Embed Size (px)
DESCRIPTION
MEDICAL GRANDROUNDS. SUWENDI, M.D. Medicine Resident January 11, 2007 Ledesma Hall Makati Medical Center. OBJECTIVES. To present a case of infection in an immunocompromised host To be able to do a thorough evaluation of an immunocompromised patient with persistent cough - PowerPoint PPT Presentation
Citation preview

MEDICAL MEDICAL GRANDROUNDSGRANDROUNDS
SUWENDI, M.D.SUWENDI, M.D.Medicine ResidentMedicine Resident
January 11, 2007January 11, 2007Ledesma HallLedesma Hall
Makati Medical CenterMakati Medical Center

OBJECTIVESOBJECTIVES To present a case of infection in an To present a case of infection in an
immunocompromised hostimmunocompromised host
To be able to do a thorough evaluation of an To be able to do a thorough evaluation of an immunocompromised patient with persistent immunocompromised patient with persistent coughcough
To discuss the pathogenesis, clinical To discuss the pathogenesis, clinical manifestations, diagnosis and management of an manifestations, diagnosis and management of an immunocompromised patient with Aspergillosisimmunocompromised patient with Aspergillosis

GENERAL DATAGENERAL DATA
Z. C.Z. C. 47 y/o, female47 y/o, female
single single FilipinoFilipino
business womanbusiness woman

CHIEF COMPLAINTCHIEF COMPLAINT
PancytopeniaPancytopenia

6 months PTA6 months PTA pallor pallor easy bruisability easy bruisability generalized generalized
body weaknessbody weakness
HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS

1 month PTA 1 month PTA consult with AMDconsult with AMD blood transfusion done blood transfusion done advised BMAadvised BMA UTZ abdomen:UTZ abdomen:
slightly enlargedslightly enlarged spleenspleen
ADMISSIONADMISSION
HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS
CBC Hb 6.4Hct 16.4WBC 27550Seg 26Lymph 6Mono 10Platelet 10,000

(-) fever (-) fever (-) cough/colds(-) cough/colds (-) weight loss(-) weight loss (-) nausea/vomiting(-) nausea/vomiting (-) difficulty of breathing(-) difficulty of breathing (-) chest pain(-) chest pain (-) urinary or bowel changes(-) urinary or bowel changes (-) hematochezia / melena(-) hematochezia / melena
REVIEW OF SYSTEMSREVIEW OF SYSTEMS

(-) Hypertension(-) Hypertension(-) Diabetes mellitus(-) Diabetes mellitus(-) Bronchial asthma(-) Bronchial asthma(+) Hyperthyroidism (2003) (+) Hyperthyroidism (2003)
-no maintenance medications -no maintenance medications (-) history of previous operations(-) history of previous operations(-) food / drug allergies(-) food / drug allergies
PAST MEDICAL HISTORYPAST MEDICAL HISTORY

(-) Hypertension (-) Hypertension (-) Diabetes mellitus(-) Diabetes mellitus(+) Chronic kidney disease & PTB –(+) Chronic kidney disease & PTB – father (deceased)father (deceased)(-) Blood dyscrasias(-) Blood dyscrasias
FAMILY MEDICAL HISTORYFAMILY MEDICAL HISTORY

Non-alcoholic beverage drinkerNon-alcoholic beverage drinker
Non-smokerNon-smoker
denies illicit drug use nor environmental denies illicit drug use nor environmental exposure to chemicalsexposure to chemicals
PERSONAL / SOCIAL HISTORYPERSONAL / SOCIAL HISTORY

conscious, coherent, ambulatoryconscious, coherent, ambulatory
BP 110/70, CR 112 bpm, RR 22 cpm, Temp. 37.2 BP 110/70, CR 112 bpm, RR 22 cpm, Temp. 37.2 CC
Good skin turgor, no jaundice, no petechial rashesGood skin turgor, no jaundice, no petechial rashes
Pale palpebral conjunctivae, anicteric scleraePale palpebral conjunctivae, anicteric sclerae
Supple neck, no cervical lymphadenopathiesSupple neck, no cervical lymphadenopathies
PHYSICAL EXAMINATIONPHYSICAL EXAMINATION

