Embed Size (px)
Citation preview
Meaningful Use Panel: Stage 3 Update
Arthur Davidson, MD, MSPHDenver Public Health
Council of State and Territorial Epidemiologists Annual Conference
Pasadena, CAJune 10, 2013
1
Agenda
• Overview of Stage 3 policy perspectives– Review of HIT Policy Committee progress
• Consolidation and Deeming
• Public health agency opportunities: on-boarding
• CSTE and member role during this phase
2
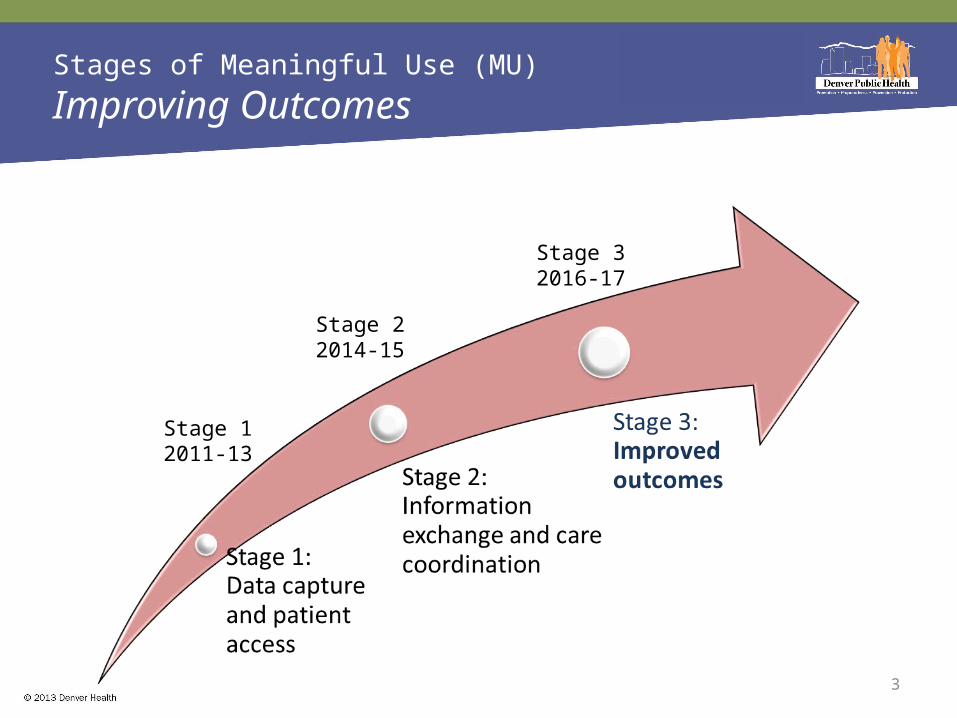
Stages of Meaningful Use (MU)
Improving Outcomes
Stage 12011-13
Stage 22014-15
Stage 32016-17
3
Original Principles for Stage 3 Recommendations
• New model of care: support team-based, outcomes-oriented, population management
• National health priorities: address National Prevention/Quality Strategies, Partnerships for Patients, and Million Hearts Campaign
• Broad applicability (since MU is a floor)– Provider specialties (e.g., primary care, specialty care)– Patient health needs– Areas of the country
• Not "topped out" or not already driven by market forces• Mature standards widely adopted or could be widely adopted
by 2016 (for stage 3)4
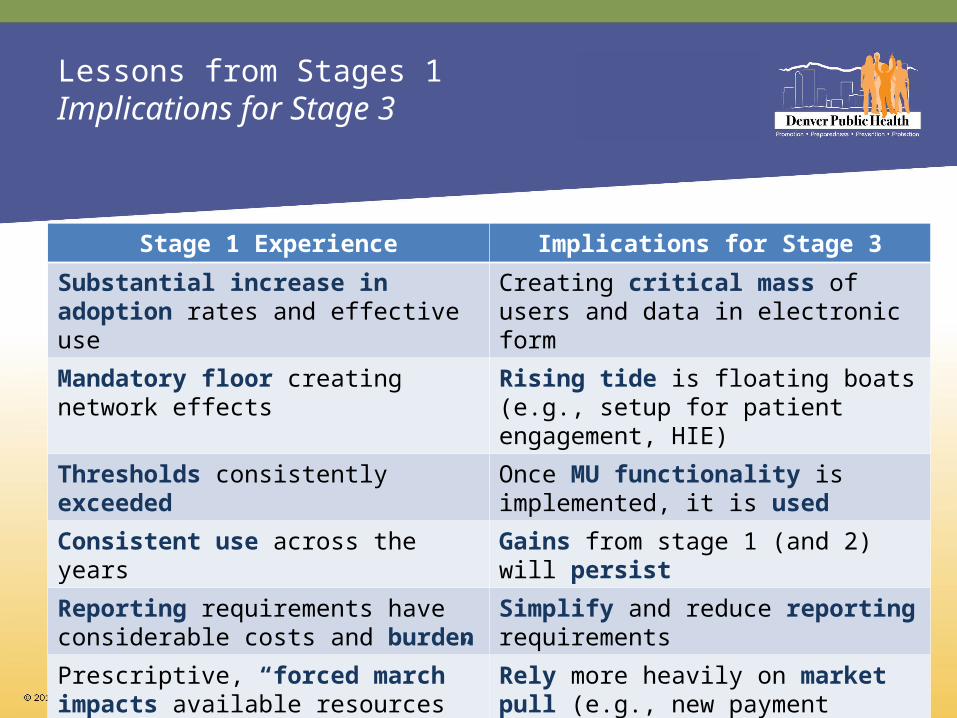
Lessons from Stages 1Implications for Stage 3
5
Stage 1 Experience Implications for Stage 3
Substantial increase in adoption rates and effective use
