Embed Size (px)
Citation preview

Medi-Cal Managed Care
Advisory Group Meeting
December 3, 2020 – (Webex Only)Webex Meeting number (access code): 145 333 5899
Meeting password: MCAG
Join by video system: Dial [email protected]
You can also dial 173.243.2.68 and enter your meeting number.
Join by phone: +1-415-655-0001 US Toll
Access Code: 145 333 589912/03/2020 1

Welcome and Introductions DHCS COVID-19 Updates
Medi-Cal Enrollment Trends Encounter Data Trends Managed Care Flexibilities
MCP COVID-19 Response Adapting to a Novel Virus COVID-19 Response Strategy
Behavioral Health Integration Children’s Preventive Care
Utilization Report Update Outreach Campaign Phase 2
Updates Managed Care Project Updates Ombudsman Report Sanctions
APLs and DPLs Update Open Discussion Next Meeting – March 11, 202112/03/2020 2
Agenda

12/03/2020 3
Welcome and Introductions

12/03/2020 4
DHCS COVID-19 Updates

Medi-Cal Enrollment Trends
Yingjia Huang
Assistant Division Chief
Medi-Cal Eligibility
12/03/2020 5

12/03/2020 6
Medi-Cal Applications
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
236,381
160,957
154,829162,234
164,529153,566
176,698
173,329
220,943
178,503
165,906
181,032
143,469148,524
157,938
143,968
120,000
140,000
160,000
180,000
200,000
220,000
240,000
Jan Feb Mar Apr May Jun Jul Aug
Applications Received Through County Offices
2019 2020
Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month

• Online
• In Person
• Phone
• Mail/Fax
• Other Includes applications received from sources not
included in the above categories, such as those received by IHSS, and CBO(s) referrals, etc.
Note: This data is reported at the application level, with a single application potentially including more than one person (for example, a parent and two children are likely to apply for health coverage on a single application).
12/03/2020 7
County Application Pathways

12/03/2020 8
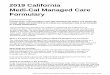
County Application Pathway
- All Pathways –
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
-
50,000
100,000
150,000
200,000
250,000Applications Pathways
Online Total Mail Total In-person Total Phone Total Other Total
Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month
12/03/2020 9
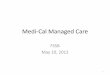
County Application Pathway
- Online Applications -
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
59,8
86
39,2
14
58,2
49
60,7
08
57,2
10
54,1
41
64,7
14
63,2
66
55,3
86
73,0
75
99,6
46
104
,45
1
102
,83
3
80,2
02
86,0
94
130
,50
6
96,1
69
93,3
96
96,6
08
86,2
68
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000Online Applications Total
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month

12/03/2020 10
County Application Pathway
- In Person Applications -
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
66,1
42
52,4
50
59,5
88
61,0
26
59,3
13
54,2
74
62,9
83
61,5
73
55,5
88
58,3
46
49,4
73
53,9
17
68,6
24
54,6
39
37,4
06
9,1
17
7,9
59
9,6
95
10,4
75
13,1
58
-
10,000
20,000
30,000
40,000
50,000
60,000
70,000In Person Applications Total
Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month.

12/03/2020 11
County Application Pathway
- Phone Applications -
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
4,5
96
3,9
77
4,2
78
4,1
01
4,1
96
3,8
73
4,1
97
4,2
48
3,7
63
4,1
71
3,5
00
3,9
78
4,7
58
3,7
76
6,1
62
9,8
25
8,5
23
9,4
83
9,6
64
9,0
04
-
2,000
4,000
6,000
8,000
10,000
12,000Phone Applications Total
Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month

12/03/2020 12
County Application Pathway
- Mail/Fax Applications -
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
23,1
17
14,1
21
15,2
54
17,7
64
16,0
84
15,4
13
16,3
92
16,0
22
14,3
13
15,3
83
12,7
06
14,0
72
16,6
17
15,6
65
15,6
52
14,8
85
12,9
17
14,1
22
15,3
08
14,4
53
-
5,000
10,000
15,000
20,000
25,000Mail/Fax Applications Total
Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month

