Embed Size (px)
Citation preview

MEDICAL APPLICATIONS OF X-RAY FLUORESCENCE FOR TRACE ELEMENT RESEARCH
Jimmy Börjesson1 and Sören Mattsson2
1Department of Diagnostic Radiology, County Hospital, SE-301 85 Halmstad, Sweden 2Department of Radiation Physics, Lund University, Malmö University Hospital, SE-205 02
Malmö, Sweden
ABSTRACT
Techniques for estimation of element levels directly in humans (non-invasive in vivo) or in sam-ples (in vitro) from humans are reviewed. Toxic, nonessential, trace elements may cause tempo-rary or permanent damage to various organs and tissues in humans. There is thus a need to con-trol the concentrations. Knowledge of the relations between toxic effects and element concentra-tion may be extracted from measurements in humans, samples from humans, and the environ-ment. Applications traditionally include occupationally exposed subjects, but an increasing re-search area is studies of members of the general population and of patients undergoing therapy for malignant and other diseases. Most in vivo XRF studies deal with lead in bone cadmium in kidneys. For retired lead workers, a clear association has been demonstrated between bone lead and blood lead, due to endogenous lead excretion from the skeleton. A study of mercury in vivo showed that the technique is capable of detecting mercury in heavily exposed worker’s kidneys. In vivo XRF in cancer and rheumatology patients has helped to understand how platinum and gold are retained in the human body. The newest in vivo applications include zinc in prostate gland and arsenic in skin.
INTRODUCTION
Elements, harmful to the human body, must be controlled. For some elements exposure is re-stricted to workers handling the particular element but for many substances exposure to the gen-eral population may be significant. Occupational and environmental research may include meas-urements in vivo as well as in vitro. Measured concentrations in organs and tissues can in this way be related to single or time cumulated concentrations of the element in e.g. air, water, blood and urine samples. Furthermore, concentrations may be linked to observable toxic effects and can eventually be used to establish exposure limits. This paper is an introduction to in vivo and in vitro XRF applied to medical science. Reviews of in vivo XRF are found elsewhere [1–6].
RATIONALE FOR XRF IN VIVO
Element concentrations in blood and urine may, in some special cases, be used to predict the ele-ment concentration in an organ. However, blood and urine levels depend on, e.g. endogenous and ongoing exposure, kidney function, individual differences in element kinetics. Thus, rela-tionships between body fluids and organs are neither simple nor well-known. Faeces and hair for the estimation of element concentrations in body tissues and the exposure level imply indirect measurements. Faeces collection is a rather unpleasant sampling method whereas hair is easily collected but possesses a risk of external contamination. Hair formation is also slow. A biopsy
1Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

This document was presented at the Denver X-ray Conference (DXC) on Applications of X-ray Analysis. Sponsored by the International Centre for Diffraction Data (ICDD). This document is provided by ICDD in cooperation with the authors and presenters of the DXC for the express purpose of educating the scientific community. All copyrights for the document are retained by ICDD. Usage is restricted for the purposes of education and scientific research. DXC Website – www.dxcicdd.com
ICDD Website - www.icdd.com
Advances in X-ray Analysis, Volume 50

presents the element concentration at the site of sampling and is not necessarily a representation of the mean level in an organ. The procedure is invasive; it may hurt and imply a risk for infec-tion. Repetition of the sampling may not be possible. An autopsy specimen provides information of element concentrations in tissues of, e.g. a deceased occupationally exposed worker. How-ever, a long time may have elapsed between exposure and sampling. Few occupationally ex-posed subjects may be available. Hence, the briefly discussed methods above should be consid-ered, not as “alternatives” to in vivo XRF but as techniques giving complementary information. ISSUES ON IN VIVO XRF Sample size, measurement depth and time The sample size and the depth to the sampled volume in a living human being are huge com-pared to, e.g. a laboratory sample studied in vitro. The attenuation of photons, directed towards the studied volume as well as the emitted X-rays from the element in that volume, is pronounced. For example, 23 keV cadmium X-rays are attenuated by 98% when passing through 50 mm of water, i.e. a typical distance between the detector at the skin and the kidney. The attenuation means that for in vivo KXRF, elements must have a Z higher than ≈ 25 and that for 25 < Z < 45 studies are limited to the most superficial tissues. The measurement time is also limited. A subject may sit or lay immobile for as long as one or maybe two hours at the most. For an ill patient, fighting cancer with cytostatic agents, a meas-urement time of ten minutes may feel like a very long time. Detection limit, radiation dose The minimum detectable concentration (MDC) we have used is defined as follows:
net
bg
N
NCMDC ∗= 3
where Nbg is the background counts under the characteristic X-ray peaks, Nnet the net counts in the peaks and C the element concentration. As Nbg and Nnet both linearly depend on the meas-urement time, the MDC is inversely proportional to the square root of the measurement time. The MDC varies strongly with measurement depth. If the detection limit for, e.g. the presently used XRF techniques for lead, cadmium and mercury, is put in perspective to the actual concen-trations found in man, cadmium and lead may be measured in the general population whereas mercury is essentially restricted to occupationally exposed subjects. The XRF radiation dose needs to fulfil at least two requirements to be acceptable. First, the equivalent dose must be low enough not to cause deterministic effects, such as skin erythema. Second, the effective dose must imply a reasonably low stochastic radiation risk of late effects, e.g. cancer induction. Thus, the effective dose should be comparable or less than at a diagnostic radiology procedure, e.g. a planar lung X-ray examination. Fortunately, the effective doses in XRF are low [7].
2Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

