Embed Size (px)
DESCRIPTION
wound up
Citation preview

MOISTURE AND WOUND HEALING
Bishara S. ATIYEH, MD, FACS Shady N. HAYEK, MDClinical Professor Chief ResidentDivision Plastic and Reconstructive Surgery Division Plastic and Reconstructive SurgeryAmerican University of Beirut Medical Center American University of Beirut Medical CenterBeirut, LEBANON Beirut, LEBANONe-mail: [email protected]
Correspondance to B. S. Atiyeh
This article was originally published in French as: Intérêt d'un Onguent Chinois (MEBO) dans le Maintient Local de l'Humidité.Bishara S. Atiyeh, Shady N. Hayek. Journal des Plaies et Cicatrisation9:7-11,2005.It is reproduced here in English by kind permission of the publishers JPC.
ABSTRACT
Good hydration is the single most important external factor responsible for optimal wound healing. Unfortunately, available moisture retentive materials, products and devices require a certain expertise for application, are relatively expensive, may be associated with some serious complications and side effects, but most of all are impractical for application over large surface areas. We present our experience in exploring the wound healing effect of Moist Exposed Burn Ointment (MEBO – Julphar, Gulf Pharmaceutical industries, UAE), a newly introduced product capable of providing optimal moisture at the wound surface without overlying secondary occlusive dressing. Though the studies we have conducted have a limited scope, they have, however, demonstrated improved primary and secondary wound healing as well as extreme ease of application and practicality of this ointment in providing the necessary moist conditions for optimal healing as compared to some currently available labor intensive and time consuming moisture retaining products and devices. They have demonstrated also the beneficial prophylactic effect of the ointment on scar quality.
INTRODUCTION
Wound healing which is the stated goal of any wound management protocol, has been described throughout recorded history, however, our understanding of its basic mechanisms has grown more in the past 2 decades than in the preceding 2 millennia [1]. The recent logarithmic growth in our knowledge about wound healing is extremely promising and has already led to the introduction of new and exciting concepts as well as several novel therapeutic modalities and innovative wound dressings [2]. There is now growing evidence that good hydration is the single most important external factor responsible for optimal wound healing [3,4,5,6,7]. Although no reliable operational definitions exist of too little or too much wound surface moisture, moist wound healing is one of the most frequently used, but least understood terms in wound care nowadays. Moist or wet wounds may not be significantly different [8]. Despite some evidence that full-thickness skin wounds may exhibit accelerated healing in a wet environment in contradistinction to a moist environment [5], the optimum environment for wound healing may be an intermediate gelatinous environment between moist and dry such as seen under highly vapor-permeable dressings [8,9]. Irrespective of this apparent controversy, allowing traumatized or ischemic tissues to dehydrate produces further tissue loss by transforming the "zone of stasis" adjacent to the zone of injury into a "zone of necrosis" [5,10,11].
Healing under both wet and moist environments has been clearly demonstrated to be significantly faster than under dry conditions. Possible mechanisms explaining the observed improved healing include easier migration of epidermal cells over the moist wound surface instead of under a dry scab, increased partial pressure of oxygen, and the preservation of growth factors and proteinases present in fluid exudates that are hence allowed to exert their potentiating effect on wound healing [5]. Increased moisture is responsible also for a decrease in capillary activity, reduced hyperemia, and reduced collagen deposition [10,12]. It is well proven also that keratinocytes need a moist milieu to down-regulate fibroblast collagen deposition [12] and that collagenolysis is enhanced by hydration [13]. Clinical healing of similar wounds during similar time-frames follows patterns that can be predicted by dressing moisture retention. This observa-tion suggests that, when other variables are held constant, use of more moisture-retentive dressings generally achieves environments supportive of earlier healing outcomes when compared with less moisture-retentive dressings [14]. Despite mounting evidence and appreciation of the biologic factors of moist environments and their ability to promote rapid infection-free re-epithelialization with less pain [13,15,16], the advantages of water-impermeable occlusive dressings on wound healing are often offset by their impracticality particularly when applied to large split thickness donor site areas or extensive burn surfaces [15]. Enthusiasm generated by better healing under moist conditions has also been tempered by concerns over the unwelcomed tissue maceration and infection following prolonged cutaneous water exposure [4,17]. These concerns may not be justified. In fact prolonged exposure of skin to physiologic fluids such as amniotic fluid [18] or saline [4] does not seem to produce maceration and is not comparable to the conditions encountered in World War I associated with trench foot [4]. Anyway, evidence suggests that maceration is not
consistently associated with increased adverse events, on the contrary, greater dressing moisture retention is associ-ated with fewer clinical infections, greater patient comfort, and reduced scarring [14].
