Embed Size (px)
DESCRIPTION
Just about all any patient would want to know about nuclear imaging.
Citation preview

http://www.medcyclopaedia.com/library/radiology/chapter07/7_5.aspx Glossary AbdomenAbdominalAbsorption characteristicsAcoustic neurinomaAdenomaAggregateAneurysmAngiographyAngioplastyAnticoagulantAortaArachnoideaArrhythmiaArtefactArteryArthrographyArticularAsbestosisAsystoleAtherosclerosisatrium (pl. atria)AtrophicBariumBenignBiliary atresiaBiopsyBlood-brain barrierBrain stemBrain, x-rayBronchialCalcificationCalcifiedCalculiCalycesCapillariesCapsuleCarcinomaCardiacCardiac imagingCardioangiographyCardiologistCardiomyopathyCardiovascular imagingCarotid (artery)Carrier moleculeCartilageCascadeCatheterCatheters, x-rayCentral nervous system (CNS)CerebellumCerebralCerebrospinal fluid (CSF)CerebrovascularCerebrumCervicalChemotoxicityCholangitisCholecystitisCirrhosisClotClottingCNSCNS imagingCollecting systemCongenitalContra-indicationContractilityContrast media (sing. medium) (CM)ContusionCoronary (artery)CTCT-myelographyCystCysticCystoscopyDecayDeep venous thrombosis (DVT)DegenerativeDementiaDemyelinatingDepolarisationDeposition diseasesDiastoleDiffuseDimericDirect injectionDiskDissectionDopplerDuodenal bulbDuodenitisDuodenumDural sacDynamicEchocardiographyEchogenicityElectromagnetic radiationEmbolusEmphysemaEndo-vascularEndoscopicEndoscopyEndothelialEnemaEnhanceErythrocyteExtracellularExtraspinalExtrasystoleExtremitiesFat-suppressedFatty liverFibrillationFibrinFibrinogenFibrinolysisFibrosisFilling defectFine-needle biopsyFlushingFocalFocal nodular hyperplasia (FNH)FpAFractureFrenchFunctional imagingGall-bladder stoneGamma cameraGantryGastritisGastro-oesophagealGastrointestinal (G.I.) tractGastrointestinal tract imagingGlandularGlomerular filtration (GF)HaemangiomaHaematomaHaemorrhageHaemosiderosisHaemostasisHalf-lifeHead and neck imagingHeart, ultrasoundHelicobacter pyloriHepatitisHerniationHigh-osmolarHilarHistamineHydrogenHypertensionHypertonicHypervascularityHypotensionHypotonicIn vitroIn vivoInfarctedInfarctionInfiltrationInflammationInotropyIntercellularInterfaceIntermittentInterstitialIntervertebral discsIntimaIntimal tearIntra-arterialIntracellularIntraspinalIntravenousInvasiveInvasivenessIonicIonising radiationIschaemicIsotonicityIsotopeKidney, X-rayLacerationLaminar flowLD50LesionLigamentLiver and gallbladder imagingLow-osmolarLower G.I. tractLumenLuxationLymphLymphadenopathyLymphangiographyLymphomaMalignantMammographyMediastinalMedical

imagingMeningesMetastasisMicroadenomaModalitiesModalityMonomericMRIMRI contrastMucosaMucous membraneMulti-sliceMultiplanarMultiple sclerosis (MS)Musculoskeletal system imagingMyelographyMyocardialMyocardiumNeoplasmNephrotoxic Effects in High-Risk Patients Undergoing AngiographyNephrotoxicityNerve-rootNeurological examinationNeurotoxicityNodularNon-ionicNuclearNuclear disk protrusionNuclear medicine (NM)ObstructionOccultOesophagusOpaqueOralOsmolalityOsmotoxicityOsteoblasticOsteolyticOsteomyelitisOsteonecrosisOsteoporosisParanasalParathyroidParenchymaPathologicalPelvisPerfusionPermeabilityPETPhlebographyPituitaryPlaquePlasma proteinsPlateletPleuralPolypoidPorus acusticusPosterior fossaPremedicationProbeProjectionProliferationProtrusionPT(C)APulmonaryRadio-pharmaceuticalRadioactivityRadiographicRadiologistRadionuclideRadiopharmaceuticalRadiotherapyReal-timeRectumReferring doctorRegion of interestRegurgitationRenalRenal pelvisRepolarisationResolutionRheumatoid arthritisRouleauxSarcoidosisScanSciaticScintigramSectionalSensitivitySinusSonographySpasmSpecificitySPECTSpinal canalSpinal cordSpinal imagingSpineSpiral CTStenosisStentingStress fractureStrokeSubacuteSubarachnoid spaceSynovialsystole99mTcTemporalTendonThoracicThorax, imagingThrombinThrombusThyroidThyrotoxicosisTIATissue characterisationTransabdominalTraumaTubularTumourUlcerationUltrasoundUltrasound contrastUpper G.I. tractUreterUrethraUrinary system imagingUrinary tractUrographyUrologistVascularVascular imagingVeinVenographyVentricleVertebraeVertebral columnWedgingWhite matterX-rayX-ray contrast Textbook of Radiology
Preface
1. W.C. Roentgen and the discovery of X-rays Peter Peters, Germany
2. Radiology in an international perspective Carl-Gustaf Standertskjöld- Nordenstam, Finland
3. Radiophysics Aaro Kiuru, Finland

4. Modalities and methods Hans-Jørgen Smith, Norway
5. Radiology worldwide - the WHO approach Philip E.S. Palmer, USA Thure Holm, Sweden Gerald P. Hanson, Switzerland
6. Digital imaging Tatsuo Kumazaki, Japan Hans Ringertz, Sweden
7. Contrast media in diagnostic radiology Torsten Almen, Sweden Peter Aspelin, Sweden
8. Interventional radiology Christoph Zollikofer, Switzerland
9. The brain Kjell Bergström, Sweden Giuseppe Scotti, Italy
10. The head and neck Sven-Göran Larsson, Saudi Arabia Anthony Mancuso, USA
11. Dental radiology Lars Hollender, USA Karl-Åke Omnell, USA
12. The spine Stig Holtås, Sweden Maximilian F. Reiser, Germany Axel Stäbler, Germany
13. Musculoskeletal radiology Niels Egund, Denmark Kjell Jonsson, Sweden Hoiger Pettersson, Sweden Donald Resnick, USA
14. Pediatric musculoskeletal radiology Andrew K. Poznanski, USA
15. Pediatric radiology Donald R. Kirks, USA Sven Laurin, Sweden
16. Pediatric neuroradiology Olof Flodmark, Sweden Derek Harwood-Nash, Canada

17. Breast imaging Ingvar Andersson, Sweden Baldur F. Sigfússon, lceland
18. The lungs and mediastinum Alf Kolbenstvedt, Norway Arnulf Skjennald, Norway Charles B. Higgins, USA
19. The heart Charles B. Higgins, USA Arnulf Skjennald, Norway
20. The peripheral vessels Christoph Zollikofer, Switzerland Frode Laerum, Norway
21. The lymphatic system Elias Zerhouni, USA
22. The gastrointestinal tract Richard M. Mendelson, Australia
23. The liver, biliary tract, pancreas and spleen David J. Allison, United Kingdom Carl-Gustaf Standertskjöld-Nordenstam, Finland
24. The acute abdomen David J. Allison, United Kingdom Olle Ekberg, Sweden Frans-Thomas Fork, Sweden
25. The genitourinary system Henrik Thomsen, Denmark Howard Pollack, USA
26. Obstetric imaging Con Metreweli, Hong Kong
27. Tropical diseases Philip E.S. Palmer, USA Stanley P. Bohrer, USA Carlos Bruguera, Argentina Xing-Rong Chen, China Mahmoud R. EImeligi, Egypt Hassen A. Gharbi, Tunisia S.E. Lagundoye, Nigeria M. W Wachira, Kenya
28. Radiology in AIDS Marie-France Bellin, France Philippe Grenier, France Nadine Martin-Duverneuil, France

PRODUCTS & SOLUTIONSNEWS & EVENTSFINANCIAL SERVICESOUR COMMITMENTABOUT GE HEALTHCAREWORLD-WIDE
Medcyclopaedia Home E-learningLibraryLexical IndexLexical TopicsGlossaryFace-a-CaseTextbook of RadiologyPrefaceW.C Roentgen and the discovery of X-raysRadiology in an international perspectiveRadiophysics Modalities and methodsRadiology worldwide – the WHO approach Digital imaging Contrast media in diagnostic radiology IntroductionContrast media for röntgen rays (X-rays)Positive contrast mediaNegative contrast mediaContrast media in magnetic resonance imaging (MRI)Interventional radiology The brainThe head and neckDental radiologyThe SpineMuskoskeletal radiology Paediatric musculoskeletal radiologyPedriatic radiology Pediatric neuroradiology Breast imaging The lungs and mediastinum The heart The peripheral vesselsThe lymphatic system The gastrointestinal tract The liver, biliary tract, pancreas and spleen The acute abdomen The genitourinary systemObstetric imaging Tropical diseases Radiology in AIDSTextbook of Radiology (e-paper)Medical Imaging Made EasyDownloadsMedcyclOasisAbout MedcyclopaediaContact Us
MedcycloPoll Did you get the help you required from Medcyclopaedia™ during today's visit?
Yes (84.8%) No (10.6%) Undecided (4.6%)
You must be logged on to vote. Please log in or register.
helpadvanced search
Library / Textbook of Radiology / Contrast media in diagn… / Contrast media in magne…

previous in index · next in index
Printer-friendly version Bookmark This Page
Translate page to (By Google): Contrast media in diagnostic radiology Contrast media in magnetic resonance imaging (MRI)
In the early years of clinical MRI it was believed that the natural contrast between different soft tissues would exclude the need for contrast media. It was soon found (just as in computed tomography) that the signal differences between the different tissues, i.e. the contrast resolution in the MR-image, could be profoundly improved by different contrast media. It was not until the first MRI contrast medium (Gd-DTPA, based on the paramagnetic gadolinium ion inside the chelate DTPA) became commercially available that MRI became equal to or better than computerized tomography in certain applications.
Mechanisms behind MR contrast media For information on the T1- and T2-weighted images in MRI, we refer the reader to the chapters on "Radiophysics" and on "Modalities". The signal intensity from a small volume unit (a voxel) in a patient undergoing MRI depends on several factors. Among the machine-related factors are the strength of the magnetic field and gradient coils, the sequences of proton-exciting radio waves from the transmitting antenna and the timing for signal registration in the receiving antenna. Among patient factors are the proton spin density inside a voxel and the T1- and T2-relaxation times of the protons inside those voxels. It is known that
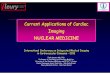
Figure 6. lnfluence of paramagnetic and
ferromagnetic contrast media on the intensity of the MR-signal.
some substances may influence the relaxation times of protons in their vicinity. The MR contrast medium inside a voxel can influence the proton relaxations times T1 and T2 or the proton dens it y inside that voxel. Depending on different magnetic properties, the MR contrast media are divided into paramagnetic and super-paramagnetic media.

Paramagnetic contrast media Atoms with one or several unpaired electrons have paramagnetic properties. The most common MRI contrast media are paramagnetic metal ions with a large magnetic moment. Examples of such ions are gadolinium, chromium, manganese, nickel and iron. Gadolinium compounds have hitherto enjoyed the largest clinical use. The large arrows in Fig. 6 illustrate that the MR signals from a voxel become stronger with higher proton density, shorter T l-time and longer T2-time. The small arrows in Fig. 6 illustrate how a paramagnetic contrast medium, in clinical doses, may increase the signal intensity through a shortening of T1-time, while the super-paramagnetic contrast media mainly decrease the MR-signal through a shortening of T2-time. The contrast medium effect of the gadolinium ions is a reduction in T1- and T2-relaxation times. In low doses it is mainly a T1-effect which increases the signal intensity, illustrated in Fig. 6. In high doses it is more a T2-effect with a reduction of the signal.
Superparamagnetic contrast media Superparamagnetic iron oxide is used as contrast medium. Its dominating effect is a reduction of T2-relaxation time. With an increasing dose there is a reduction of signal intensity (Fig. 6).
Depending on the above mentioned mechanisms the T1-weighted images are mainly influenced by paramagnetic contrast media, while T2-weighted images are mainly influenced by superparamagnetic contrast media (Figure 6).
Water soluble extracellular contrast media The first registered contrast medium is a gadolinium chelate, gadopentatedimeglumine (MagnevistR). Chelate means "claw" and describes how the gadolinium ion (Gd3+) with three positive "unit charges" is trapped in a negatively charged chelate (claw or cage) consisting of the dimeglumine salt of diethylene-triamine-penta-acetic-acid (DTPA), which has 5 negatively charged carboxyl groups (5 "unit charges"). The Gd-DTPA ion has 2 negative "charges" (+3 -5 =-2) and is accompanied by 2 positively charged meglumine ions for electroneutrality. The benefit gained by enclosing the Gd-ion in DTPA is that the Gd-DTPA ion has a ten times lower toxicity than the free or non-chelated Gd-ions. This DTPA detoxifying effect on the Gd-ion toxicity causes slight shielding of the magnetic field of the 7 unpaired electrons of the Gd-ion with some decrease of its effects on protons in the body. The pharmacokinetic properties of Gd-DTP A resemble those of the intravenous water soluble iodine contrast media. It has a high water solubility, a small binding affinity for proteins and a low intracellular penetration. It is distributed almost exclusively in the extra-cellular space and excreted by the glomeruli. At normal glomerular filtration rate its plasma half-life is 90 minutes and over 75% of the dose is excreted via the kidneys in 3 hours.
Gd-DTP A, like the iodine contrast media, does not cross the normal blood brain barrier when injected intravascularly. When there is a blood brain barrier

damage, e.g. in patients with cerebral tumors or vascular lesions, Gd-DTP A leaks out into the interstitial fluid of the CNS (within the tumor or vascular lesion). The higher the Gd concentration gets in a tissue (compartment) the shorter the T1-time in that tissue. The Gd-DTPA concentration may be different in normal brain parenchyma, edema and tumor tissue and this increases the ability to differentiate between these structures.
The clinically recommended doses vary between 0.1 and 0.2 mmol/kg body weight. Sometimes a feeling of warmth and headache can occur (12 %). Gd-DTP A (Magnevist) is extremely safe and has in clinical doses an even lower frequency of pseudoallergic reactions than the non-ionic iodine contrast media.
New Gd contrast media for the extracellular space are being developed and some have been introduced into clinical practise. Some examples follow: Gd-DTPA is a linear ionic Gd-chelate, while Gd-DOTA is a cyclic ionic chelate. Gd-DTP A-BMA (Omniscan) and Gd-HP-D03A (Prohance) are neutral or nonionic linear and cyclic chelates, respectively. Their clinical use has just started and their exact roles will be defined in the future.
Macromolecular Gd-chelates (Albumin-Gd-DTP A, Dextran-GdDTPA, Polylysin-Gd-DTPA) and paramagnetic liposomes have been tried as blood pool agents. The liposomes are taken up by the reticuloendothelial cells (RES) and may be used as media to image the reticuloendothelial system, for instance, Kupffer cells. Water soluble paramagnetic contrast media with lipophilic components in the chelate host are taken up by the liver and have been designed as contrast media for the liver parenchyma. Some examples of these are: Mn-DPDP, GdBOPTA, and Gd-EOB-DTPA.
Oral contrast media Just as in computerized tomography the oral contrast media are used mainly in abdominal imaging, in order to differentiate between intestine and surrounding normal and pathological tissues. Demarcation of the small intestine is particularly important in abdominal diagnosis.
Magnetite, Fe3O4 is a contrast medium which has been used in the gastrointestinal tract. This is a superparamagnetic contrast medium with its main effect on the T2 relaxation and it works as a negative contrast medium. This means that it decreases the signal intensity. Other negative contrast media in the gastrointestinal tract are gases and perfluor compounds which in principle do not contain any hydrogen atoms and therefore do not give any signal.
Contrast media for ultrasound In ultrasound, sound waves with a frequency of 3-15 MHz are used. These sound waves are generated by the piezoelectric crystal in the ultrasound transducer. Ultrasound energy penetrates different tissues and is attenuated both by reflection and absorption. In contrast to the roentgenogram which is created by X-rays transmitted by different structures of the body, the ultrasound image is

created by ultrasound energy reflected by different structures of the body: "echoes".
The extent to which sound is reflected by a tissue depends on the acoustic impedance of the tissue or the tissue components. The larger the difference in acoustic impedance between two tissue types, the larger the reflection of the ultrasound from the interface between those two tissues.
Except for air, fat and bone, the natural differences in acoustic impedance between different soft tissues in the body are small. The differences that exist between different tissues with regard to reflectivity of ultrasound depend on the different amounts of components such as collagen, fat and fibro-elastic tissue. Presently, contrast media are developed which increase the differences in the amount of ultrasound energy reflected by different structures of the body. An ultrasound contrast medium can thus be described as an echogenic substance which is introduced into a vessel or organ system in order to induce an increased echogenicity - increased ability to reflect ultrasound energy. Such media may be injected intravenously and examples are - suspensions of solid particles, emulsions of fluid droplets, micro bubbles of pure gas, gas bubbles encapsulated in various structures or liquids that release micro bubbles. Like other contrast media, ultrasound media should have low toxicity and fast excretion.
Examples of ultrasound contrast media, in different stages of development and/or clinical introduction, are: - Suspensions in water of solid particles of, for instance, an ethylester of the biliary medium iodipamide, which, in blood, functions as a blood pool agent and increases the reflectivity of blood and which, after being phagocytosed in the liver, increases the echogenicity (reflectivity) of the liver. - Droplets of perfluorocarbon compounds, oily liquid media, which similarly first act as a blood pool medium and then as a liver parenchyma medium. - Micro bubbles of gas encapsulated in albumin (Albunex). - Micro bubbles of gas encapsulated by galactose (Echovist) or entrapped in galactose/fatty acids (Levovist). - Liquid which is injected into the blood and then inside the blood releases micro bubbles of gas (EchoGen).
While Echovist is trapped in the lungs and therefore used only for cardiac diagnosis and for the large veins, several of the other ultrasound media pass through the lung capillaries and other capillaries and can therefore be used for a larger number of organs. The usefulness of an ultrasound medium is that it may increase the contrast resolution between normal and diseased tissue and may improve the identification of deep lying vessels and help in identifying tumorsor tumor vessels. Other possible advantages are the improved visualization of stenotic arterial segments, e.g. renal arteries and the increased ability to detect areas of infarction or ischemia. The possibility of tissue characterization might also increase with different ultrasound contrast media.

Torsten Almén and Peter Aspelin
Products & Solutions | News and Events | Financial Services | Our Commitment | About
GE Healthcare | Contact us GE Healthcare Home | GE Corporate Home | Privacy Policy | Terms of Use |
Accessibility Statement | Affiliate
Copyright General Electric Company 1997-2008 | GE Healthcare
Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Infarction: The actual closure of blood supply, usually by a blood clot ( embolism ) that blocks the artery supplying the (part of an) organ or tissue. Renal: Relating to the kidneys Resolution: 1- Spatial resolution = image "sharpness", i.e. how small details can be seen. 2 - Contrast resolution = how clearly different intensities (e.g. different shades of grey) can be differentiated. 3 - Temporal resolution = ability to "freeze" movement. Ultrasound: Sound waves with a higher frequency than can be heard

by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Capillaries: The smallest type of blood vessels. Blood flows very slowly in the capillaries enabling exchange of oxygen and nutrients from the blood into the tissues, and waste products and carbon dioxide from the tissues back into the blood. Capillaries: The smallest type of blood vessels. Blood flows very slowly in the capillaries enabling exchange of oxygen and nutrients from the blood into the tissues, and waste products and carbon dioxide from the tissues back into the blood. Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy

levels (more…) Cardiac: Relating to the heart. Parenchyma: The actual, specialised tissue(s) in an organ (heart, kidney, liver) or gland Echogenicity: Ability to create an echo, i.e. return a signal in ultrasound examinations. Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard

by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Echogenicity: Ability to create an echo, i.e. return a signal in ultrasound examinations. Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are

reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Interface: The borderline between 2 materials with different physical properties (e.g. density). Interfaces have the ability to reflect wave-form energy like sound or light, such as a water surface (= air/water interface) reflecting light, or kidney reflecting ultrasound waves, since kidney tissue is more dense than the surrounding fat and connective tissues. Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different

tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as

these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual

sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Ultrasound: Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another). Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels (more…) Hydrogen: The smallest and lightest chemical element (chemical symbol: H). Occurring naturally as a gas, but also one of the main building stones of water, proteins, fats and sugars. The protons or hydrogen nuclei behave like tiny compass needles, and can be influenced by strong external magnetic fields, as in MRI . Abdominal: Relating to the abdomen . Pathological: Relating to any disease process, as opposite to normal or healthy. Abdominal: Relating to the abdomen . Oral: Relating to the mouth. Used to describe how a drug (or contrast medium ) is administered, as opposite to injection (=parenteral) or rectal (= as an enema ) Oral: Relating to the mouth. Used to describe how a drug (or contrast medium ) is administered, as opposite to injection (=parenteral) or rectal (=

as an enema ) Parenchyma: The actual, specialised tissue(s) in an organ (heart, kidney, liver) or gland Ionic: Ionic contrast media chemically are salts of weak organic acids containing iodine. Like most salts they will split into two particles, called an anion and a cation, when dissolved in water. The anions are iodinated benzene rings, where one of the side chains is a weak organic acid (benzoic acid). They are either single benzoic rings ( monomeric contrast media) like diatrizoate, metrizoate or iothalamate, or as two linked rings ( dimeric contrast media) like iocarmate or ioxaglate. The cations are either metals like Na+ (sodium), Ca++ (calcium) or Mg++ (magnesium) or organic cations like meglumine (methylglu (more…) Ionic: Ionic contrast media chemically are salts of weak organic acids containing iodine. Like most salts they will split into two particles, called an anion and a cation, when dissolved in water. The anions are iodinated benzene rings, where one of the side chains is a weak organic acid (benzoic acid). They are either single benzoic rings ( monomeric contrast media) like diatrizoate, metrizoate or iothalamate, or as two linked rings ( dimeric contrast media) like iocarmate or ioxaglate. The cations are either metals like Na+ (sodium), Ca++ (calcium) or Mg++ (magnesium) or organic cations like meglumine (methylglu (more…) Extracellular: Outside the cells of an organ or tissue Non-ionic: Non-ionic contrast media are contrast media that do not dissociate when solved in water. The number of particles in solution per iodine atom is therefore lower than for