12/03/2020 13
County Application Pathway
- Other Applications –
Data Source: Statewide Automated Welfare Systems (SAWS) Provided One Month after the Reported Month
82,6
40
51,1
95
17,4
60
18,6
35
27,7
26
25,8
65
28,4
12
28,2
20
26,8
17
27,3
16
23,4
43
23,9
26
28,1
11
24,2
21
20,5
92
16,6
99
17,9
01
21,8
28
25,8
83
21,0
85
-
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000Other Applications Total
Data Source. Statewide Automated Welfare Systems. SAWS. Provided One Month after the Reported Month
12/03/2020 14
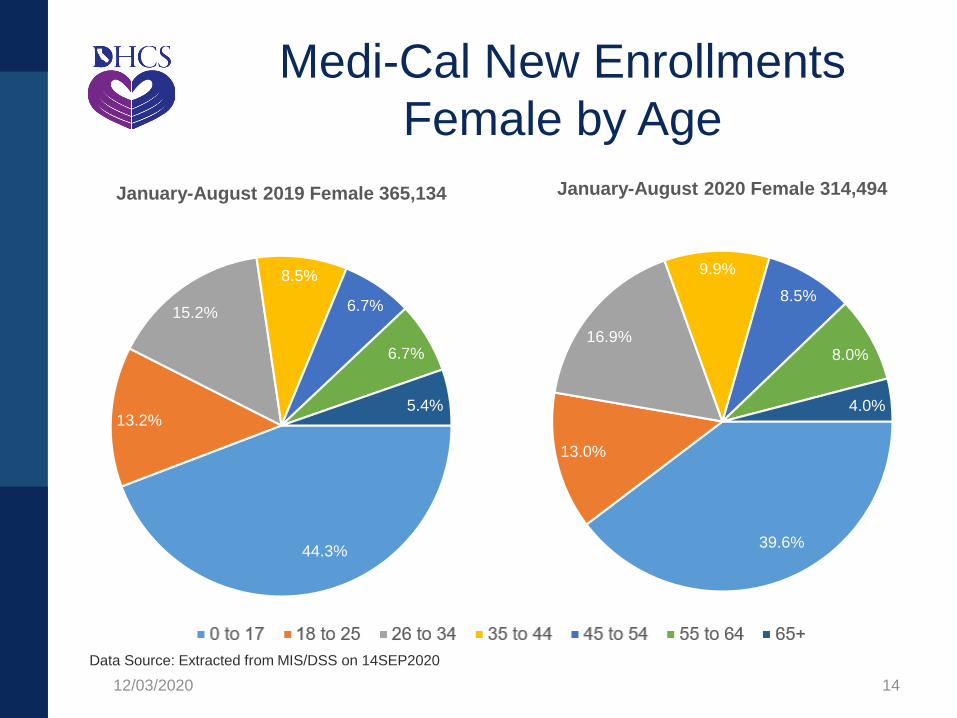
Medi-Cal New Enrollments
Female by Age
Data Source: Extracted from MIS/DSS on 14SEP2020
44.3%
13.2%
15.2%
8.5%
6.7%
6.7%
5.4%
January-August 2019 Female 365,134
39.6%
13.0%
16.9%
9.9%
8.5%
8.0%
4.0%
January-August 2020 Female 314,494
Data Source. Extracted from MIS/DSS on 14SEP2020.
12/03/2020 15
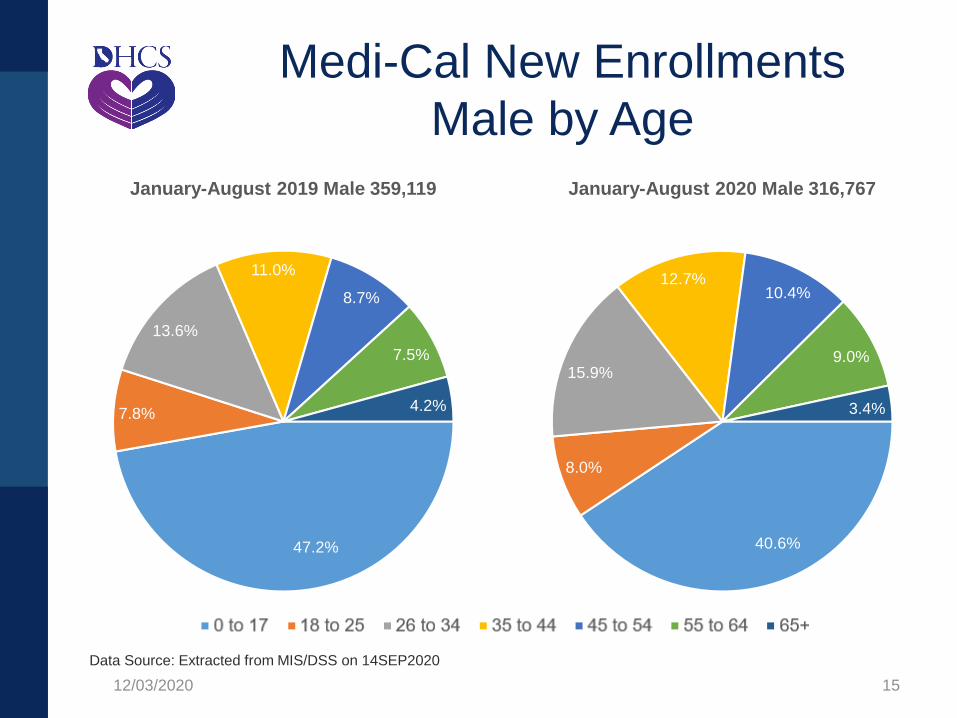
Medi-Cal New Enrollments
Male by Age
Data Source: Extracted from MIS/DSS on 14SEP2020
47.2%
7.8%
13.6%
11.0%
8.7%
7.5%
4.2%
January-August 2019 Male 359,119
40.6%
8.0%
15.9%
12.7%10.4%
9.0%
3.4%
January-August 2020 Male 316,767
Data Source. Extracted from MIS/DSS on 14SEP2020.
12/03/2020 16
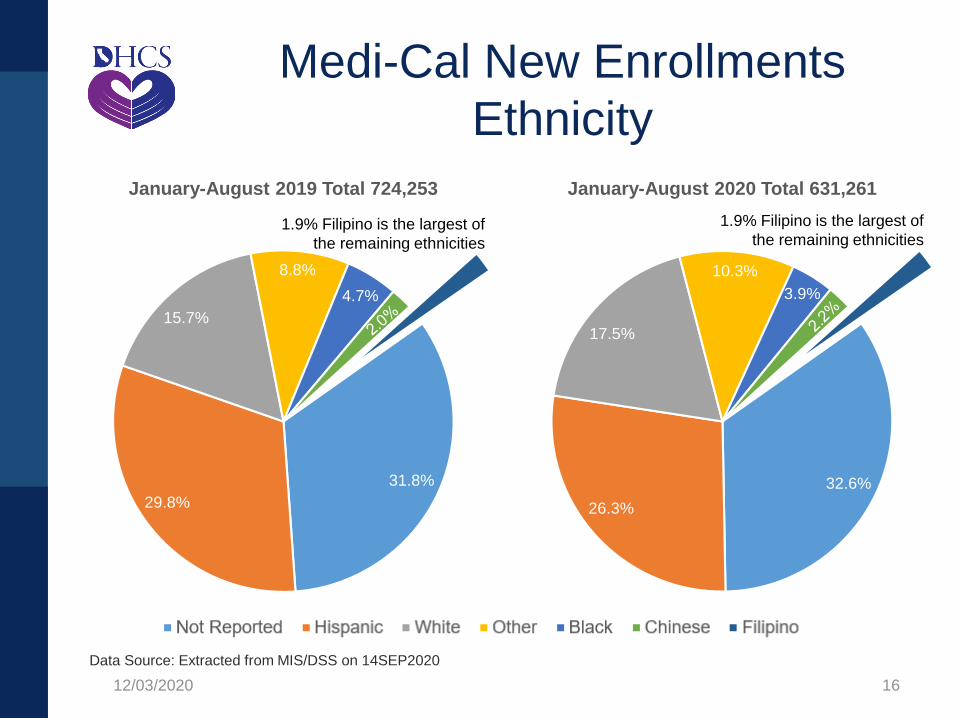
Medi-Cal New Enrollments
Ethnicity
Data Source: Extracted from MIS/DSS on 14SEP2020
31.8%
29.8%
15.7%
8.8%
4.7%
January-August 2019 Total 724,253
1.9% Filipino is the largest of
the remaining ethnicities
32.6%
26.3%
17.5%
10.3%
3.9%
January-August 2020 Total 631,261
1.9% Filipino is the largest of
the remaining ethnicities
Data Source. Extracted from MIS/DSS on 14SEP2020.
12/03/2020 17
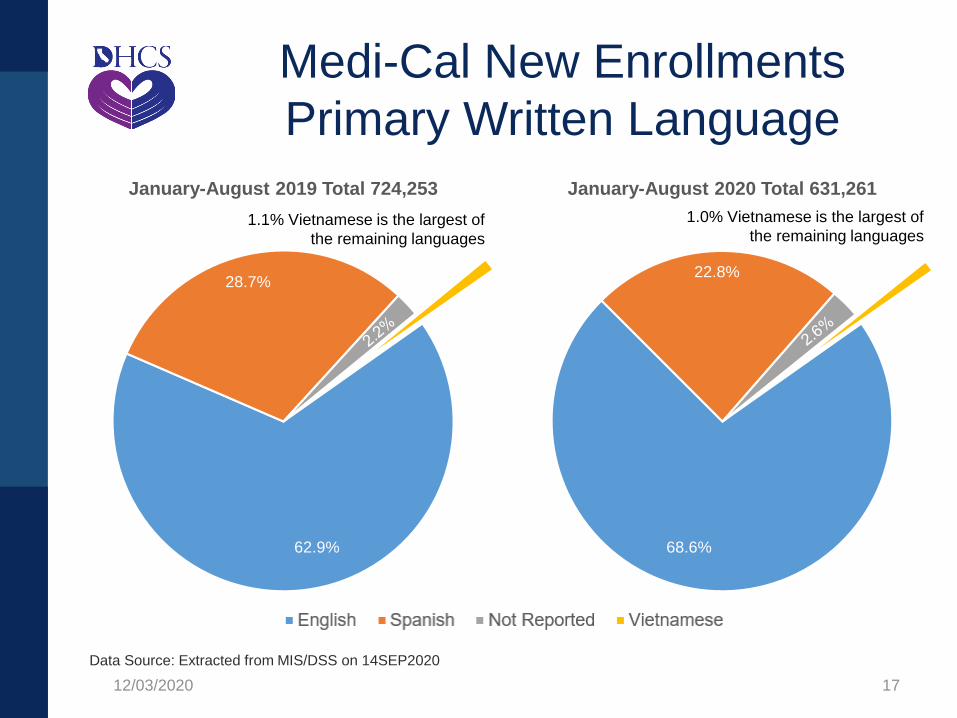
Medi-Cal New Enrollments
Primary Written Language
Data Source: Extracted from MIS/DSS on 14SEP2020
62.9%
28.7%
January-August 2019 Total 724,253
1.1% Vietnamese is the largest of
the remaining languages
68.6%
22.8%
January-August 2020 Total 631,261
1.0% Vietnamese is the largest of
the remaining languages
Data Source. Extracted from MIS/DSS on 14SEP2020.