Symmetrical chest expansion, no retractions, Symmetrical chest expansion, no retractions, clear breath soundsclear breath sounds
Adynamic precordium, AB 5Adynamic precordium, AB 5thth LICS MCL, LICS MCL, tachycardic, regular rate and rhythm, no tachycardic, regular rate and rhythm, no murmursmurmurs
Soft, flat abdomen,normoactive bowel Soft, flat abdomen,normoactive bowel sounds, non tender, no hepatosplenomegalysounds, non tender, no hepatosplenomegaly
Extremities : no edema, no cyanosis,Extremities : no edema, no cyanosis, pulses full and equalpulses full and equal
PHYSICAL EXAMINATIONPHYSICAL EXAMINATION

Intact memory Pupils 2-3 mm equally reactive to light Full extra ocular muscles (-) Facial asymmetry (-) tongue deviation
5 5
5 5
100% 100%100% 100%
(-) Babinski (-) Brudzinski (-) nystagmus
NEUROLOGIC EXAMINATIONNEUROLOGIC EXAMINATION

SALIENT FEATURESSALIENT FEATURES
47 y.o., female47 y.o., female Pallor, easy bruisability & Pallor, easy bruisability &
generalized body weaknessgeneralized body weakness Ultrasound finding: slightly Ultrasound finding: slightly
enlarged spleenenlarged spleen Pancytopenia on CBCPancytopenia on CBC

Pancytopenia Pancytopenia R/o blood dyscrasiaR/o blood dyscrasia
ADMITTING IMPRESSIONADMITTING IMPRESSION

11stst HOSPITAL DAY HOSPITAL DAYC B CC B C
HbHb 6.76.7 EosEos 11HctHct 21.921.9 MyeloMyelo 11RBCRBC 2.32.3 MetamyeloMetamyelo 33WBCWBC 50.48250.482 StabsStabs 44
Seg/NeutroSeg/Neutro 1919LymphLymph 2121MonoMono 1515BlastBlast 3636Pt countPt count 2000020000

Tranfused 2 unit of PRBC & 4 units of Tranfused 2 unit of PRBC & 4 units of platelet concentrateplatelet concentrate
11stst HOSPITAL DAY HOSPITAL DAY

Bone Marrow Aspiration Biopsy :• myeloblastosis with minimal
maturation with predominantly dysplastic and megaloblastic erythroid
22ndnd HOSPITAL DAY HOSPITAL DAY

Bone Marrow Aspiration Biopsy :• The rest of the hematopoetic cells shows
unremarkable morphology: lymp (5,18%) , mono(0.52%) , plasma cells
(0.52%), macrophages (1.55%) and megakaryocytes (0.0%)
• Histopathological Diagnosis : ACUTE MYELOGENOUS
LEUKEMIA
22ndnd HOSPITAL DAY HOSPITAL DAY

• (+) non-productive cough• (+) low grade fever• decreased breath sounds, RLF• Chest x-ray:
Pleural effusion (R) R/O concomitant pneumonia Cardiomegaly• Levofloxacin 500 mg OD• 2 u pRBC & 2 u platelet concentrate
44THTH HOSPITAL DAY HOSPITAL DAYCBC
Hb 6.6Hct 21.60WBC 12,809Eos 2Myelo 4Metamyelo
1
Stabs 1Seg 24Lymph 15Mono 4Blast 48Platelet 62000

FEVER PATTERNFEVER PATTERN
36.736.836.9
3737.137.237.337.437.537.637.7
1st HD
2nd HD
3rd HD
4th HD
5th HD
6th HD
7th HD
8th HD
9th HD
10th H
D
Levofloxacin

66thth HOSPITAL DAY HOSPITAL DAY
Acute Myelogenous Acute Myelogenous LeukemiaLeukemia
Chemotherapy started:Chemotherapy started: Idarubicin 15 mg IV Idarubicin 15 mg IV
every 24 hrs x 3 d (12mg/mevery 24 hrs x 3 d (12mg/m2 2 x x 1.5)1.5)
Cytarabine 150mg IV Cytarabine 150mg IV every 12 hrs x 7 d (100mg/mevery 12 hrs x 7 d (100mg/m2 2 x x
1.5)1.5)
CBCHb 6.8Hct 23.3WBC 19598Stabs 1Seg 21Lymph 15Mono 2Blast 61Platelet 30000

