Embed Size (px)
Citation preview

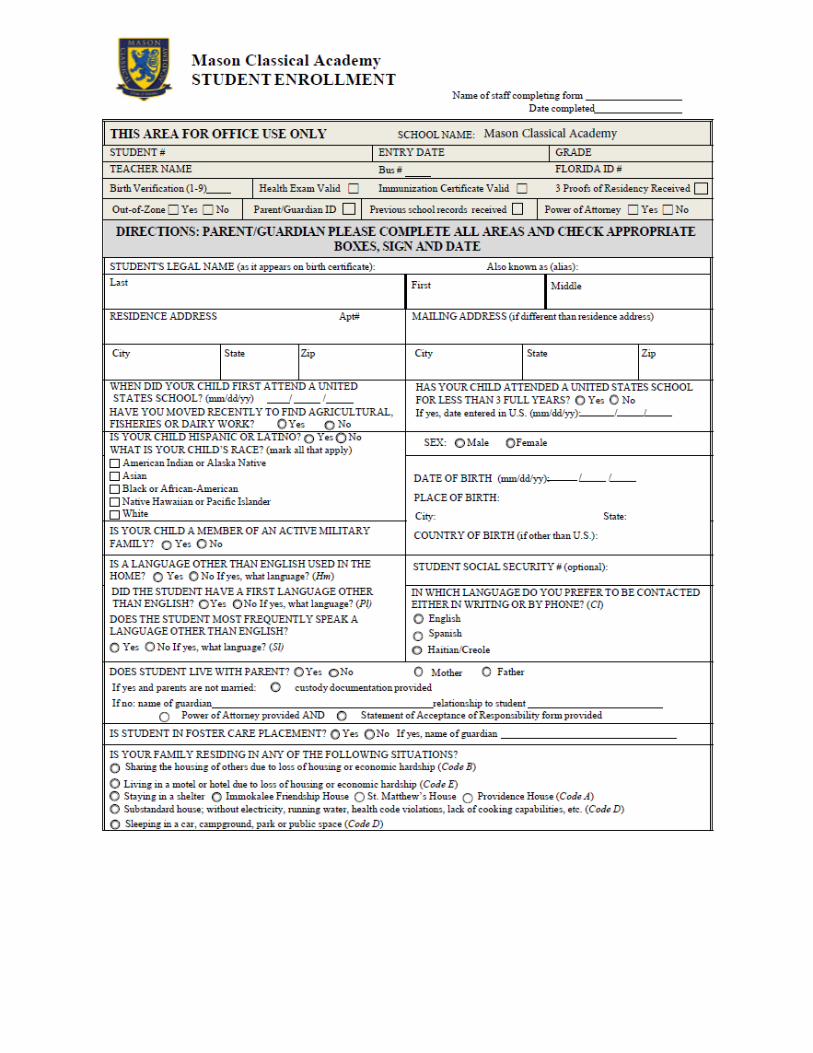
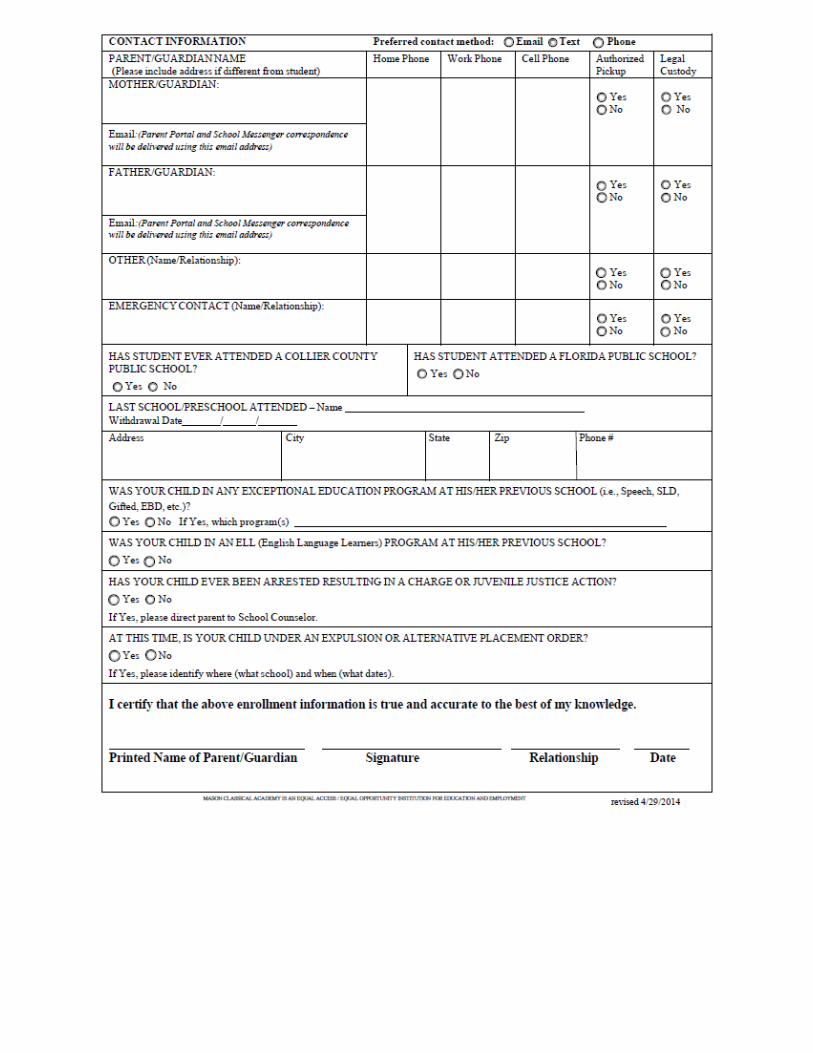
Student Records Request Mason Classical
Academy
Date: ___________________
Last School Attended:
_________________________________________________________________
Address of Last School Attended:
____________________________________________________________________________
____________________________________________________________________________
Last School Phone No: ____________________________________________________________________________
Last School Fax No: ____________________________________________________________________________
PLEASE SEND A TRANSCRIPT OR THE OFFICIAL RECORDS FOR:
__________________________________________ _________ ____________ Student Name Grade Date of Birth
PLEASE INCLUDE: • Current Grades• Test Scores• Exceptional Education Records• Last day of attendance
I hereby give permission for the above named school to release all student records as herein requested to facilitate the enrollment of my child at the Treasure Coast Classical Academy.