Creating critical mass of users and data in electronic form
Mandatory floor creating network effects Rising tide is floating boats (e.g., setup for patient engagement, HIE)
Thresholds consistently exceeded Once MU functionality is implemented, it is used
Consistent use across the years Gains from stage 1 (and 2) will persist
Reporting requirements have considerable costs and burden
Simplify and reduce reporting requirements
Prescriptive, “forced march” impacts available resources for innovation or to address local priorities
Rely more heavily on market pull (e.g., new payment incentives); promote innovative approaches i.e., reward good behavior
Additional Goals for Stage 3
• Address key gaps (e.g., interoperability, patient engagement, reducing disparities) in EHR functionality that the market will not drive alone, but are essential for all providers:– to create level playing field– to create network effects– to fulfill need for a public good
• Consolidation: combine MU objectives where higher level objective implies compliance with subsumed process objectives
• Deeming: consider alternative pathways to meet performance and/or improvement thresholds; satisfaction of subset of relevant MU functionality implicitly required to achieve performance/improvement
6
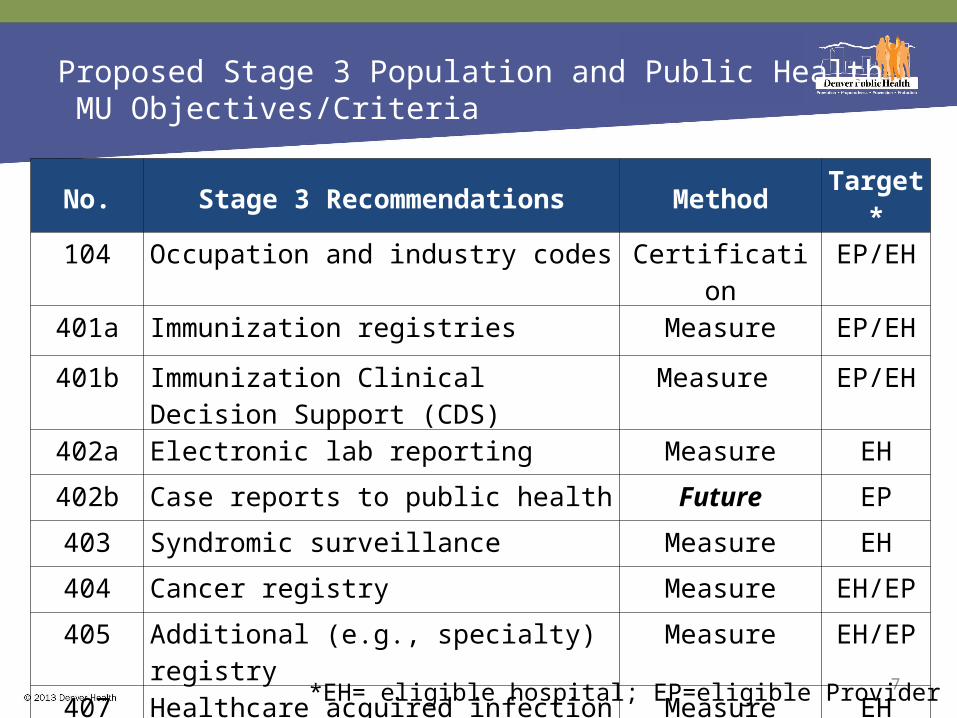
Proposed Stage 3 Population and Public Health MU Objectives/Criteria
7
No. Stage 3 Recommendations Method Target*104 Occupation and industry codes Certification EP/EH
401a Immunization registries Measure EP/EH
401b Immunization Clinical Decision Support (CDS)
Measure EP/EH
402a Electronic lab reporting Measure EH
402b Case reports to public health Future EP
403 Syndromic surveillance Measure EH
404 Cancer registry Measure EH/EP
405 Additional (e.g., specialty) registry Measure EH/EP
407 Healthcare acquired infection Measure EH
408 Adverse event reporting Future EH/EP*EH= eligible hospital; EP=eligible Provider
Consolidation Summary
• 43 MU Workgroup objectives proposed in stage 3 Request for Comment (RFC)
• Consolidated to 25 objectives• Assumptions
– Full MU Workgroup will consider RFC feedback and update criteria
– All criteria will be included in certification• Focus on advanced uses
– e.g., recording data vs. use data• Give credit for MU objectives that should be standard of practice once
passed stages 1 and 2 • Identify what needs to be “used” and certified
8
Types of Consolidation
• Advanced within concept of another objective– (no current PH example)
• Duplicative concepts -objective becomes certification only– immunization forecasting -> clinical decision support
