Embed Size (px)
Citation preview

Measles in Immunocompetent and Immunodeficient Hosts
William Moss, MD, MPHJohns Hopkins Bloomberg School of Public Health
FDA Blood Products Advisory Committee
August 16, 2007

Measles in Immuncompetent Hosts

Clinical Features of Measles
Adapted from Infectious Diseases of Children, 9th edition. Figure 13-1, page 224. Krugman S, Katz AL, Gershon AA, Wilfert CM. Eds. St. Louis, Mosby, 1992.

Measles Rash
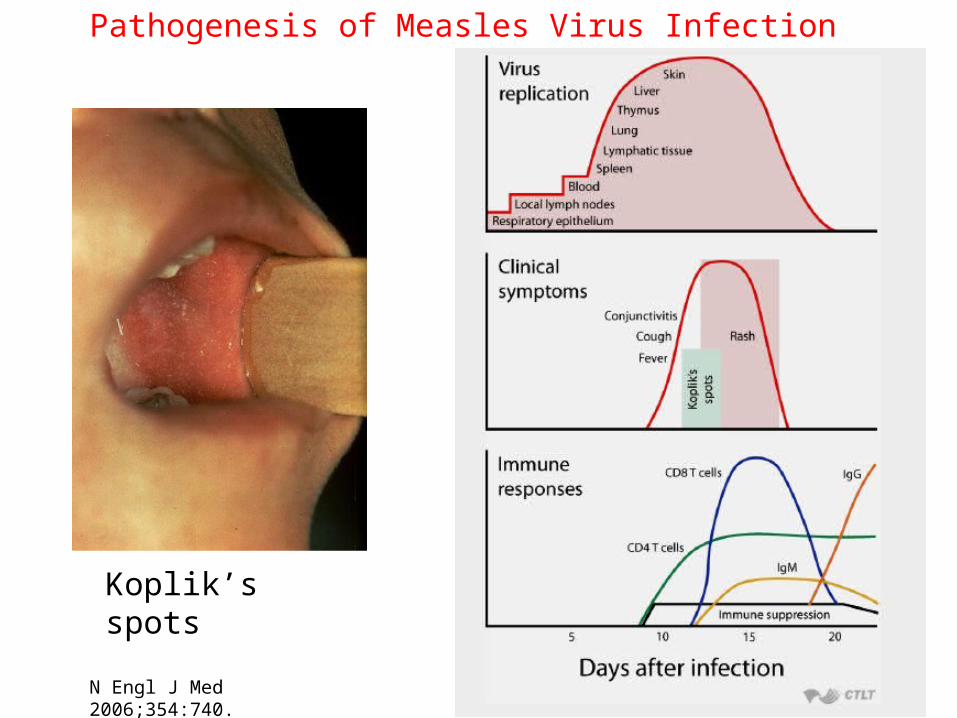
Koplik’s spots
Pathogenesis of Measles Virus Infection
N Engl J Med 2006;354:740.
Immune Responses to Measles Virus
• Innate immune responses
• Antibody responses
• Cellular immune responses
• Immunologic memory
• Immune suppression
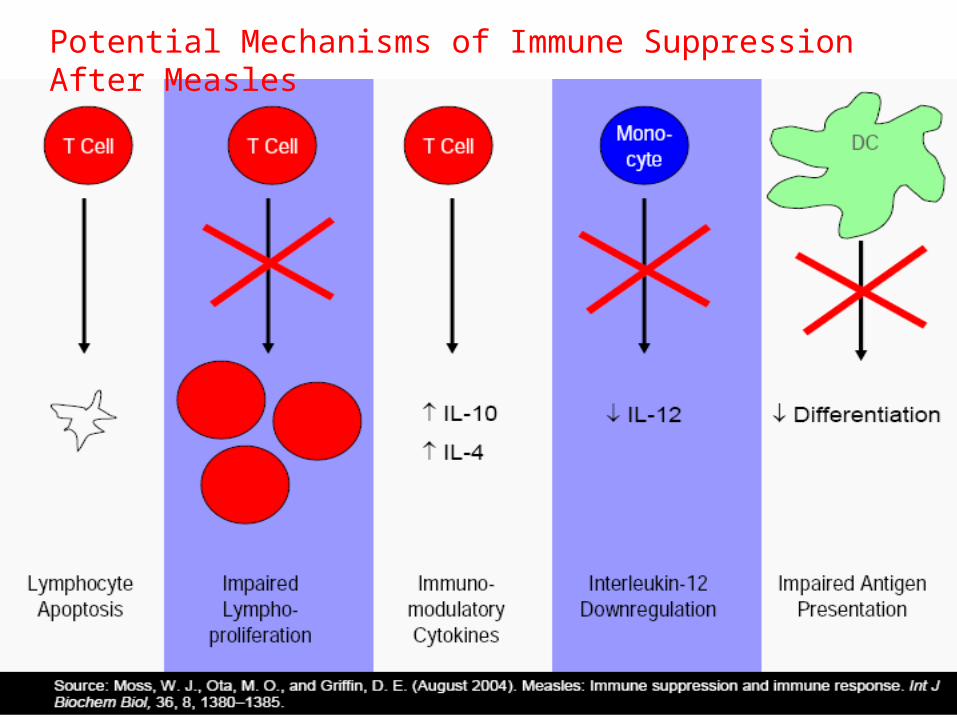
Potential Mechanisms of Immune Suppression After Measles

Measles in Immunocompromised Hosts
Observations on Measles in Persons with Impaired Immunity
Deficient antibody production• Measles virus is cleared• Host recovers but limited protection from