12/03/2020 18
Medi-Cal New Enrollment Data
Medi-Cal New Enrollment Data includes the following cohorts:
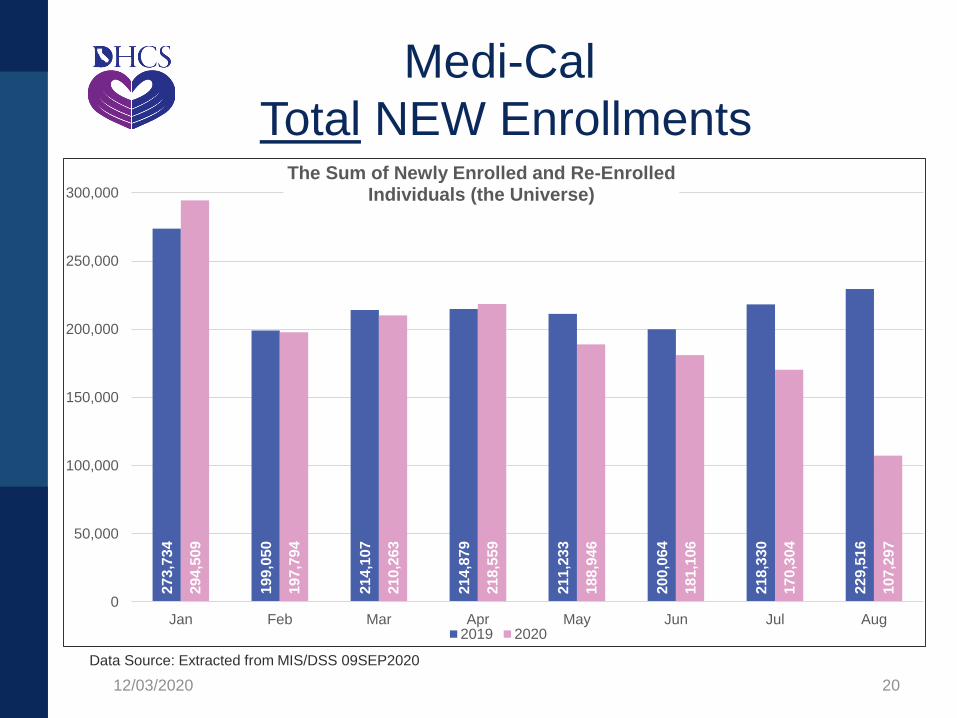
Total NEW Enrollments - The sum of Newly Enrolled and Re-Enrolledindividuals (the Universe).
Newly Enrolled - Individuals with no prior history of Medi-Cal coverage.
Re-Enrolled - Individuals who experienced a break in coverage and came back to the Medi-Cal program by reapplying, and being determined eligible for Re-Enrollment into the program.
• Different from Newly Enrolled, these are individuals with a prior history of Medi-Cal coverage within the previous 15+ year period, but whose Medi-Cal was subsequently discontinued at some point in the past, thereby requiring the individual to reapply.
Re-Enrollment Churn (A subset of Re-Enrolled) - Individuals who experienced a break in coverage and came back to the Medi-Cal program by reapplying, and being determined eligible for Re-Enrollment into the program.
• This subset of Re-Enrolled individuals have a prior history of Medi-Cal coverage within the previous 12 month period, but whose Medi-Cal was subsequently discontinued at some point in that 12 month period, thereby requiring the individual to reapply.

12/03/2020 19
Medi-Cal
New Enrollment Cohorts
Data Source: Extracted from MIS/DSS 09SEP2020
163,1
86
118
,32
9
126
,34
5
127
,79
7
125
,07
1
117
,38
9
126
,72
2
131
,82
1
182
,89
6
121,6
17
128
,78
6
138
,50
2
117
,77
5
107
,44
6
92,8
61
47,5
94
110,5
48
80,7
21
87,7
62
87,0
82
86,1
62
82,6
75
91,6
08
97,6
95
111
,61
3
76,1
77
81,4
77
80,0
57
71,1
71
73,6
60
77,4
43
59,7
03
19,5
05
14,4
60
15,4
51
15,1
68
15,2
39
13,7
17
14,6
32
15,7
21
20,8
51
14,5
40
14,4
82
13,9
96
13,2
39
12,1
74
10,8
50
6,5
73
0
50000
100000
150000
200000
250000
300000
0
50,000
100,000
150,000
200,000
250,000
300,000Comparisons of Newly Enrolled, Re-Enrolled, and Re-Enrollment Churn subset
Re-Enrolled Newly Enrolled Re-Enrollment (Churn)
Data Source. Extracted from MIS/DSS 09SEP2020.
12/03/2020 20
Medi-Cal
Total NEW Enrollments
Data Source: Extracted from MIS/DSS 09SEP2020
273
,73
4
199
,05
0
214
,10
7
214
,87
9
211
,23
3
200
,06
4
218
,33
0
229,5
16
294
,50
9
197
,79
4
210
,26
3
218
,55
9
188
,94
6
181
,10
6
170
,30
4
107
,29
7
0
50,000
100,000
150,000
200,000
250,000
300,000
Jan Feb Mar Apr May Jun Jul Aug
The Sum of Newly Enrolled and Re-Enrolled Individuals (the Universe)
2019 2020
Data Source. Extracted from MIS/DSS 09SEP2020.

12/03/2020 21
Medi-Cal
Newly Enrolled
Data Source: Extracted from MIS/DSS on 14SEP2020
110
,54
8
80,7
21
87,7
62
87,0
82
86,1
62
82,6
75
91,6
08
97,6
95
111
,61
3
76,1
77
81,4
77
80,0
57
71,1
71
73,6
60
77,4
43
59,7
03
0
20,000
40,000
60,000
80,000
100,000
120,000
Jan Feb Mar Apr May Jun Jul Aug
Newly Enrolled Individuals With No Prior History of Medi-Cal Coverage
2019 2020
Data Source. Extracted from MIS/DSS on 14SEP2020.

12/03/2020 22
Medi-Cal
Re-Enrolled
Data Source: Extracted from MIS/DSS on 09SEP2020
163
,18
6
118
,32
9
126
,34
5
127
,79
7
125,0
71
117
,38
9
126
,72
2
131
,82
1
182
,89
6
121
,61
7
128
,78
6
138
,50
2
117
,77
5
107
,44
6
92,8
61
47,5
94
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
Jan Feb Mar Apr May Jun Jul Aug
Individuals with a Prior History of Medi-Cal Coverage who Reapplied and Re-enrolled Into the Program.
2019 2020
Data Source. Extracted from MIS/DSS on 09SEP2020.

12/03/2020 23
Medi-Cal
Re-Enrollment Churn
Data Source: Extracted from MIS/DSS on 09SEP2020
19,5
05
14,4
60
15,4
51
15,1
68
15,2
39
13,7
17
14,6
32
15,7
21
20,8
51
14,5
40
14,4
82
13,9
96
13,2
39
12,1
74
10,8
50
6,5
73
0
3,500
7,000
10,500
14,000
17,500
21,000
Jan Feb Mar Apr May Jun Jul Aug
A Subset of the Re-Enrolled Data: Individuals Reapplying and Eligible for Re-Enrollment after experiencing a “Break in Aid”
within the previous 12-Month period.
2019 2020
Data Source. Extracted from MIS/DSS on 09SEP2020.
12/03/2020 24
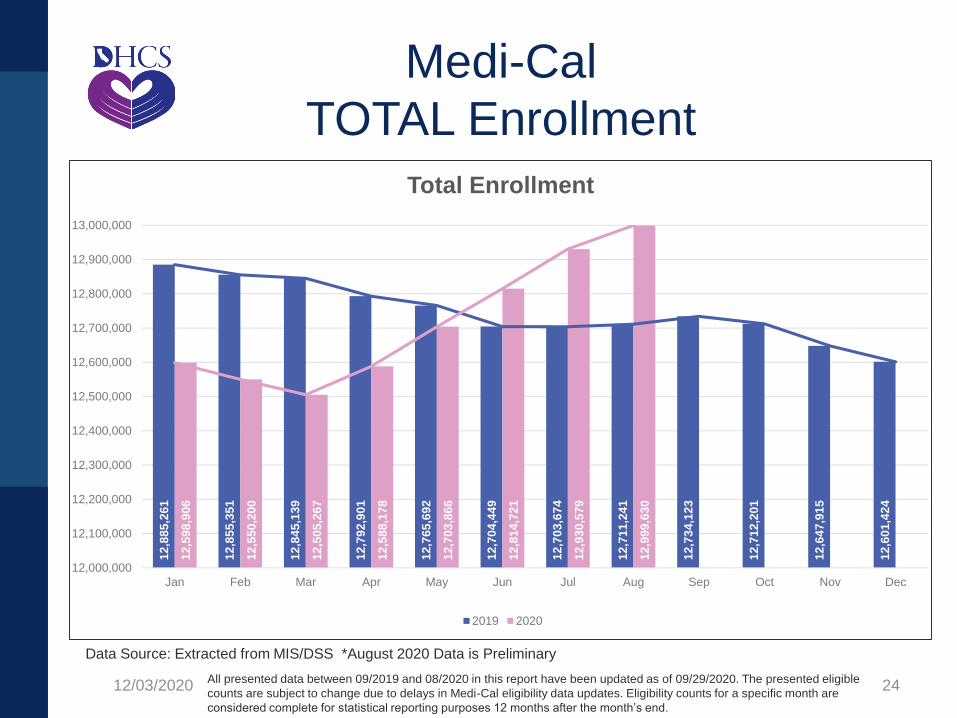
Medi-Cal
TOTAL Enrollment
Data Source: Extracted from MIS/DSS *August 2020 Data is Preliminary
All presented data between 09/2019 and 08/2020 in this report have been updated as of 09/29/2020. The presented eligible
counts are subject to change due to delays in Medi-Cal eligibility data updates. Eligibility counts for a specific month are
considered complete for statistical reporting purposes 12 months after the month’s end.
12
,88
5,2
61
12
,85
5,3
51
12
,84
5,1
39
12
,79
2,9
01
12
,76
5,6
92
12
,70
4,4
49
12
,70
3,6
74
12
,71
1,2
41
12
,73
4,1
23
12
,71
2,2
01
12
,64
7,9
15
12
,60
1,4
24
12
,59
8,9
06
12
,55
0,2
00
12
,50
5,2
67
12
,58
8,1
78
12
,70
3,8
66
12
,81
4,7
21
12
,93
0,5
79
12
,99
9,6
30
12,000,000
12,100,000
12,200,000
12,300,000
12,400,000
12,500,000
12,600,000
12,700,000
12,800,000
12,900,000
13,000,000
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total Enrollment
2019 2020
Data Source. Extracted from MIS/DSS *August 2020 Data is Preliminary.
12/03/2020 25
Continuous Medi-Cal Coverage Through
the Public Health Emergency
• To ensure Californians continued to receive Medi-Cal
health coverage during the public health emergency
(PHE), per Executive Orders N-29-20 and N-71-20,
DHCS issued guidance directing counties to delay the
processing of Medi-Cal annual renewals, and to defer
discontinuances and negative actions, effective March
16, 2020, through the duration of the PHE.
• Exceptions to the moratorium on discontinuances/
negative actions are:
• voluntary requests for discontinuance,
• death of a beneficiary, or
• individuals who move out of state.

