Embed Size (px)
Citation preview
Medical genetics
Dr. Lina Basel
Schneider Children’s
Medical Center of Israel
1. What is the problem
2 .Why did it happen
3 .What will it mean for our baby
4 .Will it happen again
Benefits of genetic evaluation
Reproductive counseling: carrier testing, prenatal diagnosis
Presymptomatic screening for associated complications
Referral to support groups
Benefits of genetic evaluation
How do you make a syndrome diagnosis?
History
Examination
Investigations
Family history
Any relative with mental retardation or known malformations
Neonatal deaths, stillbirths or childhood deaths
Familial disorders or physical features
Consanguinity in parents
Ethnic background
Prior genetic testing or screening
History
Family history – pedigree:
what is the mode of inheritance?
- AR, AD, XL, Y-linked, mitochondrial, trinucleotide repeat expansion
History
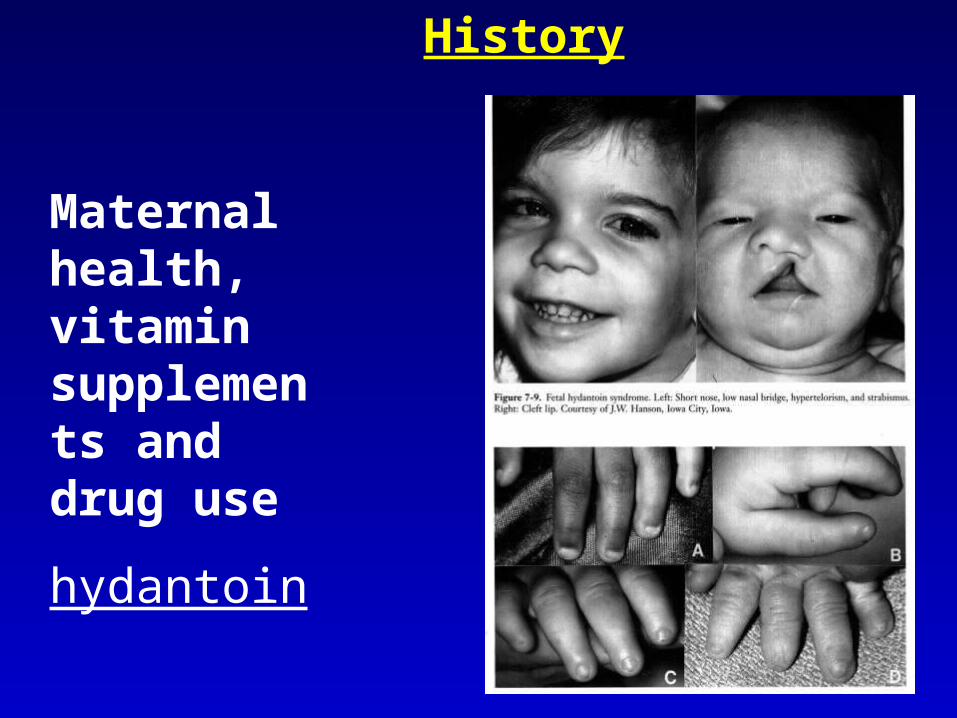
Maternal health, vitamin supplements and drug use
hydantoin
History
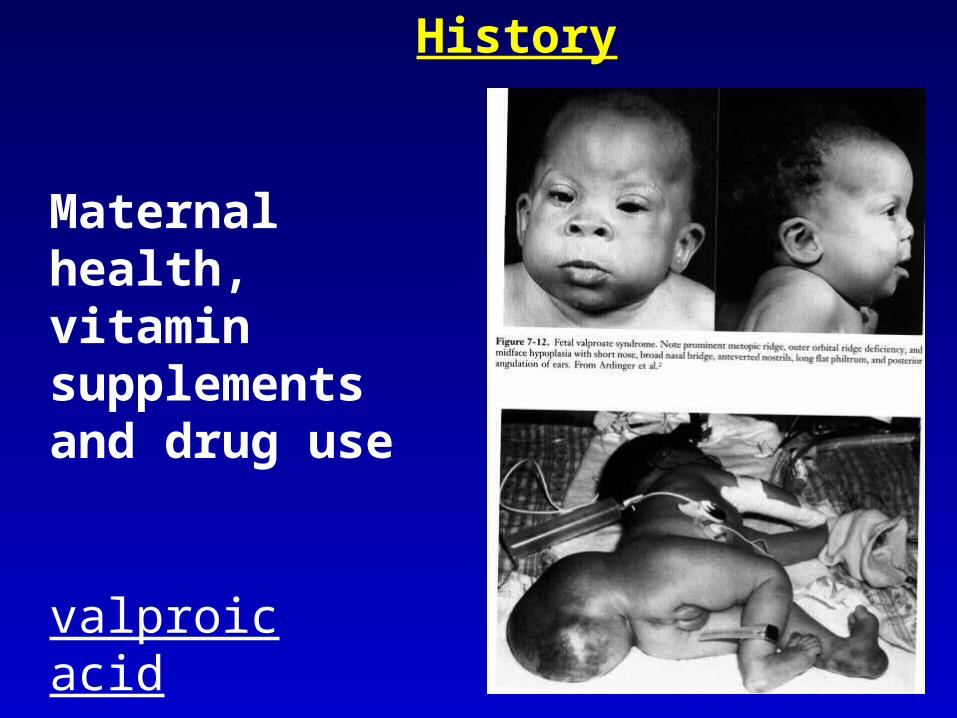
