Embed Size (px)
Citation preview

GOOD MORNING!GOOD MORNING!

MEDICAL GRANDROUNDSMEDICAL GRANDROUNDS
Antonio A. Carlos, Jr., MDAntonio A. Carlos, Jr., MD
First Year ResidentFirst Year Resident
12 June 200812 June 2008

THE GREAT IMITATORTHE GREAT IMITATOR

OBJECTIVESOBJECTIVES
1.1. To present a case of liver abscess with To present a case of liver abscess with an unusual cause;an unusual cause;
2.2. To give an overview on the etiology and To give an overview on the etiology and management of liver abscess;management of liver abscess;
3.3. To discuss melioidosis, its diagnosis and To discuss melioidosis, its diagnosis and management.management.

Santiago City, IsabelaSantiago City, Isabela

Santiago City, IsabelaSantiago City, Isabela

IDENTIFYING DATAIDENTIFYING DATA
E. B.E. B. 58 year-old female58 year-old female MarriedMarried FarmerFarmer Non-diabeticNon-diabetic Non-hypertensiveNon-hypertensive

CHIEF COMPLAINTCHIEF COMPLAINT
Abdominal painAbdominal pain

HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS
8 months prior to admission,8 months prior to admission,
crampy left upper quadrant abdominal crampy left upper quadrant abdominal painpain
occur intermittently occur intermittently no fever, vomiting, and diarrhea no fever, vomiting, and diarrhea

consulted at a local hospital consulted at a local hospital abdominal ultrasound showed the abdominal ultrasound showed the
presence of three hepatic nodulespresence of three hepatic nodules no treatment was done due to financial no treatment was done due to financial
constraints constraints lost to follow-up lost to follow-up

2 months prior to admission,2 months prior to admission,
intermittent abdominal painintermittent abdominal pain consulted in another local hospital consulted in another local hospital abdominal CT scan showed the presence abdominal CT scan showed the presence
of five hepatic nodulesof five hepatic nodules advised biopsy of the nodules advised biopsy of the nodules opted to seek second opinion opted to seek second opinion

2 weeks prior to admission,2 weeks prior to admission,
consulted a gastroenterologist in Manila consulted a gastroenterologist in Manila EGD was doneEGD was done showed gastric ulcer showed gastric ulcer biopsy of the ulcer showed positive for biopsy of the ulcer showed positive for
Helicobacter pyloriHelicobacter pylori started on started on H. pyloriH. pylori regimen regimen

advised admission for the work-up of the advised admission for the work-up of the hepatic noduleshepatic nodules

PAST MEDICAL HISTORYPAST MEDICAL HISTORY
(-) Hypertension(-) Hypertension
(-) Diabetes(-) Diabetes
(-) Bronchial asthma(-) Bronchial asthma
(-) Tuberculosis(-) Tuberculosis

FAMILY MEDICAL HISTORYFAMILY MEDICAL HISTORY
(+) Hepatitis A(+) Hepatitis A
(+) Bronchial asthma(+) Bronchial asthma
(-) Hypertension(-) Hypertension
(-) Diabetes(-) Diabetes
(-) Tuberculosis(-) Tuberculosis

PERSONAL/SOCIAL HISTORYPERSONAL/SOCIAL HISTORY
FarmerFarmer Non-smokerNon-smoker Non-alcoholic beverage drinkerNon-alcoholic beverage drinker No known allergiesNo known allergies

REVIEW OF SYSTEMSREVIEW OF SYSTEMS
(-) weight loss(-) weight loss
(-) fever(-) fever
(-) cough and colds(-) cough and colds
(-) loss of appetite(-) loss of appetite
(-) easy fatigability(-) easy fatigability
(-) chest pain(-) chest pain
(-) palpitations(-) palpitations

PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
GS: GS: conscious, coherent, ambulatory, conscious, coherent, ambulatory, not in respiratory distressnot in respiratory distress
VS:VS: BP 100/70 BP 100/70 HR 82 RR 18HR 82 RR 18 T 36.9T 36.9HEENT:HEENT: anicteric sclerae, pale palpebral anicteric sclerae, pale palpebral conjunctivae, no nasoaural conjunctivae, no nasoaural
discharge, discharge, no CLADno CLADCL:CL: symmetric chest expansion, symmetric chest expansion, clear breath soundsclear breath sounds

