Embed Size (px)
Citation preview

Medical Complications of
Pregnancy: A Brief Review for
the Internal Medicine Resident
Kristen Amann, MDJuly 9, 2010
Quick Reminders
• Give all pregnant women folate to prevent neural tube defects (most effective in the 1st trimester)
• Treat asymptomatic bacteruria (20% will develop cystitis and/or pyelonephritis)
• hCG doubles every 2 days in the first trimester– Home pregnancy tests: positive ~ 2 weeks after
conception• Gravid uterus: abdomen at 12 weeks, umbilicus at
20 weeks• GP nomenclature:
– G (gravida): # of times pregnant– P (para): # births >20 weeks gestation
• (term), (preterm), (abortions), (living children)
Some Pertinent Teratogens
• Acyclovir• ACE Inhibitors• Diazepam• Fluconazole• Lithium• Warfarin• Aminoglycosides
• Isotretinoin (Accutane)
• Antineoplastic agents
• Carbamazepine• Methotrexate• Trimethoprim• Tetracycline• Phenytoin (Dilantin)
Sheehan’s Syndrome (Postpartum Pituitary Necrosis)• Major obstetric hemorrhage resulting in hypovolemic shock
and subsequent anterior pituitary ischemia and necrosis • Most common cause of anterior pituitary insufficiency in
females– Total: 0.5% of all hypopituitarism cases
• Clinical presentation:– Severe (recognized within the first days to weeks): lethargy,
anorexia, fatigue, agalactorrhea– Less severe (weeks, months, or even years after delivery):
agalactorrhea, failure to resume menses, lethargy• Physiology:
– Hypertrophy and hyperplasia of lactotrophs during pregnancy resulting in enlargement of the anterior pituitary
– Anterior pituitary supplied by low pressure venous system (versus posterior pituitary having direct arterial supply).
– Major hormones secreted: TSH, ACTH, LH, FSH, GH, prolactin• If blood loss is severe, immediately treat for presumed
adrenal insufficiency
Diabetes Mellitus