Maternal health, vitamin supplements and drug use
valproic acid
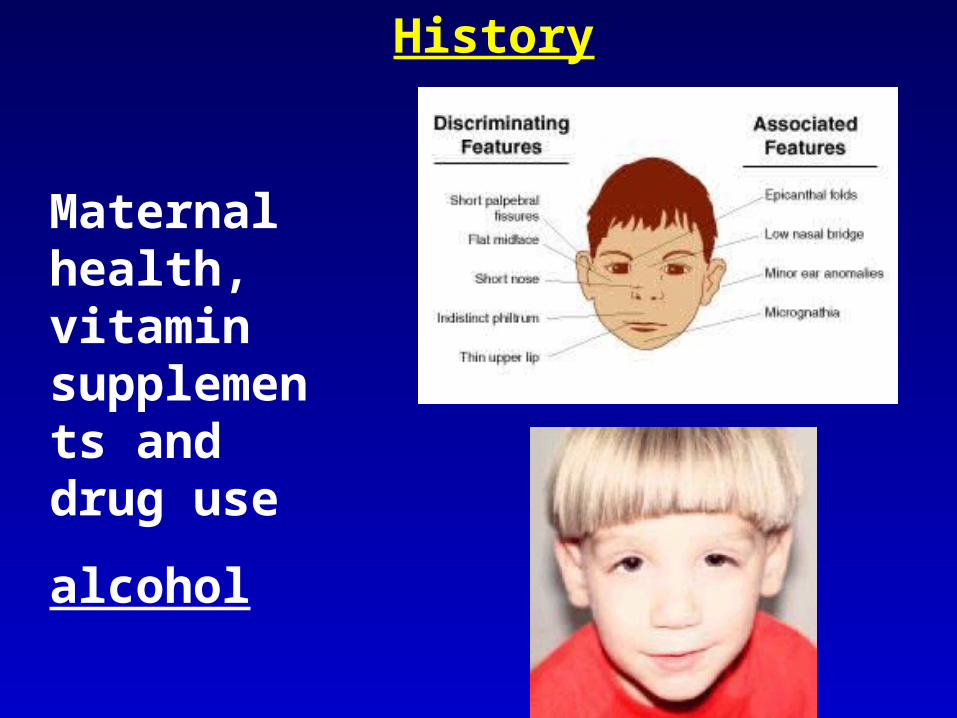
History
Maternal health, vitamin supplements and drug use
alcohol
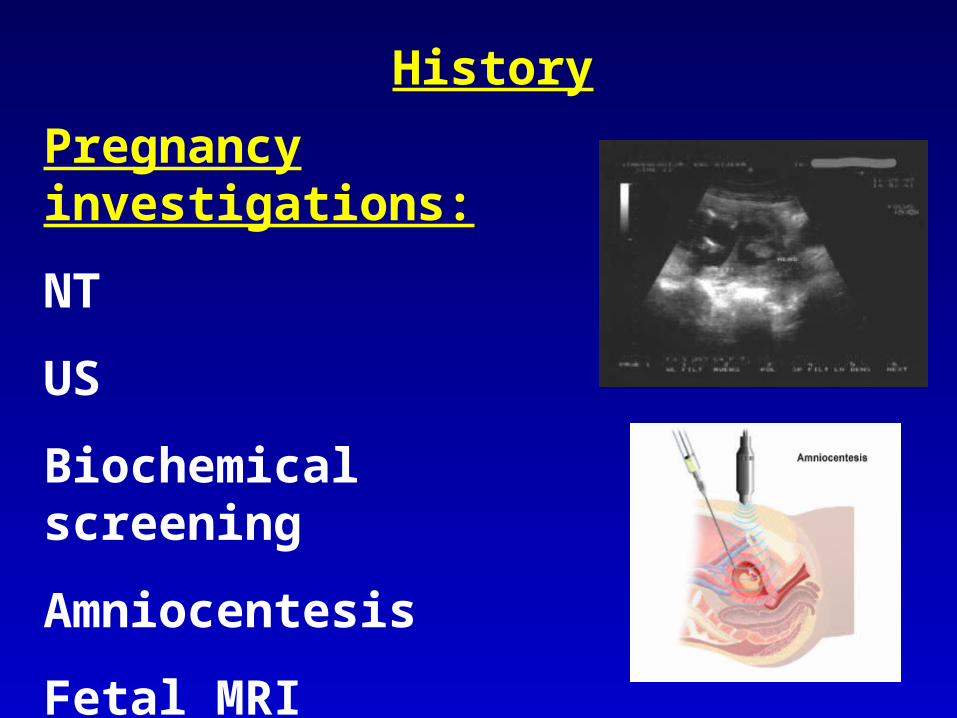
History
Pregnancy investigations:
NT
US
Biochemical screening
Amniocentesis
Fetal MRI
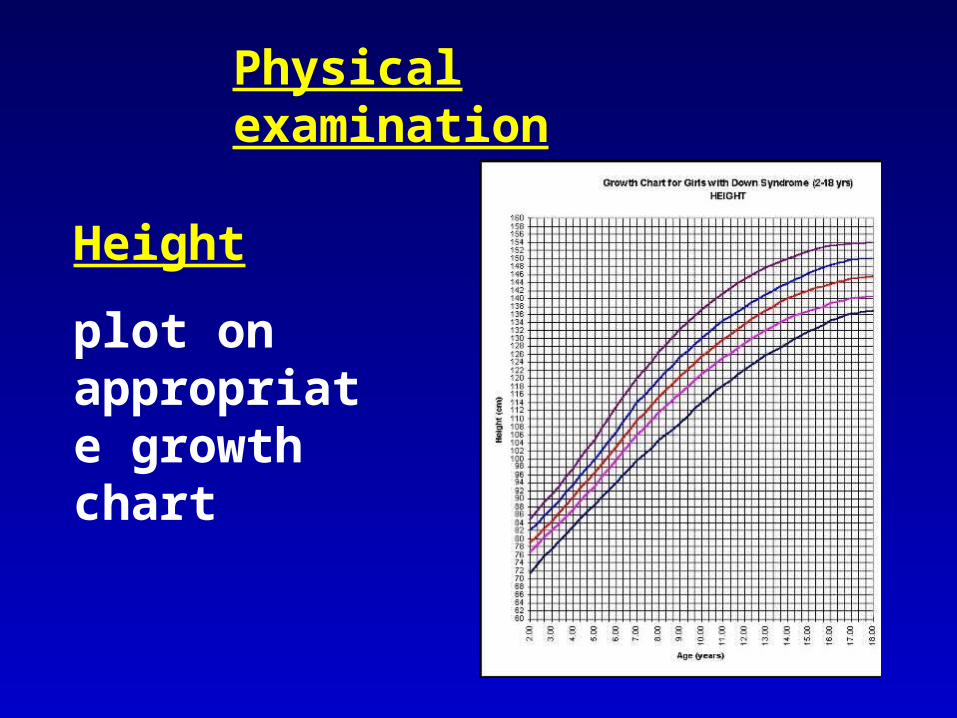
Physical examination
Height
plot on appropriate growth chart
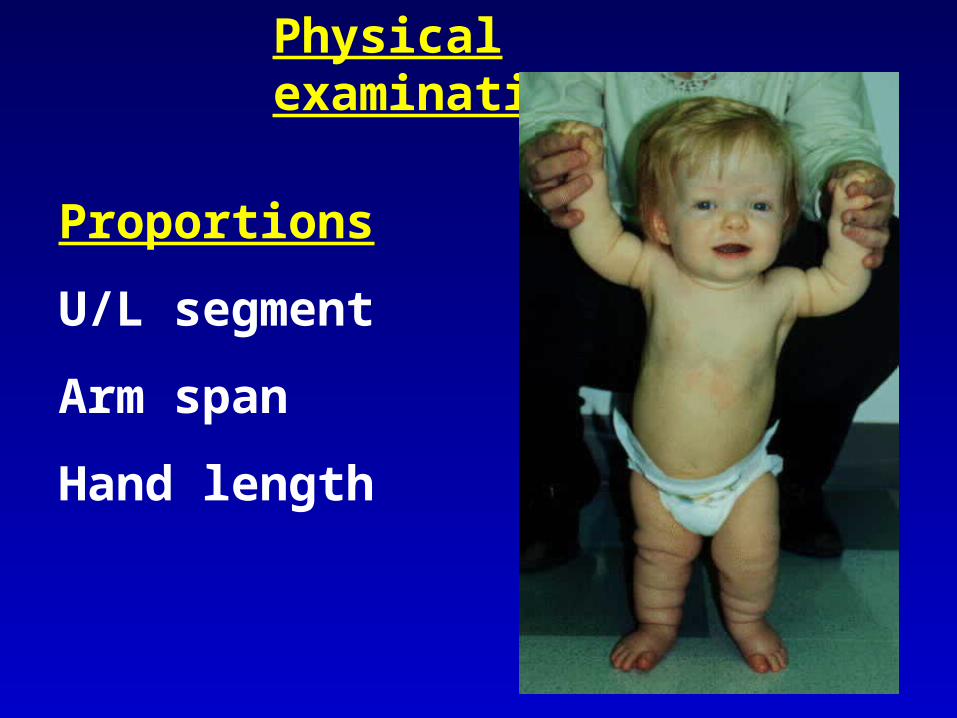
Physical examination
Proportions
U/L segment
Arm span
Hand length
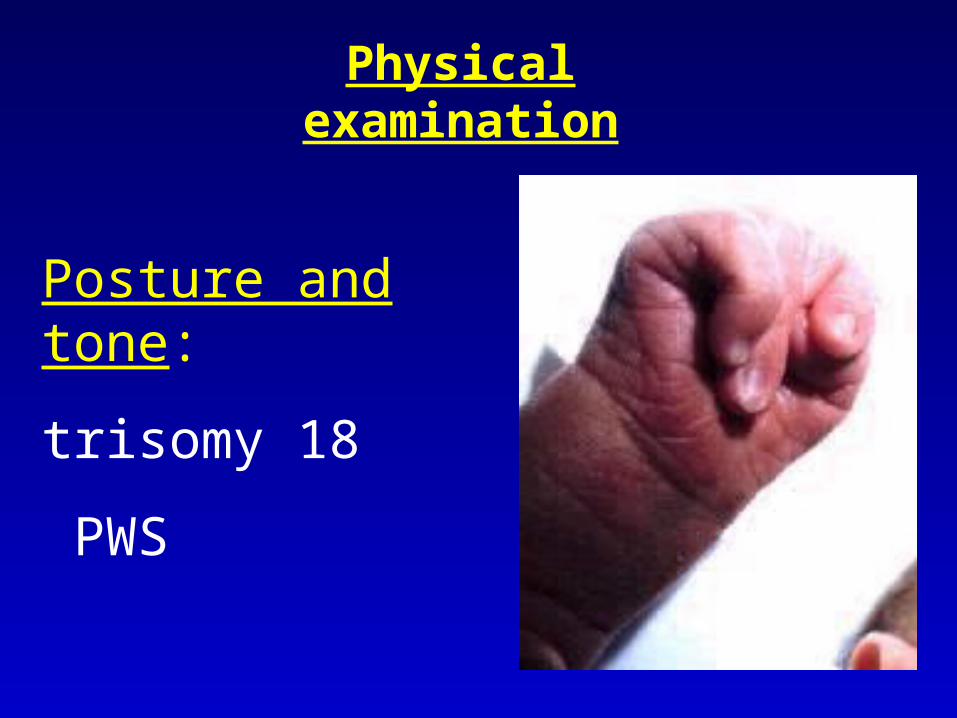
Posture and tone:
trisomy 18
PWS
Physical examination
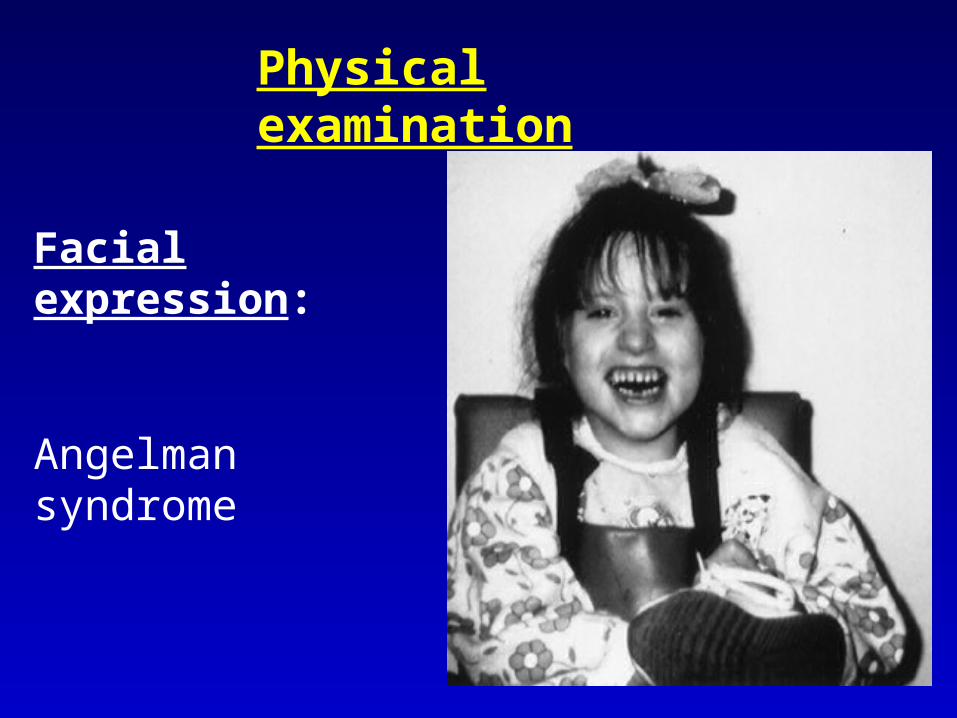
Facial expression:
Angelman syndrome
Physical examination
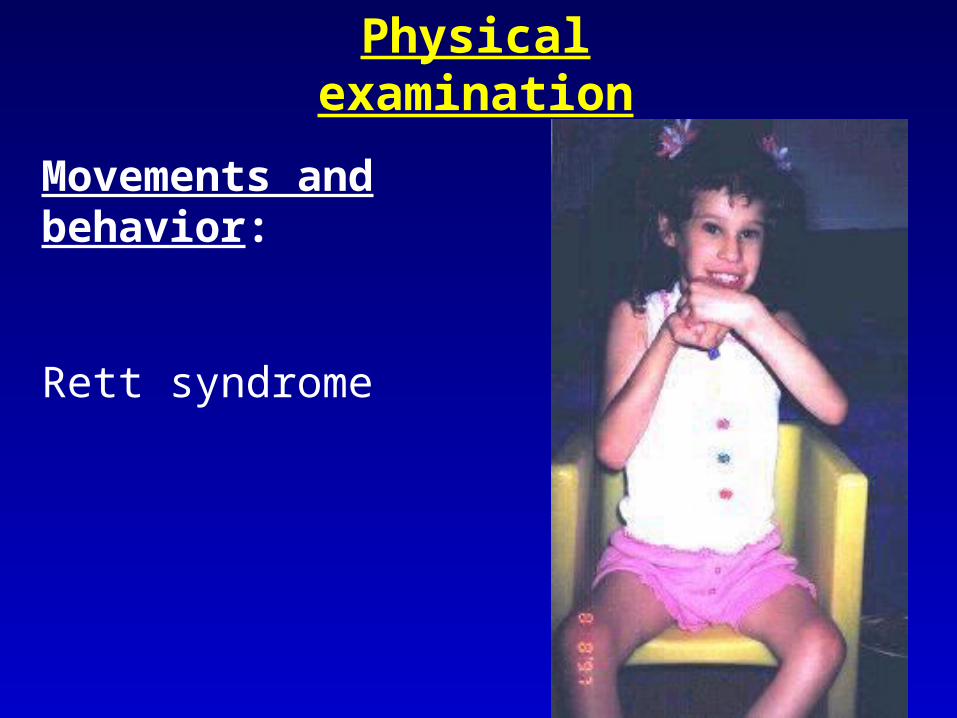
Movements and behavior:
Rett syndrome
Physical examination
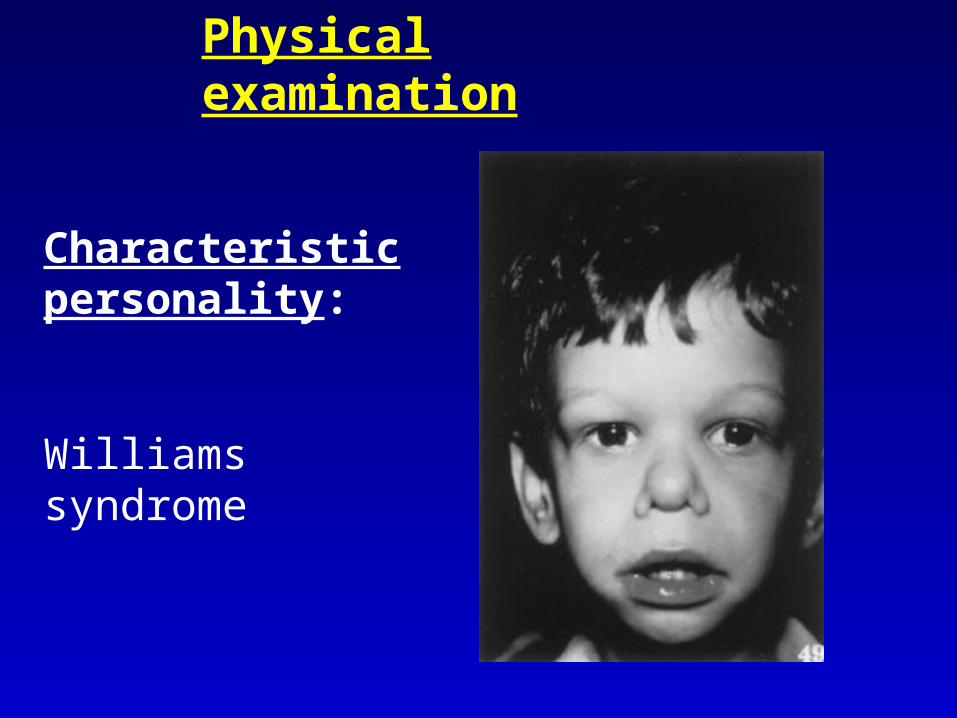
Characteristic personality:
Williams syndrome
Physical examination
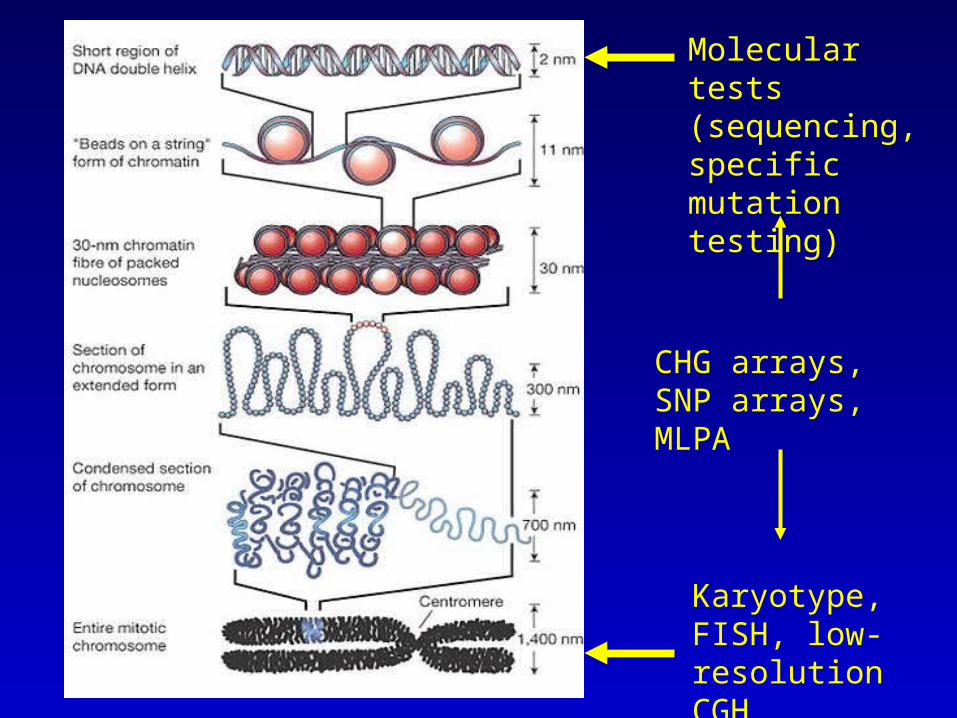
Karyotype, FISH, low-resolution CGH
Molecular tests (sequencing, specific mutation testing)