• COVID-19 Uninsured Coverage Group (aka COVID-19
PE):
For uninsured individuals
Services limited to medically necessary COVID-19
testing, testing-related, and treatment services
12-month enrollment period or end of public health
emergency, whichever comes later
• COVID-19 Uninsured Application Pathways:
All PE Qualified Providers, including:
Hospital PE
Child Health and Disability Prevention Gateway
PE for Pregnant Women
12/03/2020 26
COVID-19 Uninsured Group
Questions?
12/03/2020 27
Encounter Data Trends
Andrew Wong
Program Data Section, Chief
Data Analytics Branch
12/03/2020 28

12/03/2020 29
Outpatient and Prescription Utilization Trends
1,110
991
1,0581,087
1,061
1,159
1,009 1,007
1,129
1,056
931
756
714
653690 689 676
728
665709
759711
761
643
0
200
400
600
800
1,000
1,200
1,400
May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20
Vis
its
or
Pre
sc
rip
tio
ns
per
1,0
00
Me
mb
ers
Month of Service
Outpatient Visits Prescriptions
Data Source: MIS/DSS | Data Represents: May 2019 – April 2020 | Date Downloaded: 11/10/2020

12/03/2020 30
ER, Inpatient, and Mild to Moderate Mental
Health Utilization Trends
5351 52 52 53 52 51
54
60
55
43
26
16 15 16 16 16 1615 15 16
15 1412
2220
22
25 2427
23 22
2725 24
26
0
10
20
30
40
50
60
70
May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20
Vis
its
per
1,0
00
Me
mb
ers
Month of Service
Emergency Room Visits Inpatient Admissions Mild to Moderate Mental Health Visits
Data Source: MIS/DSS | Data Represents: May 2019 – April 2020 | Date Downloaded: 11/10/2020

12/03/2020 31
Grievances Trends
0.52 0.61 0.84 0.65 0.710.47
4.70 4.75
5.61 5.555.36
3.91
6.65
7.878.09 8.14
7.84
7.18
1.27
1.77
1.251.53 1.66
1.37
2.082.33
2.84
2.362.58
1.91
0
1
2
3
4
5
6
7
8
9
Q1 2019 Q2 2019 Q3 2019 Q4 2019 Q1 2020 Q2 2020
Gri
eva
nc
es
per
10,0
00
Me
mb
ers
Quarter
Referral Grievances Quality of Care Grievances Other Grievances
Benefits Grievances Accessibility Grievances
Data Source: Enterprise Performance Monitoring | Data Represents: January 2019– March 2020 | Date Downloaded: 11/24/2020
Questions?
12/03/2020 32

Managed Care Flexibilities
Mike Dutra
Branch Chief
Policy, Utilization & External Relations
12/03/2020 33

• State Fair Hearing: Extend timeframes to request SFH
• Provider enrollment/screening: Emergency Medi-Cal
provider enrollment application/process
• Prior Authorization: Waive PA for COVID-19 testing
and services (MCPs encouraged to implement
expedited PA processes for other services)
• Provision of Care in Alternative Settings, Hospital
Capacity, and Blanket Section 1135 Waiver
Flexibilities for Medicare and Medicaid Enrolled
Providers Relative to COVID-19: Various flexibilities to
requirements in types of services and locations
12/03/2020 34
Managed Care Flexibilities
• Pharmacy: Off-label and/or investigational drugs used to treat COVID-19 and/or related conditions and Subcutaneous Depot Medroxyprogesterone Acetate during PHE
• Telehealth: Expand use of telehealth services
• Well-Child Visits: Expand telehealth provided services
• Encounter Data: Pause the State Fiscal Year 2019-2020 Encounter Data Validation (EDV) study
• Health Homes: Allow telehealth and suspension of face to face assessment
12/03/2020 35
Managed Care Flexibilities
• Initial Health Assessment: Suspension of IHA requirements
• Quality Monitoring, Programs & Initiatives:
MCP do not need to respond to certain items on the Quarterly Monitoring Response Template (QMRT)
Extend the compliance deadline for the Managed Care Program Data Improvement Project (MCPDIP)
• File and Use: COVID-19 documents and scripts used for member communication
• Temporary Reinstatement of Acetaminophen and Cough/Cold Medicines
12/03/2020 36
Managed Care Flexibilities

• Addition of Provider Types at FQHCs and RHCs: Temporarily add
Associate Clinical Social Workers (ACSWs) and Associate Marriage
and Family Therapists (AMFTs)
• MCP Site Reviews and Subcontractor Monitoring: Temporarily
suspend the contractual requirement for in-person site reviews,
medical audits, and similar monitoring activities that would require
in-person reviews. Requirements suspended through the duration of
PHE and an additional six months following the end of the PHE
• Annual Medical Audits: Suspend the A&I annual medical audit;
however, this does not negate MCPs’ responsibility to comply with
all currently imposed CAP requirements
• Health Risk Assessments: Extend the timeframes specified in W&I
Code section 14182(c)(12)(A) and APL 17-013 for completing HRA
surveys for newly enrolled SPDs (Within 135 days for higher risk
and 195 days for lower risk)
12/03/2020 37
Managed Care Flexibilities
Questions?
12/03/2020 38

12/03/2020 39
MCP COVID-19 Response

COVID-19 Medical Condition
Risk Stratification
Gordon Arakawa MD PhD
Medical Director
Central California Alliance for Health
12/03/2020 40

• Central California Alliance for Health
COHS MCP serving Santa Cruz, Monterey,
Merced Counties
~ 370,000 members
Demographics:
• ~ 38% of population in the three counties
• Hispanic 70%, White 16%, Asian 9%, Black 2%
12/03/2020 41
Background

• My Background
Trained as a Diagnostic Radiologist
specializing in PET/CT
Health Officer in San Joaquin, Merced
Counties
Graduate degree in Data Analytics
12/03/2020 42
Background
Adapting to a Novel Virus:
Using Claims Data to Measure Risk and
Design COVID-19 Member Outreach
12/03/2020 43
Project

