Embed Size (px)
Citation preview
Endourology and Stones
Measurement of Ureteric Stone Diameter inDifferent Planes on Multidetector ComputedTomography e Impact on the ClinicalDecision MakingSyed M. Nazim, M. Hammad Ather, and Nadir Khan
OBJECTIVE To determine if the measurement of ureteric stone in coronal reconstruction plane is different
Financial Disclosure: The authoFrom the Department of Surge
Department of Radiology, Aga KReprint requests: M. Hamma
Department of Surgery, Aga Kha74800, Pakistan. E-mail: hammaSubmitted: June 21, 2013, ac
288 ª 2014 ElseAll Rights Re
from the measurement in axial plane and whether the difference can impact the managementdecision in patients with ureteric colic.
METHODS All patients who underwent unenhanced multidetector computed tomographic (MDCT) scan for
the evaluation of reno-ureteral colic in outpatient clinics and emergency room were evaluated.The scans were evaluated on Picture Archiving Computer System with a 3-mm axial andreformatted 3-mm coronal sections. Maximal stone diameter was measured in 2 dimensions in theaxial and reformatted coronal sections by 2 reviewers. Only scans with isolated, unilateral, solitaryureteric calculi were included in the final analysis. All patients were monitored up to 4 weeks afterMDCT to determine the clinical outcome.RESULTS A total of 331 patients (272 male and 59 female; mean age � standard deviation, 39.8 � 13.8
years) were included. One hundred seventy-one (51.7%) stones passed spontaneously during thefollow-up period. There was a 20% underestimation of maximal stone diameter in axial plane forall stones and a 17% for the stones that passed spontaneously or with medical expulsive therapy,as compared with measurement on coronal reconstruction.CONCLUSION Measuring the transverse stonediameter onaxial images ofMDCTscanunderestimates size of ureteric
stone. This can have an impact on counseling of patients and their clinical outcome, coronalreformatted images be used for size estimation. UROLOGY 83: 288e293, 2014.� 2014 Elsevier Inc.nenhanced helical computed tomographic (CT)scan is the imaging of choice for the diagnosis of
Uurolithiasis in symptomatic patients with re-ported sensitivity and specificity close to 100%.1,2 The 2most important factors that guide clinical managementare stone size and its location.3 There is a reverse linearrelationship between stone size and spontaneous passage;hence, determination of maximal stone size is crucialwhile counseling the patient and selecting the appro-priate treatment strategy. Determination of maximalstone size is crucial indicator in clinical decision makingfor intervention or use of medical expulsive treatment forwhich various a blockers have been used with compara-ble efficacy.4 Lee et al5 recently noted that longitudinalstone diameter was a significant predictor of stoneexpulsion with medical expulsive therapy (MET), and
rs declare that they have no relevant financial interests.ry, Aga Khan University, Karachi, Pakistan; and thehan University, Karachi, Pakistand Ather, M.B.B.S., F.C.P.S. (Urol), F.E.B.U.,n University, PO Box 3500, Stadium Road, [email protected] (with revisions): September 16, 2013
vier Inc.served
coronal reconstruction might help to better choose apatient who is suitable for MET.
With the improved resolution and multiplaner refor-mations, multidetector computed tomography (MDCT)has considerably improved imaging from cross sectional(axial) imaging to true 3-D image.6 The coronal recon-struction of CT scan helps not only for better stonedetection but also reportedly for accurately assessing thestone size oriented in vertical plane, especially theureteric stones.7 Many modifications have been suggestedto improve the stone size estimation, including using analgorithm.8 However, the most commonly used method isestimation on coronal and reconstructed images.
The present study is designed to determine if mea-surement of ureteric stone in coronal reconstructionplane is different from the measurement in axial planeand whether the difference can predict the outcome forurolithiasis in patients with renal colic.