Selection of the most appropriate dressing for any given type of wound is a laborious and complex process in view of the profusion of new and more elaborate dressing materials being proposed by the pharmaceutical industry. Various intricate algorithms proposed for wound care are impossible to memorize. Moreover they are practically very difficult to implement and render the task of dressing selection even harder. Not infrequently, whatever dressing is described to be the most appropriate in any given situation, may be impractical if not impossible to apply. If the basic principles of wound healing are respected and the aims and goals of the local wound management protocol are placed in proper perspective dressing selection need not be a seemingly desperate task. If a wound’s status permits spontaneous healing, the ideal dressing would be that which would promote wound healing. On the other hand, if healing is not expected either because of the wound’s extent or because of associated metabolic and vascular diseases, the main function of the dressing would be to prevent further tissue damage and to clean the wound surface and prepare it for subsequent surgical soft tissue coverage or maintain it in a relatively clean, socially acceptable condition. At any rate, the preferred dressing should be able to preserve wound exudates and maintain moisture over the wound surface. Further, it should constitute an effective barrier against bacteria and injurious external physical factors, and must reduce pain, be elastic and malleable [11]. Moreover, it must facilitate debridement whenever needed, and must have no antigenecity, toxicity or carcinogenicity. Reduced cost and unlimited or prolonged storage time are also factors to be considered [15]. Practical considerations with regard to dressing application and maintenance in position should not be overlooked as well.
MOISTURE RETENTIVE OINTMENT
Moist Exposed Burn Ointment (MEBO – Julphar, Gulf Pharmaceutical Industries, UAE) is the latest addition to the multitude of newly developed passive, interactive, and active moist dressings. This product is, however, peculiar in the sense that it provides the moist environment for optimal healing without the need for an expensive, cumbersome and hard to apply overlying secondary dressing [19,20]. The ointment has been used traditionally in China for topical burn injuries treatment. Only two and a half decades ago, Xu Rongxiang [21] from the Beijing Chinese Burn Center has popularized it outside China. MEBO is a Chinese burn ointment with a USA patented formulation since 1995. The active component of the ointment is ß-sitosterol in a base of beeswax, sesame oil and other components. Clinical and experimental studies reported in the Chinese literature have demonstrated that it reduces markedly evaporation from the wound surface [22]. Though MEBO does not have any demonstrable in vitro bacteriostatic and bactericidal activity probably due to its oily composition that does not allow proper diffusion in a watery culture medium [23,24], it has been shown that in vivo, it had similar action to 1% Silver Sulfadiazine in controlling burn wound sepsis and systemic infection with P. aeroginosa [25]. It has also been demonstrated experimentally that MEBO exhibited a statistically significant wound healing potential on rabbit corneal epithelium as compared to saline, homologous serum, Vitamin A and dexamethasone [26]. The ointment produces good analgesia and has a good debriding effect, moreover, it drastically reduces water loss and exudation from the open wound surface. The required frequent application of the ointment is easy and can be performed by the patient himself or a member of his family.