reinfection
Deficient cellular immunity• Delayed viral clearance• Progressive disease
Clearance and Protection
Clearance• Elimination of infected cells and circulating virus• Slowed clearance and desquamating rash with some
immune deficiencies• Progressive disease often without a rash with
deficiencies of cellular immunity
Protection• Prevention of infection (clinical)• Best correlate is level of neutralizing antibody
1000
2000
3000
4000
5000
6000
7000
8000
Lym
ph
ocy
tes/l
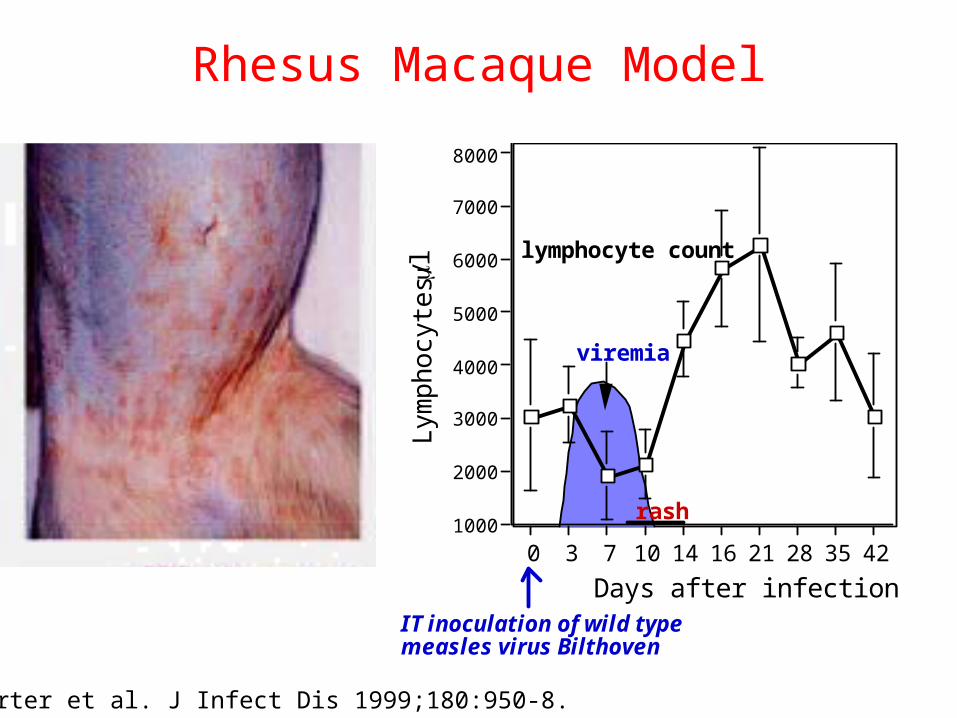
0 3 7 10 14 16 21 28 35 42
Days after infectionIT inoculation of wild typemeasles virus Bilthoven
viremia
lymphocyte count
rash
Rhesus Macaque Model
Auwaerter et al. J Infect Dis 1999;180:950-8.

Effect of CD8+ T Cell Depletion on Measles Viremia in Monkeys
Permar et al. J Virol 2003;77:4396-4400.
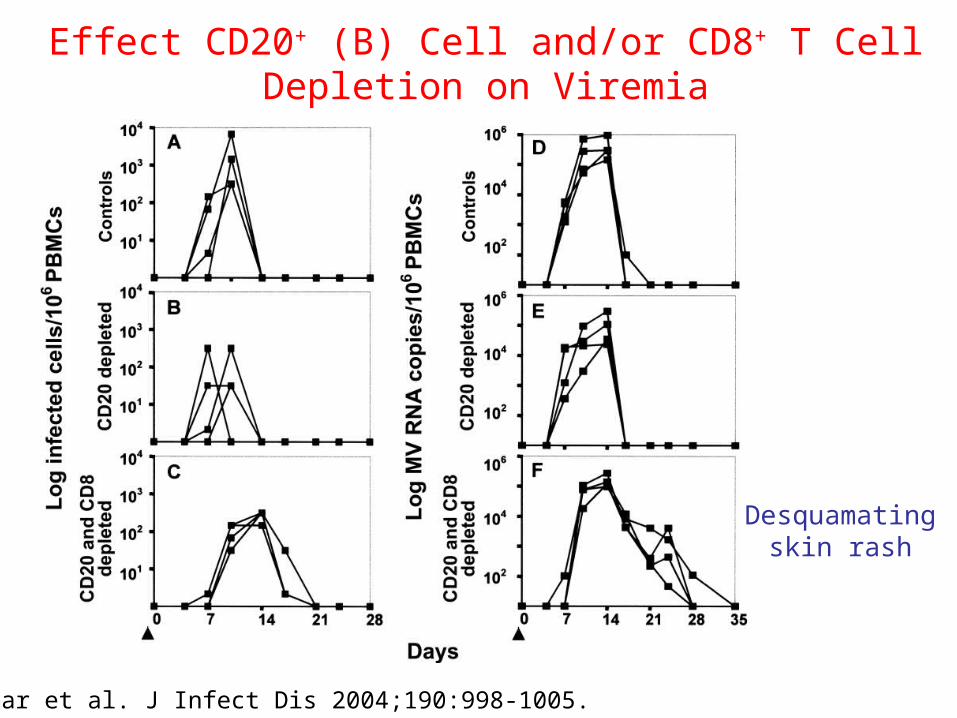
Effect CD20+ (B) Cell and/or CD8+ T CellDepletion on Viremia
Permar et al. J Infect Dis 2004;190:998-1005.