__________________________________________________ ___________________ Parent/Guardian Signature Date
3073 Horseshoe Dr. S., Naples, FL 34104 Main (239) 227-2838 Fax (239) 201-2056
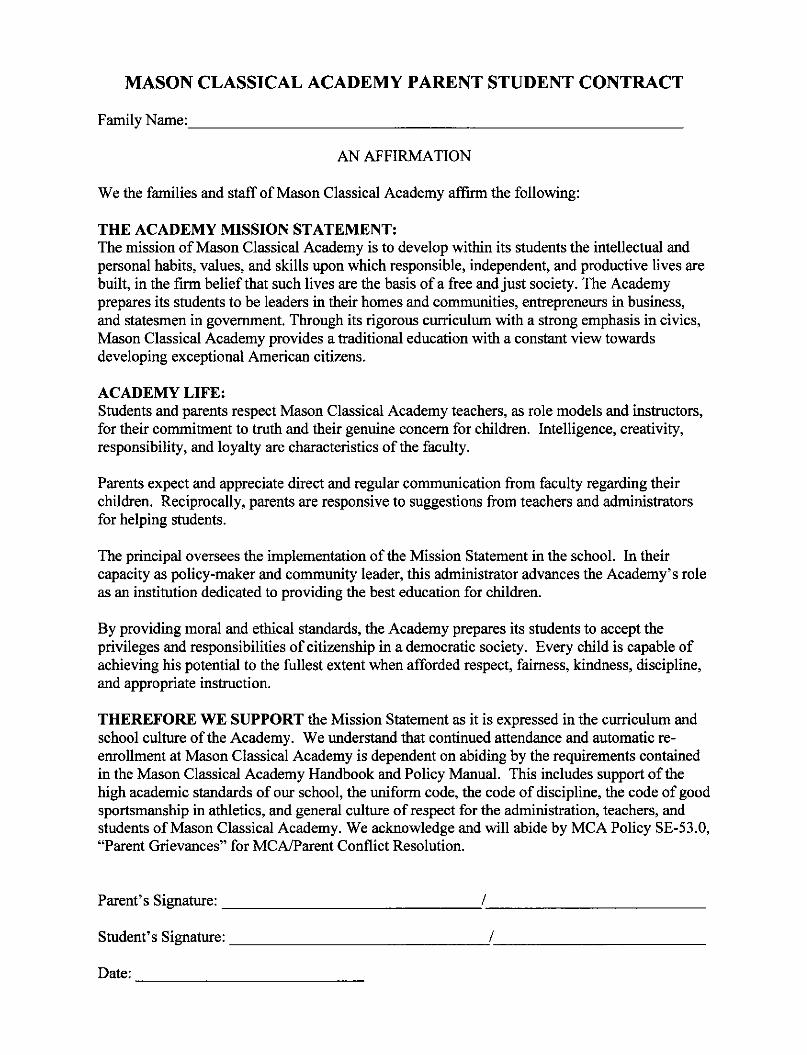
MASON CLASSICAL ACADEMY
FINANCIAL ASSISTANCE MEAL PROGRAM
Dear Parent/Guardian:
The Mason Classical Academy Financial Assistance Meal Program (F AMP) is a MCA charitable assistance program that helps supplement the diets of low-income families, by providing them with food and nutrition assistance at no or reduced cost.
Mason Classical Academy does not receive funding from the government to fund the Financial Assistance Meal program. All funds used to subsidize meals for students come out of MCA's School Budget.