• Demonstrated use and can trust that it will continue – patient lists, population management, ACO and
quality reporting
9
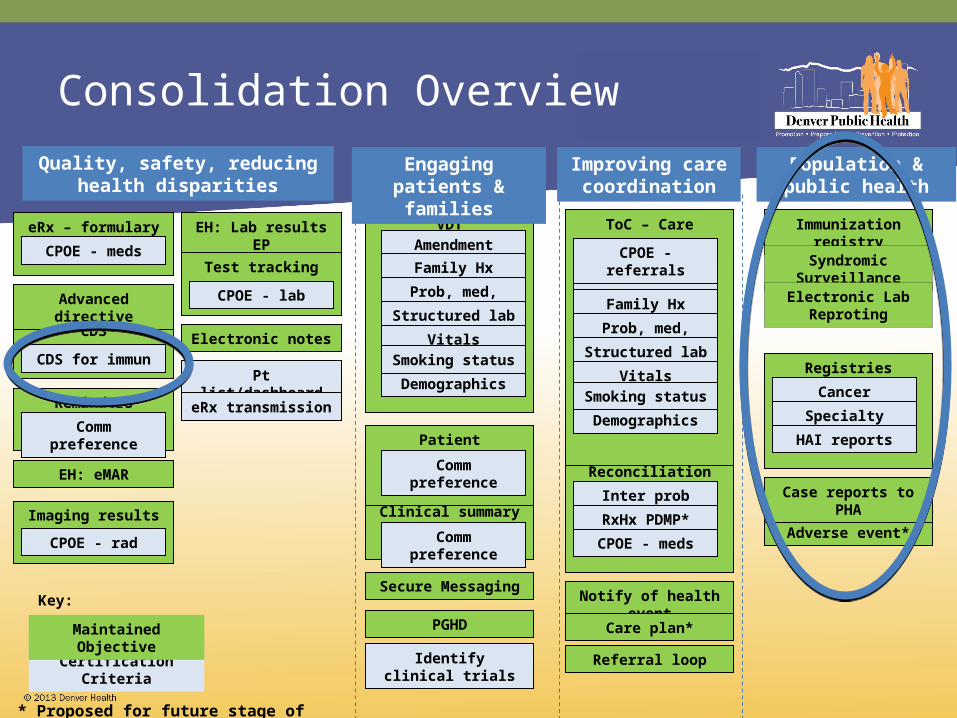
Consolidation Overview
Reconciliation
eRx – formulary
CDS
Pt list/dashboard
Reminders
EH: eMAR
EH: Lab results EP
PGHD
Clinical summary
Patient education
Secure MessagingNotify of health event
Care plan*
Immunization registry
Adverse event*
Case reports to PHA
VDT ToC – Care summary
Advanced directive
Registries
Syndromic Surveillance
Electronic Lab Reproting
Identify clinical trials
Quality, safety, reducing health disparities
Referral loop
Test tracking
Imaging results
Electronic notes
Engaging patients & families
Improving care coordination
Population & public health
eRx transmission
Certification Criteria
Maintained Objective
Key:
* Proposed for future stage of MU
Demographics
CPOE - meds
CDS for immun
Comm preference
CPOE - rad
CPOE - lab
Amendment
Family Hx
Prob, med, allg list
Structured lab
VitalsSmoking status
Comm preference
Comm preference
Cancer registry
Specialty registry
HAI reportsDemographics
Amendment
Family Hx
Prob, med, allg list
Structured lab
VitalsSmoking status
CPOE - referrals
Inter prob list*
RxHx PDMP*
CPOE - meds
Deemed MU Objectives