ELEMENTS OF INTEREST FOR IN VIVO XRF Non-invasive in vivo XRF was started by Hoffer et al.’ [8] measurements of iodine in the thyroid gland. Ahlgren et al. [9] developed a technique to measure lead in bone. Several alternative bone lead XRF techniques have evolved [10–13]. Moreover feasibility and in vivo studies of cadmium, mercury, gold, platinum, uranium, zinc, arsenic, etc. have been published [14–21]. Table I summarises elements subject to in vivo XRF.
Table I. Principal measurement site and characteristic X-ray energies of in vivo XRF applications ([7] plus refer-ences therein and in this paper). A question mark indicates that the application or measurement site is based on
scarce information. Element Application In vivo measurement
site(s) Kα X-ray energies
(keV) Iron Medical (splinters, disease) Eye, skin 6.39,6.40
Copper Medical (splinters, disease) Eye, skin 8.03,8.05 Zinc Medical (splinters, disease) Eye, skin, prostate 8.62,8.64
Arsenic Occupational Skin 10.54, 11.73Strontium Natural abundance Bone 14.10,14.17Cadmium Occupational, environmental Kidneys, liver 22.98,23.17
Iodine Natural abundance, medical (X-ray contrast) Thyroid, blood 28.32,28.62Xenon Medical (cerebral blood flow) Brain 29.46,29.78Barium Medical (X-ray contrast) Lungs 31.82,32.19
Platinum Medical (cytotoxic agent) Kidneys, liver, tu-mours
65.12,66.83
Gold Medical (anti-rheumatic agent) Kidneys, liver, bone joints
66.99,68.81
Mercury Occupational, environmental Kidneys, liver?, thy-roid?, bone?
68.89,70.82
Lead Occupational, environmental Bone 72.80,74.97Bismuth Medical (treatm. ulcus duodeni, cytostatics?) GI-tract?, brain tu-
mour? 74.81,77.11
Thorium Medical (previously used X-ray contrast) Liver, spleen 89.96,93.35Uranium Nuclear weapons industry, “war”, “crime”
(uranium covered ammunition) Bone, lung 94.66,98.44
Photon source, polarisation, optimization Photons for the excitation of the element may come from an X-ray tube or from a γ-emitting ra-dionuclide source. A radionuclide may have advantages such as a suitable energy, negligible emission of unwanted γ- and β-radiation, high yield and high specific activity. If the source is
3Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

also compact it may be used in a transportable system. A short half-life and a high price may be drawbacks. Incoherent scattering in the human body’s mainly low Z element composition adds a large back-ground to the measured pulse height distribution. Due to a generally low element concentration the result is a small characteristic X-ray peak superimposed on a large background. This may partially be overcome if photons from an X-ray tube is used for the excitation. The high fluence from a tube allows partly plane-polarisation of the primary photons. In principle the photons are incoherently scattered in 90° before they enter the subject and the detector is put in the plane de-fined by the electric vector of the polarised photon. A reduced fluence rate of scattered photons will result if the detector axis is parallel to the electric vector. Collimation and multiple scatter-ing though largely reduce the benefit of polarisation to some 50%. Generally, the setup involve a large number of parameters (e.g., tube voltage, collimation, an-gles, filters, detector) and optimization is time consuming and costly. However, modern com-puters make it possible to simulate the measurement situation, using a Monte Carlo code: A number of codes are now available [18, 22–26]. Calibration, validation Calibration of an in vivo measurement technique is difficult. There is essentially no gold stan-dard and phantoms have to be used. Technical calibration phantoms for bone lead are tradition-ally made of lead doped wax and plaster-of-Paris. Phantoms of polyurethanes and calcium car-bonates and a synthetic apatite matrix have also been proposed. For calibration of cadmium, mercury and gold in kidneys and liver our group has used phantoms made of plastic cylinders filled with a solution of water and the element under study. The containers are placed in a large water tank and an individual calibration is made at the same depth as the in vivo measurement was made at. A few studies have validated the in vivo XRF measurement with a chemically determined ele-ment concentration in a biopsy of the measured volume. Others have measured the concentration in situ, using XRF, in autopsy material and then analysed the material chemically. Another vali-dation strategy is to use animal organs, e.g. animal kidneys immersed in water for simulation of in vivo XRF in the kidney. However, compared with the in vivo situation clearly visible horse kidneys, at an accurately known depth in a water tank, are not the same as a kidney at an un-known depth in a non-transparent person. OVERVIEW OF IN VIVO XRF APPLICATIONS IN MEDICINE Lead Occupational exposure may occur in e.g. the production and recycling of lead batteries. For the general population, exposure may come from food, drinking water and from ingested lead paint in homes. Lead accumulates in bone and the skeleton contains >90% of the body burden of lead. Bone lead increases with age, thus it may be used to estimate total lead exposure. Significantly higher tibia and blood lead concentrations in adults who, as children, were exposed to lead have
4Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