MATERIALS AND METHODS
This prospective study was conducted over a duration of 12months from April 1, 2011 to March 31, 2012. All theconsecutive unenhanced CT scan (CT kidneys, ureters, and
0090-4295/14/$36.00http://dx.doi.org/10.1016/j.urology.2013.09.037
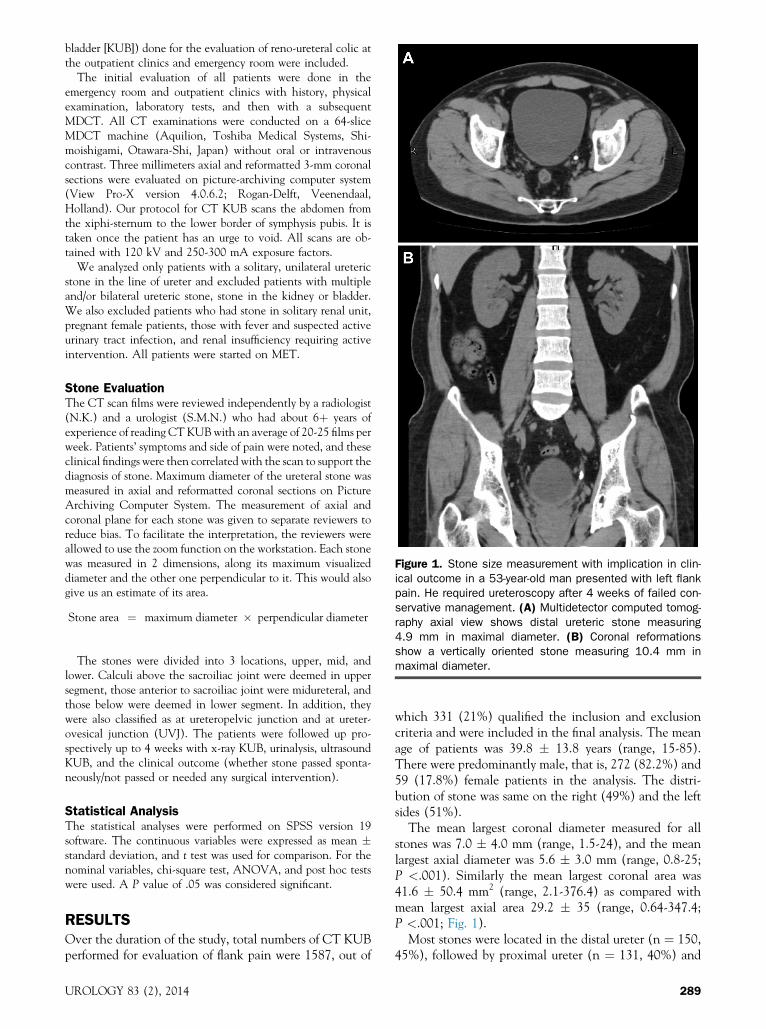
Figure 1. Stone size measurement with implication in clin-ical outcome in a 53-year-old man presented with left flankpain. He required ureteroscopy after 4 weeks of failed con-servative management. (A) Multidetector computed tomog-raphy axial view shows distal ureteric stone measuring4.9 mm in maximal diameter. (B) Coronal reformationsshow a vertically oriented stone measuring 10.4 mm inmaximal diameter.
bladder [KUB]) done for the evaluation of reno-ureteral colic atthe outpatient clinics and emergency room were included.
The initial evaluation of all patients were done in theemergency room and outpatient clinics with history, physicalexamination, laboratory tests, and then with a subsequentMDCT. All CT examinations were conducted on a 64-sliceMDCT machine (Aquilion, Toshiba Medical Systems, Shi-moishigami, Otawara-Shi, Japan) without oral or intravenouscontrast. Three millimeters axial and reformatted 3-mm coronalsections were evaluated on picture-archiving computer system(View Pro-X version 4.0.6.2; Rogan-Delft, Veenendaal,Holland). Our protocol for CT KUB scans the abdomen fromthe xiphi-sternum to the lower border of symphysis pubis. It istaken once the patient has an urge to void. All scans are ob-tained with 120 kV and 250-300 mA exposure factors.
We analyzed only patients with a solitary, unilateral uretericstone in the line of ureter and excluded patients with multipleand/or bilateral ureteric stone, stone in the kidney or bladder.We also excluded patients who had stone in solitary renal unit,pregnant female patients, those with fever and suspected activeurinary tract infection, and renal insufficiency requiring activeintervention. All patients were started on MET.
Stone EvaluationThe CT scan films were reviewed independently by a radiologist(N.K.) and a urologist (S.M.N.) who had about 6þ years ofexperience of reading CT KUBwith an average of 20-25 films perweek. Patients’ symptoms and side of pain were noted, and theseclinical findings were then correlated with the scan to support thediagnosis of stone. Maximum diameter of the ureteral stone wasmeasured in axial and reformatted coronal sections on PictureArchiving Computer System. The measurement of axial andcoronal plane for each stone was given to separate reviewers toreduce bias. To facilitate the interpretation, the reviewers wereallowed to use the zoom function on the workstation. Each stonewas measured in 2 dimensions, along its maximum visualizeddiameter and the other one perpendicular to it. This would alsogive us an estimate of its area.
