Embed Size (px)
Citation preview
Making Medi-Cal
Managed Care Work
Advanced Medical Management, Inc.
Kathy Hegstrom
President
Conifer Health Solutions
Megan North
President, Value-Based Care
SynerMed
James Mason
President and Chief Executive Officer
Presented By:

“If your plan is for 1 year, plant
rice. If your plan is for 10 years,
plant trees. If your plan is for
100 years, educate.”
- Confucius
2

• Body text goes here
– Bullet text
• Sub bullet
• Body text here
3Winter is Coming?!
4No Need to Lose Your Head
So You Pick Your Path to the Throne … 5

Unfortunately, You Also Get…
7
Commercial Break
Advanced Medical Management
• AMM as Management Services Organization (MSO)
– Independent Physician Associations
– Hospitals
• AMM specializes in Niche Clients with Custom Needs
– Language & Cultural (Korean, Vietnamese, Arabic )
– Start-ups (single owner, specialty owners)
– Unique Structures (Performance-based , Closely held)
– Geographic (Rural, Hospital-centric, International)
– Limited Knox Keene
8
Advanced Medical Management
• AMM as Fiscal Intermediary (FI)
– Government Programs
• Medically Indigent
• Custodial
• Public Health
• AMM as Contracted Claims Processing
– Health Plans
• Overflow during Rapid Expansion