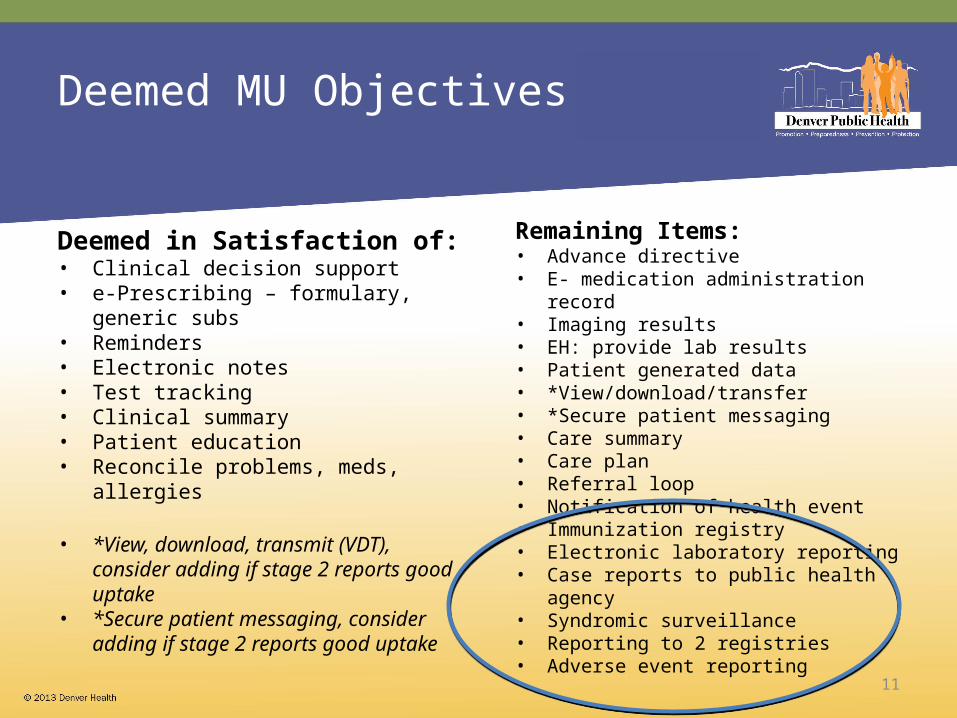
Deemed in Satisfaction of:• Clinical decision support• e-Prescribing – formulary, generic subs• Reminders• Electronic notes• Test tracking• Clinical summary• Patient education• Reconcile problems, meds, allergies
• *View, download, transmit (VDT), consider adding if stage 2 reports good uptake
• *Secure patient messaging, consider adding if stage 2 reports good uptake
Remaining Items:• Advance directive• E- medication administration record• Imaging results• EH: provide lab results• Patient generated data• *View/download/transfer• *Secure patient messaging• Care summary • Care plan• Referral loop• Notification of health event• Immunization registry• Electronic laboratory reporting• Case reports to public health agency• Syndromic surveillance• Reporting to 2 registries• Adverse event reporting
11
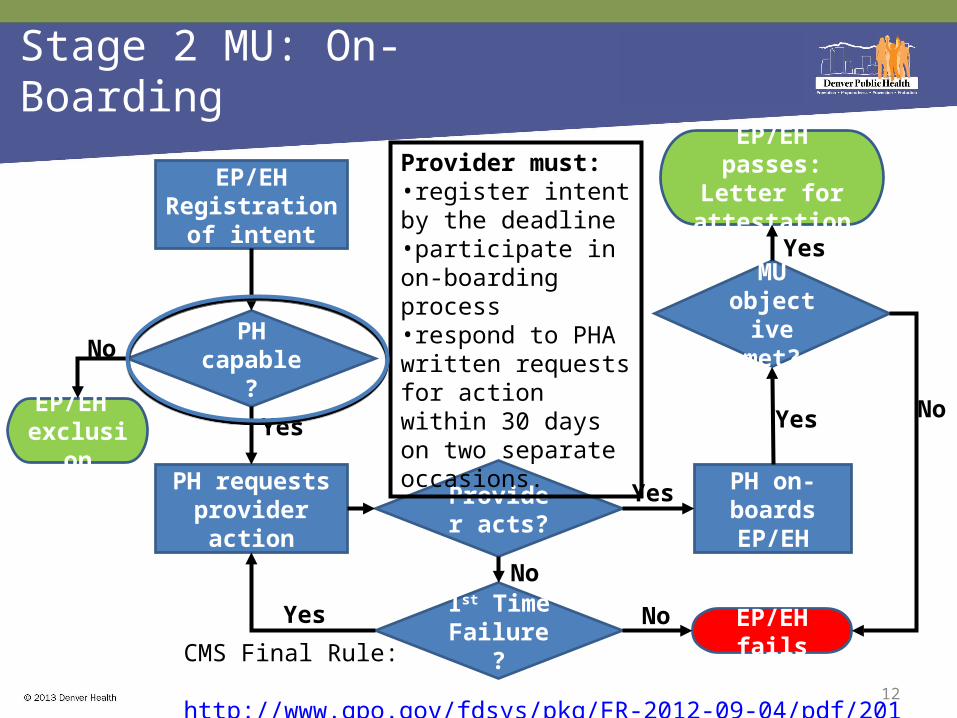
Stage 2 MU: On-Boarding
12
EP/EHRegistration of
intent
PH requests provider action
PH on-boards EP/EH
PH capable?
Provider acts?
MU objective
met?
1st Time Failure? EP/EH fails
EP/EH passes:Letter for
attestation
No
No
Yes
Yes
Provider must: •register intent by the deadline•participate in on-boarding process •respond to PHA written requests for action within 30 days on two separate occasions.