Stone area ¼ maximum diameter � perpendicular diameter
The stones were divided into 3 locations, upper, mid, andlower. Calculi above the sacroiliac joint were deemed in uppersegment, those anterior to sacroiliac joint were midureteral, andthose below were deemed in lower segment. In addition, theywere also classified as at ureteropelvic junction and at ureter-ovesical junction (UVJ). The patients were followed up pro-spectively up to 4 weeks with x-ray KUB, urinalysis, ultrasoundKUB, and the clinical outcome (whether stone passed sponta-neously/not passed or needed any surgical intervention).
Statistical AnalysisThe statistical analyses were performed on SPSS version 19software. The continuous variables were expressed as mean �standard deviation, and t test was used for comparison. For thenominal variables, chi-square test, ANOVA, and post hoc testswere used. A P value of .05 was considered significant.
RESULTSOver the duration of the study, total numbers of CT KUBperformed for evaluation of flank pain were 1587, out of
UROLOGY 83 (2), 2014
which 331 (21%) qualified the inclusion and exclusioncriteria and were included in the final analysis. The meanage of patients was 39.8 � 13.8 years (range, 15-85).There were predominantly male, that is, 272 (82.2%) and59 (17.8%) female patients in the analysis. The distri-bution of stone was same on the right (49%) and the leftsides (51%).
The mean largest coronal diameter measured for allstones was 7.0 � 4.0 mm (range, 1.5-24), and the meanlargest axial diameter was 5.6 � 3.0 mm (range, 0.8-25;P <.001). Similarly the mean largest coronal area was41.6 � 50.4 mm2 (range, 2.1-376.4) as compared withmean largest axial area 29.2 � 35 (range, 0.64-347.4;P <.001; Fig. 1).
Most stones were located in the distal ureter (n ¼ 150,45%), followed by proximal ureter (n ¼ 131, 40%) and
289
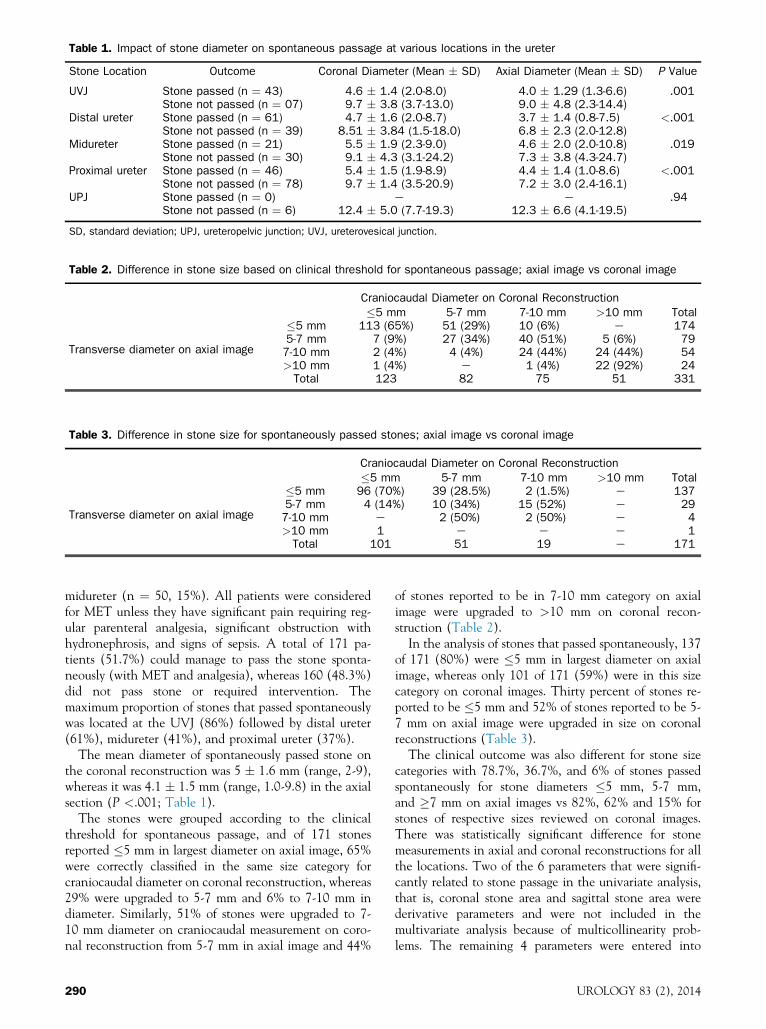
Table 1. Impact of stone diameter on spontaneous passage at various locations in the ureter
Stone Location Outcome Coronal Diameter (Mean � SD) Axial Diameter (Mean � SD) P Value
UVJ Stone passed (n ¼ 43) 4.6 � 1.4 (2.0-8.0) 4.0 � 1.29 (1.3-6.6) .001Stone not passed (n ¼ 07) 9.7 � 3.8 (3.7-13.0) 9.0 � 4.8 (2.3-14.4)
Distal ureter Stone passed (n ¼ 61) 4.7 � 1.6 (2.0-8.7) 3.7 � 1.4 (0.8-7.5) <.001Stone not passed (n ¼ 39) 8.51 � 3.84 (1.5-18.0) 6.8 � 2.3 (2.0-12.8)
Midureter Stone passed (n ¼ 21) 5.5 � 1.9 (2.3-9.0) 4.6 � 2.0 (2.0-10.8) .019Stone not passed (n ¼ 30) 9.1 � 4.3 (3.1-24.2) 7.3 � 3.8 (4.3-24.7)