Desquamatingskin rash
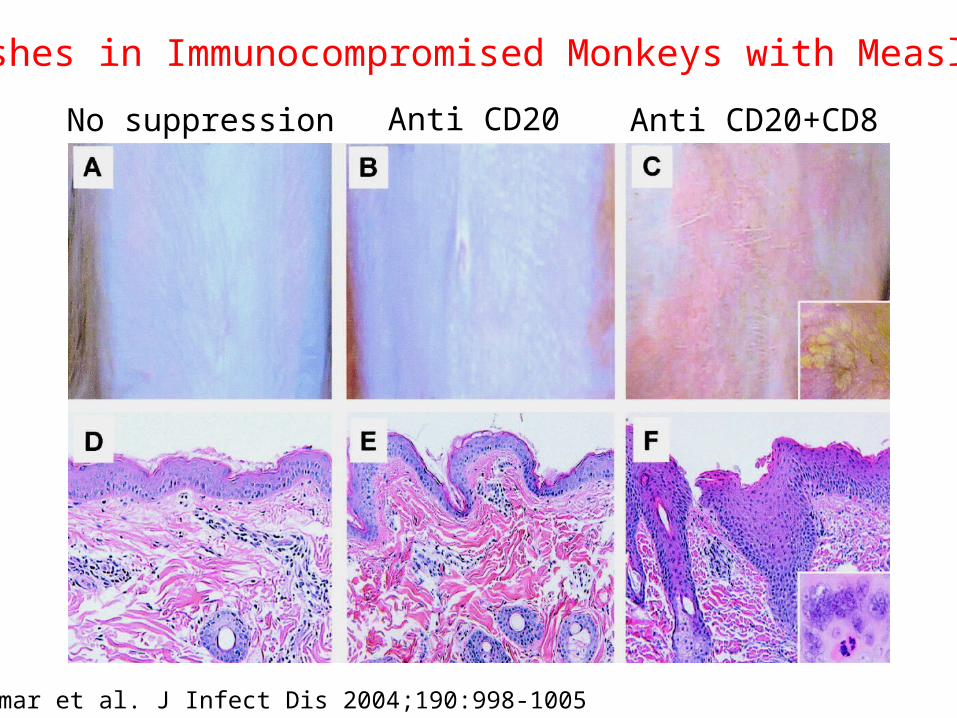
Rashes in Immunocompromised Monkeys with Measles
No suppression Anti CD20 Anti CD20+CD8
Permar et al. J Infect Dis 2004;190:998-1005
Failure to Clear Measles Virus
Diseases• Giant cell pneumonitis• Measles inclusion body encephalitis
Clinical Manifestations• Often no rash at time of measles virus infection• Progressive pulmonary or CNS disease
appears weeks to months after initial infection• Diagnosis may be difficult
Case Reports of Progressive Measles Virus Infection Associated with Immune Deficiencies
Primary immune deficiencies• Usually combined deficiencies of T and B cells• Specific diagnosis often not made
Secondary immune deficiencies• Leukemia and lymphomas• Immunosuppressive therapy (e.g. transplants)• HIV-1 infection
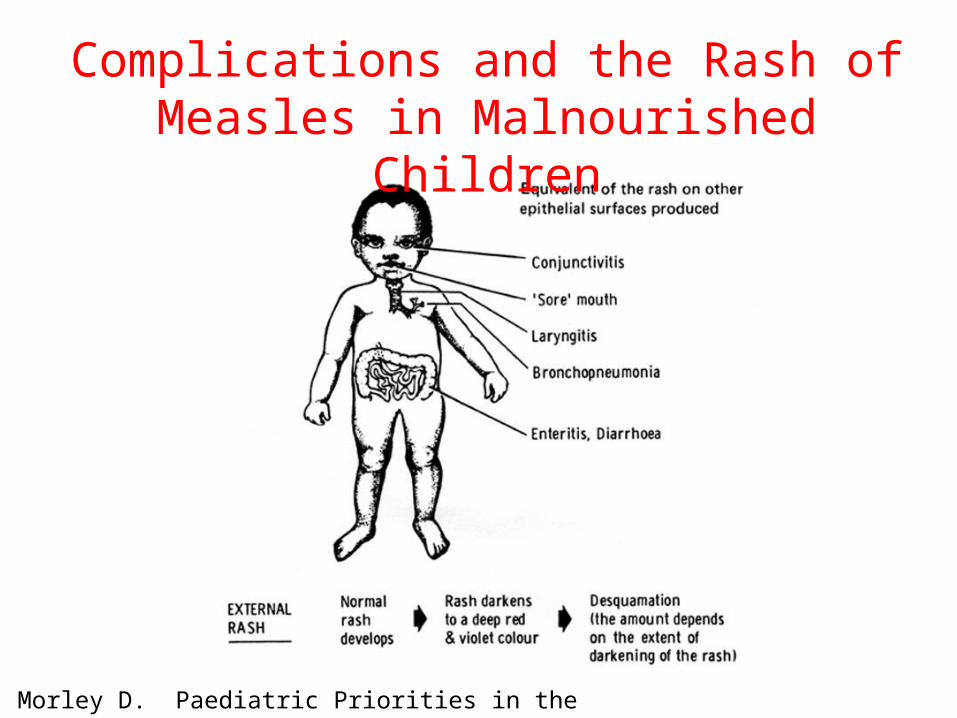
Complications and the Rash of Measles in Malnourished Children
Morley D. Paediatric Priorities in the Developing World. 1979.

Desquamating Rash in an HIV-1 Infected Child

Measles in HIV-1 Infected Children
• CDC 1988 • severe and unusual measles in 5 HIV-infected children
• Case reports of 19 co-infected children in US• ½ with absent, delayed or unusual rash• ¾ with pneumonitis• case fatality rate (CFR) 32%
• HIV-seropositive children in Africa• Zaire (1988): no difference in CFR • Zambia (1996): higher CFR (27% vs. 8%)
Moss et al. Clin Infect Dis 1999;29:106-12.