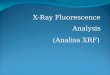
been reported [27,28]. Low-level lead exposure in childhood is suspected to result in distur-bances in mental development. Lead in fingerbone can be measured by irradiating the finger by two 57Co (122 and 136 keV) sources mounted opposite to each other [9] (see Figure 1). The lead K X-rays and incoherently scattered photons are detected using a high purity germanium detector (∅ 16 mm).
Figure 1. Photo of measurement setup for fingerbone lead measurement. The left index finger in measurement position with sources on top and bottom and the detec-tor with collimator in the background.
Another KXRF bone lead technique, for sampling of lead in tibia, calcaneus and patella, is based on an 88 keV 109Cd source and a large area detector [10]. The newest modification means that the large detector has been split into four smaller detectors with separate electronic chains, a so called clover leaf arrangement [13]. Reportedly, an improved in vivo detectability resulted and the technique seems ready for measurements in subjects of the general population. A third technique uses low photon energy LXRF from bone lead excited with a 109Cd source or an X-ray tube [29]. The “short-sighted” LXRF implies that the KXRF and LXRF methods pro-vide complementary information [30]. There is renewed interest in this method using a rhodium anode, molybdenum secondary target and a silicon detector [6]. Phantom studies indicate a de-tection limit of about 4 ppm at a depth to bone of 4 mm soft tissue. In vivo measurements are ex-pected. Bone lead XRF has mostly been applied to occupationally exposed subjects. Retired lead smelt-ers may have much higher bone lead levels than active smelters [31]. This is ascribed to the long exposure duration and high exposure levels during earlier employment periods, in combination with the slow bone lead excretion (half-time 5 to 15 years). The positive correlation, between blood and bone lead concentrations, for retired smelters confirms the skeleton as an endogenous source of lead. In active workers, the influence from ongoing exposure masks this relation. KXRF techniques sample a relatively large macroscopic volume and does not give detailed in-formation on the microscopic level. Thus, it is of interest to follow the work done, using syn-chrotron radiation, on the lead incorporation in tidemarks, i.e. the calcification zone of the bone [6,32]. Most certainly we will learn more about lead and its incorporation in bone tissue.
5Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

Cadmium Cadmium exposure takes place in various sites of industry and for the general population to-bacco smoking and the increased cadmium content in grain and vegetables, due to agricultural use phosphate fertilisers, may lead to increased cadmium levels in man. Cadmium is virtually absent in new-borns, but the element’s long biological half-life may lead to a considerable accu-mulation in the body burden during life. The kidney is sensitive to chronic poisoning and an es-tablished damage seems irreversible and may progress even though the exposure has ceased. Cadmium in kidneys and liver is readily measured with KXRF, using polarized photons from a modified X-ray apparatus [33] (see Figure 2). Kidney localization is made using ultrasound. To-day measurements can be made, not only in occupationally exposed subjects, but also in the gen-eral population. Even a group of smokers can be distinguished from nonsmokers by their XRF measured kidney cadmium.
Figure 2. Measurement setup for in vivo cadmium and mercury XRF. X-ray tube and polarizing system can be seen as well as the detector at the subject’s back.
Mercury Besides the natural movement of mercury in nature, the element is also released by human ac-tivities such as combustion of fossil fuels, cremation etc. Food and dental amalgam dominate the mercury exposure for the general population. Absorbed mercury is quickly distributed to most regions of the body with the kidneys as the major depot and risk organs. In chloralkali plants, mercury cathodes may be used for the production of caustic soda and chlo-rine gas from brine and in a study kidney mercury was determined [17] using a method analogu-ous to the one described for cadmium above. The presented concentration values, average 24 µg/g (maximum 54 µg/g), were in accordance with literature data on kidney specimen. Iron Thalassaemia is an inherited chronic blood disorder which means that the patient is unable to produce sufficient haemoglobin. Due to necessary regular blood transfusions, iron depots in
6Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