Proximal ureter Stone passed (n ¼ 46) 5.4 � 1.5 (1.9-8.9) 4.4 � 1.4 (1.0-8.6) <.001Stone not passed (n ¼ 78) 9.7 � 1.4 (3.5-20.9) 7.2 � 3.0 (2.4-16.1)
UPJ Stone passed (n ¼ 0) e e .94Stone not passed (n ¼ 6) 12.4 � 5.0 (7.7-19.3) 12.3 � 6.6 (4.1-19.5)
SD, standard deviation; UPJ, ureteropelvic junction; UVJ, ureterovesical junction.
Table 2. Difference in stone size based on clinical threshold for spontaneous passage; axial image vs coronal image
Craniocaudal Diameter on Coronal Reconstruction�5 mm 5-7 mm 7-10 mm >10 mm Total
Transverse diameter on axial image
�5 mm 113 (65%) 51 (29%) 10 (6%) e 1745-7 mm 7 (9%) 27 (34%) 40 (51%) 5 (6%) 797-10 mm 2 (4%) 4 (4%) 24 (44%) 24 (44%) 54>10 mm 1 (4%) e 1 (4%) 22 (92%) 24Total 123 82 75 51 331
Table 3. Difference in stone size for spontaneously passed stones; axial image vs coronal image
Craniocaudal Diameter on Coronal Reconstruction�5 mm 5-7 mm 7-10 mm >10 mm Total
Transverse diameter on axial image
�5 mm 96 (70%) 39 (28.5%) 2 (1.5%) e 1375-7 mm 4 (14%) 10 (34%) 15 (52%) e 297-10 mm e 2 (50%) 2 (50%) e 4>10 mm 1 e e e 1Total 101 51 19 e 171
midureter (n ¼ 50, 15%). All patients were consideredfor MET unless they have significant pain requiring reg-ular parenteral analgesia, significant obstruction withhydronephrosis, and signs of sepsis. A total of 171 pa-tients (51.7%) could manage to pass the stone sponta-neously (with MET and analgesia), whereas 160 (48.3%)did not pass stone or required intervention. Themaximum proportion of stones that passed spontaneouslywas located at the UVJ (86%) followed by distal ureter(61%), midureter (41%), and proximal ureter (37%).
The mean diameter of spontaneously passed stone onthe coronal reconstruction was 5 � 1.6 mm (range, 2-9),whereas it was 4.1 � 1.5 mm (range, 1.0-9.8) in the axialsection (P <.001; Table 1).
The stones were grouped according to the clinicalthreshold for spontaneous passage, and of 171 stonesreported �5 mm in largest diameter on axial image, 65%were correctly classified in the same size category forcraniocaudal diameter on coronal reconstruction, whereas29% were upgraded to 5-7 mm and 6% to 7-10 mm indiameter. Similarly, 51% of stones were upgraded to 7-10 mm diameter on craniocaudal measurement on coro-nal reconstruction from 5-7 mm in axial image and 44%
290
of stones reported to be in 7-10 mm category on axialimage were upgraded to >10 mm on coronal recon-struction (Table 2).