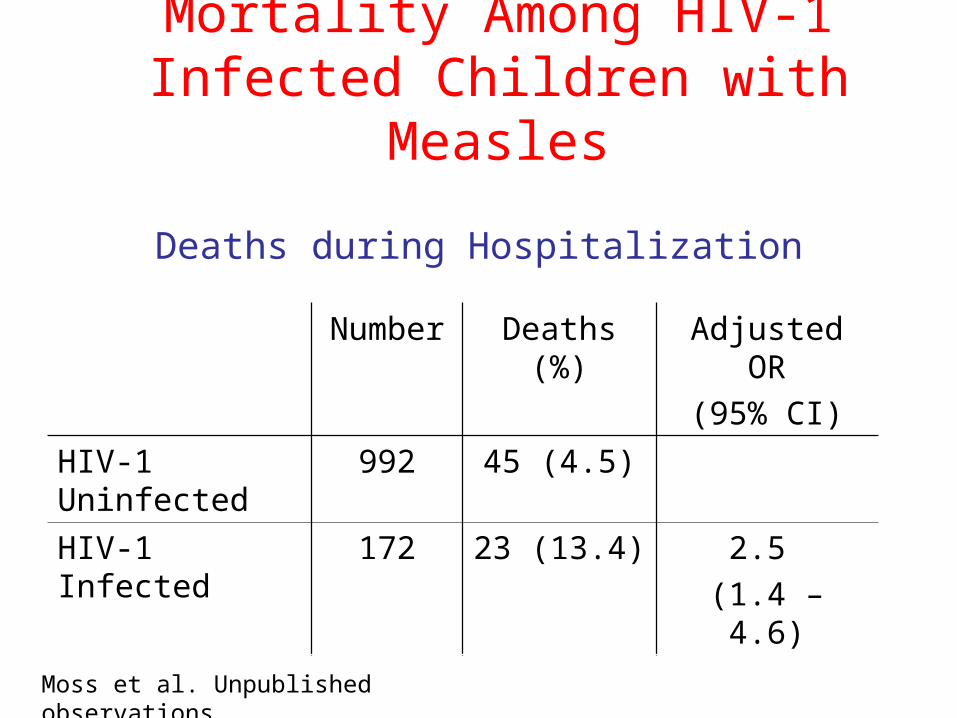
Deaths during Hospitalization
Number Deaths (%) Adjusted OR
(95% CI)
HIV-1 Uninfected 992 45 (4.5)
HIV-1 Infected 172 23 (13.4) 2.5
(1.4 – 4.6)
Moss et al. Unpublished observations.
Mortality Among HIV-1 Infected Children with Measles
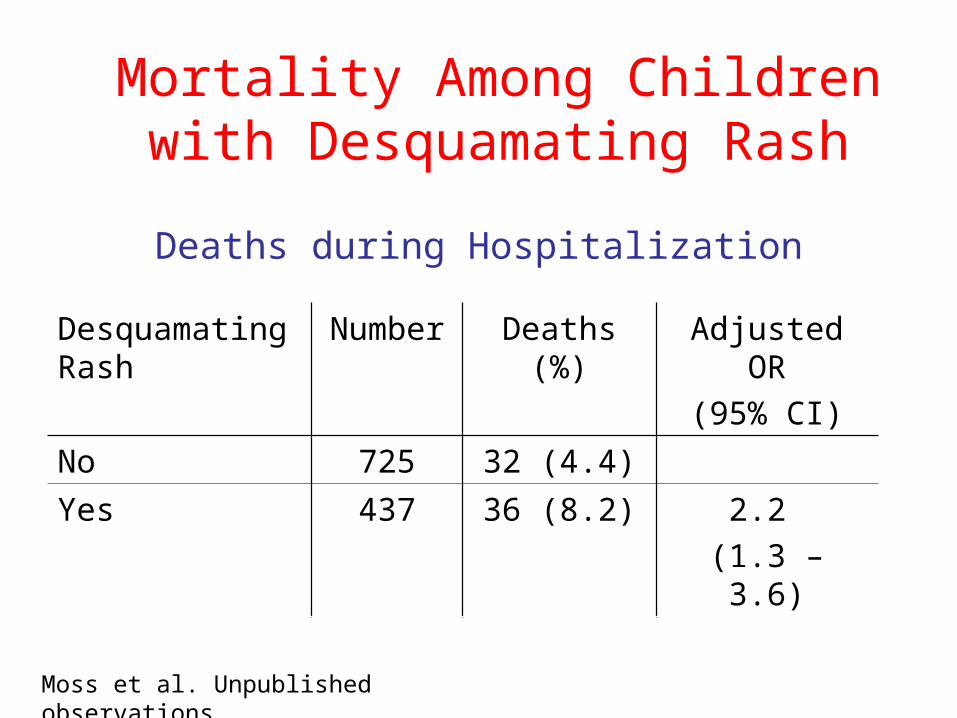
Deaths during Hospitalization
Desquamating Rash
Number Deaths (%) Adjusted OR
(95% CI)
No 725 32 (4.4)
Yes 437 36 (8.2) 2.2
(1.3 – 3.6)
Moss et al. Unpublished observations.