CHG arrays, SNP arrays, MLPA
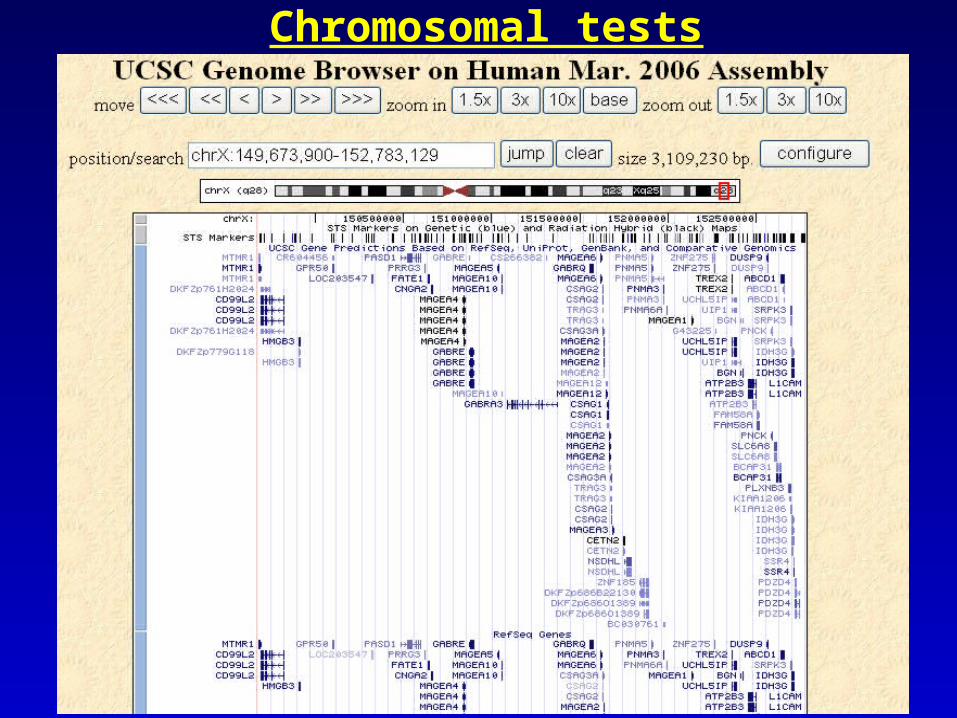
Chromosomal tests
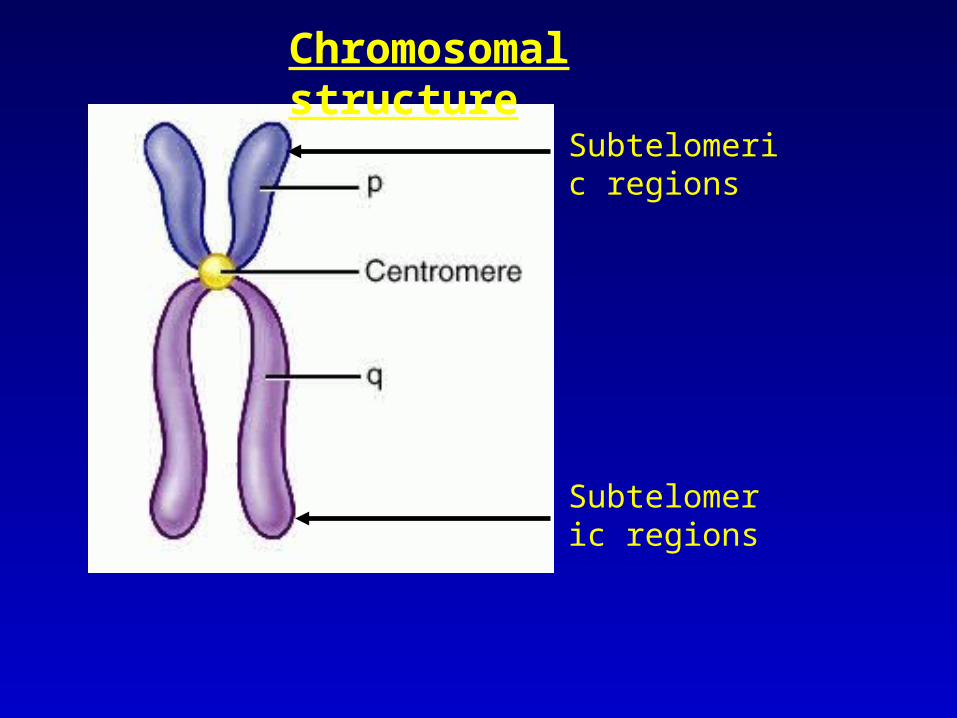
Subtelomeric regions
Subtelomeric regions
Chromosomal structure
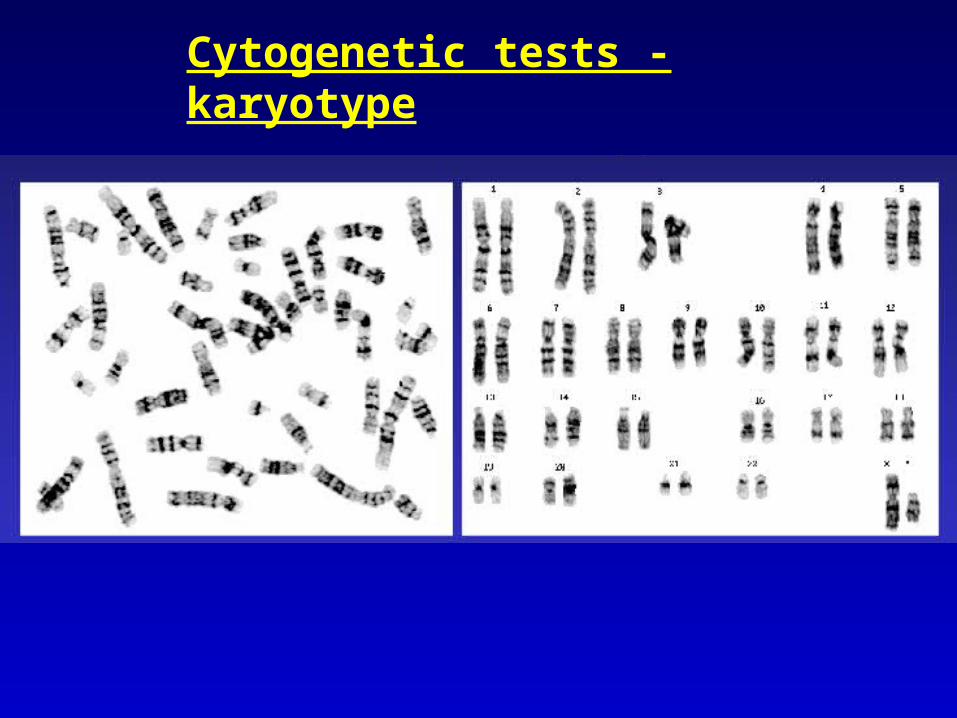
Cytogenetic tests - karyotype
Cytogenetic tests - karyotype
Indications:
Mental retardation
Dysmorphic features
Major anomaly
Recurrent spontaneous abortions
Family history of multiple affected individuals with MR/malformations
5-10 Mb resolution (300-600 cytogenetic bands)
ECARUCA
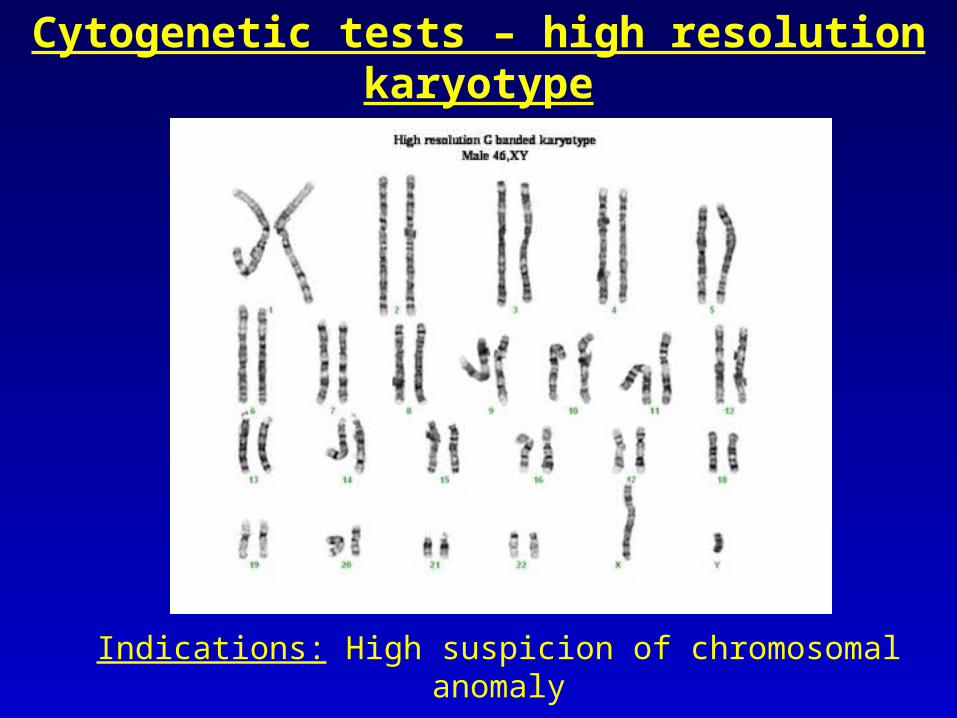
Cytogenetic tests – high resolution karyotype
Indications: High suspicion of chromosomal anomaly
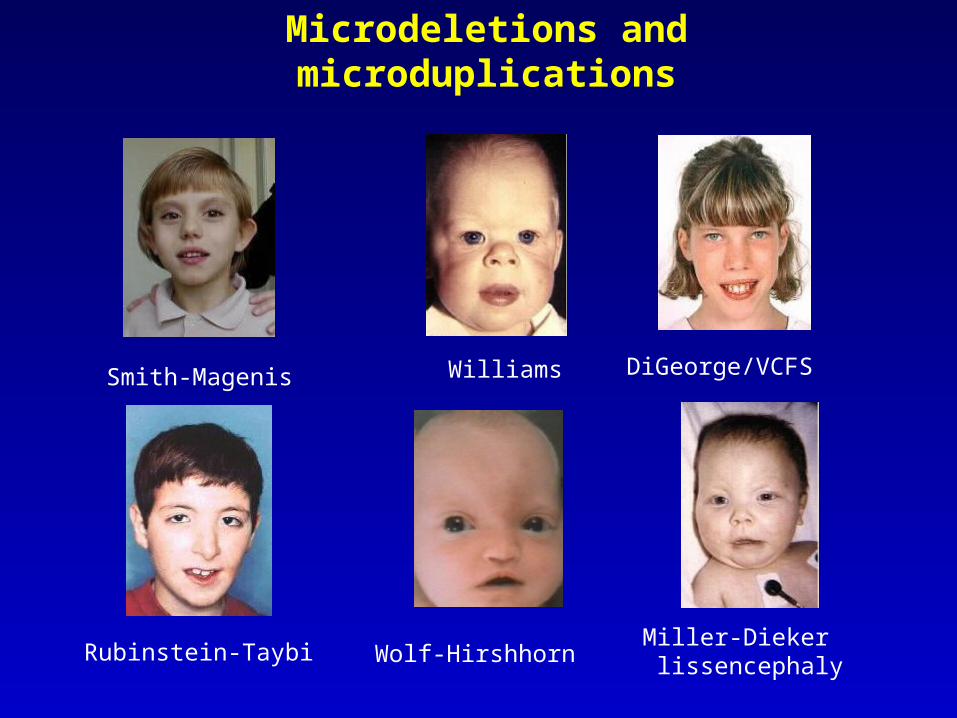
Microdeletions and microduplications
Wolf-Hirshhorn
Williams DiGeorge/VCFS
Miller-Dieker lissencephalyRubinstein-Taybi
Smith-Magenis
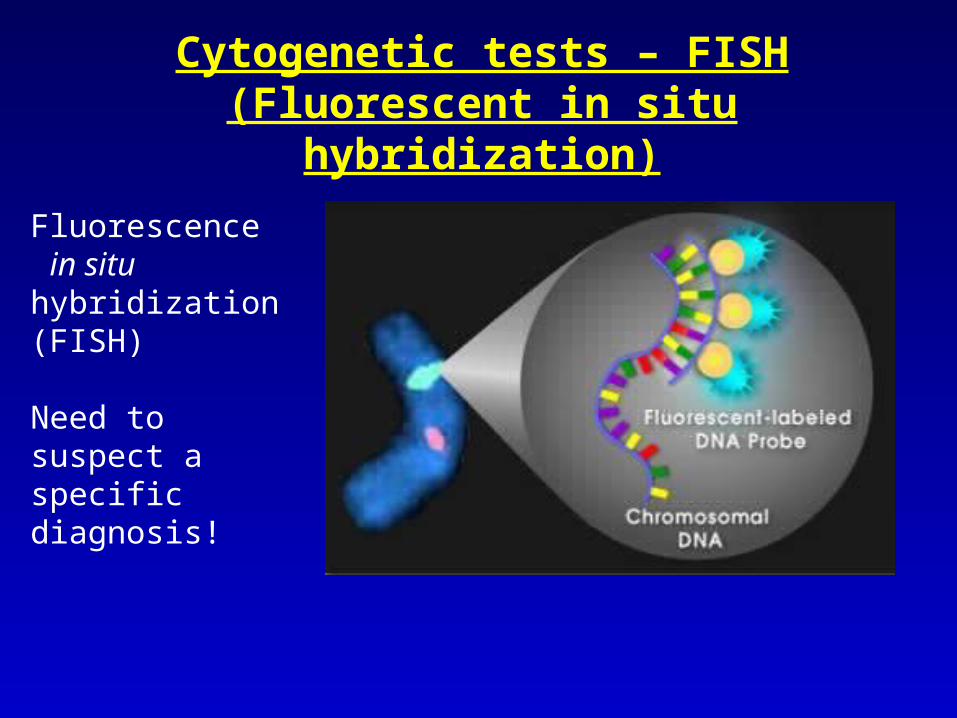
Fluorescence in situ hybridization (FISH)
Need to suspect a specific diagnosis!
Cytogenetic tests – FISH (Fluorescent in situ
hybridization)