In the analysis of stones that passed spontaneously, 137of 171 (80%) were �5 mm in largest diameter on axialimage, whereas only 101 of 171 (59%) were in this sizecategory on coronal images. Thirty percent of stones re-ported to be �5 mm and 52% of stones reported to be 5-7 mm on axial image were upgraded in size on coronalreconstructions (Table 3).
The clinical outcome was also different for stone sizecategories with 78.7%, 36.7%, and 6% of stones passedspontaneously for stone diameters �5 mm, 5-7 mm,and �7 mm on axial images vs 82%, 62% and 15% forstones of respective sizes reviewed on coronal images.There was statistically significant difference for stonemeasurements in axial and coronal reconstructions for allthe locations. Two of the 6 parameters that were signifi-cantly related to stone passage in the univariate analysis,that is, coronal stone area and sagittal stone area werederivative parameters and were not included in themultivariate analysis because of multicollinearity prob-lems. The remaining 4 parameters were entered into
UROLOGY 83 (2), 2014

backward stepwise binary logistic regression analyses thatdemonstrated an independent relationship between stonepassage and largest coronal size (odds ratio 0.63, 95% CI0.52-0.76; P <.001) and smallest axial size (odds ratio0.57, 95% CI 0.42-0.79; P <.01).
On the post hoc analysis, when comparing the stonearea of passed stones on coronal reformation, the UVJ,distal ureter, and midureteric stones were homogenous,whereas proximal ureteric stone area was significantlydifferent (P ¼ .027; Tukey test). While comparing thestone area of passed stones on axial reformations, theUVJ, midureter, and proximal ureteric stones were ho-mogenous, whereas distal ureteric stone area was signifi-cantly different (P ¼ .029; Tukey test).
COMMENTIn view of its high accuracy and short acquisition time,noncontrast CT scan has now become the gold standardfor the evaluation of patients presenting with acute flankpain.9,10 It not only provides information regardingpresence and localization of stones but also other detailsthat can help in management plan such as stone density,degree of obstruction caused by stone, and obstructiveparameters such as hydronephrosis, hydroureter, andperinephric stranding.11
High quality multiplaner reformations with excellenttemporal and spatial resolution can be generated fromMDCT, by its ability to acquire thin slice volumetricstudies. It can display the urinary tract in its longitudinalaxis, thus improving the orientation of stones withoutincreasing the evaluation times.12,13 Management ofureteric stones depends on 2 most important parameters,that is, stone location and size.14 Various methods havebeen described in the published data to measure the stonesize in radiographs, but there is no accepted standardtechnique for stone measurement using CT scan.15-18
Estimation of maximal transverse diameter from axialimage traditionally has been reported as the mostcommonly used method. In a survey to determine theradiological practices in the UK, Kampa et al16 found lackof uniformity among urologist in techniques for assessingthe stone size and they concluded that “Guestimation”was the most prevalent method among radiologists forassessing the maximal stone size.13
The ureteric stones can be rounded or elongated. Mostof these are oriented vertically along the long axis ofureter with maximal diameter in craniocaudal plane. It istherefore imperative to have this dimension measured.Accurate determination of these stone sizes is crucial inhelping the patient counseling and further management,that is, conservative/expectant management vs inter-vention, and even a difference of 1-2 mm can make asignificant difference in this regard.
Nadler et al14 in their study showed that axial imagesconsistently underestimated the stone size compared withcoronal reconstructions. The indirect estimation of cra-niocaudal diameter of ureteric stone from axial images
UROLOGY 83 (2), 2014
alone considering the slice collimation does not provideprecise measurement of stone size.13,14
Coronal reformations from MDCT have several ad-vantages. It provides important complimentary informa-tion to axial images, and combining the 2 togetherimproves the diagnostic confidence and conspicuity ofstones by facilitating its differentiation from phlebolith,calcified vascular plaques, or renal parenchymal calcifi-cations.15 It is also shown to improve better estimate themaximal stone diameter, especially for stones that areoriented in vertical plane.19
Another advantage of coronal image is that it enablesvisualization of kidney, ureter, and bladder simultaneouslyin a plane that is almost parallel to the orientation ofthese organs. This is more familiar and intuitive to urol-ogist because it is analogous to projections of anabdominal x-ray or excretory urogram.13
Metser et al7 compared axial vs coronal plane for renaland ureteric stone size measurements and showed that forall stones, the average underestimation of stone size wasapproximately 13% in axial plane. Our study showedsignificant underestimation of stone size on axial imagesas compared with the craniocaudal measurement fromcoronal plane. It also showed that for all stones, themaximal diameter in the axial plane was 20% less thanthe coronal plane, and for the stones that passed therewas 17% reduction on axial image. Similarly, a significantproportion of stones were underestimated in size on axialimage measurements. Dundee et al20 noted a 12% under-estimation when comparing the CT scan in axial planewith stone size on abdominal radiograph.