liver, heart and other organs are built up. This may in turn lead to coronary problems. A KXRF system, developed for indirect determination of organ iron stores via measurements of skin iron [19] uses photons of 8.4 keV which is just above the absorption edge of Fe (7.11 keV). A strong correlation between skin and liver iron concentrations was demonstrated in rats. This lays a ground for measurements of iron in humans. Iodine The clinical interest to study iodine deficiency or iodine overload led Hansson et al. [34] to de-velop a non-invasive XRF technique with a 241Am source and a Ge detector in 90° geometry. A combined feasibility and in vivo study was made in a group of subjects 60 to 65 years old, who had been on iodine supplementation through iodinated salt all their life, i.e. sufficient iodine in-take was assumed [35]. The average iodine concentration in the gland was 400 µg/g with a pro-nounced difference between individuals (range 50–2200). This is compatible with euthyroidism (normal function of the gland), hence, determination of the iodine pool by XRF is feasible and the method makes it possible to study the intrathyroidal iodine pool in subjects with thyroid dis-ease. Platinum Platinum is part of a cytostatic agent used for treatment of various cancer forms and it has revo-lutionized the treatment of testicular carcinoma to a nowadays almost 100% curative cancer form. Non-invasive determination of the platinum concentration in tumours is desirable in order to collect more information on platinum retention in tumour and risk organs. Various XRF sys-tems have been proposed, based on either X-ray tubes or radionuclides. Feasibility and in vivo studies have been published. In a patient with a large testicular carcinoma, and receiveing large amounts of cisplatin intrave-nously, the platinum concentration, uniquely measured directly in the tumour, was relatively low (0 to 10 µg/g) [36]. This shows that only up to 3% of the administered amount was present in the tumour during treatment and may indicate that high platinum concentrations are not necessary for cure? In another patient with a liposarcoma tumour of femur, treated with intravenous and in-tratumoural chemotherapy infusions, KXRF measurements were made at the periphery, far from the injection site, directly in the tumour. After an intratumoural infusion, platinum concentra-tions were 20 to 100 µg/g (Figure 3). A slow diffusion over the tumour volume was assumed. Af-ter the intravenous infusion high concentrations were also noted, at one time the ratio between the concentration in the tumour and the other, healthy, leg, was about 35.
7Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

Pt conc (ug/g)
-20
0
20
40
60
80
100
120
140
160
0 20 40 60 80 100 120 140 160
Time after infusion (h)
Tumour Healthy legKidney
Figure 3. Platinum in tumour, healthy tissue and kidney in a patient with a liposarcoma of the femur. Intratumoural infusion at time = 0 hours and intravenous infusion at t = 100 hours. Note that two measurements, markers overlap-
ping, in the tumour were made within the first hour after the infusion at 0 hours. Gold Gold salt is used in the treatment of rheumatoid arthritis (RA). The majority of patients respond favourably whereas the reason for non-response in others is unclear. Adverse effects include skin reactions and kidney proteinuria. In vivo XRF for basic research on gold accumulation in organs has been made by at least two groups. Shakeshaft and Lillicrap [16] used a system based on a 153Gd source and a 32 mm diame-ter Ge detector placed in 90° geometry. The kidney gold levels in patients measured were broadly consistent with those reported for RA patients measured by Börjesson et al. [36], who used the polarized photons technique. There was no strong correlation between measured con-centrations and administered amounts of gold. McNeill and O’Meara [3] also tried to estimate the gold level in bone joints, however, although characteristic gold peaks were seen in spectra, the measurements situation was complicated by gold presumed to reside in the overlying skin of the patients. Uranium Uranium is a potential health hazard and the element accumulates in bone and kidneys. The lit-erature data state bone uranium levels of 0.008 µg/g in occupationally unexposed subjects, whereas occupationally exposed may have levels up to 2 µg/g. A bone uranium KXRF method, using a 57Co source in backscatter geometry, has also been de-veloped [18]. The MDC of 20 µg uranium per g bone mineral in tibia and results from ten in vivo measured volunteers indicated that the current technique is not sensitive enough for measure-
8Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