• Commercial ACO Demonstration
– Hospitals
• Dual Risk
9
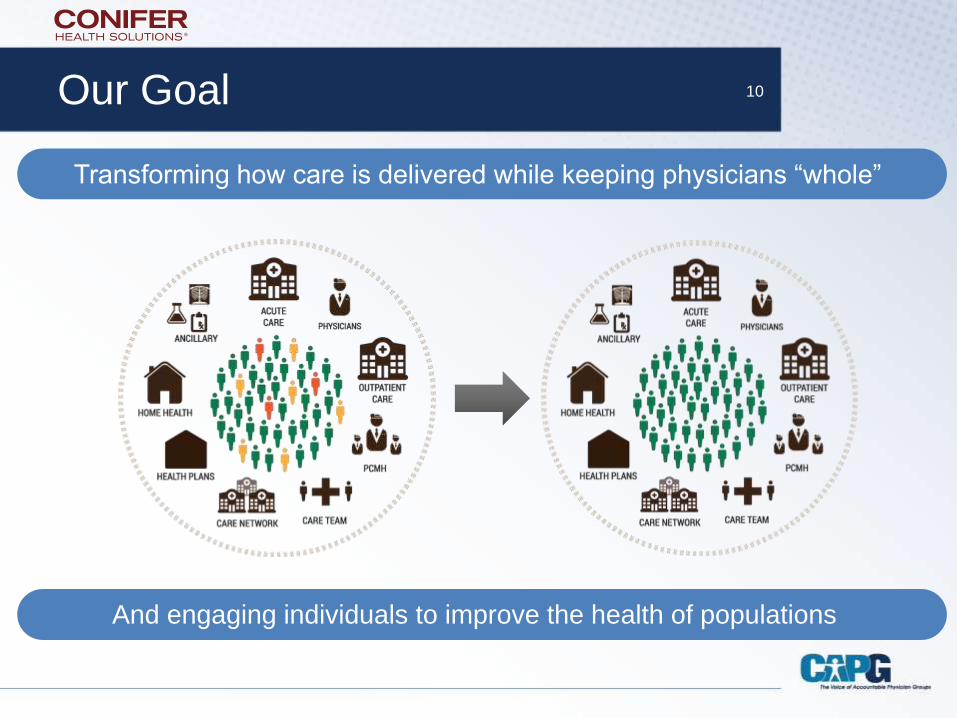
Our Goal 10
Transforming how care is delivered while keeping physicians “whole”
And engaging individuals to improve the health of populations
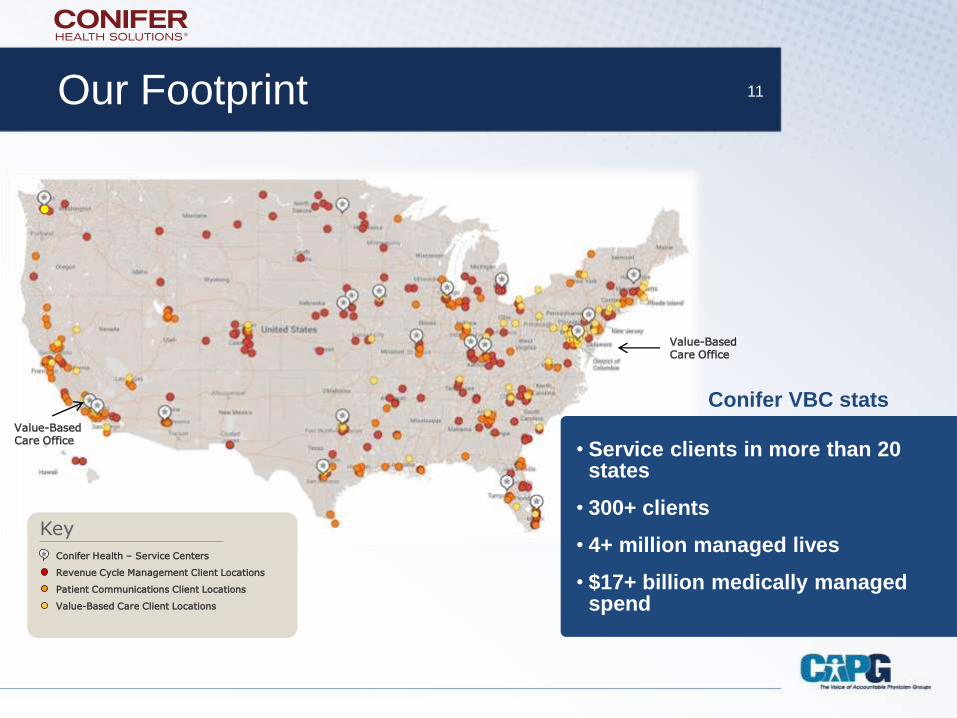
Our Footprint 11
Conifer VBC statsValue-Based Care Office
Conifer Health – Service Centers
Revenue Cycle Management Client Locations
Patient Communications Client Locations
Value-Based Care Client Locations
Key
• Service clients in more than 20 states
• 300+ clients
• 4+ million managed lives
• $17+ billion medically managed spend
Value-Based Care Office
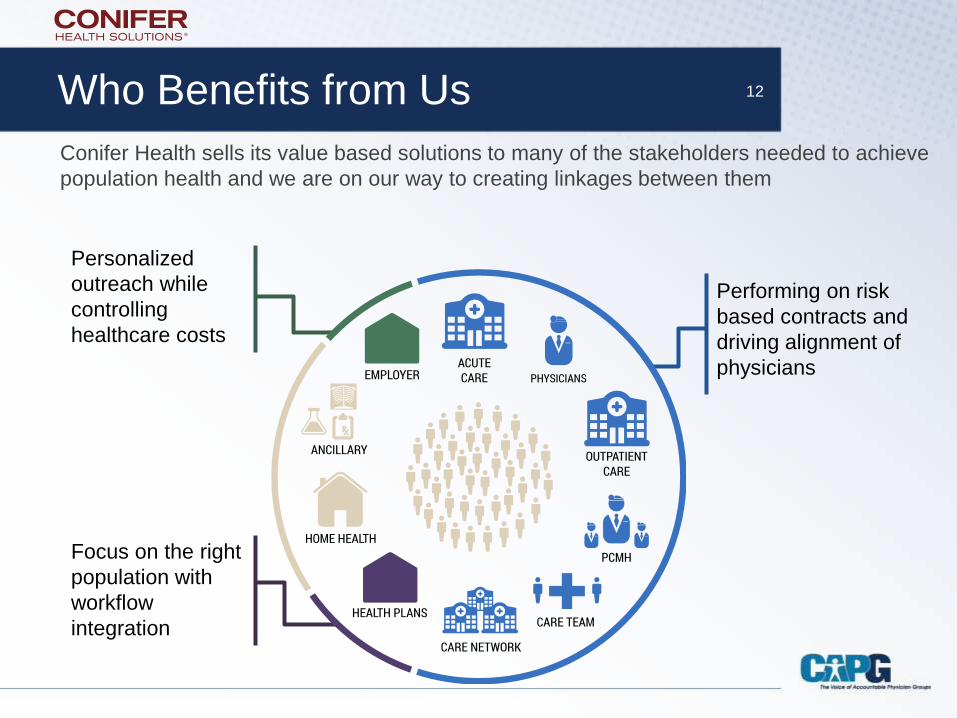
Who Benefits from Us 12
Performing on risk
based contracts and
driving alignment of
physicians
Focus on the right
population with
workflow
integration
Personalized
outreach while
controlling
healthcare costs
Conifer Health sells its value based solutions to many of the stakeholders needed to achieve
population health and we are on our way to creating linkages between them
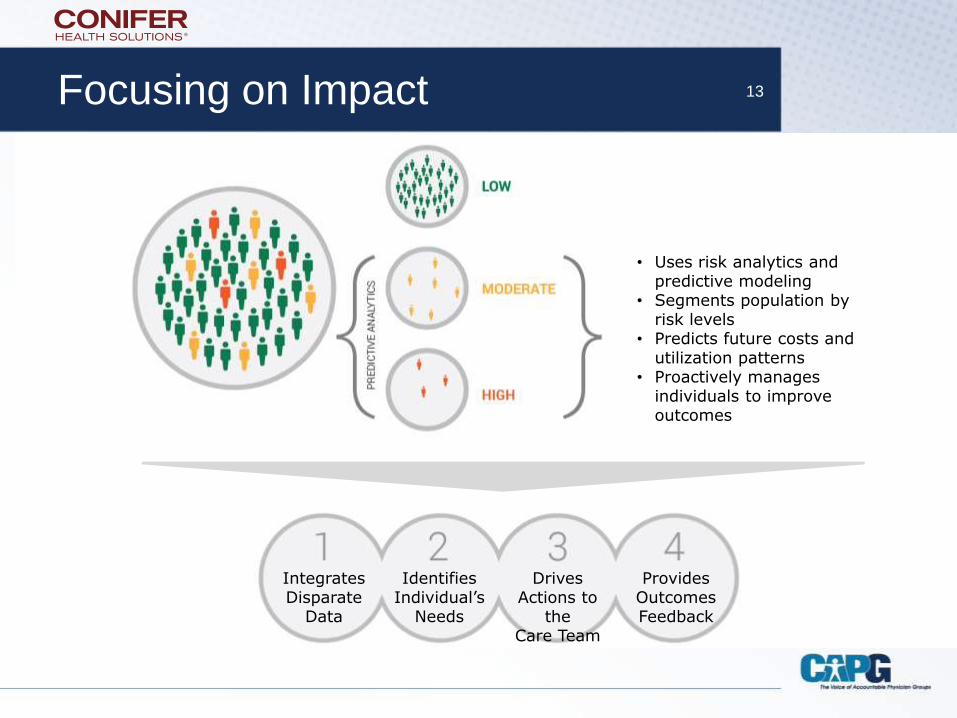
Focusing on Impact 13
IntegratesDisparate
Data
IdentifiesIndividual’s
Needs
DrivesActions to
theCare Team
ProvidesOutcomesFeedback
• Uses risk analytics and predictive modeling