• Create Outreach Program during (initial)
stages of COVID-19 pandemic
Define Population for Targeted Outreach
Construct/Perform Messaging
12/03/2020 44
Goal
• Create Outreach Program during (initial)
stages of COVID-19 pandemic
Define Population for Targeted Outreach
Construct/Perform Messaging
12/03/2020 45
Goal
• Initial Metric
Business Intelligence (BI) Tool
• Member Score
“Chance” of high cost/expenditure in the future based
upon historical payed claims data
• Member Index
Stratification result based, in part, upon the Score
described above
12/03/2020 46
Defining the Population

• Initial Metric
BI Tool Issues
• Member Score
Rather agnostic with respect to COVID-19 infection
risk
• Member Index
Influenced by member score
Each category included too many members
12/03/2020 47
Defining the Population

• Foundations of a New Metric
CDC released in March/April 2020 guidance
regarding underlying medical conditions that
predispose a person to severe illness from
COVID-19
12/03/2020 48
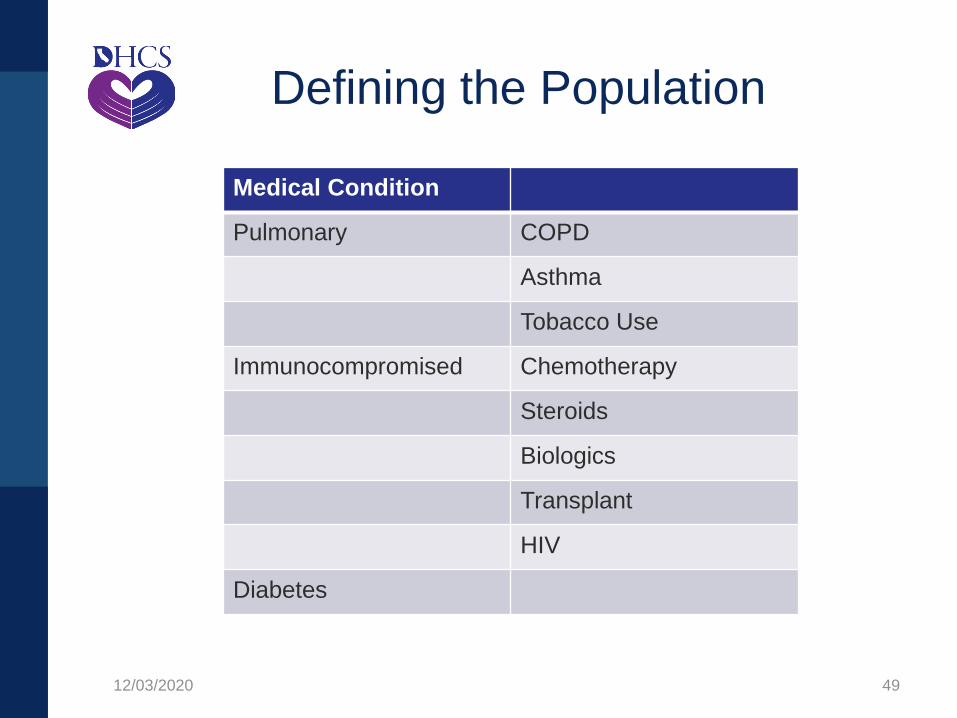
Defining the Population
12/03/2020 49
Medical Condition
Pulmonary COPD
Asthma
Tobacco Use
Immunocompromised Chemotherapy
Steroids
Biologics
Transplant
HIV
Diabetes
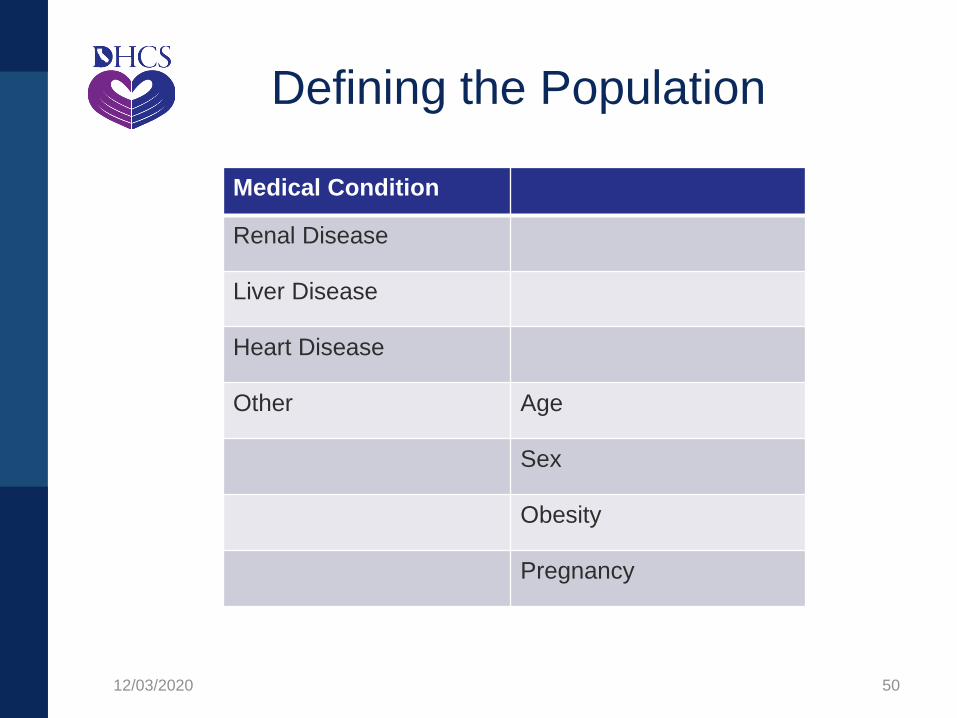
Defining the Population
12/03/2020 50
Medical Condition
Renal Disease
Liver Disease
Heart Disease
Other Age
Sex
Obesity
Pregnancy
Defining the Population

• Develop a different metric
1. Assess the chronic conditions of Alliance
members relative to COVID-19 risk
2. Create ranking of medical conditions
3. Capture combinatorics
12/03/2020 51
Defining the Population
• Assess chronic conditions of Alliance
members
BI Tool revisited
• Build medical condition profile for each member
based upon claims data
12/03/2020 52
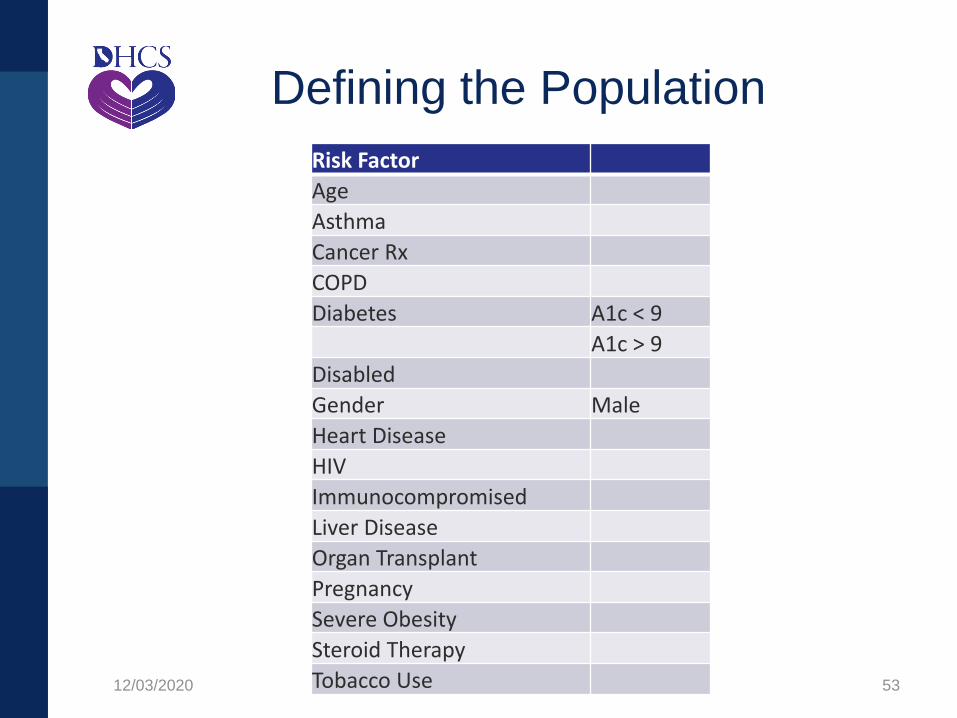
Defining the Population
12/03/2020 53
Risk Factor
Age
Asthma
Cancer Rx
COPD
Diabetes A1c < 9
A1c > 9
Disabled
Gender Male
Heart Disease
HIV
Immunocompromised
Liver Disease
Organ Transplant
Pregnancy
Severe Obesity
Steroid Therapy
Tobacco Use
Defining the Population