CVS:CVS: adynamic precordium, normal rate, adynamic precordium, normal rate,
regular rhythm, distinct S1 and S2regular rhythm, distinct S1 and S2
ABD:ABD: flat, normoactive bowel sounds, soft, flat, normoactive bowel sounds, soft,
(+) direct tenderness on LUQ, (+) direct tenderness on LUQ,
no guarding, no organomegalyno guarding, no organomegaly
EXT:EXT: no edema, no cyanosis, no edema, no cyanosis,
full and equal pulsesfull and equal pulses

SALIENT FEATURESSALIENT FEATURES
58 year-old female58 year-old female farmerfarmer left upper quadrant abdominal painleft upper quadrant abdominal pain abdominal CT scan finding of hepatic abdominal CT scan finding of hepatic
nodulesnodules

““What is the nature of the What is the nature of the hepatic nodules?”hepatic nodules?”

DAY OF ADMISSIONDAY OF ADMISSION
Primary ImpressionPrimary Impression
Hepatocellular carcinomaHepatocellular carcinoma
Differential DiagnosisDifferential Diagnosis
Liver AbscessLiver Abscess

EB
Abdominal Pain
Hepatic Nodules
Hepatocellular CA Liver Abscess
Primary Metastatic Etiology??

CBCCBC
Gram Stain
Culture and Sensitivity
AFB Smear and Culture
Cell Block
CT Guided Liver BiopsyCT Guided Liver Biopsy

1st HOSPITAL DAY1st HOSPITAL DAY
Patient had febrile episodes, maximum Patient had febrile episodes, maximum temperature of 39.4°Ctemperature of 39.4°C
Blood culture was doneBlood culture was done
Started on Metronidazole 50mg/IV q8° Started on Metronidazole 50mg/IV q8° Ciprofloxacin 500mg/tab, 1 tablet 2x a Ciprofloxacin 500mg/tab, 1 tablet 2x a day Paracetamol 500mg/tab, 1 tablet day Paracetamol 500mg/tab, 1 tablet every 4 hoursevery 4 hours

2nd HOSPITAL DAY2nd HOSPITAL DAY
Patient still had febrile episodesPatient still had febrile episodes
CBC doneCBC done
Referred to Infectious Disease ServiceReferred to Infectious Disease Service

““What is the focus of the fever?”What is the focus of the fever?”

Patient was seen by the Patient was seen by the Infectious Disease ServiceInfectious Disease Service
Transfer IV site
Urinalysis
Chest x-ray

EB
Hepatocellular CA Liver Abscess
Primary Metastatic Etiology??
Phlebitis UTI PTB

3rd HOSPITAL DAY3rd HOSPITAL DAY
Patient was still febrilePatient was still febrile
Liver aspirate culture grew gram Liver aspirate culture grew gram negative rods, T/C negative rods, T/C PseudomonasPseudomonas

Ciprofloxacin was discontinuedCiprofloxacin was discontinued
Piperacillin-Tazobactam 4.5g/IV every Piperacillin-Tazobactam 4.5g/IV every
8 hours was started8 hours was started

4th HOSPITAL DAY4th HOSPITAL DAY
Liver biopsy showed negative for Liver biopsy showed negative for malignant cellsmalignant cells
Cytomorphologic features consistent with Cytomorphologic features consistent with an acute suppurative infectionan acute suppurative infection

Liver aspirate culture grew Liver aspirate culture grew BurkholderiaBurkholderia pseudomalleipseudomallei
Piperacillin-Tazobactam was shifted to Piperacillin-Tazobactam was shifted to Ceftazidime 1g/IV every 8 hoursCeftazidime 1g/IV every 8 hours

EB
Hepatocellular CA Liver Abscess
Primary Metastatic Burkholderia pseudomallei
PTB