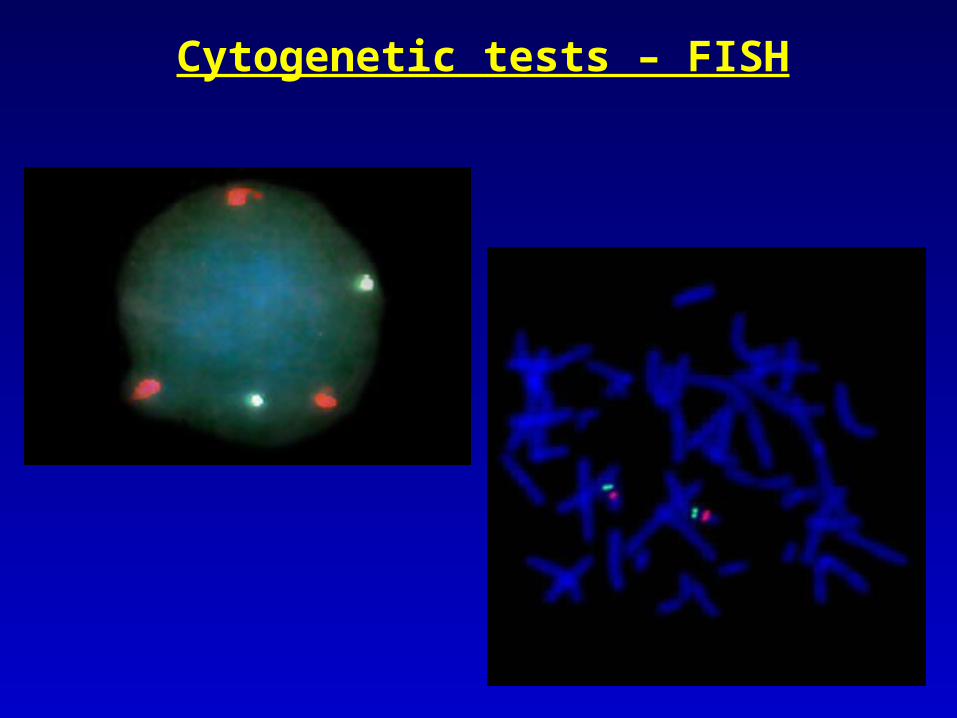
Cytogenetic tests – FISH
Cytogenetic tests – FISH
Indications:
• Detects specific microdeletions/microduplications
• Quick test for detection of abnormal chromosome number (pregnancy)
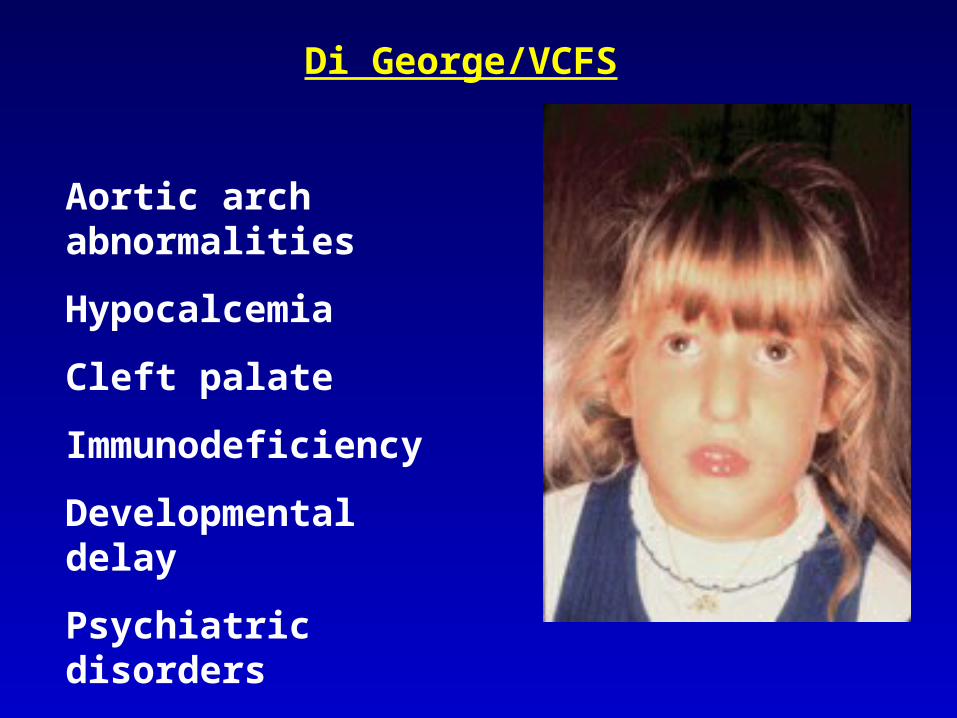
Di George/VCFS
Aortic arch abnormalities
Hypocalcemia
Cleft palate
Immunodeficiency
Developmental delay
Psychiatric disorders
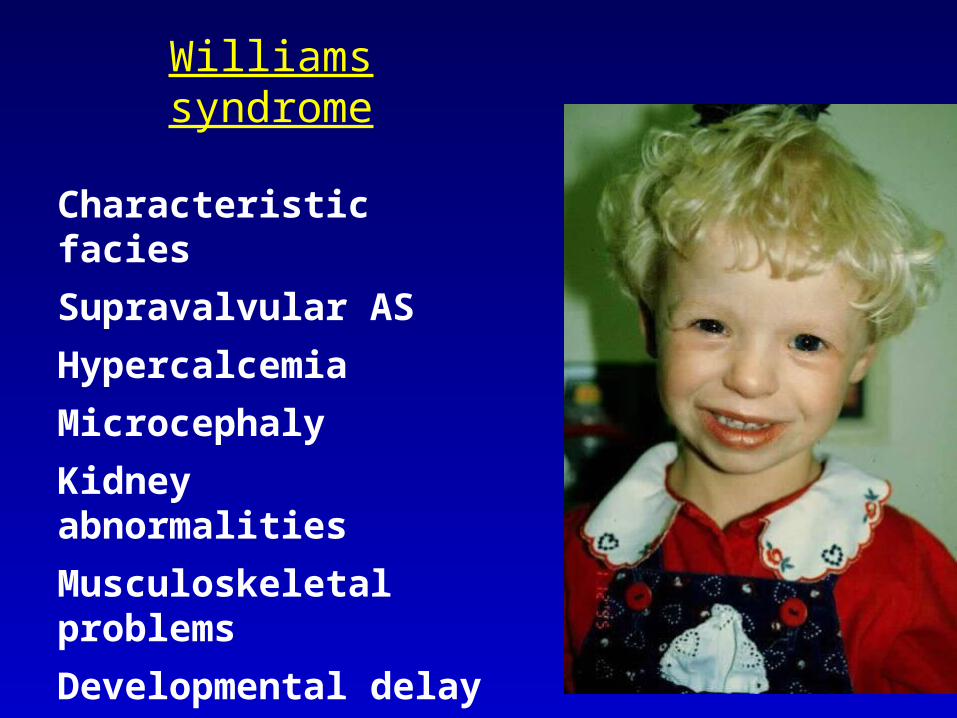
Williams syndrome
Characteristic facies
Supravalvular AS
Hypercalcemia
Microcephaly
Kidney abnormalities
Musculoskeletal problems
Developmental delay

Prader Willi/Angelman syndromePrader Willi/Angelman syndrome
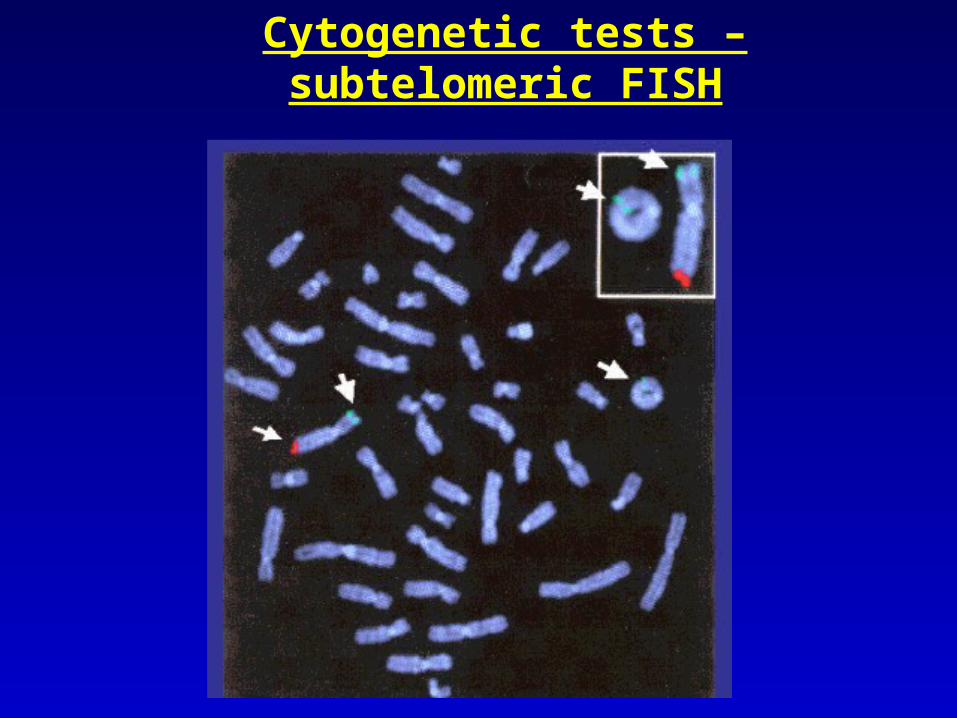
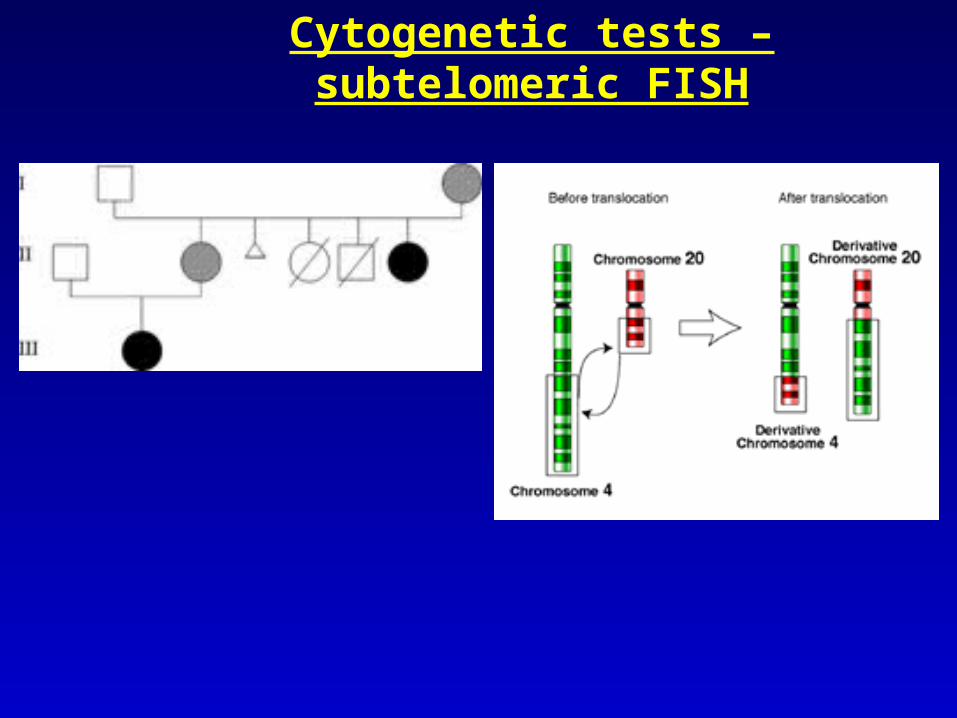
Cytogenetic tests – subtelomeric FISH
Cytogenetic tests – subtelomeric FISH
Indications:
Mental retardation/dysmorphic features/congenital anomalies
Familial cases (especially if variable clinical features
Detects deletions/duplications of the subtelomeric regions
Cytogenetic tests – subtelomeric FISH