Serial CBC monitoringSerial CBC monitoringCBC 9th HD 12nd HD
Hb 6.6 6.6Hct 21.7 21.3WBC 1100 940Eos 1 3Seg 74 55Lymph 21 40Mono 4 2Platelet 25000 10000ANC 814 517

1414thth HOSPITAL DAY HOSPITAL DAY (+) episodes of diarrhea(+) episodes of diarrhea On Day # 10 of LevofloxacinOn Day # 10 of Levofloxacin Clostridium difficile toxin test : Clostridium difficile toxin test :
negativenegative LoperamideLoperamide
Started on Diflucan 200 mg po ODStarted on Diflucan 200 mg po OD Acyclovir 400 mg po TIDAcyclovir 400 mg po TID

Serial CBC monitoringSerial CBC monitoring
CBC16th HD 19th HD
Hb 7.2 8.7Hct 22.4 26.6WBC 620 320Seg 8 5Lymph 27 44Mono 1Platelet 30000 45000ANC 50 16

• (+ low-grade fever (Tmax 37.8 C)
• (+) oral ulcers with mucositis
• D/C Levofloxacin• Started on Piperacillin-
tazobactam 4.5 gm IV q8h
1818THTH HOSPITAL DAY HOSPITAL DAY
CBC 19CBC 19thth HD HDHbHb 8.78.7HctHct 26.626.6WBCWBC 320320SegSeg 55LymphLymph 4444MonoMono 11PlateletPlatelet 45,00045,000ANCANC 1616

2323thth HOSPITAL DAY HOSPITAL DAYPost Chemotherapy Bone Marrow BiopsyPost Chemotherapy Bone Marrow Biopsy
Histopathological Diagnosis : Histopathological Diagnosis : Findings consistent with Post Findings consistent with Post
ChemotherapyChemotherapy No evidence of malignancyNo evidence of malignancy

• (+)febrile episodes, T max – 38.5 C• (+)occasional productive cough • harsh breath sounds Blood cs done• D/C Pip tazo• Started on
Cefepime 2 g IV q 12h
3131stst HOSPITAL DAY HOSPITAL DAY
CBC 31st HDCBC 31st HDHbHb 8.58.5HctHct 26.526.5WBCWBC 390390SegSegLymphLymph 4747MonoMono 33PlateletPlatelet 5000050000

FEVER PATTERNFEVER PATTERN
36
36.5
37
37.5
38
38.5
39Temperature
CefepimeLevofloxacin Pip-Tazo

• afebrile, (+) persistent cough• harsh breath sounds - CXR :RUL pneumonia• Blood CS – 1 out of 2 cultures
• (+) for oxacillin resistant, coagulase negative staphylococci• Sensitive to Vancomycin and Linezolid
• Cefepime continued Day # 2• Vancomycin 1gm IV q 12h
3333RDRD HOSPITAL DAY HOSPITAL DAY
CBC 33rd HDCBC 33rd HDHbHb 10.910.9HctHct 33.433.4WBCWBC 920920SegSeg 3131LymphLymph 6464MonoMono 55PlateletPlatelet 3000030000ANCANC 285285

• afebrile• (+)persistence of cough• (+)chest pain, right sided, pleuritic• Chest CT scan was also requested• D/C Vanco,Cefepime, Diflucan & acyclovir • Moxifloxacin 400 mg tab, 1 tab OD
3535THTH HOSPITAL DAY HOSPITAL DAY
CBC 35th HDHb 10.6Hct 32.6WBC 5040Seg 73Lymph 13Mono 11Platelet 56000ANC 3679

FEVER PATTERNFEVER PATTERN
36
36.5
37
37.5
38
38.5
39
28thH
D29t
hHD30t
hHD
31stHD
32ndH
D33r
dHD34t
hHD35t
hHD36t
hHD37t
hHD38t
hHD
Cefepime
Vancomycin
Moxifloxacin

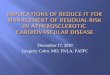
• 2.8 x 2.4 cm. lobulated soft tissue mass density, superior segment of the right lower lobe with ground glass haziness, nodular infiltrates, and air space consolidation with air bronchogram.
• Infectious vs. pulmonary new growth Aspergilloma (fungus-ball), superior segment of the right lower lobe
CHEST CT SCAN RESULT