5th HOSPITAL DAY5th HOSPITAL DAY
Blood culture and sensitivity showed no Blood culture and sensitivity showed no growth after 5 daysgrowth after 5 days
Day 1 afebrileDay 1 afebrile

6th HOSPITAL DAY6th HOSPITAL DAY
Day 2 afebrileDay 2 afebrile
Patient decided that blood transfusion Patient decided that blood transfusion
would be done in Isabelawould be done in Isabela
Patient was discharged with follow-up Patient was discharged with follow-up
after 2 after 2 monthsmonths

FINAL DIAGNOSISFINAL DIAGNOSIS
MelioidosisMelioidosis Cannot totally rule out Cannot totally rule out
Pulmonary TuberculosisPulmonary Tuberculosis Peptic ulcer diseasePeptic ulcer disease

RECOMMENDATIONRECOMMENDATION
PTB work-up should be donePTB work-up should be done

MELIOIDOSISMELIOIDOSIS

HISTORICAL BACKGROUNDHISTORICAL BACKGROUND
Named from the Greek “Named from the Greek “melismelis” (distemper ” (distemper of asses) and “of asses) and “eidoseidos” (resemblance)” (resemblance)
First described by pathologist Alfred First described by pathologist Alfred Whitmore among morphia addicts in Whitmore among morphia addicts in Burma in 1911Burma in 1911
In 1917, Stanton and Fletcher identified In 1917, Stanton and Fletcher identified the bacteria that cause the diseasethe bacteria that cause the disease

100 cases identified during the French 100 cases identified during the French occupation of Vietnam in 1948-1954occupation of Vietnam in 1948-1954
300 cases identified during the American 300 cases identified during the American occupation in the 1970’s, popularly occupation in the 1970’s, popularly known as the “Vietnamese Time Bomb”known as the “Vietnamese Time Bomb”

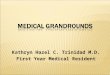
EPIDEMIOLOGYEPIDEMIOLOGY
Regarded as endemic to Southeast Asia Regarded as endemic to Southeast Asia and Northern Australiaand Northern Australia
Corresponds approximately to latitudes Corresponds approximately to latitudes between 20between 20ooN and 20N and 20ooSS

Fig. 1 Worldwide distribution of melioidosisFig. 1 Worldwide distribution of melioidosis

REPORTED CASESREPORTED CASES
In Australia, 40 cases per 100,000 in 2002In Australia, 40 cases per 100,000 in 2002 In Thailand, 1,100 cases between 2004-In Thailand, 1,100 cases between 2004-
20052005 In Malaysia, 50 cases in 2002In Malaysia, 50 cases in 2002 In Singapore, 57 cases in 2004In Singapore, 57 cases in 2004 In Taiwan, 43 cases in 2004In Taiwan, 43 cases in 2004 In Philippines, not reported in the world In Philippines, not reported in the world
literatureliterature

ETIOLOGIC AGENTETIOLOGIC AGENT
Burkholderia Burkholderia pseudomalleipseudomallei
gram negative bacillusgram negative bacillus bipolar stainingbipolar staining safety pin appearancesafety pin appearance saprophyticsaprophytic considered a Category considered a Category
3 pathogen by the CDC3 pathogen by the CDC

Resilient organism Resilient organism capable of surviving capable of surviving hostile hostile environmental environmental conditionsconditions
Produces several Produces several virulence factors: virulence factors: exopolysaccharides and exopolysaccharides and lipaselipase
phospholipase Cphospholipase C
hemolysinhemolysin
proteaseprotease
Often called the Often called the Great ImitatorGreat Imitator

RISK FACTORSRISK FACTORS
Exposure to aquatic environments and Exposure to aquatic environments and agricultural landsagricultural lands
Diabetes mellitusDiabetes mellitus Chronic obstructive pulmonary diseaseChronic obstructive pulmonary disease Use of steroidsUse of steroids

CLINICAL SYNDROMESCLINICAL SYNDROMES
SepsisSepsis PneumoniaPneumonia Liver abscessLiver abscess Splenic abscessSplenic abscess Skin and soft tissue abscessSkin and soft tissue abscess