ments in occupationally exposed subjects, in which bone uranium seems to be at least an order of magnitude less. Zinc Previous studies have observed that prostate cancer cells lose the ability to concentrate zinc [18]. Then, can the zinc concentration in the prostate and the prostate specific antigen (PSA) be used together to improve prostate cancer diagnosis? Moreover, can an improved separation between prostate cancer and benign prostate hyperplasia be established? A feasibility study of a technique with an X-ray tube using mammography energies around 17 keV and zinc XRF lines at 9 keV, was done by Vartsky et al. [37]. The idea is to determine zinc in the prostate via a probe placed in rectum. The probe is reportedly under development. The interference of zinc in the intestine wall is claimed to be corrected for. Arsenic Arsenic is a known toxic element and the health hazard is present at both occupational exposure but also for the general public through contaminated food and water. In parts of Bangladesh, ar-senic is a natural part river water sediments, however, an extensive drilling of freshwater wells have brought up arsenic rich water, despite warnings by local people about “devil’s water.” (UNESCO web information). Estimations talk about unbelievably 35 to 70 millions suffering. This makes it history’s outstanding environmental catastrophy, although not yet as much written about in media. Arsenic’s low-energy X-rays (10 to 12 keV) imply that in vivo XRF is restricted to superficial levels. Studinski et al. [21] recently developed a technique for in vivo arsenic determination us-ing a 125I source and a SiLi detector and reached a detection limit of ≈ 5 µg/g in skin. Since re-ported levels in arsenic workers may go beyond 20 µg/g there is definitely a chance to be able to make measurements on a large scale (Bangladesh?) since this presumably will be a fairly com-pact and mobile system. OVERVIEW OF IN VITRO XRF APPLICATIONS IN MEDICINE Laboratory analysis of metals, minerals, samples of the environment, food, body fluids, tissue specimen, etc. may be performed by in vitro XRF. This section exemplifies medical applications for the measurement of various elements. It is not intended to completely cover all applications, rather to give an overview of some areas of research. Mercury During dental intervention, such as drilling, amalgam particles may become absorbed in the oral mucousa and form an “amalgam tattoo.” Small amounts of mercury are believed to find their way to the blood. A correlation between inflammatory effects and the mercury content in tissue biopsies in the surroundings of the tattoos has been observed [38].
9Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

Hair mercury correlates with blood mercury at the time when the hair is formed. Toribara [39] used a scanning XRF method to investigate the mercury level in 1 mm portions of a single hair strand and could exactly determine when a fatal mercury accident had happened. A rapid in-crease (3 weeks) to maximum concentrations and a more slow decrease was observed. Levels were very high, up to 1000 µg/g. The exposed subject showed signs of intoxication, and despite chelation therapy to force the mercury to leave the body, death occurred less than a year after the accident. Chromium/Lead Small airway epithelial cells may be targets for chromium-induced lung cancer [40]. Phagocyto-sed lead chromate particles and intracellular lead inclusion bodies were observed by electron mi-croscopy and confirmed by XRF (beam size 0.5 × 0.5 µm). Interaction of chromium and lead with DNA may be involved in lead-chromate carcinogenesis. It is well-known that heavy metal compounds, e.g. lead chromate, may leach from crystal glass and ceramic glazes and imply a health risk. XRF techniques may be valuable to distinguish ce-ramic household utensils with high concentrations of toxic elements from those with low levels [41]. Lead and other toxic elements, e.g. arsenic, mercury and selenium, may be present in food stuff such as juice, yogurt and chocolate as well as in certain medicine. Normally these are tested by complicated methods but in situations where the demands on accuracy and sensitivity may be lower, XRF seems to be an alternative according to a joint study by the FDA and a research group [42, 43]. The Franklin expedition was to map out the North-West Passage from Europe to Asia, i.e. a sea route linking the Atlantic and Pacific Oceans. The three ships with 129 men were trapped in thick ice in the winter of 1846–1847 and subsequently the ships were abandoned and the crew tried to find help in small groups. However, finally all men died and few of them were found. In situ measured bone lead in remaining, scattered bones, recovered 1993 from a purported camp-site ranged up to very high levels of 1800 µg/g bone mineral [44]. Correlations between lead at different bone sites were used to identify missing bones, i.e. bones could be associated to the same individual. Improperly soldered tin containers were believed to have been a major source of lead exposure for the expedition members. Thorium An X-ray contrast medium, Thorotrast (25% thorium oxide), was used between the 1920s and 1950s. After i.v. injection, high concentrations of thorium were seen in spleen, liver, bone mar-row and lymph node. Biological and physical half-lives of 400 and 1.4 × 1010 years, respectively, mean that internal organs were irradiated by α-particles for the rest of the subject’s life. In-creased occurrences of liver cancer, liver cirrhosis and leukaemia have been reported. A ∅160 µm beam and a Si(Li) detector for the XRF of thorium Lα lines (13 keV) revealed a conglomerate shape microdistribution of thorium in the liver, whereas more of a belt shape distribution was
10Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