Mortality Among Children with Desquamating Rash
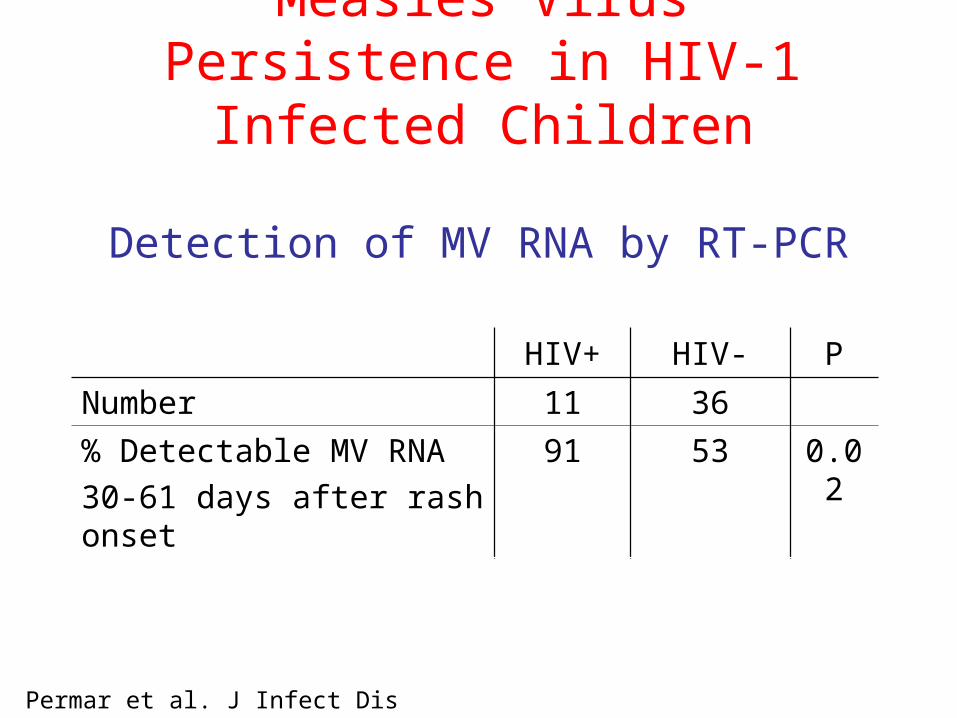
Detection of MV RNA by RT-PCR
HIV+ HIV- P
Number 11 36
% Detectable MV RNA
30-61 days after rash onset
91 53 0.02
Permar et al. J Infect Dis 2001;183:532-8.
Measles Virus Persistence in HIV-1 Infected Children

Fatal Adverse Event Due to Measles Vaccine Virus
21-year-old man with AIDS who received 2nd MMR
• No rash • Presented 11 months after measles vaccination• No clinical evidence of severe immunosuppression• Previously vaccinated against measles• Thorascopic lung biopsy• RT-PCR and genome sequencing identified measles
vaccine virus in lung tissue
Angel et al. Ann Int Med 1998;129:104-6.
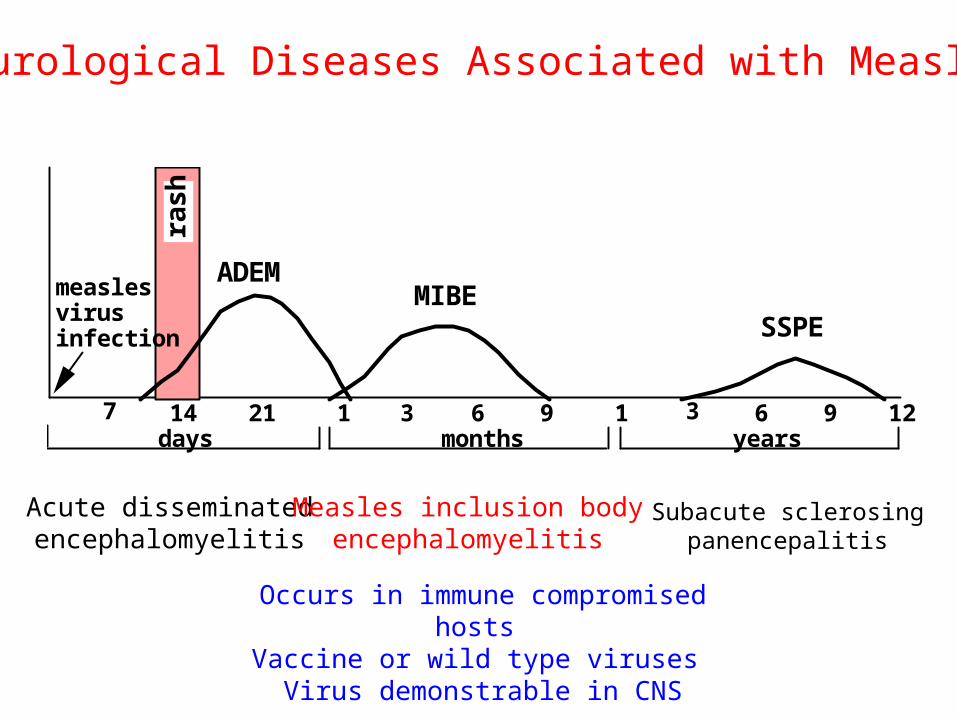
ras
h
7 14 21 1 3 6 9 1 3 6 9 12days months years
ADEMMIBE
SSPE
measles virus infection
Neurological Diseases Associated with Measles
Acute disseminatedencephalomyelitis
Measles inclusion bodyencephalomyelitis
Subacute sclerosingpanencepalitis
Occurs in immune compromised hosts Vaccine or wild type viruses Virus demonstrable in CNS

Studies Suggesting Antibodies May be Important for Measles Virus Clearance
• Levels of ADCC antibody correlate with cessation of viremia
Forthal et al., J Infect Dis 1994;169:1377-80.
• Low antibody responses predict poor outcomeWesley et al., S Afr Med J 1982;61:663-5.
• Antibodies can down regulate intracellular virus replication
Fujinami & Oldstone, Nature 1979;279:529-30.Schneider-Schaulies et al. J Virol 1992; 66:5534.

What is the role of antibody in protection from measles virus infection?