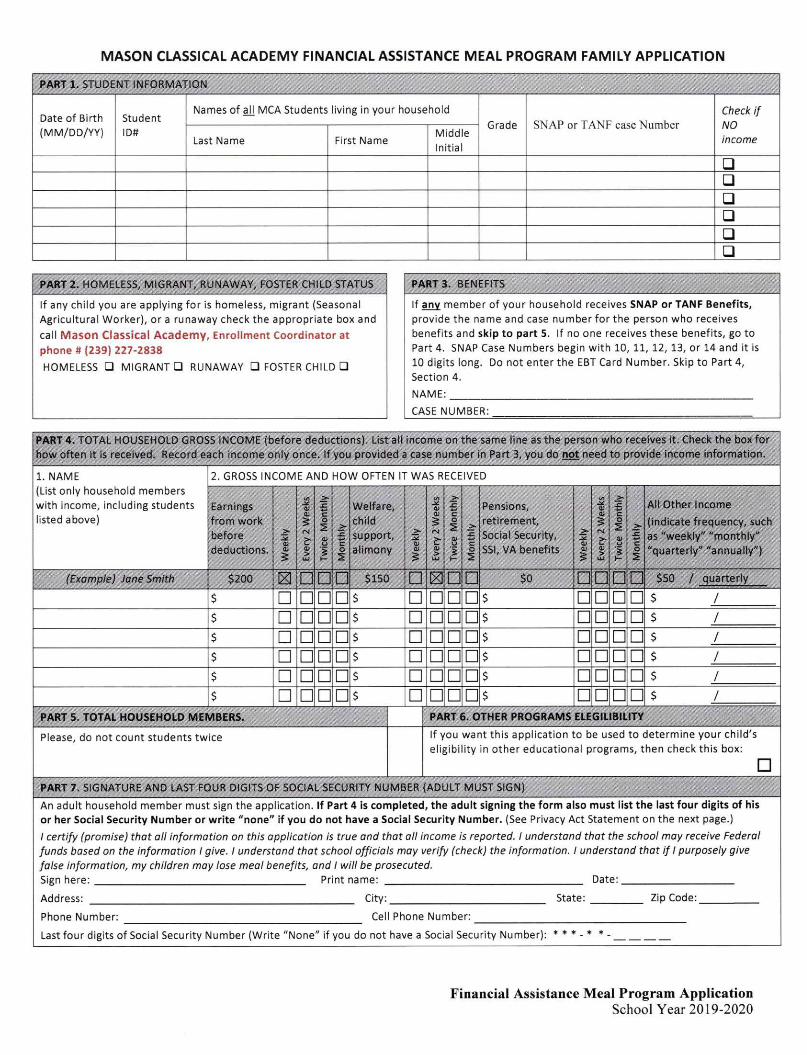
Reduced price meals are $0.30 for breakfast and $0.40 for lunch.
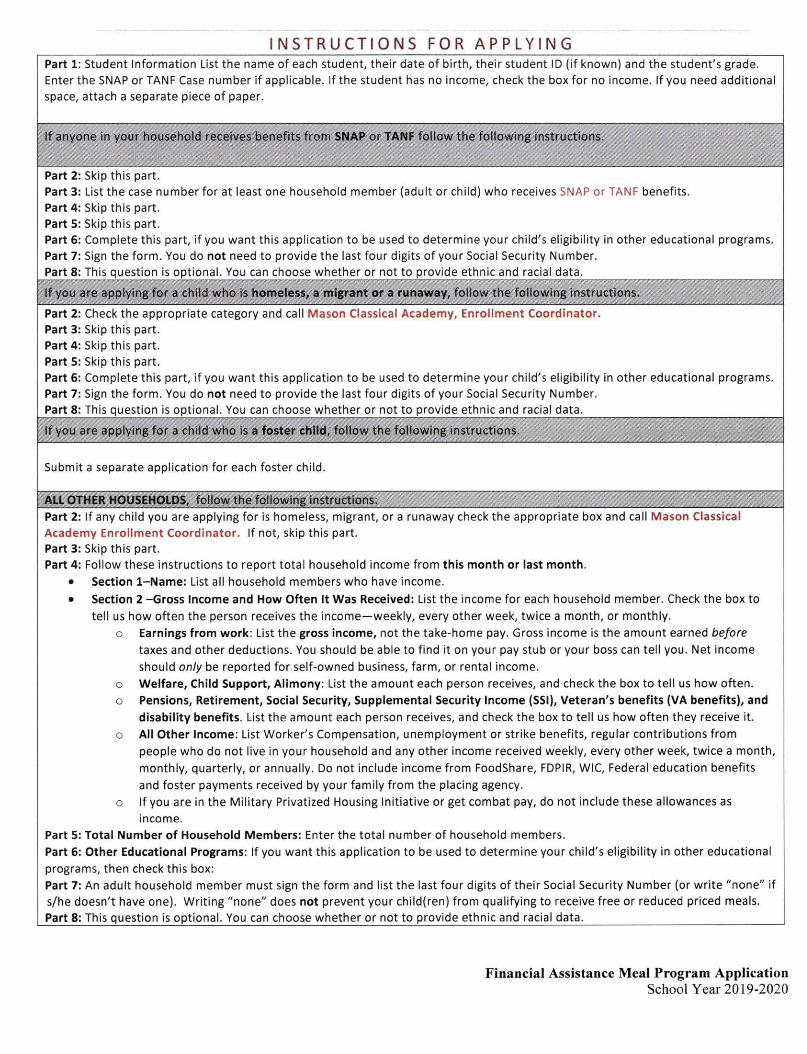
1. DO I NEED TO FILL OUT AN APPLICATION FOR EACH CHILD? No. Complete the
application to apply for free or reduced meals for all students in the household.