seen in the spleen [45]. XRF gives complementary information to γ-spectrometry and α-autoradi-ography. Element distributions other than thorium may be sampled simultaneously. Platinum Aforementioned, platinum is used for cancer treatment but adverse effects limit the amount which can be administered. In animals, treated with cisplatin for tumours, increased levels of trace elements, e.g. iron, copper and zinc, in addition to platinum, was observed in the kidneys and liver (XRF technique with Mo X-ray tube and a SiLi detector). This suggested that platinum toxicity is due to an overall accumulation of trace elements in these organs and attributable to platinum alone [46]. It has also been shown that trace element levels in blood, liver and kidneys were different between tissue samples obtained from tumour mice and normal mice [47]. Se-lenite reduced trace element levels, hence, it might have a future as chemoprotector. Calcium Inverse relations have been found between health district standardised mortality ratio (SMR) for coronary heart disease (CHD) and the hair calcium concentration as determined with 55Fe XRF [48]. The explained variance was partly due to environmental factors, believed to influence cal-cium metabolism, e.g. water hardness and number of sunshine hours. For example, a south part of England had high hair calcium, hard water and a lot of sunshine hours and the lowest mortal-ity from CHD, while the converse was true for Scotland. Additionally, confounding socio-economic conditions may have been more beneficial to the south-east part than to Scotland. Synchrotron radiation induced XRF may be a suitable method to study the interface between bone and biomaterials, i.e. substitutes for autogenous bone grafts, with regard to mineral content. Circular defects (∅ 4 mm), made in tibias of rabbits, were augmented with a composite of hy-droxyapatite (HA) granules. The calcium distribution, studied with µ-XRF line scans, suggested that calcium phosphate compositions, e.g. HA, have interesting properties as bone substitutes [49]. Nickel In order to detect allergen metals, XRF may also be used in dentistry and dermatology. Suzuki [50] reported successful allergen elimination in patients with metal allergy from dental restora-tion work. Furthermore, detected nickel and gold in skin specimens, taken from lesions in pierced earlobes, suggested that small metal fragments remain in lesions for a long time, causing irritation and cutaneous reactions, even after the studs have been removed [51]. Palladium In a global perspective, the significance of increasing palladium pollution in the environment and in the body of living species is discussed controversially. Previous studies have shown that auto-motive catalyst emitted palladium is bioavailable for aquatic animals [52]. Traditionally, the methods used for accurate measurements of precious metals in automotive catalysts are time consuming and lengthy. Thus, a more straightforward but still accurate method is on the wish
11Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

list. One such method seems to be energy dispersive XRF using a wax pellet for binding the ma-terial under study and an X-ray tube for excitation. Detection limit reported was below 5 ppm [53]. Gold Mechanisms of drowning have been studied using an immersion fluid with gold tracers (12 to 48 µm), introduced into the airways of rats [54]. Microanalyses, using electrons for excitation and studying the gold LXRF (10 to 12 keV), revealed that small diameter tracers had penetrated the intercellular gaps of the alveolar epithelium, while larger tracers were incorporated into the epithelial and endothelial cells. An active post-mortem transport in alveolar pneumonocytes and macrophages functioned for a time period even after death and cessation of circulation. CONCLUSIONS An introduction to some methods used for quantification of various elements in vitro and in vivo is given. Non-destructive in vitro XRF means that elements of medical interest in blood, urine, sweat, skin, hair, teeth, biopsies of tissues and organs, breathing air and drinking water can be measured. Allergens, carcinogens and anti-tumour substances have been studied. Removal of lead in petrol and decontamination of lead based paint, although taking time and with delayed ef-fects, may hopefully decrease the lead concentration, especially in young individuals, over the coming decades. On the other hand, palladium and cadmium may be more prominent due to the use of automotive catalysors and of fertilisers in modern agriculture, respectively. Of more his-torical interest are studies of ancient bones which give insight in lead intake long time ago. Original XRF techniques for in vivo determinations of lead, cadmium and mercury have been ex-tensively applied to studies of occupationally exposed subjects but optimized setups for lead and cadmium are now also ready for measurements in the general population. So far, in vivo studies have supplied us with data on element concentrations and kinetics. XRF can be utilised to deter-mine bone lead in relation to more traditional indices of lead exposure, e.g. lead in blood and urine. For mercury the high MDC is difficult but hopefully the technique may be improved by changes in the setup; a process guided by Monte Carlo simulation. Novel methods to study iron, arsenic, iodine, platinum, gold and uranium have been presented and applied to volunteers or pa-tients. Some of the method’s significance needs further attention. The new generation of synchrotron radiation sources needs to be evaluated, also in connection with in vivo applications, although the practical aspects of measurements need to be considered. The building of medical centers close to the synchrotron facility has been suggested. Improvements in radiation sources, e.g. semi-monoenergetic X-ray tubes and filtered beams, are worth investigating. The use of new electronics and detector configurations has already proven valuable. Calibration procedures need to be rigorous with carefully constructed phantoms. Detection limits must be stated clearly and the effect of overlying tissue need to be controlled for. Figures for ac-
12Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