CT - GUIDED LUNG BIOPSYSmears show ciliated respiratory epithelial cells mixed with abundant inflammatory cells composed of lymphocytes, polymorphonuclears and macrophages.The cellblock shows numerous fungal spores & hyphae mixed with inflammatory cells.
Diagnosis: Cytomorphologic features consistent
with a FUNGAL INFECTION
3838THTH HOSPITAL DAY HOSPITAL DAY

3838thth HOSPITAL DAY HOSPITAL DAY
CHEST X RAYCHEST X RAY No evidence of pneumothoraxNo evidence of pneumothorax
Patient was discharged pending CT guided Patient was discharged pending CT guided lung aspirate culture resultslung aspirate culture results
THM: Moxifloxacin 400 mg OD x 3 more THM: Moxifloxacin 400 mg OD x 3 more daysdays

CT - GUIDED LUNG ASPIRATE :
Light growth of Aspergillus spp.

Patient was started on Voriconazole 200 mg BID
FOLLOW UP TREATMENTFOLLOW UP TREATMENT

FOLLOW UP FOLLOW UP CT SCANCT SCAN




Blood Transfusion Blood Transfusion SummarySummary
11stst HD HD 44thth HD HD 99thth HD HD 1212thth HD HD 1616thth HD HD 1919thth HD HDHbHb 6.76.7 6.66.6 6.66.6 6.66.6 7.27.2 8.78.7HtHt 21.921.9 21.621.6 21.721.7 22.422.4 22.422.4 26.626.6RBCRBC 2.32.3 2.22.2 2.32.3 2.52.5 2.52.5 3.13.1WBCWBC 5048250482 1959819598 11001100 940940 620620 320320PlatelPlateletet
2000020000 3000030000 2500025000 1000010000 3000030000 4500045000
2 u PRBC2 u PRBC4 u 4 u
platelet platelet concentraconcentra
tete
1 u PRBC1 u PRBC2 u 2 u
platelet platelet concentraconcentra
tete
1 u PRBC1 u PRBC2 u 2 u
platelet platelet pharesispharesis
3 u 3 u PRBCPRBC2 u 2 u
platelet platelet pharesispharesis
1 u PRBC1 u PRBC 2 u PRBC2 u PRBC2 unit 2 unit
platelet platelet pharesispharesis

Blood Transfusion Blood Transfusion SummarySummary2222ndnd HD HD 2626thth HD HD 2929thth HD HD 3131stst HD HD 3333rdrd HD HD 3535thth HD HD
HbHb 8.78.7 10.710.7 9.69.6 8.58.5 10.910.9 10.610.6HtHt 27.527.5 34.334.3 30.530.5 26.526.5 33.433.4 32.632.6RBCRBC 3.13.1 3.83.8 3.53.5 3.03.0 3.93.9 3.83.8WBCWBC 590590 670670 510510 390390 920920 50405040PlatelPlateletet
6500065000 7000070000 3000030000 5000050000 3000030000 5600056000
1 u pRBC1 u pRBC1 u 1 u
platelet platelet pharesispharesis
1 unit 1 unit platelet platelet pharesispharesis
2 u 2 u PRBCPRBCGCSFGCSF
1 unit 1 unit platelet platelet pharesispharesis

DISCUSSION DISCUSSION

Immunocompromised HostImmunocompromised Host
DEFINITIONDEFINITION
These patients are defined by their These patients are defined by their susceptibility to infection with organisms susceptibility to infection with organisms of low native virulence for the of low native virulence for the immunologically normal hosts.immunologically normal hosts.

Immunocompromised HostImmunocompromised Host Spectrum of immunocompromised hosts has Spectrum of immunocompromised hosts has
expanded with prolonged survival ofexpanded with prolonged survival of
solid organ and hematopoietic transplant solid organ and hematopoietic transplant recipientsrecipients
congenital immune deficits and autoimmune congenital immune deficits and autoimmune disordersdisorders
epidemic of human immunodeficiency epidemic of human immunodeficiency syndrome/acquired immunodeficiency syndrome syndrome/acquired immunodeficiency syndrome (HIV/AIDS).(HIV/AIDS).

Immunocompromised HostImmunocompromised Host
RISK FACTOR:RISK FACTOR:
Immunosuppressive therapies create Immunosuppressive therapies create a diverse set of immune deficits that a diverse set of immune deficits that create the substrate for opportunistic create the substrate for opportunistic infections. infections.