2. WHO CAN GET FREE OR REDUCED PRICE MEALS? Your children can get free or low cost
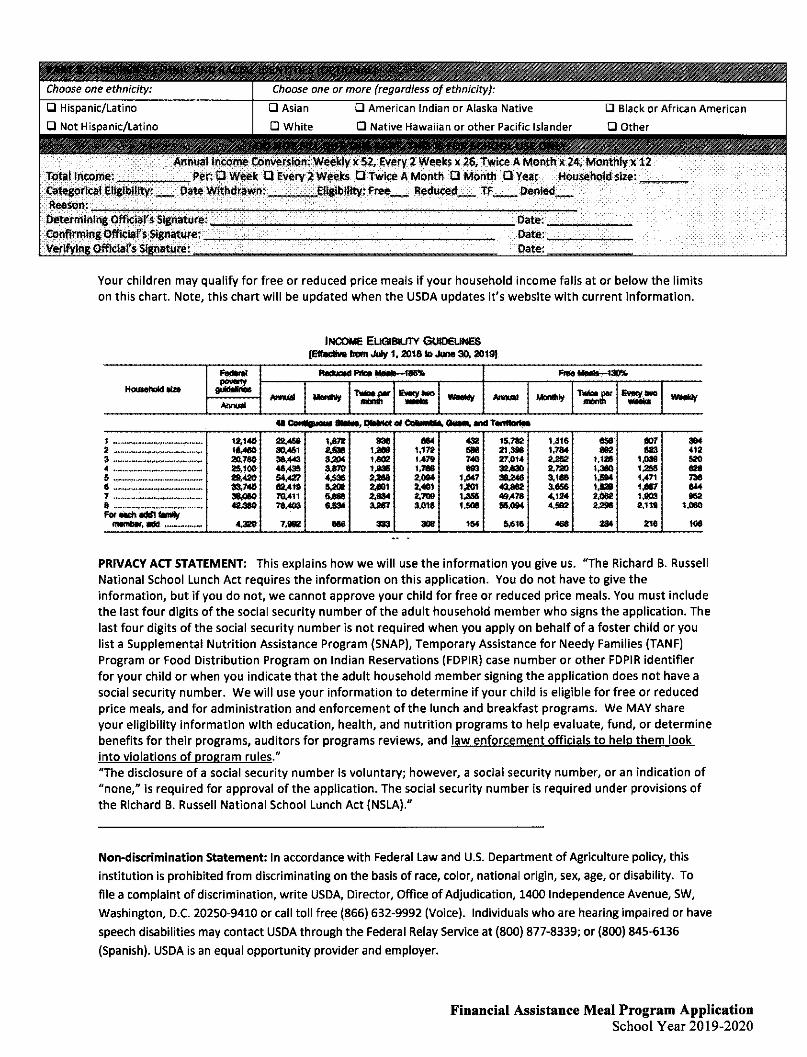
meals if your household income is within the Financial Assistance limits on the Income Eligibility
Guidelines, shown on this application.
3. WILL THE INFORMATION I GIVE BE VERIFIED? Yes. We require the most recent year's tax
filing to verify annual income. A new application will be required and annual income will be
verified for every subsequent school year the child(ren) attend(s) Mason Classical Academy.
4. WHAT WILL HAPPEN IF I GIVE FALSE INFORMATION? You may be prosecuted.
5. WHAT IF I DISAGREE WITH THE SCHOOL'S DECISION ABOUT MY APPLI CATION?
Contact Mr. Joe Whitehead, MCA's Assistant Principal. [email protected]
If you have other questions or need help, call (239) 227-2838 Si necesiLa ayuda, par favor !lame al telefono: (239) 227-2838 Si vous voudriez d'aide, contactez nous au numero: (239) 227-2838
Financial Assistance Meal Program Application School Year 2019-2020
MASON CLASSICAL ACADEMY
Student Waiver ALL EVENTS, SPORTS, CLUBS, and/or ACTIVITIES 2019-2020
This form gives permission for _____________________ to
participate in student events, sports, clubs, and/or activities at Mason Classical Academy
and/or venue designated by Mason Classical Academy.
Please carefully read the following statements below. fill in the required information. date and sign this form.
By signing this form, you are releasing MCA, and their respective officers, directors, agents, members, employees, teachers, representatives and volunteers from any claims for liability, personal injury, death, or property loss incurred in connection with any activity, sport, club, and/or event that your student attends at Mason Classical Academy and/or venue designated by Mason Classical Academy. You are also giving the Released Parties, their officers, directors, agents, members, employees, teachers, representatives, and volunteer permission to seek whatever medical attention we deem necessary in the event of an emergency.
I agree ( on behalf of myself and/or my minor child) that the Released Parties, together with their officers, directors, agents, members, employees, teachers, representatives and volunteers, shall not be responsible for and are hereby released from any claims or liability for any personal injury, death, or property loss incurred in connection with any student activity, sport, club, and/or event at Mason Classical Academy or venue designated by Mason Classical Academy.
I also authorize the Released Parties to seek emergency medical treatment on behalf of me and/or
my minor child in the event that such treatment is deemed necessary or appropriate by the Released Parties and release the Released Parties from any liability related to that decision or treatment.
I understand that participation by me and/or my minor child in student activities, sports, clubs, and/or events is volW1tary.
I understand that physical activities, sports, and the use of inflatable jumping units may be
part of student activities and events.
I understand that the Released Parties may not carry insurance to cover any injury, loss or other damages that may occur during my and/or my minor child's participation in student activities, sports, clubs, and/or events.
This waiver covers all events, sports, clubs, activities, and any other school-sponsored gathering occurring at any time during the 2019-2020 school year.