Lee et al5 in their retrospective study evaluated thedifference between transverse and longitudinal stone di-ameters on CT scan as a predictor of ureteral stoneexpulsion after MET. They found the longitudinaldiameter to be significant predictor of stone expulsion forureteral stones and concluded that this measurement incoronal reconstruction can help to better choose patientswho are suitable for MET.
The chances for spontaneous passage are more than98% for ureteric stones smaller than 5 mm, whereas it isalmost 60% and 39% for stones between 5-7 mm and>7 mm in diameter, respectively.3 Smith et al21 in a caseseries of 312 patients showed that the average size ofstones that was passed spontaneously was 4.6 mm,whereas the average size of stones requiring interventionwas 6.0 mm. Our study correlated with the findings of theexisting ones that the difference between the stones thatwere passed spontaneously vs which could not were sig-nificant. Moreover, this difference was significant be-tween the sizes measured in coronal and axial sections.
The rate of spontaneous stone passage is the functionof stone location.3,14 A linear relationship was observedin our study for location of stones in ureter with moststones located more distally could manage to pass.However, Kishore et al22 have shown a weak correlationcoefficient for comparing the actual size of passed stonesvs CT scan measurements (axial and craniocaudal) for
291

distal ureteric stones with actual size of passed intactstones significantly smaller than the one measured withCT scan. Recently, Demehri et al23 have proposed CT-based determination of maximum ureteral stone area(for complex ureteral stone) using a software program tobe superior to the stone diameter measurement. This isthe basis that long thin stones are more likely to pass thana long thick one.
Our study has few limitations. First of all, the presenceof stone was assigned by a consensus between the 2 ob-servers, and no standard of reference was followed for theconfirmation of stones. However, CT scan is the mostaccurate way to diagnose the stones. Although we fol-lowed up the patients to determine the clinical outcome,we did not measure the actual size of passed stone and didnot compare it with radiological size. Similarly, not all thepassed stones were available for analysis.
To our knowledge, this is the first study comparing theureteral stone size estimation in axial vs coronal planesalong with the clinical outcome during follow-up. Furtherprospective studies examining the clinical outcomes forpatients with ureteric stones measured on axial imagesalone vs clinical outcome of ureteric stones measured onaxial þ coronal reconstructions should be performedalong with the determination of actual stone size tocorrelate which measurement is more accurate.
CONCLUSIONMeasuring the transverse stone diameter on axial imagesof MDCT scan underestimates size of ureteric stone. Thiscan potentially impact management algorithm. Tocounsel patients for need of intervention and clinicaloutcome of MET, coronal reformatted images be used forsize estimation.
References
1. Smith RC, Verga M, McCarthy S, Rosenfield AT. Diagnosis ofacute flank pain: value of unenhanced helical CT. AJR Am JRoentgenol. 1996;166:97-101.
2. Sourtzis S, Thibeau JF, Damry N, et al. Radiologic investigation ofrenal colic: unenhanced helical CT compared with excretoryurography. AJR Am J Roentgenol. 1999;172:1491-1494.
3. Preminger GM, Tiselius HG, Assimos DG, et al. EAU/AUANephrolithiasis Guideline Panel. 2007 guideline for the manage-ment of ureteral calculi. J Urol. 2007;178:2418-2434.
4. Zehri AA, Ather MH, Abbas F, et al. Preliminary study of efficacy ofdoxazosin as a medical expulsive therapy of distal ureteric stones in arandomized clinical trial. Urology. 2010;75:1285-1288.
5. Lee SR, Jeon HG, Park DS, et al. Longitudinal stone diameter oncoronal reconstruction of computed tomography as a predictor ofureteral stone expulsion in medical expulsive therapy. Urology.2012;80:784-789.