4 DISEASE CATEGORIES (CDC, 4 DISEASE CATEGORIES (CDC, 2000)2000)
1.1. Acute localized infectionAcute localized infection▪ ▪ localized as a nodulelocalized as a nodule▪ ▪ results from inoculation through a break in results from inoculation through a break in the skinthe skin
2.2. Acute pulmonary infectionAcute pulmonary infection▪ ▪ produce a clinical picture ranging from mild produce a clinical picture ranging from mild
bronchitis to severe pneumoniabronchitis to severe pneumonia▪ ▪ radiologic findings include nodule, upper lobe radiologic findings include nodule, upper lobe
consolidation, cavitary lesionsconsolidation, cavitary lesions

3.3. Acute bloodstream infectionAcute bloodstream infection▪ ▪ patients with underlying illness such as diabetes, patients with underlying illness such as diabetes,
renal failure are affected by this type of diseaserenal failure are affected by this type of disease▪ ▪ usually results in septic shockusually results in septic shock
4.4. Chronic suppurative infectionChronic suppurative infection▪ ▪ involves the liver, lung, spleen, lymph nodesinvolves the liver, lung, spleen, lymph nodes▪ ▪ may become dormant with exacerbation may become dormant with exacerbation occurring occurring after primary infectionafter primary infection

MODES OF ACQUISITIONMODES OF ACQUISITION
1.1. InoculationInoculation
▪ ▪ major mode of acquisitionmajor mode of acquisition
▪ ▪ wounds to the feet of rice farmers are wounds to the feet of rice farmers are
common sites of inoculationcommon sites of inoculation
▪ ▪ 25% in the Darwin study gave a history 25% in the Darwin study gave a history of of
an inoculation injury prior to an inoculation injury prior to presentationpresentation

2. Inhalation2. Inhalation
▪ ▪ based on studies of US soldier based on studies of US soldier helicopter crew helicopter crew
in Vietnamin Vietnam
▪ ▪ non-ambulant patients in Singapore non-ambulant patients in Singapore acquired acquired
the disease without exposure to soil or the disease without exposure to soil or waterwater

3. Ingestion3. Ingestion
▪ ▪ contamination of potable water in two contamination of potable water in two
outbreaks in Northern Australiaoutbreaks in Northern Australia

INCUBATION PERIODINCUBATION PERIOD
Incubation period of melioidosis is not clearly Incubation period of melioidosis is not clearly defineddefined
In the Darwin Series, an incubation period of In the Darwin Series, an incubation period of 1-21 days has been defined1-21 days has been defined
Incubation periods of as long as 24 to 29 Incubation periods of as long as 24 to 29 years in ex-servicemen who were in Papua years in ex-servicemen who were in Papua New Guinea and Vietnam have been New Guinea and Vietnam have been described (hence the Vietnamese time bomb)described (hence the Vietnamese time bomb)

DIAGNOSISDIAGNOSIS
Isolation of Isolation of B. B. pseudomalleipseudomallei remains the gold remains the gold standard in standard in diagnosisdiagnosis
A modified A modified Ashdown medium Ashdown medium with colistin is with colistin is commonly usedcommonly used

Monoclonal Monoclonal antibody latex antibody latex agglutination testagglutination test
Shown to Shown to agglutinate blood agglutinate blood culture fluid culture fluid positive to positive to B. B. pseudomalleipseudomallei
Sensitivity of 95% Sensitivity of 95% Specificity of 99.7%Specificity of 99.7%

TREATMENTTREATMENT
Characteristics of Antimicrobial:Characteristics of Antimicrobial: It should have a bactericidal effect;It should have a bactericidal effect; Should be able to penetrate phagocytic Should be able to penetrate phagocytic
cells;cells; Eliminate or inhibit glycocalyxEliminate or inhibit glycocalyx

Treatment of Melioidosis is divided into Treatment of Melioidosis is divided into two stages: two stages:
1. an intravenous high intensity 1. an intravenous high intensity stagestage
2. an oral maintenance stage to 2. an oral maintenance stage to prevent prevent recurrencerecurrence