Signature of Parent/Guardian: ________________ Date: ____ _
Print signer's name: ________________ Phone No.: ______ _
Annual Student Emergency Information Card for School Year 2019-2020 Including Available Health Screenings
THIS CARD MUST BE COMPLETED BY PARENT/GUARDIAN AND SIGNED EACH SCHOOL YEAR Please notify the school immediately if any of the following information changes during the year
PLEASE COMPLETE IMPORTANT INFORMATION ON REVERSE SIDE AND RETURN SIGNED CARD TO CHILD’S SCHOOL
Rev. 4/2019
Please provide all information below (print), even if there are no changes since last year. Student’s Legal Name: Last: First: Middle:
Sex: Male Female Date of Birth: _____/____/____ Student Transportation: Walks Rides bus Car rider
Does student live with: Both Mother Father If student does not live with parent(s), name/relationship of guardian: _______________________________________________________________________________________________________________________________________________________
Student’s Home Address: City: State/ Zip code:
Names of Adults Authorized to Pick Up Student in Case of Emergency (Attach additional pages if necessary)
Emergency Contact Home/Work Phone Cell Phone E-Mail * Mother/Guardian
* Father/Guardian
*If the determination of custody / guardianship is court-ordered, please provide a copy of the Order or Parenting Plan.
Teacher: Student ID #: Grade: Reviewed by: Focus Updated (Date):
Student Health and Medical Information Does your child have any of the following health conditions? Please check all that apply.
__ Asthma (medication needed at school) __ Asthma (no medication at school) __ Heart Condition __ Seizures/Epilepsy __ Cystic Fibrosis
__ Allergy (Epi-pen required) __ Allergy (No Epi-pen) __ Cancer __ Cerebral Palsy __ Attention Deficit Disorder
__ Diabetes (Type 1) __ Diabetes (Type 2) __ Sickle Cell Disease __ Hemophilia __ Wears glasses
__ Other _______________________________________________________________________________________________
Comments: ____________________________________________________________________________________________
***You must contact the school nurse if the student has a health condition or requires nursing care at school***
Medication Does your child require regular or emergency medication at school? No Yes If yes, specify: _________________________ _________________________________________________________________________________________________________
A completed and signed Medication Authorization form must be submitted to the school if medication is required.
This form is available at: http://www.collierschools.com/HealthForms
Reviewed by:_________________________ Date: __________ Actions: ______________________________________________
Name of Child’s Physician: Phone Number:
Name of Child’s Dentist: Phone Number:
Is your child covered by: __ Private Insurance __ Healthy Kids __Medicaid __No Insurance
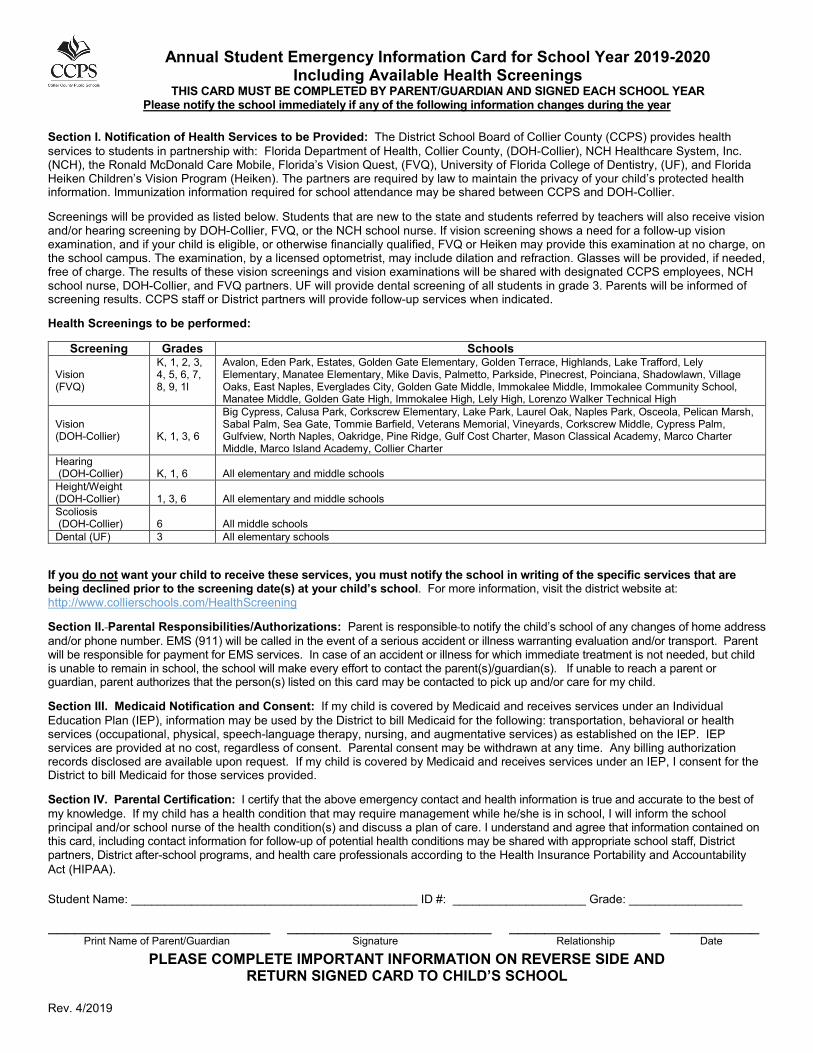
Annual Student Emergency Information Card for School Year 2019-2020 Including Available Health Screenings
THIS CARD MUST BE COMPLETED BY PARENT/GUARDIAN AND SIGNED EACH SCHOOL YEAR Please notify the school immediately if any of the following information changes during the year
PLEASE COMPLETE IMPORTANT INFORMATION ON REVERSE SIDE AND RETURN SIGNED CARD TO CHILD’S SCHOOL
Rev. 4/2019
Section I. Notification of Health Services to be Provided: The District School Board of Collier County (CCPS) provides health services to students in partnership with: Florida Department of Health, Collier County, (DOH-Collier), NCH Healthcare System, Inc. (NCH), the Ronald McDonald Care Mobile, Florida’s Vision Quest, (FVQ), University of Florida College of Dentistry, (UF), and Florida Heiken Children’s Vision Program (Heiken). The partners are required by law to maintain the privacy of your child’s protected health information. Immunization information required for school attendance may be shared between CCPS and DOH-Collier.