Evidence that Antibodies Alone Are Protective Against Measles
• Infants are protected by passively-acquired maternal antibody
• Passive administration of immune globulin can protect after exposure
• The best correlate for vaccine-induced protection is the level of neutralizing antibody
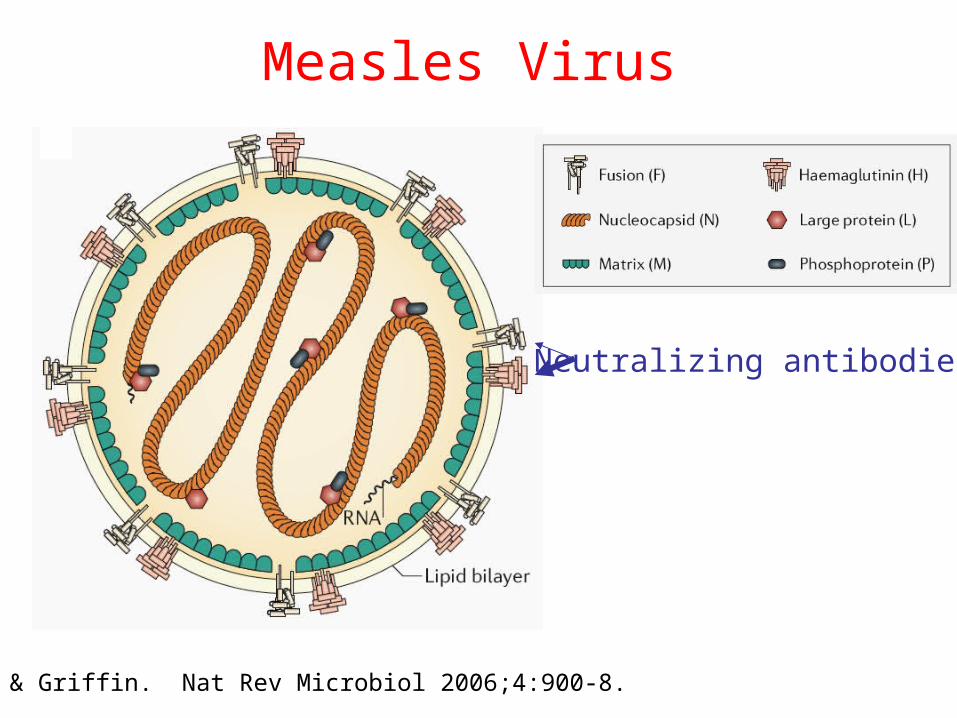
Measles Virus
Moss & Griffin. Nat Rev Microbiol 2006;4:900-8.
Neutralizing antibodies
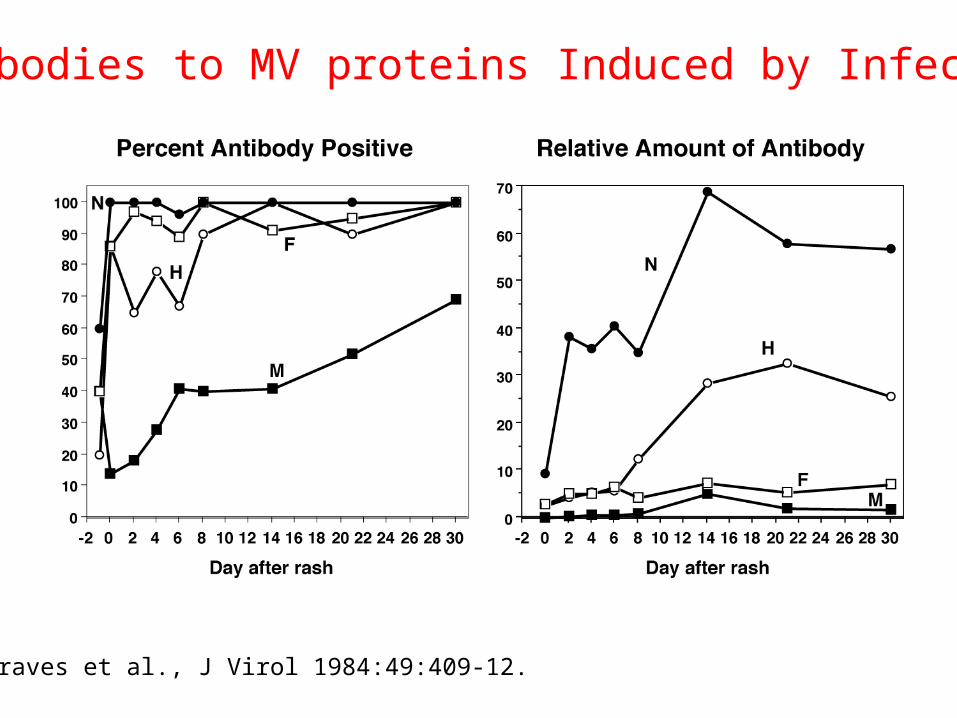
Antibodies to MV proteins Induced by Infection
Graves et al., J Virol 1984:49:409-12.
0
10
20
30
40
50
60
Pe
rce
nt
6 7 8 9 10 11 12
Months of age
% unresponsive toimmunization with livemeasles vaccine
% who havehad measles
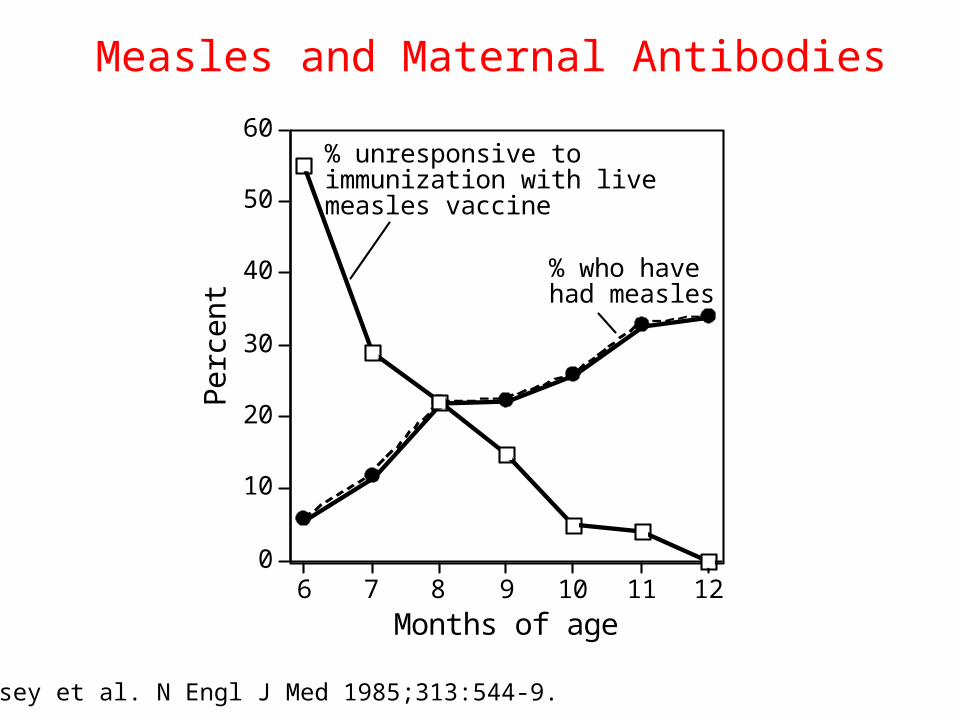
The measles problem in developing countries
Halsey et al. N Engl J Med 1985;313:544-9.