CLINICAL TRIALS
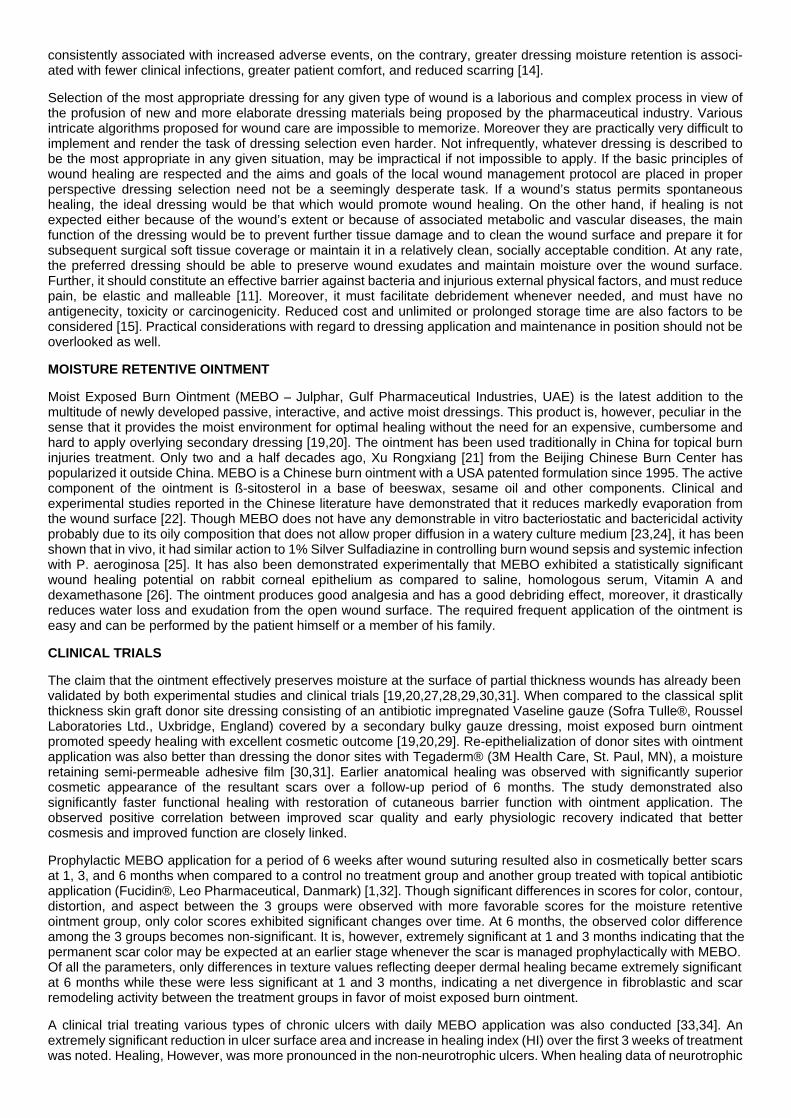
The claim that the ointment effectively preserves moisture at the surface of partial thickness wounds has already been validated by both experimental studies and clinical trials [19,20,27,28,29,30,31]. When compared to the classical split thickness skin graft donor site dressing consisting of an antibiotic impregnated Vaseline gauze (Sofra Tulle®, Roussel Laboratories Ltd., Uxbridge, England) covered by a secondary bulky gauze dressing, moist exposed burn ointment promoted speedy healing with excellent cosmetic outcome [19,20,29]. Re-epithelialization of donor sites with ointment application was also better than dressing the donor sites with Tegaderm® (3M Health Care, St. Paul, MN), a moisture retaining semi-permeable adhesive film [30,31]. Earlier anatomical healing was observed with significantly superior cosmetic appearance of the resultant scars over a follow-up period of 6 months. The study demonstrated also significantly faster functional healing with restoration of cutaneous barrier function with ointment application. The observed positive correlation between improved scar quality and early physiologic recovery indicated that better cosmesis and improved function are closely linked.