Screenings will be provided as listed below. Students that are new to the state and students referred by teachers will also receive vision and/or hearing screening by DOH-Collier, FVQ, or the NCH school nurse. If vision screening shows a need for a follow-up vision examination, and if your child is eligible, or otherwise financially qualified, FVQ or Heiken may provide this examination at no charge, on the school campus. The examination, by a licensed optometrist, may include dilation and refraction. Glasses will be provided, if needed, free of charge. The results of these vision screenings and vision examinations will be shared with designated CCPS employees, NCH school nurse, DOH-Collier, and FVQ partners. UF will provide dental screening of all students in grade 3. Parents will be informed of screening results. CCPS staff or District partners will provide follow-up services when indicated.
Health Screenings to be performed:
Screening Grades Schools Vision (FVQ)
K, 1, 2, 3, 4, 5, 6, 7, 8, 9, 1l
Avalon, Eden Park, Estates, Golden Gate Elementary, Golden Terrace, Highlands, Lake Trafford, Lely Elementary, Manatee Elementary, Mike Davis, Palmetto, Parkside, Pinecrest, Poinciana, Shadowlawn, Village Oaks, East Naples, Everglades City, Golden Gate Middle, Immokalee Middle, Immokalee Community School, Manatee Middle, Golden Gate High, Immokalee High, Lely High, Lorenzo Walker Technical High
Vision (DOH-Collier)
K, 1, 3, 6
Big Cypress, Calusa Park, Corkscrew Elementary, Lake Park, Laurel Oak, Naples Park, Osceola, Pelican Marsh, Sabal Palm, Sea Gate, Tommie Barfield, Veterans Memorial, Vineyards, Corkscrew Middle, Cypress Palm, Gulfview, North Naples, Oakridge, Pine Ridge, Gulf Cost Charter, Mason Classical Academy, Marco Charter Middle, Marco Island Academy, Collier Charter
Hearing (DOH-Collier)
K, 1, 6
All elementary and middle schools
Height/Weight (DOH-Collier)
1, 3, 6
All elementary and middle schools
Scoliosis (DOH-Collier)
6
All middle schools
Dental (UF) 3 All elementary schools
If you do not want your child to receive these services, you must notify the school in writing of the specific services that are being declined prior to the screening date(s) at your child’s school. For more information, visit the district website at: http://www.collierschools.com/HealthScreening
Section II. Parental Responsibilities/Authorizations: Parent is responsible to notify the child’s school of any changes of home address and/or phone number. EMS (911) will be called in the event of a serious accident or illness warranting evaluation and/or transport. Parent will be responsible for payment for EMS services. In case of an accident or illness for which immediate treatment is not needed, but child is unable to remain in school, the school will make every effort to contact the parent(s)/guardian(s). If unable to reach a parent or guardian, parent authorizes that the person(s) listed on this card may be contacted to pick up and/or care for my child.
Section III. Medicaid Notification and Consent: If my child is covered by Medicaid and receives services under an Individual Education Plan (IEP), information may be used by the District to bill Medicaid for the following: transportation, behavioral or health services (occupational, physical, speech-language therapy, nursing, and augmentative services) as established on the IEP. IEP services are provided at no cost, regardless of consent. Parental consent may be withdrawn at any time. Any billing authorization records disclosed are available upon request. If my child is covered by Medicaid and receives services under an IEP, I consent for the District to bill Medicaid for those services provided.
Section IV. Parental Certification: I certify that the above emergency contact and health information is true and accurate to the best of my knowledge. If my child has a health condition that may require management while he/she is in school, I will inform the school principal and/or school nurse of the health condition(s) and discuss a plan of care. I understand and agree that information contained on this card, including contact information for follow-up of potential health conditions may be shared with appropriate school staff, District partners, District after-school programs, and health care professionals according to the Health Insurance Portability and Accountability Act (HIPAA).