ionic contrast media. Non-ionic monomeric contrast media consist of one benzene ring with 3 iodine atoms ("Ratio 3 "). Their osmolalities are about half that of ionic monomeric contrast media, or 2.5-3 times the osmolality of blood at the highest available concentrations. Non-ionic dimeric contrast media have two linked iodinated benzene rings. These molecules have 6 iodine atoms per particle ("Ratio 6 "). Non-ionic contrast media are more phy (more…) Parenchyma: The actual, specialised tissue(s) in an organ (heart, kidney, liver) or gland Lesion: Any part of an organ/tissue or otherwise limited area that is damaged (e.g. tumour , fracture, inflammation , infection) Vascular: Relating to a blood vessel CNS: Central Nervous System ; the brain and spine. Interstitial: Almost synonymous to intercellular Vascular: Relating to a blood vessel Cerebral: Relating to the brain. Half-life: All radioactive substances are by definition unstable. When unstable forms (= radioactive isotope) of an element (atom) decay into stable forms (= stable isotope), they do so by releasing energy (radiation) and/or particles. The rate at which this decay occurs is called the half-life - i.e. the time required for half of the atoms of a radioactive substance present to become disintegrated. The half-lives vary greatly. Some radionuclides have a half-life of only a few seconds, while others may have a half-life of several thousand years. Radionuclides are widely used in medical imaging. Isotopes with a very

short t1 (more…) Intracellular: Within a cell Intravenous: used in relation to anything that is injected or deposited into a vein . Extracellular: Outside the cells of an organ or tissue MRI: Magnetic Resonance Imaging. The newest of the 4 imaging modalities . In an MRI examination, the patient is placed in a strong electromagnetic field. When this happens, the millions of hydrogen atoms in the body align themselves parallel with the magnetic field, either in the same direction or opposite to the direction of the field. All body tissues contain hydrogen atoms, but in different concentrations and compositions depending on the type of tissue. At the level ("slice") where it is desired to 'take a picture', a short, powerful radio signal (yet another form of electromagnetic energy) is sent through (more…) MRI: Magnetic Resonance Imaging. The newest of the 4 imaging modalities . In an MRI examination, the patient is placed in a strong electromagnetic field. When this happens, the millions of hydrogen atoms in the body align themselves parallel with the magnetic field, either in the same direction or opposite to the direction of the field. All body tissues contain hydrogen atoms, but in different concentrations and compositions depending on the type of tissue. At the level ("slice") where it is desired to 'take a picture', a short, powerful radio signal (yet another form of electromagnetic energy) is sent through (more…) Modalities: plural of modality MRI: Magnetic Resonance Imaging. The newest of the 4 imaging

modalities . In an MRI examination, the patient is placed in a strong electromagnetic field. When this happens, the millions of hydrogen atoms in the body align themselves parallel with the magnetic field, either in the same direction or opposite to the direction of the field. All body tissues contain hydrogen atoms, but in different concentrations and compositions depending on the type of tissue. At the level ("slice") where it is desired to 'take a picture', a short, powerful radio signal (yet another form of electromagnetic energy) is sent through (more…) MRI: Magnetic Resonance Imaging. The newest of the 4 imaging modalities . In an MRI examination, the patient is placed in a strong electromagnetic field. When this happens, the millions of hydrogen atoms in the body align themselves parallel with the magnetic field, either in the same direction or opposite to the direction of the field. All body tissues contain hydrogen atoms, but in different concentrations and compositions depending on the type of tissue. At the level ("slice") where it is desired to 'take a picture', a short, powerful radio signal (yet another form of electromagnetic energy) is sent through (more…) MRI: Magnetic Resonance Imaging. The newest of the 4 imaging modalities . In an MRI examination, the patient is placed in a strong electromagnetic field. When this happens, the millions of hydrogen atoms in the body align themselves parallel with the magnetic field, either in the same direction or opposite to the direction of the field. All body tissues contain hydrogen atoms, but in different concentrations and compositions depending on the type

of tissue. At the level ("slice") where it is desired to 'take a picture', a short, powerful radio signal (yet another form of electromagnetic energy) is sent through (more…) Resolution: 1- Spatial resolution = image "sharpness", i.e. how small details can be seen. 2 - Contrast resolution = how clearly different intensities (e.g. different shades of grey) can be differentiated. 3 - Temporal resolution = ability to "freeze" movement. MRI: Magnetic Resonance Imaging. The newest of the 4 imaging modalities . In an MRI examination, the patient is placed in a strong electromagnetic field. When this happens, the millions of hydrogen atoms in the body align themselves parallel with the magnetic field, either in the same direction or opposite to the direction of the field. All body tissues contain hydrogen atoms, but in different concentrations and compositions depending on the type of tissue. At the level ("slice") where it is desired to 'take a picture', a short, powerful radio signal (yet another form of electromagnetic energy) is sent through (more…)
Printer-friendly version Bookmark This Page
Translate page to (By Google): Contrast media in diagnostic radiology Positive contrast media
Water soluble iodine contrast media for the extracellular space These contrast media are used for intravenous urography, angiography and for contrast enhancement in computerized tomography.

History - mechanisms of toxicity In 1895 Wilhelm Conrad Röntgen discovered X-rays. As early as 1986 the first arteriography was performed in an amputated hand. A contrast medium consisting of a suspension of chalk in water was injected into the arteries. The first water soluble iodine contrast medium was used in 1920 and was discovered because patients with syphilis in those days were treated with sodium iodide. The sodium iodide was observed in an image of the abdomen as an "increased density" of the kidneys. Sodium iodide, however, had a high toxicity when used as contrast medium.
Table 1. Different contrast media - their structure, ratio, viscosity, osmolality and name
Structure Ratio Viscosity Osmolality Generic name Trade name
20 37o
Figure 2
ionic monomer
3:2=1.5
5+
9++
3+
5++
1500-1600
iothalamate
metrizoate amidotrizoate
ioxithalamate
Conray Vasoray Isopaque Urografin
Angiografin Gastrografin
Telebrix Figure
3 ionic dimer 6:2=3 12 6 600 ioxaglate Hexabrix
Figure 4
non-ionic monomer
3:1=3
11
6
500-700
iohexol iopamidol iopromide ioversol
Omnipaque lopamiro Ultravist Optiray
Figure 5
non-ionic dimer 6:1=6 25 10 300 iodixanol
iotrolan Visipaque
Isovist
Values of viscosity (cP) and osmolality (mOsm/kg H2O) have been approximated to an iodine concentration of 300 mg I/ml. + are viscosity values for sodium salts. ++ are viscosity values for meglumine salts.

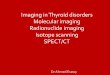
Figure 1. Transformation of an ionic monomer
(above) to a non-ionic monomer (below).
Figure2. Ionic monomer (ratio1.5).
2 ions in solution per 3 iodine atoms 3 iodine atoms per molecule
1 carboxyl group (-COO-) per molecule No hydroxyl group (-OH) except
ioxithalamate with one OH/molecule Intravenous LD50 for mouse
5-10 g I/kg mouse
The efforts to design less toxic contrast media were started in the 1920s and are still continuing. A major development occurred in the beginning of the 1950s when it was found that contrast media with three iodine atoms bound to a benzene ring had low toxicity (amidotrizoate Table 1, Fig. 2). A benzene ring with three iodine atoms is in contrast medium research defined as a "mer". A monomer, for example, contains one such three- iodinated benzene ring, while a dimer contains two such structures. In the 1960s a radiologist, T. Almen, proposed the synthesis of monomers and oligomers of non-ionic, tri-iodinated contrast media (Fig. 1). The first non-ioinic monomer was produced by the Norwegian contrast medium company, Nyegaard & Co (Today Nycomed Imaging AS).
Further factors that influence toxicity and water solubility are described below. Table 1 and Figures 2-5 show the most commonly us ed contrast media, their names, chemical structures, osmolality, viscosity and ratio between number of iodine atoms and number of contrast medium particles in an ideal solution.
Water solubility and toxicology Water is the most common molecule in the human body, both inside and outside the cells. In order to enable a high contrast medium concentration in extracellular water, high water solubility is necessary for contrast media in urography, angiography, etc. This water solubility is achieved in different ways by ionic and by non-ionic contrast media. Water is a polar solvent; the water molecules are electrically neutral (equal numbers of positive and negative unit charges within

the water molecule), but the positive and negative charges are distributed so that there is a surplus of positive charges (lack of electrons) at the site of the hydrogen atoms (which form positive poles) and a surplus of negative charges (excess of electrons) around the oxygen atom (which forms a negative pole).
lonic contrast media dissociate in water into electrically charged particles named ions. The positively charged ion may be a sodium ion or a meglumine ion. The negatively charged ion is the benzene derivative with three iodine atoms and a negatively charged carboxyl group. The ionic contrast media are water soluble because the positive and negative ions are attracted to the negative and positive poles of the water molecules.
Non-ionic contrast media are electrically neutral like the water molecules. The nonionic contrast media are water soluble because they contain polar groups (OH-groups, hydroxyl groups) which have an uneven distribution of electrical charges with excess electrons around the oxygen atoms (forming negative poles) and a deficit of electrons around the hydrogen atoms (forming positive poles). The electrical poles in the OH-groups of the contrast media are attracted to the electrical poles in the water molecules - thus achieving water solubility.
The only desirable effect of a contrast medium is to attenuate radiation. All other effects of the contrast medium in the body, regardless whether they cause clinical symptoms or not, are not desired. When these effects cause changes observable in laboratory tests or clinical symptoms they are deemed to be adverse effects. Different chemical structures have been designed to achieve high water solubility and this has resulted in contrast media with different toxicity.
The total toxicity of a contrast medium solution is the sum of the chemotoxicity of the contrast medium molecules, the osmotoxicity of the contrast medium solution and the ion toxicity - a surplus or deficit of various ions in the solution:
1. The chemotoxicity of a contrast medium molecule may depend on its effects on proteins in the extracellular space and/or in the cell membrane, and effects on cell organelles and enzymes by the small numbers of contrast medium molecules which go intracellularly. (The carboxyl ion in ionic contrast media is an example of a chemical structure with high neurotoxicity in the subarachnoid space. Therefore, ionic contrast media must not be used in myelography.)
2. Osmotoxicity. Ionic contrast media have a high osmolality per amount of iodine, because the iodinated and negatively charged ions (diatrizote, iothalamate, metrizoate) are accompanied by the non- iodinated positively charged ions (sodium ions, meglumine ions) (see also the section: "Osmolality ratio, below). The hypertonicity of the contrast medium solution causes fluid shifts from erythrocytes, endothelial cells and other structures. This induces pain in arteriography, dilatation of blood vessels with a fall in blood pressure and viscosity changes of the blood.

3. Ion-imbalance. When contrast medium instead of blood flows through blood vessels, a too high or too low concentration of different ions produce side-effects (ventricular fibrillation at coronary arteriography, influence on plasma proteins).
Osmolality and the ratio concept The ionic monomeric contrast media are highly hypertonic compared to blood. Blood has an osmolality of 300 mosmol/kg water and the ionic contrast media used in angiography have an osmolality of 1500-2000 mosmol/kg. The osmolality is proportional to the number of particles in a solution. The "ratio" of a contrast medium describes the proportions between its ability of being a "good" contrast medium (by attenuating X -rays) and its tendency to induce side-effects (by its osmotoxicity). You can calculate a theoretical ratio of a contrast medium as "the number of iodine atoms per volume contrast medium" divided by "the number of particles (contrast medium ions or contrast medium molecules) per volume contrast medium solution”.
The ionic monomeric contrast media have a ratio of 1.5 (3/2 = 1.5) (three iodine atoms per two water soluble particles [ions]). When there was a need to decrease the osmotic effects per amount of iodine, it was done by increasing the ratio, e.g. the number of iodine atoms/number of particles (Figs. 1 and 2).
Figure 3. Ionic dimer (ratio 3). 2 ions in solution per 6 iodine atoms
6 iodine atoms per molecule 1 carboxyl group (-COO-) per molecule 1 hydroxyl group (-OH) per molecule Intravenous LD50mouse 10-15 g I/kg
mouse

Figure 4. Non-ionic monomer (ratio 3). 1 molecule in solution per 3 iodine atoms 3 iodine atoms per molecule No carboxyl group (-COO-) 4-6 hydroxyl groups (-OH) per molecule Intravenous LD 50 mouse 15-20 g I/kg mouse
A non-ionic monomeric contrast medium that does not dissociate in water, has three iodine atoms per water soluble molecule and therefore ratio 3 (3/1 = 3) (Fig. 4).
The evolution of contrast media has continued and one of its goals has been to further reduce the osmolality of both the ionic and non-ionic media by making dimers of them. First the synthesis of a dimeric, ionic contrast medium, which has the ratio 3 (6/2 = 3) was made (Fig. 3). Later, in the 1980s and 1990s, dimeric non-ionic contrast media have been explored and these contrast media have such low osmolalities that electrolytes have to be added in order to make them iso-osmotic with blood (Fig. 5). They have a ratio of 6 (6/1 = 6).

Figure 5. Non-ionic dimer (ratio 6). 1 molecule in solution per 6 iodine atoms
6 iodine atoms per molecule No carboxyl group (-COO-)
More than 8 hydroxyl groups (-OH) per molecule
lntravenous LD50 mouse 20 g I/kg mouse
Different types of contrast media The strategies above about handling water solubility, chemo- and osmotoxicity have led to four different types of iodine contrast media for urography, angiography and computerized tomography (Figures 2-5). 1. Ionic monomeric contrast media 2. Ionic dimeric contrast media 3. Non-ionic monomeric contrast media 4. Non-ionic dimeric contrast media
As the ability of the iodine atom to attenuate X -rays is independent of the organic molecule in which it is chemically bound, a comparison between side-effects, toxicity, osmolality, viscosity or price of different contrast media must always be made in iodine equivalent amounts and concentrations. (It is thus important to relate adverse effects, price, etc., to the desired effect of a contrast medium, i.e. its attenuation of X-rays, which is proportional to the amount of iodine.
Contrast media kinetics The four contrast medium groups above have all high water solubility, low plasma protein binding, almost exclusive distribution to the extracellular space and minor intracellular distribution. The size of the molecules enables them to pass through the glomerular basement membrane. They are to a very small extent reabsorbed or excreted by the tubular cells and are quantitatively handled by the kidneys like Inulin. The media can therefore be used to determine glomerular filtration rate (GFR). Their half-life in plasma is dependent on the

GFR. At normal GFR they have a half-life of 1.5-2 h. If GFR is decreased by a factor 2 or 4, their plasma half-life increases by a factor 2 or 4, etc.
A small amount (at normal GFR less than 2 %) of these contrast media is excreted via the biliary system. The high-osmolar media (ratio 1.5) give in iodine equivalent doses a larger osmotic diuresis than the ratio 3 and ratio 6 media. Therefore, the ratio 1.5 media have a lower urinary concentration than the ratio 3 and 6 media.
After a rapid intravenous bolus injection of contrast medium an almost undiluted volume of contrast medium reaches the heart where it is mixed with blood and this "blood-contrast medium bolus" passes through the pulmonary vascular bed and reaches the left side of the heart and the aorta and its branches. There is rapid contrast medium diffusion through most capillary membranes from the blood mainly into the extracellular space as the media have very low binding to plasma proteins and a very small intracellular distribution. For only a few minutes after a bolus injection, the media may be regarded as representing the distribution of the blood and blood vessels in the body. This fact makes it possible to detect necrotic tumors and cysts which are not vascularized and therefore contain less contrast medium-filled blood than the surrounding normal tissue. Likewise, it is possible during the same period to detect tumors or inflammatory processes that are hypervascularized because they contain more contrast medium filled blood than the surrounding normal, less vascularized tissues.
In the brain, the normal blood-brain-barrier prevents the contrast media from escaping from the blood out into the brain parenchyma. In areas where the blood-brain barrier is damaged due to a tumor or an inflammatory process, contrast media may leak from the blood into the brain parenchyma. Regions with an injured blood-brain-barrier may thus be detected at contrast medium enhanced computerized tomography due to the higher contrast medium concentration in those regions than in the surrounding normal brain parenchyma.
Hematological effects When contrast medium is injected into the blood stream, it comes in contact with blood cells, endothelium and various proteins of the coagulation cascades.
The red blood cells are influenced by the osmotic effects of a large contrast medium bolus. This occurs particularly with the high osmotic ratio 1.5 media, which draw water out of the cells and deform them. Red blood cells thereby become rigid and lose their normal deformability, which tends to decrease their flow through small vessels, such as capillaries.
It is known that vascular endothelium may be injured by hyperosmolar solutions, such as solutions of ratio 1.5 contrast media. Damaged endothelium may elicit thrombus formation on it, particularly when a high osmotic contrast medium is used in those phlebographic techniques which cause prolonged contact between the medium and the endothelium. The new ratio 3 and ratio 6 contrast media

have lower osmolality than the ratio 1.5 media and therefore cause less damage to the endothelium and are thereby less prone to promote thrombus formation on it. They are in this context less procoagulant than the ratio 1.5 media.
All contrast media when mixed with blood in a test tube or in an angiography catheter are anticoagulants. The old, more toxic ratio 1.5 contrast media are in this context stronger anticoagulants than the new, more biocompatible, less toxic ratio 3 and ratio 6 media. Inside an arteriography catheter with end- and side-holes, the anticoagulant effect of heparinized saline or solutions of ratio 1.5, ratio 3 or ratio 6 contrast media, becomes very small, because even a few seconds after the injection of contrast medium or heparinized saline into the catheter, the injected solution is already contaminated by blood. Therefore, catheters must be flushed at least every second minute so that blood does not stay within the catheter lumen or in the holes of the catheter and coagulate there, independent of what contrast medium or flushing fluid that has been used.
Lungs When large intravenous bolus injections (urography, pulmonary angiography, intravenous contrast enhancement in computerized tomography, etc.) are performed, the lung is the first organ, after the heart, to be reached by the contrast medium bolus. When high-osmotic contrast medium is injected, there is a steep rise in pulmonary arterial pressure, and the higher the osmolality, the higher the increase in pressure due to the induced rigidity of the red cells. The increase in pressure has been shown to be particularly dangerous to patients with pulmonary hypertension and these patients should not have intravenous bolus injections of ionic ratio 1.5 media of high osmolality. Also patients with decreased lung function should have contrast media with low osmolality in order to reduce the adverse effects on the pulmonary circulation. Furthermore, the release of histamine and other vaso-active substances, when contrast media activate the large number of mast-cells in the lungs, is considered to be one of the explanations for the higher frequency of some adverse reactions (vomiting, urticaria) following intravenous injection of contrast media than following intra-arterial injections of the media. This is another reason to use low-osmotic contrast media when large intravenous doses of the media are considered.
Heart In selective coronary arteriography high-osmolarity contrast media (ratio 1.5) induce a larger reduction of the contractile force of the heart than less hypertonic (ratio 3) or plasma-isotonic contrast media (ratio 6). If, in spite of this, ionic contrast media are chosen for coronary arteriography, those containing sodium ions in the same concentration as plasma should be used due to their lower risk of inducing ventricular fibrillation compared to the pure meglumine salts of the ionic media. It is also possible that adverse effects on the heart from the non-ionic media can be further reduced by using media with optimized electrolyte content and with oxygen saturation of the contrast medium solution.
Peripheral vascular bed In femoral arteriography with a contrast medium concentration around 300 mg

I/ml, the ratio 6 media are isotonic with plasma, while the ratio 1.5 media have 5 times the plasma osmolality (1500 mOsm/kg water) and the ratio 3 media have osmolalities in between. Some adverse effects of the media in femoral arteriography parallel their osmotoxicity so that ratio 1.5 media produce most pain, most feeling of warmth and most vasodilatation while the ratio 6 media produce least pain and vasodilatation and the ratio 3 media produce something in-between. Chemotoxicity is also involved in vasodilation, because sodium chloride solutions made isotonic with ratio 1.5, ratio 3 or ration 6 contrast media produce less vasodilation than these media.
Subarachnoid space In the subarachnoid space only those contrast media should be used which do not contain carboxyl groups and furthermore have hydroxyl groups evenly distributed throughout the contrast medium molecule.
Animal experiments have shown that those media have the lowest risk of inducing seizures. You may find the media intended for subarachnoid use among the nonionic monomers and dimers. Please, look at the label of your contrast medium vial and DO NOT INJECT into the subarachnoid space those media which are NOT intended for subarachnoid use. By exchanging ionic monomers for non-ionic monomers the osmolality of the contrast medium solution was reduced by a factor of 2 while the total toxicity in the subarachnoid space of animals was reduced by a factor of 30. This decreased toxicity cannot be due to reduction in osmotoxicity alone; it must also be due to reduced chemotoxicity achieved by the elimination of carboxyl groups and by the introduction of hydroxyl groups. You may regard the non-ionic contrast media as surrounded by a cloud of water molecules which by electrostatic forces are attracted to the contrast medium molecules so that the body might recognize the latter as a cloud of water molecules with a low toxicity.
Kidneys In urography there is a need for a high iodine concentration in the cortex (cortical nephrogram) in order to analyze cortical pathology and the size and margins of a kidney. A high iodine concentration in the renal pelvis and ureter (pyelogram) is desired to detect processes in the calyces, renal pelvis and ureters. Different mechanisms regulate the contrast medium concentration obtained during urography in the cortex and in the renal pelvis. The quality of the cortical nephrogram depends on the contrast medium concentration in the cortical blood vessels and in the primary urine in Bowman's space and proximal tubules. The pyelogram depends only on the contrast medium concentration in the final urine and is independent of the contrast medium concentration in the blood vessels and primary urine.
In selective renal arteriography the ratio 3 contrast media give 10 to 100 times less proteinuria than the ionic ratio 1.5 contrast media. In cell cultures the tubular cells have a greater tolerance towards non-ionic ratio 3 contrast media than towards ratio 1.5 media. This beneficial property of the ratio 3 media is

counteracted by their higher concentration in the tubular urine than ratio 1.5 media.
There are many reports on contrast medium induced renal insufficiency. The larger the contrast medium dose and the lower the pre-injection glomerular filtration rate (GFR), the larger the risk of this contrast medium nephropathy. Patients with a markedly decreased GFR due to a long lasting diabetic nephropathy are at particular risk of developing contrast medium nephrotoxicity. The clinical manifestations of this may vary. There may be a transient rise and later normalization of serum creatinine as the only sign of toxicity; there may be a transient oliguria or anuria which may require dialysis a few times before complete or partial return of function; there may, in the worst cases, be a need for chronic dialysis or renal transplantation. There are many reports on patients with reduced GFR showing that the lower the contrast medium dose and the better the water balance before and after the contrast medium injection, the smaller the risk of inducing further renal insufficiency. There are also data indicating that the use of calcium blockers might reduce the risk of contrast medium induced renal insufficiency. Large clinical trials have shown a smaller risk of contrast medium nephrotoxicity when non-ionic ratio 3 media are used instead of ionic ratio 1.5 contrast media, while some smaller clincial trials have failed to show this advantage of non-ionic ratio 3 media.
Unpredictable, acute reactions Unpredictable reactions to contrast media and other pharmaceuticals may occur on one occasion, but not on another occasion, despite injection of the same substance in the same dose in the same patient. The symptoms may be those of an allergic type I reaction. The majority of the contrast medium reactions is not caused by an antigen-antibody reaction and they often occur without previous exposure to the contrast medium. In fact, there are only three reports of antibodies to contrast media. The majority of contrast medium reactions are called "pseudoallergic" because they cause exactly the same clinical symptoms and require the same symptomatic treatment as true allergic reactions, but they are not initiated by an antigen-antibody reaction. Instead they occur by activation of immunologic effectors through other mechanisms. Reactions with minor symptoms are named pseudo-allergic or allergoid and those with more serious symptoms pseudo-anaphylactic or anaphylactoid.
Contrast media (and other pharmaceuticals) may by chemotoxicity, hypertonicity or ion toxicity trigger immunologic effects by at least two mechanisms:
1. Interaction with cell membranes releases vasoactive substances such as histamine and platelet activating factor (mast cells), serotonin (platelets), leucotrienes (mast cells, leukocytes), thromboxane A2 (platelets, leukocytes ) and prostaglandins (endothelium).
2. Interactions with biomolecules of the complement, kinin, coagulative or fibrinolytic systems may activate these systems creating bradykinin, other vasoactive substances and anaphylatoxins and macroproteins which form