• Optimization of pre-conceptional DM and during key periods of organogenesis can reduce risk for fetal malformations – Sacral agenesis, caudal dysplasia, renal
agenesis, VSD, hypertrophic cardiomyopathy, etc.
• Increased risk for preeclampsia• DM + microvascular disease: higher risk for
IUGR• Fasting glucose goals: 105-140• Treatment: diet, insulin
– ADA and ACOG do not endorse oral hypoglycemic agents
HELLP• Hemolysis, Elevated Liver enzymes, Low Platelets• Develops in 10-20% of patients with severe
preeclampsia/eclampsia• Overall occurrence: 1-2 per 1,000 pregnancies• Usually occurs in 3rd trimester but can occur in 2nd
and post-partum• Clinical:
– RUQ/epigastric pain, nausea, vomiting, malaise– MAHA, Plt <100,000, AST >70, LDH >600
• Significant morbidity: DIC, AKI, ARDS, subcapsular liver hematoma, etc.
• Treatment: delivery, supportive management, HTN control, magnesium (seizure prevention), platelet transfusion for <20,000 or for significant bleeding
Acute Fatty Liver of Pregnancy
• Usually in the 3rd trimester but may occur in the 2nd • Maternal mortality: <3%• More common with male fetus• Etiology hypothesis: Disordered metabolism of fatty
acids in the patient’s mitochondria caused by LCHAD (long-chain-3-hydroxyl acyl DH) deficiency
• Clinical:– Liver is typically small– Transaminitis (<500 IU/L), elevated bilirubin, elevated
ammonia, hypoglycemia, prolonged INR• Usually necessitates termination of pregnancy due
to fetal distress• Treatment: supportive care, fetal delivery• Recurrence is rare
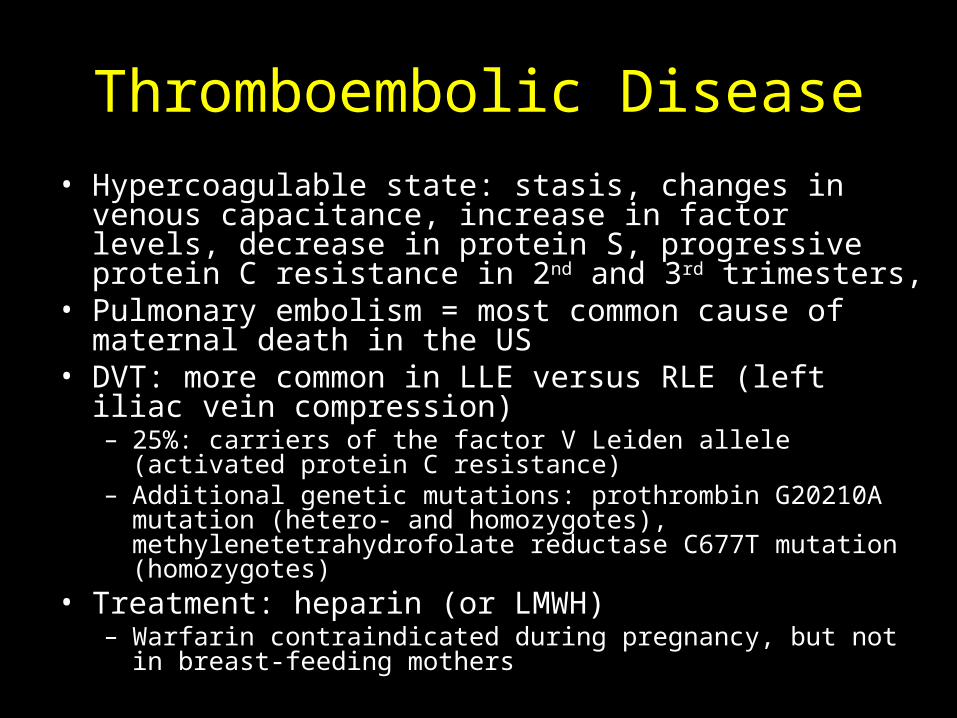
Thromboembolic Disease• Hypercoagulable state: stasis, changes in venous
capacitance, increase in factor levels, decrease in protein S, progressive protein C resistance in 2nd and 3rd trimesters,
• Pulmonary embolism = most common cause of maternal death in the US