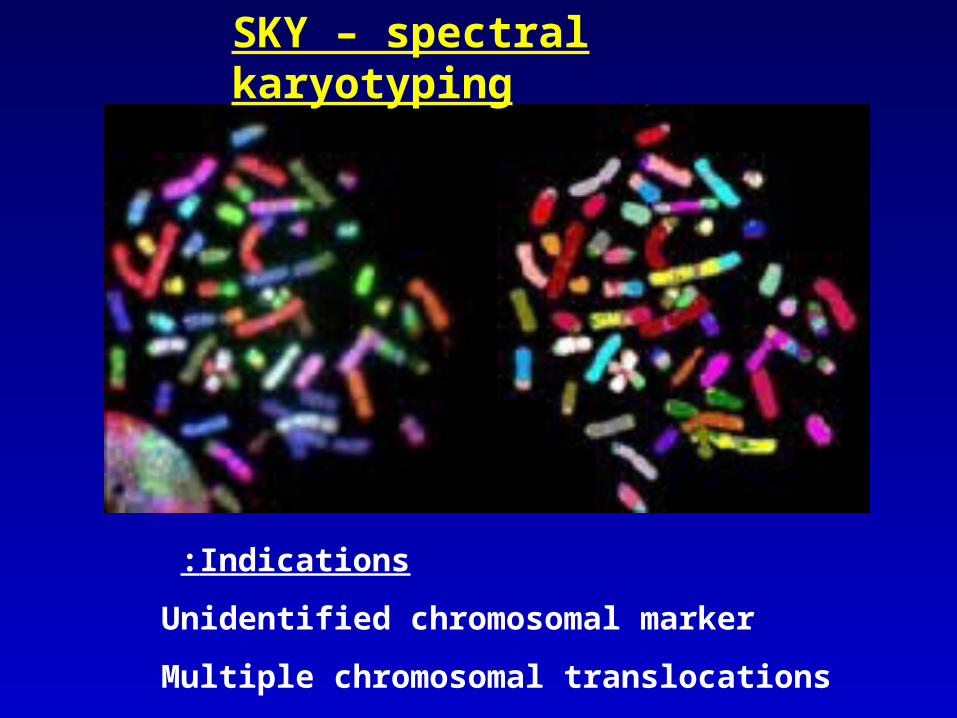
SKY – spectral karyotyping
Indications:
Unidentified chromosomal marker
Multiple chromosomal translocations
Molecular cytogenetic techniques
Array CGH
SNP array
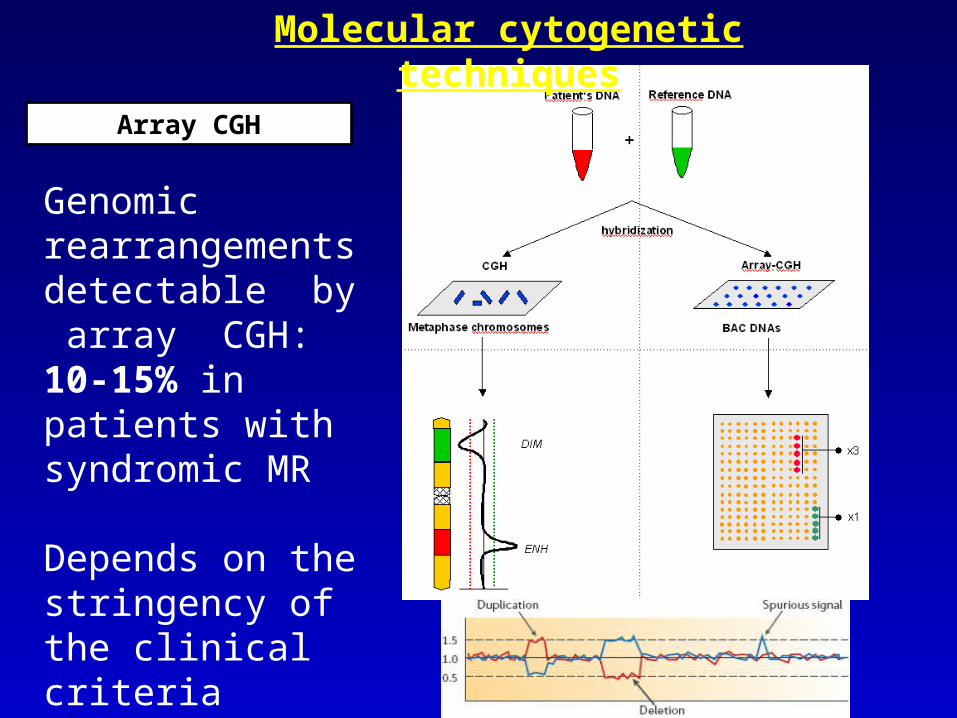
Array CGH
Genomic rearrangements detectable by array CGH: 10-15% in patients with syndromic MR
Depends on the stringency of the clinical criteria
Molecular cytogenetic techniques
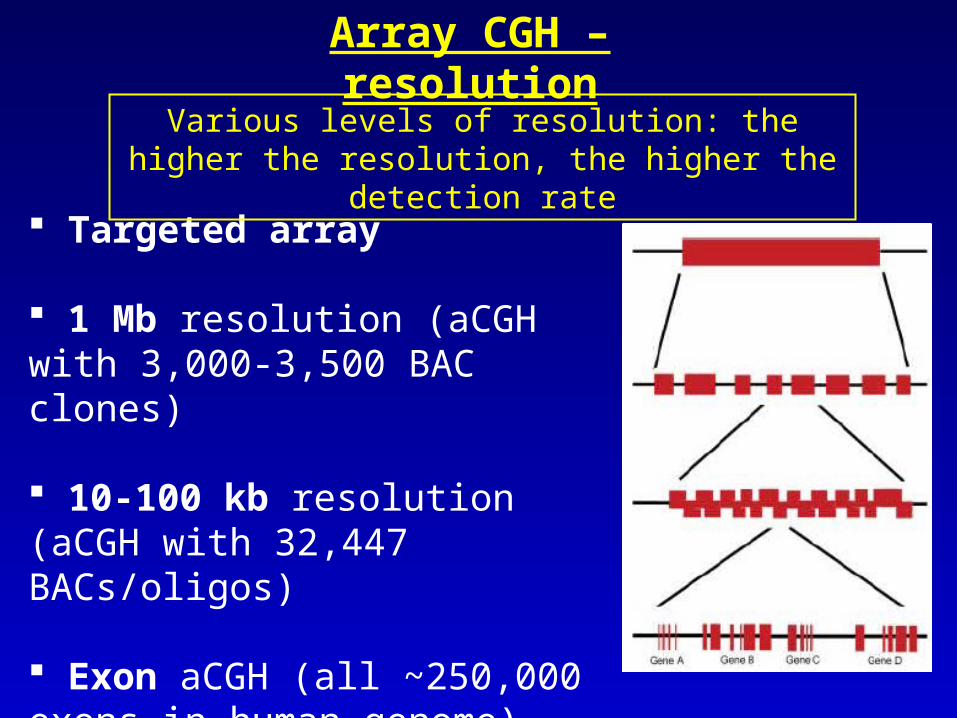
Targeted array
1 Mb resolution (aCGH with 3,000-3,500 BAC clones)
10-100 kb resolution (aCGH with 32,447 BACs/oligos)
Exon aCGH (all ~250,000 exons in human genome)
Array CGH – resolution
Various levels of resolution: the higher the resolution, the higher the detection rate
Indications:
Mental retardation/dysmorphic features/congenital anomalies
Detection of microdeletions, microduplications
No need for specific diagnosis
Array CGH
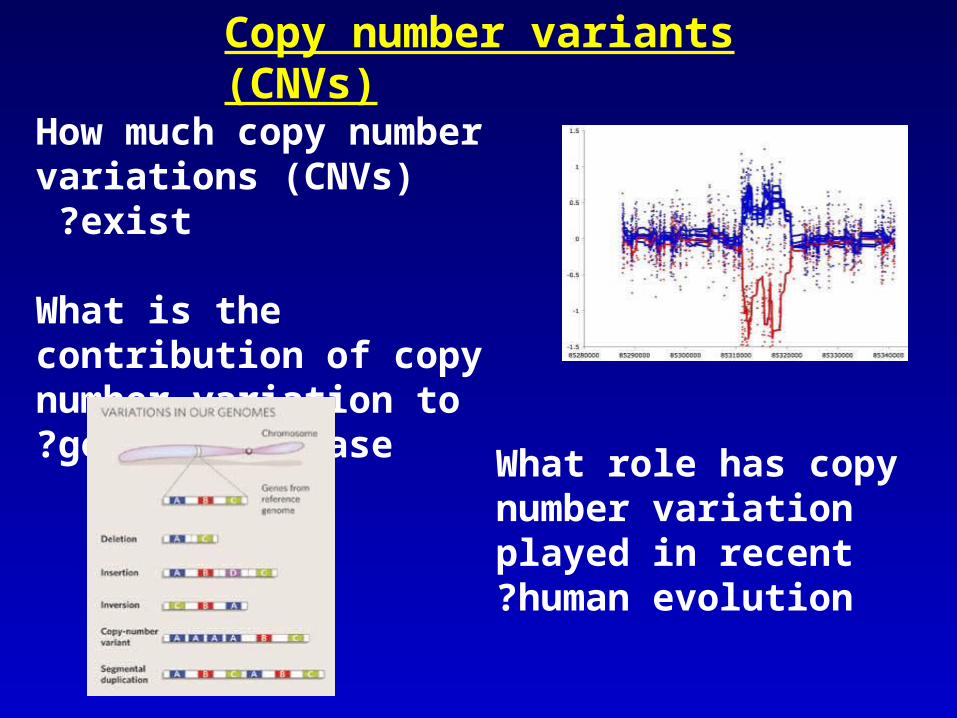
Copy number variants (CNVs)
How much copy number variations (CNVs) exist ?