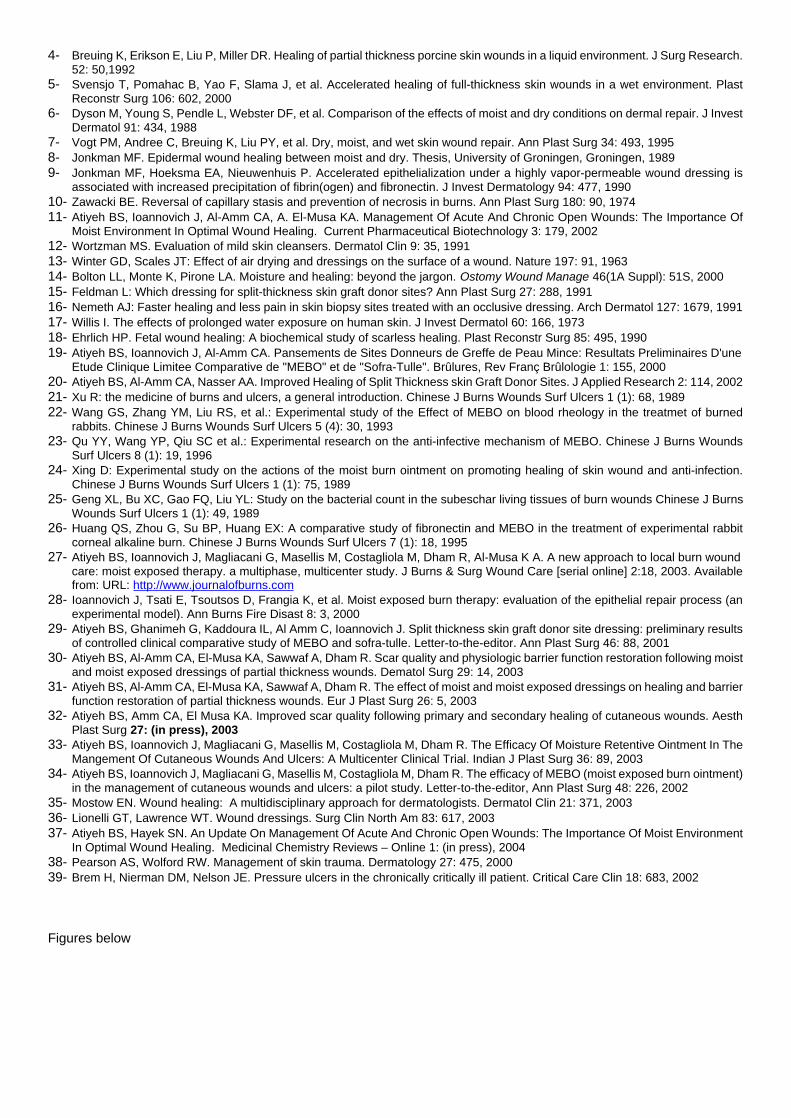
Prophylactic MEBO application for a period of 6 weeks after wound suturing resulted also in cosmetically better scars at 1, 3, and 6 months when compared to a control no treatment group and another group treated with topical antibiotic application (Fucidin®, Leo Pharmaceutical, Danmark) [1,32]. Though significant differences in scores for color, contour, distortion, and aspect between the 3 groups were observed with more favorable scores for the moisture retentive ointment group, only color scores exhibited significant changes over time. At 6 months, the observed color difference among the 3 groups becomes non-significant. It is, however, extremely significant at 1 and 3 months indicating that the permanent scar color may be expected at an earlier stage whenever the scar is managed prophylactically with MEBO. Of all the parameters, only differences in texture values reflecting deeper dermal healing became extremely significant at 6 months while these were less significant at 1 and 3 months, indicating a net divergence in fibroblastic and scar remodeling activity between the treatment groups in favor of moist exposed burn ointment.