curacy and precision should be mentioned, preferably for the in vivo situation. Finally, intercom-parison programs should be encouraged. REFERENCES [1] Bradley DA, Farquharson MJ; X-Ray Spectrom, 1999, 28, 270-4. [2] Chettle DR; 1999, 4th topical meeting on Industrial Radiation and Radioisotope Measure-
ment Applications (IRRMA), Raleigh, North Carolina, October 1999. [3] McNeill FE, O’Meara JM; Advances in X-ray Analysis, 1999, 41, 910-21. [4] Börjesson J, Mattsson S; In: “X-Ray Spectrometry: Recent Technological Advances”
(Tsuji K, Van Grieken R, Injuk J, eds), Wiley Publishing, 2004 [5] McNeill FE, Chettle DR, Nie L, Popovic M, Studinski RCN, O’Meara JM; 2006, The 55th
Annual Denver X-ray Conference, Denver, Colorado, August 2006 [6] Wobrauschek P; 2006, The 55th Annual Denver X-ray Conference, Denver, Colorado, Au-
gust 2006. [7] Börjesson J; Thesis, Department of Radiation Physics, Lund University, Malmö 1996. [8] Hoffer PB, Jones WB, Crawford RB, Beck R, Gottschalk A; Radiology, 1968, 90, 342-4. [9] Ahlgren L, Lidén K, Mattsson S, Tejning S; Scand J Work Environ Health, 1976, 2, 82-6. [10] Somervaille LJ, Chettle DR, Scott MC; Phys Med Biol, 1985, 30, 929-43. [11] Wielopolski L, Rosen JF, Slatkin DN, Zhang R, Kalef-Ezra JA, Rothman JC, Maryanski
M, Jenks ST; Med Phys, 1989, 16, 521-8. [12] Gordon CL, Chettle DR, Webber CE; In: "Human body composition. In vivo methods,
models, and assessment" (Ellis K.J., Eastman J., eds.), Plenum Publishing Corporation, 1993, pp. 285-288.
[13] Nie H, Chettle DR, Luo L, O’Meara JM; Phys Med Biol, 2006, 51, 351-60. [14] Christoffersson J-O, Mattsson S; Phys Med Biol, 1983, 28, 1135-44. [15] Jonson R, Mattsson S, Unsgaard B; In: “Recent advances in chemotherapy” (Ishigami J,
ed.). The University of Tokyo Press 1985; pp. 1222-4. [16] Shakeshaft J, Lillicrap S; Br J Rad, 1993, 66, 714-7. [17] Börjesson J, Barregård L, Sällsten G, Schütz A, Jonson R, Alpsten M, Mattsson S; Phys
Med Biol, 1995, 40, 413-26. [18] O’Meara JM, Chettle DR, McNeill FE, Webber CE; Phys Med Biol, 1997, 42, 1109-20. [19] Farquharson MJ, Bradley DA; Phys Med Biol, 1999, 44, 955-65. [20] Shilstein SSh, Breskin A, Chechik R, Feldman G, Vartsky D; Phys Med Biol, 2004, 49,
485-99. [21] Studinski RC, McNeill FE, Chettle DR, O’Meara JM; Phys Med Biol, 2005, 50, 521-30. [22] Kilic A; Ph.D. Thesis, University of Wales (1995) [23] Ao Q, Lee SH, Gardner RP; Appl Radiat Isot, 1997a, 48, 1403-12. [24] Hugtenburg RP, Turner JR, Mannering DM, Robinson BA; Appl Radiat Isot, 1998, 49,
673-6. [25] Gardner RP, Lee SH, Todd AC; Proceedings of the European conference on energy dis-
persive X-ray spectrometry EDXRS-98 (Fernandez JE and Tartari A; eds), Editrice Com-positori, Bologna, 1999: pp. 203-216.
[26] Al-Ghorabie FH; Radiat Environ Biophys, 2000, 39, 141-5. [27] McNeill FE, Stokes L, Brito JA, Chettle DR, Kaye WE; Occup Environ Med, 2000, 57,
465-71.
13Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50