channels through cell membranes causing cell lysis. Erythrocytes, leukocytes, lymphocytes and mast cells all contain complement receptors so that products of the activated complement system can cause cell membranes to release substances according to mechanism 1.
The release or creation of vaso-active substances according to mechanisms 1. and 2, may cause the same acute symptoms as those seen after a true allergic type-I-reaction when the release of vaso-active substances is caused by an antigen-antibody reaction. Whether the patient's re action is of pseudo-allergic (common) type or true allergic (uncommon) type does not matter because in the acute situation the treatment of the two types of re action is the same.
Contrast medium reactions can be divided into - mild (no treatment necessary) - moderate (treatment necessary, but no intensive care) - severe (life-threatening, intensive care necessary)
The ratio 1.5 contrast media cause mild adverse reactions in up to 10% of the patients and severe reactions in a frequency of 1 :900-1 :3000 and a mortality rate of approximate magnitude 1:50 000-1:100000. The new low-osmolar contrast media, especially the non-ionics, have a lower risk of pseudo-allergic reaction. In conclusion, we do not know the mechanisms behind these contrast medium reactions. The present opinions are that they are, in the majority of cases, not caused by an antigen-antibody reaction, not caused by the presence of iodine atoms in the contrast medium molecules and not caused by shell fish allergy.
Risk factors The statistical chance of a pseudoallergic reaction to a planned contrast medium injection increases in the presence of the following risk factors: an earlier pseudo-allergic reaction to contrast media or other pharmaceuticals, bronchial asthma, cardiac disease, the presence of any type of allergy (including shell fish allergy). The larger the dose of contrast medium, the larger the risk of an acute reaction. The larger the number of risk factors, the greater the readiness for immediate treatment of an acute reaction should be.
Treatment of adverse reactions Vasovagal reactions (falling blood pressure and bradycardia) are treated with the Trendelenburg position and intravenous fluids (normal saline or Ringers lactate). If hypertension persists, atropine 0.5-1.0 mg intravenously should be administered. If fluids and atropine are ineffective, dopamine 5-10 microgram/kg/min. intravenously may be considered.
Below is a scheme of treatment of contrast medium reactions. It includes symptomatic treatment of the effects of various vasoactive substances produced by the mechanisms of a pseudoallergic or a genuinely allergic reaction as earlier described. The symptoms are treated in the same way irrespective of whether they have true allergic or pseudo-allergic etiology.

Treatment of radiographic contrast medium induced reactions SC=subcutaneously, IM=intramuscularly, IV=intravenously
1. Acute allergoid (allergic) reaction: General urticaria and/or Quincke edema (sometimes in combination with headache, vomiting, abdominal pain -(diarrhoea), asthma-rhino-conjunctivitis) Treatment a) Epinephrine 0.5 mg (1 mg/ml) se b) Oxygen 2-6 1/min c) Diphenhydramine 50 mg IM
2. Anaphylactoid (anaphylactic) reaction: Symptoms like acute allergic reaction and: tachyeardia, fall in blood pressure, paleness Treatment a) Epinephrine 0.3-0.5 mg (0.1 mg/ml) IV b) Oxygen 2-6 l/min intravenous line should be arranged
3. Anaphylactoid (anaphylactic) shock: Symptoms resembling anaphylactic reaction, but more dramatic with: unconsciousness - status asthmatics - respiratory arrest - circulatory collapse - cardiac arrest Treatment a) Epinephrine 0.3-1.0 mg (0.1 mg/ml) IV b) Oxygen 2-6 l/min c) Hydrocortisone 250 mg IV d) Intubation + ventilation
In patients with a high risk of an acute reaction to contrast medium: 1. Re-evaluate the indication for the investigation and discuss alternative investigations with the referring physician 2. Choose a non-ionic monomer as the contrast medium. Do not choose the same as before if the patient earlier had a moderate to severe reaction on that non-ionic medium 3. If the previous reaction was: a) Mild - consider performing the investigation without premeditation b) Moderate - premeditation according to below c) Severe - premeditation according to below and have an anaesthesiologist standing by or perform the investigation under general anaesthesia
Premedication Elective investigation 1. Prednisolone 50 mg (10 tabl) orally 12 and 2 hours before the investigation 2. Clemastin 1 mg/ml, 2 ml 1M 1 hour before the investigation
Emergency investigation 1. Water soluble hydrocortisone, 200 mg IV immediately and thereafter every fourth hour until the investigation is terminated 2. Clemastin 1 mg/ml, 2 ml 1M 1 hour before the investigation

Barium contrast media Preparations of barium sulphate contain a suspension of practically insoluble barium sulphate particles with a size of 0.1-0.3 mm. The individual particles in this suspension are irregular aggregates of crystals of barium sulphate. In addition, the suspension contains additives (pectin, sorbitol, agaragar, carboxy-methyl-cellulose) which are partly bound to the surface of the particles and determine their electric al charge, and also determine the pH of the suspension and its stability and viscosity. All these factors determine the tendency of the suspension to sediment and to foam and to adhere to the mucosa during double contrast examinations. The barium sulphate particles remain in the intestinal lumen, are not absorbed from the intestine and are therefore non-toxic. Barium ions are toxic, but the extremely small amounts of barium ions in solution in the suspension, available for intestinal absorption, are regarded as having no practical importance.
Barium sulphate is available in two forms. One is a powder which is mixed with water before use (BarytgenR, BarisperseR). The other is a ready-to-use suspension for specific diagnostic purposes (MixobarR esophagus, colon).
Two levels of barium concentrations are clinically used - one for single contrast and one for double contrast.
For single contrast the intestinal lumen is filled with a low density barium suspension (0.5-1 g barium sulphate/ml suspension).
For double contrast studies (when barium sulphate covers the mucosa with a thin layer and the intestinal lumen is distended with air) a suspension with high density is used (2.0-2.5 g barium sulphate/ml suspension.
Adverse effects Oral barium sulphate may accidentally be aspirated into a bronchus or may, in the presence of gastrointestinal perforation, penetrate into the mediastinum or flow into the peritoneal cavity. Barium in the bronchial tree is less harmful than aspiration of food. It often disappears quickly and seldom causes any problems. In the mediastinum and peritoneal cavity barium sulphate may produce adhesions and/or granuloma. The pass age of barium sulphate and of food, intestinal and pancreatic enzymes and faecal matter through a perforation is considered more damaging than the passage of barium sulphate alone. This is supported by animal experiments, which also suggest that pure barium sulphate induces less damage than barium sulphate containing additives which stabilize the suspension.
Constipation may follow oral barium sulphate and can be treated with fluid and laxatives. If the equipment used during a barium sulphate enema damages the anorectal mucosa, the barium sulphate may leak into the retroperitoneum. If the enema equipment perforates a blood vessel intravascular embolization of barium sulphate may occur. This can embolize the liver via the portal vein, or the barium

sulphate may reach the pulmonary circulation. Most patients who have experienced an intravascular infusion of barium sulphate have died.
If perforation of the gastrointestinal tract is suspected, you must consider performing the gastrointestinal investigation with a water soluble iodine contrast medium. If there is a perforation and contrast medium leaks into the mediastinum or peritoneal cavity, the water soluble contrast will be resorbed into the blood stream and excreted through the kidneys and there is no risk of granuloma formation. If a water soluble gastrointestinal contrast medium is used, it should preferably be a ratio 3 or 6 contrast medium in order to avoid undesired osmotic dehydration by the hypertonic ratio 1.5 media; this is particularly important in children. Similarly, when an orally ingested contrast medium has entered the lungs via a tracheo-esophageal fistula, the ratio 3 and 6 media will draw less fluid into the lung than the ratio 1.5 media.
Organ specific contrast media - lymphography Lymphography is an investigation that has decreased in use in recent years. For lymphography we use an oily contrast medium, Lipiodol Ultrafluid, consisting of iodinated ethylesters of fatty acids from poppy seed oil. The contrast medium is injected directly into a dissected lymphatic vessel, normally simultaneously in both lower extremities. The water insoluble oil is retained only in those lymph nodes which receive lymph from the injected lymphatic vessels. On the radiographic images the contrast medium can be detected within the lymph nodes from a couple of months to several years after the injection. During this time repeated radiological examinations can give information about the status of the nodes without further injection of contrast medium.
Adverse effects The contrast medium may give an inflammatory foreign body reaction within the lymph node. During lymphography the injection rate should be controlled and the dose of the contrast medium adjusted to the smallest possible amount in order to minimize oil embolization to the lungs via the thoracic duct or other anastomoses between lymphatic vessels and veins. Oil embolization to the pulmonary capillaries can cause a 60% reduction of the diffusion capacity of the lungs after lymphography and decreased lung function is a relative contraindication to lymphography. Sometimes, a chemical pneumonitis occurs 1-7 days after lymphography. The mechanism is thought to be enzymatic breakdown of contrast medium in the lungs. The split products may then damage the vessel endothelium and the membranes of the alveoli with hemorrhages and exudation as a result. The mortality of lymphography is approximately 1 :2000.
Organ specific contrast media - biliary media
Oral contrast media

Iocetamic acid, iopanoic acid, salts of ipodate or tyropanoate are examples of cholecystographic contrast media, which are given orally. The contrast medium is absorbed in the intestines and is carried to the liver where it enters the hepatocytes. Here it is conjugated with glucuronic acid, which increases its water solubility and decreases its fat solubility. The conjugated contrast medium is excreted into the bile canaliculi. When the hepatic and cystic ducts are patent the contrast medium flows into the gallbladder in which it is concentrated by the resorption of water through the gallbladder wall. The high binding affinity of the media for albumin decreases their renal excretion and increases their hepatic excretion. In optimal pharmacokinetic circumstances the gallbladder is filled with contrast medium about 10-19 hours after its oral ingestion. Within that period different media produce their maximal gallbladder opacification at different intervals, for instance, ipodate at 10 hours and iopanoic acid at 14-19 hours.
Different mechanisms may lead to a low contrast medium concentration in the gallbladder, which on the radiographic examination results in a non-visualized gallbladder. 1. Diarrhoea caused by the intake of the contrast medium, with excessively fast passage through the intestines preventing sufficient absorption for visualization of the gallbladder. 2. Hepatic dysfunction with decreased hepatocyte uptake and biliary excretion of the medium. 3. Mechanical obstruction of bile drainage into the gallbladder (biliary calculus, tumor). 4. Decreased ability of the gallbladder wall to concentrate bile (chole-cystitis ). 5. The water soluble glucuronic acid conjugated contrast medium may diffuse back into the blood through an injured gallbladder wall (chole-cystitis ). 6. Glucuronidase activity of bacteria in the gallbladder in chole-cystitis may deconjugate the contrast media and the (now) fat soluble contrast medium is resorbed through the gallbladder wall.
Unpredictable pseudo-allergic reactions may occur at cholecystogrpahy. A serious complication after cholecystography is renal failure with oliguria-anuria. The mechanism of the latter is not clear. The frequency of severe complications after cholecystography is 1:20 000 and the mortality rate is 1:40 000.
Intravenous contrast media For intravenous cholangiography the meglumine salts of iodipamide or iotroxic acids are used. The intravenous biliary contrast media are transported in blood bound to albumin. This protein bound contrast medium is not excreted in urine by glomerular filtration, but competes with bilirubin for binding sites on albumin. Intravenous cholangiographic media, that have a high water solubility, are not conjugated in the liver but are excreted unchanged in the bile canaliculi in such a high concentration that the intrahepatic bile ducts and common bile duct are visualized on the roentgenograms; the cholegraphic media do not require concentration by the gallbladder. After intravenous injection of the medium the

biliary tract is visualized 1/2-2 hours later. No reabsorption of the cholangiograhic media occurs in the intestines.
Large series have shown a mortality rate of cholegraphy of 1:5000-1:8000 and severe complications in a frequency of 1:300-1:600. The latter are most often circulatory collapse and acute renal insufficiency. Presently, the use of intravenous cholegraphy is decreasing. A total dose of 5-6 g iodine and an infusion time of 30 minutes are most commonly used. Sometimes, in cases of decreased liverfunction an infusion time of 5-8 hours is utilized.
Colloid intravascular contrast media Blood pool contrast media are presently being investigated by different research groups. Blood pool contrast media are defined as media which after intravenous injection leave the blood slower than the presently used monomers and dimers of ionic and non-ionic iodinated media. These blood pool media would have the advantage that after an intravenous bolus injection in, for example, computed tomography, they would remain inside the large arteries and veins and show their morphology for a longer period than the presently utilized media. To achieve these effects iodinated macromolecules and iodinated suspensions have been tried. Such colloidal contrast media are often removed from the blood by the phagocytosing cells of the reticulo-endothelial system. Depending on the particle size of the contrast medium its major site of deposition will be in the bone marrow, spleen and/or liver. Some of these contrast media have successfully been used in early clinical investigations to detect liver metastases as these contrast media may reach a higher concentration in the normal hepatocytes and/or Kupffer-cells than in the cells of primary liver tumors or liver metastases.
Atoms with a higher atomic mass than iodine as contrast media Atoms with a higher atomic mass than iodine atoms attenuate more X-rays per atom than the iodine atom. Gadolinium, tungsten and lead are examples of such atoms. Attempts have been made to covalently bind these atoms in organic molecules or to include cations of these heavy atoms in water soluble chelates. So far, there has been no success in synthesizing molecules with toxicity as low as that of the iodine atom in modem contrast media. Therefore, such contrast media have not yet been introduced into clinical use.
Torsten Almén and Peter Aspelin
Printer-friendly version Bookmark This Page
Translate page to (By Google):

Radiophysics Introduction
Medical imaging plays a central part in the diagnostic examination of patients, as well as in invasive radiological procedures, which are increasingly dependent on accurate diagnostic information. Such information can be gained by applying transmitted, emitted or reflected electromagnetic radiation or mechanical vibration (ultrasound). The following physical phenomena are the basis of modern imaging: - X-rays are absorbed in tissue (X-ray examination), - radio frequency radiation is yielded by the excitation of odd atomic nuclei in a magnetic field (magnetic imaging based on nuclear magnetic resonance, NMR), - radioactive isotopes concentrated in certain tissues emit gamma radiation (nuclear medicine imaging or isotope imaging), - high frequency beams of compression and rarefaction are reflected back towards a transmitter sensor (ultrasound examination), - infrared radiation is emitted spontaneously by tissues (infrared imaging, thermography).
All of these methods except ultrasound are based on electromagnetic (em-) radiation in different energy domains. Ultrasound imaging is based on the detection of vibration, which is generated in a piezoelectric crystal. Isotope, ultrasound, and magnetic examinations were developed into useful imaging methods in the seventies and eighties, whereas X-radiation was discovered one hundred years ago in 1895.
Those types of radiation (X, gamma, beta and alpha radiation) which can impart more energy than light (2 - 4 eV), have the capacity to ionize atoms and dissociate molecules and therefore cause biological damage. The use of non-ionizing methods like ultrasound and magnetic resonance should generally be preferred, because of their inherent safety without taking account of their other advantages.
X-ray imaging methods can be grouped in the following way: - radiography with a screen and film or a cassette (about one hundred years old), and today with a digital cassette - fluoroscopy or transillumination (from the beginning of the century) with an image intensifier and a television camera tube which began in the sixties, and - computerized axial imaging methods (which began in the seventies).
Imaging methods can also be grouped according to whether a volume of tissue or a thin slice of tissue is imaged. In a conventional X-ray examination a 3-dimensional object is projected into a 2-dimensional image. Shadows of different organs are summated on film. The entire tissue volume is exposed, which means that much scattered radiation is generated which degrades image quality, particularly by reducing contrast.

In axial imaging (e.g. computed tomography, CT) radiation is directed only into a thin disc or slice of tissues. Conventional tomography is an older method, whereby shadows of objects outside the focal plane are blurred by synchronous movement of the X-ray tube and screen-film combination.
Computed Tomography (C T) was invented in 1973. A computer was used for the first time to measure, analyze and display an axial image in digital units. The greatest advantage of this method is good contrast resolution. Axial imaging is also used in magnetic resonance imaging and in nuclear medicine to a lesser extent. Ultrasound imaging is also restricted to one plane, but an image is not formed with reconstruction techniques like in the other axial modalities. Different imaging methods based on different physical principles therefore project different views of the anatomy and physiology of organs.
Digital computers play a pivotal role in all modem imaging methods. They will assume even more importance in the nineties both in digital bone and thorax imaging as well as in converting all image information (measurement, display, archiving, transmission and communication) into digital form.
The interactions of different energy forms with matter are scrutinized in this chapter, as well as the physical principles underlying imaging methods. The construction, function, and use of X-ray generating devices, the biological consequences of radiation, and radiation protection, and factors affecting image quality are also discussed.
Aaro Kiuru
Printer-friendly version Bookmark This Page
Translate page to (By Google): Radiophysics Interactions of radiation with matter and radioactivity
Matter and radiation The smallest unit of radiation, a photon or a quantum, arises in matter, when a nucleus, an atom or electrons of an atom, is affected by a disturbance coming from outside. In order to understand the physical principles of imaging methods and the technical aspect of devices, one must have knowledge of the atomic

structure of matter and of those changes which occur when an atomic microsystem is disturbed (e.g. a tungsten nucleus in an X-ray tube).
Figure 1. Energy level-diagram of the electrons of a tungsten atom. The binding energy of each
shell is shown. This is the minimum energy, which an incoming electron or
gamma quantum must have to be able to ionize the atom. Excitation with a smaller amount of energy only raises an electron to one of the higher levels provided that a vacancy exists. Two characteristic X-ray
quanta are also shown.
Fig. 1 shows the orbits or shells K, L, M etc. of tungsten. These shells are saturated with electrons up to the N-shell and even O- and P-shells are partly filled. It is normal for electrons to be situated in the lowest available orbits, in other words that their energy be as small as possible. The situation is different at higher temperatures, in radioactive substances and generally, when an atomic microsystem is disturbed. This happens for instance when an incoming electron crashes into the anode of an X-ray tube or light is produced from the heated filament of a light bulb. Microsystems become ionized or excited in these ways.
Once excited, an electron is raised from a low energy shell (e.g. the K-shell) to a higher energy shell. An excitation state is discharged by the emission of characteristic X -radiation, when simultaneously an electron from the L-shell, or less likely the M-shell, falls down to the K-shell. The energy difference between these shells in question (59 keV Kα or 67 keV Kß) is liberated as a monochromatic quantum. This filling up of an electron hole in a shell is followed by a series of similar events in higher orbits with smaller and smaller energy transfers until the system is returned to its stable state. All this happens very quickly, in a considerably shorter time period than a milliardth of a second.
Radiation is divided into two principal components: 1. particle radiation, of which only the electron (and positron, the positive electron) has importance in imaging methods, and 2. electromagnetic (em-) radiation. Its basic quantity, a quantum or a photon moves with the speed of light and lacks mass.
It is accepted in modem physics that a photon can behave as a particle or as a wave. The properties of radiation can therefore be characterized with three concepts; energy (unit being an electron volt eV, keV etc.), frequency (Hz, MHz

etc.) and wavelength (cm etc.). Frequency is directly proportional and wavelength inversely proportional to energy.
When an X-ray spectrum is generated in an X-ray tube the penetrating properties and to a lesser extent the intensity of radiation are determined by the high voltage (kilovolt kV or kVp). Em-radiation varies from very low-energies (low frequency or high wavelength) to high energies. Due to historical reasons different names for separate domains of the em-spectrum are in use, but in fact they refer to the same phenomenon, i.e. electromagnetic radiation: - X-ray, ultraviolet- and visible light arise from changes in electron shells, - infrared radiation is a consequence of heat liberated by the motion of atoms and molecules, - radio waves arise from the motion of electrons in a conductor and also from changes in nuclear orbit and spin, etc., - gamma radiation originates as a consequence of changes in the excitation of a nucleus
The different ways with which a photon interacts with matter are greatly dependent on energy. Different photon energies are utilized in imaging
Figure 2. X-ray quanta are absorbed heterogeneously in different tissues, most occurs in bone and
contrast media and least occurs in air-containing spaces like lungs (Fig. 9). The transmitted primary quanta and a significant part of the scattered, through lead grid penetrated quanta,
expose the film. Details of the object are seen in the image if large enough intensity differences (contrast, Fig. 10) have been produced by the distribution of X-rays.
methods to get information from tissues, but the direct in vivo utilization of particle radiation (electrons) in medicine happens only in radiotherapy. On the other hand, ultrasound means vibration in matter. It is transmitted through tissues at the speed of sound (compared with the much higher velocity of light). Ultrasound is not radiation.
Interactions of X-rays and gamma rays with matter X-ray imaging is the imaging of shadows (see Fig. 2). Different tissues allow the transmission of different amounts of quanta, which are projected onto the image plane. This is either a screen-film-combination, an image intensifier or a sensor, for instance in a CT unit. Radiation must therefore possess two properties for the formation of a radiograph or an X-ray image:

1. Photons must penetrate tissues to a sufficient degree (resulting in a radiation dose). 2. Quanta should be attenuated differently in different tissues (resulting in image contrast).
When X-rays are used, external radiation penetrates tissues and the quanta are detected on the other side of the patient. In nuclear medicine imaging, photons from activity distributions within body tissues are emitted.
Figure 3. The interactions of photons and electrons with matter. Pair production is possible only at
higher energies than 1.022 MeV. It has no importance in X-ray and nuclear medicine imaging, but plays an important role in radiotherapy.
In the latter case, there is a prerequisite that the target object has collected more (or less) activity than organs in the background.
The interactions of X-rays and gamma rays with tissues are the same. Their mode of production is, however, different. A gamma quantum comes from de-excitation of a nucleus and its energy therefore has a specific value. In other words, gamma radiation is monochromatic (different nuclei decay of course with quanta of different energies). On the other hand, an X-ray spectrum consists of quanta with energies between a maximum and minimum value (polychromatic radiation). These limits are determined by the high voltage and filtration of the tube (see X-ray Generator and X-ray tube and Fig. 5).
In the other types of em-radiation quanta have similar interaction properties. Light and infrared radiation for instance penetrate tissues only in small amounts. Infrared radiation, as well as high frequency radiation, penetrates matter to a certain degree, but high spatial resolution is not possible. With infrared radiation it is possible to detect heat producing phenomena only in the vicinity of the skin surface. The situation is somewhat different in magnetic resonance imaging, where tissues are stimulated with radio waves in a strong external magnetic field. Fig. 3 shows the interactions of photons with matter in the energy domains utilized in X-ray and nuclear medicine imaging, as well as in radiotherapy. The figure also shows the interactions of electrons. All phenomena