What is the contribution of copy number variation to genetic disease?
What role has copy number variation played in recent human evolution?

SNP array
CCCCAGCCTCCTTGCCAACGCCCCCTTTCCCTCTCCCCCTCCCGCTCGGCGCTGACCCCCCATCCCCACCCCCGTGGGAACACTGGGAGCCTGCACTCCACAGACCCTCTCCTTGCCTCTTCCCTCACCTCAGCCTCCGCTCCCCGCCCTCTTCCCGGCCCAGGGCGCCGGCCCACCCTTCCCTCCGCCGCCCCCCGGCCGCGGGGAGGACATGGCCGCGCACAGGCCGGTGGAATGGGTCCAGGCCGTGGTCAGCCGCTTCGACGAGCAGCTTCCAATAAAAACAGGACAGCAGAACACACATACCAAAGTCAGTACTGAGCACAACAAGGAATGTCTAATCAATATTTCCAAATACAAGTTTTCTTTGGTTATAAGCGGCCTCACTACTATTTTAAAGAATGTTAACAATATGAGAATATTTGGAGAAGCTGCTGAAAAAAATTTATATCTCTCTCAGTTGATTATATTGGATACACTGGAAAAATGTCTTGCTGGGCAACCAAAGGACACAATGAGATTAGATGAAACGATGCTGGTCAAACAGTTGCTGCCAGAAATCTGCCATTTTCTTCACACCTGTCGTGAAGGAAACCAGCATGCAGCTGAACTTCGGAATTCTGCCTCTGGGGTTTTATTTTCTCTCAGCTGCAACAACTTCAATGCAGTCTTTAGTCGCATTTCTACCAGGTTACAGGAATTAACTGTTTGTTCAGAAGACAATGTTGATGTTCATGATATAGAATTGTTACAGTATATCAATGTGGATTGTGCAAAATTAAAACGACTCCTGAAGGAAACAGCATTTAAATTTAAAGCCCTAAAGAAGGTTGCGCAGTTAGCAGTTATAAATAGCCTGGAAAAGGCATTTTGGAACTGGGTAGAAAATTATCCAGATGAATTTACAAAACTGTACCAGATCCCACAGACTGATATGGCTGAATGTGCAGAAAAGCTATTTGACTTGGTGGATGGTTTTGCTGAAAGCACCAAACGTAAAGCAGCAGTTTGGCCACTACAAATCATTCTCCTTATCTTGTGTCCAGAAATAATCCAGGATATATCCAAAGACGTGGTTGATGAAAACAACATGAATAAGAAGTTATTTCTGGACAGTCTACGAAAAGCTCTTGCTGGCCATGGAGGAAGTAGGCAGCTGACAGAAAGTGCTGCAATTGCCTGTGTCAAACTGTGTAAAGCAAGTACTTACATCAATTGGGAAGATAACTCTGTCATTTTCCTACTTGTTCAGTCCATGGTGGTTGATCTTAAGAACCTGCTTTTTAATCCAAGTAAGCCATTCTCAAGAGGCAGTCAGCCTGCAGATGTGGATCTAATGATTGACTGCCTTGTTTCTTGCTTTCGTATAAGCCCTCACAACAACCAACACTTTAAGATCTGCCTGGCTCAGAATTCACCTTCTACATTTCACTATGTGCTGGTAAATTCACTCCATCGAATCATCACCAATTCCGCATTGGATTGGTGGCCTAAGATTGATGCTGTGTATTGTCACTCGGTTGAACTTCGAAATATGTTTGGTGAAACACTTCATAAAGCAGTGCAAGGTTGTGGAGCACACCCAGCAATACGAATGGCACCGAGTCTTACATTTAAAGAAAAAGTAACAAGCCTTAAATTTAAAGAAAAACCTACAGACCTGGAGACAAGAAGCTATAAGTATCTTCTCTTGTCCATGGTGAAACTAATTCATGCAGATCCAAAGCTCTTGCTTTGTAATCCAAGAAAACAGGGGCCCGAAACCCAAGGCAGTACAGCAGAATTAATTACAGGGCTCGTCCAACTGGTCCCTCAGTCACACATGCCAGAGATTGCTCAGGAAGCAATGGAGGCTCTGCTGGTTCTTCATCAGTTAGATAGCATTGATTTGTGGAATCCTGATGCTCCTGTAGAAACATTTTGGGAGATTAGCTCACAAATGCTTTTTTACATCTGCAAGAAATTAACTAGTCATCAAATGCTTAGTAGCACAGAAATTCTCAAGTGGTTGCGGGAAATATTGATCTGCAGGAATAAATTTCTTCTTAAAAATAAGCAGGCAGATAGAAGTTCCTGTCACTTTC