A clinical trial treating various types of chronic ulcers with daily MEBO application was also conducted [33,34]. An extremely significant reduction in ulcer surface area and increase in healing index (HI) over the first 3 weeks of treatment was noted. Healing, However, was more pronounced in the non-neurotrophic ulcers. When healing data of neurotrophic

ulcers was analyzed using the paired t-test, significant increase in HI between weeks one and two became apparent. The same healing trends were also observed when ulcers of vascular etiology without a neurotrophic component were considered. More than 50% of all ulcers reached 0.25 Healing Index (HI) within the first week, more than 80% within the second week, and more than 90% within the third week. 100% of the non-neurotrophic ulcers reached 0.25 HI by the third week while only 80% of the neurotrophic ulcers reached the same stage of healing. 50% of all ulcers reached 0.75 HI by the second week, and around 80% by the fourth week, while 85% of non-neurotrophic and about 65% of neurotrophic ulcers reached 0.75 HI by the fourth week. None of the patients in the study had initially wound sepsis nor did any patient develop clear signs of wound sepsis during treatment irrespective of the treatment duration, which extended for more than 3 months in few patients for which surgery was not an option.
DISCUSSION
Despite all the recent accumulation of knowledge regarding wound healing, local wound care for wounds to heal either by primary or by secondary intention appears to be still a balance of art and science invariably based upon experience and perhaps upon perceived cost and benefit passed from teacher to student [35]. There are currently hundreds of products, devices, and dressing materials in the market to aid in wound management [11]. However, before selecting the appropriate dressing that would provide maximal benefit for a particular wound, the needs of the wound must be carefully assessed [36]. As mentioned previously, no single dressing can provide all requirements to all wounds and no available agent is perfect. Moreover, the needs of each individual wound at any particular time need to be prioritized as it may differ while it progresses through the healing process. These needs must be matched to the pros and cons of possible dressings. Frequently, there is not one clear best choice. The practitioner must decide which dressing functions are required for each particular situation in order to maximize the choice among the possibly acceptable dressing candidates [37]. The choice of dressing depends on the type of wound, its anatomic location, the patient's age, how often it needs to be changed, and the function it has to perform. Factors to consider in the type of wound include size, depth, presence of infection or pain, and amount of exudates [37,38]. Moreover, treatment decisions should be made within the context of the patient's overall care goals [39].
With regard to these basic principles, any dressing that does not provide the necessary moisture for wound healing should be disregarded except probably when dealing with infected wounds in which the moist environment would exacerbate the infection [11]. Though some dressings may be beneficial in some aspects such as the widely used topical antibacterial preparations in burn wound management and the highly absorbent cotton and gauze dressings, such open and semi-open dressings violate the basic principle of wound healing and must be replaced by better alternatives. Adherent wet to dry dressings, low adherent wound contact dressings and perforated film absorbent dressings do not seem to be appropriate for the management of open wounds healing by secondary intention. Their usage for primarily healing wounds is not so much objectionable. On the other hand, foam dressings, polysaccharide dressings and alginate dressings do not provide as such the optimum moist environment for healing unless combined with a secondary synthetic adhesive moisture-vapor-permeable (SAM) dressing which by itself is labor intensive and impractical to use over large surface areas and difficult to maintain over certain anatomical areas. Likewise, hydrocol-loids, hydrogels and the new hydroactive preparations though capable of providing the proper moisture, require the same secondary dressing for positioning. MEBO, on the other hand, produces the adequate environment for moist wound healing without the need of any cumbersome, elaborate or expensive secondary dressing [11].