Most Common Organisms Most Common Organisms in Immunocompromised in Immunocompromised HostHost
Conventional bacteria Conventional bacteria — 37% — 37%
Fungi —14 %Fungi —14 %
Viruses — 15 % Viruses — 15 %
Pneumocystis Pneumocystis carinii/jiroveci — 8 %carinii/jiroveci — 8 %
Nocardia asteroidesNocardia asteroides — — 7 % 7 %
Mycobacterium Mycobacterium tuberculosis — 1 % tuberculosis — 1 %
Mixed infections - 20% Mixed infections - 20%

CHEMOTHERAPEUTIC AGENTS: EFFECT CHEMOTHERAPEUTIC AGENTS: EFFECT ON PULMONARY HOST DEFENSEON PULMONARY HOST DEFENSE
CHEMOTHERAPY
NEUTROPENIA major dose-limiting side effectmajor dose-limiting side effect
-defined as an -defined as an absolute neutrophil count of less than absolute neutrophil count of less than 1,500/µl1,500/µl
- risk of infection begins to increase at an - risk of infection begins to increase at an absolute neutrophil absolute neutrophil count below 1,000/µl.count below 1,000/µl.
Decrease in the number of neutrophils - results in chemotactic Decrease in the number of neutrophils - results in chemotactic and phagocytic defects.and phagocytic defects.
Ladina Joos and Michael Tamm. Breakdown of Pulmonary Host Defense in the Immunocompromised Host. The Proceedings of the American Thoracic Society 2:445-448 (2005)

CHEMOTHERAPEUTIC AGENTS: EFFECT CHEMOTHERAPEUTIC AGENTS: EFFECT ON PULMONARY HOST DEFENSEON PULMONARY HOST DEFENSE
Pulmonary infiltrates emerge in Pulmonary infiltrates emerge in 15 to 25%15 to 25% of patients with profound of patients with profound
neutropenia after chemotherapy.neutropenia after chemotherapy.

Approach to Immunocompromised Approach to Immunocompromised patients with Pulmonary Infiltratespatients with Pulmonary Infiltrates

Pulmonary Fungal Pulmonary Fungal InfectionsInfections
a major problem in neutropenic patientsa major problem in neutropenic patients
usually usually angioinvasive pulmonary aspergillosisangioinvasive pulmonary aspergillosis develop in patients with hematologic malignancies develop in patients with hematologic malignancies after high-dose chemotherapyafter high-dose chemotherapy
The risk of developing invasive pulmonary The risk of developing invasive pulmonary aspergillosis is aspergillosis is directly related to the duration directly related to the duration of the neutropenic phaseof the neutropenic phase. .
Ladina Joos and Michael Tamm. Breakdown of Pulmonary Host Defense in Ladina Joos and Michael Tamm. Breakdown of Pulmonary Host Defense in the Immunocompromised Host. the Immunocompromised Host. The Proceedings of the American Thoracic The Proceedings of the American Thoracic Society 2:445-448 (2005)Society 2:445-448 (2005)

Pulmonary Fungal Pulmonary Fungal InfectionsInfections
““After intensive chemotherapy for hematologic After intensive chemotherapy for hematologic malignancies, the estimated risk of developing malignancies, the estimated risk of developing invasive pulmonary aspergillosisinvasive pulmonary aspergillosis is is
about 5%,about 5%, and the reported mortality ranges and the reported mortality ranges from from 30 to 80%30 to 80%.”.”
““The diagnostic yield of bronchoalveolar The diagnostic yield of bronchoalveolar lavage (BAL) to detect invasive pulmonary lavage (BAL) to detect invasive pulmonary aspergillosis is extremely lowaspergillosis is extremely low.”.”
Denning DW. Therapeutic outcome in invasive aspergillosis. Clin Denning DW. Therapeutic outcome in invasive aspergillosis. Clin Infect Dis 1996;23:608–615.Infect Dis 1996;23:608–615.