Intravenous Intensive PhaseIntravenous Intensive Phase Intravenous ceftazidime is the current Intravenous ceftazidime is the current
drug of choice for melioidosisdrug of choice for melioidosis Meropenem, imipenem, cefoperazone-Meropenem, imipenem, cefoperazone-
sulbactam are also activesulbactam are also active Amoxicillim-clavulanate may be used if Amoxicillim-clavulanate may be used if
none of the above are availablenone of the above are available

Maintenance PhaseMaintenance Phase Treatment with cotrimoxazole and Treatment with cotrimoxazole and
doxycycline be used for 12 to 20 weeks doxycycline be used for 12 to 20 weeks to reduce the rate of recurrenceto reduce the rate of recurrence
Co-amoxiclav is an alternative for those Co-amoxiclav is an alternative for those who are unable to take cotrimoxazole or who are unable to take cotrimoxazole or doxycyclinedoxycycline

PROGNOSISPROGNOSIS
Without access to antibiotics, the Without access to antibiotics, the septicemic form of melioidosis has a septicemic form of melioidosis has a mortality that exceeds 90%mortality that exceeds 90%
With appropriate antibiotics, mortality With appropriate antibiotics, mortality rate is about 10% for uncomplicated rate is about 10% for uncomplicated casescases
Relapse rate occurs in 10 to 20% of Relapse rate occurs in 10 to 20% of patientspatients

BIOLOGIC WEAPONS AGENTBIOLOGIC WEAPONS AGENT
CDC classified melioidosis as Category B CDC classified melioidosis as Category B biological weapons agentbiological weapons agent
Good candidate as a bioweapon because Good candidate as a bioweapon because it is easily available in the tropics, easy to it is easily available in the tropics, easy to cultivate, sturdy, high potential to cultivate, sturdy, high potential to become bacteremicbecome bacteremic
Countries studying melioidosis as a Countries studying melioidosis as a bioweapon are USA, Russia, and Egyptbioweapon are USA, Russia, and Egypt

ACKNOWLEDGMENTACKNOWLEDGMENT
Dr. Miguel ForesDr. Miguel Fores Dr. Tarcela GlerDr. Tarcela Gler Dr. Jodor LimDr. Jodor Lim Dr. Mabel AlocDr. Mabel Aloc Dr. Sasa SamsonDr. Sasa Samson Dr. Ronnie BenitezDr. Ronnie Benitez Dr. John JarinDr. John Jarin Dr. JC SevillaDr. JC Sevilla
ArianneArianne IvyIvy AbbeyAbbey MaraMara GeloGelo Ed B.Ed B. MMMM

THANK YOU!THANK YOU!

CBC April 23, 2008
Hemoglobin 9.3
Hematocrit 30.9
WBC 9.91
Neutrophils 84
Lymphocytes 10
Eosinophils 1
Monocytes 5
Basophils 0
Platelet 263,000

CBC April 25, 2008
Hemoglobin 8.6
Hematocrit 28.6
WBC 5.91
Neutrophils 65
Lymphocytes 19
Eosinophils 4
Monocytes 12
Basophils 0
Platelet 220,000

UrinalysisUrinalysisColorColor YellowYellow
TransparencyTransparency ClearClear
pHpH AcidicAcidic
Specific GravitySpecific Gravity 1.0251.025
SugarSugar NegativeNegative
ProteinsProteins NegativeNegative
KetonesKetones NegativeNegative
NitritesNitrites NegativeNegative
Leukocyte EsteraseLeukocyte Esterase NegativeNegative
BloodBlood 00
RBCRBC 00
WBCWBC 0 – 10 – 1
Epithelial CellsEpithelial Cells 22
BacteriaBacteria 33

Consider calcified granuloma in the left apex.
The rest of the lungs are clear.
Heart and other chest structures are within normal limits

Site of Collection: Post Liver Biopsy April 23, 2008
Results:Identified Organism/s: Burkholderia pseudomallei Light growth
Sensitivities: Amikacin 6 R Ticarcillin/Clavulanic acid 28 S Piperacillin/Tazobactam 29 S Cotrimoxazole 32 S Ceftazidime 25 S Cefepime 18 S Ciprofloxacin 24 S