[28] Todd AC, Buchanan R, Carroll S, Moshier EL, Popovac D, Slavkovich V, Graziano JH; Environ Res, 2001, 86, 60-5.
[29] Rosen JF; Toxicol Ind Health, 1997, 13, 211-8. [30] Todd AC; Phys Med Biol, 2002b, 47, 507-22 [31] Schütz A, Olsson M, Jensen A, Gerhardsson L, Börjesson J, Mattsson S, Skerfving S; Int
Arch Occup Environ Health, 2005, 78, 35-43. [32] Zoeger N, Pepponi G, Wobrauschek P, Streli C, Roschger P, Falkenberg G, Tampieri A;
2006, The 55th Annual Denver X-ray Conference, Denver, Colorado, August 2006. [33] Börjesson J, Bellander T, Järup L, Elinder CG, Mattsson S; Occup Environ Med, 1997a,
54, 424-31. [34] Hansson M, Berg G, Larsson A, Nyström E, Isaksson M; Int. J. Body Compos. Res., 2004,
2, 155-163. [35] Milakovic M, Berg G, Eggertsen R, Nystrom E, Olsson A, Larsson A, Hansson M; J Intern
Med, 2006, 260, 69-75. [36] Börjesson J, Alpsten M, Huang S, Jonson R, Mattsson S, Thornberg C; In: "Human body
composition. In vivo methods, models, and assessment" (Ellis K.J., Eastman J.; eds.), Ple-num Publishing Corporation, 1993, pp. 275-80.
[37] Vartsky D, Shilstein S, Bercovich A, Huszar M, Breskin A, Chechik R, Korotinsky S, Mal-nick SD, Moriel E; J Urol, 2003, 170, 2258-62
[38] Forsell M, Larsson B, Ljungqvist A, Carlmark B, Johansson O; Eur J Oral Sci, 1998, 106, 582-7.
[39] Toribara TY; Hum Exp Toxicol, 2001, 20, 185-8. [40] Singh J, Pritchard DE, Carlisle DL, Mclean JA, Montaser A, Orenstein JM, Patierno SR;
Toxicol Appl Pharmacol, 1999, 161, 240-8. [41] Anderson DL, Cunningham WC; J AOAC Int, 1996, 79, 1141-57. [42] Palmer PT, Yamamoto K, Webber S, Ferguson K, Jacobs R; 2006, The 55th Annual Den-
ver X-ray Conference, Denver, Colorado, August 2006. [43] Jacobs R, Palmer PT; 2006, The 55th Annual Denver X-ray Conference, Denver, Colorado,
August 2006. [44] Keenleyside A, Song X, Chettle DR, Webber CE; J Archeolog Sci, 1996, 23, 461-5. [45] Muramatsu Y, Ishikawa Y, Yoshida S, Mori T; Radiat Res, 1999, 152, S97-S101. [46] Shenberg C, Boazi M, Cohen J, Klein A, Kojler M, Nyska A; Biol Trace Elem Res, 1994,
40, 137-49. [47] Feldstein H, Cohen Y, Shenberg C, Klein A, Kojller M, Maenhaut W, Cafmeyer J, Cornelis
R; Biol Trace Elem Res, 1998, 61, 169-80. [48] MacPherson A, Bacsó J; Sci Total Environ, 2000, 255, 11-9. [49] Liljensten EL, Attaelmanan AG, Larsson C, Ljusberg-Wahren H, Danielsen N, Hirsch JM,
Thomsen P; Clin Implant Dent Relat Res, 2000, 2, 50-9. [50] Suzuki N; Int J Prosthodont, 1995, 8, 351-9 [51] Suzuki H; Arch Dermatol Res, 1998, 290, 523-7 [52] Sures B, Zimmermann S, Messerschmidt J, von Bohlen A, Alt F; Environ Pollut, 2001,
113, 341-5. [53] Van Grieken R, Van Meel K, Makarovska Y, Smekens A, Behets M, Kazandjian P; 2006,
The 55th Annual Denver X-ray Conference, Denver, Colorado, August 2006. [54] Bajanowski T, Brinkmann B, Stefanec AM, Barckhaus RH, Fechner G; Int J Legal Med,
1998, 111, 57-61.
14Copyright ©JCPDS-International Centre for Diffraction Data 2007 ISSN 1097-0002Advances in X-ray Analysis, Volume 50