CONCLUSION
Our investigation of this new moisture retentive ointment indicates so far that it has a definite positive effect on wound healing. The nature of the studies and their limited clinical scope, allow us, however, only to speculate on its mechanism of action as well as on its effect on the various phases and components of the wound healing cascade. Further research is still required to explore the bio-cellular mechanisms involved and its action on the different cytokines and metallopro-teinases proven lately to be essential in determining the final outcome of healing. These reported studies have demonstrated the extreme ease of application and practicality of this ointment in providing the necessary moist conditions for optimal healing as compared to currently available labor intensive and time consuming moisture retaining products and devices. Though it is not an antibiotic and definitely not suitable for the treatment of established wound sepsis, adequate local antibacterial action of the ointment maintaining open wounds in a healthy “none infected” condition has also been demonstrated. Even when used for prolonged periods of time, emergence of resistant strains was not observed [33,34]. The prophylactic effect of MEBO application on improving the cosmetic appearance and preventing pathologic scar formation is another important beneficial aspect that needs further investigation.
REFERENCES
1- Atiyeh BS, Ioannovich J, Al-Amm CA, A. El-Musa KA, Dham R. Improving Scar Quality: A Prospective Clinical Study. Aesthetic Plastic Surgery 26: 470, 2002
2- Cohen KI. Wound healing: Key advances in research and clinical care. Contemp Surg Suppl Sept: 2, 20003- Winter GD. A note on wound healing under dressings with special reference to perforated-film dressings. J Investig Dermatol 45:
299, 1965
4- Breuing K, Erikson E, Liu P, Miller DR. Healing of partial thickness porcine skin wounds in a liquid environment. J Surg Research. 52: 50,1992
5- Svensjo T, Pomahac B, Yao F, Slama J, et al. Accelerated healing of full-thickness skin wounds in a wet environment. Plast Reconstr Surg 106: 602, 2000
6- Dyson M, Young S, Pendle L, Webster DF, et al. Comparison of the effects of moist and dry conditions on dermal repair. J Invest Dermatol 91: 434, 1988
7- Vogt PM, Andree C, Breuing K, Liu PY, et al. Dry, moist, and wet skin wound repair. Ann Plast Surg 34: 493, 19958- Jonkman MF. Epidermal wound healing between moist and dry. Thesis, University of Groningen, Groningen, 19899- Jonkman MF, Hoeksma EA, Nieuwenhuis P. Accelerated epithelialization under a highly vapor-permeable wound dressing is
associated with increased precipitation of fibrin(ogen) and fibronectin. J Invest Dermatology 94: 477, 199010- Zawacki BE. Reversal of capillary stasis and prevention of necrosis in burns. Ann Plast Surg 180: 90, 197411- Atiyeh BS, Ioannovich J, Al-Amm CA, A. El-Musa KA. Management Of Acute And Chronic Open Wounds: The Importance Of
Moist Environment In Optimal Wound Healing. Current Pharmaceutical Biotechnology 3: 179, 200212- Wortzman MS. Evaluation of mild skin cleansers. Dermatol Clin 9: 35, 199113- Winter GD, Scales JT: Effect of air drying and dressings on the surface of a wound. Nature 197: 91, 196314- Bolton LL, Monte K, Pirone LA. Moisture and healing: beyond the jargon. Ostomy Wound Manage 46(1A Suppl): 51S, 200015- Feldman L: Which dressing for split-thickness skin graft donor sites? Ann Plast Surg 27: 288, 199116- Nemeth AJ: Faster healing and less pain in skin biopsy sites treated with an occlusive dressing. Arch Dermatol 127: 1679, 199117- Willis I. The effects of prolonged water exposure on human skin. J Invest Dermatol 60: 166, 197318- Ehrlich HP. Fetal wound healing: A biochemical study of scarless healing. Plast Reconstr Surg 85: 495, 199019- Atiyeh BS, Ioannovich J, Al-Amm CA. Pansements de Sites Donneurs de Greffe de Peau Mince: Resultats Preliminaires D'une
Etude Clinique Limitee Comparative de "MEBO" et de "Sofra-Tulle". Brûlures, Rev Franç Brûlologie 1: 155, 200020- Atiyeh BS, Al-Amm CA, Nasser AA. Improved Healing of Split Thickness skin Graft Donor Sites. J Applied Research 2: 114, 200221- Xu R: the medicine of burns and ulcers, a general introduction. Chinese J Burns Wounds Surf Ulcers 1 (1): 68, 198922- Wang GS, Zhang YM, Liu RS, et al.: Experimental study of the Effect of MEBO on blood rheology in the treatmet of burned
rabbits. Chinese J Burns Wounds Surf Ulcers 5 (4): 30, 199323- Qu YY, Wang YP, Qiu SC et al.: Experimental research on the anti-infective mechanism of MEBO. Chinese J Burns Wounds
Surf Ulcers 8 (1): 19, 199624- Xing D: Experimental study on the actions of the moist burn ointment on promoting healing of skin wound and anti-infection.