6. Flohr TG, Schaller S, Stierstorfer K, et al. Multi-detector row CTsystems and image-reconstruction techniques. Radiology. 2005;235:756-773.
7. Metser U, Ghai S, Ong YY, et al. Assessment of urinary tract calculiwith 64-MDCT: the axial versus coronal plane. AJR Am J Roent-genol. 2009;192:1509-1513.
8. Lid�en M, Andersson T, Broxvall M, et al. Urinary stone size esti-mation: a new segmentation algorithm-based CT method. EurRadiol. 2012;22:731-737.
292
9. Miller OF, Kane CJ. Unenhanced helical computed tomography inthe evaluation of acute flank pain. Curr Opin Urol. 2000;10:123-129.
10. Chen MY, Zagoria RJ, Saunders HS, et al. Trends in the use ofunenhanced helical CT for acute urinary colic. AJR Am J Roent-genol. 1999;173:1447-1450.
11. Takahashi N, Kawashima A, Ernst RD, et al. Ureterolithiasis: canclinical outcome be predicted with unenhanced helicial CT?Radiology. 1998;208:97-102.
12. Schmidt S, Chevallier P, Chalaron M, et al. Multidetector CTenteroclysis: comparison of the reading performance for axial andcoronal views. Eur Radiol. 2005;15:238-246.
13. Paulson EK, Harris JP, Jaffe TA, et al. Acute appendicitis: addeddiagnostic value of coronal reformations from isotropic voxels atmulti-detector row CT. Radiology. 2005;235:879-885.
14. Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneouspassage of ureteral calculi to stone size and location as revealedby unenhanced helical CT. AJR Am J Roentgenol. 2002;178:101-103.
15. Kawashima A, Sandler CM, Boridy IC, et al. Unenhanced helicalCT of ureterolithiasis: value of the tissue rim sign. AJR Am JRoentgenol. 1997;168:997-1000.
16. Kampa RJ, Ghani KR, Wahed S, et al. Size matters: a survey of howurinary-tract stones are measured in the UK. J Endourol. 2005;19:856-860.
17. Nadler RB, Stern JA, Kimm S, et al. Coronal imaging to assessurinary tract stone size. J Urol. 2004;172:962-964.
18. Lin WC, Uppot RN, Li CS, et al. Value of automated coronalreformations from 64-section multidetector row computerized to-mography in the diagnosis of urinary stone disease. J Urol. 2007;178(3 Pt 1):907-911.
19. Berkovitz N, Simanovsky N, Katz R, et al. Coronal reconstructionof unenhanced abdominal CT for correct ureteral stone size classi-fication. Eur Radiol. 2010;20:1047-1051.
20. Dundee P, Bouchier-Hayes D, Haxhimolla H, et al. Renal tractcalculi: comparison of stone size on plain radiography and non-contrast spiral CT scan. J Endourol. 2006;20:1005-1009.
21. Smith RC, Verga M, Dalrymple N, et al. Acute ureteral obstruction:value of secondary signs of helical unenhanced CT. Am J Roent-genol. 1996;167:1109-1113.
22. Kishore TA, Pedro RN, Hinck B, et al. Estimation of size of distalureteral stones: non-contrast CT scan versus actual size. Urology.2008;72:761-764.
23. Demehri S, Steigner ML, Sodickson AD, et al. CT-based deter-mination of maximum ureteral stone area: a predictor of sponta-neous passage. AJR Am J Roentgenol. 2012;198:603-608.
EDITORIAL COMMENT
Urologists recognize that small distal ureteral stones are likely topass; however, predicting which patient with a ureteral stonewill fail medical expulsive therapy (MET) remains challenging,as there is no threshold size for ureteral stone passage. In thepresent study, this axiom is held true because, regardless oflocation in the ureter, stones that passed were approximately 4-5mm in coronal size and those that did not pass averaged 8-9 mmin coronal length.Noncontrast computed tomographic scanning (NCCT) is the
cornerstone of diagnosing urinary calculi, especially in anemergency department setting.1 Simply measuring the coronallength of a ureteral stone is an additional data point that allradiologists and urologists can easily ascertain and thereby betterdiscriminate who is likely to fail MET. In addition, usingmagnified bone windows on the NCCT, as described by Eisneret al,2 might offer the most accurate size estimate of ureteralstones. Biomarkers such as C-reactive protein might help
UROLOGY 83 (2), 2014

discriminate which patients with stones of a “passable size” willfail MET and require surgical intervention.3,4
Using these data to create a nomogram would help patientcounseling; however, the means of assessing stone passage in thisstudy and in the stone literature in general remain far fromstandardized.5 Since not all patients in this study presented withtheir passed stone for analysis or had a repeat NCCT to provethey were stone free, the rate of passage might be less than re-ported by the authors, and thus bias a nomogram constructedfrom these data.