CLASSIFICATION OF CLASSIFICATION OF ASPERGILLUSASPERGILLUS INFECTIONINFECTION
ALLERGIC ASPERGILLOSIS
-Allergic bronchopulmonary aspergillosis
-Allergic aspergillus sinusitis
SAPROPHYTIC ASPERGILLOSIS
-Pulmonary aspergilloma
-Sinus aspergilloma
SUPERFICIAL ASPERGILLOSIS
-Otomycosis
-Onchomycosis
-Cutaneous aspergillosis
IN AN IMMUNOCOMPROMISED HOST-1º Cutaneous or mucous mem. aspergillosis
- Pulmonary aspergillosis
- Airway aspergillosis
- Nasal or paranasal sinusitis
- ACUTE INVASIVE ASPERGILLOSIS

in the immunocompromised host- acute, rapidly progressive, with densely consolidated pulmonary infiltrate- spread through direct extension across tissue planes & by hematogenous dissemination to the lungs, brain and other organs
INVASIVE ASPERGILLOSISINVASIVE ASPERGILLOSIS

Aspergillus conidia reaches the alveoli Aspergillus conidia reaches the alveoli
high inoculum of fungihigh inoculum of fungi macrophage dysfunction macrophage dysfunction Decreased macrophagesDecreased macrophages (post chemotherapy) (post chemotherapy) conidia germinates conidia germinates
forms hyphaeforms hyphae
PATHOGENESISPATHOGENESIS

PATHOGENESIS
With the development of Aspergillus hyphaeWith the development of Aspergillus hyphae influx of neutrophilsinflux of neutrophils recruited neutrophils attaches & damages the recruited neutrophils attaches & damages the
hyphaehyphae
During hyphal growth, the fungus produces various During hyphal growth, the fungus produces various metabolites that help it evade host defenses.(i.e. metabolites that help it evade host defenses.(i.e. complement inhibitors, proteases, and several complement inhibitors, proteases, and several mycotoxins, including gliotoxin and aflatoxin)mycotoxins, including gliotoxin and aflatoxin)

-
PATHOLOGYPATHOLOGY
progression of the infection across tissue planesprogression of the infection across tissue planes
vascular invasionvascular invasion
subsequent infarctionsubsequent infarction
tissue necrosistissue necrosis

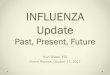
INVASIVE PULMONARY INVASIVE PULMONARY ASPERGILLOSISASPERGILLOSIS
Dense right lower lobe consolidation, consistent with invasive pulmonary aspergillosis

ASPERGILLOMAASPERGILLOMA Vast majority of fungus balls in the lungs are due to aspergillus, with rare cases caused by Pseudoallescheria boydii or Mucorales
Clinical manifestations:
• asymptomatic • some may present with persistent
productive cough, hemoptysis, wheezing, weight loss and finger clubbing.

ASPERGILLOMAASPERGILLOMA• Complications: mild or massive hemoptysis, spread of infection to
the pleura and contiguous vertebral bodies, dissemination to distant body sites (rare)
• Approx. 10% resolve spontaneously• Tx : -Intracavitary Amphotericin B by transthoracic inj -Oral itraconazole -Surgical resection -Embolization

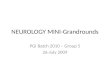
ASPERGILLOMAASPERGILLOMA
Aspergilloma or fungus ball on Chest CT scan

TYPE OF DISEASE PREFERRED TX ALTERNATIVES
Fungus ball of the lung surgical resection bead embolization
Allergic bronchopul. Short courses of Itraconazole
aspergillosis glucocorticoids prophylaxis
Invasive aspergillosis Voriconazole, Amphotericin B,
(liposomal or Itraconazole or
conventional) Caspofungin
TREATMENTTREATMENT

TREATMENTTREATMENT 3 classes of antifungal agents are 3 classes of antifungal agents are
available for the treatment of available for the treatment of Aspergillosis :Aspergillosis :
1.1. Polyenes (eg : Amphotericin B)Polyenes (eg : Amphotericin B)2.2. Azoles (eg : Itraconazole, Azoles (eg : Itraconazole,
Voriconazole)Voriconazole)3.3. Echinocandins (eg : Caspofungin)Echinocandins (eg : Caspofungin)

TREATMENTTREATMENTAMPHOTERICIN BAMPHOTERICIN B
Treatment is limited by poor Treatment is limited by poor toleration & nephrotoxicitytoleration & nephrotoxicity
Dose : 1 – 1,5 mg / kg per dayDose : 1 – 1,5 mg / kg per day Lipid formulation is currently Lipid formulation is currently
available which can be administered available which can be administered with larger doses but showed fewer with larger doses but showed fewer toxic effectstoxic effects