Yes
NoYesEP/EH exclusion
No
Yes
CMS Final Rule: http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-21050.pdf
13
Formed to discuss and develop consensus around standardization of the new processes across domains and across jurisdictions
Representatives from: •ASTHO, NACCHO, AIRA, ISDS, CSTE, JPHIT, NAACCR, state PHAs, ONC, CDC, PHII, others
Stage 2 MU Public Health Reporting Requirements Task Force
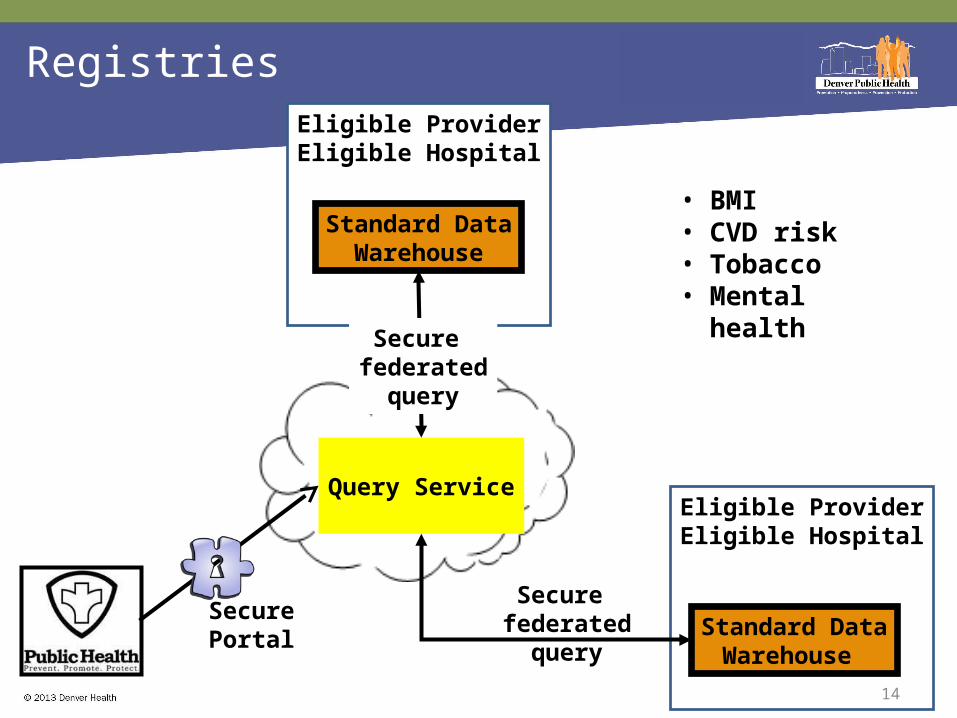
SecurePortal
Eligible ProviderEligible Hospital
Eligible ProviderEligible Hospital
Registries
14
Standard DataWarehouse
Query Service
Standard DataWarehouse
Secure federated
query
Secure federated
query
• BMI• CVD risk• Tobacco• Mental health
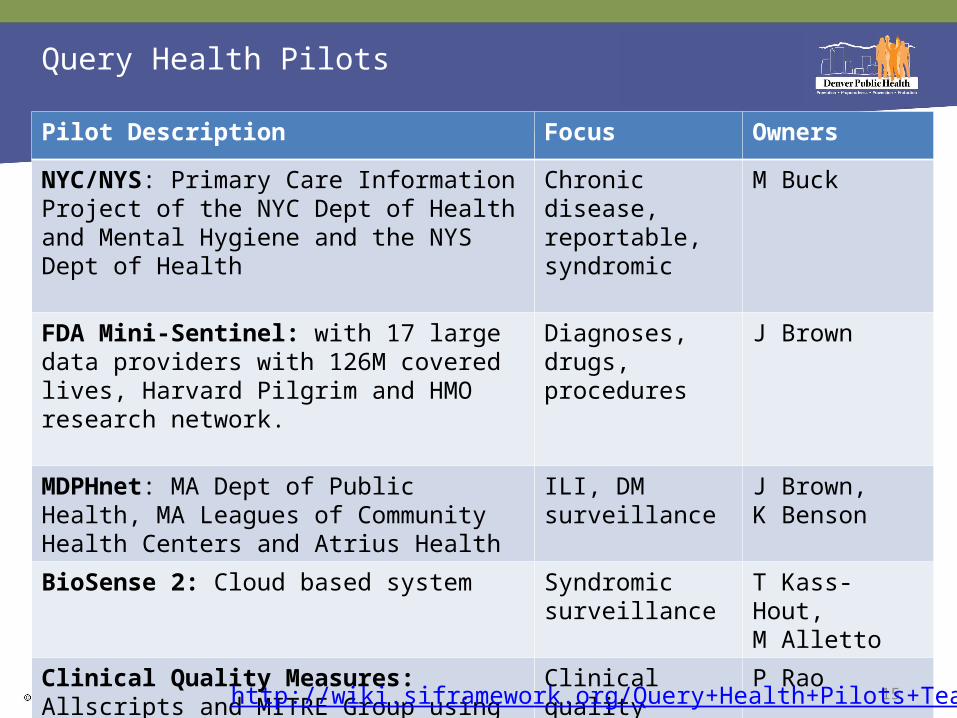
Query Health Pilots
Pilot Description Focus Owners
NYC/NYS: Primary Care Information Project of the NYC Dept of Health and Mental Hygiene and the NYS Dept of Health
Chronic disease, reportable, syndromic
M Buck
FDA Mini-Sentinel: with 17 large data providers with 126M covered lives, Harvard Pilgrim and HMO research network.