• Segments population by risk levels
• Predicts future costs and utilization patterns
• Proactively manages individuals to improve outcomes

Technology Platform to Improve Performance 14
What We Do
SynerMed provides an agnostic provider network for Plans
• PLANS GET– Low cost, high quality networks
• PHYSICIANS GET– Advanced technology, market leverage and better economics
through population health management
• PATIENTS GET– More choices, high quality networks and a team approach to
medicine
15
Vital Statistics
• 400 FTEs
• 800,000 members
• Serving:
• Sacramento
• Fresno
• Madera
• Kings
• San Bernardino
• Riverside
• Los Angeles County
• San Diego County
• Georgia
16
• $500 Million in
healthcare spend under
management
• All healthcare products:
• TANF
• SPD
• SCHIP
• Medi-Medi
• Medicare
• Commercial

17
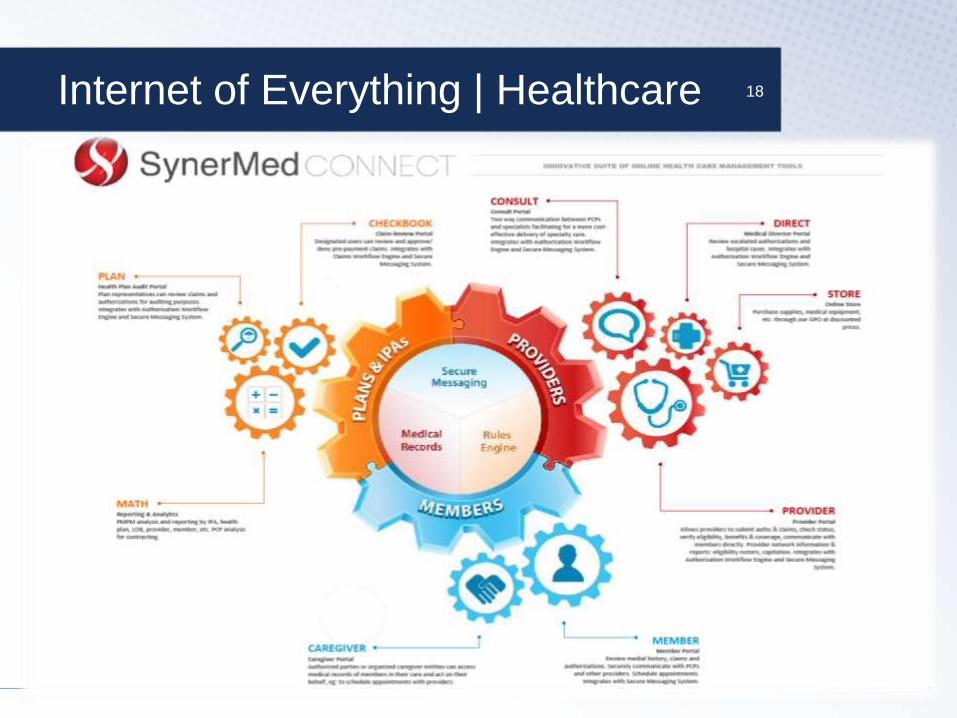
Internet of Everything | Healthcare 18
19
Back to Your Regular Programming
• SPDs Lessons Learned
• Covered California
– Welcome Mat Effect
• MCEs
• CCI Dual Demo
20The Others! Winter is Coming!
SPDs
• Sicker
• Pent up utilization due to
lack of access
• Dual and Tri DX
• Homelessness or near
homelessness
21
• 20% sicker than SPDs
that opted into Managed