Chinese J Burns Wounds Surf Ulcers 1 (1): 75, 198925- Geng XL, Bu XC, Gao FQ, Liu YL: Study on the bacterial count in the subeschar living tissues of burn wounds Chinese J Burns
Wounds Surf Ulcers 1 (1): 49, 198926- Huang QS, Zhou G, Su BP, Huang EX: A comparative study of fibronectin and MEBO in the treatment of experimental rabbit
corneal alkaline burn. Chinese J Burns Wounds Surf Ulcers 7 (1): 18, 199527- Atiyeh BS, Ioannovich J, Magliacani G, Masellis M, Costagliola M, Dham R, Al-Musa K A. A new approach to local burn wound
care: moist exposed therapy. a multiphase, multicenter study. J Burns & Surg Wound Care [serial online] 2:18, 2003. Available from: URL: http://www.journalofburns.com
28- Ioannovich J, Tsati E, Tsoutsos D, Frangia K, et al. Moist exposed burn therapy: evaluation of the epithelial repair process (an experimental model). Ann Burns Fire Disast 8: 3, 2000
29- Atiyeh BS, Ghanimeh G, Kaddoura IL, Al Amm C, Ioannovich J. Split thickness skin graft donor site dressing: preliminary results of controlled clinical comparative study of MEBO and sofra-tulle. Letter-to-the-editor. Ann Plast Surg 46: 88, 2001
30- Atiyeh BS, Al-Amm CA, El-Musa KA, Sawwaf A, Dham R. Scar quality and physiologic barrier function restoration following moist and moist exposed dressings of partial thickness wounds. Dematol Surg 29: 14, 2003
31- Atiyeh BS, Al-Amm CA, El-Musa KA, Sawwaf A, Dham R. The effect of moist and moist exposed dressings on healing and barrier function restoration of partial thickness wounds. Eur J Plast Surg 26: 5, 2003
32- Atiyeh BS, Amm CA, El Musa KA. Improved scar quality following primary and secondary healing of cutaneous wounds. Aesth Plast Surg 27: (in press), 2003
33- Atiyeh BS, Ioannovich J, Magliacani G, Masellis M, Costagliola M, Dham R. The Efficacy Of Moisture Retentive Ointment In The Mangement Of Cutaneous Wounds And Ulcers: A Multicenter Clinical Trial. Indian J Plast Surg 36: 89, 2003
34- Atiyeh BS, Ioannovich J, Magliacani G, Masellis M, Costagliola M, Dham R. The efficacy of MEBO (moist exposed burn ointment) in the management of cutaneous wounds and ulcers: a pilot study. Letter-to-the-editor, Ann Plast Surg 48: 226, 2002
35- Mostow EN. Wound healing: A multidisciplinary approach for dermatologists. Dermatol Clin 21: 371, 200336- Lionelli GT, Lawrence WT. Wound dressings. Surg Clin North Am 83: 617, 200337- Atiyeh BS, Hayek SN. An Update On Management Of Acute And Chronic Open Wounds: The Importance Of Moist Environment
In Optimal Wound Healing. Medicinal Chemistry Reviews – Online 1: (in press), 200438- Pearson AS, Wolford RW. Management of skin trauma. Dermatology 27: 475, 200039- Brem H, Nierman DM, Nelson JE. Pressure ulcers in the chronically critically ill patient. Critical Care Clin 18: 683, 2002
Figures below
Fig. 1: Secondary healing of STSG donor site with MEBO, Sofra-Tulle, and Tegaderm. Better quality scar is observed with MEBO
Fig. 2: Primarily healed scar over face treated prophylactically with MEBO. Rapid scar maturation is observed with good scar quality.