CCCCAGCCTCCTTGCCAACGCCCCCTTTCCCTCTCCCCCTCCCGCTCGGCGCTGACCCCCCATCCCCACCCCCGTGGGAACACTGGGAGCCTGCACTCCACAGACCCTCTCCTTGCCTCTTCCCTCACCTCAGCCTCCGCTCCCCGCCCTCTTCCCGGCCCAGGGCGCCGGCCCACCCTTCCCTCCGCCGCCCCCCGGCCGCGGGGAGGACATGGCCGCGCACAGGCCGGTGGAATGGGTCCAGGCCGTGGTCAGCCGCTTCGACGAGCAGCTTCCAATAAAAACAGGACAGCAGAACACACATACCAAAGTCAGTACTGAGCACAACAAGGAATGTCTAATCAATATTTCCAAATACAAGTTTTCTTTGGTTATAAGCGGCCTCACTACTATTTTAAAGAATGTTAACTATATGAGAATATTTGGAGAAGCTGCTGAAAAAAATTTATATCTCTCTCAGTTGATTATATTGGATACACTGGAAAAATGTCTTGCTGGGCAACCAAAGGACACAATGAGATTAGATGAAACGATGCTGGTCAAACAGTTGCTGCCAGAAATCTGCCATTTTCTTCACACCTGTCGTGAAGGAAACCAGCATGCAGCTGAACTTCGGAATTCTGCCTCTGGGGTTTTATTTTCTCTCAGCTGCAACAACTTCAATGCAGTCTTTAGTCGCATTTCTACCAGGTTACAGGAATTAACTGTTTGTTCAGAAGACAATGTTGATGTTCATGATATAGAATTGTTACAGTATATCAATGTGGATTGTGCAAAATTAAAACGACTCCTGAAGGAAACAGCATTTAAATTTAAAGCCCTAAAGAAGGTTGCGCAGTTAGCAGTTATAAATAGCCTGGAAAAGGCATTTTGGAACTGGGTAGAAAATTATCCAGATGAATTTACAAAACTGTACCAGATCCCACAGACTGATATGGCTGAATGTGCAGAAAAGCTATTTGACTTGGTGGATGGTTTTGCTGAAAGCACCAAACGTAAAGCAGCAGTTTGGCCACTACAAATCATTCTCCTTATCTTGTGTCCAGAAATAATCCAGGATATATCCAAAGACGTGGTTGATGAAAACAACATGAATAAGAAGTTATTTCTGGACAGTCTACGAAAAGCTCTTGCTGGCCATGGAGGAAGTAGGCAGCTGACAGAAAGTGCTGCAATTGCCTGTGTCAAACTGTGTAAAGCAAGTACTTACATCAATTGGGAAGATAACTCTGTCATTTTCCTACTTGTTCAGTCCATGGTGGTTGATCTTAAGAACCTGCTTTTTAATCCAAGTAAGCCATTCTCAAGAGGCAGTCAGCCTGCAGATGTGGATCTAATGATTGACTGCCTTGTTTCTTGCTTTCGTATAAGCCCTCACAACAACCAACACTTTAAGATCTGCCTGGCTCAGAATTCACCTTCTACATTTCACTATGTGCTGGTAAATTCACTCCATCGAATCATCACCAATTCCGCATTGGATTGGTGGCCTAAGATTGATGCTGTGTATTGTCACTCGGTTGAACTTCGAAATATGTTTGGTGAAACACTTCATAAAGCAGTGCAAGGTTGTGGAGCACACCCAGCAATACGAATGGCACCGAGTCTTACATTTAAAGAAAAAGTAACAAGCCTTAAATTTAAAGAAAAACCTACAGACCTGGAGACAAGAAGCTATAAGTATCTTCTCTTGTCCATGGTGAAACTAATTCATGCAGCTCCAAAGCTCTTGCTTTGTAATCCAAGAAAACAGGGGCCCGAAACCCAAGGCAGTACAGCAGAATTAATTACAGGGCTCGTCCAACTGGTCCCTCAGTCACACATGCCAGAGATTGCTCAGGAAGCAATGGAGGCTCTGCTGGTTCTTCATCAGTTAGATAGCATTGATTTGTGGAATCCTGATGCTCCTGTAGAAACATTTTGGGAGATTAGCTCACAAATGCTTTTTTACATCTGCAAGAAATTAACTAGTCATCAAATGCTTAGTAGCACAGAAATTCTCAAGTGGTTGCGGGAAATATTGATCTGCAGGAATAAATTTCTTCTTAAAAATAAGCAGGCAGATAGAAGTTCCTGTCACTTTC
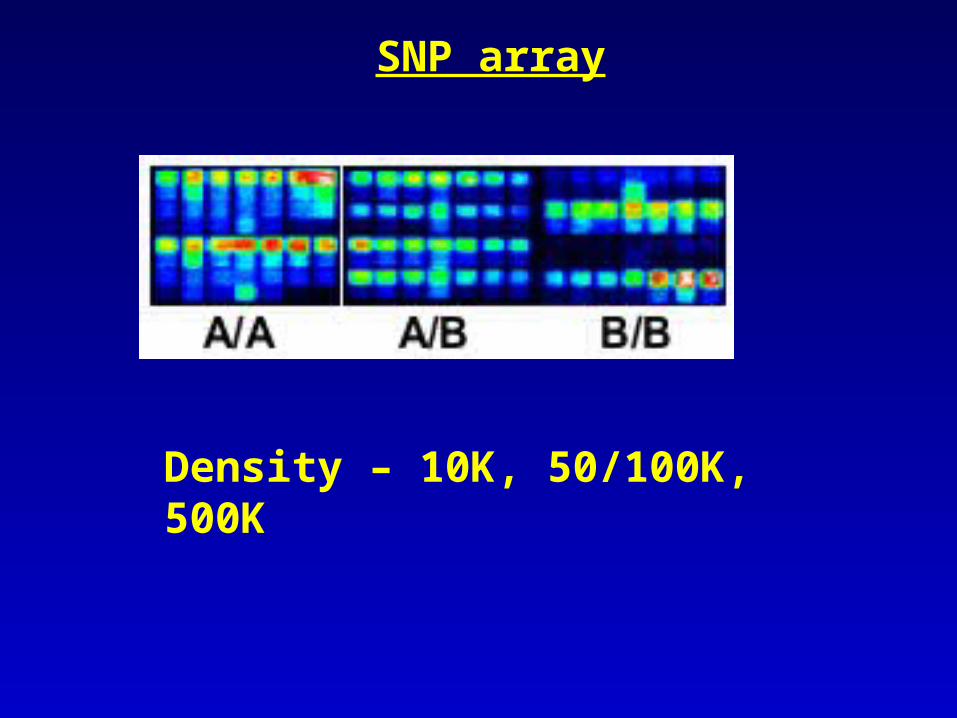
SNP array
Density – 10K, 50/100K, 500K
DNA tests
DNA tests
• Direct mutation analysis– DNA sequencing– Specific mutation analysis– Deletion analysis
• Linkage analysis – utilization of traceable gene markers
next to the gene of interest
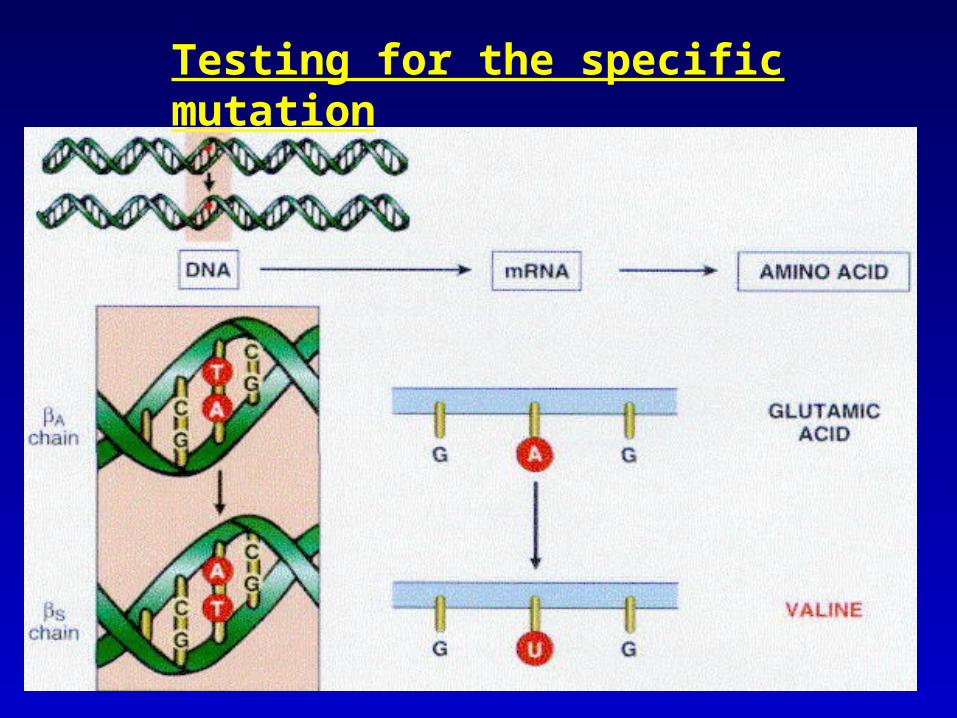
Testing for the specific mutation
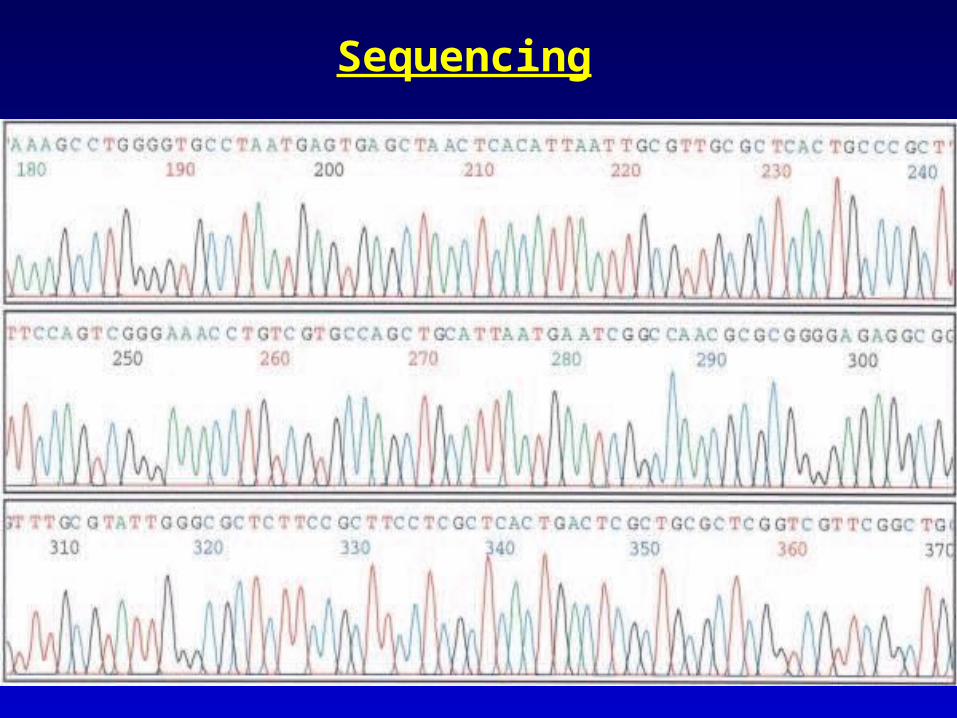
Sequencing
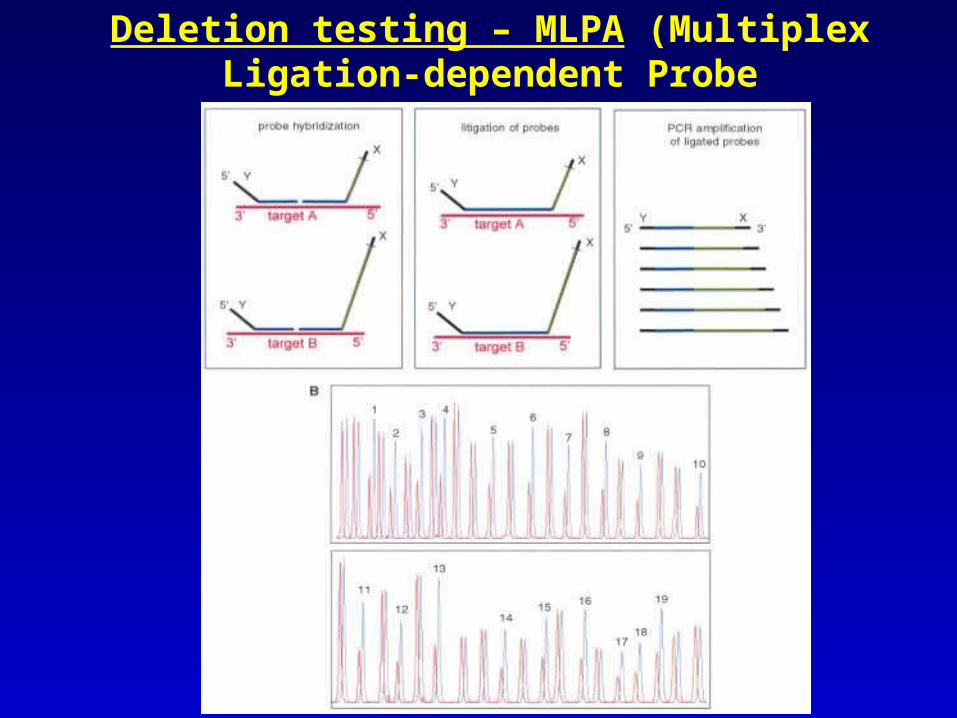
Deletion testing – MLPA (Multiplex Ligation-dependent Probe