Care versus those
passively enrolled
• Gaps in the PCP model
of care
• Is the delegated
risk/revenue ratio
appropriate?
MCEs
• L1s
– Who are they?
• M1s
– What’s the difference?
22
• We don’t know yet –
hopefully by the time we
speak, we will know
more about utilization
patterns
• Is the delegated
risk/revenue ratio
appropriate?
Duals
• High-cost, high needs
patient population
• 55% have 3 or more
chronic conditions
• 1 in 6 live in an
Institution
• 50% are Dual DX
• Old model was
fragmented, confusing
and inefficient
23
• Part A
• Part B
• MLTSS
– LTC/Custodial
– IHSS
– CBAS
– MSSP
– PACE
Duals Demo
• 456,000 in 8 Pilot
Counties:
– Alameda
– Los Angeles
– Orange
– San Diego
– San Mateo
– Riverside
– San Bernardino
– Santa Clara
24
• 4/1 San Mateo
• 5/1 San Diego, San
Bernardino/Riverside
• 7/1 Alameda and
Los Angeles
• 1/1/15 Santa Clara
25Questions?
This presentation is subject to copyright. Any reproduction or republication of all or part of this presentation is expressly prohibited. All other rights
reserved. The names, trademarks, service marks and logos or the sponsors appearing in this presentation may not be used in any advertising or
publicity, or otherwise to indicate sponsorship or affiliation with any product or service.