Measles and Maternal Antibodies
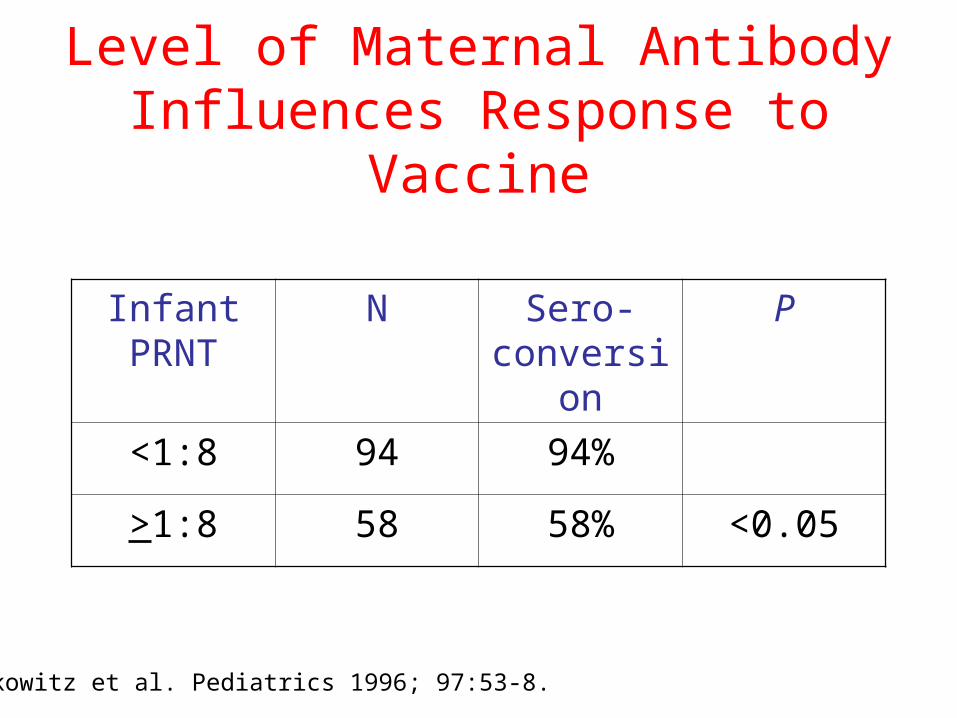
Level of Maternal Antibody Influences Response to Vaccine
Infant PRNT
N Sero-conversion
P
<1:8 94 94%
>1:8 58 58% <0.05
Markowitz et al. Pediatrics 1996; 97:53-8.
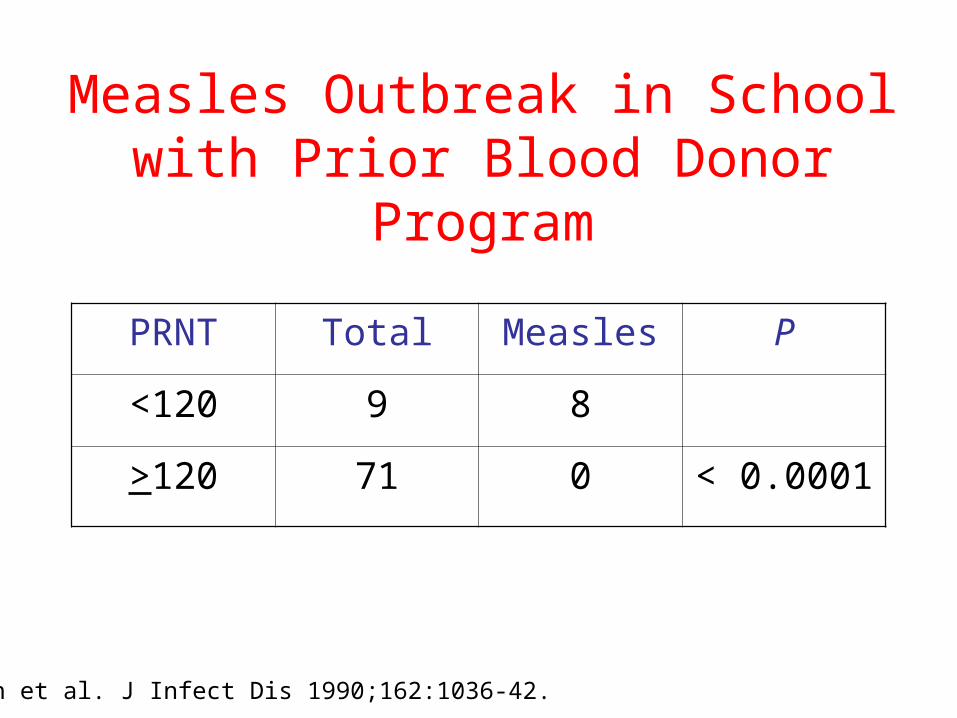
Measles Outbreak in School with Prior Blood Donor Program
PRNT Total Measles P
<120 9 8
>120 71 0 < 0.0001
Chen et al. J Infect Dis 1990;162:1036-42.
