvasive fungal rhinosinusitis was diagnosed because these find-ings were consistent with its diagnostic criteria.
The standard management of invasive fungal rhinosinusitisinvolves a combination of surgical debridement and antifungal

Fig. 2. (a and b) Initial coronal computed tomography (CT) scans showing opacification of the left maxillary sinus extending into the orbital floor and pterygopalatine
fossa. (c and d) After 2 months, coronal CT scans revealed progressed lesions in comparison to the initial CT findings.
T. Hoon Kim et al. / Medical Mycology Case Reports 1 (2012) 107–111 109
agent administration with the treatment of underlying diseasessuch as immunosuppression and diabetes. Unlike other types ofinvasive fungal rhinosinusitis, granulomatous invasive fungalrhinosinusitis can be treated by surgery alone without the useof antifungal agents [8]. However, DeShazo et al. [3] suggesteddebridement, aeration, and itraconazole as the best treatments forgranulomatous invasive fungal rhinosinusitis.
Invasive fungal rhinosinusitis is primarily treated using anti-fungal agents such as amphotericin B and itraconazole, which areadministered after surgery. It is known that amphotericin B iseffective against species of Aspergillus, which belong to the orderMucorales, and Candida, whereas itraconazole is effective againstAspergillus spp. Itraconazole has relatively fewer side effects thanamphotericin B. Recently, voriconazole has been introduced clini-cally as a new antifungal agent. This is a new broad-spectrum
triazole with efficacy against fungi such as Candida and Aspergillus
spp. Moreover, it is superior to amphotericin B for the treatment ofinvasive aspergillosis with respect to its therapeutic effects [9].Thus, voriconazole has been widely used for the treatment ofinvasive aspergillus rhinosinusitis since its approval by the Foodand Drug Administration. However, we did not use voriconazole inour case because the patient did not satisfy the applicationstandard of Korean health insurance. Although the duration ofantifungal agent administration for the treatment of granuloma-tous invasive fungal rhinosinusitis is disputable, Stringer et al. [10]recommended that patients should receive amphotericin B for6 weeks and should additionally receive amphotericin B oritraconazole for a little longer to control the disease. In our case,the patient received antifungal agents for 3 months and displayedno clinical symptoms or recurrence 18 months after the surgery.

Fig. 3. (a) Fibrosis demonstrated by hematoxylin and eosin (H&E) staining (�100). (b) Granuloma and giant cells as identified by H&E staining (�200). (c) Periodic acid-
Schiff staining showing fungal hyphae in the giant cells (�200). (d) Narrow septate hyphae and 41 dichotomous branching hyphae consistent with Aspergillus, as identified
by Gomori methenamine silver staining (�100).
Fig. 4. Endoscopic findings. We observed healthy mucosa and no recurrence in the
nasal cavity sinus after 6 months of follow-up (Day 250).
T. Hoon Kim et al. / Medical Mycology Case Reports 1 (2012) 107–111110
Therefore, we agree that antifungal agents should be administeredto patients with granulomatous invasive fungal rhinosinusitis formore than 6 weeks.
The prognosis of invasive fungal rhinosinusitis is generallypoor. Although granulomatous invasive fungal rhinosinusitis hasa good prognosis in comparison to the other types of invasivefungal rhinosinusitis, it tends to have a high relapse rate [3].Gumaa et al. [11] reported that itraconazole effectively reduces
the high relapse rate of granulomatous invasive fungal rhinosi-nusitis after surgery.
Because granulomatous invasive fungal rhinosinusitis is extre-mely rare in Korea, its diagnosis is delayed due to the lack ofknowledge about the disease. Despite the increasing lesion size inthe orbital area on follow-up CT scans, we treated this diseasesuccessfully with surgery and antifungal agents (amphotericin Bfollowed by itraconazole), preserving the vision of the patient.Therefore, based on our experience and other studies, we suggestthat a combination of surgery and antifungal agents (amphoter-icin B or itraconazole) is essential for the treatment of granulo-matous invasive fungal rhinosinusitis rather than surgery alone toachieve optimal outcomes.
Author’s contribution
TH Kim: Manuscript writing and data collection; HU Jangand YY Jung: data collection and proofreading of the manuscript;JS Kim: study design and responsibility for the integrity of thecontent of the paper.
All the authors have read and approved the final version of themanuscript.
Conflict of interest
None.

T. Hoon Kim et al. / Medical Mycology Case Reports 1 (2012) 107–111 111
Acknowledgment
There are no acknowledgment for this paper.
References
[1] Stammberger H, Jakse R, Beaufort F. Aspergillosis of the paranasal sinusesx-ray diagnosis, histopathology, and clinical aspects. Annals of OtologyRhinology and Laryngology 1984;93(3 Pt 1):251–256.
[2] Chakrabarti A, Denning DW, Ferguson BJ, Ponikau J, Buzina W, Kita H, et al.Fungal rhinosinusitis: a categorization and definitional schema addressingcurrent controversies. Laryngoscope 2009;119(9):1809–1818.
[3] deShazo RD, Chapin K, Swain RE. Fungal sinusitis. New England Journal ofMedicine 1997;337(4):254–259.
[4] Nakaya K, Oshima T, Kudo T, Aoyagi I, Katori Y, Ota J, et al. New treatment forinvasive fungal sinusitis: three cases of chronic invasive fungal sinusitis treatedwith surgery and voriconazole. Auris, Nasus, Larynx 2010;37(2):244–249.
[5] Kim DK, Nam SK, Lee KA, Cho JHA. Case of chronic invasive fungal sinusitisinvading pterygopalatine fossa. Korean Journal of Otorhinolaryngology—Headand Neck Surgery 2010;53(5):316–319.
[6] McGill TJ, Simpson G, Healy GB. Fulminant aspergillosis of the nose and paranasalsinuses: a new clinical entity. Laryngoscope 1980;90(5 Pt 1):748–754.
[7] Aribandi M, McCoy VA, Bazan III C. Imaging features of invasive andnoninvasive fungal sinusitis: a review. Radiographics 2007;27(5):1283–1296.
[8] Milosev B, el-Mahgoub S, Aal OA, el-Hassan AM. Primary aspergilloma ofparanasal sinuses in the Sudan. A review of seventeen cases. British Journal ofSurgery 1969;56(2):132–137.
[9] Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW,et al. Voriconazole versus amphotericin B for primary therapy of invasive
aspergillosis. New England Journal of Medicine 2002;347(6):408–415.[10] Stringer SP, Ryan MW. Chronic invasive fungal rhinosinusitis. Otolaryngolo-
gic Clinics of North America 2000;33(2):375–387.[11] Gumaa SA, Mahgoub ES, Hay RJ. Post-operative responses of paranasal
Aspergillus granuloma to itraconazole. Transactions of the Royal Society ofTropical Medicine and Hygiene 1992;86(1):93–94.