Figure 4. Probabilities for photoelectric absorption and Compton scattering, (these phenomena are
schematically inserted in the figure with the diameters of an average atom and a nucleus) in various elements and at various energies. On the line in the picture the probabilities are
equal. Scattering occurs therefore very frequently in soft tissues (atomic number approximately 7,5). Egamma' Ebind and Ekin mean the energy of the incoming quantum, the
binding energy of the shell and the kinetic energy of the electron.
described in the figure are simultaneously possible with different probabilities, except pair production (which occurs in radiotherapy) which requires a minimum energy. Each interaction of a photon gives energy to one or more electrons. High-energy electrons are then able to ionize and excite atoms and dissociate tissue molecules. Radiation dose, so characteristic of ionizing radiation is closely connected to these so called secondary electrons.
Photoelectric absorption and Compton scattering are the important photon interaction phenomena in the diagnostic energy domain of 15-500 keV (Fig. 4). In X-ray and isotope examinations, so-called coherence scattering is of little importance and does not need to be considered. The former phenomenon is an absorption event, at which a photon gives all its energy to an electron, frequently in one of the inner atom shells. This photoelectron is slung from the atom with kinetic energy equal to the original energy of quantum reduced with the binding energy of the shell.
In Compton scattering a photon scatters (changes its direction) with a reduction in energy caused by giving part of its energy to an electron. The relationship between photoelectric and Compton phenomena varies so that in low atomic weight substances, such as soft tissues (and in all matter at high energies), scattering happens much more often than photoelectric absorption (Fig. 4). The frequency of occurrence of these two phenomena is the reverse at low energies and particularly in heavy substances (i.e. in protective layers like lead apron), where quanta are almost entirely absorbed.
Depending on the thickness of the object, a fraction of the number of primary photons is able to penetrate through tissue in the original direction. The remainder is stopped in tissue. Effects of radiation in tissues are later described

incorporating such concepts as absorbed dose and dose equivalent (Radiation protection and patient dose).
Fig. 3 shows one photon and its path through matter. But in an X-ray examination nearly parallel quanta are coming in very great quantities from the focus of the X-ray tube. The number of quanta, i.e. the intensity of radiation (quantalcm2 s) diminishes as the radiation penetrates more deeply through matter. In addition to the previous description of absorption and scattering phenomena, the effects of radiation can also be described statistically as a great number of quanta (the magnitude of 1012 quanta hit the patient's skin during the creation of an X-ray image). It is therefore postulated that radiation is attenuated which implies two things; 1. photons are absorbed in electron shells, and 2. photons are deviated from their original direction i.e. they are scattered.
Attenuation follows the exponential function I = Io exp -x here Io is the incoming and I the transmitted intensity of radiation, x is the thickness of the tissue and is a coefficient of attenuation. is a constant and characteristic of every element and every combination of elements, in other words characteristic of substances and tissues. It depends strongly on radiation energy and other factors.
Interactions of electron; X-ray spectrum from X-ray tube Fig. 3 shows that an electron with kinetic energy excites and ionizes atoms and dissociates molecules in matter. When kinetic energy increases, this also increases the probability of a braking radiation interaction. This
Figure 5. Braking radiation is generated in the anode of an x-ray tube. In medical imaging the energy
of the incoming electron may vary between 15-200 keV (see also text of Fig. 8).
phenomenon means that when a negatively charged electron passes a positively charged nucleus, the former changes direction and loses part of its energy as an em-radiation quantum (Fig. 5). The nearer the electron comes to the nucleus, the greater the change in direction and hence the greater the amount of energy loss. The quantum can gain any amount of energy from the maximal energy of electron (a straight hit) to the energy of a light photon or infrared photon (that is in

the range of a few e V). The latter events are the most common. Therefore, the number of low-energy photons inside the anode is greater than the number of high-energy photons (the upper curve in Fig. 5). This makes the anode surface glow, and there is a risk that the anode can even melt under excessively long exposures.
The lower curve in Fig. 5 depicts the quantum radiation spectrum used in patient examinations. It is worth remembering that the secondary electron set in motion by a quantum is particularly important when considering radiation biology and patient dose.
Interactions in a magnetic field In a magnetic examination a patient on the examination table is exposed to a strong and very homogeneous magnetic field. The field strength can be between 0.04-2 T, (400-20 000 gauss), which is much bigger than the magnetic field of the earth. In the Nordic Countries this is approximately 0.6 gauss. This static magnetic field changes the direction of all of the spinning hydrogen nuclei, (i.e. protons), so that they are aligned parallel to the direction of the field. Radio frequency (rf-) radiation is then applied to tissues where energy quanta are absorbed by some of the protons. These become excited as a result and while decaying send quanta of em-radiation to the environment. These photons are detectable and slice images are reconstructed from the resultant interference pattern (magnetic imaging). During this procedure, magnetic field gradients are utilized to extract three-dimensional information.
The photons which make up the radio-frequency interference pattern have such a low energy that they are not able to ionize matter. Magnetic resonance imaging, however, combines strong static and quickly varying magnetic fields, as well as quickly varying rf-pulses which can cause eddy currents. These eddy currents can generate heat in metallic foreign bodies, if such exist in tissue. The theory and practice of magnetic resonance imaging are described more closely in the chapter on Modalities, with possible biological effects and contraindications.
Interactions of ultrasound A vibrating ultrasound crystal in contact with skin (using a gel coupling medium for good transmission of vibration energy) forces tissues to move synchronously with the crystal's characteristic frequency, which may vary between 2 and 20 MHz in medical ultrasound examinations. This phenomenon can not be used in a vacuum like em-radiation, it always needs matter. In soft tissues vibrations occur back and forth in the examined cone of tissues the dimensions of which are fixed by the characteristics of the crystal. Motion amplitudes are small, but even so dynamic (changing in time) areas of compression and rarefaction are generated in matter. The resolution of ultrasound imaging (something between 0.8-0.08 mm) is determined by the wave characteristics of the transmitted beam.
Matter is composed of molecules bound to one another with varying degrees of elasticity. Matter is somewhat slow to set in motion, and it opposes the genesis

and propagation of motion. Translation speed in soft tissues varies between 1460-1580 m/s (approximately five times faster than in air) and in bone between 2500-4700 m/s. Ultrasound advances straight in homogeneous matter and it behaves very much like light; it is reflected, refracted, absorbed and scattered. This means that energy diminishes
Figure 6. Ultrasound is reflected at all boundary surfaces according to the coefficient of reflection R.
Calculated values of vibration intensity in the figure are given in percentages of the incoming intensity. Boundary surfaces are seldom perpendicular to the ultrasound ray, therefore
according to the reflection law a considerable share of vibration energy is lost from the main direction (this also causes artefacts). Vibration energy is scattered and absorbed everywhere in matter, in other words energy is attenuated on its way into tissues and on its way back to
the crystal.
continuously in the cone of tissues in the direction of the motion (and also after reflection while returning back towards the crystal), in other words vibration is attenuated.
The ultrasound image is constructed with that part of the vibration energy which is reflected back towards to the crystal at each boundary surface or tissue interface. The amount of reflected energy depends on the characteristics of the tissue, its acoustic impedance (= ultrasound's translation speed multiplied by the density of tissue), the frequency of the beam, the orientation of the reflecting surface in relation to the direction of the applied ultrasound cone, as well as the interface structure and "roughness" compared with the wavelength of the applied beam (Fig. 6).
From an even surface ultrasound is reflected in the same way as light from an even metal surface; the angle of reflection equals the angle of incidence. Reflected energy is determined by the coefficient of reflexion R. At the boundary surface between soft tissue and air almost all energy is reflected (it is almost impossible to examine lung) and very little at the boundary surface between two tissues with approximately the same value of acoustic impedance. Vibration energy is scattered in all directions particularly at surfaces with rough structure compared with the wavelength. This is the reason that inclined tissue surfaces can not well be imaged. Ultrasound imaging method and applications are described in the chapter on Modalities.
Radioisotopes and radiopharmaceuticals

An organ can be visualised by measuring the emission of gamma radiation from a radioisotope with which a physiological or metabolic agent is labelled. Such an agent (a "radiopharmaceutical"), is introduced into the body by intravenous injection or oral ingestion. The imaging or measurement of a patient is performed with a gamma camera or a PET -camera (see chapter on Modalities).
In contrast to X-ray imaging, radioisotopes emit radiation from their nuclei. In nature almost one hundred elements can be found, whereas the number of known elements is greater than this. Every element (with a fixed number of protons) has several isotopes, which differ from each other by the number of neutrons. An isotope is stable if the ratio between the number of protons and neutrons is in "balance"; in light elements the number of neutrons is approximately the same as the number of protons, in heavy elements there are more neutrons. Most of known isotopes are radioactive, which means that they are in an excited state. Radioisotopes for medical purposes are produced artificially in a nuclear reactor or a particle accelerator.
The energy of a radioactive isotope is released by the emission of emradiation (a monochromatic gamma quantum) and also by the emission of particle radiation (an electron = beta-minus particle, a positron = positively charged electron = beta-plus particle, an alpha particle, etc.). In these latter cases an element is simultaneously transformed to another substance. Radionuclides which emit only gamma radiation are most commonly utilized in diagnostic nuclear medicine, because only em-radiation with suitable energy (60-600 keV) has the capacity to travel from tissues to a gamma camera. Fast electrons with kinetic energy lose this energy in tissues and contribute only to the radiation dose.
Table 1. Clinically important radionuclides (with type of emission and half-life) and with them labelled examination substances, so-called radiopharmaceuticals, which are often produced in hospitals by the injection of Tc solution into a so-called "kit"-bottle. The notation 2 x 511 keV implies that two photons of 511 keV are simultaneously emitted by the nuclide concerned.
Nuclide Domain
Emission keV Half-life Application
Carbon-11 2 x 511 20 min Glucose metabolism
Nitrogen-13 2 x 511 10 min Amino acid metabolism
Oxygen-15 2 x 511 2 min 02, CO, C02
Fluorine-18 2 x 511 110 min Receptor imaging
Gallium-67 92, 182 72h Malignancy, infection
Technetium-99m 140 6h Majority of examinations

Indium-111 173,247 2,8 d Components of blood
lodine-123 160 13 h Kidney
lodine-131 360 8 d Thyroid
Xenon-133 81 5.3 d Lung embolus
Thallium-201 80 73 h Heart infarct, ischemia
An excellent example of a pure gamma radiation emitter is 99mTc which has a gamma quantum of 140 keV and a half-life of 6 hours (that time, after which half of the original nuclides are in existence). 99mTc is used in most nuclear medicine examinations. Table l shows clinically important radionuclides and some of their areas of application.
The parent substance of technetium is molybdenum 99Mo with a half-life of 66 hours. This so-called Mo-Te-generator is transported to hospital once or two times in a week. It is "milked", that is rinsed with saline, to produce sterile sodiumpertechnetate solution which is used to label different examination agents. The labelling happens by injecting some of the solution into a sterilized vial, containing freeze dried physiologically or metabolically active agent. The product is then normally ready to be injected to patient. Typically, the amount of effective radioactive labelled substance is extremely small (the agent can even be poisonous) and it is always dissolved in some millilitres of saline.
The number of decaying radioisotope nuclei per unit time is described as activity A. Its unit is one decay event/s = one Becquerel, Bq. The older unit is the curie, Ci, = 3,7 x 1010 decay events/s. Thus, a typical in vivopatient dose of 99mTc is 370 MBq = 10 mCi. If the mass and volume of radiopharmaceutical agents are also taken into account, the concepts of mass and volume specific activity (Bq/kg and correspondingly Bq/m3) can be used.
Radioactive decay follows the exponential function A = Ao exp-lambda x t where lambda is the constant of disintegration or decay (characteristic to each radioactive nuclide) and t is time. The decay constant and half-life have the following relationship: half-life = 0.693/decay constant. In addition to the physical half-life, the concept of the biological half-life is also used. The combination of these terms is called the effective half-life.
Aaro Kiuru

Printer-friendly version Bookmark This Page
Translate page to (By Google): Radiophysics Radiation protection and patient dose
Both ionizing and non-ionizing radiation as well as ultrasound are used in medical imaging methods. Somatic (occurs in own tissues) or genetic (in descendants) damage in patients or personnel are always a risk of examinations which employ ionizing radiation. Photons of non-ionization radiation (radio wave radiation in a strong magnetic field), as well as ultrasound, carry insufficient energy to cause injuries at diagnostic energy levels. Consequently, radiation protection is needed in practice only in X-ray and isotope examinations and in radiotherapy.
There are many factors which influence image quality. By increasing the amount of radiation (and patient dose) image quality can be increased to a certain level, but simultaneously several factors in the imaging chain can diminish quality. The quality control of imaging methods should be arranged such that high image quality with a dose as low as reasonably achievable (ALARA) is maintained.
The purpose of radiation protection is to eliminate the acute toxicity of radiation exposure and diminish the somatic and genetic risks to patients and personnel. It is useful to remember that the natural background radiation in the Nordic Countries varies between 3-6 mSv (300-600 mrem) per year. There is radiation coming from space, soil (radon gas is a very considerable source of radiation) and construction materials, as well as from our own tissues. Background radiation can vary depending on residential area, life style, etc. This value of 3-6 mSv is the same order as the skin dose from an X-ray image of the body.
Quantities and units of radiation dose Interactions of X-ray and gamma photons always set electrons in motion with sufficient energy to ionize and excite atoms and molecules (see Interactions of radiation with matter). An electron therefore deposits energy in its wake. Around 10-100 ionizations/ m caused by an electron are generated at diagnostic X-ray energies (approximately 33 eV/ion pair). The concept of linear energy transfer, LET (unit keV/ m) can be used to describe this phenomenon together with the concept quality factor Q, explained later. In addition, part of the energy of the electron is absorbed by secondary electrons, so-called delta particles; they in turn have sufficient energy to cause new ionizations.
Exposure Exposure implies that ions are generated in air as a consequence of the passage of radiation. Ions can be measured with an ionization chamber, which is an air space between two conducting plates coupled to the positive and negative poles

of a voltage source. The exposure = the number of ions with negative (or positive) charges divided by the mass of air in the ionization chamber. The SI-unit is C/kg (C = coulomb). The older unit is roentgen R = 2,58 10-4 C/kg.
Absorbed dose This quantity is the energy per unit mass, which matter has absorbed from radiation. The SI-unit is the gray Gy = J/kg (the old unit was rad = 0.01 Gy). At X-ray and isotope imaging energies (15-500 keV) one R exposure causes approximately 10 mGy (one rad) absorbed dose in all other tissues except in bone, where the absorbed dose at low energies (around 20 keV) reaches up to around 40 mGy.
Kerma The concept kerma comes from the words Kinetic Energy Released in Matter. It takes into account the dose generated by the aforementioned delta electrons. It is approximately equal to the absorbed dose in air at diagnostic X-ray energies.
Dose equivalent When energy has been absorbed in tissue the biological effect varies depending on the organ in question, the type of radiation and energy, dose rate, exposure time etc. These are incorporated in the concept quality factor Q, by which the absorbed dose must be multiplied to get the equivalent dose. Its unit is sievert Sv = J/kg (= 100 rem, the old unit).
In X-ray and isotope imaging, Q is approximately 1, because X and gamma radiation deposit relatively small amounts of energy in tissue. Another concept, effective dose, describes the probability of damage to different organs with a weighting coefficient, which is high for radiation sensitive organs such as gonads, bone marrow, lungs, colon, breast etc. and small for other tissues, e.g. muscle. The sum of the weighting factors equals to 1.
From the foregoing it is clear that in diagnostic imaging, the units Gy and Sv, as well as R, rad and rem, have about the same numeric values, although the concepts have different meanings.
Dose rate One useful concept in dosimetry is the rate, with which a given amount of radiation strikes tissues, for instance kerma rate and exposure rate mR/min, R/h etc. Activity (see the chapter Radioisotopes and radio pharmaceuticals) is also a concept which incorporates the function of time. Whether X-rays from an X-ray device or gamma radiation from radionuclides are discussed, the same concepts can be used to describe radiation phenomena and the biological effects of radiation.
Radiation biology

Ionization and excitation result in fragmentation of molecular bonds with potentially harmful consequences to cell structure, metabolism and organ function. Injuries are divided into genetic and somatic ones. The former can appear in descendants after a long time has elapsed, and the latter may occur quickly (acute consequences) or after a considerable delay. In the peaceful usage of ionizing radiation acute toxicity does not occur.
A distinction is also made between stochastic and non-stochastic effects of radiation. Stochastic implies that even a single "hit" of radiation to one cell or to a small cell group can cause a biological consequence. Damage may be either hereditary (in gonads) or carcinogenic (in tissue). There is no threshold, i.e. the extent of the damage does not depend on absorbed dose (cancer is contracted or not), although the probability of an adverse event increases with dose. This stochastic nature of radiation is therefore the basis of conservative radiation protection.
The non-stochastic effect of radiation has a definite threshold (normally different for every tissue and organ). These have been found from past experience, e.g. in cancer treatment with radiotherapy during this century. Diagnostic radiation examinations (where skin dose varies between 0.1 mSv and 0.1 Sv / examination) expose the patient to very small doses so the consequences of non-stochastic effects do not evolve. One clear exception is the dose to a fetus, particularly during the sensitive period of organogenesis. Therefore, the indications for pediatric examinations involving ionizing radiation must be examined particularly closely.
It is estimated that if 200 000-2 000 000 people get a dose of l mSv (the same as the background dose per year without radon) it is probable that one person will develop cancer. It is, however, impossible to separate so few cases from cancers caused by other factors, such as environmental toxins and unknown reasons etc.
Many other factors such as the type of radiation and energy, LET value, dose rate, time between exposures or fractionation of dose, different sensitivity of tissues for radiation, biological variations etc. have a significant effect on the likelihood of injury.
Radiation protection Because injuries from small doses can partly be stochastic the starting point of radiation protection is to avoid and reduce somatic and genetic doses to as low a level as possible (ALARA, As Low As Reasonably Achievable). The consequences of small doses given over long periods of time are partly unknown, and as the time for a carcinoma to appear can be decades, damages caused by low level radiation are often impossible to separate from diseases caused by other factors. On the other hand it is important to use sufficient radiation to achieve good quality images. These examinations, which are clinically indicated, must be performed with sufficient radiation to achieve an image of diagnostic value.

Patient The dose can be measured or estimated at different depths in the patient, or in different parts of the environment. Terms like skin dose (or surface or entrance dose), depth dose, dose in patient's centre, exit dose (approximately the same as dose to the screen without a grid) and organ dose are fairly self-evident. Dose diminishes as the depth at which it is measured increases. In the diagnostic examination of the body only a 1/100-1/1000
Figure 7. Patient thickness very strongly influences the entrance dose needed for an image. Measurement conditions are also shown.
part of the initial dose penetrates through. Dose decreases also without matter, even in air. Radiation intensity (as well as light intensity) decreases in inverse proportion to the square of the distance from the focus.
Fig. 7 shows how skin dose and exit dose are changed with patient thickness when the exposure of film to a constant blackness (optical density) is made with an automatic exposure meter. In this case exit dose does not depend on thickness, because a screen-film combination always requires a certain amount of radiation.
Many features of X-ray devices and properties of patient tissues influence the dose needed for good image quality. In Table 2 the most important factors are mentioned.
Table 2. Factors influencing patient dose
- radiography (mAs value x number of images) or fluoroscopy (mA value x examination time)
- high voltage (kVp) and its stability - filtration
- distance from focus - field size
- thickness of object and absorption in tissues - lead grid

- sensitivity of screen, image intensifier and detectors - usage of image memory (for instance in surgical operations)
There are big differences in the properties of different imaging methods and in radiation detectors. Screen-film-combinations are always used in practise instead of film alone. Screen sensitivities vary from speed value 20 to 1600 (that of the reference screen-film-combination being 100), when the speed of the film alone has a value of about l. Consequently corresponding alterations can be found in patient doses.
Personnel The first rule in the radiation protection of personnel is to go outside the X-ray laboratory when a patient exposure is made. In fluoroscopic examinations one must work l) quickly, 2) with sufficient protective clothing, and 3) at an appropriate distance from radiation sources. These three measures are of primary importance in both X-ray and isotope work. The staff who are most likely to be exposed to radiation are those who work
Figure 8. Diagnostic x-ray device: generator, X-ray tube and console (control board). Exposure is
ended when the ionization chamber(s) in the automatic exposure system has (have) collected enough radiation (ionization) to blacken the film adequately (after development).
The positions of the three chambers are shown in the radiation field, as well as spectra (number of photons as a function of energy) in different phases of the X-ray chain.
with fluoroscopic devices (radiologists, surgeons etc.), nurses who hold small children or non-cooperative patients, as well as staff working with the nuclear medicine imaging of patients.
National and international radiation legislation and recommendations are universally in use. According to these regulations, for instance, examination rooms, devices and working conditions must be adapted so that doses are diminished to as low a level as possible and that the quality of images and examinations attains the highest possible level. The most recent ICRP recommendation (publication 60, 1991) puts the maximum dose level of 20 mSv per one year to the whole body of personnel. This value is 40% of the earlier

maximum limit, which shows the increasingly conservative attitude in radiation protection.
One should remember that the dose to personnel from scattered radiation is 100-1000 times smaller than the dose in the entrance field on the patient's skin. Therefore it is essential for the radiation worker to avoid putting his hands in the primary radiation field (use lead gloves). The patient's body can also serve as good protection, if one can place oneself in such a position that one does not directly see the entrance field of radiation.
Aaro Kiuru
Printer-friendly version Bookmark This Page
Translate page to (By Google): Radiophysics X-ray generator and X-ray tube
X-rays are obtained from an X-ray tube, to which an X-ray generator feeds energy in the form of kinetic energy of electrons (Fig. 8). The primary function of a generator is to accelerate electrons to a constant energy value during the whole period of exposure by generating constant high voltage (kVp) between the glow cathode and rotary anode of the tube. There are also other requirements: 1. The system should tolerate continuous lasting use. 2. The intensity of radiation should be sufficiently high to enable short exposure times (diminishes motion artefacts) at a focus-film distance of approximately 1 m (diminishes distortions and dose as well as proves resolution). 3. The size of the focus should be as small as possible (between 0.1 x 0.1 and 2x2 mm2, improves resolution), and the radiation field must be limited to the immediate vicinity of the organ in question (radiation protection, reduces scattered radiation).
The generator is an electric transformer which converts 220 V (1-phase) or 380 V (3-phase) alternating voltage to high voltage somewhere between 20-150 kV. High voltage is rectified with a diode bridge. Depending on the electric coupling in the transformer, 6 or l2-pulse (during the period of 20 ms) high voltage is generated, with corresponding pulsatile variations in the radiation yield (both in intensity and in the ability to penetrate tissues). However, so-called medium or high frequency generators have progressively come into use; they use modem small scale electronics to generate constant (as opposed to pulsed) high voltage. In the past, 2-pulse generators were used especially in dental radiography which

meant that voltage (and X -ray output also) went down to zero between peaks of pulses.
Filtration of X-ray spectrum There is often both a small and a big focus in the cathode (dual-focus). Electrons emitted from the cathode wire hit the anode in an oblong area, the surface of which in the direction of the patient is a square of normally 0.3x0.3, 0.6x0.6 or 1.2x1.2 mm2. Both braking radiation and characteristic radiation (see Interactions of electron; X-ray spectrum from X-ray tube) are generated in the anode. X-rays leave the focal point in all directions from the focus, but they are utilized for imaging purposes only in the direction of the patient by using a multileaf collimator.
In an X-ray tube there is also an aluminium (1-5 mm) and/or a copper (0.1-0.5 mm) filter and a light source with a mirror to simulate the radiation field on the skin. The filtration of the X-ray spectrum diminishes particularly the number of low energy quanta and therefore raises the average energy of the beam. The patient's body diminishes further the total intensity (area) of the spectrum and simultaneously hardens the average energy. Spectra at different phases in the imaging chain are shown in Fig. 8.
The lower curve of Fig. 5 (and the curve labelled "leaves tube" in Fig. 8) shows that the glass or metal envelope and filter have removed all very low energy photons, which have only a small probability of penetrating the patient. In the braking radiation spectrum in Fig. 8 one can see the peaks of characteristic radiation (59 and 67 keV from tungsten anode), if the energy of incoming electrons is sufficient to excite electrons in the K-shell (Fig. 1). The area underneath these peaks is only a small percentage of the total area of the spectrum.