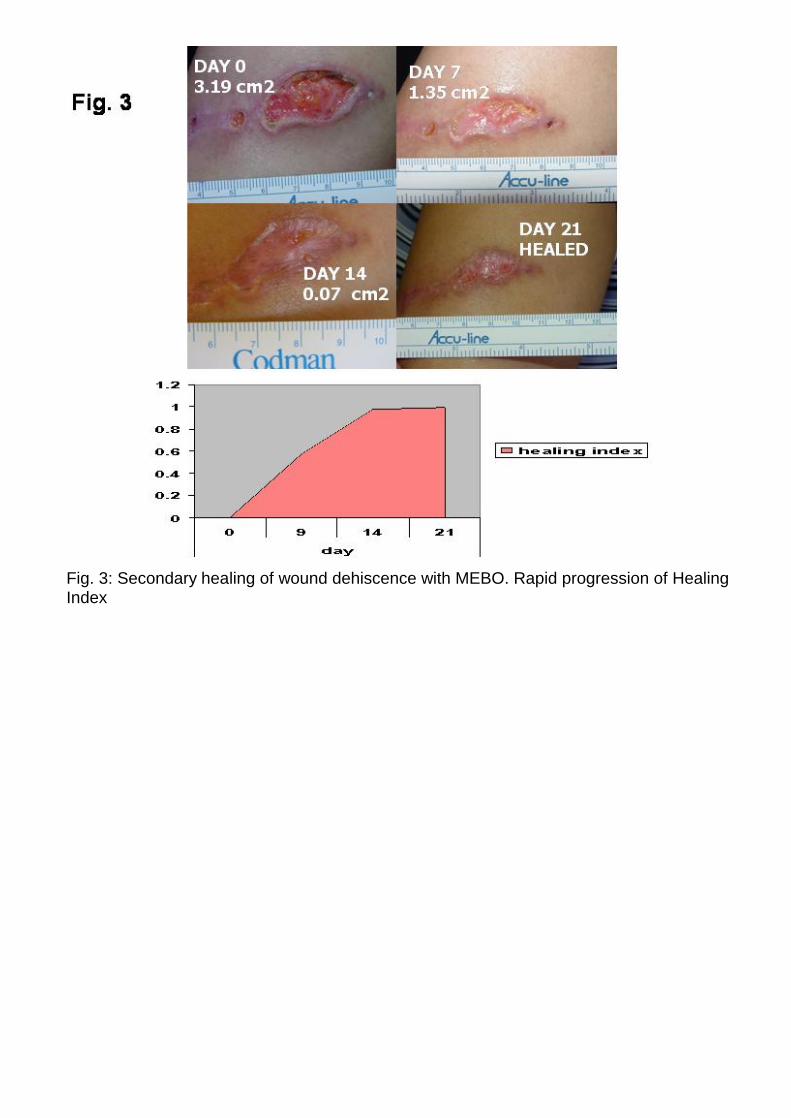
Fig. 3: Secondary healing of wound dehiscence with MEBO. Rapid progression of Healing Index




















![Untitled-1 [] · Construction kicks off in Noida Extension. homes a reality soon Mebo plan for Noida Extn](https://img.pdfslide.us/doc/110x75/5ff1c69f8239fe43c619972e/untitled-1-construction-kicks-off-in-noida-extension-homes-a-reality-soon-mebo.jpg)