Student Name: ___________________________________________ ID #: ____________________ Grade: _________________
_________________________ _______________________ _________________ __________ Print Name of Parent/Guardian Signature Relationship Date
DH 3040, 6/02 (Obsoletes previous editions which may not be used) Stock Number: 5744-000-3040-2
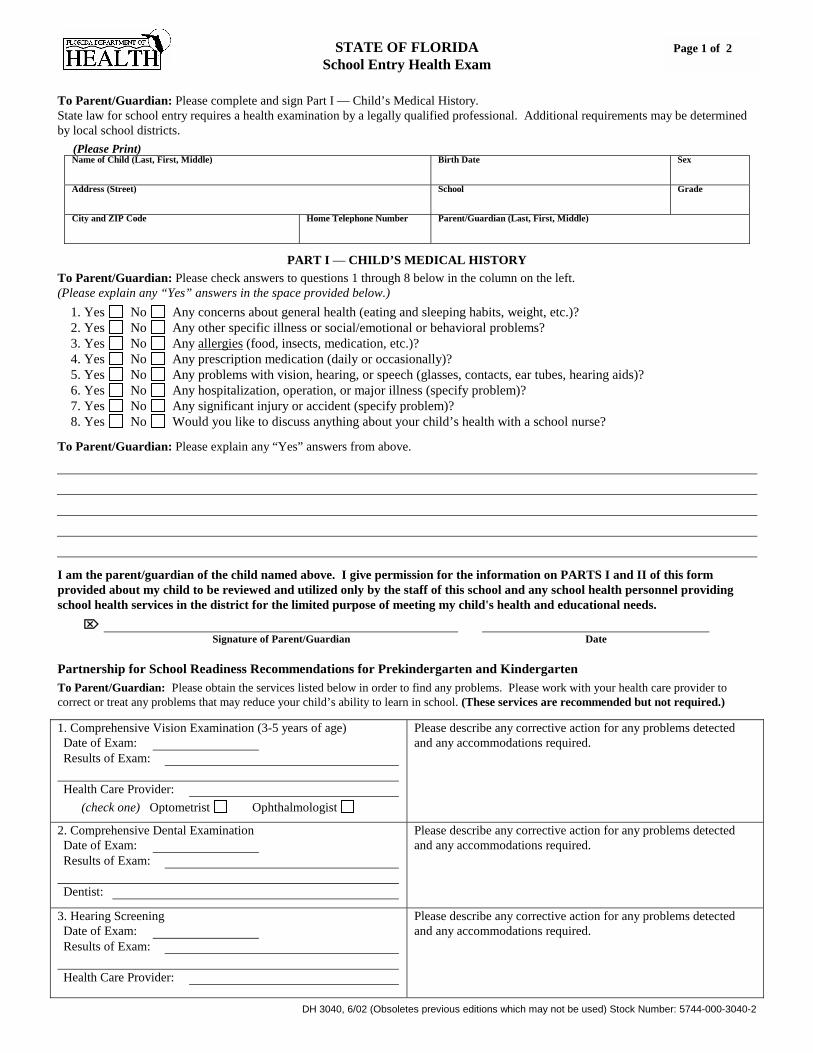
STATE OF FLORIDA School Entry Health Exam
To Parent/Guardian: Please complete and sign Part I — Child’s Medical History. State law for school entry requires a health examination by a legally qualified professional. Additional requirements may be determined by local school districts.
(Please Print) Name of Child (Last, First, Middle) Birth Date Sex
Address (Street) School Grade
City and ZIP Code Home Telephone Number Parent/Guardian (Last, First, Middle)
PART I — CHILD’S MEDICAL HISTORY To Parent/Guardian: Please check answers to questions 1 through 8 below in the column on the left. (Please explain any “Yes” answers in the space provided below.)
1. Yes No Any concerns about general health (eating and sleeping habits, weight, etc.)? 2. Yes No Any other specific illness or social/emotional or behavioral problems? 3. Yes No Any allergies (food, insects, medication, etc.)? 4. Yes No Any prescription medication (daily or occasionally)? 5. Yes No Any problems with vision, hearing, or speech (glasses, contacts, ear tubes, hearing aids)? 6. Yes No Any hospitalization, operation, or major illness (specify problem)? 7. Yes No Any significant injury or accident (specify problem)? 8. Yes No Would you like to discuss anything about your child’s health with a school nurse?
To Parent/Guardian: Please explain any “Yes” answers from above.
I am the parent/guardian of the child named above. I give permission for the information on PARTS I and II of this form provided about my child to be reviewed and utilized only by the staff of this school and any school health personnel providing school health services in the district for the limited purpose of meeting my child's health and educational needs. �
Signature of Parent/Guardian Date Partnership for School Readiness Recommendations for Prekindergarten and Kindergarten To Parent/Guardian: Please obtain the services listed below in order to find any problems. Please work with your health care provider to correct or treat any problems that may reduce your child’s ability to learn in school. (These services are recommended but not required.)
1. Comprehensive Vision Examination (3-5 years of age) Date of Exam: Results of Exam:
Health Care Provider:
(check one) Optometrist Ophthalmologist
Please describe any corrective action for any problems detected and any accommodations required.
2. Comprehensive Dental Examination Date of Exam: Results of Exam:
Dentist:
Please describe any corrective action for any problems detected and any accommodations required.
3. Hearing Screening Date of Exam: Results of Exam:
Health Care Provider:
Please describe any corrective action for any problems detected and any accommodations required.