Amplification )
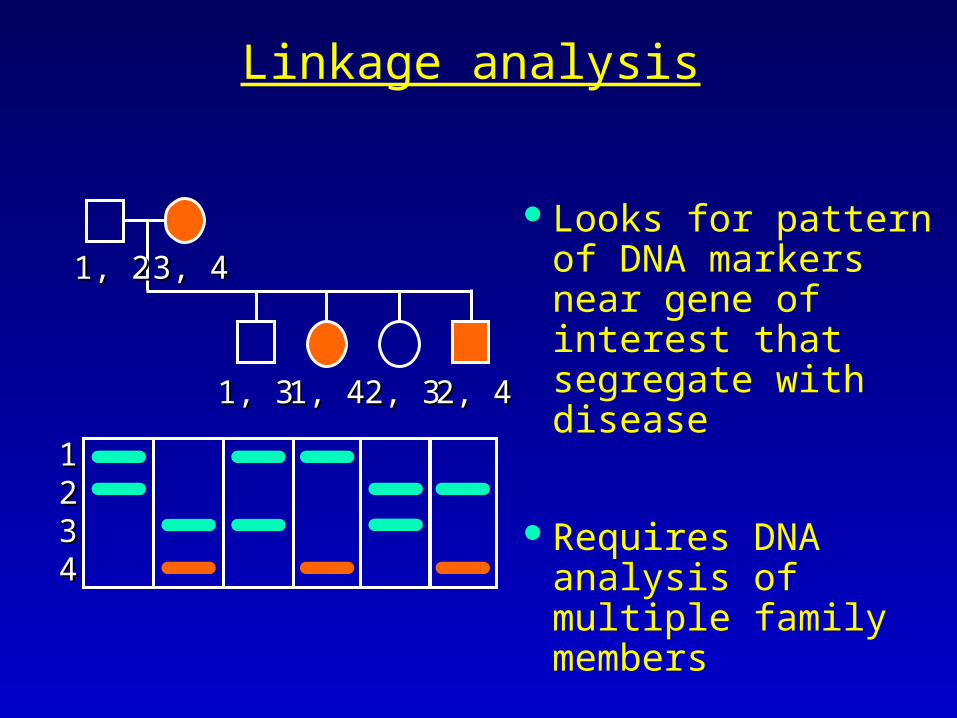
Linkage analysis
Looks for pattern of DNA markers near gene of interest that segregate with disease
Requires DNA analysis of multiple family members
1, 21, 2 3, 43, 4
1, 31, 3 1, 41, 4 2, 32, 3 2, 42, 4
11223344
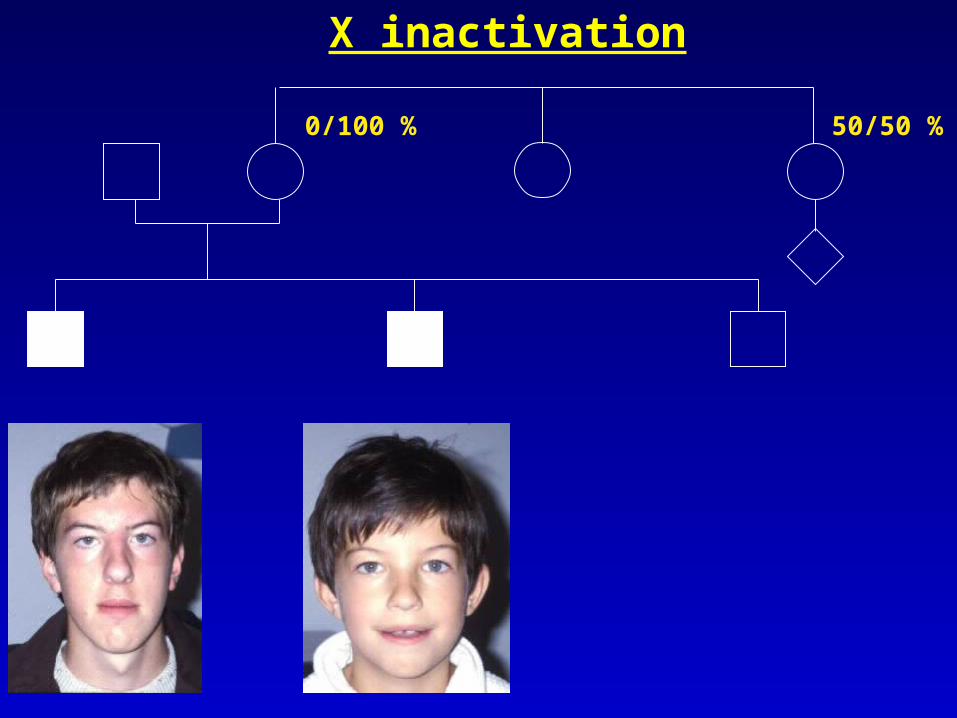
0/100 %
50/50 %
X inactivation
Genetic testing in the fetus
Non-disclosing prenatal testing
The parent is at 50% risk and is not showing symptoms. In this case, to find
that the fetus carries the gene for Huntington's disease automatically
reveals that the parent is a gene-carrier as well
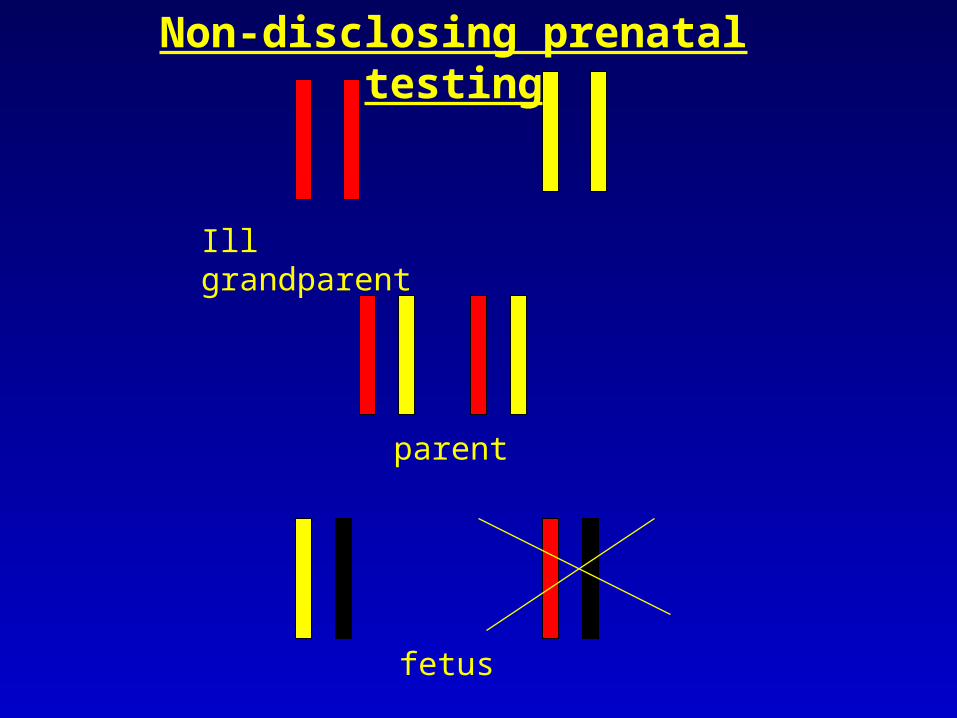
Ill grandparent
parent
fetus
Non-disclosing prenatal testing
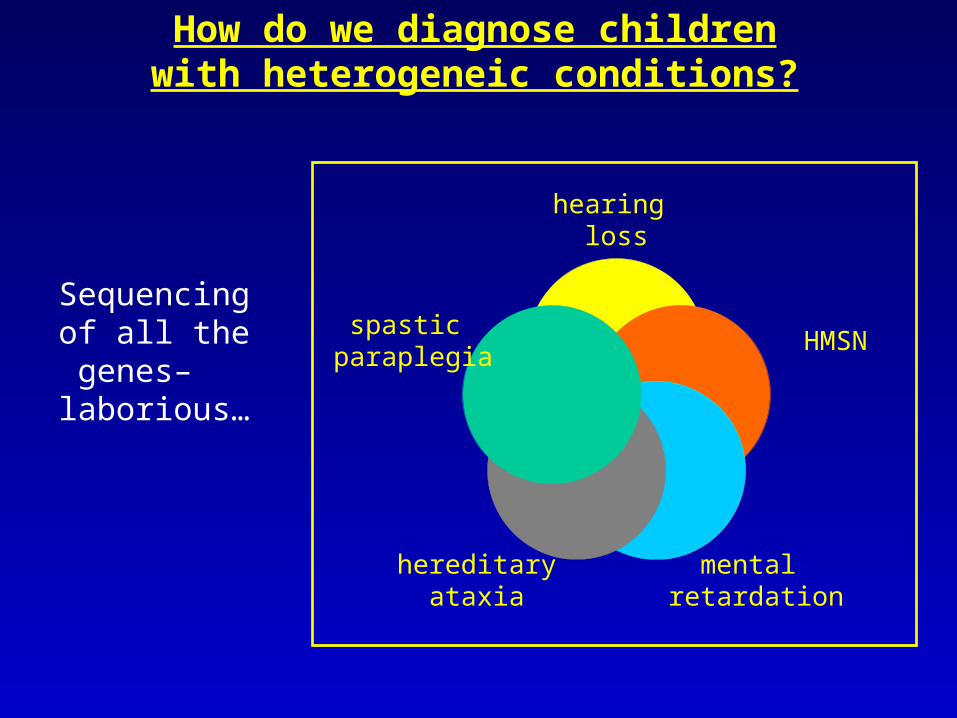
Sequencing of all the genes– laborious…
How do we diagnose children with heterogeneic conditions?
hearing loss
HMSN
mental retardation
hereditaryataxia
spastic paraplegia
MR: etiology
Resequencing microarray
Recently, a resequencing microarray has been developed for XLMR genes
On this chip 17 XLMR genes are represented, including frequently mutated genes such as ARX, JARID1C and PQBP1
Together they account for approximately 40% of all mutations in MR genes on the X chromosome
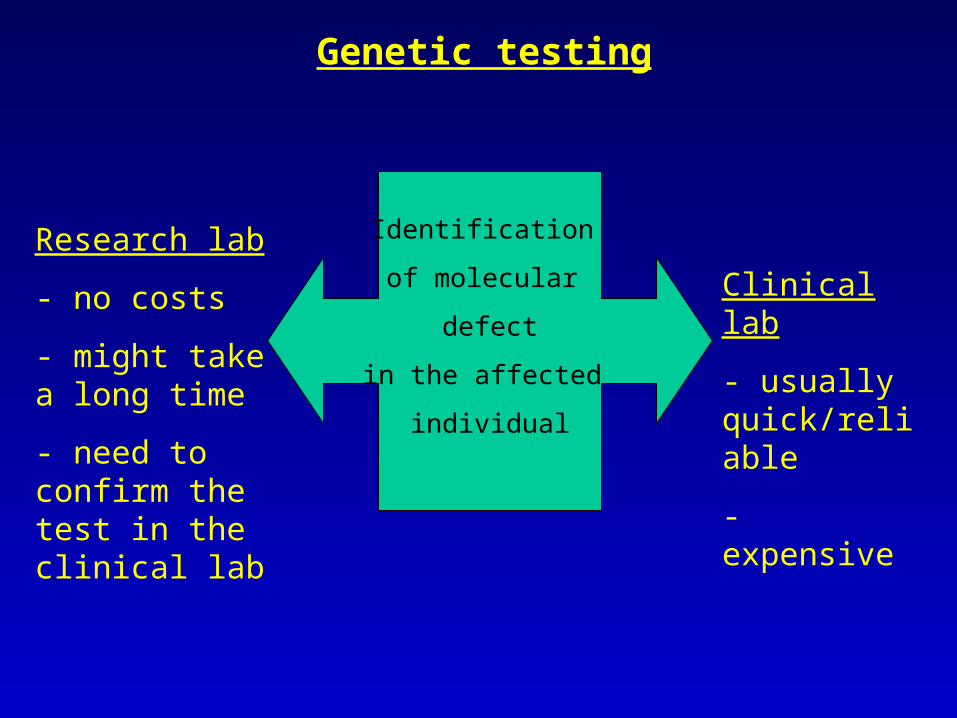
Genetic testing
Identification
of molecular
defect
in the affected
individual
Research lab
- no costs
- might take a long time
- need to confirm the test in the clinical lab
Clinical lab
- usually quick/reliable
- expensive
Attitude of different populations towards
prenatal testing
Non religious Jews: prenatal testing by CVS or amniocentesis (pregnancy interruption possible up to birth, even at 40 weeks of pregnancy); preimplantation genetic diagnosis
Orthodox Jews: preimplantation genetic diagnosis (pregnancy interruption possible up to 40 days only – no prenatal testing possible)
Muslim Arabs: prenatal testing by CVS or amniocentesis; (pregnancy interruption possible up to 120 days of pregnancy); preimplantation genetic diagnosis
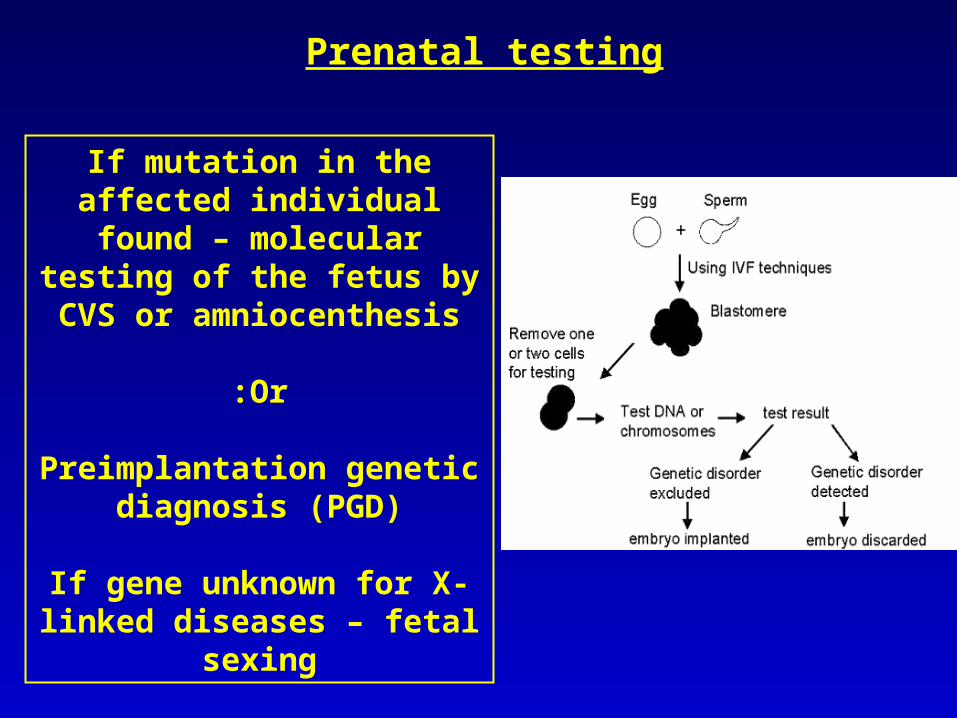
If mutation in the affected individual found – molecular
testing of the fetus by CVS or amniocenthesis
Or:
Preimplantation genetic diagnosis (PGD)
If gene unknown for X-linked diseases – fetal
sexing
Prenatal testing




















![biologi [lina].pptx](https://img.pdfslide.us/doc/110x75/55cf8680550346484b983780/biologi-linapptx.jpg)