• Create ranking of medical conditions
Some conditions are more severe than
others, e.g.
• Chemo vs Biologics
• COPD vs Asthma
12/03/2020 54
Defining the Population

• Create ranking of medical conditions
Approach based upon previous work as
Health Officer
Risk factors for developing active TB
Medical conditions: COPD, smoking,
Diabetes, etc.
12/03/2020 55
Defining the Population

• Create ranking of medical conditions
Scoring for conditions (range 1-5)
Chemo=2, Biologics=1.5
COPD=3, Asthma=2
Age: exponentially increasing function after
age 60
12/03/2020 56
Defining the Population

• Capture combinatorics
Combination of medical conditions should to
reflect increased risk compared to singular
conditions
12/03/2020 57
Defining the Population
• Capture combinatorics
Formal calculation of cumulative risk from
multiple conditions not (yet) possible
Use simple counting procedure
• Addition versus multiplication
12/03/2020 58
Defining the Population
• Capture combinatorics
Formal calculation of cumulative risk from
multiple conditions not (yet) possible
Use simple counting procedure
• Addition versus multiplication
12/03/2020 59
Defining the Population
• Build rank list of (entire) membership
Identified the 5,000/10,000 members most at
risk for targeted outreach
12/03/2020 60
Defining the Population

• What’s next?
Compare BI Tool Metric and New Metrics
• Results did NOT match
Compare calculated risk to true outcomes
Re-examine Metric
12/03/2020 61
Defining the Population
Questions?
12/03/2020 62

COVID-19 Response Strategy
Shelly LaMaster, MSW
Director of Integrated Care
Inland Empire Health Plan
12/03/2020 63

Target Population
• IEHP’s 1.3 million Members, our Providers, health care
workers, and community partners
• 2,200+ Team Members and their families
• Our most vulnerable populations and those directly
impacted by COVID-19, including:
All Members admitted to inpatient acute care
All Members transitioned to a lower level of care (post-
acute and custodial)
All Members in hospice, palliative, transplant and
ESRD programs
All Members in the community settings impacted by
COVID-19
12/03/2020 64

Removal of Barriers to Care
• Created innovative, best-in-class funding mechanisms to make sure our Providers have resources to care for patients
• Created first-of-their-kind emergency amendments with our county hospitals to make sure they have cash flow
• Purchased PPE for local hospitals, Providers and counties
• Teamed up with FQHCs to provide a $100,000 grant to support COVID-19 testing
• Supported county homeless initiatives, community food bank and delivery systems, and a first-of-its-kind county-211-Nurse Advice Line strategy to support 400,000 uninsured residents
12/03/2020 65

Member Outreach
Campaigns
• In response to DMHC APL 20-012, we organized and
implemented a Member live Outbound Call Campaign, which
launched on April 8th.
• We utilized GIS mapping to identify geographic regions of other
high-risk Members in COVID hotspots for outbound call
campaigns.
• To date, our Teams made live outbound calls to more than 43,000
of our most vulnerable Members, successfully making contact
with 45% of these Members.
• During the month of May, a total 92,393 Members received
robocalls.
• Our new social isolation texting program helped us reach out to
the more than 94,000 Members who are seniors and have
disabilities.
12/03/2020 66
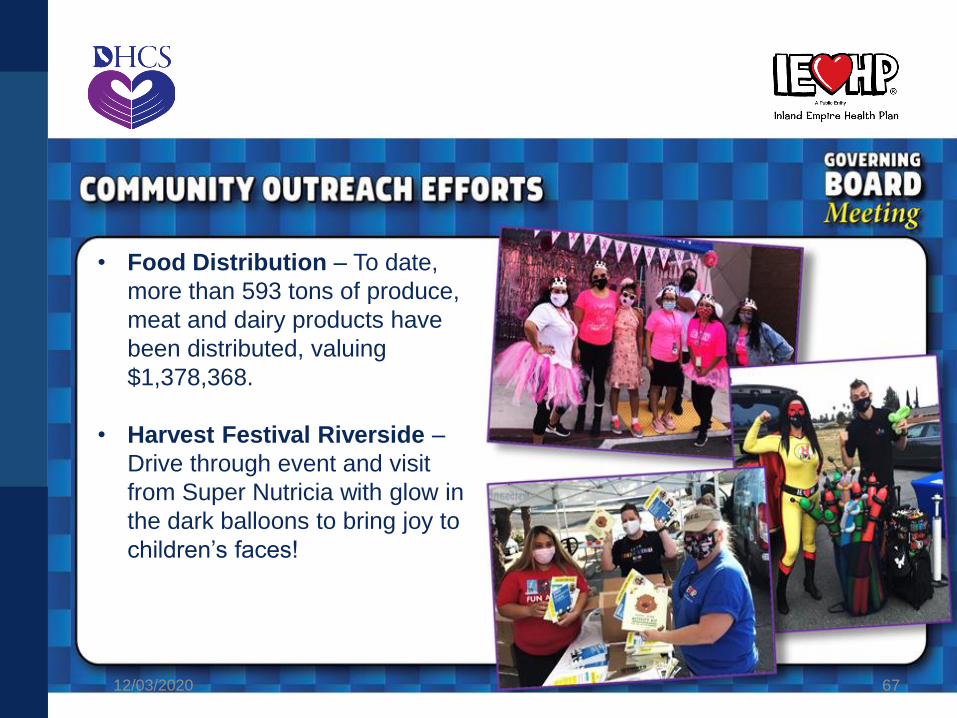
• Food Distribution – To date,
more than 593 tons of produce,
meat and dairy products have
been distributed, valuing
$1,378,368.
• Harvest Festival Riverside –
Drive through event and visit
from Super Nutricia with glow in
the dark balloons to bring joy to
children’s faces!
12/03/2020 67
COMMUNITY OUTREACH EFFORTS
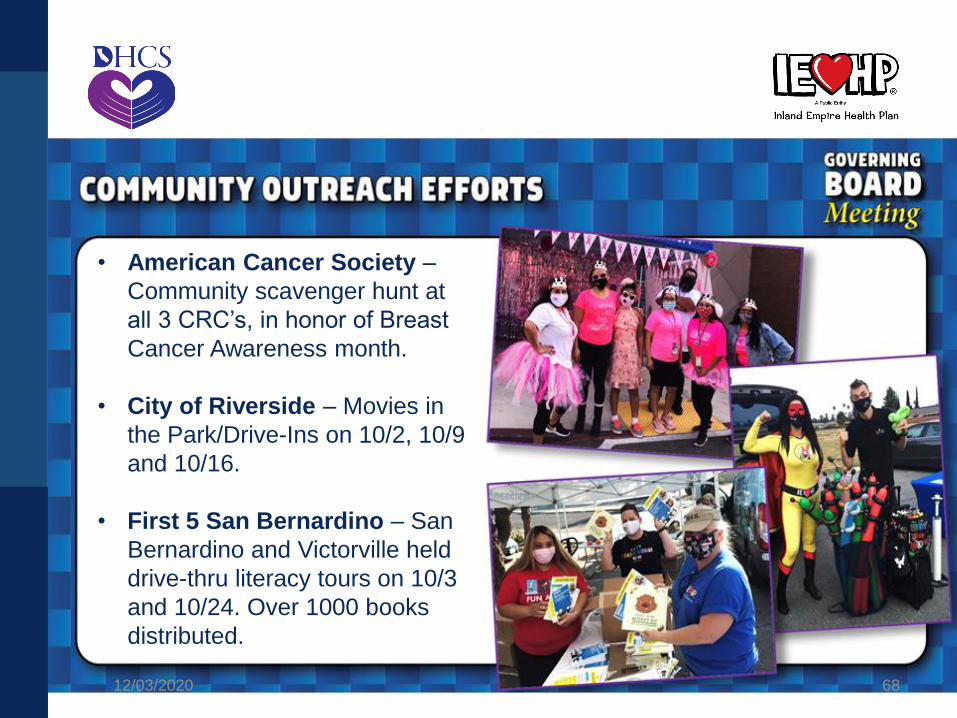
• American Cancer Society –
Community scavenger hunt at
all 3 CRC’s, in honor of Breast
Cancer Awareness month.
• City of Riverside – Movies in
the Park/Drive-Ins on 10/2, 10/9
and 10/16.
• First 5 San Bernardino – San
Bernardino and Victorville held
drive-thru literacy tours on 10/3
and 10/24. Over 1000 books
distributed.
12/03/2020 68
COMMUNITY OUTREACH EFFORTS