Page 1 of 2
DH 3040, 6/02 (Obsoletes previous editions which may not be used) Stock Number: 5744-000-3040-2
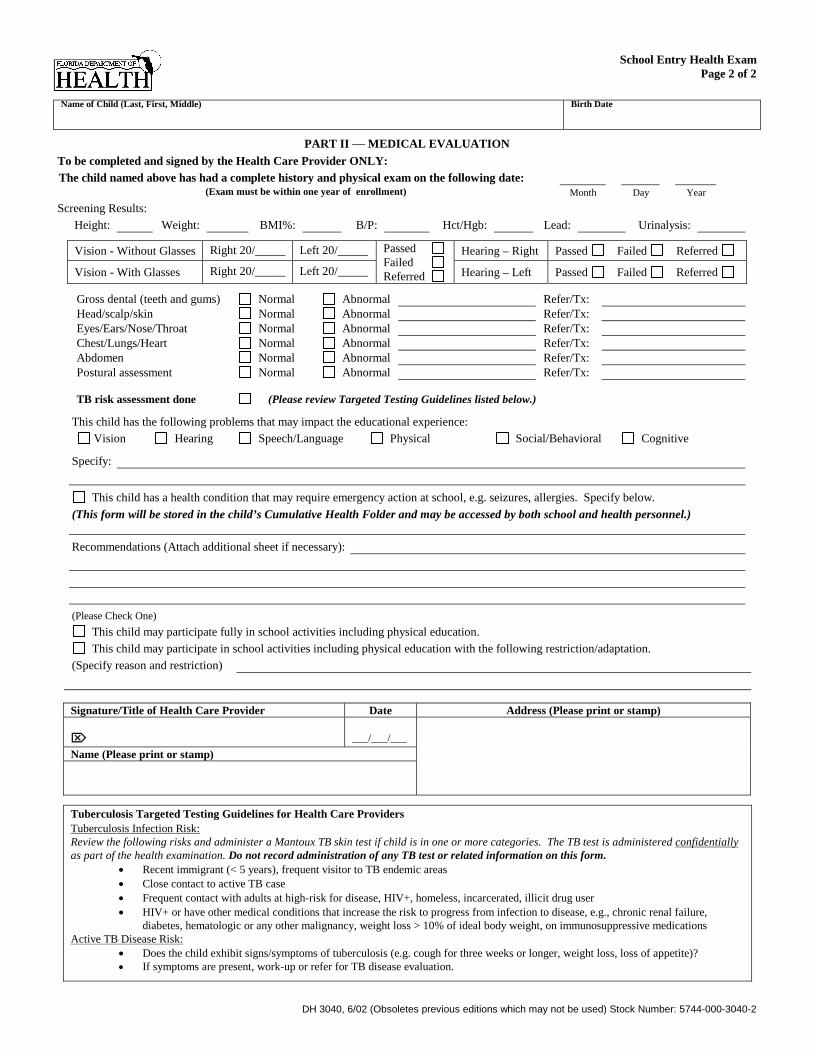
School Entry Health Exam
Page 2 of 2 Name of Child (Last, First, Middle) Birth Date
PART II — MEDICAL EVALUATION To be completed and signed by the Health Care Provider ONLY: The child named above has had a complete history and physical exam on the following date:
(Exam must be within one year of enrollment) Month Day Year Screening Results:
Height: Weight: BMI%: B/P: Hct/Hgb: Lead: Urinalysis:
Vision - Without Glasses Right 20/_____ Left 20/_____ Hearing – Right Passed Failed Referred
Vision - With Glasses Right 20/_____ Left 20/_____
Passed Failed Referred Hearing – Left Passed Failed Referred
Gross dental (teeth and gums) Normal Abnormal Refer/Tx: Head/scalp/skin Normal Abnormal Refer/Tx: Eyes/Ears/Nose/Throat Normal Abnormal Refer/Tx: Chest/Lungs/Heart Normal Abnormal Refer/Tx: Abdomen Normal Abnormal Refer/Tx: Postural assessment Normal Abnormal Refer/Tx:
TB risk assessment done (Please review Targeted Testing Guidelines listed below.)
This child has the following problems that may impact the educational experience: Vision Hearing Speech/Language Physical Social/Behavioral Cognitive
Specify:
This child has a health condition that may require emergency action at school, e.g. seizures, allergies. Specify below. (This form will be stored in the child’s Cumulative Health Folder and may be accessed by both school and health personnel.)
Recommendations (Attach additional sheet if necessary):
(Please Check One) This child may participate fully in school activities including physical education. This child may participate in school activities including physical education with the following restriction/adaptation.
(Specify reason and restriction) Signature/Title of Health Care Provider Date Address (Please print or stamp)
� ___/___/___ Name (Please print or stamp)
Tuberculosis Targeted Testing Guidelines for Health Care Providers Tuberculosis Infection Risk: Review the following risks and administer a Mantoux TB skin test if child is in one or more categories. The TB test is administered confidentially as part of the health examination. Do not record administration of any TB test or related information on this form.
�� Recent immigrant (< 5 years), frequent visitor to TB endemic areas �� Close contact to active TB case �� Frequent contact with adults at high-risk for disease, HIV+, homeless, incarcerated, illicit drug user �� HIV+ or have other medical conditions that increase the risk to progress from infection to disease, e.g., chronic renal failure,
diabetes, hematologic or any other malignancy, weight loss > 10% of ideal body weight, on immunosuppressive medications Active TB Disease Risk:
�� Does the child exhibit signs/symptoms of tuberculosis (e.g. cough for three weeks or longer, weight loss, loss of appetite)? �� If symptoms are present, work-up or refer for TB disease evaluation.















![[Center for chemical_process_safety_(ccps)]_layer_(book_fi.org)](https://img.pdfslide.us/doc/110x75/587a626d1a28ab8a2a8b47af/center-for-chemicalprocesssafetyccpslayerbookfiorg.jpg)
![CCPS Metric Pres Customizable[1]](https://img.pdfslide.us/doc/110x75/577cc37b1a28aba711961ae1/ccps-metric-pres-customizable1.jpg)