• DVT: more common in LLE versus RLE (left iliac vein compression)– 25%: carriers of the factor V Leiden allele (activated
protein C resistance)– Additional genetic mutations: prothrombin G20210A
mutation (hetero- and homozygotes), methylenetetrahydrofolate reductase C677T mutation (homozygotes)
• Treatment: heparin (or LMWH)– Warfarin contraindicated during pregnancy, but not in
breast-feeding mothers
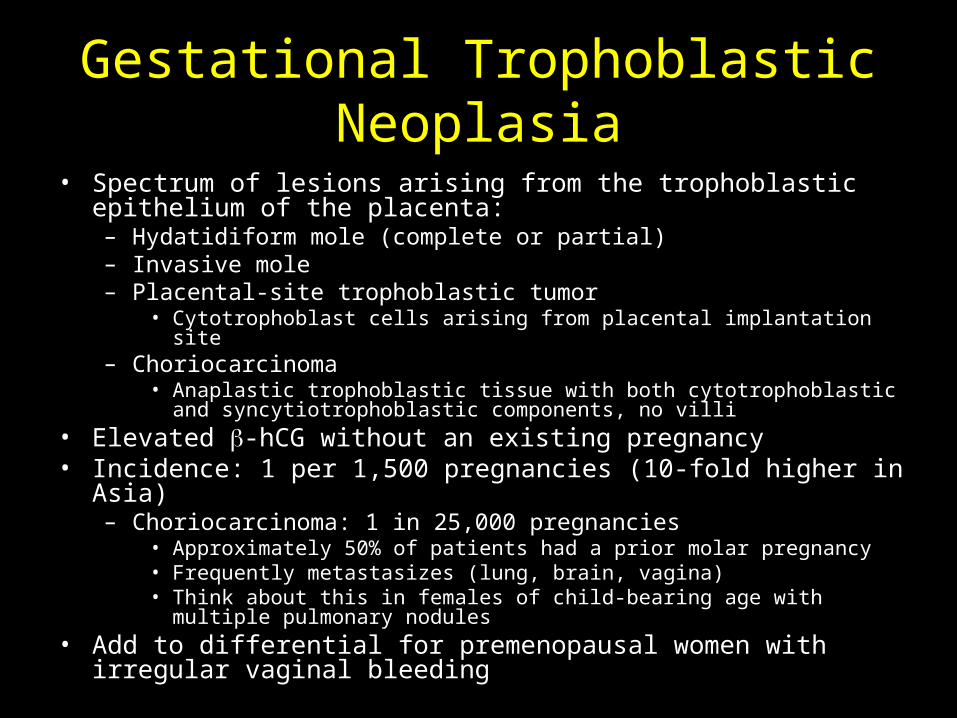
Gestational Trophoblastic Neoplasia
• Spectrum of lesions arising from the trophoblastic epithelium of the placenta:– Hydatidiform mole (complete or partial)– Invasive mole– Placental-site trophoblastic tumor
• Cytotrophoblast cells arising from placental implantation site– Choriocarcinoma
• Anaplastic trophoblastic tissue with both cytotrophoblastic and syncytiotrophoblastic components, no villi
• Elevated -hCG without an existing pregnancy• Incidence: 1 per 1,500 pregnancies (10-fold higher in Asia)
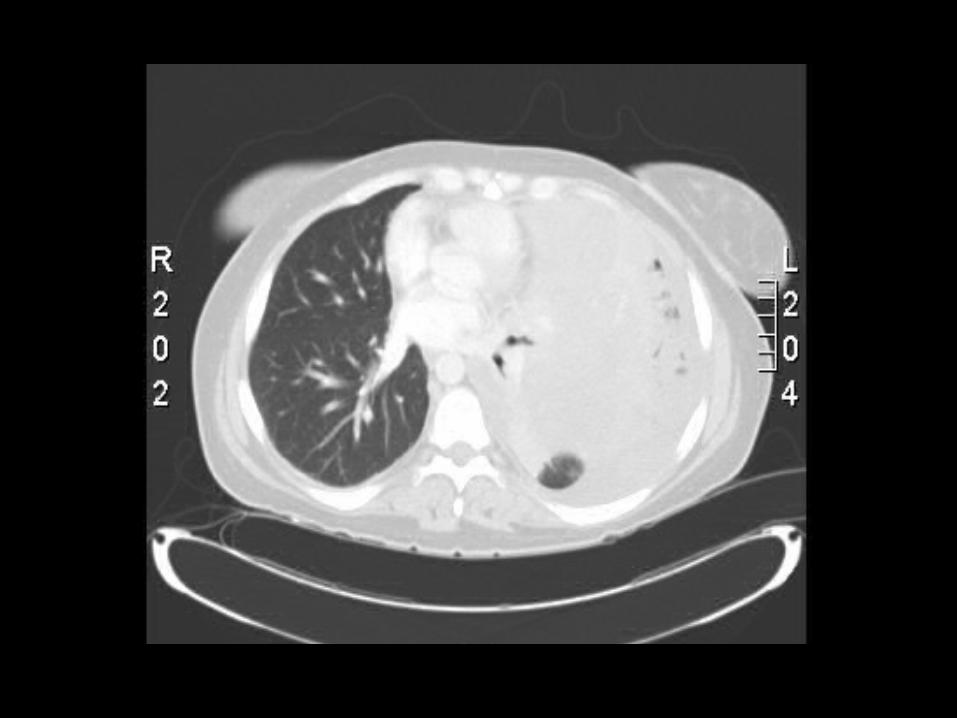
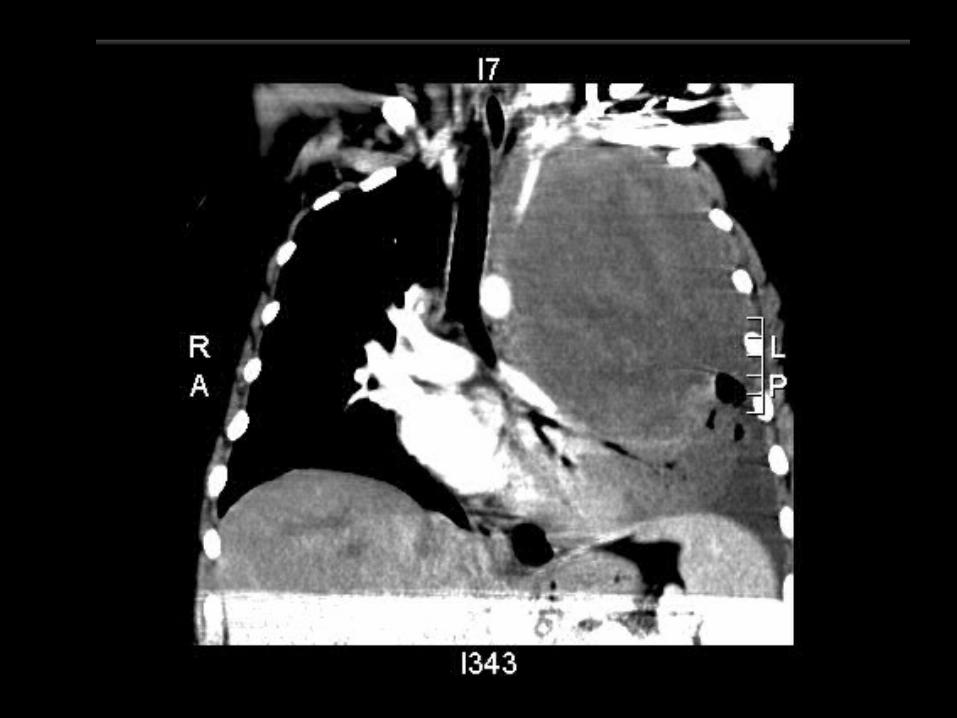
– Choriocarcinoma: 1 in 25,000 pregnancies• Approximately 50% of patients had a prior molar pregnancy• Frequently metastasizes (lung, brain, vagina)• Think about this in females of child-bearing age with multiple
pulmonary nodules• Add to differential for premenopausal women with irregular
vaginal bleeding
Thanks for listening!(See next slide for sources)
Sources• Dunaif, A. Women’s Health. Harrison’s Principles of Internal Medicine, 16th
edition. McGraw-Hill, New York. 2005.• Snyder, P. Causes of Hypopituitarism. www.uptodate.com. • Teratogens. http://sis.nlm.nih.gov.• The American College of Obstetrics and Gynecology. www.acog.org.• Young, D. Gynecologic Malignancies. Harrison’s Principles of Internal
Medicine, 16th edition. McGraw-Hill, New York. 2005.