Isolation in Skilled
Nursing Facilities (SNFs)
• In collaboration with our partners at Molina, have reached out to
SNFs in Riverside and San Bernardino Counties to assess
Member needs for social support
• Distribution of activity books
• Card campaign – continue to distribute greeting cards
handmade by IEHP Team Members and their family members
• Have partnered with La Sierra University for a “Warm Line”
service staffed by student volunteers
• Arranged for live entertainment via Facebook
• Conducted multiple “IEHP Parades” where Team Members and
their family Members drive to SNFs and greet the Members
while remaining in their vehicles
12/03/2020 69

12/03/2020 70
Questions?

Behavioral Health Integration
Dana Durham
Branch Chief
Quality & Medical Policy
12/03/2020 71
• The Behavioral Health Integration (BHI) Incentive Program is designed to incentivize improvement of physical and behavioral health outcomes, care delivery efficiency, and patient experience while aiming to continue integration activities after the end of the program.
• The goal of the BHI Incentive Program is to:
o Increase MCP network integration for providers at all levels of integration (those just starting behavioral health integration in their practices as well as those that want to take their integration to the next level),
o focus on new target populations or health disparities, and
o improve the level of integration or impact of behavioral and physical health.
72
Objective
12/03/2020

• Proposition 56 allocated $190 million to the BHI
Incentive Program.
• Due to COVID-19, the original April 1, 2020 start
date was deferred to January 1, 2021.
• Determination letters were sent to MCPs in early
November 2020.
• The program period consists of:
o Program Year 1 (01/01/21 – 12/31/21), and
o Program Year 2 (01/01/22 – 12/31/22).
73
Overview
12/03/2020

• 3.1 Basic Behavioral Health Integration
• 3.2 Maternal Access to Mental Health and
Substance Use Disorder Screening and Treatment
• 3.3 Medication Management for Beneficiaries with
Co-occurring Chronic Medical and Behavioral
Diagnoses
• 3.4 Diabetes Screening and Treatment for People
with Serious Mental Illness
• 3.5 Improving Follow-Up after Hospitalization for
Mental Illness
• 3.6 Improving Follow-Up after Emergency
Department Visit for Behavioral Health Diagnosis
74
Project Options
12/03/2020

Examples of criteria used to evaluate applications:
• Information provided in the BHI Incentive Program
applications,
• Other plan-submitted supporting documentation,
• MCP scoring,
• Number of project options submitted,
• The number of beneficiaries that will be impacted,
and/or
• The cost to implement the project option across the
state.
12/03/2020 75
Application Vetting Criteria
• MCPs determined final awards to providers.
• Aiming to approve as many projects as possible,
DHCS reviewed and recommended approval of 369
Projects from 131 providers.
• 22 MCPs submitted over 500 Project Options from
160 providers.
12/03/2020 76
Application Awardees

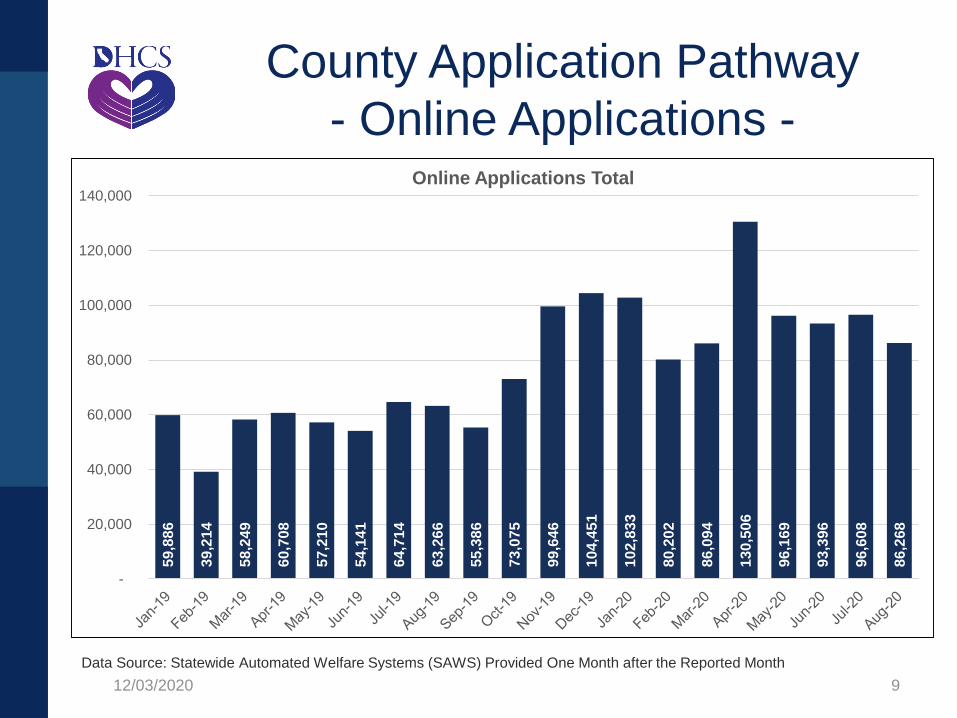
62
56
25
56
62
108
0 20 40 60 80 100 120
3.6
3.5
3.4
3.3
3.2
3.1
Number of Project Options
Number of Project Options
77
Awards
12/03/2020
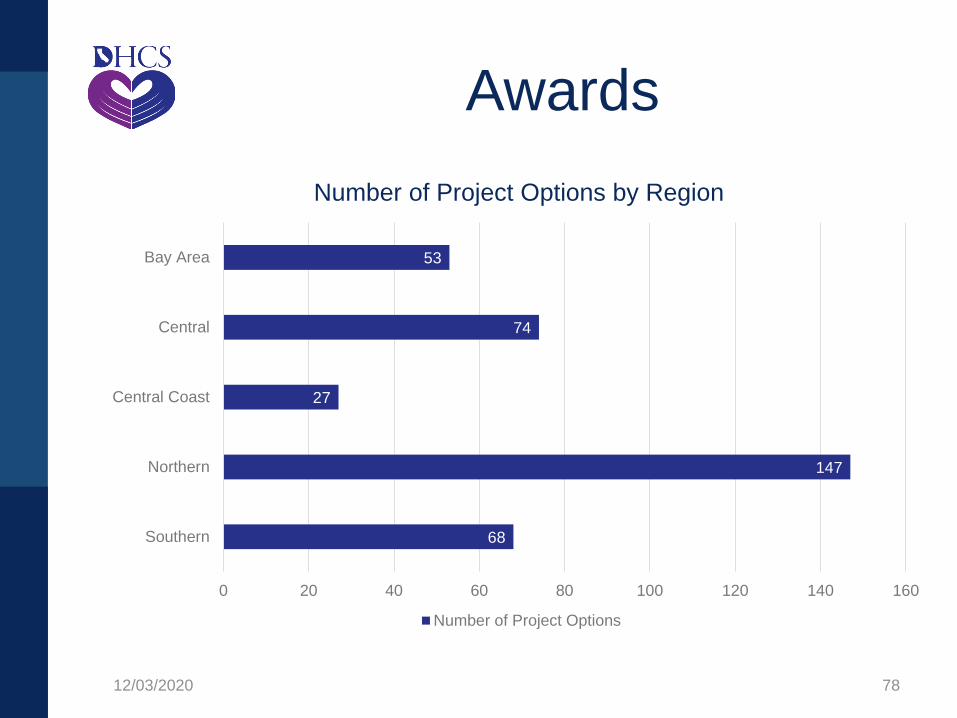
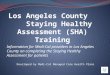
68
147
27
74
53
Southern
Northern
Central Coast
Central
Bay Area
0 20 40 60 80 100 120 140 160
Number of Project Options by Region
Number of Project Options
78
Awards
12/03/2020