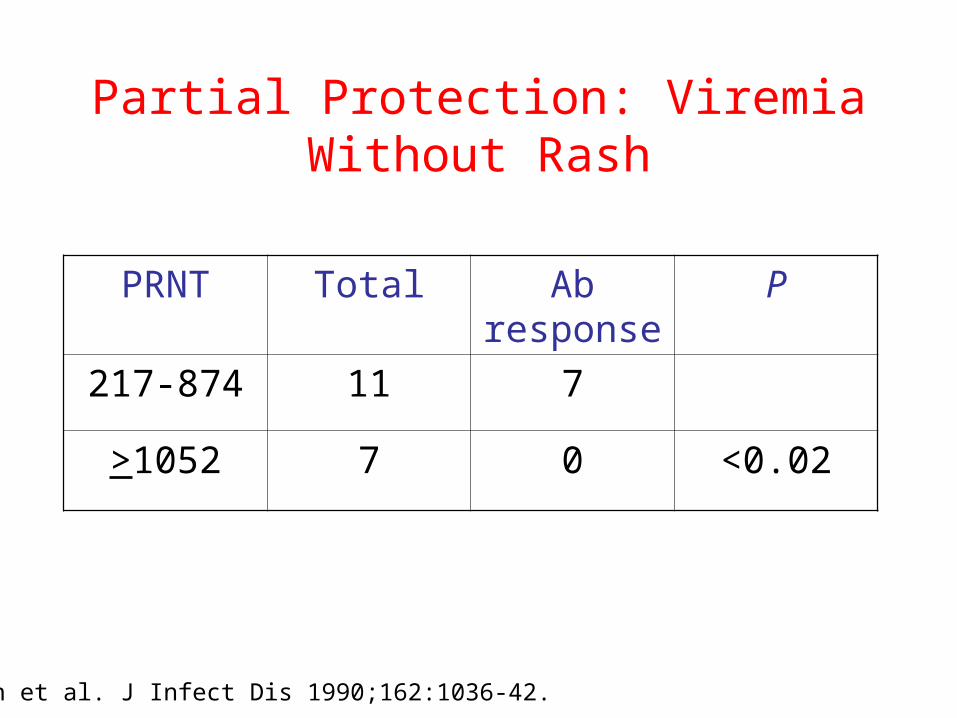
Partial Protection: Viremia Without Rash
PRNT Total Ab response
P
217-874 11 7
>1052 7 0 <0.02
Chen et al. J Infect Dis 1990;162:1036-42.
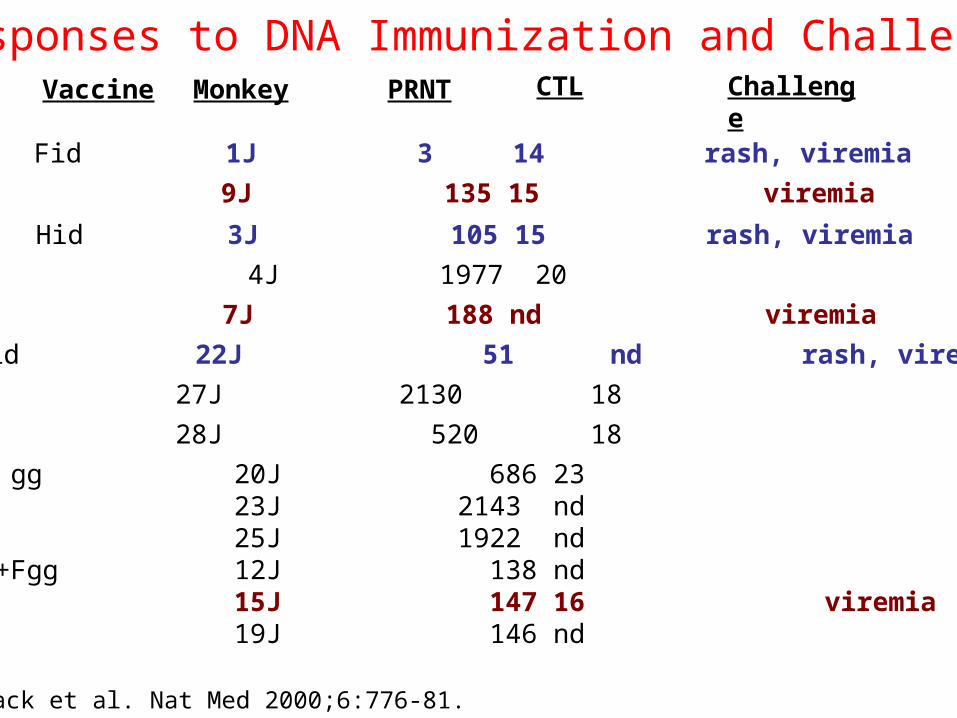
Responses to DNA Immunization and ChallengeVaccine Monkey PRNT CTL Challenge
Fid 1J 3 14 rash, viremia
9J 135 15 viremia
Hid 3J 105 15 rash, viremia
4J 1977 20
7J 188 nd viremia
F+Hid 22J 51 nd rash, viremia
27J 2130 18
28J 520 18
H gg 20J 686 23 23J 2143 nd 25J 1922 nd
H+Fgg 12J 138 nd 15J 147 16 viremia 19J 146 nd
Polack et al. Nat Med 2000;6:776-81.

Conclusions
• Clearance of MV is dependent primarily on cellular immunity
• Defects in clearance are associated with unusual manifestations of measles
No rash and progressive infection in severe immune suppression
Desquamating rash with eventual clearance in moderate immune suppression
• Protection from infection is best correlated with the level of neutralizing antibody
>120 for protection from disease (rash)>1028 for protection from infection (viremia, Ab response)
Acknowledgments
• Diane Griffin
• Sallie Permar
• Felicity Cutts
• Susana Scott
• Mwaka Monze
• Francis Kasolo