TREATMENTTREATMENTCASPOFUNGINCASPOFUNGIN
Is approved for the treatment of Is approved for the treatment of invasive aspergillosis in pts who invasive aspergillosis in pts who cannot tolerate or who are refractory cannot tolerate or who are refractory to standard therapyto standard therapy
Dose : IV :loading dose 70mg/day, Dose : IV :loading dose 70mg/day, followed by 50 mg/dayfollowed by 50 mg/day

TREATMENTTREATMENTITRACONAZOLEITRACONAZOLE
Is considered a 2Is considered a 2ndnd line agent for the line agent for the tx of aspergillosis and is rarely used tx of aspergillosis and is rarely used in immunocompromised pts with in immunocompromised pts with invasive diseaseinvasive disease
Dose : 400 mg per day poDose : 400 mg per day po Require acid environment for Require acid environment for
absorption, poor bioavailability and absorption, poor bioavailability and important drug interactionimportant drug interaction

VORICONAZOLEVORICONAZOLE• A triazole that is structurally related to fluconazole. Its clinical use was approved by FDA in May 2002. The trade name of voriconazole is Vfend™. • It was approved for primary treatment of acute invasive aspergillosis and salvage therapy for rare but serious fungal infections caused by the pathogens Scedosporium apiospermum and Fusarium spp

VORICONAZOLEVORICONAZOLE
- works principally by inhibition of cytochrome P450 14a-demethylase (P45014DM).
- favorable in vitro activity against a variety of fungi. These include, Candida spp., Aspergillus spp., Cryptococcus neoformans, Blastomyces dermatitidis, Coccidioides immitis, Histoplasma capsulatum, Fusarium spp., and Penicillium marneffei.
- a fungistatic agent against Candida spp. and Cryptococcus neoformans. It may be fungicidal against Aspergillus spp.

VORICONAZOLEVORICONAZOLE
- active following both oral and intravenous administrations
Doses Oral: 200 mg twice daily IV: 3 to 6 mg/kg every 12 h doses
SIDE EFFECTS: transient visual disturbances, skin rash and elevated hepatic enzyme levels

TREATMENTTREATMENTPOSACONAZOLEPOSACONAZOLE
is a broad spectrum triazole that is is a broad spectrum triazole that is currently in development.currently in development.
Its activity is similar to Voriconazole Its activity is similar to Voriconazole against Aspergillus sp, but there is against Aspergillus sp, but there is little published to date on its efficacylittle published to date on its efficacy

CLINICAL STUDIESCLINICAL STUDIESVoriconazole vs. Amphotericin B: Acute invasive aspergillosisNational Institute of Allergy and Infectious Diseases Mycoses Study GroupJune 2001
- 277 patients treated for 12 weeks with Voriconazole and Amphotericin B
- majority of study patients had underlying hematologic malignancies, including bone marrow transplantation; patients with solid organ transplantation, solid tumors, and AIDS. CONCLUSION: A satisfactory global response at 12 weeks was seen in 53% of voriconazole treated patients compared to 32% of amphotericin B treated patients. A benefit of voriconazole compared to amphotericin B on patient survival at Day 84 was seen with a 71% survival rate on voriconazole compared to 58% on amphotericin B.

CLINICAL STUDIESCLINICAL STUDIESFluconazole and Voriconazole Multidisk Testing of Candida Species for Disk Test Calibration and MIC Estimation Göran Kronvall* and Inga Karlsson Department of Microbiology and Tumor Biology, Sweden January 2001
Fluconazole and voriconazole MICs were determined for 114 clinical Candida isolates, including isolates of Candida albicans, Candida glabrata, Candida krusei, Candida lusitaniae, Candida parapsilosis, and Candida tropicalis. All strains were susceptible to voriconazole, and most strains were also susceptible to fluconazole, with the exception of C. glabrata and C. krusei, the latter being fully fluconazole resistant. Single-strain regression analysis (SRA) was applied to 54 strains.CONCLUSION: Voriconazole might be a first-choice azole in treating Candida infections.

THANK YOU!THANK YOU!