Figure 9. The attenuation coefficient for iodine contrast media, bone, muscle and fat
depends on radiation energy; -vales are biggest at low energies in heavy materials (photoelectric effect). Differences between bone-muscle and muscle-fat coefficients are shown with dotted lines. The K-edges
of medium and heavy elements are situated in the energy range of diagnostic
X-ray imaging. Therefore, an incoming electron or photon must have more energy
than 33.2 keV to excite or ionize an electron from the K-shell of iodine.
Figure 10. Properties of an object, such as its
thickness and tissue composition, as well as radiation energy are important factors
when adjacent tissues are to be seen separately in an image.
Printer-friendly version Bookmark This Page
Translate page to (By Google): Radiophysics The object and its influence on image characteristics

Tissue contrast and total contrast After X-rays have gone through the object and lead grid the quality of radiation (X -ray distribution in Fig. 2) cannot be further influenced. Local variations in the intensity of radiation, in other words tissue contrast must be conferred as effectively as possible to the image.
Tissue contrast is visualised in a radiograph when two (nearby) areas can be separated from each other due to their different optical densities or darkness of film. Reasons for this can be 1) that tissues with equal thickness have different coefficients of attenuation, or, 2) that their thickness is not the same (Figs. 9 and 10).
Tissue contrast is therefore a property of an object, and it depends on the inner structure and tissue or elemental composition of the object. The visualisation of tissue contrast depends in addition on kVp and radiation spectrum as well as on the amount of scattered radiation. Fig. 9 shows how attenuation of tissues, based on attenuation of elements, changes as a function of energy.
Tissue contrast is caused mainly by differences in the coefficients of tissue attenuation, which depend on energy. An X-ray image is produced by an X-ray spectrum, in other words by a huge number of polychromatic quanta with different energies (Fig. 5). The probability of each photon ending up in a photoelectric absorption or Compton scattering depends on its energy. Photons with medium energy are most abundant in a spectrum, but a radiograph is the result of all interactions of photons in tissues. The low-energy photons cause the biggest contrast, but their ability to penetrate an object is the lowest.
With radiation detectors such as a screen-film combination (radiography) or image intensifier (fluoroscopy) or with a digital subtraction device (DSA) it is possible to increase total contrast (which is tissue contrast amplified by detector contrast). The amplification factor for film (gamma value) is usually between 2 and 3. An image intensifier does not generally reinforce contrast, but with DSA one can very substantially emphasize contrast between soft tissues and blood when a contrast media bolus is used (e.g. in angiography).
When the current (mA) of an X-ray tube, exposure time (s) or their product (mAs) is increased, the spectrum also changes, its total area or intensity increases in the same proportion. The image becomes darker, as blackness or optical density on the film increases. On the other hand, when voltage (kVp) is increased, this also increases photon energy and the radiation beam becomes more penetrating (resulting in a smaller dose), but contrast is reduced.
In an X -ray image or radiograph the shadows of bones are demonstrated white or light, because bone efficiently stops radiation quanta, especially at low X -ray energies. Soft tissues are seen in grey tones and organs containing gas in dark tones. In digital image manipulation this grey shade scale is easy to turn upside

down. In DSA strongly absorbing objects, like veins filled with contrast media are normally displayed black, etc.
Photographically speaking, an X-ray film is a negative. Normal X-ray imaging without contrast media (plain radiography) is suitable for the examination of bones and organs containing gas (like the lungs), but soft tissues cannot be separated from one another. Liver and kidney for instance, as well as brain and cerebrospinal fluid are equally grey in a radiograph. For the visualization of soft tissues contrast media and/or digital methods with a computer must be used.
Influence of scattering After Compton scattering the photon continues with reduced energy in a new direction (see Interactions of X -ray and gamma quantum with matter). All scattering angles have nearly the same probability, but at higher energies scattering in small, forward directed angles is more probable. This is regrettable, because film is positioned in the direction of the primary photons and these small angle scattered photons. Primary photons make the image, but scattered photons only reduce contrast.
Scattered radiation is present in all X-ray and nuclear medicine imaging. Its influence is smallest in thin objects imaged with small field size and at low energy. When examining large and thick objects (body) the number of scattered photons in the exit field, in other words at the film, can be 5 or even 10 times bigger than the number of primary photons.
The following ways are efficient in diminishing the adverse influence of scattered radiation in X-ray examinations: 1. Keep the field size as small as possible. In other words, collimation of radiation, e.g. with a blade-type diaphragm must be used. 2. Use a grid against scattered radiation. 3. The space between an object and the film can be used to reduce scatter (so-called air gap technique). 4. The object can be compressed 5. Low voltages reduce scattering (but this is against the main principle of radiation protection as it increases the patient dose).
A lead grid allows primary photons from the focus to go through to the film like a Venetian blind allows light to go through. The grid consists of thin non transparent lead lamellae placed side by side with transparent aluminium or carbon fibre lamellae. It lets only merely parallel or almost parallel photons pass through (Fig. 2). The relation between the height of a lamella (a few mm) and the distance from a non-transparent lamella to the next one (0.1-0.5 mm) is called the grid ratio. It is generally between 5 and 15. Both parallel and focused grids are in use. The

Figure 11. Distortions arise in an image due to imaging
geometry and thecharacteristics of
an object.
grid can also be set in motion during the exposure so that the lamellae can not be seen in the image.
Imaging geometry In conventional X-ray examinations tissues can be divided into four main groups: skeletal structures (seen as white or in light tones in the image), soft tissues (grey), fat (somewhat darker than soft tissues) and gas (dark). The basic X-ray examination is well suited to skeleton and thorax examinations, because the boundaries between tissues (with the exception of soft tissues and fat) can clearly be seen. To separate muscles, inner soft tissue organs etc. from one another, contrast media or newer examination methods like CT or magnetic resonance imaging must be used.
Electromagnetic radiation travels in straight lines. Without scattering, the understanding of the formation of an X-ray image would demand only appreciation of laws of geometry, in the same manner as articles between a light source and a screen cause shadows. Fig. 11 shows the geometrical enlargement in exaggeration, as well as different distorted shadows of object details on a film surface.
There is always enlargement in a radiograph. It is biggest on the edges of an image and from those objects which are most distant from the film surface. Enlargement is smallest in the middle of the image field and from objects nearest to the film surface. A shadow on an image is caused by a real object, i.e. a lesion in tissue with different absorption properties to its surroundings, or it can be a sum of shadows of two or more objects on each other in the direction of the radiation beam. It can happen that a small or rather poorly absorbing object lying behind a bigger, more strongly absorbing object, can not be distinguished at all (for instance a small tumour lesion behind a rib).

Figure 12. Factors in having a greater or lesser influence on image quality in the imaging chain. Abbreviations
C, R, N, and D stand for Contrast, Resolution (sharpness), Noise (proportional to the square root
of the number of quanta) and exposure Dose.
The understanding of geometrical facts is of primary importance for an image interpreter and user of an X-ray device. Long exposure time when an object moves causes, for instance, unsharp images of sharp bone edges. Short exposure times are always recommended; they require large amounts of current and demand a big load from the X-ray tube.
An important factor is the shape of an object. Many organs are cylinders or they have curved surfaces. More radiation is absorbed in the middle of spherical objects and therefore a radiograph tends to be darker at its edges. This absorption unsharpness (for instance in a lung tumour) can be seen in an image.
Aaro Kiuru
Printer-friendly version Bookmark This Page
Translate page to (By Google): Radiophysics Image quality

In all imaging methods there are many factors which influence image properties and quality. X-radiography is mainly described in this chapter, but the following concepts are usable in all medical imaging methods. Fig. 12 shows factors and parameters divided into eight groups which have significant effects on image quality.
What is image quality? An image is always a two-dimensional presentation of a three-dimensional organ (possibly 3D, if slices are taken side by side or if changes in time are taken into account). The chain from target tissue via transmitted or emitted radiation to the interpreter's brain (with a more or less definitive understanding of the normal and pathological findings) is long and complicated. There are factors which influence the interpretation in different directions. The first part of the chain is rather well known; physically measurable quantities: contrast, resolution, and noise do exist. The terminal parts of the chain, i.e. the tasks and functions of the eye and brain for the detection and recognition of findings are not so well known.
Connection between the physical quality parameters and diagnostic applicability is difficult and laborious to determine objectively. To compare two imaging methods objectively it is possible to measure sensitivity and specificity for studied objects and diagnosis, and express results in the form of a so called ROC-analysis (Receiver Operating Curve). Randomized groups of images are compared by several interpreters. The functioning point of each interpreter is situated (he uses a threshold between pathological and normal findings) somewhere in the ROC-curve.
Physical parameters of the image Contrast, resolution, noise, and signal to noise ratio as well as the position of the image and image portions on a grey scale are important parameters in all imaging. By changing the latter in a digital image (windowing) the usability of the image can be greatly improved (see chapter on Digital image processing).
Contrast (the difference of blackness or optical density of film between nearby areas in an image, Figs. 2 and 10) is caused by properties of tissues and properties of the film or other radiation detector. The difference of transmitted X-ray intensities in Fig. l0 can be normalized with the sum of intensities resulting in contrast scale from 0 to 1. The human eye can detect differences in contrast of 0.02 under good light conditions. With digital methods it is possible to go down to the 0.001 level (Fig.13). While viewing images on a lightbox it is important to mask light from any side of the image reaching the eye. A magnifying glass or a bright light should be used when necessary. These measures improve greatly the detection of low contrast areas.
Many factors which strongly affect contrast have already earlier been described. Noise in an image also frequently plays an important role particularly at low contrast levels. Noise can be seen as a locally variant, fine or rough change in

optical density which occurs even in an image of an evenly exposed water or Plexiglas phantom. There are two principal causes of noise in an X-ray image:
1. The number of X-ray quanta varies both as a function of time and site (quantum noise, statistical nature of radiation). 2. The construction of the film, screen and image amplifier, as well as the electric circuits in the imaging devices causes noise.
Relatively few X-ray quanta per exposure are collected while working with fast screen-film combinations and a very grainy image may result, like spots of rain on an asphalt surface. With normal or slow screen- film combinations (as well as with mere film) much more quanta, "raindrops" (dose increases) are detected, and an image looks as if it is "calming" out, and not so noisy. The signal-to-noise ratio is a fundamental concept, with which image characteristics can quantitatively be compared, particularly in digital imaging methods.
In the image of a sharp edge the film blackness changes to another level of blackness on a short distance serving as a measure of image sharpness. Unsharpness is caused by many factors in imaging chain; focus size, motion of the object, thickness of the screen, geometrical factors etc. Sharpness is in practice defined by spatial resolution, which tells how many details or lines (line pair, lp) can be distinguished for instance in one mm (unit lp/mm). The following values are in general use: - 20 lp/mm (film alone) - 10 lp/mm (normal screen-film-combination) - 5 lp/mm (fast screen-film-combination) - 1-2 lp/mm (image intensifier-television chain, magnetic camera) - 1 lp/mm (CT device and ultrasound device) - 0.1 lp/mm (gamma camera)
Resolution can also be defined as the smallest distance (mm) between two objects, which can be separated from each other in an image. The concept of modulation transfer function, MTF is also useful when comparing the contrast and resolution properties of imaging methods.
Comparison of imaging methods In Fig. 13 general imaging methods are compared in terms of resolution and contrast. Both, i.e. low contrast level and small details, can not be achieved simultaneously. For instance contrast must be high when small details are to be separated, (e. g. in the inner ear or fine structure of bone). On a thorax image "shadows" in lung parenchyma are usually looked for;

Figure 13. Mean values of contrast and resolution in various imaging methods. The CR-curve of digital cassette radiography lies in the neighbourhood of that of the CT curve, but shifted to the left
for smaller detail.
the areas of such lesions must therefore be relatively large especially if their density does not differ much from the surroundings. Low contrast at an edge, large focus size and geometrical magnification make it more difficult to see small objects in thorax imaging. Different imaging methods can consequently be used depending on the information which one is seeking.
Digital imaging methods improve the ability to register small contrast differences (Fig. 13). The aforementioned windowing method can play a central role in the image interpretation performed in modem image work stations, where digital images from different devices (CT, DSA, magnetic resonance imaging, nuclear medicine, PET, ultrasound) are compared and analyzed. Fig. 13 contains no information regarding the dynamic characteristics of imaging methods or of noise.
Aaro Kiuru
Printer-friendly version Bookmark This Page
Translate page to (By Google): Digital imaging Analogue and digital images

Historically, radiological images were recorded on glass plates covered with a light-sensitive emulsion. This emulsion, sensitive to a wide range of photon energies, consisted of microscopic particles of silver compounds which following exposure, developing and fixation built up an image, consisting of small black dots, of the radiographed object. Different types of intensifying screens and filmbased materials have not changed the basic principle that the information content of the image consists of microscopic dark dots, the dens it y of which determines the darkness in a given image area. The darkness thus varies continuously and the image produced is called an analogue image.
If the darkness along a line across an analogue image is measured with a densitometer as in Fig. 1 a, the result will be an irregular curve where the finest irregularities represent the individual silver particles. If the registered curve is divided into equal parts the dens it y in each part can be calculated as an average that can be given a numerical value. The averages are seen in Fig. l b and the corresponding numerical values in Fig. 1 c. When the whole surface of a radiological film is measured with a densitometer line by line in this way the analogue image can be transformed into a so called digital image (Fig. 2).
The distances between the lines and the size of the equal parts dividing each line defines the resolution of the digital image. A quadrilateral, as high as the distance between two lines and with the width of one division along a line, is called a picture element or a pixel. The digital image is naturally adapted to computer techniques. Thus, the images are normally divided into a number of pixels equal to powers of 2, e.g. 512 x 512, 1024 x 1024 or 2048 x 2048 pixels. The
Figure 1. Analogue to digital conversion of a photometry recording along a line into a
sequence of binary Y signals. A) Schematic photometry curve of a line, e.g. across a radiographic film
B) The same curve divided into equal distances. For each segment the average photometer recordings have been assessed on a scale from 0 to 15 (24 steps)
C) Digital printout of the photometer averages in 1 B D) Binary representation of the digital series of numbers in 1 C.

Figure 2. The influence of spatial and density resolution on
image quality in an analogue to digital image transformation.
a) Analogue image with moderate spatial and density resolution. A low spatial resolution matrix
is superimposed upon the image. b) The same analogue image with a 10 by 10
pixel spatial matrix and 2 bits contrast resolution, i.e. 4 density levels.
e) The final digital representation of the low spatial and density resolution image.
number of possible shades between black and white are also often referred to by a binary value, for example 8 bits = 28 or 256 shades, 10 bits = 1024 shades, or 12 bits = 4096 shades. In Fig. l d the darkness is given as 4 bits or 16 shades or levels and in Fig. 2 as 2 bits or only 4 levels.
Tatsuo Kumazaki and Hans Ringertz
Printer-friendly version Bookmark This Page
Translate page to (By Google): Digital imaging Image acquisition
Radiological images today are acquired utilizing a wide spectrum of different techniques, ranging from analogue via various acquisition modalities to direct digital registration. The technique is usually dependent on the radiological modality in question.
Conventional radiology techniques usually acquire an analogue image on photographic film where the density varies continuously without any discrete steps. The image is normally formed through direct or indirect radiation on the emulsion layer of the film by X-rays emanating from an X-ray tube and by light emitted by the intensifying screens (see Chapter 4). This category also contains techniques such as scanograms and ultrasonography where analogue image information is amplified electronically and transmitted as a video signal to image

screens and photographic film. The video signal is the means by which analogue information is transmitted electronically.
The images created on image plates, during digital fluoroscopy, digital subtraction angiography, in certain ultrasonographic equipment, and in gamma cameras are initially registered in digital form. These data can subsequently be transformed and presented either in analogue or digital form on image screen or photographic film.
Finally, we have the group of modalities which comprised the breakthrough for digital techniques in radiology, namely computed tomography (CT), and later Single Photon Emission Computerised Tomography (SPECT), Positron Emission Tomography (PET), and Magnetic Resonance Imaging (MRl). In these modalities transmitted or emitted electromagnetic photons not primarily depicting anatomy are registered and the image is calculated by computer from the photon information. They are thus producing calculated digital images and the density of each pixel has been obtained as the solution of a series of equations.
Analogue/digital transformation Image content, transmitted by electronic or optical means within radiological equipment, a radiological department, or between different departments is sent in analogue form via an electric current or by an optical signal varying in intensity in a similar manner to that shown in the curve in Fig. 1 a. The image can also be transmitted as binary digital signals demonstrated in Fig. 1 d.
Acquisition of radiological information as well as presentation of images on a monitor are thus sometimes digital and sometimes analogue. This means that there is a need for units that convert electronic image information from analogue to digital and vice versa. Such units are called A/D and DIA converters.
Digital image plates The radiological image on a photographic film is produced through illumination with light from intensifying screens and to a lesser degree as a direct effect of X-ray quanta. On digital image plates the information is stored as excited electrons in phosphorous plates containing complex inorganic substances.
Thus, the radiological information, after passage of the radiation through the object/body, is temporarily stored on the image plate in inverse proportion to the absorbed radiation dose. In order to read this information a laser beam is used to release the trapped energy stored in the image plate as emitted light. The laser beam sweeps over the image plate line by line until the whole surface has been read. After the laser stimulation the stored information is transformed from emitted light to electronic signals using a photo multiplier. The image plate can be reused many thousands of times.
The electronic signal is amplified, digitized, and transferred to an image processor. This unit has a twofold function. Firstly, it calculates the mean

darkness of the image and the total range between the light and the dark parts of the image. Secondly, it uses this information to calculate an optimal image that is transmitted to a laser printer which produces the image on transparent film.
The digital information can also be transmitted to a Picture Archiving and Communications System (PACS), which used in combination with high resolution monitors for diagnostic work and conferences can eliminate the use of photographic film.
The use of digital images from image plates has a number of advantages: 1. There is increased sensitivity to X-ray quanta which can be utilised to increase the image quality and/or reduce the radiation dose. 2. Erroneous exposures are greatly reduced as nearly all exposures can be salvaged by the image processing. 3. The digital image can be transmitted, manipulated, and presented in many different ways.
Calculation of a tomographic image CT and other modalities where the image is calculated from emitted or transmitted electromagnetic information, use tomographic sections. This means that the calculated images represent parallel planes through the anatomy in question. Such a section is defined as the plane in which the detectors of the CT, SPECT, or PET units are located. In MRI, the image reconstruction can be made in any selected plane (2D) or volume (3D).
The calculations involved are complex and time-consuming even for powerful computers. As a simplified description in the case of CT each detector reading can be said to represent the absorption along the line of volume elements through which the X-ray beam has passed.
This will give an equation where the absorption in each single volume element is the unknown parameter that represents the darkness of the corresponding pixel. As a large number of detector readings is made, a huge equation system is obtained, for example in a 512 x 512 matrix there are 262,144 unknown parameters.
These equations are solved with different, more or less approximate mathematical techniques. The result will be a density value for each pixel of the tomographic image.
Spatial and density resolution The most important aspect of image quality is resolution. The number of line pairs per mm that can be resolved by the eye under defined circumstances is often used. However, this definition is only valid for analogue images. Digital images cannot of course resolve details that are smaller than one pixel. This type of resolution is called spatial resolution, compare Figs. 2 a, b.