For more information, please visit the
BHI Incentive Program Webpage
79
Thank You
12/03/2020
Questions?
12/03/2020 80

Children’s Preventive Care
12/03/2020 81
Preventative Services Report
December Updates
Mike Dutra
Branch Chief
Policy, Utilization & External Relations
12/03/2020 82
• PSR remains on target with an expected release
date to be toward the end of December 2020
• As a reminder, the Report will be released in 2
phases.
The 1st part of the Report will contain statewide
and regional reporting of the rates.
The 2nd part of the Report will be released in
February 2021 and will serve as an Addendum
with MCP-level rates.
• COVID-19 continues to have a significant impact on
CDPH and resources needed from CDPH for this
Report. 12/03/2020 83
Ongoing Work
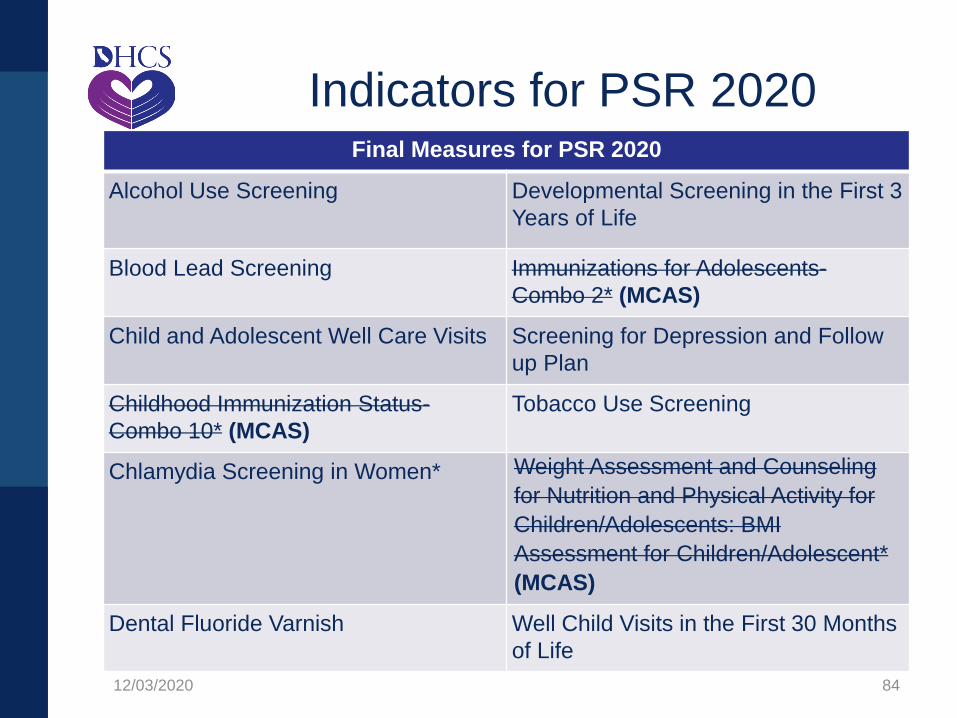
Final Measures for PSR 2020
Alcohol Use Screening Developmental Screening in the First 3
Years of Life
Blood Lead Screening Immunizations for Adolescents-
Combo 2* (MCAS)
Child and Adolescent Well Care Visits Screening for Depression and Follow
up Plan
Childhood Immunization Status-
Combo 10* (MCAS)
Tobacco Use Screening
Chlamydia Screening in Women* Weight Assessment and Counseling
for Nutrition and Physical Activity for
Children/Adolescents: BMI
Assessment for Children/Adolescent*
(MCAS)
Dental Fluoride Varnish Well Child Visits in the First 30 Months
of Life
12/03/2020 84
Indicators for PSR 2020

• Overall, this new level of analysis and reporting will allow DHCS to do a deeper dive and better understand patterns and trends in underutilization so we can deploy targeted interventions and ensure children are receiving the right care at the right time.
• This Report will be used to develop alternative indicators to track utilization for areas of the Bright Futures recommendations that are not currently captured in existing performance metrics.
12/03/2020 85
Subsequent Reports

Questions?
12/03/2020 86

Outreach Campaign Phase 2
Heather M. Jones
Senior Manager, Center for Health Literacy
Nicole Donnelly
Senior Director, Center for Health Literacy
12/03/2020 87
Updates
12/03/2020 88

Managed Care Project Updates
Michelle Retke
Division Chief
Managed Care Operations
12/03/2020 89

Ombudsman Report
Michelle Retke
Division Chief
Managed Care Operations
12/03/2020 90

Sanctions
Nathan Nau
Division Chief
Managed Care Quality & Monitoring
12/03/2020 91
APLs and DPLs Update
Nikki Fogarty Rengstorff
Unit Chief
Policy & Regulatory Compliance
12/03/2020 92
• Date of Issue: 09/29/2020
• Revised:11/02/2020
• APL 20-016 (Revised)
• Supersedes: APL 18-017This APL describes Medi-Cal managed care health plan (MCP) requirements for blood lead screening tests and associated monitoring and reporting. Along with clarifications of existing requirements, it includes new requirements aimed at improving compliance with state regulations. Starting no later than January 1, 2021, MCPs will be required to quarterly identify members under the age of six years who have no record of receiving a required blood lead screening test and notify the network provider who is responsible for the care of an identified child member of requirement to test that child. The APL was revised to address the passage of Assembly Bill (AB) 2276 (Chapter 216, Statutes of 2020).
12/03/2020 93
Blood Lead Screening of Young Children
• Date of Issue: 10/14/2020
• APL 20-017
• Supersedes: APL 14-012 and APL 14-013 (Revised)
This APL provides guidance to MCPs on the updated requirements for submitting program data to the Department of Health Care Services (DHCS). Program Data includes:
• Grievances data;
• Appeals data;
• Medical Exemption Request denial reports and other continuity of care data;
• Out-of-Network request data; and
• Primary Care Provider assignment data.
12/03/2020 94
Requirements for Reporting Managed
Care Program Data
• Date of Issue: 10/14/2020
• APL 20-017
• Supersedes: APL 14-012 and APL 14-013 (Revised)
MCPs have historically submitted Program Data via various Microsoft Excel templates. Beginning no later than July 1, 2021, MCPs will instead be required to report Program Data to DHCS using standardized JavaScript Object Notation (JSON) reporting formats, in compliance with the most recent “DHCS Managed Care Program Data (MCPD) Primary Care Provider Assignment (PCPA) Technical Documentation” and the associated JSON schema files, on a monthly basis.
12/03/2020 95
Requirements for Reporting Managed
Care Program Data (continued)
12/03/2020 96
Ensuring Access to Transgender Services
• Date of Issue: 10/26/2020
• APL 20-018
• Supersedes: APL 16-013
This APL reminds MCPs of their obligations to provide transgender services to members. It also reminds MCPs of laws prohibiting discrimination against individuals based on gender, gender identity, and gender expression. The APL is a clarification of current policy and does not represent a policy change.
MCPs are contractually obligated to provide medically necessary covered services and reconstructive surgery to all members, including transgender members. APL 20-018 clarifies DHCS policy in regard to analyzing transgender service requests, with consideration of nationally recognized clinical guidelines, under both the applicable medical necessity standard for services to treat gender dysphoria and the statutory criteria for reconstructive surgery. The APL further clarifies DHCS policy regarding permissible utilization management.

12/03/2020 97
Governor’s Executive Order N-01-19, Regarding
Transitioning Medi-Cal Pharmacy Benefits From
Managed Care to Medi-Cal Rx
• Date of Issue: 11/4/2020
• APL 20-020
This APL describes MCP requirements related to the transition of Medi-Cal pharmacy services from the managed care delivery system to the Fee-For-Service delivery system known as Medi-Cal Rx, effective January 1, 2021, as required by Governor Gavin Newsom’s Executive Order N-01-19.
This APL details specific MCP pre- and post-transition responsibilities that span across a variety of topics.
Questions?
12/03/2020 98
Next Meeting: March 11, 2021
For questions, comments or to request future
agenda items please email:
Open Discussion
12/03/2020 99