Diagnoses, drugs, procedures
J Brown
MDPHnet: MA Dept of Public Health, MA Leagues of Community Health Centers and Atrius Health
ILI, DM surveillance
J Brown, K Benson
BioSense 2: Cloud based system Syndromic surveillance
T Kass-Hout, M Alletto
Clinical Quality Measures: Allscripts and MITRE Group using Health Quality Measure Format (HQMF) for Stage 2 CQM reporting.
Clinical quality measures in EHR
P Rao
15http://wiki.siframework.org/Query+Health+Pilots+Team
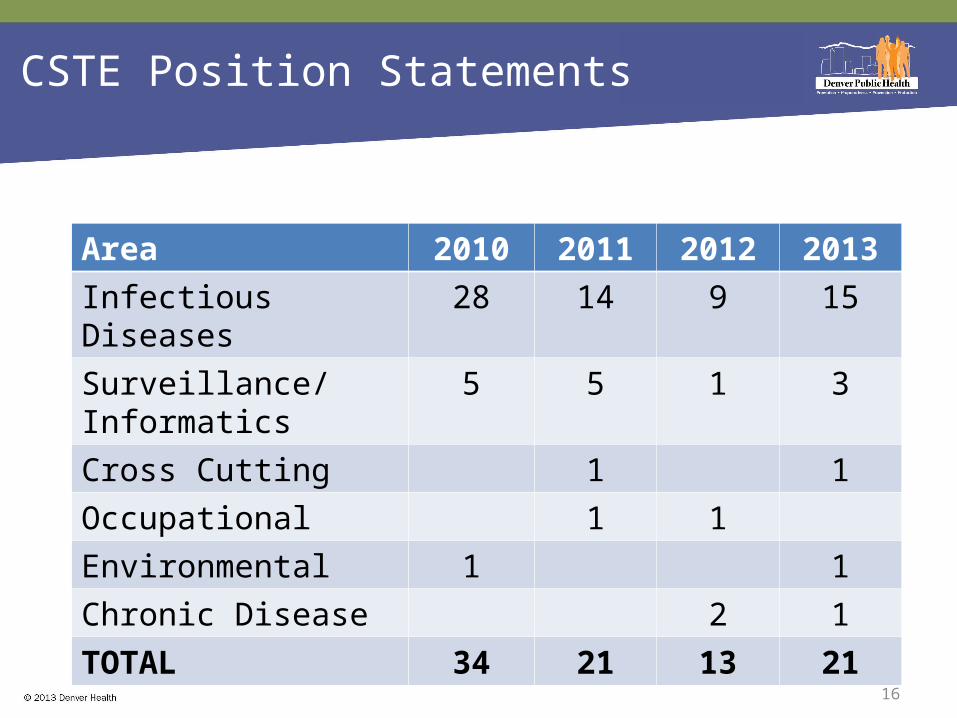
CSTE Position Statements
16
Area 2010 2011 2012 2013Infectious Diseases 28 14 9 15Surveillance/Informatics 5 5 1 3Cross Cutting 1 1Occupational 1 1Environmental 1 1Chronic Disease 2 1TOTAL 34 21 13 21
17
Conclusions
• Stage 3 MU will push for improved outcomes with greater emphasis on health information exchange
• Public health agencies will demonstrate their capacity/desire to participate through on-boarding in Stage 2
• CSTE can provide new data regarding functionality and standards to influence policy decisions
• CSTE and its members have a unique opportunity to be more strategic, with cross-cutting approaches to informatics investments