If the spatial resolution of a conventional radiological film is determined it is comparable to a digital image with a resolution as high as 4096 x 4096 pixels. Under certain circumstances even higher spatial resolution is used, e.g. in mammography.
In order to assess the spatial resolution the contrast resolution has to be maximal. This means that the line pairs and the background have to be black and white. If the contrast resolution is less the spatial resolution will be reduced. The contrast resolution in a digital image depends upon the number of possible shades of darkness and is often better than that of an analogue image.
Figure 3.
The settings of a typical grey scale in computed tomography. The digital image in the computer memory has a contrast resolution from about -1000 (air) to +1000 (bone). An
example of the setting of the window width and level is indicated. The level is -600 HU and the width 800 HU. The resulting image with these settings will/ show -1000 and below, as
black, and -200 and above, as white.
Tatsuo Kumazaki and Hans Ringertz
Printer-friendly version Bookmark This Page
Translate page to (By Google): Digital imaging Image manipulation
The digital image is thus inferior to a conventional analogue radiographic image when it comes to spatial resolution. This is compensated for by the nature and potential of digital technology. The contrast resolution is superior which is an advantage when the potential for the eye to observe the different shades of

darkness is enhanced by the ability to shift the contrast scale, for example on a monitor (Figs. 3,4).
It is possible to carry out a number of manipulations of the digital image in order to enhance the information content of the image. Most of these manipulations can also be carried out with analogue images but this is more cumbersome and time-consuming. As digital images should be assessed on a monitor, simple measures such as changing black and white (Fig. 4 C) or magnification of a detail can be routinely performed.
The goal for image manipulation in radiology is to increase diagnostic accuracy (Fig. 5). In the process of object-image production and final diagnostic image assessment, the image manipulation is included as a quality enhancement. In addition, the potential for different image interpretation techniques is increased compared with conventional film reading. Techniques for both interactive interpretation and automatic image analysis are being evaluated presently.
Figure 4. Examples of different simple manipulations
of one digital image of a computed tomography section through the chest. A) A limited density range image with a window level of 0 HU corresponding to
water attenuation and a window width of 000 HU Pixels with a value equal to or less
than -500 are black, and pixels with a value equal to or above +500 are white. B) The same image with a pulmonary
setting. Window level is -600 HU and the window width is between 1000 and -200
HU as in Fig. 3. It can be seen that the soft tissue details disappear in the chest wall
while the structure of the lung is visualised compared with a).
C) Fig. A) with reversal of the scale so that pixels of +500 HU and above are black, while pixels of -5 00 or below, are white. D) The full density range from -1000 to
+1000 HU Observe the diminished contrast resolution between muscle, fat, and glandular structures in the chest wall and breasts.
E) The same image as Fig. D) with single application of an edge enhancement algorithm. Some new structures are seen in the lung.
F) The same image as Fig. D) with double application of an edge enhancement algorithm. Most of the lung structures seen in Fig. B) are seen but a disturbing back ground noise has
been added to other tissues.

Figure 5. Schematic representation of the diagnostic imaging process and image manipulation. Image acquisition from the object, in this
case the liver, may give possibly important but vague diagnostic information. Image manipulation will give a processed image that enhances the diagnostic findings - or discards them. Image analysis, normally visual, leads to diagnostic assessment in
the form of a report.
Darkness level and window width The simplest form of digital image manipulation is the normal use of darkness (contrast) level and windowing when evaluating CT or MRI images on the monitor. A digital image with 2048 darkness shades will lack contrast if all 2048 levels are visualized with 0 as black and 2047 as white (Fig. 4 d). A darkness level of 1024 and a window of 2048 steps has then been chosen. On a CT the scale normally runs from -1024 to + 1024 Hounsfield units, HU, as seen in Fig. 3.
In order to assess the lungs optimally on a CT chest slice, a darkness level dose to the average CT dens it y of the lungs (between -600 and 900 HU) ought to be chosen (Fig. 4 b). The window width 800 and the level -600 means that -1000 HU is seen as black and -200 HU and above is white (Fig. 3). If the same digital image is used to assess the skeletal details of the chest a window width of 1000 and the level +500 HU will result in a complete grey-scale between 0 and +1000 HU (Fig. 4).
Image subtraction The subtraction of a pre-contrast film from a radiographic film after contrast medium injection into the arteries - angiography - has been practised for many decades. This technique was especially used when the background to the vascular tree was very irregular or dense as for example in the base of the skull or the upper part of the chest. The pre-contrast film was inverted photographically so that black became white and vice versa and then matched to the post-contrast film so that only the vascular structures were seen.
This procedure is of course both faster and simpler to perform electronically with a computer. Whole sequences of cine background images can be subtracted from moving contrast-filled vascular structures such as the coronary arteries of the beating heart. The technique is called Digital Subtraction Angiography (DSA). The subtraction is often made in real time while the contrast injection is being recorded. A computerized advantage is to be able to find automatically the

optimal subtraction orientation of the two images, if a slight movement has occurred between the pre- and post-contrast image.
To manipulate an image The possibilities of performing mathematical manipulations on digital images are more or less unlimited. In practice, only relatively few manipulations are used, primarily edge enhancement and contrast equalization. They are used to even out the contrast span over the whole image, to enhance contours that can be difficult to see, and to even out irregularities in homogenous structures. The reason for evening out the contrast span is to be able to assess equally structures that are located in very dark or very light areas on the original image.
Figure 6. Examples of simple radiological measurements
performed on digital images by the modality computer.
A) Distances 1, 2, and 3 within the chest are given in centimetres (DI) together with the angle in
degrees between the line (indicating the distance) and the vertical direction (AN).
B) Angles in degrees between the indicated lines are given on the image.
C) The circular Region of Interest (ROI) in the lung indicates an average attenuation of-815 HU (ME) with an average pixel deviation from the mean of
70. 76 (SD). The surface of the circle is also calculated (AR) and is 30.73 cm2.
The methods for image manipulation are mathematically based on a recalculation of each pixel based on the values in surrounding pixels. Squares of pixels, e.g. 3 times 3 or 5 times 5, are used to influence the value of the middle pixel. Edge enhancement gives an image that mimicks the manipulation made by the eye sending visual information to the cerebral cortex. This means that the

second derivative of the densitometric curve is used around an edge resulting in an extra bright zone on the light side of the edge and an extra dark zone on the dark side (Figs. 4 e, t).
Radiological measurements The ruler and the protractor have always been radiological tools. Measurement in radiology was then advanced when the development of ultrasound introduced the ability to make simple measurements such as distances and angles between identified points on the image. This capability was especially important when no relative size estimate was available on the screen. Subsequently, area and examination- specific measurements were developed.
The same options are nowadays accessible for most screen oriented modalities independent of whether the images are analogue or digital. Simultaneous measurements of multiple distances (Fig. 6 a) and angles (Fig. 6 b) can be obtained. Both regularly and irregularly shaped surfaces can also be analysed with respect to area, mean dens it y (e.g. HU attenuation), and the standard deviation of the density (Fig. 6 c). In the future the ability to make measurements on the image will be combined with normal values for the measurement related to measures such as patient age, height, or weight. It ought, for example to be possible to measure the projected area or volume of a kidney and relate the result to an appropriate parameter of body size. This should also be true for cardio-thoracic ratio or cardiac volume per square meter body surface area, etc.
PACS As mentioned above this abbreviation means "Picture Archiving and Communications System". A first step in the development of PACS in a hospital or health care organization, is a HIS or "Hospital Information System". The corresponding system in a radiological department is called RIS or "Radiological Information System". Such computer systems contain data about the patient, e.g. name, address, previous examinations, modalities, and diagnoses, scheduled visits, referring physician, ward, etc. When linked to a PACS and the units that produce digital radiological images they form the basis of a digital radiological unit.
A PACS technically contains five parts: 1. The communication network with the image sources (Modalities) 2. A registry of examinations and patients and the archive for storage of such demographic data 3. Programs for implementing the demonstration and manipulation of images 4. An archive of all images 5. A unit for communication via a telephone connection or computer net to other digital systems
It is important that the patient administration system also keeps track of the digital images in order to maintain professional secrecy and order in the system.

The access time for an examination in a PACS depends on many factors. This time is longer if multiple image sources are connected, if complex manipulations are made, or if frequent requests for previous examinations are made.
In a completely developed PACS, radiological conferences are performed on image screens rather than photographic films. During a transition period analogue films and image screens often coexist and both may be used during conferences.
Archival of digital images Developments in the computer field have made it possible to store large numbers of digital images even if a very large memory capacity is necessary. A binary figure is called a bit. In most instances eight bits form one character (a decimal figure, a letter or comparable entity) and is called a byte. One kilobyte is 1024 bytes and a megabyte is about one million bytes in a computer. The hard disc of an ordinary personal computer contains of the order of 100 megabyte.
One image with a spatial resolution of 1000 x 1000 pixels uses one megabyte of memory with the possibility of 8 bite or 256 levels of contrast resolution. As larger radiological departments produce millions of images per year the required computer archive is enormous if all images are digital.
In order to reduce storage requirements the digital image information is normally compressed in one of two ways. In the first type of compression an image identical to the original can be obtained from reversibly compressed data. The gain in computer storage is about 50 to 70 % and the compression is in the order of two or three times. The reduction can be described in a simplified way as putting together all neighbouring pixels with the same value and storing them as one piece of information, indicating the start and the end of these pixels.
In the second type of compression the compression factor can be up to 40, or even more. This means, however, that the recalculated image differs somewhat from the original. In the case of higher compression ratios the differences between the original and final images may be marked and could influence their diagnostic usefulness. There is thus a balance between image quality on the one hand and computer memory on the other.
A second such balance exists between retrieval time and cost. If the image has to be retrieved immediately from the memory the cost is high, especially if the archive is large. Using tape, laser- or CD disks that might be searched for and mounted prior to image retrieval will increase the time cost but reduce the economic cost.
Image communication Digital images in a PACS are transmitted between image producing modalities, image workstations, image screens for conferences, and computer archives. The large volumes of data makes great demands on the communication network. The

network of special computer lines can be separate for PACS but sometimes when there are large distances between image producing units and computers and work-stations, the general computer network of the hospital is used. In such a case the demands for professional secrecy is high and the large amount of image data tend to block even medium capacity networks. In such cases optical cables can be used for transmission of images since such cables have large capacity and better security.
The first system for data communication in a hospital often deals with administrative data and comprises a computer in contact with a computer terminal. The components of PACS are so complex and take up so much computer memory that image communication is between computers. The main reason for this is the time needed to produce an image on screen. If each image were transmitted to the viewing station when it was requested, the time required would be unacceptably long. For this reason whole image packages are transmitted to the work station at the same time as the first image is made ready for viewing and manipulation.
Teleradiology One extreme of image communication within PACS is teleradiology or transmission of digital radiological images between radiology departments or to a referring unit over the telephone network. It is not yet very common but can be used for consultations between radiologists or when radiological examinations are performed without a radiologist on site.
The radiological evaluation is made after image transmission over a telephone line. It is, however, important that the clinical data and other information is given verbally or in written form. One line of development is to use teleradiology to enable for the radiologist on call to perform most of his consultations at home. Another is to have sub specialized radiological service available for large are as via teleradiology. Radiological conferences with smaller referring units or practices with no radiologist can be performed without travel if the consultation is made over the telecommunication network.
Most current teleradiological systems are either connected to digital archives or to a video camera or laser digitiser that digitises an analogue film and records the data in a separate teleradiological memory. In the video camera case it is important for the quality of the diagnostic image that possible magnifications of parts of the original image are made through zooming with the video camera and not on the transmitted image. If the magnification is made on the teleradiologically transmitted image the spatial resolution is much lower.
The equipment on the receiving side depends upon the application. Normal and high resolution screens as well as laser printers for films can be used.
The digital radiological department

A digital radiology department only using digital images and screens would have a branched or circular network connecting all involved functions. These are l) image producing units (modalities), 2) image workstations, 3) the archive, and 4) a central or divided computer system.
The image producing units include MRI and CT machines, gamma cameras, digital ultrasound, and image plate systems. In addition, there are digitizing units where analogue images on film will be digitised into the PACS of the department. There is probably also a need for laser printers to produce analogue films to be sent outside the institution.
The image workstations are also of different types. The simplest requiring a minimum of computer power is directly connected to the examination room. It is used as a check to ensure that the image contains the appropriate part of the anatomy, correct projection, etc. The next type is used for demonstration during conferences and may consist of multiple screens placed to resemble a conventional film alternator. Conventional viewing boxes should also be available in the conference area to allow hard copy analogue film.
The third type of workstation is intended for the diagnostic work. The monitor screen has to be of high quality with good resolution and sufficient brightness and frame rate. The advantages of high spatial resolution is lost if the brightness is inadequate and will necessitate a higher monitor frame rate. The computer capacity must be sufficient to perform all types of image manipulations fast. The conferences can be prepared at this diagnostic workstation, with appropriate image manipulation, such as selecting relevant recording of magnified areas of importance, reduced number of, informative images of magnified areas, etc.
The PACS archive requirements differ for the patient/examination demographic database and for the digital image data. The most recent examinations ought to be immediately available and thereafter there is a progressively diminishing retrieval frequency of older images with time. It might be acceptable to wait for a couple of minutes for older films and even longer for educational cases, research material, etc.
Tatsuo Kumazaki and Hans Ringertz
Printer-friendly version Bookmark This Page
Translate page to (By Google): Textbook of Radiology
The liver, biliary tract, pancreas and spleen

1. The liver
2. The biliary tract
3. The pancreas
4. The spleen
Printer-friendly version Bookmark This Page
Translate page to (By Google): The liver, biliary tract, pancreas and spleen The liver
1. Modalities
2. Normal anatomy
3. Pathological conditions
4. Interventional procedures
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version Bookmark This Page
Translate page to (By Google): The liver
Pathological conditions
Benign tumours

The three most important benign tumours of the Liver are cavernous haemangioma, adenoma, and focal nodular hyperplasia. Cysts are frequently seen in the liver. Haemangioma is the most frequently occurring liver tumour, both in adults and children, and is an important lesion to consider in the differential diagnosis of malignant tumours. On US a haemangioma is often seen as a hyper-echogenic localized lesion (Fig. 4). On unenhanced CT it is seen as a low-attenuation lesion but with intravenous contrast medium it exhibits a characteristic enhancement from periphery to centre within a few minutes (Fig. 5), a phenomenon that is particularly evident in large tumours. On MRI a haemangioma shows a high signal intensity on T2 weighted images with similar contrast dynamics to those seen on CT. Fine-needle biopsy of a haemangioma may yield only blood and this finding is not specific. The diagnosis is usually made on a combination of at least two imaging methods but angiography is rarely necessary.
Liver adenomas and focal hyperplasia (Fig. 6) (both of which are reported as being more frequent in females), may be isodense or hypodense on non-enhanced CT, but may show some transient enhancement with contrast medium.
Figure 5. Contrast-enhanced CT of the liver. An initially low-density tumour is seen centrally in the liver (*) (upper left
image). After contrast injection sequential scanning over three minutes shows contrast medium slowly filling in the
tumour from the periphery to the centre. This fin ding is typical of a haemangioma.

Figure 6. MRI of the liver. A high-signal les ion with a dark centre is seen anteriorly in the liver
(arrows) on this sagittal, T1 weighted image. The finding is consistent with the diagnosis of nodular hyperplasia. The kidney is seen to the right, posteriorly.
Cysts of varying sizes are frequently seen in the liver and may be solitary or multiple. Multiple cysts in the liver, pancreas and kidneys are a feature of some specific disorders (e.g. autosomal dominant polycystic disease, von Hippel-Lindau disease). On US a cyst has characteristic features, with well-defined sharp borders, echo-free contents and peripheral echo enhancement. On CT the lesions are well defined, with contents approximating to the dens it y of water and exhibiting no contrast enhancement of either their contents or walls (Fig. 7). Cyst walls may rarely be
Figure 7. CT of the liver. A rounded structure is seen
which has well demarcated walls and whose contents are of water density (*). No
contrast enhancement is noted. These features are typical of a liver cyst. calcified.
Hydatid cysts of the liver are common in endemic areas; they may show a
characteristic appearance, especially on CT, with septa and walls that are frequently
calcified (see Chapter 27).

Malignant tumours Hepatomas or hepatocellular carcinomas are the commonest primary tumours of the liver. They occur with varying frequency in different parts of the world and are commoner in males than females. Cirrhosis and hepatitis B are predisposing factors. They are usually well shown on US, with both hypo- and hyper-echogenic areas (Fig. 8). On non-enhanced CT the tumour may be isodense and identified solely by the fact that it is a space-occupying lesion, but on contrast-enhanced CT the tumour is characterized by an uneven pattern of contrast enhancement, usually with areas of diminished density in the (necrotic) centre. There is often evidence of portal or hepatic venous invasion. It is important for surgical planning to delineate the tumour borders and localize the lesion with respect to the surgical lobar liver anatomy. This also applies to grading of the tumour with reference to any extrahepatic spread. In this respect, MRI may offer some advantage over CT, because of its multiplanar features (Fig. 9). The tumour may require differentiation from a cholangiocarcinoma (Fig. 10).
Figure 8. US of the liver. Subdiaphragmatically there is a large 6 cm tumour (between arrows)
which is of slightly higher echogenicity than the surrounding liver parenchyma, and which is well demarcated from it. These
features are consistent with the diagnosis of a hepatoma.

Figure 9. MRI of the liver (fat suppression STIR
sequence). Posteriorly, a lobulated tumour of high signal intensity is seen, with several
smaller satellite tumours. These features are consistent with the diagnosis of hepatoma.
Figure 10. Contrast-enhanced CT of the liver. Centrally in the liver there is a large tumour (arrows)
with dark areas of central necrosis and mixed attenuation in its periphery. In the ventral part of the liver a separate small
lesion is seen (arrowhead), suggestive of a metastasis. This tumour, however, proved to
be a cholangiocarcinoma,

Figure 11. US of the liver. A large tumour of mixed
echogenicity (between arrows) is seen which is well demarcated from the liver
parenchyma (L). The tumour proved to be a metastasis from a breast carcinoma.
a
Figure 12. CT of liver metastases. (a) Two large,
expanding lesions (arrows) are seen within the liver. They show mixed attenuation and enhancement, with dark areas of necrosis. In addition, two smaller lesions are seen in the lateral segment of the left lobe (arrow-heads). These tumours were metastatic
deposits from an angioneurosarcoma. (b) A 2 cm metastasis (arrows) is demonstrated
as a lesion with decreased contrast enhancement in comparison with the
surrounding liver parenchyma. In this case the contrast medium was injected directly in

b
the superior mesenteric artery, which is said to be the most efficient way to demonstrate small foci in the liver on CT. Note that no
contrast medium is seen in the aorta.
The therapeutic embolization of liver tumours by catheter or direct injection is a technique in widespread use. Its value has not yet been determined with certainty, however, not least because embolization methods are continually evolving - a factor that makes long-term controlled trials difficult to conduct.
Figure 13. MRI of liver metastases. On this T1-
weighted image two metastatic lesions (arrows) are seen, showing varying
signal intensities.
The most frequent malignant tumours in the liver are metastases from other primary carcinomas. On US metastatic deposits may be seen as lesions which may be hypo- or hyper-echogenic in comparison to the surrounding parenchyma, or may show mixed echogenicity (Fig. 11). Metastatic lesions are usually multiple. On CT metastases are often seen as hypodense lesions that remain as such after the injection of contrast medium (Fig. 12). Certain metastases (e.g. hypernephroma) are hypervascular and therefore show increased contrast enhancement. MRI seems to be the most sensitive method for detecting liver metastases and the accuracy of the method may be enhanced by the use of magnetic contrast agents (Fig. 13). CT-portography may also help in the diagnosis of metastases.

Other focal lesions Abscesses usually result from systemic infections, but may also result from a focus of infection elsewhere in the body, or be amoebic in origin. The abscesses may be solitary or multiple and vary in size and shape. On US an abscess is well seen, but the findings are non-specific. On CT abscesses are hypodense, with contrast enhancement of their peripheral wall (Fig. 14). On MRI there may be increased signal intensity on T2weighted images (Fig. 15), with contrast features similar to those seen in CT. Fine-needle biopsy is usually necessary to establish the diagnosis. Percutaneous drainage has become an important alternative to surgery in the treatment of hepatic abscesses.
Trauma to the abdomen may result in rupture of the liver, with the formation of an intraparenchymal and/or subcapsular haematoma. In these
Figure 14. CT of the liver. Two typical abscesses are
demonstrated, one showing a thick abscess wall (large arrow), the other
showing a well demarcated smooth wall (small arrow).
Figure 15. MRI of the liver. On this T2weighted fat
suppression STIRsequence image multiple foci of increased density are seen, the
cause being fungal abscesses of the liver. Only the largest foci were seen on
ultrasound or CT, and this study shows the sensitivity of MRI in detecting small focal
hepatic lesions.

Figure 16. CT of liver trauma. Contrast enhancement
brings out the hepatic veins, and CT demonstrates decreased perfusion of the right lobe of the liver, demarcated by the middle hepatic vein (arrow). This finding
indicates that the artery of the right hepatic lobe is severed. A traumatic rift is also seen in the left lobe in the region of the
falciform ligament. .
Figure 17. US of fatty liver. The echogenicity of the liver is coarse and clearly increased in
comparison with normal liver (the so-called "brightliver "-pattern). L = liver; K = kidney
cases the other parenchymal organs have to be studied for traumatic lesions as well, On US a rupture of haematoma is seen as a hypo-echoic area. The imaging method of choice in traumatic cases is contrast-enhanced CT (Fig. 16), which makes it possible to differentiate between haematoma, other fluid collections (bile) and normal parenchyma. On MRI a haematoma is seen usually as a lesion with increased signal. Since many focal liver lesions, with the exception of cysts, do not show diagnostically characteristic features on any imaging method, fine-needle biopsy

verification is usually essential to establish the diagnosis. For some liver disorders a cutting-needle biopsy may be preferable and this can be obtained with embolization of the track, particularly if there is a likelihood of haemorrhage (see below).
Parenchymal disease Fatty degeneration of the liver is fairly common, especially with certain diseases such as alcoholism, diabetes or chronic infections. On ultrasound this condition may give increased echogenicity of the liver parenchyma ("bright liver") (Fig. 17). CT allows direct dens it y measurements of the liver, and since fat shows low attenuation this permits quantitative evaluation of the disease (Fig. 18). The degree of fatty
Figure 18. CT of fatty liver. The attenuation of the liver is
markedly reduced, and clearly less than that of the spleen, a feature evident even without contrast enhancement. Note that the hepatic veins are visible against the dark liver parenchyma even
without contrast enhancement. The density of the liver parenchyma (ROI 1) was measured as -5, 7 HU, and that of the spleen (ROI 2) as 37,5 HU. Very low and even negative attenuation values
may be seen on CT of a fatty liver.
infiltration may change rather rapidly, according to the stage of the underlying disease. An attenuation of less than 30 HU is a clear indication of fatty infiltration. The changes may only be segmental or focal. Other focal lesions such as tumours or metastases, are well seen in a fatty liver, since they have normal density. A fatty liver is usually larger than a normal liver. Liver cirrhosis may vary in appearance and depending on its aetiology the liver may be either smaller or larger than normal. Dynamic CT may show pathological patterns of perfusion of the liver and spleen, which may also be seen on colour Doppler US.
Clinical information is also important in the evaluation of parenchymal liver disease.
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version

Bookmark This Page
Translate page to (By Google): The liver
Modalities
With the introduction of cross-sectional imaging methods such as US, CT, and MRI, direct imaging of the liver parenchyma became possible where previously only angiography and radionuclide imaging had been available.
Ultrasonography Because of the location, size and structure of the liver, US is very well suited for imaging its parenchyma and is therefore usually the first method employed. It is widely available, easily performed and has no contraindications. An excessive amount of bowel gas may degrade the study. Ultrasound gives information on the size and structure of the liver and demonstrates both localized lesions (e.g. hepatic tumours, cysts and abscesses) and diffuse disease. Intrahepatic structures, such as portal vessels and biliary ducts can be identified. The vascular systems in the liver may be studied with Doppler US, which can give important differential diagnostic information especially when a colour-system is used (Fig. 1).
Figure 1. US of the liver. The normal echo pattern of the liver is demonstrated. The echo-
free, tubular structures within the liver are hepatic veins (arrows).