Until a biomarker is widely available, stone size remains oneof the best indicators of passage for ureteral calculi. The prac-ticing urologist should use measurements of ureteral stones inthe axial and coronal planes to better counsel patients with aureteral calculus.
Peter L. Steinberg, M.D., Division of Urology, Department ofSurgery, Beth Israel Deaconess Medical Center, Boston, MA
References
1. Fulgham PF, Assimos DG, Pearle MS, et al. Clinical effectivenessprotocols for imaging in the management of ureteral calculous dis-ease: AUA technology assessment. J Urol. 2013;189:1203-1213.
2. Eisner BH, Kambadakone A, Monga M, et al. Computerized to-mography magnified bone windows are superior to standard soft tissuewindows for accurate measurement of stone size: an in vitro andclinical study. J Urol. 2009;181:1710-1715.
3. Aldaqadossi HA. Stone expulsion rate of small distal ureteric calculicould be predicted with plasma C-reactive protein. Urolithiasis. 2013;41:235-239.
4. Angulo JC, Gaspar MJ, Rodriguez N, et al. The value of C-reactiveprotein determination in patients with renal colic to decide urgenturinary diversion. Urology. 2010;76:301-306.
5. Deters LA, Jumper CM, Steinberg PL, et al. Evaluating the definitionof “stone free status” in contemporary urologic literature. ClinNephrol. 2011;76:354-357.
http://dx.doi.org/10.1016/j.urology.2013.09.040UROLOGY 83: 292e293, 2014. � 2014 Elsevier Inc.
REPLY
The indication for intervention in the treatment of uncompli-cated ureteral stones in both the major international urologicassociation guidelines (ie American Urological Association andEuropean Association of Urology)1 is based on stone size.However, methods for determining stone size are not stan-
UROLOGY 83 (2), 2014
dardized. Even in contemporary published data there are onlysparse reports regarding the preferred method for stone mea-surement using the noncontrast computed tomography. Themost commonly used method is by estimation of maximaltransverse dimension from axial images.Medical expulsive therapy has become the standard of care for
most symptomatic small- to medium-sized uncomplicatedstones. However, success of medical expulsive therapy (MET) isdifficult to predict. Currently, the most studied parameter isstone size and site. Therefore, it is important that the stone sizeestimation should be as accurate as possible. Some recent work,2
including the present one is an attempt to see if size estimationon reconstructed film is a better predictor of successful METcompared with conventional axial films. The transverse calculusmeasurement on axial slices often underestimates stone size andprovides incorrect clinical parameter for management decision.Use of bone windows in particular when low-dose protocol isused. Recently, Sohn et al3 noted no significant difference in themeasurement of stone size, Hounsfield units, or skin to stonedistance between the low-dose and conventional-dosecomputed tomographic scans. However, the low-dose computedtomographic scan have an inherent advantage of markedreduction in the radiation dose to the patient.Stone clearance spontaneously or with pharmacologic support
is dependent on many diverse factors; therefore, it also makessense that multiparametric models should be developed for ac-curate assessment of successful MET. Studies with robust designlooking at various clinical, demographic, anatomic, andbiochemical parameters besides stone size and location areneeded to answer these questions.
M. Hammad Ather, M.D., F.C.P.S. (Urol), F.E.B.U.,Aga Khan University, Karachi, Pakistan
References
1. Preminger GM, Tiselius HG, Assimos DG, et al. 2007 guideline forthe management of ureteral calculi. J Urol. 2007;178:2418-2434.
2. Berkovitz N, Simanovsky N, Katz R, et al. Coronal reconstruction ofunenhanced abdominal CT for correct ureteral stone size classifica-tion. Eur Radiol. 2010;20:1047-1051.
3. Sohn W, Clayman RV, Lee JY, et al. Low-dose and standardcomputed tomography scans yield equivalent stone measurements.Urology. 2013;81:231-234.
http://dx.doi.org/10.1016/j.urology.2013.09.041UROLOGY 83: 293, 2014. � 2014 Elsevier Inc.
293