Computed tomography A CT study of the liver entails imaging of the entire organ from its superior border at the dome of the diaphragm to its caudal tip. Contiguous 10 mm thick slices are obtained, usually before and after the intravenous injection of contrast medium (Fig. 2). Because of its iron content, the density of the liver is slightly higher than that of other intra-abdominal organs, usually of the order of 65 ± 5 HU. Most pathological lesions have a density less than that of normal parenchyma. This difference is accentuated following a contrast medium injection, but because of pharmacodynamic considerations care has to be taken to perform the enhanced study during a narrow time window of 30-60 seconds following the bolus injection of contrast medium. Because of the size of the liver, the contrast injection may have to be repeated in order to study the entire organ but this requirement has diminished considerably since the advent of fast CT scanning and spiral CT. Sequential scans at a single, predetermined level after a bolus of contrast medium are useful for determining contrast enhancement dynamics, which are of decisive importance in the diagnosis of, for example, a haemangioma.
a
b
Figure 2. CT of the liver. (a) Without i. v. contrast enhancement the texture of the liver is
even. The blood vessels are seen faintly as low-attenuating structures against the liver parenchyma. The attenuation of the
liver (l) is equal to that of the spleen (s). (b) After i.v. contrast enhancement the
attenuation of the liver increases, as does that of the spleen. The hepatic veins are now clearly visible as highly attenuating (white) structures and are well discerned
against the liver parenchyma. On this scan contrast medium is also seen in the aorta
(a).
The size of the liver and information on both focal and diffuse parenchymal disease are all clearly evaluated by CT. Newer CT technology has also made it

possible to visualize blood vessels (CT -angiography, CT -portography) and to perform 3-dimensional reconstructions which are important in studying anatomically complex areas, such as the liver hilum. Magnetic resonance imaging
MRI is, in many respects, equal to CT in imaging of the liver. It has, however, certain advantages, that probably make it the best available method for studying disease in this organ. The free choice of imaging planes permits better anatomical orientation (Fig. 3) and the utilization of multiple imaging sequences facilitates the identification of smaller lesions, especially those associated with oedema. MRI gives new information on parenchymal and metabolic disease, 3-dimensional imaging enables visualization of, for instance, the biliary tree and the liver hilum,
Figure 3. MRI of the liver. In these T1-weighted images the anatomy of the liver is well displayed in the transverse, sagittal and coronal projections. The portal and hepatic veins are seen
as dark tubular structures.
and MR -angiography delineates the blood vessels. Various types of magnetic and paramagnetic contrast media that increase the signal intensity of either the lesion or the parenchyma, add significantly to the precision of MR studies. Drawbacks of MRI include its sensitivity to movement artefacts, and the rather long duration of study, though with new technology and rapid sequences examination times can be considerably reduced. MR spectroscopy may become clinically useful in the study of, for example, metabolic liver disease.
Angiography Arteriography us ed to be the most precise method for evaluating liver disease, but its diagnostic use is now limited to the investigation of certain special problems such as the pre-operative mapping of liver vessels or the detailed evaluation of certain liver tumours.

Therapeutic angiography is particularly important in the liver as the organ has a dual blood supply (making embolization a relatively safe procedure) and interventional procedures are associated with a far lower morbidity than surgery in a variety of circumstances such as acute arterial bleeding and porto-systemic shunting. Hepatic venography is valuable in the evaluation of the Budd-Chiari syndrome.
Percutaneous transhepatic portography is used for studying the portal circulation or for venous sampling of the pancreas. The use of this approach for the embolization of varices is now virtually obsolete except in the most special circumstances.
Radionuclide imaging Radionuclide imaging used to be an important method for studying the liver, particularly focal lesions in the organ, but it has diminished in importance mainly because of its poor spatial resolution and non-specificity in comparison with other methods. Nevertheless, several specialised agents may be useful for imaging specific pathology, such as radiolabelled leucocytes for intrahepatic abscess, In-III octreotide for GFP tumours metastasing to the liver, and 1-123 SAP (serum amyloid P component) for hepatic amyloidosis. Hepatic haemangioma is a lesion which is characteristically associated with low blood flow but high blood volume and may be diagnosed by dynamic Tc-99m labelled red cell imaging.
Biliary imaging Proper evaluation of the liver frequently requires imaging of the biliary tract. This is considered separately in the succeeding section.
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version Bookmark This Page
Translate page to (By Google): The liver
Interventional procedures
One of the commonest and important interventional techniques is guided fine-needle biopsy which is most easily performed under US-contral (Fig. 19). Needle biopsies are important, since neither focal nor diffuse liver disease necessarily exhibit diagnostic features on imaging. In some disorders a cutting needle biopsy is required and in patients with abnormal coagulation parameters this is most

safely obtained using either the transjugular approach or a percutaneous technique with embolization of the biopsy track after obtaining the specimen.
The drainage of liver abscesses or sub-phrenic abscesses is another important interventional technique that has greatly reduced the need for
Figure 19. US guidance of fine needle biopsy. A
percutaneous fine needle biopsy of a liver tumour is demonstrated, showing the echo from the needle (curved arrows) within the tumour (between straight arrows). Normal
liver parenchyma (L) is seen to the left.
surgery in the management of such lesions. Liver tumours may be treated by embolization or direct ethanol injection. Both methods are under investigation. Embolization can be particularly useful in the palliative treatment of functioning endocrine metastases in the liver. Hepatic bleeding from trauma, biopsy, aneurysm or other causes is often most effectively treated by embolization. In institutions with the requisite interventional expertise, embolization is the treatment method of first choice for most types of hepato-biliary haemorrhage.
here are a number of interventional procedures such as percutaneous transhepatic portography and percutaneous transhepatic cholangiography that use the liver as the most suitable access point. Through these routes a number of interventional procedures may be performed, described elsewhere in this book. Another important new technique is that of percutaneous porto-systemic shunting (TIPPS).
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam

Printer-friendly version Bookmark This Page
Translate page to (By Google): The liver, biliary tract, pancreas and spleen The biliary tract
1. Introduction
2. Modalities
3. Normal anatomy
4. Pathological conditions
5. Interventional procedures
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version Bookmark This Page
Translate page to (By Google): The biliary tract Introduction
Imaging the gallbladder has changed dramatically in the past two decades. Peroral cholecystography used to be, and in some countries still is, the primary method for studying the gallbladder. In recent years, however, ultrasonography has almost completely replaced this technique. Ultrasonography is also important in imaging the biliary ducts, but a complete assessment still relies on their opacification with contrast medium.

David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version Bookmark This Page
Translate page to (By Google): The biliary tract Modalities
Ultrasonography The gallbladder is studied by US with a 3.5-5 mHz transducer. The organ is studied in both its longitudinal (Fig. 20) and transverse axes, with the patient lying supine. Views are also obtained with the patient turned to the left and upright views are sometimes required. Positional changes help in the diagnosis of gallstones that move with gravity. The extrahepatic biliary ducts are well seen by US, but the intrahepatic ducts are more difficult to image unless they are dilated. The most distal part of the common bile duct is not usually seen, because of interference with the image by gas in the duodenum. The overall diagnostic accuracy of US of the gallbladder is 90-95%.
Peroral cholecystography Peroral cholecystography was the primary method for imaging the gallbladder for over 50 years (since its introduction in 1925), until ultrasonography largely replaced it in the early 1980's. In some departments, however, oral cholecystography is still employed (Fig. 21).
In peroral cholecystography the contrast medium is administered by mouth as tablets, absorbed through the intestinal mucosa, bound to albumin in the blood and transported to the liver. From the liver the medium is excreted into the biliary ducts and concentrated in the gallbladder. Sodium ipodate and calcium ipodate, however, are concentrated by the liver and are thus not dependent on the gallbladder's concentrating

Figure 20. US of the gallbladder. The normal gallbladder (gb) is seen as a cystic
structure with echo-free contents. The walls of the gallbladder are smooth.
Normal liver parenchyma (L) is seen to the left of the gallbladder.
a
b
Figure 21. A normal cholecystogram. (a) In the initial
phase the contrast medium is seen evenly filling the gal/bladder, the walls of which are smooth. (b) After a fatty meal, the gallbladder has contracted. Now both
the fundus and the neck of the gallbladder, as well as the cystic duct is
filled with contrast medium and the common bile duct is demonstrated
(arrows).
capacity. When its iodine content exceeds 0.5% the gallbladder is visible on fluoroscopy and conventional radiographs. The concentration of contrast medium reaches its maximum 10-15 hours after ingestion and imaging usually takes place on the day following ingestion. Some centres advocate a scheme whereby

a double dose of contrast medium is ingested on two consecutive days before the study. Non-opacification of the gallbladder may indicate gallbladder disease, such as obstruction of the cystic duct. It may, however, also result from liver disease or disorders resulting in disturbances in the absorption of contrast medium from the gut, e.g. diarrhoea. Sometimes the patient may not even have taken the contrast medium or there may have been a previous cholecystectomy. Gallstones are seen as filling defects in the opacified gallbladder. Most gallstones contain some calcium, and in 15-20% of cases this is enough for the stones to be seen on a plain radiograph.
The gallbladder is radiographed in multiple projections including same using external compression. The study is often completed by exposing a so-called contraction film of the gallbladder 1/2-1 hour after the ingestion of a fatty meal. This may show the changes of adenomyomatosis or cholesterolosis.
The diagnostic accuracy of cholecystography in diagnosing gall-stones is 85-90%, i.e. slightly less than that of US though the methods are to some extent complementary. The use of peroral cholecystography has undergone a modest revival with the increasing popularity of non-operative methods of treating gallstones.
Cholangiography, biligraphy Visualization of the extrahepatic biliary ducts may require the intravenous administration of contrast medium. On intravenous cholangiography the contrast medium is given intravenously as a slow infusion for approximately 1/2 hour. The contrast medium is bound to the albumin in the blood and excreted by the liver into the bile. The concentration of contrast medium in the biliary tree is usually so low that the ducts can only be demonstrated by tomography. Some contrast material is also seen in the gallbladder, but since it is immiscible with bile and forms a separate layer in the organ, the method is unsuitable for the diagnosis of gallbladder disease or stones. Allergic reactions may still occur on intravenous cholangiography, and the mortality is not insignificant. The diagnostic accuracy of the method is only 50-60% and it should be employed only when good indications exist and in those cases where other available methods (US, ERC, PTC, CT) are unhelpful. There has been some renewed interest in this technique in patients prior to laparoscopic cholecystectomy.
Percutaneous transhepatic cholangiography Percutaneous transhepatic cholangiography (PTC) (see Fig. 35) entails the puncture of an intrahepatic biliary duct, by a percutaneously introduced needle. The procedure is performed under US guidance, and is successful in 95-98 % of subjects with dilated ducts and 80 % of those with non-dilated ducts. The biliary ducts are filled with contrast medium through the needle. The frequency of complications is not insignificant, but depends on the type of needle used. With a Chiba needle it is approximately 2 %. Through the needle a guide wire can be

negotiated into the biliary ducts, for the introduction of various catheters or instruments (see Chapter 8).
Endoscopic retrograde cholangiography Endoscopic retrograde cholangiography (ERC) (see Fig. 36) entails cannulation of the papilla of Vater through an endoscope introduced via the stomach into the duodenum. Contrast medium (low osmolar) is injected through the cannula retrogradely into the common bile duct filling the extra- and intrahepatic biliary ducts and the pancreatic duct. The contrast medium injection is performed under fluoroscopic control. Overdistension of the biliary tree and especially the pancreatic duct should be avoided; in the latter case it may cause pancreatitis. Radiographs are exposed in various projections when the injection is complete. The study requires an experienced endoscopist and has an 80-90% success rate. Care should be taken not to introduce air into the biliary tree, since air bubbles may be mistaken for stones; bubbles, however, are always round and move freely with gravity into the uppermost part of the duct when the patient is moved into an upright position.
Peroperative cholangiography Peroperative cholangiography is performed in the operating theatre during operative procedures involving the biliary ducts, and entails the injection of contrast medium directly into the exposed biliary ducts through a needle or cannula. Several injections may be necessary during the study for maximum diagnostic benefit. Peroperative cholangiography is performed in order to diagnose or exclude the existence of concretions in the biliary tree or to demonstrate a biliary leak. It is also occasionally used to record biliary tract anatomy. In many centres it is performed routinely during cholecystectomy. Care should be taken to avoid the introduction of air bubbles into the biliary tracts (see section on ERC).
Postoperative cholangiography Postoperative cholangiography entails the injection of contrast medium through the T -tube used to decompress the biliary tree following operative procedures. The procedure is usually performed 7-10 days after cholecystectomy to check for any residual biliary concretions. The contrast medium should be diluted so that small stones are not obscured. The procedure is performed under fluoroscopic control and films are exposed in various projections. Care should be taken to avoid the introduction of air into the biliary tract, since this may simulate stones (see section on ERC).
Radionuclide imaging Radionuclide imaging or gammascintigraphy is performed to evaluate biliary dynamics. The most commonly used agent is 99m Tc-HIDA which is injected intravenously, where it is bound to albumin and then excreted through the liver into the bile. The activity over the liver, biliary ducts and small intestine is

sequentially recorded using a gamma camera. The study gives information on hepatic function and biliary flow. It may show reduced flow in, for example, strictures of the biliary tree or calculus obstruction, non-filling of the gallbladder in obstruction of the cystic duct, or leakage of bile from the biliary tree. In normal subjects the study takes approximately one hour, but it may take up to 24 hours if the flow of bile is retarded. Radionuclide imaging of the biliary tree has lost much of its importance with the introduction of other imaging methods, such as US, CT and MRI, but may still be useful in special cases where information on biliary dynamics is important, where direct visualization of the biliary tree with injected contrast medium is unsuccessful, or if the patient is strongly allergic to contrast medium.
Magnetic resonance imaging The value of MRI has yet to be established in the study of the biliary ducts but newer techniques that permit so-called MRI-cholangiography may be valuable in the near future. In gallbladder cancer MRI may be important in both diagnosis and staging.
Choice of imaging method Ultrasonography has become the primary imaging technique in the evaluation of the gallbladder. It has the advantages of being precise, easy and quick to perform. It gives information on the contents and wall of the organ, as well as the surrounding tissues. Stones, cholesterolosis, adenomyomatosis, inflammation and tumours are all diagnosed with great precision. Peroral cholecystography is still used in many centres, as being a relatively easily performed and accurate diagnostic method, especially in calculus disease. It is still a useful secondary method if the findings on US are unclear, if there is a discrepancy between the clinical assessment and the US findings, or if non-operative treatment of gallstones is planned. Computed tomography is performed if gallbladder cancer is suspected.
Ultrasound is also the primary method for studying the intrahepatic and proximal extrahepatic biliary ducts, giving information on ductal calibre. This is important when studying an icteric patient for example, when it can distinguish between extrahepatic obstruction and intrahepatic disease. CT gives additional information concerning the biliary tree and surrounding structures, PTC or ERCP direct information concerning the biliary tree.
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam

Printer-friendly version Bookmark This Page
Translate page to (By Google): The biliary tract Normal anatomy
The biliary ducts The intrahepatic biliary ducts from the right and left lobes unite at the hilum to form the common hepatic duct. This lies to the right of the hepatic artery and ventral to the portal vein. The hepatic duct runs caudally and medially towards the duodenum. The cystic duct, 3-4 cm in length, joins the hepatic duct to form the common bile duct. This is 6-8 cm long and approximately 6 mm wide. The common bile duct and the portal vein both lie in the hepatoduodenal ligament. The most distal part of the common bile duct runs in the head of the pancreas, surrounded by pancreatic tissue, before it joins the pancreatic duct from the right to run into the duodenum in the major papilla of Vater.
The gallbladder The gallbladder lies on the inferior surface of the liver, and its own inferior surface is covered by peritoneum. The organ is 7-10 cm long and 3 cm in diameter with a volume of 30-50 ml. The thickness of its wall is 2-3 mm. The fundus of the gallbladder points ventrally and the neck runs dorsally into the cystic duct.
Gallbladder anomalies occur, the commonest being a septum, usually situated in the fundus which partially divides the organ (the "Phrygian cap"). Very infrequently agenesis occurs resulting in absence of the gallbladder. Duplication or even triplication of the gallbladder may occur but these anomalies are very rare.
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version Bookmark This Page
Translate page to (By Google): The biliary tract Pathological conditions

Gallbladder
Gallstone disease
Stones or concretions frequently occur in the gallbladder. Clinically the stones do not occur in isolation, but form part of an entity, gallstone disease. Stones occur about twice as frequently in women as in men. The majority of stones are cholesterol stones and less than 10% are pigment stones. Approximately 15-20% of calculi contains calcium and can be seen on a plain radiograph (Fig. 22). US is the primary method for identifying gallstones. A stone is seen as a rounded, echodense structure, with a typical acoustic shadow behind it (Fig. 23). Sometimes, especially if the gallbladder is small and deformed, only the acoustic shadow is seen, the stone itself being difficult to visualize. There are a multitude of US features associated with the presence of gallbladder stones and the accuracy of detection of stones on US is very high, approximately 95-98%. In contrast, stones in the extrahepatic bile ducts may be difficult to visualize on US, bowel gas often interfering with interpretation. Oral cholecystography has traditionally been regarded as one of the most accurate radiological methods so far as the diagnosis of gallstones is concerned but its accuracy is only 85-90%. Gallstones are seen in the contrast-filled gallbladder as dark filling defects (Fig. 24). The drawback with

Figure 22. Gallstones containing calcium may be seen
on a plain film, without contrast medium. Here several gallstones are seen as a row of
white circles on an abdominal overview roentgenogram.
Figure 23. US of a gallstone. The gallbladder (gb) is
seen as a dark, echo-free cystic structure. It contains a stone (arrow) giving distal acoustic shadow ing (arrowheads).

cholecystography is that a diseased gallbladder does not concentrate contrast medium, which means that in circumstances in which the gallbladder wall is inflamed or fibrotic, or the cystic duct obliterated, the organ
Figure 24. Cholecystogram showing multiple gallstones,
which are seen as filling defects in the contrast-filled gallbladder.
Figure 25. Floating gallstones, seen as a layer of filling defects in the contrast-filled gallbladder with
the patient erect.
remains unopacified. Ultrasound is not dependent upon contrast medium concentration and demonstrates calculi irrespective of the presence of other

gallbladder disorders. Plain film or CT scanning may give some clues as to the likely composition of stones. Cholesterol stones are usually uncalcified but if calcium is present it often occurs as a ring-like structure in the stone. In pigment stones the calcium is usually centrally located. Cholesterol stones may be lighter than the contrast-filled bile
Figure 26. US of acute cholecystitis. The gallbladder
(arrows) is filled with echogenic biliary sludge, and there is a stone (arrowhead)
giving an acoustic shadow.
and may thus be "floating" on oral cholecystography; they may also form a layer in the contrast-filled gallbladder, which is seen when a film is exposed with the patient in the upright position (Fig. 25). In cholesterol stones gas- filled fissures may be seen as dark linear structures - the so-called Mercedes- Benz sign. Cholecystitis Cholecystitis may be acute or chronic. Acute cholecystitis used to be a diagnosis in which imaging was unhelpful. Peroral cholecystography could only show that the gallbladder was "non-functioning" as the inflamed organ does not concentrate oral contrast medium. Fortunately, the situation is now very different.
Ultrasound has become the primary method for imaging acute cholecystitis, because the technique demonstrates not only the gallbladder wall and its contents, but also the adjacent tissues (Fig. 26). On US an inflamed gallbladder wall appears thicker than normal (over 3 mm) and with good technique even the various layers of the wall may be identified. Other diseases such as pancreatitis and liver disease, however, may also cause thickening of the bladder wall. Changes in the surrounding tissues may include oedema or fluid collections. On US the organ can be palpated under visual control, and may be tender, the so-called "ultrasound Murphy's sign". The gallbladder often contains gallstones (present in 90-95 % of cases) or sedimentation of its contents ("sludge"), but

Figure 27. Porcelain gallbladder. The walls of the
gallbladder are calcified, and visible on the plain film without contrast medium; this
phenomenon may be seen as a sequela to chronic cholecystitis.
Figure 28. Limey-bile. As a sequel of chronic
cholecystitis, the gallbladder may contain calcified biliary "sludge", which is here visible
on a plain film, without the patient having taken contrast medium.
these are non-specific findings which may occur in the absence of cholecystitis.

Conversely, in so-called acalculous cholecystitis, stones are not present although the other signs of acute cholecystitis described above are often present. CT may show the same findings as US and though the information given by CT is often not as detailed and precise as that given by ultrasound, any changes present in the surrounding tissues may be
Figure 29. US of the gallbladder. The gallbladder wall is
thicker than normal and slightly uneven. There are several rounded polypoid
structures (arrows) arising from the bladder wall and protruding into the bladder lumen. These structures do not show any acoustic
echo. The findings are compatible with hyperplastic cholecystosis.
better shown on CT. A radionuclide study performed with 99m Tc-HIDA may show non-activity over the gallbladder, as a sign of cystic duct obstruction. As a sequela to chronic cholecystitis, the gallbladder wall may calcify and appear on the plain film as a so-called "porcelain gallbladder" (Fig. 27). For the same reason the organ may contain calcified "sludge" which is also visible on the plain film, i.e. "limey bile" (Fig. 28).
Hyperplastic cholecystoses

Cholesterolosis and adenomyomatosis belong to a group of disorders termed the hyperplastic cholecystoses, which share the feature of polypoid lesions of the gallbladder wall. The term cholesterolosis implies the presence of polypoid deposits of cholesterol in the bladder mucosa ("strawberry gallbladder"). In adenomyomatosis there are epithelial mucosal sinuses ("Rokitansky-Aschoff sinuses") extending between polypoid formations of localized muscular hypertrophy; these sinuses may vary greatly in size from the minute to the very large. If the polyps are bigger than 1 mm, they will show on both ultrasound and peroral cholecystography as typical lesions protruding from the surface of the wall into the bladder lumen (Fig. 29). Larger polyps may be difficult to distinguish from stones, but stones usually move with changes in posture
a
Figure 30. Gallbladder carcinoma. (a) US of the
gallbladder. There is an exophytic growth of a lobulated tumour (*) into the
gallbladder (gb), with infiltration of the tumour beyond the gallbladder wall. This
tumour did not move with changes in posture. These features are suggestive of gallbladder carcinoma. (b) CT of the same patient shows the tumour (arrow) extending
into the gallbladder. Possible tumour infiltration into the surrounding liver cannot
be visualized even on this contrast-enhanced CT scan.

b
whereas polyps do not. Furthermore, on US there is no acoustic shadow behind a polyp.
Gallbladder carcinoma Gallbladder carcinoma is relatively rare, seen in approximately 0.1 % of patients with gallstones. On US a carcinoma may be seen as a space-occupying lesion in the gallbladder area, as a hypo-echoic mass within the gallbladder, or as a generalised thickening of the bladder wall (Fig. 30). It is important to note any extension of the tumour into the surrounding

Figure 31. Intravenous eholangiography (tomography)
shows dilated extrahepatie biliary duets. Distally in the eholedoehal duet an
obstrueting eoneretion is seen as a filling defeet (arrows).
tissues but this may be difficult to define on US. Peroral cholecystography is not usually helpful, because of non-visualization of the gallbladder. CT may show similar changes to ultrasound but usually demonstrates the extent of the tumour better than the latter technique and should always be obtained in order to assess the potential operability of the lesion.
Biliary duct disease Gallstones in the extra-hepatic biliary ducts are difficult to evaluate by US, which has an accuracy of 20-50% in this examination. The biliary tree is difficult to visualize throughout its length and the common bile duct in particular may be obscured by bowel contents and gas. A sto ne in a normal duct, under 6 mm, may be difficult to discem, whereas a stone in a dilated duct is easier to see. In non-diagnostic or doubtful cases contrast media studies such as intravenous cholangiography (Fig. 31), ERC or PTC should be undertaken. Thin-slice computed tomography may also be helpful but without oral contrast medium (which may obscure a calculus in the lower common bile duct). Peroperative and postoperative cholangiography is performed to rule out or diagnose residual stones in the biliary ducts (Fig. 32). Stenosis or obstruction of the extrahepatic ducts is sometimes seen as a consequence of trauma occurring during abdominal operations involving the biliary

a
Figure 32. (a)Peroperative needle cholangiography
reveals multiple sto nes in the extrahepatic biliary ducts, seen as roundedfilling
defects. The needle is marked by arrows. (b)Postoperative T-tube cholangiography
reveals several residual sto nes in the intra and extrahepatic biliary ducts (arrows). The T-tube is marked by arrowheads.

b
tree, such as a cholecystectomy (Figs. 33,34). Most obstrueting lesions are, however, tumours (fig. 35), principally carcinoma of the head of the panereas. Sclerosing cholangitis causes multiple strietures in both the intra- and extrahepatic ducts (Fig. 36). In Caroli's disease there are ectatic dilatations ofthe intrahepatic ducts. A choledochal cyst shows as an area of dilatation of the distal choledochal duct (Fig. 37). All these changes are best shown on endoscopic or percutaneous cholangiography.

Figure 33. Endoscopic retrograde cholangiography.
Contrast medium has been introduced in a retrograde fashion through cannulation of
the papilla of Vater. The endoscope is seen in the picture. There is a post-operative
stricture in the hepatic duct (arrow) and a stone (arrowheads) is seen as a filling defect
in the dilated biliary ducts above the stricture.

a
b
Figure 34. A patient who had undergone a previous
transduodenal papillotomy, presented with jaundice and epigastric pain. (a) Ultrasonogram, showing dilated
intrahepatic biliary ducts, seen as dark, branching streaks in the liver parenchyma. (b) Endoscopic retrograde cholangiography
demonstrates dilated intra- and extrahepatic biliary ducts and a very tight narrowing of the distal sphincter area. At
autopsy purulent cholangitis was diagnosed, the common bile duct
measured 3 cm in diameter and had a fibrotic narrowing at its distal end,
extending for 3 cm above the papilla of Vater.

Figure 35.Percutaneous transhepatic cholangiography shows narrowing
(between broad arrows) of the biliary ducts in the area of the liver hilum and the
proximal hepatic duct. The biliary ducts in both the right and the left liver lobes are dilated above the central narrowing (fine
arrows). Note absence of filling of the gallbladder. The patient presented with
jaundice, colourless stools and epigastric pain. Cholangiocarcinoma.
Figure 36. ER CP. There are several areas of narrowing of both the intra- and extrahepatic ducts (arrows), compatible
with sclerosing cholangitis. The patient had had ulcerative colitis for several years.

Figure 37. Peroperative cholangiography. A cystic
dilatation (arrows) of the most distal segment of the common bile duct is
demonstrated on this left oblique image. The finding is compatible with a
choledochocele or choledochal cyst.

a
Figure 38.Stenting of biliary duets. (a) A short stricture is seen in the liver hilum (arrow) on an ERCP of a patient with
Klatzkin-tumour. Dilatation of the proximal intrahepatic bile duets is noted. (b) A stent
(arrows) has been introduced via the endoscope into the biliary duet and
through the stricture, the proximal end of the stent lodging in the confluence of the intrahepatic bile duets above the stricture
and its distal end in the duodenum.

b
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam
Printer-friendly version Bookmark This Page
Translate page to (By Google): The biliary tract Interventional procedures

The biliary ducts may be approached in a number of ways; retrogradely through the papilla of Vater, antegradely by means of percutaneous transhepatic puncture or through the gallbladder.
A sphincterotomy or papillotomy may be performed through an endoscope, and this facilitates the passage of gallstones from the extrahepatic ducts into the duodenum; the technique can be used in poor-risk patients.
Figure 39. Cholecystostomy. A drainage tube has been
introduced percutaneously into the gallbladder. The draining catheter has
slipped out of the gallbladder and its tip now lodges in a fistula from the gallbladder to the
skin.
The transhepatic approach allows the institution of either external or internal biliary drainage and can also be used for the percutaneous introduction of instruments for the dilatation of stenosed biliary ducts. The same treatment may also be performed via the endoscopic route (Fig. 38). The gallbladder can be percutaneously punctured and drained through a catheter, a technique that is particularly suitable in those cases of acute cholecystitis where surgery is thought to be inappropriate (Fig. 39).
David J. Allison and Carl-Gustaf Standertskjold-Nordenstam

Echogenicity Ability to create an echo, i.e. return a signal in ultrasound examinations.
Fatty liver A liver with fat deposits, making it yellowish and softer than a normal liver. May have many causes, but is most often the result of alcoholism.
GE Healthcare Glossary
Contrast media (sing. medium) (CM) Chemical substances, containing chemically bound iodine, used to highlight tissues and organs that are not distinguished from their surroundings on plain X-ray pictures. Usually injected with a needle into an arm vein, or directly into an artery via a catheter inserted into an artery in the groin and moved to the target organ/tissue. Other types of contrast media are based on barium, and are used to highlight the stomach and/or gut, and can either be swallowed or given as an enema. Contrast media are also used in MRI, but most of these are based on a metal called gadolinium Ideally a contrast medium should not have any effects at all except the physical ability to influence the diagnostic technique, in the case of X-ray contrast media the ability to absorb X-rays. All pharmacological effects are unwanted and they are expressions of toxic effects. Toxic effects of contrast media may be divided into osmotoxic effects and chemotoxic effects. Chemotoxicity is related to the toxicity of the molecule and may be linked to high binding of plasma protein, high tendency to release histamine, inhibition of biological functions like coagulation etc. Most frequently, high chemotoxicity will clinically show itself as a high incidence of nausea and vomiting. CM are also called contrast agents.
Chemotoxicity The part of the toxic effect of contrast media that is related to the chemical properties of the molecule. A high chemotoxicity in contrast media is associated with a high degree of protein binding, a high tendency to release histamine or to inhibit biological processes like enzymes. The inhibition of clotting by ionic contrast media is a consequence of high chemotoxicity. Contrast media with high chemotoxicity will have higher general toxicity (low LD50) regardless of osmolality. Adverse events during X-ray examinations typically associated with chemotoxicity include nausea and vomiting.
GE Healthcare Glossary

LD50 LD50 is the abbreviation of "lethal dose in 50%", i.e. the dose of a substance that will kill 50% of an animal population. The higher the LD50 of a substance, the more is needed to kill an animal, which again means a higher safety margin. For most new drugs and contrast media the safety margin is established in an early phase of development by means of LD50. Usually LD50 is measured in small populations of small animals like mice or rats.
GE Healthcare Glossary
MedcycloPoll
Did you get the help you required from Medcyclopaedia™ during today's visit? Yes (84.9%) No (10.5%) Undecided (4.6%)
You must be logged on to vote. Please log in or register.
helpadvanced search
Library / Glossary / Modality previous in index · next in index
Printer-friendly version Bookmark This Page
Translate page to (By Google): Modality The 4 medical imaging techniques: X-ray (incl. CT), Nuclear Medicine, ultrasound and MRI.
Each modality is an imaging technique with different features that, under various conditions, reveal particular properties of the part of the body examined.
With x-ray, electromagnetic radiation is sendt through the body, with MRI the body is caused to transmit radio signals (on the FM bandwidth), in nuclear medicine radioactive substances are injected into the body and in ultrasound, high frequencey sound waves are reflected by the body.
The signals reflected/transmitted by the body are recorded by computers to produce an image of the structures examined.
GE Healthcare Glossary

Metastasis A "daughter" or secondary tumour. One feature of malignant tumours is their tendency to metastasise. This can happen spontaneously e.g. if one or a few tumour cells break off the "parent" or primary tumour and follow the blood stream to other organs or body parts. Organs most likely to get metastases from tumours elsewhere in the body are the liver, kidneys and brain, but metastases may be found anywhere in the body. Typically metastases tend to be multiple. Therefore it is important to use imaging techniques that will show up all metastases, including the very small ones.
GE Healthcare Glossary
Nephrotoxicity Disturbances of the kidney function. Conventional ionic contrast media may significantly reduce the glomerular filtration and affect the tubular function. This risk should be kept in mind particularly when using large contrast volumes or when the patient is to have repeat contrast medium injections within a short time, and it is advisable to check the kidney function before further contrast procedures are performed. Non-ionic and isosmolar contrast media have a very low risk of causing loss of kidney function, only very minor changes have been shown in well controlled clinical trials. Patients in whom kidney function is already impaired are more vulnerable to further kidney function damage. With the large variation between patients, it is advisable to check kidney function before subjecting patients to large contrast doses on consecutive days.
GE Healthcare Glossary
Nephrotoxic Effects in High-Risk Patients Undergoing Angiography Aspelin,P et al. N Engl J Med 2003;348:491-9 Background The use of iodinated contrast medium can result in nephropathy. Whether iso-osmolar contrast medium is less nephrotoxic than low-osmolar contrast medium in high-risk patients is uncertain.
Methods We conducted a randomized, double-blind, prospective, multicenter study comparing the nephrotoxic effects of an iso-osmolar, dimeric, nonionic contrast medium, iodixanol, with those of a low-osmolar, nonionic, monomeric contrast medium, iohexol. The study involved 129 patients with diabetes with serum creatinine concentrations of 1.5 to 3.5 mg per deciliter who underwent coronary or aortofemoral angiography. The primary end point was the peak increase from base line in the creatinine concentration during the three days after angiography. Other end points were an increase in the

creatinine concentration of 0.5 mg per deciliter or more, an increase of 1.0 mg per deciliter or more, and a change in the creatinine concentration from day 0 to day 7.
Results The creatinine concentration increased significantly less in patients who received iodixanol. From day 0 to day 3, the mean peak increase in creatinine was 0.13 mg per deciliter in the iodixanol group and 0.55 mg per deciliter in the iohexol group (P=0.001; the increase with iodixanol minus the increase with iohexol, –0.42 mg per deciliter [95 percent confidence interval, –0.73 to –0.22]). Two of the 64 patients in the iodixanol group (3 percent) had an increase in the creatinine concentration of 0.5 mg per deciliter or more, as compared with 17 of the 65 patients in the iohexol group (26 percent) (P=0.002; odds ratio for such an increase in the iodixanol group, 0.09 [95 percent confidence interval, 0.02 to 0.41]). No patient receiving iodixanol had an increase of 1.0 mg per deciliter or more, but 10 patients in the iohexol group (15 percent) did. The mean change in the creatinine concentration from day 0 to day 7 was 0.07 mg per deciliter in the iodixanol group and 0.24 mg per deciliter in the iohexol group (P=0.003; value in the iodixanol group minus the value in the iohexol group, –0.17 mg per deciliter [95 percent confidence interval, –0.34 to –0.07]).
Conclusions Nephropathy induced by contrast medium may be less likely to develop in high-risk patients when iodixanol is used rather than a low-osmolar, nonionic contrast medium.
GE Healthcare Glossary
Osmolality A measure of total number of particles dissolved in a fluid, usually in water. Particles can be small or large, have an electrical charge (ions from salts, acids or bases) or be electrically neutral (sugars, proteins). High osmolality is an important contributing factor to toxicity. Ioniccontrast media are salts and split into an anion and a cation when dissolved, while non-ionic contrast media result in a solution of solution of intact molecules. This means that ionic contrast media will have 2 particles per 3 iodine atoms ("ratio 1.5 ") while non-ionic monomeric contrast media will have only particle per 3 iodine atoms ("ratio 3"), i.e. more iodine per unit. Ionic dimeric contrast media behave like "ratio 3" contrast media or low-osmolar contrast media. Dimeric non-ionic contrast media have 6 iodine atoms per particle ("ratio 6 "), and are isosmolar with blood and body fluids at all available concentrations.
GE Healthcare Glossary
Osmotoxicity The part of the toxic effect of the contrast medium that is related to osmolality. High-osmolar contrast media have a strong osmotoxicity, low-osmolar contrast media only very limited, and isosmolar products no osmotoxicity at all. Adverse effects attributed to

osmotoxicity are feeling of warmth during injection, hypotension due to reduced resistance in the peripheral circulation, hypertension due to increased plasma volume, stiffening of erythrocytes affecting blood pressure and lung function and many more.
GE Healthcare Glossary
Ultrasound contrast Ultrasound images can be improved by using a contrast agent, although these are entirely different from those used for X-ray contrast media. (Foetal examinations, though, do not employ contrast agents.) With X-rays, the contrast agent's ability to absorb these rays is the determining factor in giving good discrimination. An ultrasound contrast agent's task is to increase the refraction and reflection of the ultrasonic waves.
One way of doing this is to use a contrast agent which consists of millions of tiny air bubbles. Each of the air bubbles will reflect the sound wave. In this new and rapidly developing field, tiny gas bubbles with a size of less than 10 µm are stabilised within a biodegradable shell. Without this shell, the bubbles would be stable only transitorily (for a matter of perhaps some seconds), as the unstabilised bubbles would soon merge into larger bubbles. Besides being potentially hazardous to the patient, large bubbles have different, and less suitable, reflective properties. By filling the blood stream with the ultrasound contrast agent, it is possible, for example, to increase significantly the reflections from the blood-filled chambers of the heart, so that their image on the monitor will be clearly differentiated from those of the heart muscle itself.
Ultrasound Sound waves with a higher frequency than can be heard by the human ear. Ultrasound is used to examine many parts of the body as these waves can penetrate through our tissues (exceptions bone and air), and will be reflected from tissue interfaces (=where one tissue borders to another).
Ultrasound utilises high-frequency sound waves, which are reflected in specific ways by different tissues, normal or pathological, in the body. Ultrasound is mechanical high frequency longitudinal vibration of molecules, and differs from usual sound only by its frequency. It is not ionising and not harmful at the energy levels used for diagnostic purposes. The reflected sound (echo) is processed by a computer to produce a real-time image which is displayed on a screen instantly.
The principle for ultrasound, or ultrasonography, is the same as for underwater sonar or echo sounding. An apparatus sends an ultrasonic wave through the body at a speed of about 1,500 meters per second. At the interface between two types of tissue, the wave will be refracted or 'broken up', and part of the wave will be reflected back and detected by the apparatus. The rest of the ultrasonic wave continues deeper into the body, and is reflected as an echo from the surface of tissues lying further inside the body. How much is reflected depends on the densities of the respective tissues, and thus the speed of the sound wave as it passes through them. The time taken for the reflected wave to return

indicates how deep the tissue lies within the body. In this way, one obtains a picture of the relative locations of the tissues in the body, in the same way that one may visualise the contours of a school of fish with a sonar.
Not all of the sound waves will be reflected by the first interface they encounter; quite a few of them will continue until they strike a new surface, etc. Using the same analogy, this explains why we can see stones lying at the bottom of a stream, because the water-stone interface reflects some of the light that has penetrated through the water-air interface. Some structures will also absorb the sound waves, so that in the end there is little or nothing left to reflect. In this way, a kind of "sound-shadow" is formed. Based on these properties, we can create a picture of what the structures inside the body look like.
The location of the various structures is calculated based on the speed of sound as it travels through tissue, which in almost all tissues (and water) is about 1500 m/s (300 m/s in air). The distance between the skin and the interfase can be calculated from the time it takes for a reflected sound wave (echo) to return to the ultrasound probe.This again constitutes the basis for building up an image.
The time a sound wave uses from when it is transmitted, encounters an interface, is reflected and returns to the acoustic source which both transmits and receives the signals, is divided by 2 (because the sound has travelled the distance twice, back and forth) and multiplied by the velocity. If something produces an echo after 0.0002 seconds has elapsed, then it is located 15 cm inside the body.
Ultrasound examinations are best suited for investigations of soft tissues. Ultrasonic waves penetrate poorly through air and bone, and ultrasonography is therefore not suitable for examining organs behind bony structures, such as the brain within the skull. Clear advantages of the technique, though, are that the equipment is small and easily portable, and that ultrasound produces 'living pictures', i.e. 'real-time' images.
Blood and other fluids reflect sound waves rather poorly, allowing them to pass through more or less unweakened (unattenuated) until they encounter the surface of something denser. For this reason, ultrasound has traditionally been used in examinations of the liver, kidneys, various abdominal organs and, last but not least, the heart.
An ultrasound examination is often done of the fetus in the eighteenth week of pregnancy.
GE Healthcare Glossary
Vascular imaging Angiography, which is performed with contrast media (CM) injected directly in the vessel through an inserted catheter, has for several decades been used for vascular imaging. This technique in most cases still offers the best visualisation of arteries and veins.
Ultrasound is a suitable tool to detect aneurysms in abdominal aorta and greater vessels, and is fast and cheap compared with other modalities. Fast CT and MRI

techniques offer a non-invasive method of imaging. Currently these are used in imaging thoracic and abdominal aorta, renal and cerebral arteries - with some limitations.
CT and MRI is also used to evaluate abnormal vascularity as aneurysms and malformations in various locations. Probably MRI will become increasingly popular because of its non-invasiveness, ability to produce multiplanar images with very high resolution and no potentially harmful radiation. Ultrasound and Doppler is used mainly to assess carotid arteries and veins in the lower extremities.
GE Healthcare Glossary Radio-pharmaceutical Also called nuclear medicine. An imaging technique where radioactive substances (radio-isotopes/radiopharmaceuticals) are injected into a patient to trace disease processes. Sometimes the radioactive substance may concentrate directly in an organ/tissue, but in most cases it has to be attached to a carrier molecule with a "preference" for a certain tissue or disease process. The concentrated radioactivity may be detected by a so-called gamma camera as typical "hot spots".
GE Healthcare Glossary
Radioactivity All elements (=the building stones of all chemical substances - incl. biological) have nuclei that are made from protons (carrying a positive electrical charge) and neutrons (without an electrical charge). If the balance between the number of protons and neutrons is not optimal, the nucleus will be unstable, and will try to become stable by getting rid of excess protons or neutrons, or to add either to "improve" the balance. These processes to improve the balance is accompanied by different types of high energy radiation, called alpha, beta and gamma radiation, all of which are radioactive. Radioactivity is a type of ionising radiation and occurs naturally or may be a result of a nuclear reactor process.
GE Healthcare Glossary
Radiographic By means of X-rays.

Radiologist Doctor specialising in radiology, i.e. X-ray, MRI and ultrasound examinations.
Radionuclide A radioactive isotope.
Radiopharmaceutical Isotope used in nuclear medicine. In addition to having an appropriate half-life, it must be absorbed by or in some other way become attached to a certain type of tissue, a specific organ or an active disease process.
Some nuclides can be used "as is". A good example is radioactive iodine, which is absorbed directly by the thyroid gland. The thyroid needs iodine to build the hormones it produces and cannot distinguish between radioactive and non-radioactive iodine. Another example is radioactive thallium, which is absorbed directly by the heart muscle and can be used to investigate whether parts of the heart are not functioning normally (indicated by reduced uptake of thallium).
GE Healthcare Glossary
Parenchyma The actual, specialised tissue(s) in an organ (heart, kidney, liver) or gland
GE Healthcare Glossary
Pathological Relating to any disease process, as opposite to normal or healthy.
Liver and gallbladder imaging

Imaging of the liver can de done with different modalities. Ultrasound is very useful for detection of various focal abnormalities such as benign and malignant changes or neoplasm. It is also useful in detection of fatty liver changes which could proceed to cirrhosis. Although the sensitivity for detection of focal pathology is good, the specificity (what we actually see) is not always as good as could be wished. Therefore further investigations are often needed, especially with CT. Computer tomography with time-related injection of contrast medium will often characterise a lesion sufficiently.
Based upon clinical history and findings, the radiologist in co-operation with the referring doctor will tailor the best examination for different clinical settings.
Gall-bladder stones are easily detected on ultrasound, and so is dilation of the bile ducts. Diseases of the biliary system can also be visualised by NM.
Parenchymal disorders Ultrasound can detect fatty infiltration very easily indeed, due to increased echogenicity in the parenchyma. Likewise, CT will detect similar findings because of a reduced general density (increased fat content in the liver cells). Some deposition diseases, e.g. haemosiderosis are readily detected on CT.
On the other hand hepatitis (acute or chronic) can not be detected by any imaging modality. Unspecific findings like increased liver size can be measured, but do not give any explanations as to what may be the cause.
Benign and malignant lesions of the parenchyma Focal expansive lesions are readily detected by ultrasound, CT and MRI. The sensitivity of the different modalities varies somewhat, but for practical purposes a normal ultrasound examination may nearly always rule out significant focal pathology, provided there are no technical limitations, like significant overweight.
Simple cysts are easily detected by ultrasound, CT and MRI.
Haemangioma can often be confirmed by ultrasound or NM upon "tagging" blood cells with a radioactive marker. Some haemangioma behave differently, and in such cases dynamic CT or MRI (where several scans are taken at short intervals after injection of a contrast medium) is preferred.
Focal nodular hyperplasia and adenoma require specially tailored CT-examinations or MRI.
Metastases are mostly detected by ultrasound, but are often characterised better with CT or MRI. If surgery is planned, a preoperative mapping has to be done with either CT or MRI. Though is it important to know that a fine-needle biopsy may be mandatory to confirm the diagnosis.
Bile duct including gallbladder Ultrasound has a very high sensitivity and specificity for detecting gallbladder stones, and also to rule out associated inflammation (cholecystitis). Ultrasound will also show dilation of the ducts which can be caused by various mechanisms. The exact cause is, however, not always demonstrated by ultrasound, so further imaging with CT or MRI in these circumstances may be necessary.

NM biliary scintigraphy shows cystic duct obstruction in acute cholangitis, will visualise post-operative bile leakage, and can diagnose biliary atresia.
GE Healthcare Glossary
Liver MRI Protocol - GE HD-X